 Xuren Wang1,2†‡
Xuren Wang1,2†‡ Demeng Xia
Demeng Xia Xisha Long
Xisha Long Shuogui Xu
Shuogui Xu Li Gui
Li Gui
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health , 25 June 2021
Sec. Occupational Health and Safety
Volume 9 - 2021 | https://doi.org/10.3389/fpubh.2021.707264
This article is part of the Research Topic Environmental or occupational exposure to optical radiation: risk evaluation, health effects and prevention - tangible innovation for public and occupational health? View all 10 articles
Background: Military personnel are widely exposed to risk factors for heat-related illnesses. Knowledge, attitudes, and practices (KAP) are three of the most important means by which to prevent such illnesses, but there has been a lack of investigations into and correlation analyses of KAP. This study aimed to explore the heat-related KAP of military personnel in China.
Methods: We conducted a cross-sectional study (June 1-25, 2019). A total of 646 military personnel were recruited from two Chinese Navy troops in the tropical zone and one troop in the temperate zone. We collected data on demographic characteristics and KAP scores using questionnaires. Univariate analysis and Scheffe's method were used for data analyses.
Results: The mean KAP scores were 10.37 (range = 3–13, standard deviation = 1.63) for knowledge (K-score), 7.76 (range = 0–16, SD = 2.65) for attitudes (A-score), and 3.80 (range = 1–6, SD = 1.12) for practices (P-score). There were noticeable differences in mean K-score according to age, military rank, and educational level (P < 0.05). Participants from the tropical zone had higher A-scores (P < 0.05) and higher P-scores (P < 0.001) than those from the temperate zone. Additionally, participants with relevant experience also had higher A-scores (P < 0.05) than those without such experience.
Conclusions: Military personnel's awareness of preventive and first-aid measures against heat-related illnesses need to be strengthened. It will be very important to develop educational programmes and enrich systematic educational resources to raise this awareness.
- Since military personnel are widely exposed to risk factors for heat-related diseases, and this is the first time that the Chinese Navy has investigated KAP for heat-related diseases, research on this population may be of great significance.
- Military personnel scored highly on most common-sense questions about heat-related illnesses,but the accuracy rate of questions about exertional heat stroke were extremely low.
- Some misinformation related to media consumption with commercial purpose may be fatal at the critical moment for rescuing severe exertional heat stroke patients.
- The majority of respondents had good awareness of heat-related illnesses,and those from the humid tropical zone had higher mean A-scores than the temperate zone.
- Pearson's correlation coefficient indicated a weak correlation between the A- and P-scores.
The Intergovernmental Panel on Climate Change (IPCC) projects that the frequency, duration, and intensity of extreme weather may increase in the coming decades (1). A heat wave (HW) is a natural hazard characterized by an episode of hot weather. However, there is currently no universally accepted definition of HWs around the world in different fields. Especially in the military system, various definitions are employed (2). Thus, given this divergence, this study adopted the definition of three or more consecutive days with a maximum temperature over 35°C as published by the Chinese Meteorological Administration (3). The frequency of heat waves has increased in most parts of Asia (4), Europe (5, 6), and Australia (7, 8). Furthermore, heat waves can have significant effects on health and present a challenge for occupational-health protection. Heat-related illnesses include heat stroke, heat exhaustion, rhabdomyolysis, heat spasm, heat syncope, and heat rash. The inverse effects of heat-related illnesses on mortality have been widely reported. Mortality from heat stroke among the elderly exceeds 50% (9). Another study, conducted in 66 cities in China, showed that 5.0% of excess deaths may be associated with heat waves (10). The estimated number of heat-related deaths worldwide is expected to increase to 90,000 annually in 2030 and more than 255,000 in 2050 (11). Therefore, more attention should be paid to the insidious health effects of heat-related illnesses.
Risk factors associated with heat-related illnesses may be environmental or individual. Environmental risk factors, also known as exogenous factors, may include high temperatures, high humidity, and direct sun exposure. Individual risk factors, also known as endogenous factors, may include insufficient fluid intake, physical exertion, overall physical condition, medications, and pregnancy (12). Military personnel, especially those at low latitudes, where soldiers routinely experience high levels of physical exertion under high ambient temperatures and high humidity, are widely exposed to both exogenous and endogenous risk factors for heat-related illnesses. Military endeavors in heat wave conditions can alter the judgement and physical performance of military personnel, leading to significant impairment of individuals' ability to work, possibly even leading to death (13, 14). Therefore, reducing heat-related illnesses is a key factor in ensuring the combat effectiveness of the military during heat waves.
The purpose of knowledge, attitudes, and practices (KAP) surveys is to collect data on the knowledge, perceptions, and behaviors of specific populations in relation to a certain topic. The literature shows that knowledge of heat waves, attitudes toward risk factors, and adaptation practices are three of the most important factors in preventing heat-related illnesses (15). These findings could merely be local indicators that are representative of a particular field. KAP studies on heat-related illnesses have been performed among the general public for different occupations, and it is reported that several factors influence public KAP, such as age, educational level, economic level, nationality, and gender (16–18). However, only a few studies have focused on knowledge of heat-related illnesses among Chinese military personnel. There is a lack of investigations and correlation analyses of knowledge, attitudes, and practices. Therefore, in this study, we selected three Chinese naval troops with different risk factors that were working at low latitudes to explore the heat-related KAP of military personnel for the first time. Our aim was to provide data for future policy formulation and implementation in response to heat waves and associated side effects.
A total of three naval troops took part in the study. Two of these troops were stationed in the tropics (~9° north latitude), where they worked in a high-temperature and high-humidity environment all year round. The hottest month (in terms of average maximum temperature) was May (32°C). The month with the lowest average temperature was January (26.1°C); the wettest month (with the most rainfall) was September (251.4 mm), and the driest month (with the least rainfall) was January (8 mm). The month with the longest sunshine duration was June (average sunshine duration: 13.2 h). The month with the shortest sunshine duration was December (average sunshine duration: 11 h). The other sampled troop was stationed in a warm, temperate, continental monsoon climate zone (~30° north latitude). The hottest month (with the highest average temperature) was July (28°C). The month with the lowest average temperature was January (−12.4°C). The wettest month (with the most rainfall) was July (128.8 mm). The driest month (with the least rainfall) was January (1.5 mm). The month with the longest sunshine duration was June (average sunshine duration: 15.9 h). The month with the shortest sunshine duration was December (average sunshine duration: 8.6 h). The geographical location and climatic characteristics of the three troops mentioned above was shown in Figure 1.
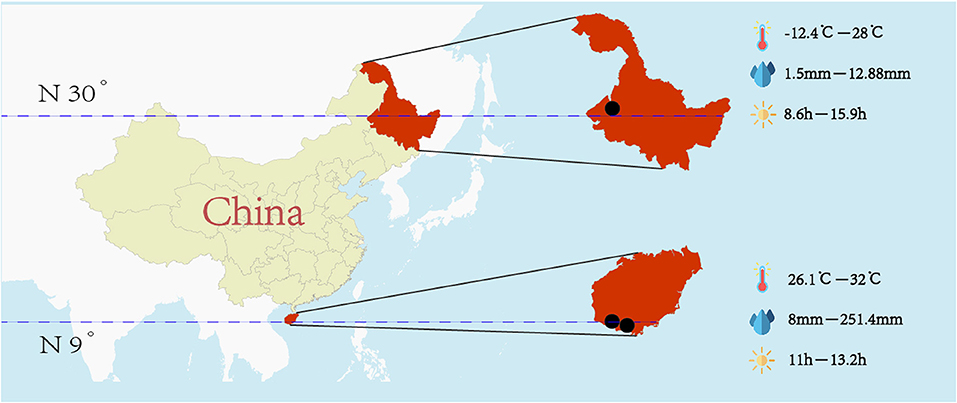
Figure 1. Geographical location and climatic characteristics of the three sample troops.
We used convenience sampling to select military personnel from these three naval troops. The target population of this study was active-duty sailors without experience working in health care. A platoon is a military unit containing 30–50 sailors. We included a total of 15 platoons of troops in the tropical zone, including 560 sailors in total, in this study. In the temperate zone, we included three platoons with a total of 86 sailors.
We developed a questionnaire based on a review of the literature on heat waves and heat-related illnesses (Supplementary Material 1). The questionnaire “Research Questionnaires on knowledge, attitude and practice toward heat-related illnesses during field training exercises” was initially drafted in English by Li Gui and Sarathchadra, and was translated from English to Chinese by Demeng Xia, Xuren Wang, and then was translated then back to English by Yixin Wang, Xisha Long to ensure the meaning of the content. The questionnaire consisted of four sections: (1) sociodemographic information, including age, years of military service, educational level, marital status, military rank, and heat-related illnesses experience; (2) the knowledge (K) section including 18 items on clinical symptoms, treatment, risk factors, prevention and control of heat-related illnesses (13 true–false items and five multiple-choice items); (3) the attitude (A) section including four items about attitude of sailors toward heat-related illnesses; and (4) the practice (P) section including six items related to practices and behavior of heat-related illnesses prevention.
In the K section, participants received one point for answering each true–false item or multiple-choice question correctly; incorrect answers received zero points, with high scores indicated better knowledge of heat-related illness risk factors. Items in the A section were scored on a four-point scale, a high score indicates a positive attitude. The scale used Cronbach's α to assess internal reliability. Cronbach's alpha coefficient is 0.73, indicating internal reliability. The P section consisted of yes-or-no questions, with each “Yes” response earning one point and each “No” response earning zero points. The score ranges for the K, A, and P sections were 0–18, 1–16, and 0–6, respectively.
This cross-sectional quantitative survey collected data face-to-face using the time of regular assembly from 1 June 2019, to 25 June 2019. Well-trained researchers interviewed participants using the structured questionnaires, and respondents were informed that all information and opinions provided would be anonymous and confidential. Various actions were taken to ensure questionnaire quality. First, a panel of experts was consulted at the development stage, and then a pilot study including only a few sailors was carried out for semantic analysis. Before the survey, all the researchers were systematically trained in the unified interview guide and questionnaire instructions. All questionnaires were completed and collected immediately to increase the response rate. Two independent researchers performed data collation and entry to minimize errors in data processing.
We used SPSS for Mac software version 25.0 (IBM Corp., Armonk, New York, US) for data analysis. Mean and standard deviation (SD) values were calculated for continuous variables; categorical variables are expressed as the percentage of subjects. We used univariate analysis of variance to test the associations of each demographic characteristic with K-, A-, and P-scores and the overall score. Scheffe's method was used in further paired comparisons if necessary. Finally, we used Pearson's correlation coefficient to clarify the correlations between K-, A-, and P-scores. P < 0.05 was considered statistically significant.
The study was approved by the Ethics Committee of the Institutional Review Board of the Naval Medical University, Shanghai, China (NMUMREC-2021-022). Written informed consent was obtained from all participants before the survey. All data obtained were anonymous.
In the baseline survey, a total of 646 subjects were approached and invited to join this study. However, six of them did not complete the questionnaires, leaving 640 (99.1%) in the final analysis. Their sociodemographic characteristics are presented in Table 1. All participants were male, and their mean age was 25.1 years (range = 18–43 years, SD = 4.09). The greatest share of participants (43.9%) had been in military service for 1–5 years. Educational levels and military ranks varied. Of all participants, 86.8% were stationed in the tropical zone, and 29.1% had heat-related illness experience.
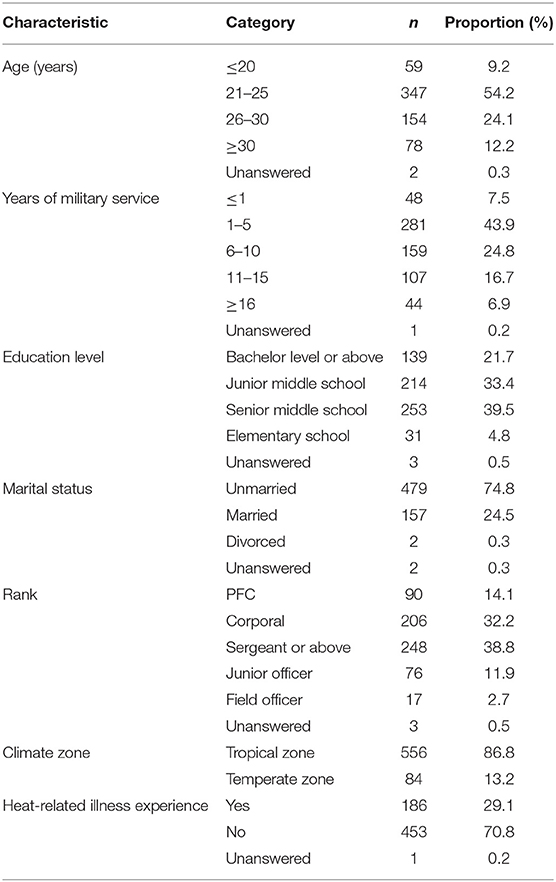
Table 1. Demographic characteristics (n = 640).
Table 2 details the responses showing participants' knowledge about heat-related illnesses. More than half of the true–false questions received correct answers from >80% of respondents. Most participants (95.9%) were familiar with heat exhaustion management, including transferring victims to a cool environment; drinking fluids; and using cool water, ice packs, and fanning. However, over one-third of participants (34.7%) did not know that sweating could reduce body temperature, and 37.5% of participants thought that only physically weak persons were susceptible to heat-related illnesses during field training exercises. Moreover, 81.2% of participants deemed that heat exhaustion is characterized by a body temperature higher than 40°C, which showed that most participants did not have basic knowledge of heat stroke. The multiple-choice items received far fewer correct answers than the true–false items did. Alcohol was considered by 77.4% of participants to be the best means of decreasing health risks from heat waves, when actually it is a risk factor. The World Health Organization (WHO) recommends drinking water or using oral rehydration salts (ORS) (19), but 85.0% of participants said that they preferred to drink soda during field training exercises.
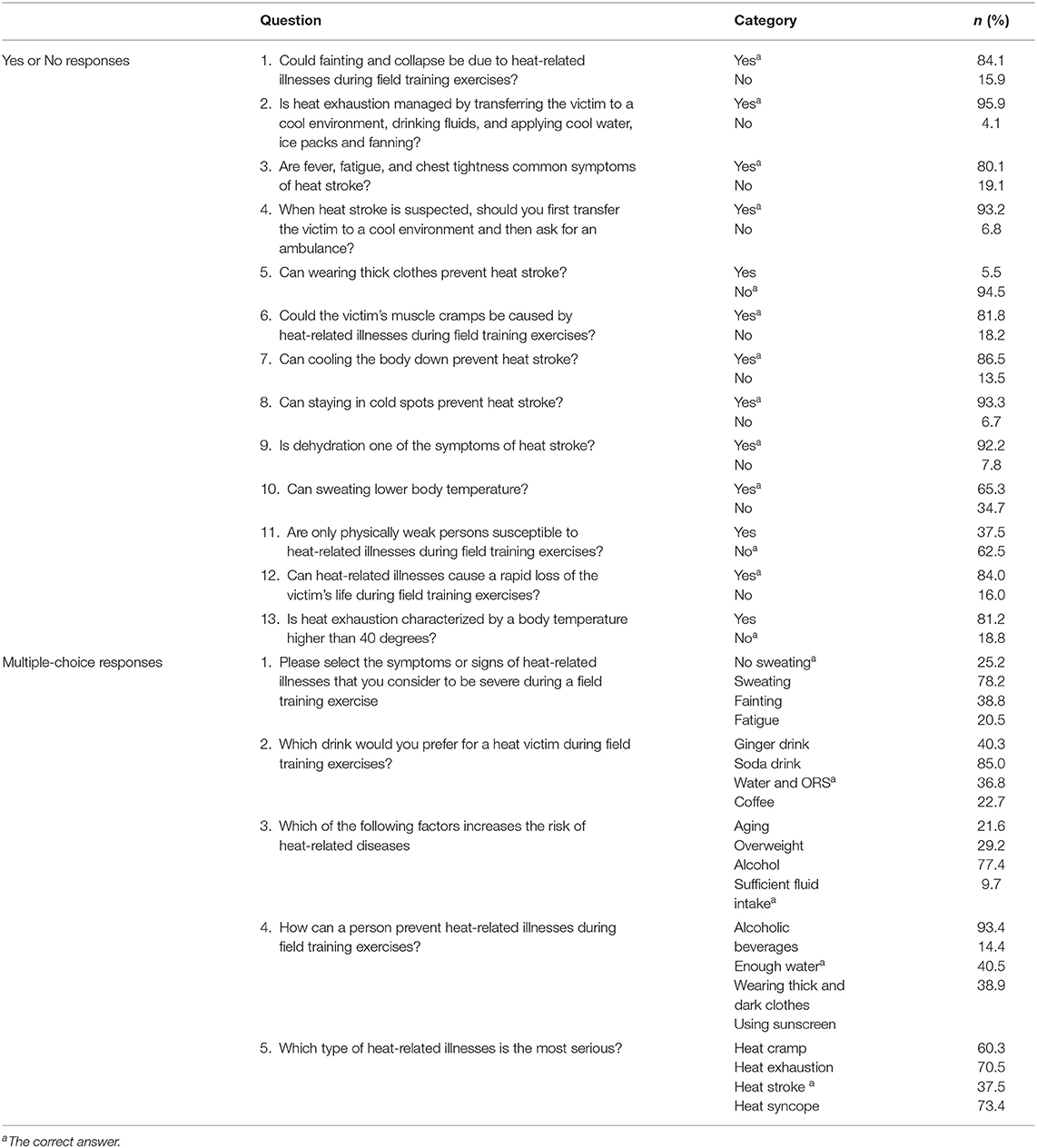
Table 2. Responses to knowledge items (n = 640).
In the attitudes section, only 26.2% of participants said they were very concerned about the risks of heat-related illnesses. Additionally, 40.4% reported they were somewhat sensitive to heat-related illnesses, whereas <12.8% said they were “not at all” sensitive. In the practices section, most participants (79.7%) reported that when a high-temperature alert was released, their leaders generally arranged outdoor activities at relatively cooler times, and medics took intervention measures (74.4%). Additionally, 71.9% of participants were aware that it is necessary to implement good preventive measures against heat-related illnesses. However, only 64.8% of participants had received health education prior to field training, and nearly three-quarters of participants (74.4%) said that they drank water only when they were thirsty (Table 3).
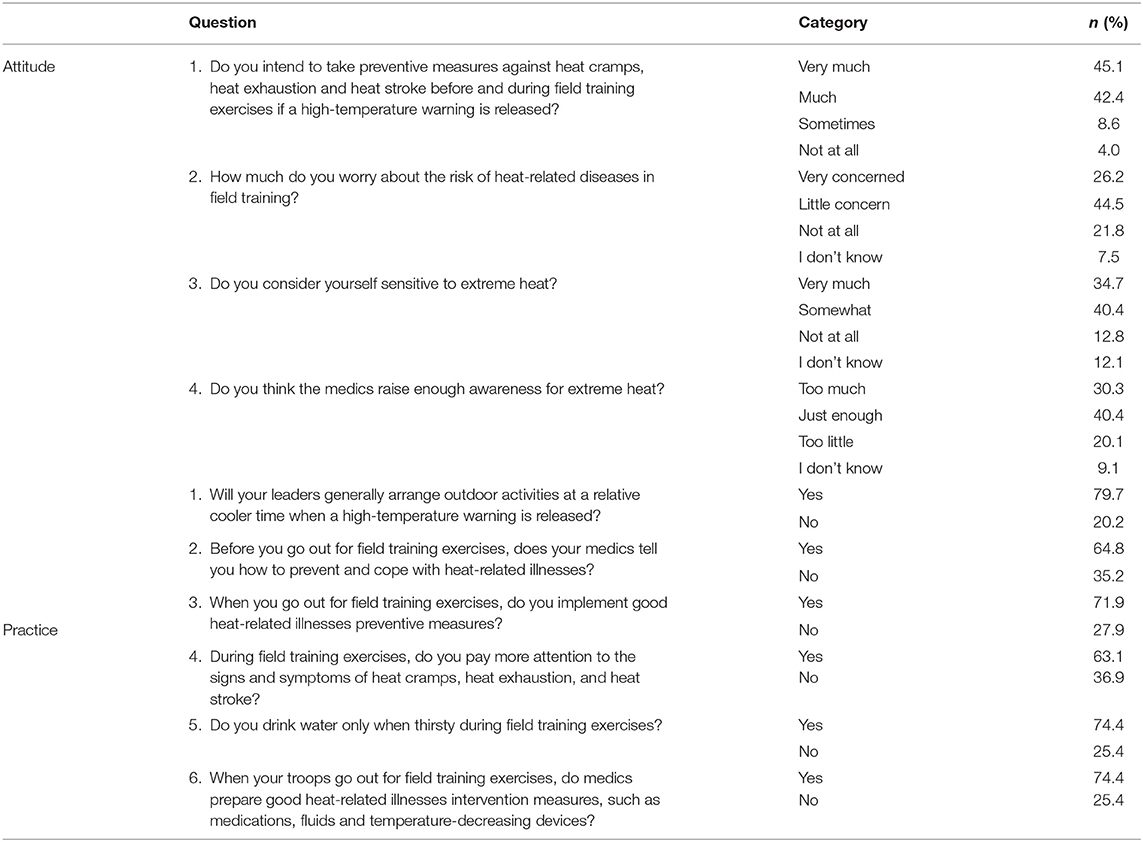
Table 3. Responses to attitude and practice items (n = 640).
Detailed mean KAP scores and mean overall scores according to demographic characteristics are shown in Figure 2. The mean K-score was 10.37 (range = 3–13, SD = 1.63). There were noticeable differences in mean K-score according to age, military rank, and educational level (P < 0.05). Paired comparisons using Scheffe's method indicated that the mean K-score was lower among participants <20 years old compared with the other age groups (P < 0.05) and higher among junior officers (P < 0.05) and participants who had at least a bachelor's degree (P < 0.05).

Figure 2. Mean KAP scores according to demographic characteristics. *P < 0.05, **P < 0.001.
The mean A-score was 7.76 (range = 0–16, SD = 2.65). Participants from the tropical zone had higher A-scores than those from the temperate zone (8.2, SD = 3.08 vs. 6.9, SD = 2.34; P < 0.05). Participants with heat-related illness experience had higher A-scores than those who did not have such experience (7.8, SD = 2.65 vs. 6.9, SD = 2.58; P < 0.05).
The mean P-score was 3.80 (range = 1–6, SD = 1.12). Participants from the troops stationed in the tropical zone had higher P-scores (4.3, SD = 0.90 vs. 3.6, SD = 1.22; P < 0.001) than those from the temperate zone.
Correlation analyses suggested a significant positive correlation between A- and P-scores (r = 0.170, P < 0.001). No positive correlation was found between K- and A-scores or between K- and P-scores (Table 4).
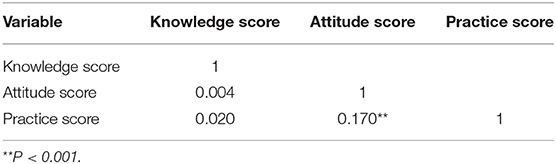
Table 4. Correlations between knowledge, attitude, and practice scores.
Several studies have reported that heat waves have adverse effects on human health (19). People's awareness of the risks of, knowledge about, and protective practices against heat-related illnesses are crucial elements in reducing the harmful health effects of heat waves (20). However, to the best of our knowledge, this is the first study to survey KAP of heat-related illnesses in the Chinese Navy. Studies on this population could be greatly significant, as military personnel are widely exposed to risk factors for heat-related illnesses. Therefore, the findings of this study might provide essential references for the training and health education of military personnel.
In this survey, the majority of participants had high scores for most K-related questions and demonstrated good awareness of and protective practices against heat-related illnesses. However, some subgroups showed lower K-, A-, and P-scores based on demographic factors, environmental differences, and personal experiences.
Knowledge plays an important role in mitigating the adverse effects of heat waves (2). By analyzing participants' answers to K-questions in this study, we found that military personnel scored highly on most common-sense questions about heat-related illnesses (e.g., 95% of participants knew that being in a cool environment; drinking fluids; and applying cool water, ice packs and fanning were interventional measures against heat-related illnesses). However, the accuracy rate of questions about exertional heat stroke were extremely low. Only 37.5% of participants recognized the severity of exertional heat stroke, and only 25.2% of participants considered not sweating to be a danger sign. Exertional heat stroke is a medical emergency that is directly related to strenuous physical activity. Military personnel in high-temperature environments performing high-intensity exercise are vulnerable to exertional heat stroke (21). An epidemiological survey of military personnel showed a steady increase in the morbidity and mortality of exertional heat stroke over the past decade (22), but effective recognition and prompt treatment can greatly reduce this rate (23). Therefore, it is necessary to strengthen military personnel's awareness of how to prevent and administer first-aid in the event of exertional heat stroke.
Strikingly, 85% of participants chose soda as a drink for heat victims, and 93.4% of participants believed that alcoholic beverages were beneficial for preventing heat-related illnesses during field training. This misinformation that alcoholic beverages and soda contribute to the prevention and treatment of heat-related illnesses might be related to media consumption. Military personnel may access information via television, the Internet, and smart phones (24), but information from these media usually has a commercial purpose, which can mislead the audience. For example, advertisements often link ice-cold beer to hot summer weather and depict sportsmen in high-ambient temperatures delightedly drinking ice-cold soda. This erroneous information may be fatal at the critical moment for rescuing severe exertional heat stroke patients. According to a report in the New England Journal of Medicine, alcohol heightens the metabolic response to physical activity and is therefore a risk factor for exertional heat stroke. Thus, military administrators should strive to develop educational programmes in order to improve military personnel's knowledge about heat-related illnesses; moreover, governments should disseminate relevant knowledge on mass media.
By analyzing demographic characteristics, we found that participants who were younger than 20 years of age had lower K-scores than other participants (P < 0.05). This result was in contrast to the findings of Jing Li et al. (21). This might have been because participants in Jing Li's study had a large age range of 15–91 years, whereas the military personnel in our study were all young, with a mean age of 25.1 years. Additionally, K-scores were higher among junior officers (P < 0.05) with higher educational levels, which was similar to the results of previous studies (25). These findings suggest that we should provide health education on heat-related illnesses, especially to young military personnel. At the same time, since military officers have high educational levels and good mastery of relevant knowledge, administrators should take advantage of this, perhaps training these officers as instructors in health education projects.
The majority of respondents had good awareness of heat-related illnesses. Additionally, 87.5% of participants intended to take preventive measures at high ambient temperatures, and 75.1% of participants considered themselves sensitive to heat. Moreover, participants from the humid tropical zone had higher mean A-scores than those from the temperate zone. Conversely, when it came to the risks of heat-related illnesses, most participants (44.5%) reported little concern, possibly due to insufficient knowledge of these risks (26). Therefore, it is very important to enrich systematic educational resources with information about the risks of heat-related illnesses.
Pearson's correlation coefficient indicated a weak correlation between the A- and P-scores. This was consistent with the results of previous studies (27), whose authors reported that risk awareness is positively correlated with adaptation practices. An explanation for this correlation could lie in the health belief model, which asserts that health-related practices are determined by whether people recognize the seriousness of the problem and perceive themselves to be susceptible to particular illnesses (28). Therefore, good awareness of heat-related illnesses and the perception that there are benefits to taking action and fostering self-sufficiency against such illnesses promote preventive practices, which in turn reduce the adverse effects of heat waves. However, one subgroup in this study showed an interesting result: military personnel in the tropical zone had good awareness but low P-scores. This finding might be explained in part by three factors. First, people at low latitudes become better adapted to heat through behavioral and structural adjustment than people at high latitudes; this is called thermal acclimatization (29). Therefore, despite their positive attitudes toward heat-related illnesses, military personnel in the tropical zone performed limited protective behaviors. Second, the majority of participants were young men, who tend to be more willing than other people to take risks and to believe they can handle heat. Third, motivation and pressure from peers and instructors are likely to drive youths to perform beyond their physiological capability, which is also one of the major risk factors for exertional heat stroke (30). In summary, many factors might influence people's behavior, so further studies are needed to explore how to best promote and reinforce protective behaviors.
There were several limitations in our research. First, our present study investigated only KAP of heat-related illnesses in Chinese naval officers and sailors; thus, caution should be used when generalizing the results to other military forces. Second, this study adopted convenience sampling, which could limit the representativeness of the results. Third, the questions in the questionnaires relating to KAP of heat-related illnesses were limited rather than comprehensive and sufficiently detailed, meaning that we might not have explored the relevant knowledge mastery, behaviors, and attitudes in depth. Fourth, in the designed questionnaire, the answer options varied among questions. Specifically, there were three- and four-point Likert scales, which may have biased the research results. Finally but importantly, the sampling error was enlarged due to the difference in sample size between the two subgroups.
Our research revealed that participants scored highly on most common-sense questions and demonstrated good awareness of and protective practices against heat-related illness. However, awareness of exertional heat stroke risks was inadequate. In addition, some differences, and personal experience. Thus, military personnel's awareness of preventive and first-aid measures against heat-related illnesses needs to be strengthened. To address these issues, it is very important to develop educational programmes and enrich systematic educational resources addressing heat-related illnesses.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by the study was approved by the ethics committee of the institutional review board of the Naval Medical University. Written informed consent was obtained from all participants before the survey. All the data obtained was anonymous. The patients/participants provided their written informed consent to participate in this study.
LG and SX conceived and designed the study and administrative support. XW undertook data analysis, results interpretation, and manuscript preparation. DX and XL organized the field works and collected the data. YW and KW was responsible for critical revision of the manuscript. All authors contributed to the article and approved the submitted version.
This study was supported by Shanghai Municipal Education Research projects (C17008) and Special Project of Military Medical Service (21WQ016).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The authors acknowledge with special thanks to all military personnel who participated in this study.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2021.707264/full#supplementary-material
1. Iturbide M, Gutiérrez JM, Alves LM, Bedia J, Cerezo-Mota R, Cimadevilla E, et al. An update of IPCC climate reference regions for subcontinental analysis of climate model data: definition and aggregated datasets. Earth Syst Sci Data. (2020) 124:2959–70. doi: 10.5194/essd-12-2959-2020
2. Li M, Gu S, Bi P, Yang J, Liu Q. Heat waves and morbidity: current knowledge and further direction-a comprehensive literature review. Int J Environ Res Public Health. (2015) 12:5256–83. doi: 10.3390/ijerph120505256
3. Huang W, Kan H, Kovats S. The impact of the 2003 heat wave on mortality in Shanghai, China. Sci Total Environ. (2010) 408:2418–20. doi: 10.1016/j.scitotenv.2010.02.009
4. Kang Y, Yang Q, Bartocci P, Wei H, Liu SS, Wu Z, et al. Bioenergy in China: evaluation of domestic biomass resources and the associated greenhouse gas mitigation potentials. Renew Sustain Energy Rev. (2020) 127:109842. doi: 10.1016/j.rser.2020.109842
5. Vanderplanken K, Hazel P, Marx M, Shams AZ, Guha-Sapir D, van Loenhout JA, et al. Governing heatwaves in Europe: comparing health policy and practices to better understand roles, responsibilities and collaboration. Health Res Policy Syst. (2021) 19:1–14. doi: 10.1186/s12961-020-00645-2
6. Ward K, Lauf S, Kleinschmit B, Endlicher W. Heat waves and urban heat islands in Europe: a review of relevant drivers. Sci Total Environ. (2016) 569:527–39. doi: 10.1016/j.scitotenv.2016.06.119
7. Wang XY, Barnett AG, Yu W, FitzGerald G, Tippett V, Aitken P, et al. The impact of heatwaves on mortality and emergency hospital admissions from non-external causes in Brisbane, Australia. Occup Environ Med. (2012) 69:163–9. doi: 10.1136/oem.2010.062141
8. Varghese B, Beaty M, Panchuk S, Mackie B, Chen C, Jakab M, et al. Heatwave-related Mortality in Australia: who's impacted the most. Eur J Public Health. (2020) 30(Suppl. 5):ckaa165.377. doi: 10.1093/eurpub/ckaa165.377
9. Harlan SL, Declet-Barreto JH, Stefanov WL, Petitti DB. Neighborhood effects on heat deaths: social and environmental predictors of vulnerability in Maricopa County Arizona. Environ Health Perspect. (2013) 121:197–204. doi: 10.1289/ehp.1104625
10. Ma W, Zeng W, Zhou M, Wang L, Rutherford S, Lin H, et al. The short-term effect of heat waves on mortality and its modifiers in China: an analysis from 66 communities. Environ Int. (2015) 75:103–9. doi: 10.1016/j.envint.2014.11.004
11. Zhang J, Liu SQ, Zhou L, Gong SP, Liu YL, Zhang Y, et al. Impact of heat waves on non-accidental deaths in Jinan, China. Zhonghua Lao Dong Wei Sheng Zhi Ye Bing Za Zhi. (2016) 34:115–7. doi: 10.3760/cma.j.issn.1001-9391.2016.02.009
12. Criteria for a Recommended Standard: Occupational Exposure to Ethylene Glycol Monomethyl Ether, Ethylene Glycol Monoethyl Ether, Their Acetates. MMWMorbidity R, and Mortality Weekly Report (1992). 41:386.
13. Hunt AP, Billing DC, Patterson MJ, Caldwell JN. Heat strain during military training activities: the dilemma of balancing force protection and operational capability. Temperature. (2016) 3:307–17. doi: 10.1080/23328940.2016.1156801
14. O'Hara R, Vojta C, Henry A, Caldwell L, Wade M, Swanton S, et al. Effects of a new cooling technology on physical performance in US air force military personnel. J Spec Oper Med. (2016) 16:57–61.
15. Zhang K, Li Y, Schwartz JD, O'Neill MS. What weather variables are important in predicting heat-related mortality? A new application of statistical learning methods. Environ Res. (2014) 132:350–9. doi: 10.1016/j.envres.2014.04.004
16. Ibrahim JE, McInnes JA, Andrianopoulos N, Evans S. Minimising harm from heatwaves: a survey of awareness knowledge and practices of health professionals and care providers in Victoria Australia. Int J Public Health. (2012) 57:297–304. doi: 10.1007/s00038-011-0243-y
17. Gil Cuesta J, van Loenhout JA, Colaço MD, Guha-Sapir D. General population knowledge about extreme heat: a cross-sectional survey in Lisbon and Madrid. Int J Environ Res Public Health. (2017) 14:122. doi: 10.3390/ijerph14020122
18. WHO and UNICEF Recommend New Oral Rehydration Salts (ORS) Formulation. Bulletin of the Pan American Health Organization (1985) 19:99–101.
19. Cai M, Hu J, Zhou C, Hou Z, Xu Y, Zhou M, et al. Mortality burden caused by diurnal temperature range: a nationwide time-series study in 364 Chinese locations. Stochas Environ Res Risk Assess. (2021) 1–10. doi: 10.1007/s00477-021-02016-x
20. Li J, Xu X, Ding G, Zhao Y, Zhao R, Xue F, et al. A cross-sectional study of heat wave-related knowledge, attitude, and practice among the public in the Licheng District of Jinan City, China. Int J Environ Res Public Health. (2016) 13:648. doi: 10.3390/ijerph13070648
21. Hosokawa Y, Adams WM, Belval LN, Davis RJ, Huggins RA, Jardine JF, et al. Exertional heat illness incidence and on-site medical team preparedness in warm weather. Int J Biometeorol. (2018) 62:1147–53. doi: 10.1007/s00484-018-1517-3
24. Akompab DA, Bi P, Williams S, Grant J, Walker IA, Augoustinos M. Awareness of and attitudes towards heat waves within the context of climate change among a cohort of residents in Adelaide, Australia. Int J Environ Res Public Health. (2012) 10:1–17. doi: 10.3390/ijerph10010001
25. Rahaman KS, Majdzadeh R, Holakouie Naieni K, Raza O. Knowledge, Attitude and Practices (KAP) regarding chronic complications of diabetes among patients with type 2 diabetes in Dhaka. Int J Endocrinol Metab. (2017) 15:e12555. doi: 10.5812/ijem.12555
26. McConnell AR, Rydell RJ, Strain LM, Mackie DM. Forming i.mplicit and explicit attitudes toward individuals: social group association cues. J Pers Soc Psychol. (2008) 94:792–807. doi: 10.1037/0022-3514.94.5.792
27. Liu T, Xu YJ, Zhang YH, Yan QH, Song XL, Xie HY, et al. Associations between risk perception, spontaneous adaptation behavior to heat waves and heatstroke in Guangdong province, China. BMC Public Health. (2013) 13:913. doi: 10.1186/1471-2458-13-913
28. Li J, Xu X, Wang J, Zhao Y, Song XP, Liu ZD, et al. Analysis of a community-based intervention to reduce heat-related illness during heat waves in Licheng, China: a Quasi-experimental study. Biomed Environ Sci. (2016) 29:802–13. doi: 10.3967/bes2016.107
29. Harduar Morano L, Watkins S, Kintziger K. A comprehensive evaluation of the burden of heat-related illness and death within the florida population. Int J Environ Res Public Health. (2016) 13:551. doi: 10.3390/ijerph13060551
Keywords: heat wave, heat-related illness, military personnel, China, knowledge, attitude, practice
Citation: Wang X, Xia D, Long X, Wang Y, Wu K, Xu S and Gui L (2021) Knowledge, Attitudes, and Practices of Military Personnel Regarding Heat-Related Illness Risk Factors: Results of a Chinese Cross-Sectional Study. Front. Public Health 9:707264. doi: 10.3389/fpubh.2021.707264
Received: 09 May 2021; Accepted: 27 May 2021;
Published: 25 June 2021.
Edited by:
Alberto Modenese, University of Modena and Reggio Emilia, ItalyReviewed by:
Mainul Haque, National Defence University of Malaysia, MalaysiaCopyright © 2021 Wang, Xia, Long, Wang, Wu, Xu and Gui. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Li Gui, Z3VpbGkyMDAwQHFxLmNvbQ==; Shuogui Xu, c2h1b2d1aTEyNkAxMjYuY29t
†These authors have contributed equally to this work and share first authorship
‡Present address: Xuren Wang, Nursing Department, The Second Naval Hospital of Southern Theater Command of PLA, Hainan, China
Demeng Xia, Department of Orthopaedics, The Naval Hospital of Eastern Theater Command of PLA, Zhejiang, China
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.