 Aboma Motuma
Aboma Motuma Tesfaye Gobena2
Tesfaye Gobena2 Kedir Teji Roba
Kedir Teji Roba- 1School of Nursing and Midwifery, College of Health and Medical Sciences, Haramaya University, Harar, Ethiopia
- 2Department of Environmental Health Science, College of Health and Medical Sciences, Haramaya University, Harar, Ethiopia
- 3Department of Epidemiology and Biostatics, Addis Continental Institute of Public Health, Addis Ababa, Ethiopia
- 4Department of Epidemiology and Biostatistics, School of Public Health, Addis Ababa University, Addis Ababa, Ethiopia
Background: Sedentary behavior is a major risk factor for non-communicable diseases. Due to changes in lifestyle, sedentary behavior is increasing in sub-Saharan Africa. However, information on the extent of sedentarism among various segments of the population is scant in low-income countries. The objective of this study was to assess the extent of high sedentary behavior and associated factors among working adults in eastern Ethiopia.
Methods: A crosssectional study was conducted among 1,164 working adults at Haramaya University from December 2018 to February 2019. Data were collected through face-to-face interviews using the WHO STEPS and sedentary behavior questionnaire. All reported sedentary activities were added to calculate the total number of hours spent on sedentary behavior, which was then dichotomized into two categories. Those who had ≥8 sedentary hours per day were categorized as having high sedentary behavior. The prevalence ratio (PR) with 95% confidence intervals (CIs) was calculated. Factors associated with outcome variables were identified using Poisson regression with a robust variance statistical model.
Results: The prevalence of high sedentary behavior was 20.3% (95% CI, 18.0–22.7%) among the study participants. The prevalence of high sedentary behavior was associated with age 45–54 years adjusted PR (APR: 2.00; 95% CI = 1.01–3.97) and 55–64 years (APR: 2.16; 95% CI = 1.03–4.57), being a non-manual worker (APR: 2.11; 95% CI = 1.46–3.05), frequent khat chewers (APR: 1.57; 95% CI = 1.22–2.01), with body mass index of ≥25 kg/m2 (APR: 1.93; 95% CI = 1.53–2.44), and regular alcohol drinker (APR: 1.39; 95% CI = 1.11–1.76).
Conclusion: One-fifth of working adults had high sedentary behavior. Factors associated with high sedentary behaviors were older age, being a non-manual worker, substance-use behaviors, and having a high body mass index.
Introduction
Sedentary behavior is characterized by low energy expenditure (1), whether that behavior is due to leisure or occupation (2). The increasing availability of modern technology, transportation, and communication systems have exacerbated the problem in low-income countries (3). Sedentary behavior has emerged as a public health concern due to the increasing trend in non-communicable diseases (NCDs) (4) with grave consequences of morbidity, death, and disability (5–8).
Sedentary behavior has an important implication on the health status of working adults (9). Evidence shows that white collar workers such as university employees accumulate a high sedentary time at workplaces (10), which often extends to outside normal working hours (11, 12). Studies have shown that university workers spend over two-thirds of their workday sitting (9, 13, 14). Studies conducted among college employees also indicated that the working days of the administrative staff were more sedentary when compared with faculty members (15). Evidence shows that high sedentary behaviors were associated with metabolic syndrome (16) and obesity (17) among university faculty.
Evidence indicates that occupational sedentary behavior was not significantly associated with productivity (9); however, employees with increased sedentary behavior were more prone to illnesses such as back pain, mental health, diabetes, and cardiovascular diseases, which indirectly can influence productivity at work (12, 18). Generally, high sedentary behavior is one of the modifiable risk factors contributing to premature mortality among adults in low-income countries (6, 19), although sedentarism is still is relatively low in the general population compared with higher-income countries (20).
However, this difference is rapidly closing in some occupational categories such as that of university employees (21). The risk factors for high sedentary behavior have been well-studied in high and middle-income countries. The information on the extent of and risk factors associated with high sedentary behavior is scant in the sub Saharan Africa. Therefore, the aim of this study was to assess the prevalence of high sedentary behavior and its associated factors among working adults in Eastern Ethiopia.
Materials and Methods
Study Setting, Design, and Period
This study was conducted at a public university (Haramaya University) found in East Ethiopia. Haramaya University has four campuses, eleven academic and research units, and four health clinics that provide services to the university community. The university also runs a specialized referral hospital in Harar town that provides services to the general population. The total student population in both regular program and non-regular programs is 30,355. The students attend their education at the undergraduate and graduate levels. The university has about 7,176 employees, with a gender mix of 28.1% female and 71.9% male, and a job mix of 21.1% academic and 78.9% administrative staff. This university was considered for the study because of its large employee size and diversity of jobs, which ranges from senior academic positions to manual work. The university's main campus is located in a rural setting where khat (a locally cultivated stimulant plant) production and consumption is high. A crosssectional study was conducted among 1,164 working adults from December 2018 to February 2019.
Study Population and Sampling Procedures
The study involved all permanent employees who worked for at least 6 months at the university. All departments and units of the university were considered for the study. The study participants were selected from each unit proportional to the size of their respective department staff size. In each unit, the study participants were selected randomly from the payroll roster, which was used as the sampling frame. We calculated the sample size assuming a 29.6% prevalence of sedentary behavior (22), 95% level of confidence, 3% margin of error, and 20% non-response rate. Accordingly, the calculated sample size was 1,106. The total sample size was distributed to each unit as described above.
Study Tool and Data Collection Procedures
Data were collected using a structured questionnaire adapted from the WHO STEPS and sedentary behavior questionnaires (23, 24). The questionnaire was previously used in Ethiopia in various settings. The English questionnaire was translated to Amharic by language experts who are competent in both English and Amharic to ensure the consistency and accuracy of the translation. Then, the tool was pretested in a nearby public university. Some questions and the translation were refined based on the feedback we obtained during the pretest.
Variables and Measurement
High sedentary behavior was measured for 10 activities: watching television, playing computer/video games or social media, sitting during eating and drinking, sitting while listening to music, sitting and talking on the phone, doing paperwork or office work, napping, sitting and reading, sitting for socializing with friends and/or family activities, and sitting and driving/riding in a car or bus (24). The items were completed for weekdays and weekends separately and grouped into three domain-specific (occupation, leisure time, and transportation) sedentary behavior. The occupation domain included paperwork or desk-based office work; leisure time domain comprised watching television, napping, playing computer/video games, sitting during eating and drinking, sitting while listening to music, sitting and talking on the phone, sitting during reading, and sitting for socializing with family or/and friends; and transportation domain comprised of sitting and driving motorized vehicle (1, 6).
The average total sedentary time per day was obtained by computing the sum of the 10 items. Currently, there is no well-accepted threshold to categorize a cut-off point for high sedentary behavior (25). However, previous evidence indicated that 8 or more hours of sedentary behavior was associated with a high risk for premature mortality (26–30). Hence, we used ≥8 h/day as a cut-off point for high sedentary behavior (6, 26, 27). For the specific domains (occupation, transportation, and leisure) a 75th percentile or above was used as a thresholds cut-off of high occupation sedentary behavior ≥3 h/day, high leisure sedentary behavior ≥5.05 h/day, and high transportation sedentary behavior ≥1 h/day (6).
The age of respondents was recorded based on their response and categorized into 18–24 years, 25–34 years, 35–44 years, 45–54 years, and 55–64 years of age groups. Education level was grouped into ≤ grade 8, grade 9–12, college and undergraduate, and postgraduate. The working status of the respondent was grouped into manual/laborer work or non-manual based on the classification of the Human Resource Office of the university. The income cut-off of the study participants was set to roughly correspond to the poverty line in accordance with the World Bank (31).
Body weight was measured using a digital weighing scale to the nearest 0.1 kg with the participants barefooted and wearing light clothes. Height was measured using a stadiometer to the nearest 0.1 cm with the shoes and any hats or hair ornaments of the participant removed. Body mass index was calculated as weight in kilograms over height in meters squared, and was categorized according to World Health Organization (WHO) criteria (underweight: BMI < 18.5 kg/m2; normal: BMI = 18.5–24.9 kg/m2; overweight: BMI = 25.0–29.9 kg/m2; and obese: BMI ≥ 30.0 kg/m2) (23).
Smoking status was categorized as never smoked, former smoker, and current smoker. Alcohol consumption was measured based on the WHO Stepwise approach. In this study, we asked about the drinking habits of the participant. The alcohol drinking habits of the study participants during the survey period were classified as never, occasional, and frequent drinkers (23). Khat (catha edulis) use habit was grouped into never, the occasional, and habitual (frequent) user. The total physical activity score was computed as the sum of all metabolic equivalent (MET)-minutes per week for vigorous intensity physical activity, moderate intensity physical activity, and walking. The sum MET-minutes per week was categorized as high (3,000 MET-minutes or above), moderate (between 2,999 and 600 MET-minutes), and low (<600 MET-minutes) (32). Data collection methods and study procedures have been presented in detail in a previous publication (33).
Data Management and Analysis
The completed questionnaires were double entered into EpiData Version 3.1, cleaned, and exported to STATA 14 statistical software for data analysis. The missing values of each variable were <1%, and the chance of missing was unrelated to any of the variables and considered as missing completely at random. Hence, a complete case analysis was used to handle the missing data. Descriptive statistics were used to calculate the frequency distribution, proportions with 95% confidence interval for categorical variables, and mean and standard deviation for continuous variables. A Poisson regression model with robust variance estimation was used to assess factors associated with the outcome variable. The Poisson regression analysis model is an appropriate analytical model for estimating the prevalence ratio (PR) in crosssectional studies binary and common outcomes (34). The backward regression was fitted with selected explanatory variables. Crude PRs (CPRs) with 95% CIs were estimated to assess the association between each independent variable and the outcome variable. Variables with a p-value of ≤0.25 in the bivariate analysis were considered for multivariable analysis. A p-value of <0.05 was used to declare the level of statistical significance in the multivariable analysis, and adjusted PRs (APRs) along with 95% CIs were estimated. The explanatory variables were tested for multicollinearity and checked for interaction among the explanatory variables before fitting them into multivariable model.
Results
Socio-Demographic Characteristics
A total of 1,200 study participants were invited for the study and 1,164 study subjects actually participated in the study, which yields a response rate of 97%. Nearly half (51.4%) of the participants were males and the mean age of the study participants was 35.5 years. The proportion of currently married was 57.3%, diploma or higher degree holders was 63.5%, and those with 10 years or below at the university were 76.1% (Table 1).
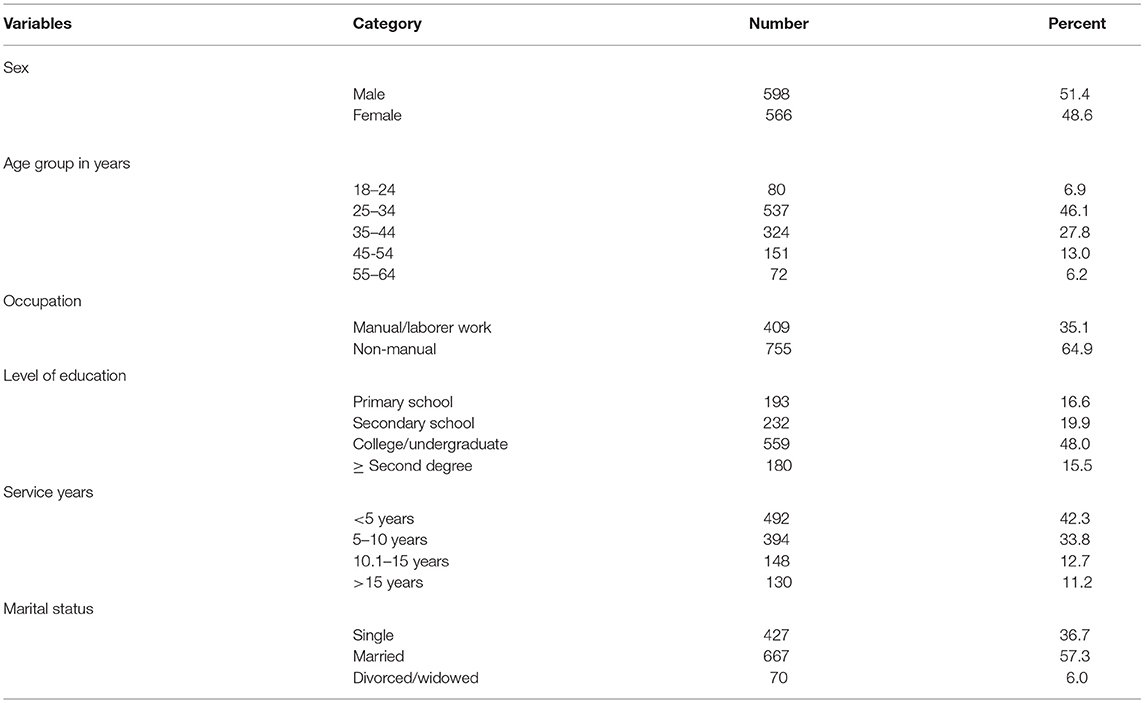
Table 1. Socio-demographic characteristics of the study participants in Eastern Ethiopia, 2019 (n = 1,164).
Lifestyle and Health Related Characteristics
About half of the study participants around 571 (49.1%) had low physical activity (<600 MET-minutes per week), 396 (34.0%) were regular khat users, and 553 (47.5%) were frequent alcohol consumers. Few of the study participants 131(11.3%) were ever smokers of whom 9.4% were males. Out of these, 59 (5.1%) were current smokers. Four hundred and thirteen (35.5%) and 109 (9.8%) working adults were overweight and obese, respectively. Most of the study participants 512 (44%) reported their health status rank from fair to poor health status (Table 2).
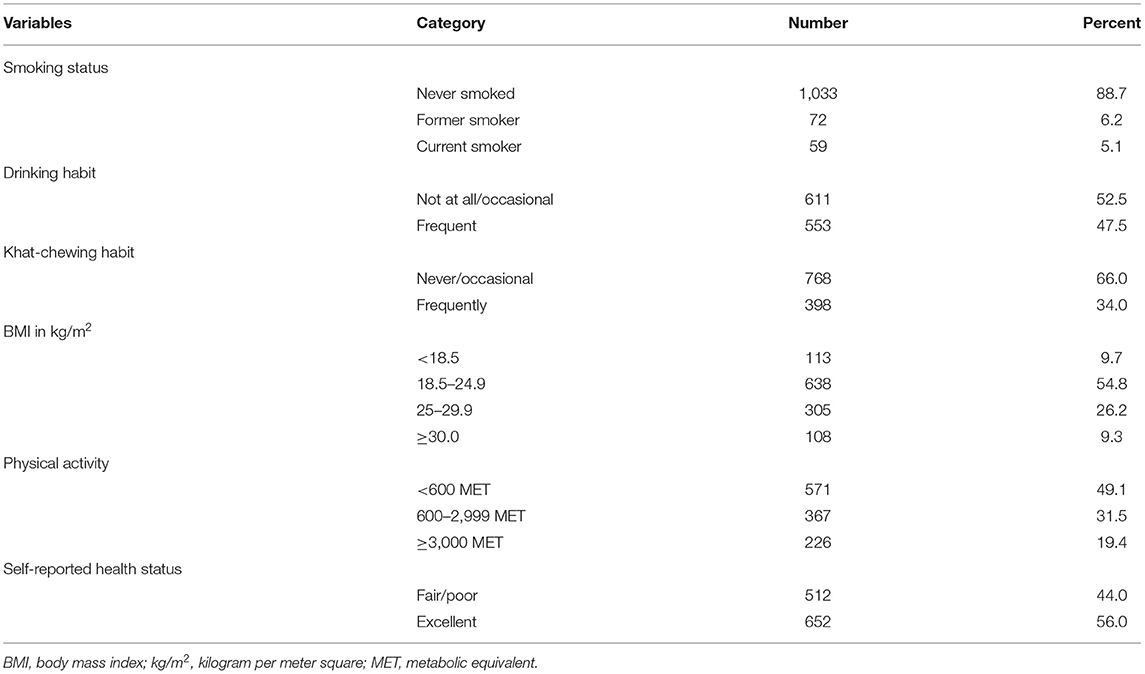
Table 2. Lifestyle and health related characteristics of study participants in Eastern Ethiopia, 2019 (n = 1,164).
The Mean Self-Report Sedentary Behavior Among Study Participants
The total mean (±SD) time of sedentary behavior was 5.9 (±2.1) hours per day, 6.2 (±2.2) on weekends, and 5.8 (±2.3) hours per day on working days. The mean (±SD) sedentary time reported during leisure time was 3.7 (±1.5) hours per day, 1.9 (±1.8) hours per day at workplace, and 0.4 (±0.5) hours per day while using transportation (Table 3). The commonest sedentary activities included watching TV/video or playing social media, doing paperwork or desk-based office work, and socializing with friends and/or family. Almost all sedentary time spent on different activities showed a slight increase on weekends compared with weekdays (Table 4).
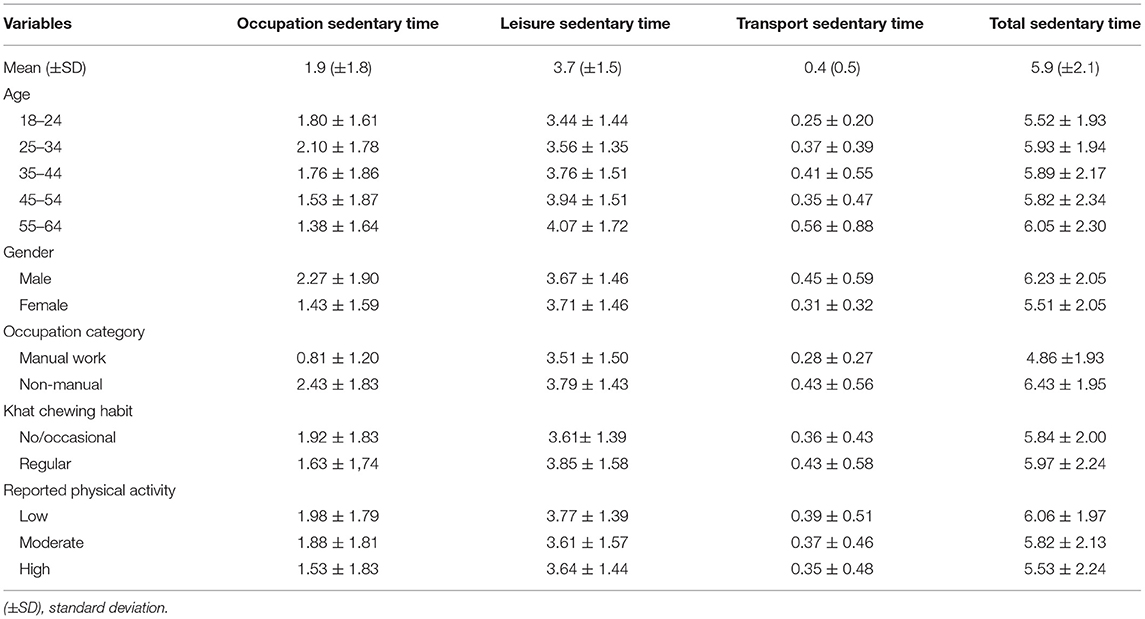
Table 3. The mean (±SD) sedentary behavior by specific domain in hours per day among the study participant's characteristics in Eastern Ethiopia, 2019.
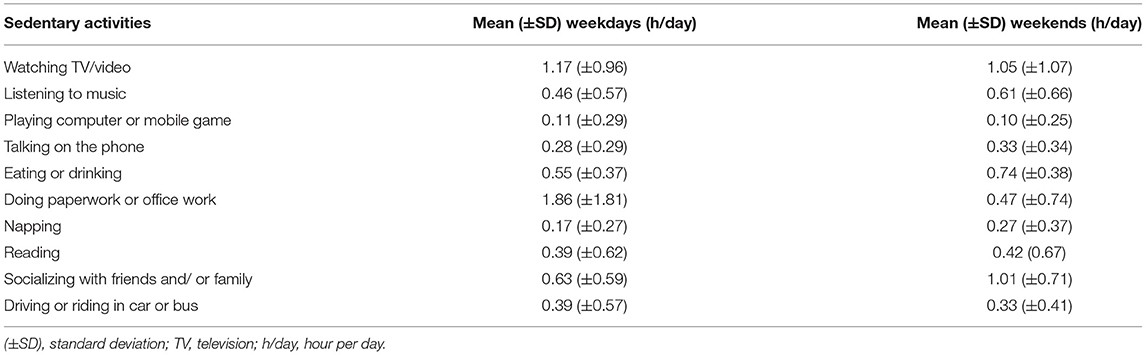
Table 4. Self-report sedentary time by doing different activities among study participants in Eastern Ethiopia, 2019.
Prevalence of High Sedentary Behavior
The prevalence of high sedentary behavior was 20.3% (95% CI: 18.0, 22.7) among study participants. The prevalence of high sedentary behavior was higher among males (23.8%) compared with females, (16.6%) (Table 5). Based on the cut-off value 75th percentile, the prevalence of high occupation sedentary behavior (≥3 h per day) was 25.6%, the prevalence of high leisure sedentary behavior (≥5.05 h per day) was 18.8%, and the prevalence of high transportation sedentary behavior (≥1 h per day) was 7.9% (Table 6).
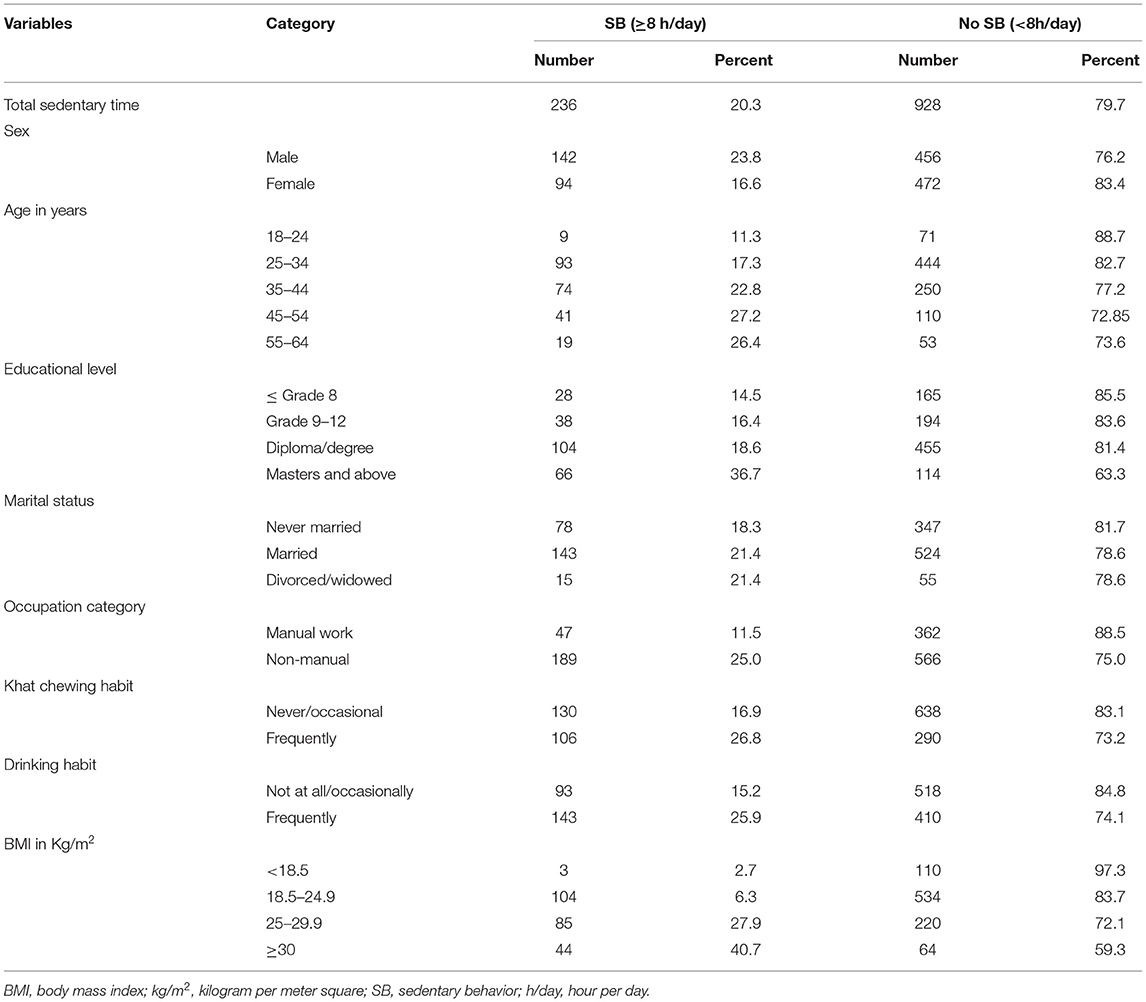
Table 5. Prevalence of high sedentary behavior by characteristics of study participants in Eastern Ethiopia, 2019 (n = 1,164).
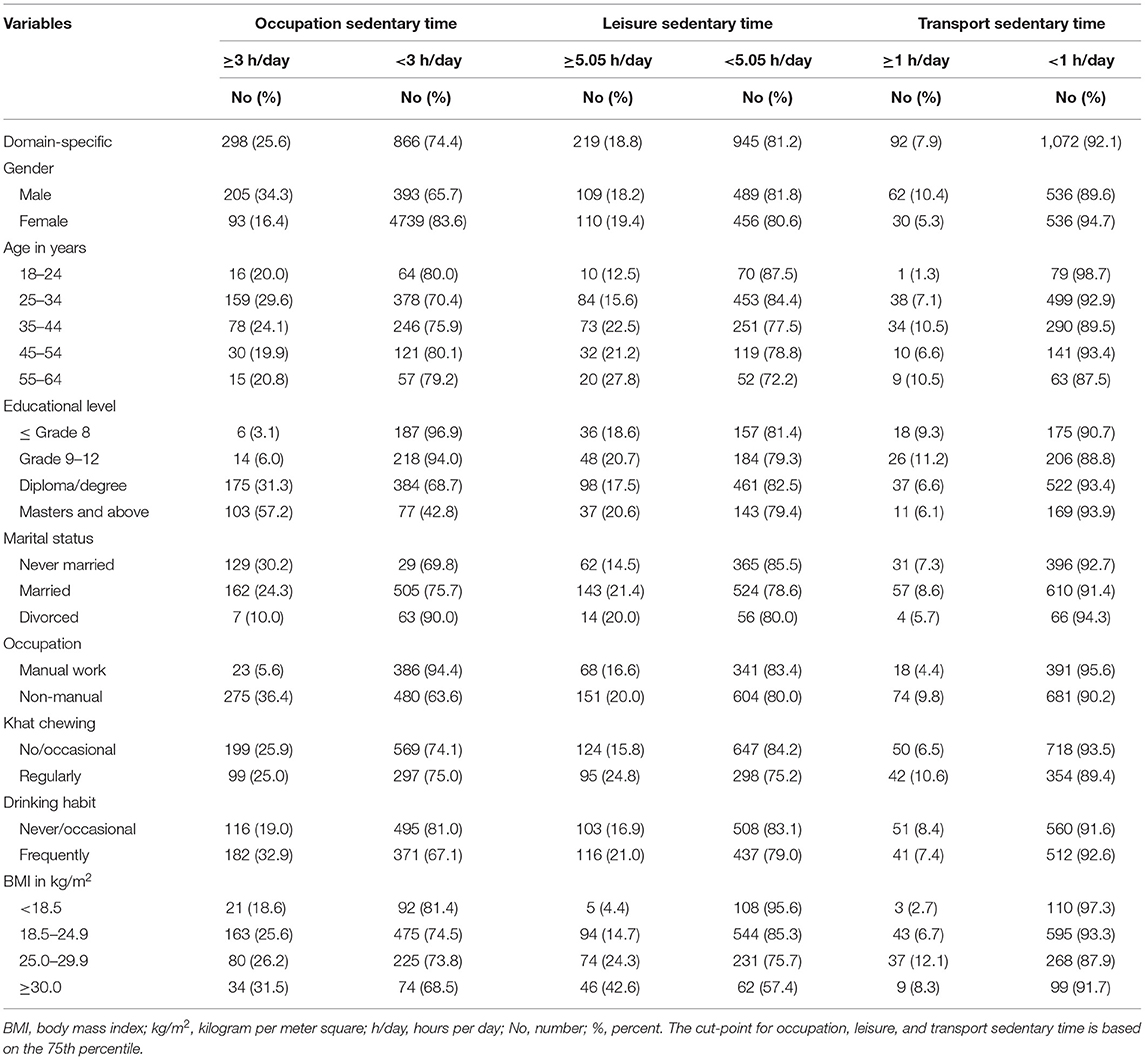
Table 6. Selected characteristics of participants by specific domain occupation, leisure, and transport sedentary time among working adults in Eastern Ethiopia, 2019.
Factors Associated With High Sedentary Behaviors Among Study Participants
The prevalence of high sedentary behavior was higher among the age group of 45–54 years (APR: 2.00; 95% CI = 1.01–3.97) and 55 and above years (APR: 2.16; 95% CI = 1.03–4.57) as compared with the age group 18–24 years. The prevalence of high sedentary behavior was higher among being a non-manual worker compared with manual workers (APR: 2.11; 95% CI = 1.46–3.05). The prevalence of high sedentary behavior was higher among individuals who frequently use/chew khat compared with those who never or occasionally chew khat (APR: 1.57; 95% CI = 1.22–2.01); among individuals who regularly drink alcohol compared with never or occasional drinkers (APR:1.39; 95% CI = 1.11–1.76); and among individuals who had a BMI 25 kg/m2 or above compared with those who had a BMI <25 kg/m2 (APR: 1.93; 95% CI = 1.53–2.44) (Table 7).
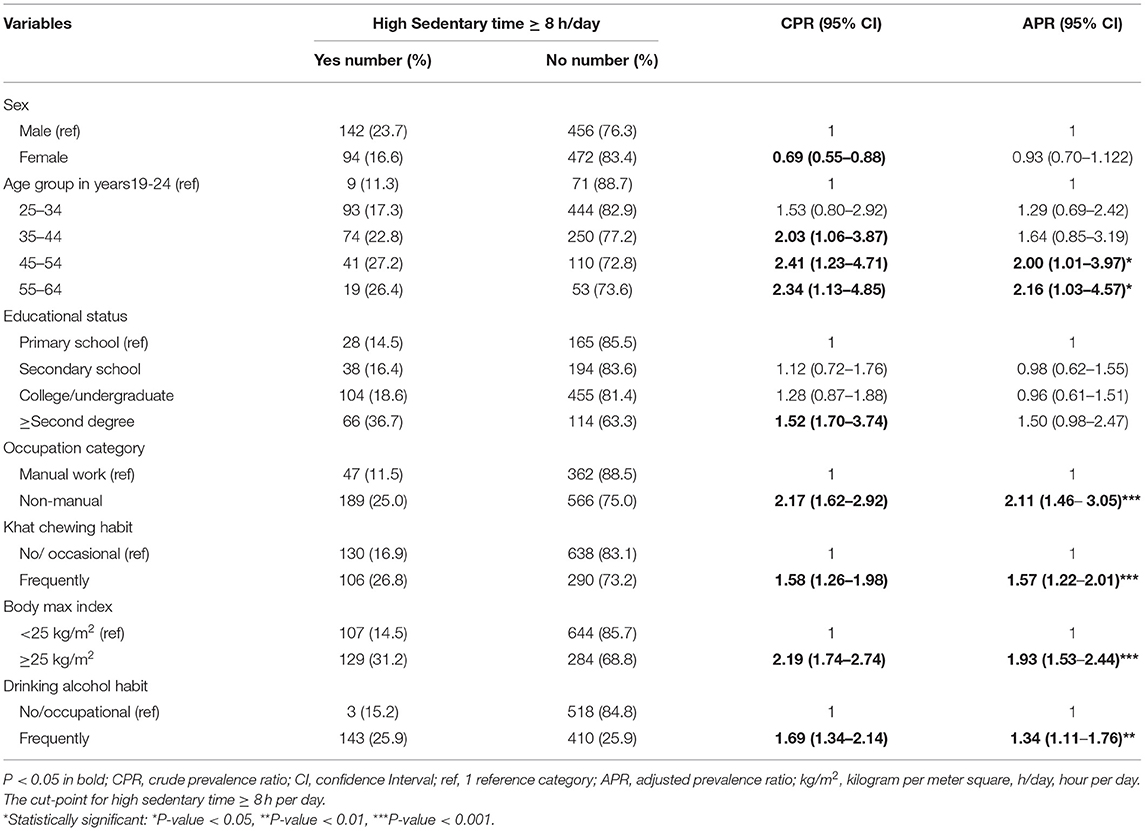
Table 7. Factors associated with high sedentary behavior among study participants in Eastern Ethiopia, 2019.
Discussion
The study found that about one-fifth of the working adults reported high sedentary behavior. The overall reported mean sedentary behavior time was 5.9 h/day. A large portion of the high sedentary behavior was due to leisure activities. High sedentary behavior was higher among persons in the older age group, in those involved in non-manual work, among frequent khat users, and regular alcohol drinkers, and in those with high body mass index.
The prevalence of high sedentary behavior observed in this study was within the range reported from low-and middle-income countries (25, 35). Our study showed that the mean (±SD) sedentary behavior was 5.9 (±2.1) hours per day, despite 51% of the study participants meeting WHO physical activity recommendations. The mean sedentary behavior is comparable with previous reports among university employees in low-and middle-income countries (14, 15, 36), and urban civil-servants (37). Our findings show that high sedentary behavior is prevalent in working adults in low-income countries. This might be due to labor-saving technology which is increasing the amount of high sedentary behavior. It might also be speculated that being employed increases levels of social connectedness, which may lead to high sedentary behavior and less opportunities for leisure time physical activity. Another consideration is that typical jobs in lower and middle income countries often involves non-manual labor, thus resulting in less physical activity and high sedentary behavior.
The fact that sedentary behavior occurred more often in leisure time than at work, which is consistent with previous studies (12, 14). This might be due to the increased TV viewing, computer use, video games, and social media engagements which has become more common these days (38). In addition, working and educated adults are more privileged to have access to technological advances (39). Our data were in agreement with research conducted in Western countries (35), demonstrating that working adults were more likely to be highly sedentary in China and Ghana. In urban centers of low-and-middle income countries, a more Western lifestyle may be evident, such as the use of more motorized transport, less labor-demanding jobs, and physically undemanding, mostly screen-based leisure, which may account for the higher sedentary levels in working adults in these settings.
Sedentary behavior was higher among the older age in line with the previous literature in low-and-middle income countries (25, 27). Moreover, evidence also showed that as age progresses physical activity and mobility decrease due to either loss of energy or disorders/illness that compromise physical fitness such as arthritis and musculoskeletal pain (40, 41).
Our finding related to higher sedentary behavior among those engaged in non-manual work is related to the nature of their work that requires prolonged sitting (42). Non-manual works these days involve using a computer that potentially requires minimal or no physical activity (43). In such occupations, sedentary behavior may not affect productivity (44, 45).
Our study shows that sedentary behavior was associated with frequent consumption of alcohol and khat. Similar findings were reported previously (46, 47). The use of alcohol and especially Khat involves prolonged sitting. Khat chewing/consumption in eastern Ethiopia is ceremonial and lasts up to 6 h at a time. Frequent attendance to such Khat chewing ceremony increases the time spent in sedentary status (48).
High body mass index was significantly associated with a high prevalence of sedentary behavior in line with previous studies in sub-Saharan Africa (49). The consistency with past studies confirms that the hypothesis of individuals with high BMI may go into a vicious cycle whereby a decrease in mobility reduces body energy expenditure leading to weight gain and then weight gain reduces mobility and leads to the adoption of sedentarism (50).
Although dichotomous analyses of sedentary behavior are regarded as more informative (51), there is no consensus on a single cut-off for sedentary behavior; thus we used a cut-off point from recent publications (6, 26, 52). Thus comparing our findings must be done cautiously as researchers use different cut-off points and diverse sedentary behavior assessment tools (53). The use of different tools can significantly influence the results; a self-reported domain-specific sedentary behavior questionnaires give substantially higher sedentary time estimates than using single-item sedentary time questions.
Limitation and Strengths
The main limitation of this study includes reliance on self-reporting, which is less accurate than sedentary behavior assessed using devices available for this purpose (54). Self-report is likely to be affected by recall bias and social desirability bias that potentially underestimates sedentary behavior. Furthermore, the study did not consider ecological variables such as psychosocial factors, organizational/community, environmental, and policy factors related to sedentary behavior due to resource constraints. Lastly, this study may not be generalizable to all working adults in eastern Ethiopia as the study population was drawn only from one institution. However, the strengths of this study include a large sample size and the use of standardized data collection tools. Moreover, this study was the first of its kind among university employees in Ethiopia and can be fairly generalized for this category of workers in areas where there are contextual working adults.
Conclusions
About one-fifth of Ethiopia university workers reported high sedentary behavior, and leisure sedentary time was the predominant domain. Factors associated with high sedentary behavior among Ethiopia university workers were older age, being a non-manual worker, regular alcohol drinker, frequent khat-chewer, and overweight/obesity. Further study is needed by using device measurement and a representative population to check the reputability of self-report sedentary behavior and to reduce the source of errors and bias.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
The studies involving human participants were reviewed and approved by Haramaya University, College of Health and Medical Sciences Institutional Health Research Ethics Review Committee (IHRERC). The patients/participants provided their written informed consent to participate in this study.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data, took part in drafting the article or revising it critically for important intellectual content, gave final approval of the version to be published, agreed to be accountable for all aspects of the work, read, and approved the final manuscript.
Funding
This study was supported by Haramaya University (Grant # HURG-2017-02-02-05) only for data collection purpose. The university has no role on deciding the study design, data collection, analysis and interpretation, and manuscript writing and publication. Addis Continental Institute of Public Health provided technical assistance.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
The authors would like to thank Haramaya University study participants, data collectors, and Addis Continental Institute of Public Health (ACIPH) for their cooperation, support, and participation in our study.
Abbreviations
BMI, body Mass Index; MET, metabolic equivalent of task; SB, sedentary behavior; SBQ, sedentary behavior questioner; SD, standard deviation; WHO, World Health Organization; NCDs, non-communicable diseases.
References
1. Tremblay MS, Aubert S, Barnes JD, Saunders TJ, Carson V, Latimer-Cheung AE, et al. Sedentary behavior research network (SBRN)–terminology consensus project process and outcome. Int J Behav Nutr Phys Act. (2017) 14:75. doi: 10.1186/s12966-017-0525-8
2. Mohammed OY, Tesfahun E, Mohammed A. Magnitude of sedentary behavior and associated factors among secondary school adolescents in Debre Berhan town, Ethiopia. BMC Public Health. (2020) 20:86. doi: 10.1186/s12889-020-8187-x
3. Albawardi NM, Jradi H, Almalki AA, Al-Hazzaa HM. Level of sedentary behavior and its associated factors among Saudi women working in office-based jobs in Saudi Arabia. Int J Environ Res Public Health. (2017) 14:659. doi: 10.3390/ijerph14060659
4. Rawlings G, Williams R, Clarke D, English C, Fitzsimons C, Holloway I, et al. Exploring adults' experiences of sedentary behaviour and participation in non-workplace interventions designed to reduce sedentary behaviour: a thematic synthesis of qualitative studies. BMC Public Health. (2019) 19:1099. doi: 10.1186/s12889-019-7365-1
5. WHO. Sedentary Lifestyle: A Global Public Health Problem. Geneva: World Health Organization (2002).
6. Bakker EA, Hopman MT, Lee D-c, Verbeek AL, Thijssen DH, Eijsvogels TM. Correlates of total and domain-specific Sedentary behavior: a cross-sectional study in Dutch adults. BMC Public Health. (2020) 20:220. doi: 10.1186/s12889-020-8316-6
7. McAlister KL, Rubin DA, Fisher KL. A Cross-sectional examination of patterns of sedentary behavior and cardiometabolic risk in community-dwelling adults aged 55 years and older. J Aging Res. (2020) 2020:1–9. doi: 10.1155/2020/3859472
8. Elmberg Sjöholm M, Eriksson G, Bii A, Asungu J, von Koch L, Guidetti S. Living with consequences of stroke and risk factors for unhealthy diet- experiences among stroke survivors and caregivers in Nairobi, Kenya. BMC Public Health. (2021) 21:511. doi: 10.1186/s12889-021-10522-4
9. Rosenkranz SK, Mailey EL, Umansky E, Rosenkranz RR, Ablah E. Workplace sedentary behavior and productivity: a cross-sectional study. Int J Environ Res Public Health. (2020) 17:6535. doi: 10.3390/ijerph17186535
10. Bennie JA, Pedisic Z, Timperio A, Crawford D, Dunstan D, Bauman A, et al. Total and domain-specific sitting time among employees in desk-based work settings in Australia. Aust N Z J Public Health. (2015) 39:237–42. doi: 10.1111/1753-6405.12293
11. George ES, Kolt GS, Rosenkranz RR, Guagliano JM. Physical activity and sedentary time male perceptions in a University work environment. Am J Men's Health. (2013) 2013:1557988313497217. doi: 10.1177/1557988313497217
12. Faghy MA, Duncan M, Pringle A, Buchanan Meharry J, Roscoe C. UK University Staff experience high levels of sedentary behaviour during work and leisure time. Int J Occup Saf Ergon. (2021) 2021:1–21. doi: 10.1080/10803548.2021.1874704
13. Huysmans MA, Srinivasan D, Mathiassen SE. Consistency of sedentary behavior patterns among office workers with long-term access to sit-stand workstations. Ann Work Exposures Health. (2019) 63:583–91. doi: 10.1093/annweh/wxz022
14. Fountaine CJ, Piacentini M, Liguori GA. Occupational sitting and physical activity among university employees. Int J Exerc Sci. (2014) 7:295.
15. Headley S, Hutchinson J, Wooley S, Dempsey K, Phan K, Spicer G, et al. Subjective and objective assessment of sedentary behavior among college employees. BMC Public Health. (2018) 18:768. doi: 10.1186/s12889-018-5630-3
16. Takanori H, Chen S, Yonemoto K, Kishimoto H, Chen T, Narazaki K, et al. Sedentary bout durations and metabolic syndrome among working adults: a prospective cohort study. BMC Public Health. (2016) 16:888. doi: 10.1186/s12889-016-3570-3
17. Keenan M, Greer AE. Sedentary behavior and related factors among full-time, university faculty. Int J Workplace Health Manag. (2015) 8:206–13. doi: 10.1108/IJWHM-09-2014-0034
18. Hanna F, Daas RN, Elshareif TJ, Almarridi HHFH, Al-Rojoub ZMdB, Adegboye D. The relationship between sedentary lifestyle, back pain and psychosocial correlates among university employees. Front Public Health. (2019) 7:80. doi: 10.3389/fpubh.2019.00080
19. Chau JY, Grunseit AC, Chey T, Stamatakis E, Brown WJ, Matthews CE, et al. Daily sitting time and all-cause mortality: a meta-analysis. PLoS ONE. (2013) 8:e80000. doi: 10.1371/journal.pone.0080000
20. Mclaughlin M, Atkin A, Starr L, Hall A, Wolfenden L, Sutherland R, et al. Worldwide surveillance of self-reported sitting time: a scoping review. Int J Behav Nutr Phys Act. (2020) 17:1–12. doi: 10.1186/s12966-020-01008-4
21. Keown MK, Skeaff CM, Perry TL, Haszard JJ, Peddie MC. Device-measured sedentary behavior patterns in office-based university employees. J Occup Environ Med. (2018) 60:1150–7. doi: 10.1097/JOM.0000000000001467
22. Jogunola OO, Awoyemi A. Prevalence of sedentary lifestyle among bankers in Ilorin metropolis. Niger J Med Rehabil. (2012) 15:44–50.
23. WHO. WHO STEPS Instrument (core and expanded). The WHO STEPwise Approach to Noncommunicable Disease Risk Factor Surveillance (STEPS). Geneva: The World Health Organization (2016).
24. Rosenberg DE, Norman GJ, Wagner N, Patrick K, Calfas KJ, Sallis JF. Reliability and validity of the Sedentary Behavior Questionnaire (SBQ) for adults. J Phys Act Health. (2010) 7:697–705. doi: 10.1123/jpah.7.6.697
25. Tcymbal A, Andreasyan D, Whiting S, Mikkelsen B, Rakovac I, Breda J. Prevalence of physical inactivity and sedentary behavior among adults in Armenia. Front Public Health. (2020) 8:157. doi: 10.3389/fpubh.2020.00157
26. Pengpid S, Peltzer K. Correlates of sedentary behavior among university students with depression from 22 low-and middle-income countries. J Hum Behav Soc Environ. (2019) 29:833–9. doi: 10.1080/10911359.2019.1610134
27. Vancampfort D, Stubbs B, Mugisha J, Firth J, Schuch FB, Koyanagi A. Correlates of sedentary behavior in 2,375 people with depression from 6 low-and middle-income countries. J Affect Disord. (2018) 234:97–104. doi: 10.1016/j.jad.2018.02.088
28. Stubbs B, Vancampfort D, Firth J, Schuch FB, Hallgren M, Smith L, et al. Relationship between sedentary behavior and depression: A mediation analysis of influential factors across the lifespan among 42,469 people in low-and middle-income countries. J Affect Disord. (2018) 229:231–8. doi: 10.1016/j.jad.2017.12.104
29. Ekelund U, Steene-Johannessen J, Brown WJ, Fagerland MW, Owen N, Powell KE, et al. Does physical activity attenuate, or even eliminate, the detrimental association of sitting time with mortality? A harmonised meta-analysis of data from more than 1 million men and women. Lancet. (2016) 388:1302–10. doi: 10.1016/S0140-6736(16)30370-1
30. Peltzer K P-MN, Pengpid S. Correlates of sedentary behaviour among adolescents and adults with hazardous, harmful or dependent drinking in South Africa. S Afr J Psychiat. (2019) 25:1–6. doi: 10.4102/sajpsychiatry.v25i0.1217
31. Fosu AK. Growth, inequality and poverty in Sub-Saharan Africa: recent progress in a global context. Oxf Dev Stud. (2015) 43:44–59. doi: 10.1080/13600818.2014.964195
33. Motuma A, Gobena T, Roba KT, Berhane Y, Worku A. Metabolic syndrome among working adults in Eastern Ethiopia. Diabetes Metab Syndr Obes. (2020) 13:4941–51. doi: 10.2147/DMSO.S283270
34. Zhu C, Blizzard L, Stankovich J, Wills K, Hosmer D. Be wary of using Poisson regression to estimate risk and relative risk. Biostat Biomet Open Access J. (2018) 4:1–3. doi: 10.19080/BBOAJ.2018.04.555649
35. Koyanagi A, Stubbs B, Vancampfort D. Correlates of sedentary behavior in the general population: a cross-sectional study using nationally representative data from six low-and middle-income countries. PLoS ONE. (2018) 13:e0202222. doi: 10.1371/journal.pone.0202222
36. Wooley SE, Dempsey K, Matthews TD, Laguilles R, Hutchinson J, Rowe DA, et al. Occupational sitting and physical activity among college employees: 227 Board# 48 May 31 11: 00 AM-12: 30 PM. Med Sci Sports Exer. (2017) 49:42. doi: 10.1249/01.mss.0000516937.72055.e2
37. Baye MY. Sedentary behaviour among urban civil servants in Eastern Part of Southern Nations, Nationalities and Peoples' Region, Ethiopia. BioMed Res Int. (2021) 2021:1–13. doi: 10.1155/2021/8847107
38. Clark B, Sugiyama T. Prevalence, Trends, and Correlates of Sedentary Behavior. Physical Activity, Exercise, Sedentary Behavior and Health. Springer (2015). p. 79–90.
39. Muthuri SK, Wachira L-JM, Leblanc AG, Francis CE, Sampson M, Onywera VO, et al. Temporal trends and correlates of physical activity, sedentary behaviour, and physical fitness among school-aged children in Sub-Saharan Africa: a systematic review. Int J Environ Res Public Health. (2014) 11:3327–59. doi: 10.3390/ijerph110303327
40. Vancampfort D, Stubbs B, Koyanagi A. Physical chronic conditions, multimorbidity and sedentary behavior amongst middle-aged and older adults in six low-and middle-income countries. Int J Behav Nutr Phys Act. (2017) 14:147. doi: 10.1186/s12966-017-0602-z
41. Kim Y, Lee E. The association between elderly people's sedentary behaviors and their health-related quality of life: focusing on comparing the young-old and the old-old. Health Qual Life Outcomes. (2019) 17:131. doi: 10.1186/s12955-019-1191-0
42. Wahlström V, Olsson D, Öhberg F, Olsson T, Slunga Järvholm L. Underlying factors explaining physical behaviors among office workers—an exploratory analysis. Int J Environ Res Public Health. (2020) 17:9158. doi: 10.3390/ijerph17249158
43. Duncan MJ, Rashid M, Vandelanotte C, Cutumisu N, Plotnikoff RC. Development and reliability testing of a self-report instrument to measure the office layout as a correlate of occupational sitting. Int J Behav Nutr Phys Act. (2013) 10:16. doi: 10.1186/1479-5868-10-16
44. Clemes SA, O'connell SE, Edwardson CL. Office workers' objectively measured sedentary behavior and physical activity during and outside working hours. J Occup Environ Med. (2014) 56:298–303. doi: 10.1097/JOM.0000000000000101
45. Carter SE, Draijer R, Thompson A, Thijssen DH, Hopkins ND. Relationship between sedentary behavior and physical activity at work and cognition and mood. J Phys Act Health. (2020) 17:1140–52. doi: 10.1123/jpah.2019-0632
46. Müller AM, Chen B, Wang NX, Whitton C, Direito A, Petrunoff N, et al. Correlates of sedentary behaviour in Asian adults: a systematic review. Obes Rev. (2020) 21:e12976. doi: 10.1111/obr.12976
47. West AB, Bittel KM, Russell MA, Evans MB, Mama SK, Conroy DE. A systematic review of physical activity, sedentary behavior, and substance use in adolescents and emerging adults. Transl Behav Med. (2020) 10:1155–67. doi: 10.1093/tbm/ibaa008
48. Haile D, Lakew Y. Khat chewing practice and associated factors among adults in Ethiopia: further analysis using the 2011 demographic and health survey. PLoS ONE. (2015) 10:e0130460. doi: 10.1371/journal.pone.0130460
49. Gichu M, Asiki G, Juma P, Kibachio J, Kyobutungi C, Ogola E. Prevalence and predictors of physical inactivity levels among Kenyan adults (18–69 years): an analysis of STEPS survey 2015. BMC Public Health. (2018) 18:1217. doi: 10.1186/s12889-018-6059-4
50. Middelbeek L, Breda J. Obesity and sedentarism: reviewing the current situation within the WHO European Region. Curr Obes Rep. (2013) 2:42–9. doi: 10.1007/s13679-013-0054-y
51. Mullane SL, Toledo MJ, Rydell SA, Feltes LH, Vuong B, Crespo NC, et al. Social ecological correlates of workplace sedentary behavior. Int J Behav NutrPhys Act. (2017) 14:117. doi: 10.1186/s12966-017-0576-x
52. Uijtdewilligen L, Yin JD-C, van der Ploeg HP, Müller-Riemenschneider F. Correlates of occupational, leisure and total sitting time in working adults: results from the Singapore multi-ethnic cohort. Int J Behav Nutr Phys Act. (2017) 14:169. doi: 10.1186/s12966-017-0626-4
53. Owen N. The emerging public-health science of sedentary time: what is the relevance to low and middle income countries? Revista Brasileira de Atividade Física Saúde. (2013) 17:457–60. doi: 10.12820/2317-1634.2012v17n6p457
Keywords: high, prevalence, sedentary behavior, working adults, Ethiopia
Citation: Motuma A, Gobena T, Roba KT, Berhane Y and Worku A (2021) Sedentary Behavior and Associated Factors Among Working Adults in Eastern Ethiopia. Front. Public Health 9:693176. doi: 10.3389/fpubh.2021.693176
Received: 10 April 2021; Accepted: 03 August 2021;
Published: 07 September 2021.
Edited by:
Daniel P. Bailey, Brunel University London, United KingdomReviewed by:
Siti Munira Yasin, MARA University of Technology, MalaysiaRudy Foddis, University of Pisa, Italy
Copyright © 2021 Motuma, Gobena, Roba, Berhane and Worku. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Aboma Motuma, YWJvbWFhYmRpMUBnbWFpbC5jb20=