 Lvkan Weng
Lvkan Weng Na Li
Na Li Tienan Feng
Tienan Feng Rongjia Zhu
Rongjia Zhu Zhi-Jie Zheng
Zhi-Jie Zheng
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health , 27 September 2021
Sec. Environmental Health and Exposome
Volume 9 - 2021 | https://doi.org/10.3389/fpubh.2021.716153
The epidemiological evidence on relationships between air pollution, temperature, and stroke remains inconclusive. Limited evidence is available for the effect modification by apparent temperature, an indicator reflecting reactions to the thermal environment, on short-term associations between air pollution and hospital admissions for stroke. We used a generalized additive model with Poisson regression to estimate the relative risk (RR) of stroke admissions in Shanghai, China, between 2014 and 2016 associated with air pollutants, with subgroup analyses by age, sex, apparent temperature, and season. During the study period, changes in the daily number of stroke admissions per 10 μg/m3 increase in nitrogen dioxide (at lags 0, 1, 0–1, and 0–2) ranged from 1.05 (95% CI: 0.82%, 2.88%) to 2.24% (95% CI: 0.84%, 3.65%). For each 10 μg/m3 increase in sulfur dioxide concentrations at lags 1, 2, 0–1, and 0–2, the RR of daily stroke admissions increased by 3.34 (95% CI: 0.955%, 5.79%), 0.32 (95% CI: −1.97%, 2.67%), 3.33 (95% CI: 0.38%, 6.37%), and 2.86% (95% CI: −0.45%, 6.28%), respectively. The associations of same-day exposure to nitrogen dioxide with stroke admissions remained significant after adjustment for ozone levels. These associations were not modified by sex, age, apparent temperature, or season. More research is warranted to determine whether apparent temperature modifies the associations between air pollution and stroke admissions.
Stroke is an important driver of the growing global disease burden and the second largest contributor to disability-adjusted life lost years in individuals aged over 50 years (1). China has the highest estimated lifetime risk of stroke (39.3%; 95% CI: 37.5%, 41.4%) (2), and a considerable increase in mortality and the prevalence and incidence of stroke have been observed in recent years, of which 69.6% were ischemic stroke and 23.8% were hemorrhagic stroke (3). In addition to genetic and lifestyle factors, adverse environmental factors such as air pollution and extreme temperatures have been identified as risk factors for stroke. The association of air pollution exposure with stroke incidence has been analyzed but with divergent findings by pollutant (4–6). Moreover, studies from low- and middle-income countries are relatively scarce, although the incidence and prevalence of stroke are higher in these regions (7) and air pollution is worse.
In addition, most prior reports have focused on cerebrovascular disease or ischemic stroke, while some studies examined ischemic and hemorrhagic stroke separately but reported inconsistent results (8). There are relatively few studies on hemorrhagic stroke, and the evidence remains equivocal (5, 9, 10). Climate change is another environmental concern with public health implications, in particular, for cardiovascular and cerebrovascular events (11, 12). Several studies have shown that both higher levels of air pollution and nonoptimum temperature are associated with a higher incidence of stroke (4, 5, 13–15), and other studies have suggested a possible modifying effect of temperature in associations between air pollution and stroke (11, 16). Nonetheless, these studies showed conflicting results as to whether lower temperatures or higher temperatures could enhance the effects. In addition to ambient temperature, natural factors such as relative humidity, air pressure, precipitation, and wind speed could have a significant effect on the pattern of air pollution in China (8, 17). It might be, therefore, imperative to examine the modifying effect of a biometeorological index combining several meteorological factors. Apparent temperature (AT) combined ambient temperature, humidity, and wind speed, which can be employed to evaluate the human body reactions to various thermal environments and represent the actual human perception of ambient temperature. Some studies have explored the effects of AT on several health outcomes; nevertheless, only limited evidence exists for the effect modification of AT in air pollution-stroke associations (18).
In this study, we analyzed the associations between five air pollutants (particulate matter with a diameter ≤ 10 μm [PM10], particulate matter with a diameter ≤ 2.5 μm [PM2.5], sulfur dioxide [SO2], nitrogen dioxide [NO2], and ozone [O3]) and hospital admissions for stroke in Shanghai, China, between January 2014 and December 2016. The study also examined whether the association differed by stroke subtype, patient age and sex, and AT.
The Shanghai Municipality is located in eastern China, between 120°52′-122°12′ E longitude and 30°40′-31°53′ N latitude, with a subtropical monsoon climate. Shanghai is the largest city in China and one of the most developed cities in the world as well. Shanghai has become a global financial center and a transport hub with the busiest container port in the world. Industrial production, heavy urban traffic, and a massive increase in urban population have aggravated the emission of air pollutants (19).
Data on daily stroke admissions during the study period of January 2014–December 2016 were obtained from four tertiary general hospitals with the capacity to treat patients with stroke (Shanghai First People's Hospital, The No. 10 People's Hospital of Shanghai, Renji Hospital Affiliated to Shanghai Jiao Tong University School of Medicine, and Xinhua Hospital Affiliated to Shanghai Jiao Tong University School of Medicine). These hospitals have made achievements in treating neurological disease, especially stroke, and all four hospitals have widely distributed branches in urban and suburban areas covering most districts in Shanghai (Figure 1). We collected eligible cases by reviewing the admission records and electronic medical records of the neurology department at each hospital. For this study, the date of admission, sex, age, and discharge diagnosis were extracted from the records. We identified the cause of hospital admission by the International Classification of Diseases, 10th Revision (ICD-10) code of the discharge diagnosis: total stroke (ICD-10: I60–I64), ischemic stroke (ICD-10: I63), intracerebral hemorrhage stroke (ICD-10: I61), and subarachnoid hemorrhage (ICD-10: I60). We excluded stroke cases caused by trauma, tumor, abnormal coagulation function, or infection, patients who were admitted again within 28 days, cases with missing information, and those who were not permanent residents of Shanghai.
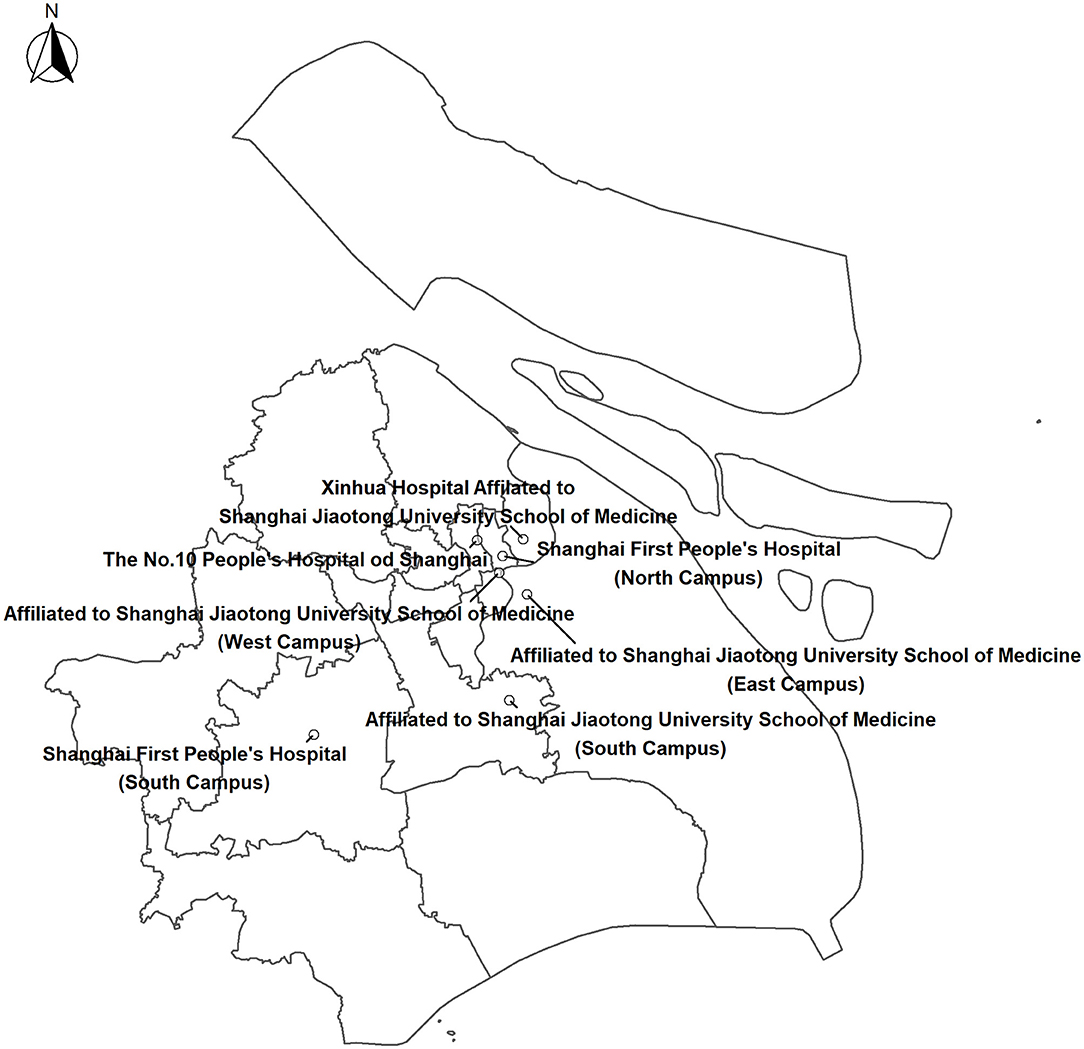
Figure 1. Locations of four tertiary hospitals in Shanghai.
Data on concentrations of PM10, PM2.5, SO2, NO2, and O3 were obtained from the National Air Pollution Monitoring System. Ten national monitoring stations are located in eight districts in Shanghai. We derived daily 24-h average concentrations of PM2.5, SO2, and NO2 and maximum 8-h average concentrations of O3, averaged across all valid monitoring sites, to represent the population exposure to ambient air pollution. We obtained daily mean levels of PM2.5, PM10, SO2, NO2, and maximum daily 8-h mean O3 concentrations averaged across the monitors. The daily mean concentration of air pollutants for each district was calculated by averaging the concentrations of all stations in that district. A series of standards or regulations exist for the locations of monitors and the monitoring process of air pollutants by the Chinese government to ensure that the monitoring measurements reflect the air pollution levels of the urban background (20). The monitoring data have been extensively used as a proxy for population exposure to air pollution in China (21). All measurement procedures complied with Ambient Air Quality Standards of China (GB3095-2012). Meteorological data, namely, daily mean temperature, relative humidity, wind speed, rainfall, and vapor pressure, were obtained from the Shanghai Meteorological Information Center, China Meteorological Bureau. The data are collected from the Shanghai Observatory (Station No. 54511) in Xuhui District, one of the national essential meteorological stations.
The AT was calculated by daily mean temperature, relative humidity, and barometric pressure using the following equations (18, 22, 23):
where T, e, and WS denote the daily mean temperature, water vapor pressure, and average wind velocity, respectively. The water vapor pressure e is calculated from Equation 2 using the daily mean temperature and relative humidity.
A generalized additive model with Poisson regression was used to estimate the RR of stroke admissions associated with air pollutants. The potential confounding covariates were incorporated into the model, namely, temperature, relative humidity, public holidays, and day of the week, and were predefined by previously published studies. The potential confounding effects of weather, seasonality, and long-term patterns were controlled by smoothing functions (natural cubic splines). Specifically, we introduced the following covariates into the models: (1) a natural cubic spline smoother of calendar day with 7 degrees of freedom (df) per year; (2) natural cubic spline smoothers of the temperature on the same day as admission with 3 df; (3) natural cubic spline smoothers of the relative humidity with 3 df; and (4) indicator variables for the day of the week and public holidays. The df values for a calendar day, temperature, and relative humidity were selected by the parameters used in the previous studies (21, 24, 25). Consequently, the regression model was constructed as follows:
where E(Yt) is the expected count of admissions for ischemic stroke on day t; β represents the log-RR of ischemic stroke associated with a unit increase in air pollutant levels, and ns() indicates natural cubic spline function. Public holidays and days of the week were included in the model as indicator variables, and temperature and relative humidity indicate current-day air temperature and relative humidity, respectively. We used same-day air pollutant concentrations (lag 0) in our main analyses because lag 0 often produces the largest effect estimates (4, 17, 26, 27).
To investigate the lag effect associated with air pollutants, we used the following lag periods: single-day lags (the same day [lag 0], the previous day [lag 1], and the day before the previous day [lag 2]) and multiday lags (average concentration of the same day and previous day [lag 0–1], and average concentration of the same day and previous two days [lag 0–2]). Subgroup analyses were performed to examine whether the association differed by age (<65 years and ≥65 years), sex, AT (cool days: ≤ 19.6°C, warm days: >19.6°C; and median temperature used as the cutoff), and season (April–September, warm season; October–March, cool season). We used a Z test to compare differences in the association between subgroups (28). In addition to the single-pollutant model, we also assessed potential confounding by other pollutants by establishing a series of two-pollutant models. To avoid collinearity caused by high correlativity between pollutants, we incorporated O3 into the two-pollutant model using Spearman's correlation coefficients between air pollutants.
All results are reported as percentage changes and 95% CIs in daily hospital admissions for ischemic stroke, in association with increases of 10 μg/m3 in the levels of PM2.5, SO2, NO2, and O3. All analyses were conducted in R version 4.0.3 (R Foundation for Statistical Computing, Vienna, Austria).
This study was approved by the Ethics Committee of the School of Public Health, Shanghai Jiao Tong University. The health information was primarily hospital-specific daily counts of admissions, i.e., overall summarized data and stratified by age and sex subgroups without any individual identifiers. The need for informed consent was therefore waived by the institutional review board.
We identified a total of 18,651 hospital admissions for stroke in four general hospitals in Shanghai between 2014 and 2016, namely, 15,554 admissions for ischemic stroke, 2,888 admissions for intracerebral hemorrhage stroke, and 209 admissions for subarachnoid hemorrhage. Table 1 summarizes the characteristics of daily hospital admissions for stroke. On average, in these four hospitals, there were 17 admissions for stroke per day over the study period. More than half of the patients (62.5%) were men and 53.8% were aged ≥65 years. The number of stroke admissions during cool days (9,250 admissions) was similar to the number of stroke admissions during warm days (9,341 admissions).
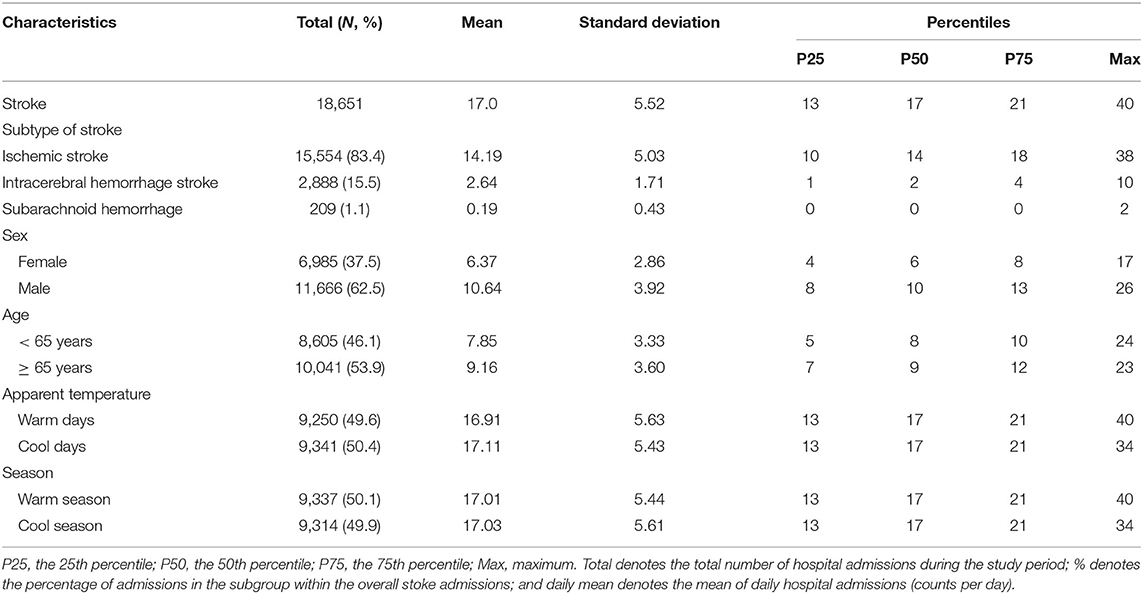
Table 1. Summary statistics of daily hospital admissions for stroke in four hospitals in Shanghai, 2014–2016.
Table 2 presents the summary statistics of air pollutants and meteorological variables in Shanghai between 2014 and 2016. The average AT for Shanghai was 18.67°C and peaked at 40.02°C, which is slightly higher than a mean of 18.02°C and maximum of 34.5°C for ambient temperature. The wider range of ATs compared with the ambient temperature can be explained that including wind speed and humidity described the perceived thermal environment more correctly. The annual means (SD) of air pollutants were 50.18 (32.2) μg/m3 for PM2.5, 70.16 (39.24) μg/m3 for PM10, 44.29 (20.07) μg/m3 for NO2, 16.44 (9.01) μg/m3 for SO2, and 91.14 (43.2) μg/m3 for O3 (Figure 2). Supplementary Table 1 lists the summary statistics of 7-day average concentrations of air pollutants. On warm days (AT >19.56°C), the means of PM2.5, PM10, NO2, and SO2 concentrations were higher than in the means on cool days (AT ≤ 19.56°C), while the average levels of O3 on warm days were lower than on cool days.
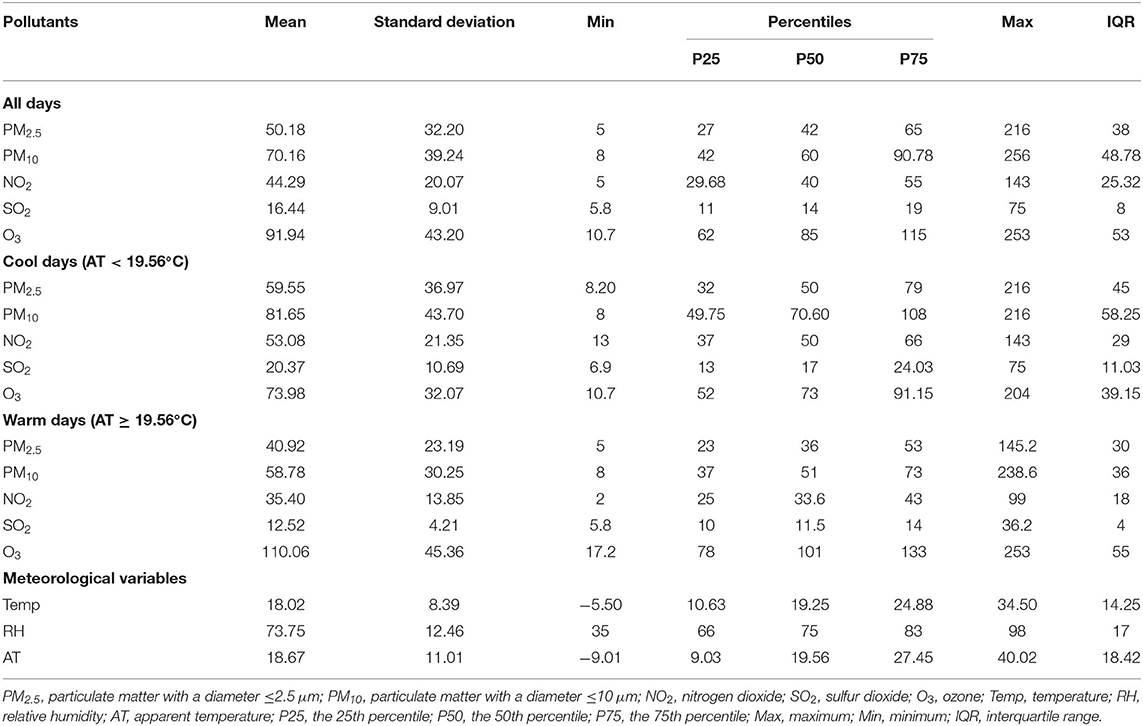
Table 2. Summary statistics of air pollutants and meteorological variables in Shanghai, 2014–2016.
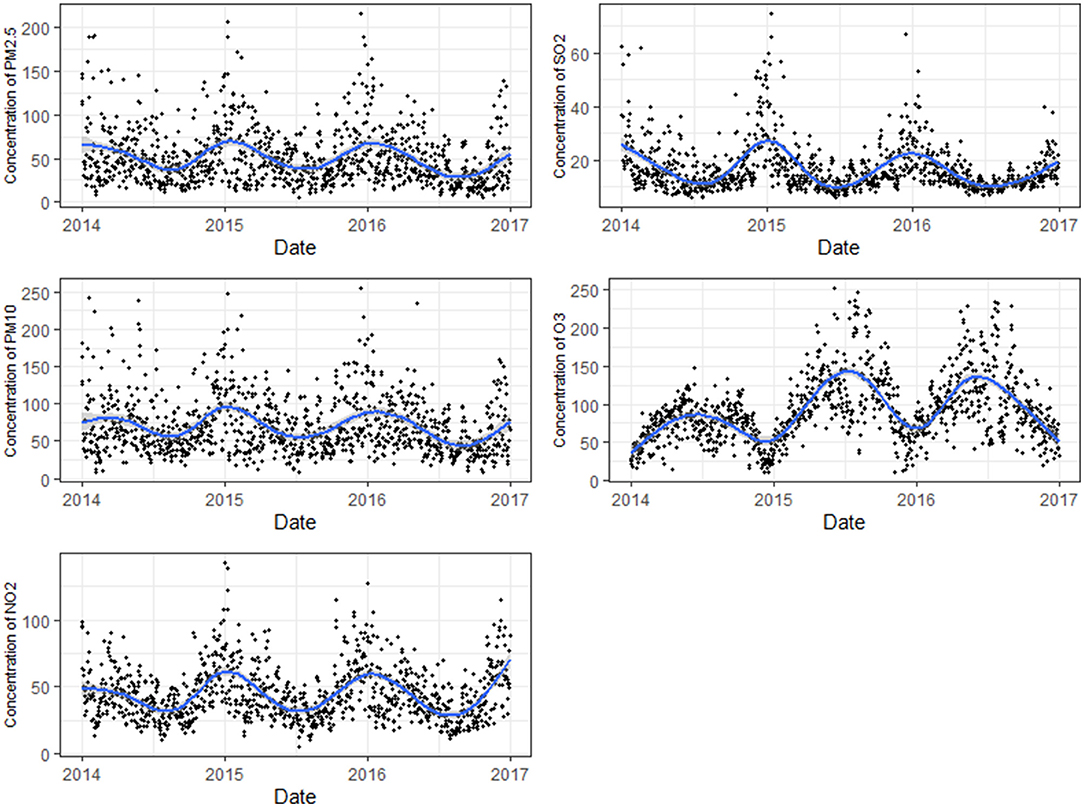
Figure 2. Concentrations of air pollutants in Shanghai during 2014–2016.
Table 3 lists Spearman's correlation coefficients for exposure variables. PM2.5 was highly correlated with PM10 (r = 0.92, P < 0.001). PM2.5, PM10, NO2, and SO2 were moderately correlated with each other (median r = 0.70, P < 0.001), while O3 levels were weakly negatively correlated with NO2 and SO2 and not correlated with PM2.5 (r = 0.02, P > 0.05) and PM10 (r = 0.06, P < 0.001). Ambient temperature, relative humidity, and AT were all negatively correlated with all air pollutants except O3.
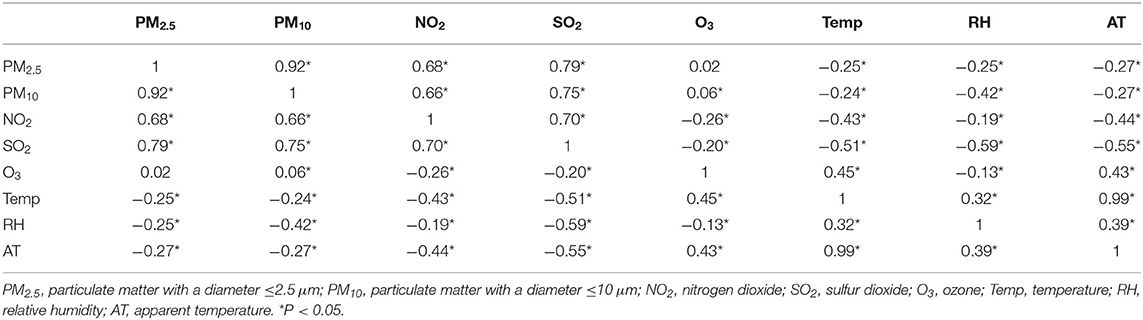
Table 3. Spearman's correlation coefficients between exposure variables.
Figure 3 and Supplementary Table 2 present the percentage changes in hospital admissions for stroke with single-day lags of 0, 1, and 2 days and lags of 0–1 and 0–2 days associated with a 10 μg/m3 increase in the levels of the five air pollutants. Overall, NO2 and SO2 were consistently and significantly associated with hospital admissions for all types of stroke. Increases of 10 μg/m3 in concurrent-day PM2.5, PM10, SO2, NO2, and O3 levels corresponded to 0.2 (95% CI: −0.36%, 0.76%), 0.3% (95% CI: −0.17%, 0.78%), 1.05 (95% CI: 0.03%, 2.08%), 0.9 (95% CI: −1.53%, 3.39%), and 0.4% (95% CI: −0.2%, 1.01%) increases in hospital admissions for stroke, respectively. A significant lag effect of NO2 and SO2 exposure on stroke admissions was also observed. For NO2, the estimated effects were significant for same-day, prior-day, and moving average of lags 0–1 and 0–2 exposure, with the largest effect size observed for moving average of lag 0–2. Percent changes in the daily number of stroke admissions per 10 μg/m3 increase in NO2 ranged from 1.05 (95% CI: 0.82%, 2.88%) to 2.24% (95% CI: 0.84%, 3.65%). For SO2, the largest effect estimates were observed for a prior-day exposure. For each 10 μg/m3 increase in SO2 concentrations at lags 1, 2, 0–1, and 0–2, the RR of daily stroke admissions increased by 3.34 (95% CI: 0.955%, 5.79%), 0.32 (95% CI: −1.97%, 2.67%), 3.33 (95% CI: 0.38%, 6.37%), and 2.86% (95% CI: −0.45%, 6.28%), respectively. We did not observe significant lag effects for exposure to PM2.5, PM10, or O3. In the two-pollutant models, effect estimates for same-day exposure to NO2 were largely unchanged, but the effects of same-day exposure to SO2 became statistically insignificant when controlling for the effect of O3 (Table 4).
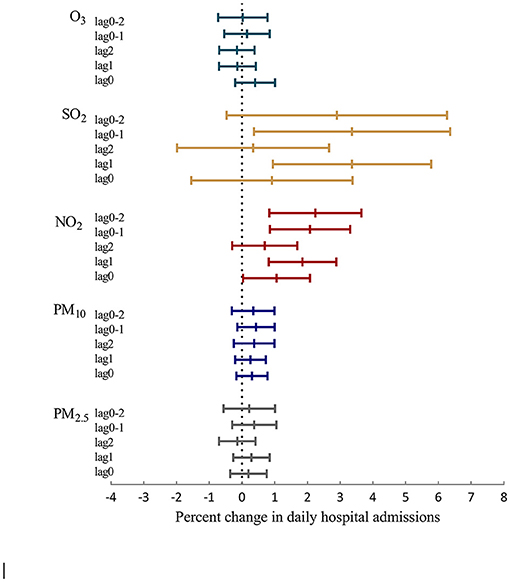
Figure 3. Percentage changes and 95% CIs in daily hospital admissions for stroke per 10 μg/m3 increase in PM2.5, PM10, NO2, SO2, and O3 concentrations at different lag days.
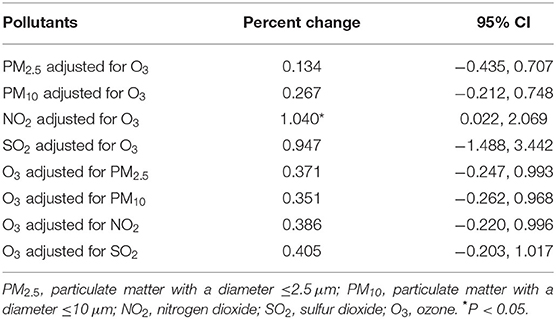
Table 4. Percent changes in daily hospital admissions for ischemic stroke associated with a 10 μg/m3 increase in air pollutant concentrations in two-pollutant models.
Figure 4 and Supplementary Table 3 show the associations between air pollutant levels (lag 0) and admissions for ischemic stroke stratified by sex, age, stroke subtype, AT, and season. We did not observe evidence for effect modification by these characteristics. Table 4 lists the results from the two-pollutant models.
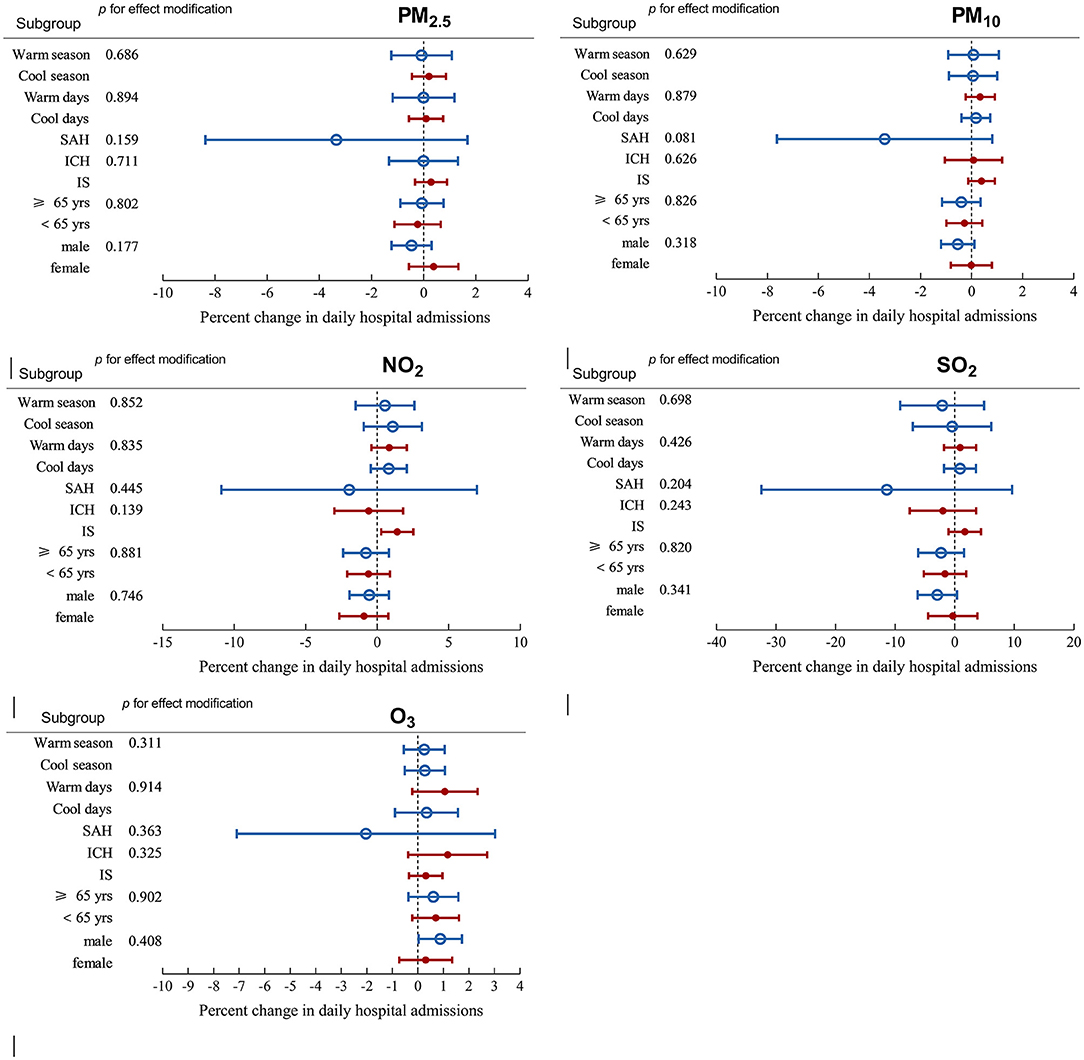
Figure 4. Percentage changes with 95% CIs in hospital admissions for stroke with 10 μg/m3 increase in particulate matter with a diameter ≤ 2.5 μm (PM2.5), particulate matter with a diameter ≤ 10 μm (PM10), nitrogen dioxide (NO2), sulfur dioxide (SO2), and ozone (O3) on lag 0 stratified by sex, age, apparent temperature, and season. The first column from the left in each panel indicates the subgroup and the second column indicates the P value generated from the Z test.
Overall, our findings indicated that transient increases in SO2 and NO2 were associated with increased hospitalization for stroke in the single-pollutant models. The association between the NO2 levels and hospitalization for stroke remained significant in the two-pollutant models. However, we did not find evidence that the associations were modified by sex, age, season, or AT. Our findings add to the body of knowledge on the acute effects of air pollution on stroke in low- and middle-income countries. Although the magnitude of association appears to be relatively small, the public health burden derived from the risk could be substantial. The study could strengthen the rationale for reducing concentrations of air pollutants in megacities in low- and middle-income countries.
We found that prior 1- or 2-day exposure to NO2 and SO2 was positively associated with increased risk of hospital admission for stroke in the single-pollutant model, in general accordance with prior studies (6, 17, 29–33). However, the biological mechanisms underlying these perceived associations are unknown, and most studies have focused on the effects of particulate matter. Several potential mechanistic pathways have been proposed, namely, systemic inflammation (34, 35), thrombosis, (36–38) artery calcification (39), and vascular endothelial dysfunction (40). Some controlled studies have indicated that exposure to air pollutants (namely, NO2 and SO2) could adversely affect vascular endothelial function, increase systemic inflammation and platelet activation and the activity of the sympathetic nervous system, and decrease the activity of antioxidant enzymes. These effects may result in vasoconstriction, elevated blood pressure, ischemia, and risk of thrombosis (38, 41, 42). Another plausible mechanism of action is atrial arrhythmia, which may predispose patients to thromboembolic events (6).
Epidemiological studies of short-term exposure to air pollution and hospital admissions for stroke have generated inconclusive results (43). A 2021 systematic review and meta-analysis reported that 10 μg/m3 increases in the concentrations of all five pollutants were associated with hospital admissions for stroke; odds ratios ranged from 1.002 for O3 to 1.023 for NO2. However, these odds ratios are all very close to 1, indicating no association. Additionally, a meta-analysis published in 2015 observed robust and clear associations between both gaseous (RR 1.019 per 10 ppb increase in SO2, 95% CI: 1.011–1.027; RR 1.014 per 10 ppb increase in NO2, 95% CI: 1.009–1.019) and particulate air pollution (1.011 per 10 μg/m3 (1.011–1.012) for PM2.5 and 1.003 per 10 μg/m3 (1.002–1.004) for PM10). This study also noticed significant heterogeneity across pollutants that could be attributed to different study designs, different exposure lags, systemic differences in the baseline characteristics of the underlying population, misclassification of exposure measurement, and a different definition of stroke cases (6).
For example, a study conducted among individuals aged > 65 in the United States reported that interquartile range increases in same-day concentrations of PM10 (22.96 μg/m3), NO2 (11.93 μg/m3), and SO2 (6.96 ppb) concentrations that were associated with 1.03, 2.94, and 1.35% increases in admissions for ischemic stroke admissions, respectively (44). Epidemiological studies in numerous cities in China have also provided evidence of elevated risk of stroke or mortality associated with increases in daily concentrations of these air pollutants (8, 21, 29, 32, 45, 46). However, a study conducted in eight cities in France did not find an association between short-term exposure to air pollution and stroke (47). A nonsignificant increase in emergency hospital admissions for stroke related to particulate air pollutants was reported for one hospital in Taipei (46). Similarly, a case-crossover study in seven cities in Australia and New Zealand failed to observe associations between air pollutant levels and stroke among elderly individuals (48). The heterogeneity of results may be attributable to geographic variations, differences in pollutant concentrations, outcomes measured, population susceptibility, and the sources and constituents of the pollutants. For example, the greater adverse effects of PM2.5 and PM10 observed in other studies may be partly attributable to the relatively higher levels of particulate pollution at those study sites. According to Huang et al. (8) the median concentration of PM2.5 and PM10 in 2013–2014 in Beijing (a typical northern city in China) was 71.4 and 105.4 μg/m3, respectively, notably higher than the 50.2 and 70.2 μg/m3 in Shanghai (a typical southern city) in this study. Additionally, we only observed short-term associations of NO2 and SO2 with the risk of hospital admission for stroke; as the most densely populated city in China, pollution sources of Shanghai are mainly the gaseous emissions from motor vehicles, explaining why the effects of NO2 and SO2 were much more evident in our study than those of particulate pollutants.
We did not observe differences in the effect between warm days (AT > 19.6°C) and cool days (AT ≤ 19.6°C). Several studies have reported mixed results on the effect modification by temperature in air pollution-stroke associations. A study examining the associations between air pollutant levels and hospital admissions for transient ischemic attack reported that the effects of PM2.5, PM10, SO2, and O3 were more pronounced on warm days. Huang and colleagues reported that the positive associations of PM2.5 and PM10 with hospital admissions for both ischemic and hemorrhagic stroke were higher on warm days (>13.5°C) 0.8 Similar findings were also reported in studies of stroke admissions and cause-specific mortality in Taipei, Tianjin (China), and Canada (49–51). However, a study in Wuhan reported an association of NO2 with stroke only during the cold season (52). A national-scale in China reported a stronger association for ischemic stroke in the cool season than in the warm season (8). These findings perhaps indicated the combined effects of temperature, high levels of air pollution, and variations in ventilation conditions across seasons, or reflected seasonal differences in chemical compositions and toxicological characteristics of air pollutants (5, 8). In addition, stronger association on warm days could be explained that high ambient temperature may accelerate the emission, play an important role in determining transportation, dilution, chemical transformation of pollutants, and influence the eventual deposition. Besides, people tend to spend more time outdoors on warm days, resulting in more exposure to ambient air pollution (8, 17). Unlike the previous studies, which considered ambient temperature, we used AT to define warm/cool days. Combining temperature, humidity, and wind speed, AT can represent thermal comfort. Humidity conditions and wind could affect mechanisms of heat exchange to maintain homeostasis under heat-stress situations (53). The previous study reported that the air temperature alone seemed to overestimate the potential risks while the combination of air temperature, humidity, and wind speed adjusts the exposure to the thermal environment better (53, 54). Perspiration regulates body temperature, and high humidity may impair heat-exchange efficiency by reducing the rate of moisture evaporation from skin surfaces. At the same time, the convective rate is enhanced under windy conditions. However, we did not detect an effect modification by AT in associations between air pollution and stroke admissions, perhaps because of the relatively small number of admissions, the limited study duration, and the single-city study design. As a recent review suggested, the evaluation of the interaction between temperature and air quality and assessment of both on human health still retain some uncertainties (11). Thus, well-designed and multicenter studies with large samples are warranted to investigate these relationships.
There are several limitations to our study. First, the admission date may result in temporal misalignment between exposure and outcome, as the onset of stroke symptoms often began in the days before admission. Second, we used average city-wide concentrations of air pollutants rather than individual exposure, which may lead to exposure measurement errors and a more conservative conclusion. Third, the current study did not consider the direct association of AT with stroke outcomes because previous studies have suggested that temperature affects air pollution rather than the reverse (55). However, there may be synergistic effects of ambient temperature and air pollution on health (12). Therefore, further analysis is warranted to check the interaction between ambient air pollution and AT on health outcomes. Fourth, we dichotomized days as cool/warm days using median AT, which may have diluted the potential effect modification of temperature. Future studies with larger samples could classify days according to the distribution (percentiles) of temperature, which may assist in elucidating the effect modification. Finally, we used mean values of all monitoring sites as air pollution exposure levels and did not consider potential variations within the city, which might dilute the exposure levels in some districts with high levels of air pollution.
We found that elevated levels of NO2 and SO2 were associated with an increase in hospital admissions for stroke, with a significant lag effect. Further research is warranted to determine whether AT modifies the associations between air pollution and admissions for stroke. This study adds to the available evidence in megacities in low- and middle-income countries and may promote the development of related public health policy.
The data analyzed in this study is subject to the following licenses/restrictions: The data on hospital admission was derived from hospitals, which cannot be public. Requests to access these datasets should be directed to a2V2aW53bGsyMUAxMjYuY29t.
The studies involving human participants were reviewed and approved by Ethics Committee of School of Public Heath Shanghai Jiao Tong University. The ethics committee waived the requirement of written informed consent for participation.
Z-JZ and LW: conceptualization and validation. NL: methodology, software, formal analysis, and visualization. TF: investigation. RZ: resources. TF and RZ: data curation. LW: original draft preparation. Z-JZ and NL: review and editing. Z-JZ: supervision. All authors have read and agreed to the published version of the manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2021.716153/full#supplementary-material
CI, confidence interval; df, degree of freedom; NO2, nitrogen dioxide; PM2.5, particulate matter with a diameter ≤ 2.5 μm; PM10, particulate matter with a diameter ≤ 10 μm; SO2, sulfur dioxide.
1. GBD 2019 Diseases and Injuries Collaborators. Global burden of 369 diseases and injuries in 204 countries and territories, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet. (2020) 396:1204–22. doi: 10.1016/S0140-6736(20)30925-9
2. Feigin VL, Nguyen G, Cercy K, Johnson CO, Alam T, Parmar PG, et al. Global, regional, and country-specific lifetime risks of stroke, 1990 and 2016. N Engl J Med. (2018) 379:2429–37. doi: 10.1056/NEJMoa1804492
3. Wang WZ, Jiang B, Sun HX, Ru XJ, Sun DL, Wang LH, et al. Prevalence, incidence, and mortality of stroke in china results from a nationwide population-based survey of 480 687 adults. Circulation. (2017) 135:759. doi: 10.1161/CIRCULATIONAHA.116.025250
4. Ban J, Wang Q, Ma R, Zhang Y, Shi W, Zhang Y, et al. Associations between short-term exposure to PM2 5 and stroke incidence and mortality in China: A case-crossover study and estimation of the burden. Environ Pollut. (2021) 268:115743. doi: 10.1016/j.envpol.2020.115743
5. Gu J, Shi Y, Chen N, Wang H, Chen T. Ambient fine particulate matter and hospital admissions for ischemic and hemorrhagic strokes and transient ischemic attack in 248 Chinese cities. Sci Total Environ. (2020) 715:136896. doi: 10.1016/j.scitotenv.2020.136896
6. Shah AS, Lee KK, McAllister DA, Hunter A, Nair H, Whiteley W, et al. Short term exposure to air pollution and stroke: systematic review and meta-analysis. BMJ. (2015) 350:h1295. doi: 10.1136/bmj.h1295
7. Li ZX, Jiang Y, Li H, Xian Y, Wang YJ. China's response to the rising stroke burden. BMJ-British Medical Journal. (2019) 364:7. doi: 10.1136/bmj.l879
8. Huang F, Luo Y, Guo Y, Tao L, Xu Q, Wang C, et al. Particulate matter and hospital admissions for stroke in Beijing, China: modification effects by ambient temperature. J Am Heart Assoc. (2016) 5:e003437. doi: 10.1161/JAHA.116.003437
9. Ljungman PL, Mittleman MA. Ambient air pollution and stroke. Stroke. (2014) 45:3734–41. doi: 10.1161/STROKEAHA.114.003130
10. Chiu H-F, Chang C-C, Yang C-Y. Relationship between hemorrhagic stroke hospitalization and exposure to fine particulate air pollution in Taipei, Taiwan. J Toxicol Environ Health A. (2014) 77:1154–63. doi: 10.1080/15287394.2014.926801
11. Lou J, Wu Y, Liu P, Kota SH, Huang L. Health effects of climate change through temperature and air pollution. Current Pollution Reports. (2019) 5:144–58. doi: 10.1007/s40726-019-00112-9
12. Analitis A, De' Donato F, Scortichini M, Lanki T, Basagana X, Ballester F, et al. Synergistic effects of ambient temperature and air pollution on health in Europe: results from the PHASE project. Int J Environ Res Public Health. (2018) 15:1856. doi: 10.3390/ijerph15091856
13. Hirel C, Berton L, Preda C, Richard O, Lambert Y, Pico F. Air pollution and humidity as triggering factors for stroke. Results of a 12-year analysis in the West Paris area. Rev Neurol (Paris). (2019) 175:614–8. doi: 10.1016/j.neurol.2019.03.002
14. Hsu WH, Hwang SA, Kinney PL, Lin S. Seasonal and temperature modifications of the association between fine particulate air pollution and cardiovascular hospitalization in New York state. Sci Total Environ. (2017) 578:626–32. doi: 10.1016/j.scitotenv.2016.11.008
15. Yang J, Yin P, Zhou M, Ou CQ, Li M, Li J, et al. The burden of stroke mortality attributable to cold and hot ambient temperatures: Epidemiological evidence from China. Environ Int. (2016) 92–93:232–8. doi: 10.1016/j.envint.2016.04.001
16. Zanobetti A, Peters A. Disentangling interactions between atmospheric pollution and weather. J Epidemiol Community Health. (2015) 69:613. doi: 10.1136/jech-2014-203939
17. Guo P, Wang Y, Feng W, Wu J, Fu C, Deng H, et al. Ambient air pollution and risk for ischemic stroke: a short-term exposure assessment in South China. Int J Environ Res Public Health. (2017) 14:1091. doi: 10.3390/ijerph14091091
18. Steadman RG. Norms of apparent temperature in Australia. Australian Meteorological Magazine. (1994) 43:1–16.
19. Available, online at: www.gov.cn. 2021.
20. Zhao B, Su Y, He S, Zhong M, Cui G. Evolution and comparative assessment of ambient air quality standards in China. J Integr Environ Sci. (2016) 13:85–102. doi: 10.1080/1943815X.2016.1150301
21. Tian Y, Liu H, Zhao Z, Xiang X, Li M, Juan J, et al. Association between ambient air pollution and daily hospital admissions for ischemic stroke: A nationwide time-series analysis. PLoS Med. (2018) 15:e1002668. doi: 10.1371/journal.pmed.1002668
22. Krstic G. Apparent temperature and air pollution vs. elderly population mortality in metro vancouver. PLoS ONE. (2011) 6:e25101. doi: 10.1371/journal.pone.0025101
23. Niu Y, Gao Y, Yang J, Qi L, Xue T, Guo M, et al. Short-term effect of apparent temperature on daily emergency visits for mental and behavioral disorders in Beijing, China: A time-series study. Sci Total Environ. (2020) 733:139040. doi: 10.1016/j.scitotenv.2020.139040
24. Chen R, Yin P, Meng X, Liu C, Wang L, Xu X, et al. Fine particulate air pollution and daily mortality. A nationwide analysis in 272 Chinese cities. Am J Respir Crit Care Med. (2017) 196:73–81. doi: 10.1164/rccm.201609-1862OC
25. Dominici F, Peng RD, Bell ML, Pham L, McDermott A, Zeger SL, et al. Fine particulate air pollution and hospital admission for cardiovascular and respiratory diseases. JAMA. (2006) 295:1127–34. doi: 10.1001/jama.295.10.1127
26. Zhang R, Jiang Y, Zhang G, Yu M, Wang Y, Liu G. Association between short-term exposure to ambient air pollution and hospital admissions for transient ischemic attacks in Beijing, China. Environ Sci Pollut Res Int. (2021) 28:6877–85. doi: 10.1007/s11356-020-10963-1
27. Liu C, Yin P, Chen R, Meng X, Wang L, Niu Y, et al. Ambient carbon monoxide and cardiovascular mortality: a nationwide time-series analysis in 272 cities in China. The Lancet Planetary Health. (2018) 2:e12–8. doi: 10.1016/S2542-5196(17)30181-X
28. Altman DG, Bland JM. Statistics Notes - Interaction revisited: the difference between two estimates. BMJ. (2003) 326:219–219. doi: 10.1136/bmj.326.7382.219
29. Huang F, Luo Y, Tan P, Xu Q, Tao L, Guo J, et al. Gaseous Air pollution and the risk for stroke admissions: a case-crossover study in Beijing, China. Int J Environ Res Public Health. (2017) 14:189. doi: 10.3390/ijerph14020189
30. Tian Y, Liu H, Liang T, Xiang X, Li M, Juan J, et al. Fine particulate air pollution and adult hospital admissions in 200 Chinese cities: a time-series analysis. Int J Epidemiol. (2019) 48:1142–51. doi: 10.1093/ije/dyz106
31. Wang Z, Peng J, Liu P, Duan Y, Huang S, Wen Y, et al. Association between short-term exposure to air pollution and ischemic stroke onset: a time-stratified case-crossover analysis using a distributed lag nonlinear model in Shenzhen, China. Environ Health. (2020) 19:1. doi: 10.1186/s12940-019-0557-4
32. Liu H, Tian Y, Xu Y, Huang Z, Huang C, Hu Y, et al. Association between ambient air pollution and hospitalization for ischemic and hemorrhagic stroke in China: A multicity case-crossover study. Environ Pollut. (2017) 230:234–41. doi: 10.1016/j.envpol.2017.06.057
33. O'Donnell MJ, Xavier D, Liu L, Zhang H, Chin SL, Rao-Melacini P, et al. Risk factors for ischaemic and intracerebral haemorrhagic stroke in 22 countries (the INTERSTROKE study): a case-control study. Lancet. (2010) 376:112–23. doi: 10.1016/S0140-6736(10)60834-3
34. Rich DQ, Kipen HM, Huang W, Wang G, Wang Y, Zhu P, et al. Association between changes in air pollution levels during the Beijing Olympics and biomarkers of inflammation and thrombosis in healthy young adults. JAMA. (2012) 307:2068–78. doi: 10.1001/jama.2012.3488
35. Mills NL, Tornqvist H, Robinson SD, Gonzalez M, Darnley K, MacNee W, et al. Diesel exhaust inhalation causes vascular dysfunction and impaired endogenous fibrinolysis. Circulation. (2005) 112:3930–6. doi: 10.1161/CIRCULATIONAHA.105.588962
36. Bind M-A, Baccarelli A, Zanobetti A, Tarantini L, Suh H, Vokonas P et al. Air Pollution and Markers of Coagulation, Inflammation, and Endothelial Function: Associations and Epigene-environment Interactions in an Elderly Cohort. Epidemiology. (2012) 23:332–40. doi: 10.1097/EDE.0b013e31824523f0
37. Franchini M, Mannucci PM. Thrombogenicity and cardiovascular effects of ambient air pollution. Blood. (2011) 118:2405–12. doi: 10.1182/blood-2011-04-343111
38. Lucking AJ, Lundback M, Mills NL, Faratian D, Barath SL, Pourazar J, et al. Diesel exhaust inhalation increases thrombus formation in man†. Eur Heart J. (2008) 29:3043–51. doi: 10.1093/eurheartj/ehn464
39. Kaufman JD, Adar SD, Barr RG, Budoff M, Burke GL, Curl CL, et al. Association between air pollution and coronary artery calcification within six metropolitan areas in the USA (the Multi-Ethnic Study of Atherosclerosis and Air Pollution): a longitudinal cohort study. Lancet. (2016) 388:696–704. doi: 10.1016/S0140-6736(16)00378-0
40. Törnqvist H, Mills NL, Gonzalez M, Miller MR, Robinson SD, Megson IL, et al. Persistent endothelial dysfunction in humans after diesel exhaust inhalation. Am J Respir Crit Care Med. (2007) 176:395–400. doi: 10.1164/rccm.200606-872OC
41. Mills NL, Miller MR, Lucking AJ, Beveridge J, Flint L, Boere AJF, et al. Combustion-derived nanoparticulate induces the adverse vascular effects of diesel exhaust inhalation. Eur Heart J. (2011) 32:2660–71. doi: 10.1093/eurheartj/ehr195
42. Lucking AJ, Lundback M, Barath SL, Mills NL, Sidhu MK, Langrish JP, et al. Particle traps prevent adverse vascular and prothrombotic effects of diesel engine exhaust inhalation in men. Circulation. (2011) 123:1721–U66. doi: 10.1161/CIRCULATIONAHA.110.987263
43. Niu Z, Liu F, Yu H, Wu S, Xiang H. Association between exposure to ambient air pollution and hospital admission, incidence, and mortality of stroke: an updated systematic review and meta-analysis of more than 23 million participants. Environ Health Prev Med. (2021) 26:15. doi: 10.1186/s12199-021-00937-1
44. Wellenius GA, Schwartz J, Mittleman MA. Air pollution and hospital admissions for ischemic and hemorrhagic stroke among medicare beneficiaries. Stroke. (2005) 36:2549–53. doi: 10.1161/01.STR.0000189687.78760.47
45. Liu H, Tian Y, Xu Y, Zhang J. Ambient particulate matter concentrations and hospitalization for stroke in 26 Chinese cities:a case-crossover study. Stroke. (2017) 48:2052–9. doi: 10.1161/STROKEAHA.116.016482
46. Chan C-C, Chuang K-J, Chien L-C, Chen W-J, Chang W-T. Urban air pollution and emergency admissions for cerebrovascular diseases in Taipei, Taiwan. Eur Heart J. (2006) 27:1238–44. doi: 10.1093/eurheartj/ehi835
47. Larrieu S, Jusot J-F, Blanchard M, Prouvost H, Declercq C, Fabre P, et al. Short term effects of air pollution on hospitalizations for cardiovascular diseases in eight French cities: The PSAS program. Sci Total Environt. (2007) 387:105–12. doi: 10.1016/j.scitotenv.2007.07.025
48. Barnett AG, Williams GM, Schwartz J, Best TL, Neller AH, Petroeschevsky AL, et al. The effects of air pollution on hospitalizations for cardiovascular disease in elderly people in Australian and New Zealand cities. Environ Health Perspect. (2006) 114:1018–23. doi: 10.1289/ehp.8674
49. Tsai SS, Goggins WB, Chiu HF, Yang CY. Evidence for an association between air pollution and daily stroke admissions in Kaohsiung, Taiwan. Stroke. (2003) 34:2612–6. doi: 10.1161/01.STR.0000095564.33543.64
50. Qi X, Wang Z, Guo X, Xia X, Xue J, Jiang G, et al. Short-term effects of outdoor air pollution on acute ischaemic stroke occurrence: a case-crossover study in Tianjin, China. Occup Environ Med. (2020) 77:862. doi: 10.1136/oemed-2019-106301
51. Villeneuve PJ, Chen L, Stieb D, Rowe BH. Associations between outdoor air pollution and emergency department visits for stroke in Edmonton, Canada. Eur J Epidemiol. (2006) 21:689–700. doi: 10.1007/s10654-006-9050-9
52. Xiang H, Mertz KJ, Arena VC, Brink LL, Xu X, Bi Y, et al. Estimation of short-term effects of air pollution on stroke hospital admissions in Wuhan, China. PLoS ONE. (2013) 8:e61168. doi: 10.1371/journal.pone.0061168
53. Roye D, Zarrabeitia MT, Riancho J, Santurtun A. A time series analysis of the relationship between apparent temperature, air pollutants and ischemic stroke in Madrid, Spain. Environ Res. (2019) 173:349–58. doi: 10.1016/j.envres.2019.03.065
54. Basu R, Gavin L, Pearson D, Ebisu K, Malig B. Examining the association between apparent temperature and mental health-related emergency room visits in California. Am J Epidemiol. (2018) 187:726–35. doi: 10.1093/aje/kwx295
55. Xu R, Zhao Q, Coelho MSZS, Saldiva PHN, Abramson MJ Li S, et al. Socioeconomic inequality in vulnerability to all-cause and cause-specific hospitalisation associated with temperature variability: a time-series study in 1814 Brazilian cities. Lancet Planet Health. (2020) 4:e566–76. doi: 10.1016/S2542-5196(20)30251-5
Keywords: air pollution, stroke, hospital admissions, apparent temperature, generalized additive model (GAM)
Citation: Weng L, Li N, Feng T, Zhu R and Zheng Z-J (2021) Short-Term Association of Air Pollutant Levels and Hospital Admissions for Stroke and Effect Modification by Apparent Temperature: Evidence From Shanghai, China. Front. Public Health 9:716153. doi: 10.3389/fpubh.2021.716153
Received: 28 May 2021; Accepted: 23 August 2021;
Published: 27 September 2021.
Edited by:
Dimirios Nikolopoulos, University of West Attica, GreeceReviewed by:
Ka Hung Chan, University of Oxford, United KingdomCopyright © 2021 Weng, Li, Feng, Zhu and Zheng. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Zhi-Jie Zheng, emhlbmd6akBiam11LmVkdS5jbg==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.