 Brenda Robles
Brenda Robles Tony Kuo
Tony Kuo Adriana Galván
Adriana Galván- 1Department of Community Health Sciences, Fielding School of Public Health, University of California, Los Angeles, Los Angeles, CA, United States
- 2Department of Epidemiology, Fielding School of Public Health, University of California, Los Angeles, Los Angeles, CA, United States
- 3Department of Family Medicine, David Geffen School of Medicine at the University of California, Los Angeles, Los Angeles, CA, United States
- 4Population Health Program, Clinical and Translational Science Institute, University of California, Los Angeles, Los Angeles, CA, United States
- 5Department of Psychology, Brain Research Institute, University of California, Los Angeles, Los Angeles, CA, United States
Introduction
Obesity and depression are widespread problems that have major public health implications, both in the United States and abroad. An assessment of the World Health Organization's 2015 Global Health Estimates found that obesity-related chronic conditions (e.g., heart disease, stroke, diabetes) were among the top ten leading causes of death globally (1). Depression, which is associated with heightened mortality risk (2), is the leading cause of disability worldwide (3). The burden of these two conditions has grown in recent years. Between 1990 and 2017, the global incidence of depression increased by nearly 50% (4). The global prevalence of excess body weight has also continued to rise among adults in most countries (5).
Excess adiposity and depressive symptomatology, if unabated, can each or in combination result in deleterious consequences to individuals and their communities. Obesity, for example, is associated with an array of chronic medical conditions, including cancer, hypertension, type 2 diabetes, coronary heart disease, and other forms of cardiovascular disease (6). Direct medical costs associated with obesity (and with overweight status) have been estimated to account for more than 20% of all health care spending in the United States (U.S.) (7). Similarly, the social and economic ramifications of depression also appear to be substantial around the world (3, 8).
In clinical practice, there is growing recognition that when an individual is diagnosed with obesity or depression, healthcare practitioners should check for the presence of and/or treat the other condition (9). This call to action is bolstered by established evidence that these two conditions co-occur (9). Several studies, for instance, have found that adults who are overweight/obese are at increased risk of depression (10). Yet, public health practice often falls short in addressing them. This represents a missed opportunity to intervene.
In this article, we discuss the need for public health to expand its scope and understanding of neuroscience, learning from this discipline to include depression detection and management as part of a more holistic approach to preventing obesity. Namely, we argue that breaking existing silos between the fields of public health and neuroscience may help strengthen the effectiveness of policy, systems, and environmental change interventions (PSEs) which are frequently used to combat obesity at the population-level. To facilitate this dialogue, we first reviewed the current literature on the neural correlates of obesity and depression. We then highlight the potential advantages of considering these correlates in developing PSEs and other interventions for obesity prevention.
What is Known in the Literature
Neural Correlates of Obesity
Neuroscience is a field that elucidates the underlying mechanisms that motivate individuals to eat, which in excess, may result in overweight and obesity. In essence, the brain plays a central role in controlling hunger and regulating eating behaviors (11). The prefrontal cortex or “control” region of the brain, in addition to other functions, helps individuals control their behavior, inhibit their impulsive responses, and evaluate and make decisions about environmental stimuli (12). Several studies have found that overeating (i.e., a behavior linked to overweight/obesity) is attributed to impaired inhibitory control in networks of the brain where the prefrontal cortex is a key node (13).
The limbic system, a set of brain structures connected to the prefrontal cortex, also shapes individuals' motivation behaviors (14). For example, there is evidence that the mesolimbic structures of the brain, and the mesocorticolimbic circuitry or “reward pathway” of the brain, are responsible for the hedonic aspects of eating and incentive salience in food motivation behaviors (15). Other core brain regions associated with dietary self-control include the anterior insula, middle frontal gyrus, supplementary motor cortex, parietal cortices, and fronto-stratrial region (16). Moreover, neurotransmitters (e.g., the hormones leptin and ghrelin) are implicated in the gut-brain reward axis which affects neural functions and controls individuals' eating behaviors and thus obesity status (17).
A growing body of research highlights the intersections between brain activation, food motivation, and eating behaviors (i.e., those characterized by self-control and the ability to delay gratification). For example, adult binge eaters appear to have a lower activation in the fronto-striatal (limbic) region of the brain, and greater trait impulsivity and lower inhibitory control abilities, compared to non-binge eaters (18). It also appears that adolescents with food addiction experience this condition due to hypo-activation in areas of the brain that inhibit control (19). Overall, such studies implicate the brain in food motivation behaviors that can put individuals at risk for excess adiposity.
Neuroscience research also explains the role that stress can play in eating behaviors and on obesity-related outcomes. Stress is considered a common risk factor for both obesity and addiction (20), and there is strong empirical evidence that stress may lead individuals to engage in dietary behaviors that put them at risk for this condition (21). Stress may activate certain brain regions, which could explain conditions such as stress-induced overeating and obesity in adult patients with coronary artery disease (22). Mood may also interact with stress and, in turn, influence what people eat (20). The complex and synergistic relationships between physiological, environmental, and cognitive factors that influence food consumption behaviors of adults and children eating are highlighted by recent advances in neuroscience research (23).
Neural Correlates of Depression
The etiology of depression is complex, as evidenced by past and recent studies. For example, gene-environment interactions have been linked to depression (24). Meanwhile, others have argued that this mental health condition occurs as a result of alterations in spine synapse connectivity in certain areas of the brain (25) or due to structural and/or functional brain abnormalities (26). There is also growing recognition that depression is a neural circuit-based disease (27) and that different areas of the brain contribute to the development of this condition (28). For example, individuals with major depression may have abnormally reduced activity in the medial and lateral prefrontal cortex (i.e., brain regions that regulate emotions) (29). Other studies have found that individuals with mood disorders such as depression exhibit differences in emotional regulation than individuals with anxiety disorder, highlighting distinctions in neural recruitment of emotional or regulatory brain (30).
Several studies have also used functional magnetic resonance imaging (fMRI) or functional neuroimaging to better understand depression in various adult populations (31–35). For example, a study employing fMRI found that individuals with major depressive disorder exhibit greater activation of the amygdala insula and ventrolateral prefrontal cortex when exposed to social exclusion than those without depression (33). Previous neuroimaging studies have found that cognitive-behavioral therapy, a popular psychotherapy treatment, may decrease “resting state activity in the dorsal ACC” (34), and suggest that such a therapy may help with emotion regulation (35). Neuroimaging studies are not limited to adults and neuroimaging techniques have also been used to examine depression among youth (36, 37).
Neural Linkages Between Obesity and Depression
Neuroscience research has increasingly become a resource for scientists and health professionals to examine the relationships between obesity and depression. There is emerging data which suggest that neural adaptations in brain circuitry may explain the associations between obesity and depression/depressive symptoms (38, 39). For example, both of these conditions may occur due to the loss of gray matter in the same medial prefrontal cortex of the brain (40). Abnormal inflammation in the brain has also been implicated in both obesity and depression pathophysiology (41). Moreover, data suggests that depression may be rooted in adiposity-related inflammation within the brain (42) and that the gut-brain axis plays a key role in the development of depression (43, 44) and obesity (45).
Recent Obesity Prevention Efforts at the National and Local Level in the United States
Although correlates such as neural pathways to food motivation can offer important insights for policy development and intervention design, most obesity prevention efforts in the United States do not apply neuroscience in their implementation, choosing to focus primarily on mitigating structural or environmental barriers to healthy eating (46). Unfortunately, data on these structural-level interventions have been mixed, suggesting this socio-ecological approach may be insufficient for fully changing individual consumption behaviors. Various systematic reviews have found an absence of clear evidence demonstrating the effectiveness of these interventions (primarily PSEs) in significantly improving population-level obesity or related health outcomes (47, 48). It is possible that increasing the availability of “healthier” foods does not guarantee that individuals will select them, especially if these individuals are used to consuming inexpensive and highly palatable foods. Sugary and nutrient-poor beverages such as soda, for instance, put individuals at risk for obesity (49). There is accumulating evidence that consuming sugary beverages engender a physiological response similar to that of drugs (50). In contrast, healthy foods that reduce individuals' obesity risk (e.g., fruits and vegetables) do not appear to produce a similar response, but they do generally cost more to purchase relative to the unhealthier food options, creating an economic disincentive (51).
To summarize, recent obesity prevention interventions may be limited in their reach and effectiveness because they fail to consider the underlying neuropsychological mechanisms that may prevent individuals from eating healthy. After all, many have argued that tailoring obesity prevention interventions to specific groups require public health to understand the drivers of food consumption behaviors (52). In this regard, federal and local obesity prevention efforts have fallen short in optimizing these drivers of food decisions. Los Angeles County serves as an example of a metropolitan region that has not traditionally sought to intervene in mental health (including depressive symptomatology and related neurobiological factors) and incorporate this aspect of care into ongoing prevention efforts to reduce overweight/obesity (see Table 1).
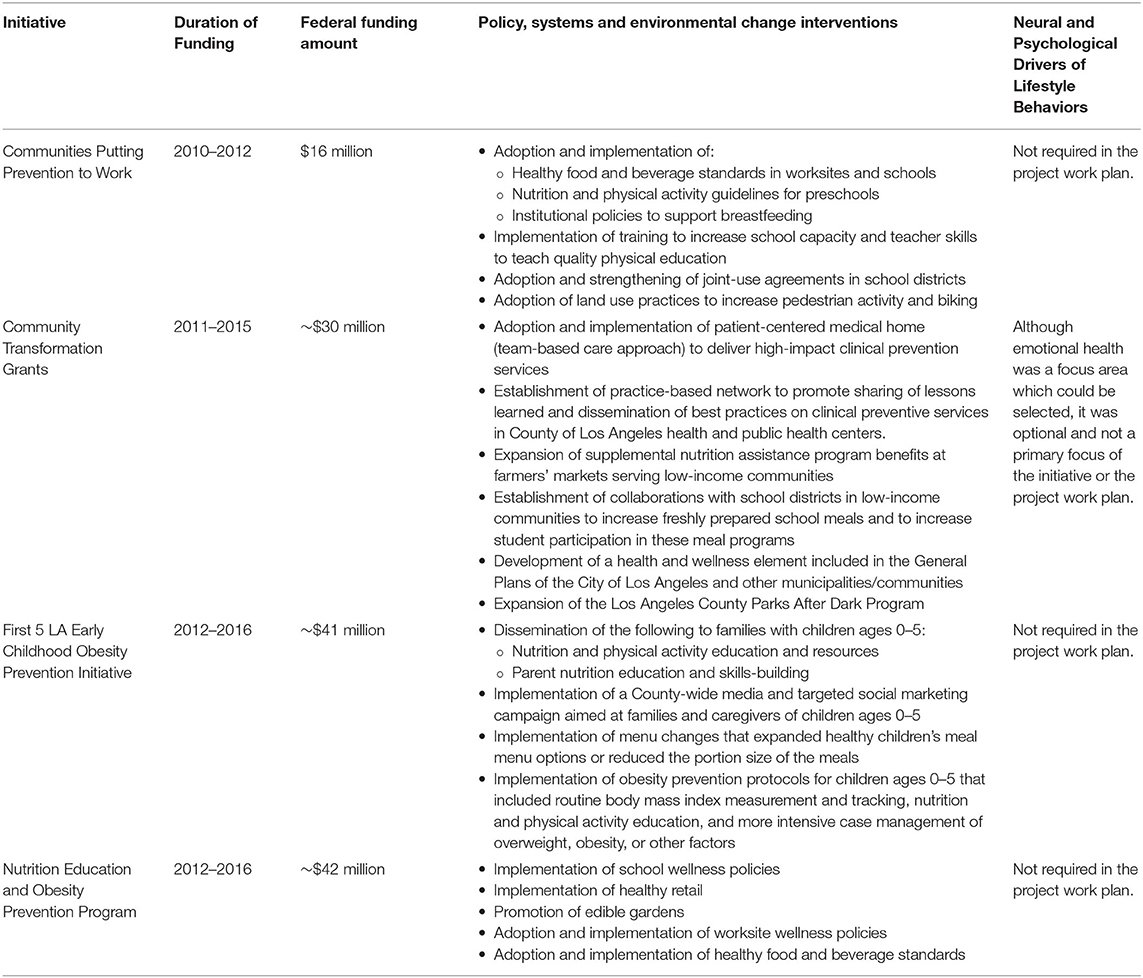
Table 1. Obesity prevention initiatives implemented in Los Angeles County, 2010–2016.
Discussion
So where do we go from here? Now, more than ever, there is a need for public health to find effective solutions to combat obesity and related chronic conditions. This is especially relevant to population health given the 2019 outbreak of the novel coronavirus disease (COVID-19), which has exposed the deleterious nexus the brain, psychological distress, and chronic conditions like obesity. In the COVID-19 era, individuals with hypertension and/or diabetes, conditions associated with obesity (53, 54), appear to be at increased risk for more severe COVID-19 (55). Individuals with these conditions are generally more likely to be hospitalized and to experience greater medical complications from this infection (56). It is also important to consider the pandemic's impact on mental health, especially depression, which appears to be relatively pronounced; this is in part due to the social isolation caused by the lockdowns and mandates to practice social distancing (57). Collectively, the COVID-19 situation offers a cautionary tale about the inter-connectedness of infectious, psychological distress, and chronic conditions, lending further support for public health to expand its reach and scope to encourage cross-pollination with disciplines such as neuroscience, to better serve the population and improve overall population health in the U.S. and across the globe.
Author Contributions
BR conceptualized and drafted the initial article. TK provided subject matter expertise and guidance on chronic disease interventions described in the article. AG provided subject matter expertise related to the neuroscience literature discussed in this article. All authors helped to draft or revise the article.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Mathers C, Stevens G, Hogan D, Mahanani WR, Ho J. Global and regional causes of death: patterns and trends, 2000–15. In: Jamison DT, Gelband H, Horton S, Jha P, Laxminarayan R, Mock CN, et al., editors. Disease Control Priorities: Improving Health and Reducing Poverty, 3rd Edn. Washington, DC: The International Bank for Reconstruction and Development/The World Bank (2017).
2. Gilman SE, Sucha E, Kingsbury M, Horton NJ, Murphy JM, Colman I. Depression and mortality in a longitudinal study: 1952–2011. CMAJ. (2017) 189:E1304–10. doi: 10.1503/cmaj.170125
3. Friedrich MJ. Depression is the leading cause of disability around the world. JAMA. (2017) 317:1517. doi: 10.1001/jama.2017.3826
4. Liu Q, He H, Yang J, Feng X, Zhao F, Lyu J. Changes in the global burden of depression from 1990 to 2017: findings from the Global Burden of Disease study. J Psychiatr Res. (2020) 126:134–40. doi: 10.1016/j.jpsychires.2019.08.002
5. Abarca-Gómez L, Abdeen ZA, Hamid ZA, Abu-Rmeileh NM, Acosta-Cazares B, Acuin C, et al. Worldwide trends in body-mass index, underweight, overweight, and obesity from 1975 to 2016: a pooled analysis of 2416 population-based measurement studies in 128·9 million children, adolescents, and adults. Lancet. (2017) 390:2627–42. doi: 10.1016/S0140-6736(17)32129-3
6. Bray GA, Kim KK, Wilding JPH, World Obesity Federation. Obesity: a chronic relapsing progressive disease process. a position statement of the World Obesity Federation. Obes Rev. (2017) 18:715–23. doi: 10.1111/obr.12551
7. Spieker EA, Pyzocha N. Economic impact of Obesity. Prim Care. (2016) 43:83–95. doi: 10.1016/j.pop.2015.08.013
8. Greenberg PE, Fournier A-A, Sisitsky T, Pike CT, Kessler RC. The economic burden of adults with major depressive disorder in the United States (2005 and 2010). J Clin Psychiatry. (2015) 76:155–62. doi: 10.4088/JCP.14m09298
9. Jantaratnotai N, Mosikanon K, Lee Y, McIntyre RS. The interface of depression and obesity. Obes Res Clin Pract. (2017) 11:1–10. doi: 10.1016/j.orcp.2016.07.003
10. Pereira-Miranda E, Costa PRF, Queiroz VAO, Pereira-Santos M, Santana MLP. Overweight and Obesity associated with higher depression prevalence in adults: a systematic review and meta-analysis. J Am Coll Nutr. (2017) 36:223–33. doi: 10.1080/07315724.2016.1261053
11. Berthoud H-R, Morrison C. The brain, appetite, and obesity. Annu Rev Psychol. (2008) 59:55–92. doi: 10.1146/annurev.psych.59.103006.093551
13. Lavagnino L, Arnone D, Cao B, Soares JC, Selvaraj S. Inhibitory control in obesity and binge eating disorder: a systematic review and meta-analysis of neurocognitive and neuroimaging studies. Neurosci Biobehav Rev. (2016) 68:714–26. doi: 10.1016/j.neubiorev.2016.06.041
14. Cardinali DP. Fourth Level: The Limbic System. Autonomic Nervous System (2018). p. 245–85. doi: 10.1007/978-3-319-57571-1_6
15. Berridge KC. Evolving concepts of emotion and motivation. Front Psychol. (2018) 9:1647. doi: 10.3389/fpsyg.2018.01647
16. Han JE, Boachie N, Garcia-Garcia I, Michaud A, Dagher A. Neural correlates of dietary self-control in healthy adults: a meta-analysis of functional brain imaging studies. Physiol Behav. (2018) 192:98–108. doi: 10.1016/j.physbeh.2018.02.037
17. Zanchi D, Depoorter A, Egloff L, Haller S, Mählmann L, Lang UE, et al. The impact of gut hormones on the neural circuit of appetite and satiety: a systematic review. Neurosci Biobehav Rev. (2017) 80:457–75. doi: 10.1016/j.neubiorev.2017.06.013
18. Oliva R, Morys F, Horstmann A, Castiello U, Begliomini C. The impulsive brain: neural underpinnings of binge eating behavior in normal-weight adults. Appetite. (2019) 136:33–49. doi: 10.1016/j.appet.2018.12.043
19. Hardee JE, Phaneuf C, Cope L, Zucker R, Gearhardt A, Heitzeg M. Neural correlates of inhibitory control in youth with symptoms of food addiction. Appetite. (2020) 148:104578. doi: 10.1016/j.appet.2019.104578
21. Sinha R. Role of addiction and stress neurobiology on food intake and obesity. Biol Psychol. (2018) 131:5–13. doi: 10.1016/j.biopsycho.2017.05.001
22. Moazzami K, Wittbrodt MT, Lima BB, Levantsevych O, Kaseer B, Martini A, et al. Neural correlates of stress and abdominal obesity in patients with Coronary Artery Disease. Psychosom Med. (2020) 82:272–80. doi: 10.1097/PSY.0000000000000776
23. Berthoud H-R, Münzberg H, Morrison CD. Blaming the brain for obesity: integration of hedonic and homeostatic mechanisms. Gastroenterology. (2017) 152:1728–38. doi: 10.1053/j.gastro.2016.12.050
24. Normann C, Buttenschøn HN. Gene-environment interactions between HPA-axis genes and stressful life events in depression: a systematic review. Acta Neuropsychiatr. (2019) 31:186–92. doi: 10.1017/neu.2019.16
25. Duman RS, Sanacora G, Krystal JH. Altered connectivity in depression: GABA and glutamate neurotransmitter deficits and reversal by novel treatments. Neuron. (2019) 102:75–90. doi: 10.1016/j.neuron.2019.03.013
26. Scheepens DS, van Waarde JA, Lok A, de Vries G, Denys DAJP, van Wingen GA. The link between structural and functional brain abnormalities in depression: a systematic review of Multimodal Neuroimaging Studies. Front Psychiatry. (2020) 11:485. doi: 10.3389/fpsyt.2020.00485
27. McTeague LM, Huemer J, Carreon DM, Jiang Y, Eickhoff SB, Etkin A. Identification of common neural circuit disruptions in cognitive control across psychiatric disorders. Am J Psychiatry. (2017) 174:676–85. doi: 10.1176/appi.ajp.2017.16040400
28. Iwabuchi SJ, Krishnadas R, Li C, Auer DP, Radua J, Palaniyappan L. Localized connectivity in depression: a meta-analysis of resting state functional imaging studies. Neurosci Biobeh Rev. (2015) 51:77–86. doi: 10.1016/j.neubiorev.2015.01.006
29. Murrough JW, Abdallah CG, Anticevic A, Collins KA, Geha P, Averill LA, et al. Reduced global functional connectivity of the medial prefrontal cortex in major depressive disorder. Hum Brain Mapp. (2016) 37:3214–23. doi: 10.1002/hbm.23235
30. Zilverstand A, Parvaz MA, Goldstein RZ. Neuroimaging cognitive reappraisal in clinical populations to define neural targets for enhancing emotion regulation. a systematic review. Neuroimage. (2017) 151:105–16. doi: 10.1016/j.neuroimage.2016.06.009
31. Gudayol-Ferré E, Peró-Cebollero M, González-Garrido AA, Guàrdia-Olmos J. Changes in brain connectivity related to the treatment of depression measured through fMRI: a systematic review. Front Hum Neurosci. (2015) 9:582. doi: 10.3389/fnhum.2015.00582
32. Stickel S, Wagels L, Wudarczyk O, Jaffee S, Habel U, Schneider F, et al. Neural correlates of depression in women across the reproductive lifespan-an fMRI review. J Affect Disord. (2019) 246:556–70. doi: 10.1016/j.jad.2018.12.133
33. Kumar P, Waiter GD, Dubois M, Milders M, Reid I, Steele JD. Increased neural response to social rejection in major depression. Depress Anxiety. (2017) 34:1049–56. doi: 10.1002/da.22665
34. Franklin G, Carson AJ, Welch KA. Cognitive behavioural therapy for depression: systematic review of imaging studies. Acta Neuropsychiatr. (2016) 28:61–74. doi: 10.1017/neu.2015.41
35. Rubin-Falcone H, Weber J, Kishon R, Ochsner K, Delaparte L, Doré B, et al. Neural predictors and effects of cognitive behavioral therapy for depression: the role of emotional reactivity and regulation. Psychol Med. (2020) 50:146–60. doi: 10.1017/S0033291718004154
36. Samea F, Soluki S, Nejati V, Zarei M, Cortese S, Eickhoff SB, et al. Brain alterations in children/adolescents with ADHD revisited: a neuroimaging meta-analysis of 96 structural and functional studies. Neurosci Biobehav Rev. (2019) 100:1–8. doi: 10.1016/j.neubiorev.2019.02.011
37. Rakesh D, Allen NB, Whittle S. Balancing act: neural correlates of affect dysregulation in youth depression and substance use – a systematic review of functional neuroimaging studies. Dev Cogn Neurosci. (2020) 42:100775. doi: 10.1016/j.dcn.2020.100775
38. Hidese S, Ota M, Matsuo J, Ishida I, Hiraishi M, Yoshida S, et al. Association of obesity with cognitive function and brain structure in patients with major depressive disorder. J Affect Disord. (2018) 225:188–94. doi: 10.1016/j.jad.2017.08.028
39. Milaneschi Y, Simmons WK, van Rossum EFC, Penninx BW. Depression and obesity: evidence of shared biological mechanisms. Mol Psychiatry. (2019) 24:18–33. doi: 10.1038/s41380-018-0017-5
40. Opel N, Redlich R, Kaehler C, Grotegerd D, Dohm K, Heindel W, et al. Prefrontal gray matter volume mediates genetic risks for obesity. Mol Psychiatry. (2017) 22:703–10. doi: 10.1038/mp.2017.51
41. Chaves Filho AJM, Lima CNC, Vasconcelos SMM, de Lucena DF, Maes M, Macedo D. IDO chronic immune activation and tryptophan metabolic pathway: a potential pathophysiological link between depression and obesity. Prog Neuropsychopharmacol Biol Psychiatry. (2018) 80:234–49. doi: 10.1016/j.pnpbp.2017.04.035
42. Capuron L, Lasselin J, Castanon N. Role of adiposity-driven inflammation in depressive morbidity. Neuropsychopharmacology. (2017) 42:115–28. doi: 10.1038/npp.2016.123
43. Schachter J, Martel J, Lin C-S, Chang C-J, Wu T-R, Lu C-C, et al. Effects of obesity on depression: a role for inflammation and the gut microbiota. Brain Behav Immun. (2018) 69:1–8. doi: 10.1016/j.bbi.2017.08.026
44. Mörkl S, Wagner-Skacel J, Lahousen T, Lackner S, Holasek SJ, Bengesser SA, et al. The role of nutrition and the gut-brain axis in psychiatry: a review of the literature. Neuropsychobiology. (2018) 79:1–9. doi: 10.1159/000492834
45. Agustí A, García-Pardo MP, López-Almela I, Campillo I, Maes M, Romaní-Pérez M, et al. Interplay between the gut-brain axis, obesity and cognitive function. Front Neurosci. (2018) 12:155. doi: 10.3389/fnins.2018.00155
46. Rohan EA, Chovnick G, Rose J, Townsend JS, Young M, Moore AR. Prioritizing population approaches in cancer prevention and control: results of a case study evaluation of policy, systems, and environmental change. Popul Health Manag. (2019) 22:205–12. doi: 10.1089/pop.2018.0081
47. Mayne SL, Auchincloss AH, Michael YL. Impact of policy and built environment changes on obesity-related outcomes: a systematic review of naturally occurring experiments. Obes Rev. (2015) 16:362–75. doi: 10.1111/obr.12269
48. Tseng E, Zhang A, Shogbesan O, Gudzune KA, Wilson RF, Kharrazi H, et al. Effectiveness of policies and programs to combat adult obesity: a systematic review. J Gen Intern Med. (2018) 33:1990–2001. doi: 10.1007/s11606-018-4619-z
49. Ruanpeng D, Thongprayoon C, Cheungpasitporn W, Harindhanavudhi T. Sugar and artificially sweetened beverages linked to obesity: a systematic review and meta-analysis. QJM. (2017) 110:513–20. doi: 10.1093/qjmed/hcx068
50. Falbe J, Thompson HR, Patel A, Madsen KA. Potentially addictive properties of sugar-sweetened beverages among adolescents. Appetite. (2019) 133:130–7. doi: 10.1016/j.appet.2018.10.032
51. Bennett R, Zorbas C, Huse O, Peeters A, Cameron AJ, Sacks G, et al. Prevalence of healthy and unhealthy food and beverage price promotions and their potential influence on shopper purchasing behaviour: a systematic review of the literature. Obes Rev. (2020) 21:e12948. doi: 10.1111/obr.12948
52. Leng G, Adan RAH, Belot M, Brunstrom JM, de Graaf K, Dickson SL, et al. The determinants of food choice. Proc Nutr Soc. (2017) 76:316–27. doi: 10.1017/S002966511600286X
53. Jiang S-Z, Lu W, Zong X-F, Ruan H-Y, Liu Y. Obesity and hypertension. Exp Ther Med. (2016) 12:2395–9. doi: 10.3892/etm.2016.3667
54. Verma S, Hussain ME. Obesity and diabetes: an update. Diabetes Metab Syndr. (2017) 11:73–9. doi: 10.1016/j.dsx.2016.06.017
55. Fang L, Karakiulakis G, Roth M. Are patients with hypertension and diabetes mellitus at increased risk for COVID-19 infection? Lancet Respir Med. (2020) 8:e21. doi: 10.1016/S2213-2600(20)30116-8
56. Emami A, Javanmardi F, Pirbonyeh N, Akbari A. Prevalence of underlying diseases in hospitalized patients with COVID-19: a systematic review and meta-analysis. Arch Acad Emerg Med. (2020) 8:e35. doi: 10.1371/journal.pone.0241265
Keywords: neuroscience, obesity, depression, public health interventions, policies, systems, environments, program planning
Citation: Robles B, Kuo T and Galván A (2021) Understanding the Neuroscience Underpinnings of Obesity and Depression: Implications for Policy Development and Public Health Practice. Front. Public Health 9:714236. doi: 10.3389/fpubh.2021.714236
Received: 25 May 2021; Accepted: 29 July 2021;
Published: 20 August 2021.
Edited by:
Rahul Shidhaye, Pravara Institute of Medical Sciences, IndiaReviewed by:
Joanne Harris, Swinburne University of Technology, AustraliaCopyright © 2021 Robles, Kuo and Galván. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Brenda Robles, YnJyb2JsZXNAcGgubGFjb3VudHkuZ292