 Arunah Chandran
Arunah Chandran Shurendar Selva Kumar
Shurendar Selva Kumar Noran Naqiah Hairi
Noran Naqiah Hairi Wah Yun Low
Wah Yun Low Feisul Idzwan Mustapha
Feisul Idzwan Mustapha
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
POLICY AND PRACTICE REVIEWS article
Front. Public Health, 06 July 2021
Sec. Public Health Policy
Volume 9 - 2021 | https://doi.org/10.3389/fpubh.2021.698741
In 2012, the World Health Organization (WHO) set a comprehensive set of nine global voluntary targets, including the landmark “25 by 25” mortality reduction target, and 25 indicators. WHO has also highlighted the importance of Non-Communicable Disease (NCD) surveillance as a key action by Member States in addressing NCDs. This study aimed to examine the current national NCD surveillance tools, activities and performance in Malaysia based on the WHO Global Monitoring Framework for NCDs and to highlight gaps and priorities moving forward. A desk review was conducted from August to October in 2020, to examine the current national NCD surveillance activities in Malaysia from multiple sources. Policy and program documents relating to NCD surveillance in Malaysia from 2010 to 2020 were identified and analyzed. The findings of this review are presented according to the three major themes of the Global Monitoring Framework: monitoring of exposure/risk factor, monitoring of outcomes and health system capacity/response. Currently, there is a robust monitoring system for NCD Surveillance in Malaysia for indicators that are monitored by the WHO NCD Global Monitoring Framework, particularly for outcome and exposure monitoring. However, Malaysia still lacks data for the surveillance of the health system indicators of the framework. Although Malaysia has an NCD surveillance in place that is adequate for the WHO NCD Global Monitoring Framework, there are areas that require strengthening. The country must also look beyond these set of indicators in view of the increasing burden and impact of the COVID-19 pandemic. This includes incorporating mental health indicators and leveraging on alternate sources of data relating to behaviors.
The World Health Organization (WHO) has described strengthening surveillance at national level as a priority for tackling Non-Communicable Diseases (NCDs) (1–3). The first global strategy for the prevention and control of NCDs endorsed by the World Health Assembly in 2000 highlighted “surveillance to track and monitor the major risk factors” as a key priority (1). The WHO however has also recognized that several key steps must be taken to strengthen surveillance for NCDs (3):
• NCD surveillance systems should be strengthened and integrated into existing national health information systems;
• All three components of the NCD surveillance framework, i.e., outcomes, exposure/risk factors and health system capacity/response should be established and strengthened;
• Monitoring and surveillance of behavioral and metabolic risk factors in low-resource settings should receive the highest priority; and
• A significant acceleration in financial and technical support is necessary for health information system development in low- and middle-income countries (LMICs).
In 2012, the WHO set a comprehensive set of nine global voluntary targets, including the landmark “25 by 25” mortality reduction target, and 25 indicators (1). These targets, a balance between prevention and treatment, introduced priority and accountability for NCDs in member countries. Malaysia is an Upper-Middle-Income country with a current population of 32.73 million (4). Demographic and behavioral shifts, including rapid urbanization, rapid aging, low health literacy, and an obesogenic environment, have contributed to steady increase in the prevalence of NCDs in the country (5). NCDs accounted for 67% of premature deaths in Malaysia, and over 70% of the burden of disease in 2014 (6).
To strengthen Malaysia's response to the increasing burden of NCDs, the National Strategic Plan for Non-Communicable Diseases (NSP-NCD) 2010-2014 was first published in (7). This was then followed by the National Strategic Plan for Non-Communicable Diseases (NSP-NCD) 2016-2025 published in (8). The NSP-NCD is also aligned to the Government's aspiration for nation building, as stated in the medium-term national plan, i.e., 11th Malaysia Plan 2016-2020 (9). The NSP-NCD 2016-2025 had incorporated the WHO NCD global monitoring targets and underscores the critical importance of an effective surveillance system to track, monitor and interpret trends in risk factors, morbidity, and mortality, as well as responsiveness to policies and public health interventions.
The main objective of this study is to examine the current national NCD surveillance tools, activities and performance in Malaysia based on the Global Monitoring Framework for NCDs and to highlight gaps and priorities moving forward.
A desk review was conducted from August to October 2020 to examine the current national NCD surveillance activities in Malaysia from multiple sources using several search strategies: literature databases, search engines, targeted websites and consultations with content experts. These strategies were employed for comprehensiveness and to minimize the risk of omitting relevant key information.
The search strategy included the following groups of terms: Non-Communicable Diseases; Surveillance; Policy (guidelines, standards, frameworks); and Malaysia. For this desk review, a search was conducted in August 2020 using PubMed and Google Scholar. A second strategy involved Google Searches for documents published on the Internet. Due to the vast amount of information available on the Internet and for effective time management, authors relied on relevancy ranking within the search engine to ascertain documents most pertinent to the research objectives. Authors also browsed targeted websites of relevant organizations for gray literature. Recommendations for suitable organizations were solicited from content experts on the research team as well as reviewing lists of organizations related to the research topic. Websites of these organizations were searched for potentially relevant documents (reports, guidelines, policy, and program documents). Finally, content experts were contacted to identify other documents for possible inclusion in the review. The authors also reviewed routine data collected by content experts for the monitoring and evaluation of NCD-related activities in Malaysia.
Implementation of NCD Surveillance in Malaysia is described in this study based on the three major themes of the WHO Global Monitoring Framework for the 25 indicators: monitoring of outcomes; monitoring of exposure/risk factors; and health system capacity/response. An overview of the findings is shown in Table 1.
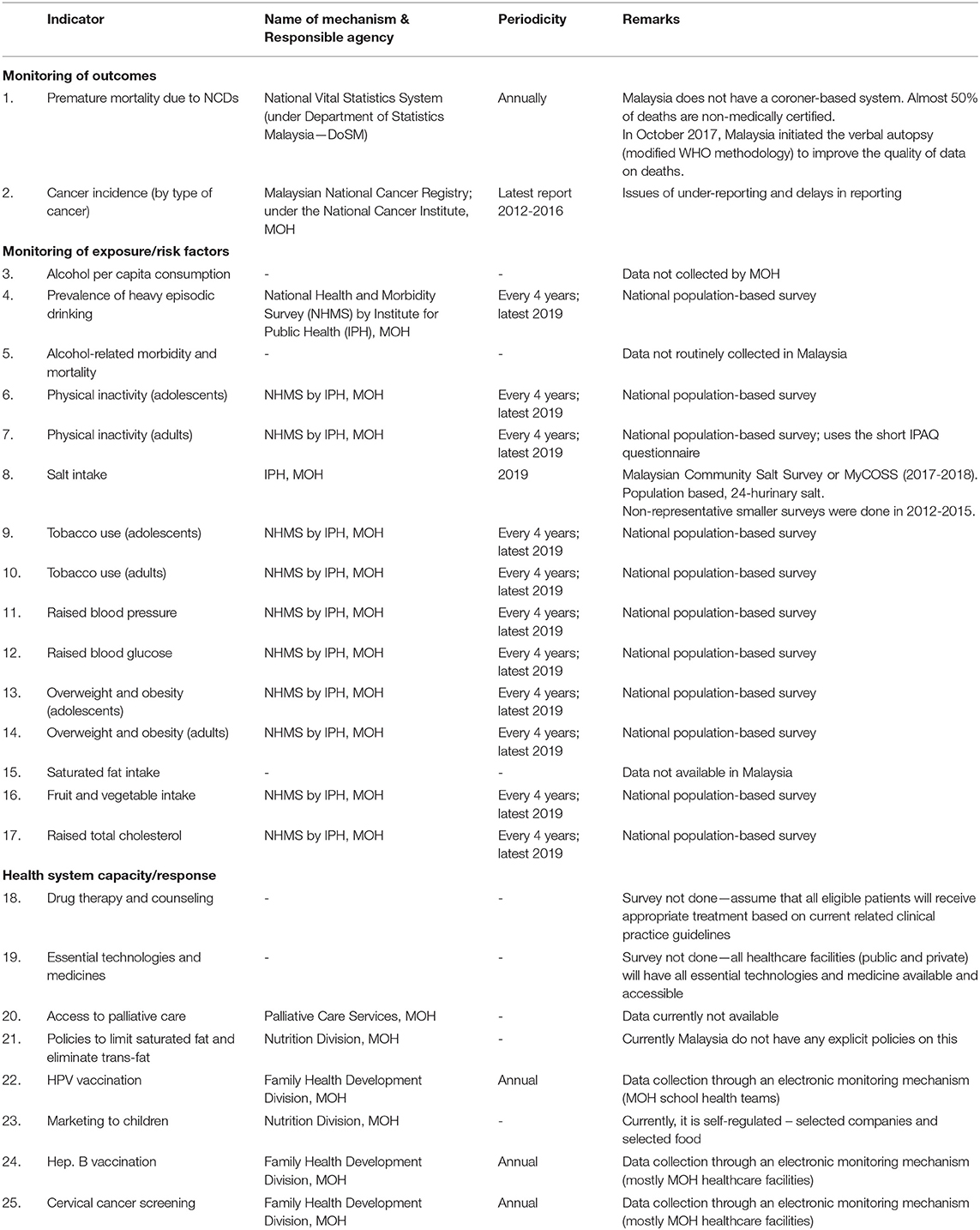
Table 1. Overview of the 25 indicators for the Global Monitoring Framework for Malaysia.
For the data on premature mortality due to NCDs, Malaysia relies on the national vital statistics data by the Department of Statistics, Malaysia (DoSM) to monitor the unconditional probability of dying between ages of 30 and 70 from cardiovascular diseases, cancer, diabetes, or chronic respiratory diseases. However, due to the absence of a coroner-based system, almost 50% of all deaths in the country are non-medically certified.
In order to improve the quality of causes of death data collected by DoSM, the government has introduced the Verbal Autopsy (VA) initiative to improve the quality of data for the death registration (10, 11). This is achieved by increasing the proportion of deaths with medically certified causes through the VA initiative. This was initiated in 2017, through a national circular by the Director General of Health Malaysia, mandating a national system for verification of non-medically certified deaths using the VA methodology (12). The circular prescribes that causes of death for non-medically certified deaths should be verified using VA questionnaires. A mechanism was also established to facilitate data sharing and collaboration between local offices of the National Registration Department (NRD), DoSM, and MOH.
To monitor the incidence of cancer in Malaysia, the Malaysian National Cancer Registry (MNCR) was established in all states in 2007 under the Public Health Program of the MOH (13). The MNCR receives notifications from all data source providers in government and private health facilities using a standardized format. Comprehensive cancer registration is achieved through data obtained from a combination of sources using both passive and active case finding methods, (a) notifications by the medical profession; (b) pathology records; (c) hospital discharges records; (d) mortality data from the NRD and hospital death notification; and (e) Hospital based cancer registry. For cancer cases obtained from sources other than physician notifications, the data will be checked against known registered cases in the registry (14).
In Malaysia, cancer is not a notifiable disease. However, in April 2020, the Director General of Health Malaysia issued an administrative circular, mandating reporting of all cancer patients to MNCR by all registered medical practitioners in both public and private healthcare facilities involved in diagnosing and treating cancer. Public or private health facilities that are not involved directly in the confirmation of a cancer diagnosis, but are involved in cancer treatment, are also encouraged to notify to MNCR if they have complete diagnosis information (for cancer cases that have never been notified).
The National Health and Morbidity Survey (NHMS) for NCD risk factors, which is based on the WHO STEPs survey (15), is a population based cross-sectional survey administered with an interval of four years to monitor NCD risk factors among the adult population (16). There are also other nationally representative surveys that monitor adolescents, and the elderly. This survey monitors all the NCD risk factors monitored in the Global NCD Framework, except for salt and saturated fat intake. A separate population-based survey to monitor salt intake called the MyCOSS study which was specially commissioned in 2018 (17). Saturated fat intake is not routinely monitored at the population level in Malaysia, although data on the population-level overall fat intake is available from NHMS (18).
NHMS uses a standard methodology for a household survey for adults and a school-based survey for adolescents. A multi-stage stratified sampling method is used to produce a nationally representative data. It covers both urban and rural areas in all states in Malaysia. Data is collected by face-to-face interview using structured questionnaires, as well as self-administered questionnaires. Clinical assessment and biochemistry tests are also conducted. Since 2015, the survey information was collected electronically using handheld devices.
MOH does not routinely conduct healthcare facilities surveys to enable reporting for the indicators “drug therapy and counseling” and “essential technologies and medicines.” All healthcare facilities in Malaysia are equipped with essential technologies and first-line medications, both available and accessible, to the population, as Malaysia provides universal health coverage (UHC) to its population (19, 20).
Coverage of the hepatitis B immunization from MOH healthcare facilities is monitored using the HIMS e-reporting system. It is a web-based reporting system, through which, selected health related data from MOH healthcare facilities are transacted to ensure timely and quality health information. However, for non-MOH healthcare facilities, aggregated data is collected through a manual paper-based system.
The HPV Immunization Program in Malaysia was launched in August 2010 and added to the list of the National Immunization Program (NIP), which provides selected vaccines free of charge to all residents as a public health service (21, 22). High rates of school enrolment for 13-year-old (96.0%) and retention of female students in secondary schools have made it possible for the HPV vaccination to be integrated into the School Health Service Program (under MOH) and ensures equal access to the HPV vaccine between urban and rural area (22). The immunization coverage is monitored through a dedicated web-based reporting system.
Cervical cancer screening is conducted in Malaysia as an opportunistic screening. Data on coverage of screening in MOH healthcare facilities is collected via the HIMS e-reporting system. For some non-MOH healthcare facilities, aggregated data is collected through a manual-based system. The NHMS 2011 and 2019 also collected and reported data on the prevalence of pap-smear screening among eligible populations.
Malaysia does not routinely collect data on access to palliative care, which is assessed by morphine-equivalent consumption of strong opioid analgesics (excluding methadone) per death from cancer. MOH launched the “National Palliative Care Policy and Strategic Plan 2019-2030” in (23) in order to strengthen overall policies related to palliative care, including surveillance.
The MOH gazetted the mandatory declaration on the amount of trans fatty acids together with the amount of saturated fatty acids, monounsaturated fatty acids and polyunsaturated fatty acids on nutrition labels, when a claim is made regarding the amount and/or types of fatty acids in (24). In addition, the Malaysian Food Act 1983 Food (Amendment) Regulation 2003 has also made provisions for nutrient content claims on low and free trans fatty acids in foods. However, there is no law or policy as yet to limit the amount of trans fat in food. MOH also does not have specific policies related to marketing of foods and non-alcoholic beverages high in saturated fats, trans fatty acids, free sugars, or salt.
Currently, there is a robust monitoring system for NCD Surveillance in Malaysia for indicators that are monitored by the WHO NCD Global Monitoring Framework, particularly for outcome and exposure monitoring. However, Malaysia still lacks data for the surveillance of the health system indicators of the framework.
For monitoring of mortalities, despite the existence of laws on civil registration in Malaysia that requires registration of all deaths occurring in the country, deaths that occur outside a health facility can still be certified by a non-medical enforcement officer. In 2018, this was approximately half the death that occurred. For these deaths, the top causes cited are often non-medical terms such as “old age” (10). The coroner system for death inquiry only applies for investigation of suspicious and violent deaths, and other deaths as specified under the Criminal Procedure Code [Act 593]. Due to the socio-cultural context of the need for rapid burial of the dead in Malaysia, it is unlikely that any changes to the registration of deaths system will occur soon.
With regards to cancer incidence, there are possibilities of under-reporting of cancer cases in the country, due to the lack of mandatory requirement for reporting by medical practitioners in the country. We also postulate that some patients with cancers may not seek treatment at healthcare facilities and instead seek alternative non-proven therapies elsewhere. There are several studies that have shown delays in presentation and diagnosis of cancer patients in Malaysia due to these factors (25–27).
The challenges to fulfill the criteria for indicators in the health system category arises from the dichotomous healthcare system in Malaysia, whereby the public and private healthcare services co-exist and there is an absence of a national and interconnected electronic medical record (EMR) system. There is also an absence of a regular facility-based surveillance for NCD management at both primary and secondary care levels.
Although there are already several web-based systems in place to collect data for hepatitis B vaccination, HPV vaccination and cervical cancer screening, these still require primary data entry by the healthcare providers. Limited availability of computers, poor connectivity, limited time for data entry by healthcare providers may affect quality. While data submission for public facilities can be made compulsory by a top-down administrative circulars, there is no regulatory mechanism for mandatory data submission by private healthcare facilities. However, some limited data on private healthcare facilities are available through ad hoc primary care and hospital surveys (28, 29).
There are two major challenges posed by COVID-19 and the movement restrictions on NCD surveillance, firstly on data collection, and secondly monitoring for the NCD-related consequences due to COVID-19 and the movement restrictions. A recent review has shown people living with NCDs are at higher risk of more severe infection and mortality due to COVID-19, and that the movement restrictions have already caused disruptions to the screening, treatment, self-care and surveillance of NCD patients (30).
Supplementation of mortality data with VA has been affected due to the COVID-19 pandemic. Implementation of the VA initiative requires home visits and face-to-face interviews. During the movement restrictions, members of the public are also reluctant to come into contact with healthcare workers. In addition, the healthcare workers assigned for VA work have been re-assigned to support COVID-19 response. The re- assignment of healthcare workers has also disrupted data collection and data entry at primary healthcare facilities.
For population-based surveys, despite the fact that data collection can still be continued under the new COVID-19 standard operating procedures (SOPs), modifications have to be made in terms of the work processes to limit face-to-face interactions. For example, for NHMS 2020, blood taking was conducted at the study locations. These modifications, that also includes the use of PPE by the survey enumerators, add to the costs of data collection. This added to the fear of COVID-19 infection risk by the general population would negatively impact the response rate of participants and the quality of data collected.
We would need to look beyond the NCD WHO Global Monitoring Framework as the current NCD surveillance systems in many LMICs, including Malaysia, will not be able to monitor the NCD-related consequences due to COVID-19 in a timely manner. For Malaysia, firstly, this will require strengthening surveillance of mental health problems in the country, focusing on vulnerable groups. Some data is currently available on the utilization of mental health and psychosocial support services helplines that have been made available during this COVID-19 pandemic, as well as other existing social support services by the government. However, the coverage, representativeness and utility of this data is limited.
Secondly, the disruption to the availability and accessibility of primary healthcare services, from both the healthcare providers' perspective as well as the patients' perspective, must also be monitored at regular intervals. There is currently no existing efficient mechanism for such monitoring in the country. Thirdly, clinical process indicators and several selected clinical outcome indicators must also be measured at regular intervals. In the absence of electronic medical records, effective collection of data for these variables will require novel approaches.
The adoption of electronic health records (EHR) could improve the availability and accuracy of data from healthcare facilities. Databases of healthcare facilities providing longitudinal electronic health records data allow patterns to be detected in real time, as well as rapid shifts in morbidity, risk factors and delivery of health care. These databases become a reliable repository for NCD surveillance if it can be cross-referenced across public and private health facilities and provide a platform for meaningful local action.
In Malaysia, data capture procedures are mostly done manually and conducted retrospectively by tracing the patient's health characteristics and care characteristics. This approach is costly with a high risk of missed values and imprecisions. Research has shown that the use of EHRs has the potential to help enhance the privacy, efficiency and cost- effectiveness of healthcare services (31). However, many factors may lead to the low acceptance of the EHR method, including high costs, respect for the data of the privacy user, social effects, too difficult to use method and lack of training (32, 33).
Under current circumstances, such a comprehensive EHR will be beyond the country's financial capacity. Therefore, one option moving forward could be an augmented sentinel surveillance at the primary care level can provide important information on the progression of the different aspects of NCD services and utilization on a routine basis (34).
Beyond population-based surveys, we should also leverage on the use of existing technologies to closely monitor behavioral NCD risk factors. This will enable us to monitor both the current status as well as the immediate impact of any intervention activities or initiatives relating NCD-related behaviors.
In Malaysia, an estimated 87.4% of the population are internet users (35). Smartphones remained at the most common device used to access the Internet with 93.1% of users use smartphones to go online (35). Online technologies such as smartphone apps, messaging platforms and e-learning are changing how improving health education programmes are delivered. The WHO's “Be He@lthy, Be Mobile” Initiative for example, has created a population-wide digital health preventive toolkit, including SMS notifications, mobile physical application, and digital health education (36).
In one study, phone usage data provided behavioral indicators that were strongly related to depressive symptom severity (37), while another international study of smartphone data highlighted global physical activity inequalities and potential areas for intervention (38). Another study found a linkage between anger and fatigue expressed on Twitter, to an increased risk of heart disease (39). Social media has also shown the association between likelihood of alcohol consumption and number of Facebook likes (40).
Additionally, high-frequency and high-resolution sensor data, from wearable technologies to environmental sensors offer the prospect of identifying new NCD risk factors, insights into lifestyle behaviors, and tracking patient engagement in self-care and chronic illnesses management (41, 42). For example, such sensors have been extensively used for remote monitoring of patients with cardiovascular disease (43).
Mining of virtual digital trails such as social media data offers the opportunity to assess self- reported health related attitudes and behaviors pertaining to NCDs and their risk factors in near real-time and can complement other NCD surveillance data (44, 45). Real-life digital trails are signals produced by people's everyday actions, recorded digitally through devices and sensors measuring individuals' movements and behaviors. There is need to innovate and expand NCD Surveillance with the use of big data and artificial intelligence (AI). The practicality of these solutions remains to be seen but it nevertheless remains an interesting option. Achieving NCD Surveillance using big data and AI needs to consider legal, ethical and technical challenges (46).
NCD surveillance is an essential component in a country's response on the increasing burden of NCDs, affecting the health outcomes and quality of life of the population, as well as the negative impact on a nation's economic development.
Although the current NCD surveillance in Malaysia is able to provide most of the data for the indicators in the WHO NCD Global Monitoring Framework, there is a need for the country to look beyond these set of indicators. There is also an urgent need for strengthening the surveillance, incorporate the appropriate mental health component indicators, as well leverage on alternate sources of data (e.g., social media data), in view of the expected increasing burden of NCDs and current challenges in planning, monitoring and evaluation of interventions.
While much attention has been put on the burden of chronic physical illness, mental health is an area that tends to be neglected. It is hoped that the whole-of-government approach can be strengthened with the involvement of partnership with various stakeholders to prevent and control NCDs in Malaysia. The current COVID-19 pandemic and movement restrictions, resulting in NCD-related collateral damages, will provide further justification for the need for strengthening the NCD surveillance systems in all countries, including Malaysia.
AC and SS conceived, designed the framework, and prepared the initial draft. AC, SS, and FM further refined the draft based on interpretation of the data. All authors reviewed and approved the final manuscript.
We acknowledge funds from Thai Health in supporting this project.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
We would like to thank the Director General of Health, Malaysia for his permission to publish this article.
1. WHO. Global Action Plan for the Prevention and Control of Noncommunicable Diseases 2013–2020. Geneva: WHO (2013).
2. World Health Organization. Preventing Chronic Diseases: A Vital Investment: WHO Global Report. Geneva: World Health Organization (2005).
3. Alwan A, MacLean DR, Riley LM, d'Espaignet ET, Mathers CD, Stevens GA, et al. Monitoring and surveillance of chronic non-communicable diseases: progress and capacity in high-burden countries. Lancet. (2010) 376:1861-8. doi: 10.1016/S0140-6736(10)61853-3
4. Department of Statistics Malaysia. Population and Demography. Available online at: https://www.dosm.gov.my/v1/index.php?r=column/ctwoByCat&parent_id=115&menu_id=L0pheU43NWJwRWVSZklWdzQ4TlhUUT09 (accessed August 25, 2020).
5. Miranda JJ, Kinra S, Casas JP, Davey Smith G, Ebrahim S. Non-communicable diseases in low- and middle-income countries: context, determinants and health policy. Trop Med Int Health. (2008) 13:1225-34. doi: 10.1111/j.1365-3156.2008.02116.x
6. Institute for Public Health. Malaysian Burden of Disease and Injury Study 2009-2014. Kuala Lumpur: Ministry of Health Malaysia (2017).
7. Ministry of Health. National Strategic Plan for Non-Communicable Disease (NSP- NCD) 2010-2014. Putrajaya: Ministry of Health (2010).
8. Ministry of Health. National Strategic Plan for Non-Communicable Disease (NSP- NCD) 2016-2025. Putrajaya: Ministry of Health (2016).
9. Government of Malaysia. Eleventh Malaysia Plan 2016-2020. Putrajaya: Office of the Prime Minister (2015).
10. Ganapathy SS, Yi KY, Omar MA, Anuar MFM, Jeevananthan C, Rao C. Validation of verbal autopsy: determination of cause of deaths in Malaysia 2013. BMC Public Health. (2017) 17:653. doi: 10.1186/s12889-017-4687-8
11. Omar A, Ganapathy SS, Anuar MFM, Khoo YY, Jeevananthan C, Awaluddin SM, et al. Cause-specific mortality estimates for Malaysia in 2013: results from a national sample verification study using medical record review and verbal autopsy. BMC Public Health. (2019) 19:1-12. doi: 10.1186/s12889-018-6384-7
12. Rao C, Omar MA, Ganapathy SS, Tamin NSI. Strengthening mortality statistics for health programs in Malaysia: lessons from the field. Dr Sulaiman Al Habib Med J. (2019) 1:52-4. doi: 10.2991/dsahmj.k.191214.003
13. Omar Z, Ibrahim Tamin N. National Cancer Registry Report: Malaysia Cancer Statistics- Data and Figure. National Cancer Registry (2011) p. 85-7.
14. Ministry of Health. Malaysian National Cancer Registry Report 2012-2016. Putrajaya: Ministry of Health (2019).
15. WHO STEPS Surveillance Manual: The WHO STEPwise Approach to Chronic Disease Risk Factor Surveillance. Geneva: WHO (2005).
16. Fadhli Y, Azaadi O, Noor Ani A, Balkish M, Ahmad Jessree K, Tahir A. Approaches in methodology of a population-based study in Malaysia: the National Health and Morbidity Survey 2011 (NHMS 2011). Malays J Med Health Sci. (2013) 9:25-33. Available online at: https://medic.upm.edu.my/upload/dokumen/FKUSK1_MJMHS_2013V09N2_OP04.pdf
17. Institute for Public Health. Population-Based Salt Intake Survey to Support the National Salt Reduction Programme for Malaysia (Malaysian Community Salt Survey - MyCoSS). Kuala Lumpur: Ministry of Health Malaysia (2019).
18. Institute for Public Health. National Health and Morbidity Survey 2014: Malaysian Adult Nutrition Survey Volume 1: Methodology and General Findings. Kuala Lumpur: Institute for Public Health (2014).
19. Savedoff WD, Smith AL. Achieving Universal Health Coverage: Learning From Chile, Japan, Malaysia and Sweden. Washington, DC: Results for Development Institute. (2011).
20. Wan NC, Hairi NNM, Jenn NC, Kamarulzaman A. Universal health coverage in Malaysia: issues and challenges. In: Peng TN, Cheok CK, Rasiah R, editors. Revisiting Malaysia's Population–Development Nexus. Kuala Lumpur: Faculty of Economics and Administration (FEA), University of Malaya (2014). p. 175.
21. Buang SN, Ja'afar S, Pathmanathan I, Saint V. Making multisectoral collaboration work: human papillomavirus immunisation of adolescent girls: improving coverage through multisectoral collaboration in Malaysia. BMJ. (2018) 363:2. doi: 10.1136/bmj.k4602
22. Muhamad NA, Buang SN, Jaafar S, Jais R, Tan PS, Mustapha N, et al. Achieving high uptake of human papillomavirus vaccination in Malaysia through school-based vaccination programme. BMC Public Health. (2018) 18:1402. doi: 10.1186/s12889-018-6316-6
23. Ministry of Health. National Palliative Care Policy and Strategic Plan 2019-2030. Putrajaya: Ministry of Health Malaysia (2019).
24. Fauziah A, Sundram K. Trans-fatty acids - an update on its regulatory status. Palm Oil Dev. (2003) 39:16-9. Available online at: http://palmoilis.mpob.gov.my/publications/POD/pod39-p16.pdf
25. Mohd Mujar NM, Dahlui M, Emran NA, Abdul Hadi I, Wai YY, Arulanantham S, et al. Complementary and alternative medicine (CAM) use and delays in presentation and diagnosis of breast cancer patients in public hospitals in Malaysia. PLoS ONE. (2017) 12:e0176394. doi: 10.1371/journal.pone.0176394
26. Taib NA, Yip CH, Low WY. A grounded explanation of why women present with advanced breast cancer. World J Surg. (2014) 38:1676-84. doi: 10.1007/s00268-013-2339-4
27. Zulkipli AF, Islam T, Mohd Taib NA, Dahlui M, Bhoo-Pathy N, Al-Sadat N, et al. Use of Complementary and Alternative Medicine Among Newly Diagnosed Breast Cancer Patients in Malaysia: An Early Report From the MyBCC Study. Integr Cancer Ther. (2017) 17:312-21. doi: 10.1177/1534735417745248
28. Sivasampu S, Wahab Y, Ong SM, Ismail S, Goh P, Sinnadurai J. National Medical Care Statistics (NMCS) 2014. Kuala Lumpur: National Clinical Research Centre, National Healthcare Statistics Initiative (2016).
29. Hwong W, Sivasampu S, Aisyah A, Shantha Kumar C, Goh P, Hisham A. National Healthcare Establishment & Workforce Statistics (primary care) 2012. Kuala Lumpur: National Clinical Research Centre (2014).
30. Chang AY, Cullen MR, Harrington RA, Barry M. The impact of novel coronavirus COVID-19 on noncommunicable disease patients and health systems: a review. J Intern Med. (2021) 289:450–62. doi: 10.1111/joim.13184
31. Heart T, Ben-Assuli O, Shabtai I. A review of PHR, EMR and EHR integration: a more personalized healthcare and public health policy. Health Policy Technol. (2017) 6:20-5. doi: 10.1016/j.hlpt.2016.08.002
32. Enaizan O, Eneizan B, Almaaitah M, Al-Radaideh AT, Saleh AM. Effects of privacy and security on the acceptance and usage of EMR: the mediating role of trust on the basis of multiple perspectives. Inform Med Unlocked. (2020) 21:100450. doi: 10.1016/j.imu.2020.100450
33. Arman AA, Hartati S editors. Development of user acceptance model for electronic medical record system. In: 2015 International Conference on Information Technology Systems and Innovation (ICITSI). IEEE (2015). doi: 10.1109/ICITSI.2015.7437724
34. Kroll M, Phalkey R, Dutta S, Shukla S, Butsch C, Bharucha E, et al. Involving private healthcare practitioners in an urban NCD sentinel surveillance system: lessons learned from Pune, India. Glob Health Action. (2016) 9:32635. doi: 10.3402/gha.v9.32635
35. Malaysian Communications and Multimedia Commission. Internet Users Survey 2018. Cyberjaya: Malaysian Communications and Multimedia Commission (2018).
36. World Health Organization and International Telecommunication Union. Be He@lthy, Be Mobile Annual Report 2018. Geneva: World Health Organization and International Telecommunication Union (2019).
37. Saeb S, Zhang M, Karr CJ, Schueller SM, Corden ME, Kording KP, et al. Mobile phone sensor correlates of depressive symptom severity in daily-life behavior: an exploratory study. J Med Internet Res. (2015) 17:e175. doi: 10.2196/jmir.4273
38. Althoff T, Sosič R, Hicks JL, King AC, Delp SL, Leskovec J. Large-scale physical activity data reveal worldwide activity inequality. Nature. (2017) 547:336-9. doi: 10.1038/nature23018
39. Eichstaedt JC, Schwartz HA, Kern ML, Park G, Labarthe DR, Merchant RM, et al. Psychological language on Twitter predicts county-level heart disease mortality. Psychol Sci. (2015) 26:159-69. doi: 10.1177/0956797614557867
40. Hendriks H, Van den Putte B, Gebhardt WA, Moreno MA. Social drinking on social media: content analysis of the social aspects of alcohol-related posts on Facebook and Instagram. J Med Internet Res. (2018) 20:e226. doi: 10.2196/jmir.9355
41. Elgendi M, Howard N, Lovell N, Cichocki A, Brearley M, Abbott D, et al. A six-step framework on biomedical signal analysis for tackling noncommunicable diseases: current and future perspectives. JMIR Biomed Eng. (2016) 1:e1. doi: 10.2196/biomedeng.6401
42. Khakurel J, Pöysä S, Porras J editors. The use of wearable devices in the workplace-a systematic literature review. In: International Conference on Smart Objects and Technologies for Social Good. Springer (2016).
43. Meng K, Chen J, Li X, Wu Y, Fan W, Zhou Z, et al. Flexible weaving constructed self- powered pressure sensor enabling continuous diagnosis of cardiovascular disease and measurement of cuffless blood pressure. Adv Funct Mater. (2019) 29:1806388. doi: 10.1002/adfm.201806388
44. Balicer RD, Luengo-Oroz M, Cohen-Stavi C, Loyola E, Mantingh F, Romanoff L, et al. Using big data for non-communicable disease surveillance. Lancet Diabetes Endocrinol. (2018) 6:595-8. doi: 10.1016/S2213-8587(17)30372-8
45. Kite J, Foley BC, Grunseit AC, Freeman B. Please like me: Facebook and public health communication. PLoS ONE. (2016) 11:e0162765. doi: 10.1371/journal.pone.0162765
Keywords: health systems, Malaysia, non-communicable disease, public health, surveillance
Citation: Chandran A, Selva Kumar S, Hairi NN, Low WY and Mustapha FI (2021) Non-communicable Disease Surveillance in Malaysia: An Overview of Existing Systems and Priorities Going Forward. Front. Public Health 9:698741. doi: 10.3389/fpubh.2021.698741
Received: 22 April 2021; Accepted: 10 June 2021;
Published: 06 July 2021.
Edited by:
Georgi Iskrov, Plovdiv Medical University, BulgariaReviewed by:
Jamal Hisham Hashim, Universiti Selangor, MalaysiaCopyright © 2021 Chandran, Selva Kumar, Hairi, Low and Mustapha. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Feisul Idzwan Mustapha, ZHIuZmVpc3VsQG1vaC5nb3YubXk=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.