
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health , 29 June 2021
Sec. Public Mental Health
Volume 9 - 2021 | https://doi.org/10.3389/fpubh.2021.691680
 Bjarne Schmalbach1†
Bjarne Schmalbach1† Ileana Schmalbach1,2†
Ileana Schmalbach1,2† Christoph Kasinger3Katja Petrowski1
Christoph Kasinger3Katja Petrowski1 Elmar Brähler3,4Markus Zenger4,5Yve Stöbel-Richter6Ernst Peter Richter2Hendrik Berth2*
Elmar Brähler3,4Markus Zenger4,5Yve Stöbel-Richter6Ernst Peter Richter2Hendrik Berth2*A substantial body of research has shown worse health conditions for East- vs. West-Germany in the wake of reunification. In the present study, we investigate how these differences between the two formerly divided regions developed and what maintains them. Specifically, we consider the associations between health status, income satisfaction, and health-related locus of control. In a quasi-experimental and longitudinal study design, we are particularly interested in the differences between individuals who stayed in East-Germany and those who were born in the East but migrated to West-Germany. To this end, we examined data from seven waves of the Saxony Longitudinal Study (2003–2009). Specifically, we tested a cross-lagged panel model with random effects, which evinced very good model fit. Most parameters and processes were equivalent between individuals who stayed in East-Germany vs. moved to West-Germany. Crucially, there was the expected pattern of positive correlations between health, income, and locus of control. In addition, we found substantially lower values for all three of these variables for the individuals who stayed in East-Germany (vs. moved to West-Germany). A possible explanation is the increase in socio-economic status that the internal migrants experienced. These findings present an important contribution of research in order to foster a better understanding on the social dynamics in Germany related to internal/domestic migrants and implications in the context of health outcomes (e.g., significantly more unemployment in East vs. West-Germany), especially since almost 20–25% of East-German citizens migrated to West-Germany. Until now, there are no similar studies to the Saxony longitudinal project, since the data collection started in 1987 and almost every year an identical panel has been surveyed; which can be particularly useful for health authorities. The study mainly focuses on social science research and deals with the phenomenon of reunification, approaching several subjects such as mental and physical health, quality of life and the evaluation of the political system. Yet even though many people have experienced such a migration process, there has been little research on the subjects we approach. With our research we deepen the understanding of the health consequences of internal migration.
The separation of Germany after the end of World War II and the subsequent existence of two German states—the German Democratic Republic (GDR; East Germany) and the Federal Republic of Germany (FRG; West Germany)—between 1949 and 1990 offers an opportunity to study the influence of factors such as socialization and social and political transformation on mental health. The distinct societies and cultures were not synchronized immediately in the course of reunification (1, 2). Instead, they assimilated over time (3, 4). With regard to citizens' health status in the formerly divided regions, many studies have shown that East-Germans were more at risk, when Germany was first reunited but assimilated over time (5–8). In this regard, there are several areas to consider, such as quality of life, psychological health, and job opportunities. However, the broad unemployment exemplifies its relevance in the German social system. In the course of German reunification, there were massive changes in the economy of East Germany. As a result, many people lost their jobs and had to reorient themselves professionally. To date, despite an economic upswing in recent years, the unemployment rates in the new federal states are about twice as high as in western Germany, which negatively affected the psychological and physical health of its citizens. For example, unemployed citizens reported significantly higher psychological stress, higher scores in depression, and lower quality of life than people who have never been unemployed. In addition, unemployment was significantly correlated with greater alcohol consumption, body weight, and somatic complaints (9–13), which on the long run significantly affect the overall health. Further studies replicated these results showing a higher psychological burden in citizens living in eastern Germany, compared to those living in West-Germany. Or to put it the other way around: People who have moved to the West were more relaxed and less stressed (14–16). What is more, it was suggested that specially the German population in East-Germany will shrink due to domestic migration to West-Germany (17).
Migration is usually associated with psychological and physical health difficulties and is mostly studied in the context of experiencing a different culture [e.g., language, food, etc.; (16)]. However, (18) reported greater depression in both, migrants from East to West-Germany as well as from West to East-Germany. Nevertheless, other studies reported greater quality of life in people who migrate from East to West-Germany (14, 15). Further, Albani et al. (19) showed a lower quality of life in citizens from West-Germany who migrate to East-Germany. On the other hand, even if the unemployment rate is still significantly higher in the east than in the west, a greater convergence can be observed after 30 years of reunification (20). For example, while the difference to the west was more than 10% points at the turn of the millennium, it was only around 2% points in 2018. This can be attributed to a positive development on the labor market and research into key technologies. Further, the development of living conditions in East and West since the fall of the Berlin Wall were no longer significantly different between the eastern and western federal states (20). Taking this background into consideration, a main questions that researchers are grappling with in this context is: Where did the differences in health between East- and West-Germany originate? And consequently, how can one explain the convergence that has been observed since reunification?
Health is a multiply determined construct (21, 22). In the present investigation, we combine psychological and socio-economic indicators to paint a complete picture as possible of the health development. First, we consider health-related locus of control (LoC). Decades of research have shown that the ability to control one's health, and—as if not more important—knowledge of and confidence in that ability are crucial determinants of health behavior and thus health in general (23). This confidence feeds on past achievements, and leads to a sense of control and a positive outlook which in turn results in more success. There is convincing evidence for the positive role of LoC—and its cousin self-efficacy (24, 25). Among others, both have been shown to be predictive of smoking cessation (26–28), nutrition, weight control (29, 30), and adherence to health programs and preventive health behaviors (31–35).
Second, we consider socio-economic status (SES) in the shape of satisfaction with one's income. Health-related outcomes are well-known to be determined by socio-economic factors and specifically the extent to which individuals have access to health care services (36, 37). Like any association, the factors influence each other. On the one hand, better health also offers better opportunities in life (38–40). For example, access to education is a positive factor and it is easier to find a well-paying job (41–44). On the other hand, a higher income is associated with better health. Through the higher income, one has better access to medical care, the possibility of an adequate nutrition and the opportunity to afford hygiene products and medical treatments (45–48). Finally, a higher income is to a substantial degree based on better education and thus a greater awareness of good health related behaviors (48–50).
Returning to the topic of questions that researchers are dealing with in the wake of reunification: A third question is inevitably intertwined with the second question mentioned above. That is, what role does the internal or domestic migration that took place following reunification (and still does to this day) play in this process? While Germany was divided as well as after the opening of the inner German border, a large number of East-Germans moved to the Western part of the country (16, 51, 52). Throughout the GDR's existence, around four million individuals fled the regime. After reunification, an average of 134 thousand East-Germans migrated to West-Germany each year, and only 89 thousand West-Germans moved to East-Germany. Over time, the gap narrowed, with comparable absolute numbers being reported from 2014 onward. Yet, when considering the smaller base population in East- vs. West-Germany, East-Germans are still much more likely to move to West-Germany than the other way around.
Based on previous research, we know that migration of all kinds is associated with stressful life events and acculturative stress (53–55). Psychosocial stress situations also arise where familiar habits are disturbed by social changes (56). In addition to the transformation experiences and reunification, changes of residence can also represent such a stressor. As mentioned above, millions of people moved from East Germany to West Germany because of the former established regime, which is a push factor. After the reunification and with the fall of the GDR, people moved for other reasons, such as better occupational opportunities and social structures, which are pull factors [e.g., (57)]. These may adversely affect the migrant's mental health and manifest themselves in somatic symptoms. At the same time, numerous studies have demonstrated a positive selection bias with regard to those who migrate for work-related reasons, known as the healthy migrant effect (58–60). In addition, it should be noted that a migration from East- to West-Germany (or vice-versa) is likely much less stressful than a “typical” migration, where an individual has to adapt to a completely different culture. Especially coupled with the fact that the migration to the West was largely perceived as an opportunity [e.g., better job and career perspectives; (14–16, 61), p. 15; (62, 63)], a positive effect of migration seems more likely (16, 64, 65).
For the study at hand, we are interested in internal/domestic migration in the wake of German reunification and how it affected individuals' health. To this end, we examined a longitudinal survey, the Saxony Longitudinal Study, which started collecting data even before the Fall of the Berlin Wall and followed its participants up until today (2020). We started our analysis in the 2003 wave, because by this point a respectable amount of internal migration had taken place, enabling reasonable statistical analyses. The last wave under consideration is 2009 because, starting here, there are gaps in the variables of interest, which until that point were collected on a yearly basis. Until now, there are no similar studies to the Saxony longitudinal project since the data collection has been going on for over 30 years; which can be particularly useful for health authorities.
We formulated the following hypotheses. We formulated the following hypotheses. (H1) First and foremost, we expect that our main outcome (health status) will be highly correlated with the two predictors (i.e., 1. income satisfaction and 2. health-related LoC).
(H2) Furthermore, in line with previous investigations (8), we assume that individuals in West-Germany (vs. East-Germany) will exhibit higher values of health status along with higher values for income satisfaction and LoC. On top of the general effects stated above, we hypothesize longitudinal dependencies in the auto-regressive latent trajectory model (66). Specifically, we expect that income satisfaction and LoC at Time x predict health at Time x+1 (H3 = cross-lagged effect). In addition, we postulate that health at Time x predicts health at Time x+1 (H4 = auto-regressive effect).
The sample at hand was collected within the scope of the Saxony Longitudinal Study (67). Beginning in 1987, a group of N = 1,407 8th graders at the time in East-German schools (Leipzig and Chemnitz—then Karl-Marx-Stadt—areas) has been assessed on a yearly basis with regard to political and health-related issues. In Wave 3 (1989), N = 587 individuals gave written consent for further participation in the study. In the seven survey waves of interest to the study at hand (2003–2009) n = 417 (71.0% of those who initially gave consent) individuals participated. However, 66 participants were missing more than half of the data points across time and were thus excluded. This resulted in a final sample of n = 351 participants. Of those, 266 remained in East-Germany throughout the time frame of analysis, whereas 85 migrated to West-Germany. Individuals that moved between 2003 and 2009 were not included in the analysis. The average age of the final sample was 30.03 (SD = 0.35) in 2003. We reported further sample details in Table 1.
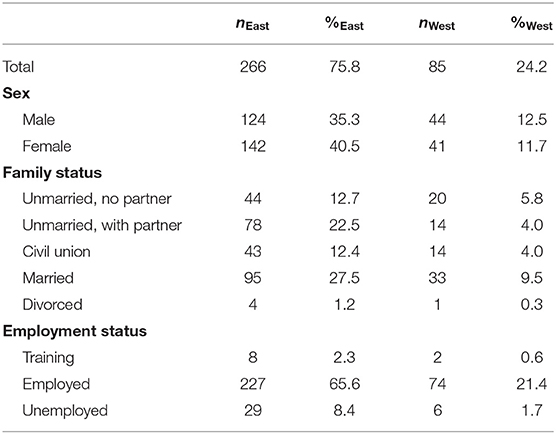
Table 1. Sociodemographic variables of the sample (in 2003).
We used the following three items to depict our main outcome variables for all seven measurement points:
Current health status was captured with the item “How would you describe your current health status?” The response options ranged from 1 (bad) to 5 (very good).
We inquired in to satisfaction with one's income among other issues. Respondents indicated their “Satisfaction with income” on a scale from 1 (unsatisfied) to 4 (satisfied).
Finally, we assessed locus of control (LoC) with the item “To what extent can you influence your own health status?” The response options ranged from 1 (not at all) to 5 (very much).
We conducted all analyses in R, using the bnstruct, ezCutoffs, ggcorrplot, ggplot2, Hmisc, and lavaan packages (68–73). Since there were still 6.3% missing data across all measurement points, we imputed missing values using k-nearest-neighbor imputation. Initially, we calculated bivariate Pearson correlations between the three variables within and between all seven measurement points. For the main analysis, we then tested an autoregressive latent trajectory model with structured residuals (66). This model allowed us to differentiate within-subject and between-subject variation. The former will be captured by the classic cross-lagged parts of the model, whereas the latter will be captured in the random intercepts and slopes. Thus, the main advantage of this model is that it accounts for change as well as for stability. We modified the model suggested by Mund and Nestler by allowing the random intercept means to vary between groups and instead constraining the intercepts of the observed variables of the first measurement point to 0 in both groups. A simplified schematic of the model is displayed in Figure 1.
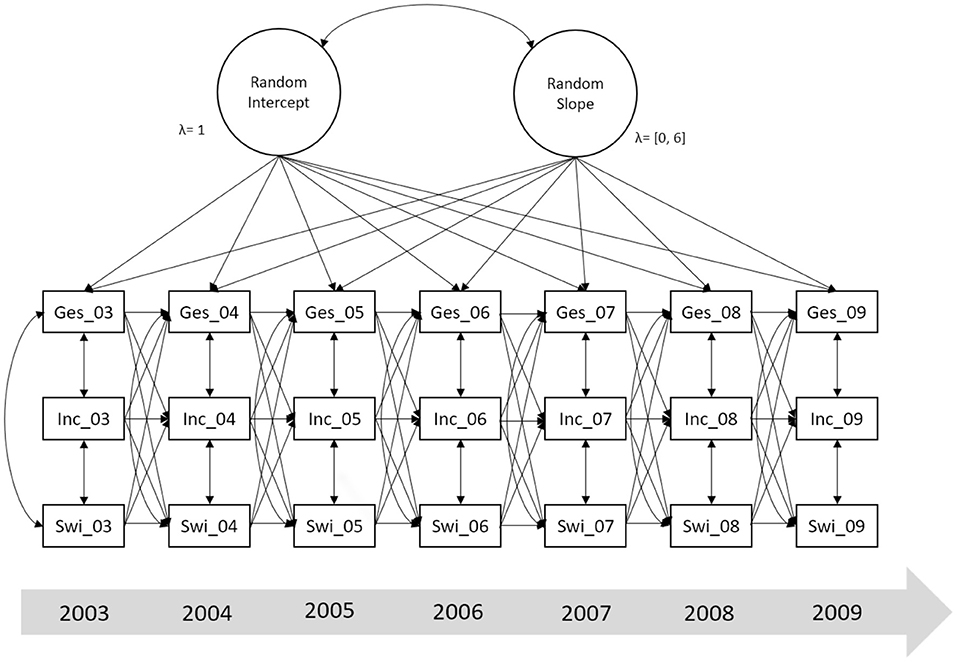
Figure 1. Simplified schematic of the autoregressive latent trajectory model of health status, income satisfaction, and locus of control. ges, subjective health status; inc, satisfaction with income; swirk, locus of control; 03–09, years. The diagram is simplified to facilitate understanding and interpretation. The actual model includes random intercepts and random slopes for all three constructs. Additionally, it includes phantom latent variables that act as go-betweens between the observed variables and the random intercepts and slopes. Furthermore, residual variances are not displayed.
We estimated the model using the robust maximum likelihood method and evaluated it based on the scaled χ2 provided by Yuan and Bentler (74). In, addition to the χ2-test, we utilized the Comparative Fit Index (CFI), the Tucker-Lewis Index (TLI), the Root Mean Squared Error of Approximation (RMSEA), and the Standardized Root Mean Squared Residual (SRMR) to evaluate model fit. Here, we utilized the robust formulas to calculate CFI, TLI, and RMSEA (75, 76). We judged these indices based on the traditionally recommended cutoff values: the p-value of the χ2-test should be >0.05 (0.01), CFI/TLI >0.97 (0.95), RMSEA smaller than 0.05 (0.08), and SRMR smaller than 0.05 (0.10), respectively, to indicate good (acceptable) fit between theoretical model and empirical data (77). To supplement these traditional fixed cutoff values, we employed the simulation-based approach introduced by Schmalbach et al. (72). In the latter approach, the empirically derived fit values are compared to the fit index distributions obtained by simulating a large number of data sets with the same underlying parameter table and overall same properties as the empirical one. We then successively introduced parameter constraints, and evaluated them using the Δχ2-test.
Because all individuals originally lived in East-Germany and remained there for a while after the start of the survey (1987), we have a quasi-experimental design. Nonetheless, we compared the baseline for the two subsamples of migrants and those who remained in East-Germany. For that purpose, we examined an earlier measurement point (Wave 10, in 1994) for the same individuals. Here, all respondents still resided in East-Germany. Unfortunately, health-related variables were only introduced in later waves of the survey, but we used a number of variables to capture the overall living conditions and thus examine whether any differences we may find later might be pre-existing. As can be seen in Table 2, there were no meaningful differences between any of the five variables. Overall, this evidence that individuals who stayed in East-Germany and those who later on moved to West-Germany were similar psychologically, at least prior to migration.

Table 2. Comparison of living conditions and life satisfactions at baseline (1994).
We reported the distributions of the three variables of interest—subjective health status, satisfaction with income, and locus of control—across all seven measurement points in Table 3 and Figure 2. Next, as a rudimentary check of the associations between the observed variables, we calculated bivariate correlations across all measurement points (see Figure 3). Auto-regressions were significant with rs of 0.40–0.50 for health and LoC, and rs of 0.60–0.70 for income. Cross-correlations and cross-lagged correlations were slightly smaller. Health status correlated 0.20–0.30 with income at the same and the subsequent measurement points, and 0.30–0.40 with LoC. In contrast, correlations between income and LoC were comparatively smaller—in the 0.10–0.20 range.
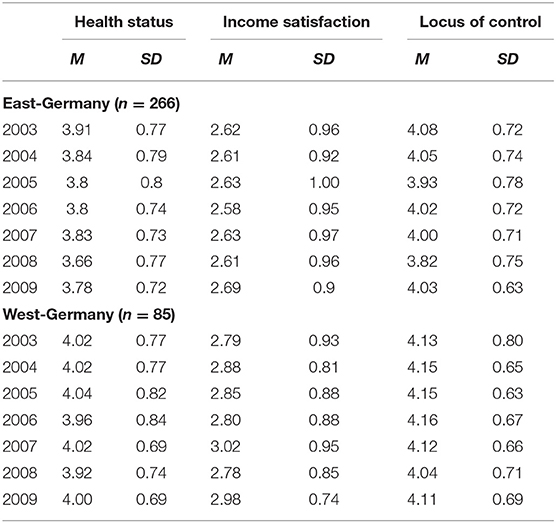
Table 3. Descriptive statistics of subjective health status, satisfaction with income, and locus of control for individuals in East- and West-Germany across time.
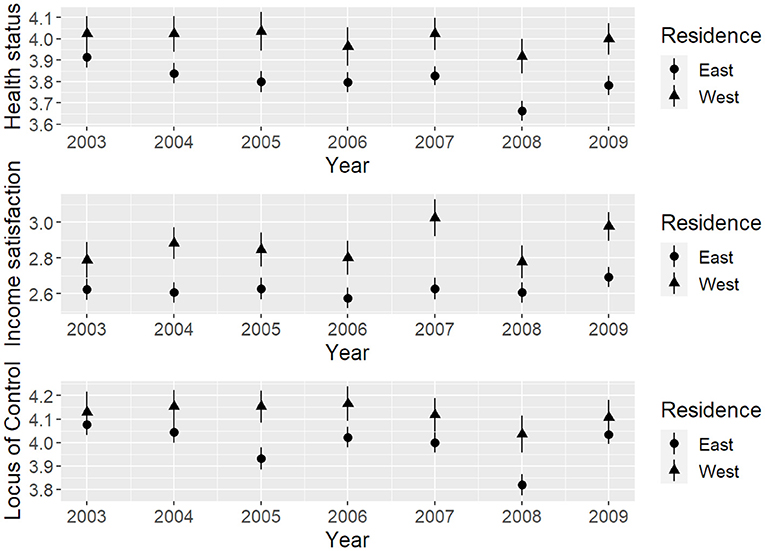
Figure 2. Observed mean scores of subjective health status, satisfaction with income, and locus of control for individuals in East- and West-Germany across time.
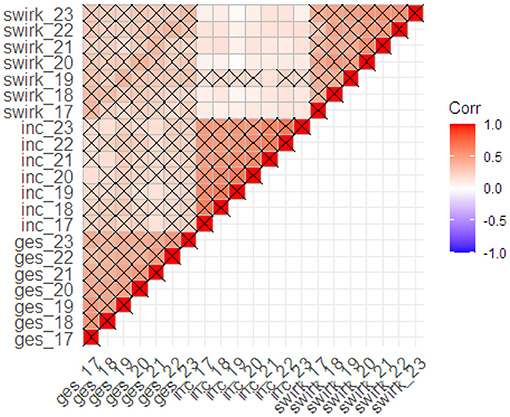
Figure 3. Observed correlations between the three dependent measures across all measurement points. ges, subjective health status; inc, satisfaction with income; swirk, locus of control; 17–23, survey wave (corresponding years: 2003–2009). Crossed cells are significant at p < 0.001.
The initial unconstrained model evinced very good fit, = 396.561, p = 0.037, CFI = 0.985, TLI = 0.982, RMSEA = 0.029, SRMR = 0.055. Goodness-of-fit was furthermore confirmed in the simulatory approach: Simulated cutoff values at α = 0.05 were χ2 = 428.533, CFI = 0.975, TLI = 0.970, RMSEA = 0.039, SRMR = 0.072. Thus, the empirical fit indices were never worse than the simulated cutoff values.
In order to compare the model between the two subsamples of individuals living in East- and West-Germany, we then introduced parameter constraints in a successive fashion. As can be seen in Table 4, the majority of parameters should be considered equal between the two groups. Only the random intercept means and time-point-specific cross-correlations differed substantially between groups. Specifically, the random intercepts for health status and income satisfaction were significantly higher for those respondents who had moved to West-Germany (see Table 5). A marginally significant effect was found for locus of control. The effect cross-correlations for the first measurement point were significantly higher for individuals in West- vs. East-Germany (see Table 6). The associated effect sizes were q = 0.282 and 0.247 for the difference in correlation coefficients between health status and income satisfaction, and health status and LoC, respectively.
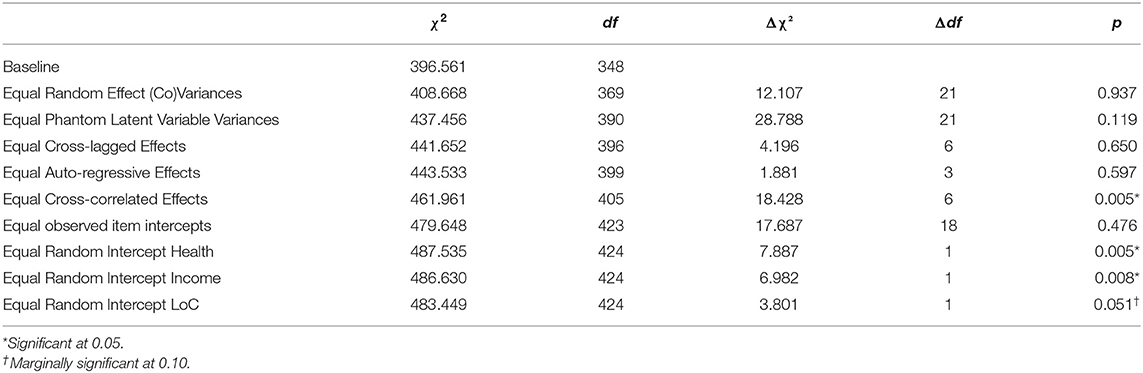
Table 4. Nested model comparisons.
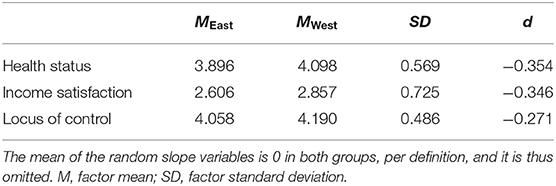
Table 5. Random intercept means.
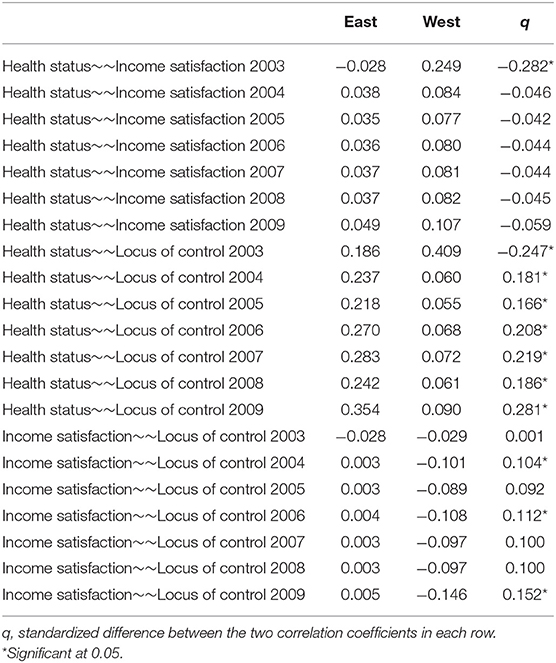
Table 6. Cross-correlation effects.
The following parameters were statistically equivalent between East and West and can thus be expected to function in comparable ways. First, the latent correlation matrix was equivalent (see Table 7): There were high correlations between the random intercept of health and income satisfaction, and health and LoC. In addition, there was a moderate correlation between income satisfaction and LoC. Furthermore, there was a significant correlation between the slopes of health status and income satisfaction. This means that as an individual's income increased so did their health and vice-versa. The same was not true for the slope of LoC.
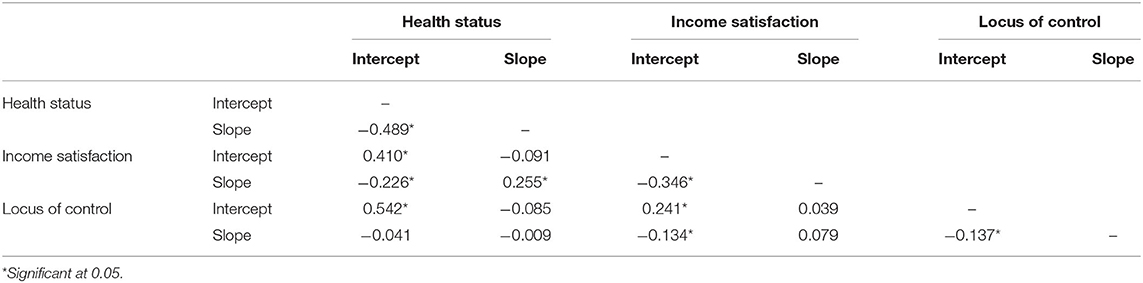
Table 7. Random intercept and slope correlations.
As can be seen in Table 8, auto-regressive and cross-lagged effects did not reach a substantial magnitude for any of the associations (β < 0.10). Only the auto-regressions of income satisfaction reached βs of 0.20 and greater. Given our sample size, none of the effects (except for the auto-regression of income satisfaction) were significant. This implies that time point-specific variation in the variables explains only about 2–3% in health status in the next measurement. It should be noted, however, that this effect is controlled for the aforementioned effects of the random intercept correlations. This means that, in general across all time points, individuals with higher income satisfaction and a more internal locus of control had a better health status.
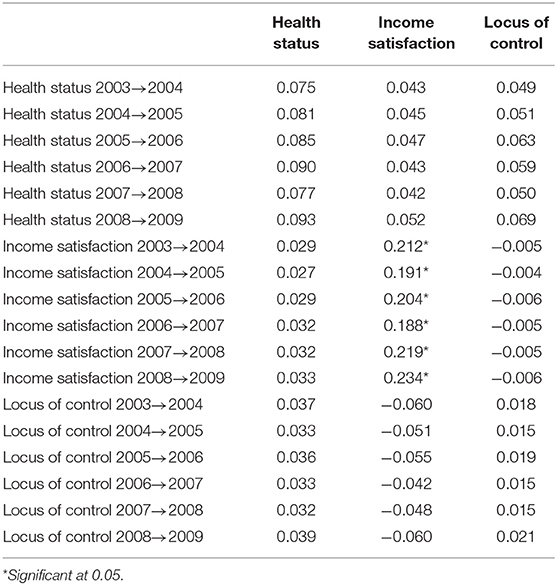
Table 8. Standardized auto-regressive and cross-lagged effects.
The aim of the present study was to investigate the health development of individuals in East- and West-Germany. Specifically, we compared a group of young adults that stayed in East-Germany vs. moved to West-Germany. First we hypothesized high correlations between (a) health and income satisfaction and (b) health and LoC. In addition, we assumed that individuals in West-Germany (vs. East-Germany) will exhibit higher values of health along with higher values for income satisfaction and LoC. Finally, we expected a cross-lagged and auto-regressive effects of the analyzed variables. For the main analysis, we tested an autoregressive latent trajectory model with structured residuals that enables to capture within-subject and between-subject variation. The model evinced very good fit, allowing us to conduct the examinations, we previously explained. As predicted, (H1) health status was strongly correlated with both, income satisfaction and LoC. These findings are in line with previous research demonstrating strong ties between health status, socio-economic status and self-regulation (23, 36, 37). Our second hypothesis (H2) was confirmed, indicating small- to moderately-sized effects in favor of the individuals that had moved to West-Germany (vs. had not moved) on all three of the variables of interest: Health, income satisfaction, health LoC. Yet, we found even larger effects in the correlations of the random intercepts, which is in line with previous analyses. Based on the overall analyses, this means that (irrespective of time) individuals with better SES and better LoC are also generally healthier. Our results emphasized that individuals with greater internal locus of control had a better health status, which corresponds with previous evidence on the subject (78–80). These studies also underlined the relevance of positive health attitudes, which tend to motivate individuals to behave in beneficial ways, rather opting for choices that promote health and at the same time reducing risks (81).
Concerning our last hypotheses (H3 and H4), our results point out a random slope of “0.” Thus, there is no general time-dependent change. Similarly, longitudinal effects (i.e., auto-regressive and cross-lagged effects) were small, and largely non-significant. The sole exception to this statement was the auto-regressive effect of income satisfaction. Finally, cross-correlative effects were also relatively small. The exceptions here are moderate correlations for health status with income satisfaction. These were also different between East- and West-German habitants. While the correlation was much larger for West-Germans at T1, it was close to zero after that, while remaining relatively constant for East-Germans. In sum this means, that the majority of systematic variance is found in general between-subject effects, namely in random intercept correlations and group differences. We observed little to no change over time. A possible explanation of these results could be that most individuals had already lived in their new residence for multiple years and were thus already habituated to the overall living conditions. Assuming equivalence prior to migration (which we showed for several central variables), this means that the East-West migrants assimilated to West-German levels of health and income rather quickly and stably. As previously reported (57), pull factors often play a decisive role in internal migration, which is also reflected in the study at hand in those people who moved from East to West (due the overall better living conditions). Additionally, the structures of the German social system that were established in Western Germany after World War II reflect a more open society, which possibly facilitated adaptation (82–84). Importantly, it should be noted that people who migrate due to occupational concerns are more likely to have positive attitudes, which reduces the stressful experience of relocation.
Overall, we suppose that the improvement in socio-economic standing is a likely cause for the difference that emerges between the two groups in our study. This assumption is based on the fact that West-Germany has had (and still has to this day) higher objective income levels than East-Germany (85). Higher income, better living conditions, and overall higher social security are known to improve health behaviors and related outcomes (36, 37, 49, 86). However, future studies are needed to confirm the interpretation of this data.
The present study suggested better health outcomes for the citizens living in West-Germany. Nevertheless, the results of the study at hand should be consider under the lens of the following limitations. First, a central limitation of the study is that we did not have information about respondents' health status prior migration to West-Germany. We approximated this variable by examining respondents' overall life satisfaction (among other variables). To ascertain our findings, future studies should aim to include pre-migration health status. Secondly, we focused exclusively on psychological indicators, which are based on the subjective perception of the respondents. Even for income, we used satisfaction with income, rather than the monetary income itself. Future research could complement our analyses by instead examining objective indicators of health and SES or combining subjective and objective variables. A further limitation represents the fact, that we investigated exclusively the migration processes from East- to West-Germany without comparing the migration processes from West-to East Germany. Future research may benefit from this comparison too.
Finally, we only analyze the changes in health status, income satisfaction, and locus of control by using one-item scales for each construct. We fully acknowledge the limited depth of the assessment that is offered by single-item measures, particularly for more complex constructs. However, in our case the criteria under investigation can easily be boiled down to a single sentence. It is very common for health status to be assessed with a singular item (87–89). Similarly, satisfaction with income (and other socio-economic variables) is very straightforward and has often been measured using short scales or even single items (90–92). For locus of control, it can be argued that this construct is more complex and should ideally be captured using multiple indicators. Overall, however, it should be noted that we did not rely on singular assessments for any of the three constructs. While we did only use one type of wording for each latent variable, each item was assessed on seven occasions leading to a highly reliable assessment for the random intercept and slope. Nevertheless, this procedure limits the validity of the results to a certain extent. It should also be noted however, that the repeated measures design (including seven timepoints) leads to a highly valid assessment when general processes across time are concerned (random intercept and slope). Even so, the findings should be replicated using more comprehensive, validated scales in the future.
In the study at hand, we examined the health development of citizens in East and West-Germany. In general, our data suggested positive outcomes in individuals that moved to East-Germany compared to those who did not in terms of health, income satisfaction, and health LoC. We concluded that the East-West migrants assimilated to West-German levels of health and income rather quickly and stably. In this context, we reasoned that the better living conditions (e.g., pull factors, better income, open society, etc.) contributed to the differences between the two studied groups. In addition, other factors might have contributed to the favorable outcomes such as positive expectations about migrating to West-Germany. In this case having a buffering effect, making the adaptation process easier.
The datasets generated during and/or analysed during the current study are not publicly available, but are available from the corresponding author on reasonable request.
Ethical review and approval was not required for the study on human participants in accordance with the local legislation and institutional requirements. The patients/participants provided their written informed consent to participate in this study.
BS: conceptualization, methodology, and writing of the main paper. IS: writing, introduction, discussion, review, and editing. KP and EB: software and validation. YS-R and HB: investigation. MZ, CK, and ER: visualization and editing. EB, KP, and HB: project administration. All authors contributed to the article and approved the submitted version.
Open Access Funding by the Publication Fund of the TU Dresden.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
1. Ekman J, Linde J. Communist nostalgia and the consolidation of democracy in Central and Eastern Europe. J Commun Stud Trans Polit. (2005) 21:354–74. doi: 10.1080/13523270500183512
2. Wagner G. Differenzierung als absoluter Begriff? Zeitschrift Soziol. (1996) 25:89–105. doi: 10.1515/zfsoz-1996-0201
3. Burda MC, Weder M. The Economics of German Unification after Twenty-five Years: Lessons for Korea. Berlin: Humboldt University (2017).
5. Atzpodien K, Bergmann E, Bertz J, Busch M, Eis D, Ellert U, et al. 20 Jahre nach dem Fall der Mauer: Wie hat sich die Gesundheit in Deutschland entwickelt? RKI: Deutschland (2009).
6. Hessel A, Geyer M, Brähler E. Somatoforme Beschwerden in der Bevölkerung Deutschlands. Zeitschrift für psychosomatische Medizin und Psychotherapie. (2002) 48:38–58. doi: 10.13109/zptm.2002.48.1.38
7. Lampert T, Müters S, Kuntz B, Dahm S, Nowossadeck E. Beschreibung der gesundheitlichen Lage in Ost und West sowie deren Entwicklung in den letzten 30 Jahren. RKI: Deutschland (2019).
8. Prütz F, Rommel A, Kroll LE, Lampert T. 25 Jahre nach dem Fall der Mauer: Regionale Unterschiede in der Gesundheit. RKI: Deutschland (2014).
9. Berth H, Förster P, Brähler E. Gesundheitsfolgen von Arbeitslosigkeit und Arbeitsplatzunsicherheit bei jungen Erwachsenen. Das Gesundheitswesen. (2003) 65:555–60. doi: 10.1055/s-2003-43026
10. Berth H, Förster P, Balck F, Brähler E, Stöbel-Richter Y. Arbeitslosigkeitserfahrungen, Arbeitsplatzunsicherheit und der Bedarf an psychosozialer Versorgung. Das Gesundheitswesen. (2008) 70:289–94. doi: 10.1055/s-2008-1065363
11. Berth H, Brähler E, Zenger M, Stöbel-Richter Y editors. Innenansichten der Transformation: 25 Jahre Sächsische Längsschnittstudie (1987-2012). Psychosozial-Verlag (2012).
12. Berth H, Förster P, Brähler E, Zimmermann A, Zenger M, Stöbel-Richter Y. Arbeitslosigkeit und körperliche Gesundheit. Ausgewählte Ergebnisse einer Längsschnittschtudie. In: Fangerau H, Kessler S, editors. Achtung und Missachtung in der Medizin. Anerekennung und Selbstkonstitution als Schlüsselkategorien zur Deutung von Krankheit und Armut. Freiburg: Alber (2013). p. 215–32.
13. Zenger M, Berth H, Brähler E, Stöbel-Richter Y. Health complaints and unemployment: The role of self-efficacy in a prospective cohort study. J Soc Clin Psychol. (2013) 32:97–115. doi: 10.1521/jscp.2013.32.1.97
14. Berth H, Förster P, Brähler E. Psychosoziale Folgen einer Migration aus den neuen in die alten Bundesländer. Ergebnisse einer Längsschnittstudie. Psychosozial. (2004) 26:81–95.
15. Berth H, Förster P, Brähler E, Stöbel-Richter Y. Go west! migration in die alten länder, ihre ursachen und folgen. In: Berth H. Förster P, Brähler E, Stöbel-Richter Y, editors. Einheitslust und Einheitsfrust. Junge Ostdeutsche auf dem Weg vom DDR- zum Bundesbürger. Eine sozialwissenschaftliche Langzeitstudie von 1987-2006. Gießen: Psychosozial-Verlag (2007). p. 177–98.
16. Berth H, Förster P, Brähler E, Zenger M, Zimmermann A, Stöbel-Richter Y. Innerdeutsche Migration und seelische Gesundheit. Ergebnisse aus der Sächsischen Längsschnittstudie. In: Brähler E, Wagner W, editor. Kein Ende mit der Wende? Perspektiven aus Ost und West. Gießen: Psychosozial-Verlag (2014). p. 89–101. doi: 10.30820/9783837969269-89
17. Destatis. Qualitätsbericht - Mikrozensus. (2013). Available online at: https://www.destatis.de/DE/Methoden/Qualitaet/Qualitaetsberichte/Bevoelkerung/mikrozensus-2013.html
18. Grulke N, Bailer H, Albani C, Blaser G, Schmutzer G, Geyer M, et al. Migration in die depression? Innerdeutsche Migr Psychische Befindlichkeit Psychosozial. (2004) 95:97–106.
19. Albani C, Blaser G, Geyer M, Bailer H, Grulke N, Schmutzer G, et al. Innerdeutsche migration und gruppenidentitäten. Psychoanalyse. (2007) 11:26–45.
20. Statista. Statistiken zu DDR. (2021). Available online at: https://de.statista.com/themen/17/ddr/#dossierSummary (accessed May 21, 2021).
21. Adler NE, Glymour MM, Fielding J. Addressing social determinants of health and health inequalities. JAMA. (2016) 316:1641–2. doi: 10.1001/jama.2016.14058
22. Hanson MD, Chen E. Socioeconomic status and health behaviors in adolescence: a review of the literature. J Behav Med. (2007) 30:263. doi: 10.1007/s10865-007-9098-3
23. Strudler Wallston B, Wallston KA. Locus of control and health: a review of the literature. Health Educ Monogr. (1978) 6:107–17. doi: 10.1177/109019817800600102
24. Bandura A. Self-efficacy. In: Ramachandran VS, editor. Encyclopedia of Human Behavior. Vol. 4. New York, NY: Academic Press (1992). p. 71–81.
25. O'Leary A. Self-efficacy and health. Behav Res Ther. (1985) 23:437–51. doi: 10.1016/0005-7967(85)90172-X
26. Kaplan GD, Cowles A. Health locus of control and health value in the prediction of smoking reduction. Health Educ Monogr. (1978) 6:129–37. doi: 10.1177/109019817800600104
27. Sheffer C, MacKillop J, McGeary J, Landes R, Carter L, Yi R, et al. Delay discounting, locus of control, and cognitive impulsiveness independently predict tobacco dependence treatment outcomes in a highly dependent, lower socioeconomic group of smokers. Am J Addict. (2012) 21:221–32. doi: 10.1111/j.1521-0391.2012.00224.x
28. Stuart K, Borland R, McMurray N. Self-efficacy, health locus of control, and smoking cessation. Addict Behav. (1994) 19:1–12. doi: 10.1016/0306-4603(94)90046-9
29. Anastasiou CA, Fappa E, Karfopoulou E, Gkza A, Yannakoulia M. Weight loss maintenance in relation to locus of control: the MedWeight study. Behav Res Ther. (2015) 71:40–4. doi: 10.1016/j.brat.2015.05.010
30. Balch P, Ross AW. Predicting success in weight reduction as a function of locus of control: a unidimensional and multidimensional approach. J Consult Clin Psychol. (1975) 43:119. doi: 10.1037/h0076495
31. Helmer SM, Krämer A, Mikolajczyk RT. Health-related locus of control and health behaviour among university students in North Rhine Westphalia, Germany. BMC Res Notes. (2012) 5:703. doi: 10.1186/1756-0500-5-703
32. Norman P, Bennett P, Smith C, Murphy S. Health locus of control and health behaviour. J Health Psychol. (1998) 3:171–80. doi: 10.1177/135910539800300202
33. Schlenk EA, Hart LK. Relationship between health locus of control, health value, and social support and compliance of persons with diabetes mellitus. Diabetes Care. (1984) 7:566–74. doi: 10.2337/diacare.7.6.566
34. Steptoe A, Wardle J. Locus of control and health behaviour revisited: a multivariate analysis of young adults from 18 countries. Br J Psychol. (2001) 92:659–72. doi: 10.1348/000712601162400
35. Wurtele SK, Britcher JC, Saslawsky DA. Relationships between locus of control, health value, and preventive health behaviors among women. J Res Pers. (1985) 19:271–8. doi: 10.1016/0092-6566(85)90018-2
36. Ivaldi E, Bonatti G, Soliani R. Objective and subjective health: an analysis of inequality for the European Union. Soc Indicat Res. (2018) 138:1279–95. doi: 10.1007/s11205-017-1686-1
37. Veenstra G. Social capital, SES and health: an individual-level analysis. Soc Sci Med. (2000) 50:619–29. doi: 10.1016/S0277-9536(99)00307-X
38. Adams RJ. Improving health outcomes with better patient understanding and education. Risk Manag. Healthc Policy. (2010) 3:61–72. doi: 10.2147/RMHP.S7500
39. Forrest CB, Bevans KB, Riley AW, Crespo R, Louis TA. Health and school outcomes during children's transition into adolescence. J Adolesc Health. (2013) 52:186–94. doi: 10.1016/j.jadohealth.2012.06.019
40. Katz DL. Life and death, knowledge and power: why knowing what matters is not what's the matter. Archiv Inter Med. (2009) 169:1362–3. doi: 10.1001/archinternmed.2009.238
41. Daley AJ, Parfitt G. Good health - is it worth it? Mood states, physical well-being, job satisfaction and absenteeism in members and non-members of a British corporate health and fitness club. J Occupat Org Psychol. (1996) 69:121–34. doi: 10.1111/j.2044-8325.1996.tb00604.x
42. Suhrcke M, de Paz Nieves C. The impact of health and health behaviours on educational outcomes in high-income countries: a review of the evidence. In: International Conference on Education, Social Capital and Health. Oslo (2010). p. 25–6.
43. Virtanen M, Kivimäki M, Elovainio M, Vahtera J. Selection from fixed term to permanent employment: prospective study on health, job satisfaction, behavioural and risks. J Epidemiol Commun Health. (2002) 56:693–9. doi: 10.1136/jech.56.9.693
44. Woolf SH, Johnson RE, Phillips RL Jr., Philipsen M. Giving everyone the health of the educated: an examination of whether social change would save more lives than medical advances. Am J Public Health. (2007) 97:679–83. doi: 10.2105/AJPH.2005.084848
45. Rosengren A, Smyth A, Rangarajan S, Ramasundarahettige C, Bangdiwala SI, AlHabib KF, et al. Socioeconomic status and risk of cardiovascular disease in 20 low-income, middle-income, and high-income countries: the Prospective Urban Rural Epidemiologic (PURE) study. Lancet Global Health. (2019) 7:e748–60. doi: 10.1016/S2214-109X(19)30045-2
46. Stringhini S, Sabia S, Shipley M, Brunner E, Nabi H, Kivimaki M, et al. Association of socioeconomic position with health behaviors and mortality. JAMA. (2010) 303:1159–66. doi: 10.1001/jama.2010.297
47. Wardle J, Waller J, Jarvis MJ. Sex differences in the association of socioeconomic status with obesity. Am J Public Health. (2002) 92:1299–304. doi: 10.2105/AJPH.92.8.1299
48. Woolf SH, Simon SM, Aron L, Zimmerman E, Dubay L, Luk KX. How Are Income and Wealth Linked to Health and Longevity? Washington: Urban Institute (2015).
49. Chesters J, Daly A. Do peer effects mediate the association between family socio-economic status and educational achievement? Austr J Soc Issues. (2017) 52:63–77. doi: 10.1002/ajs4.3
51. Destatis. Ost-West-Wanderungen [East-West migrations]. (2020). Retrieved from: https://www.destatis.de/DE/Themen/Gesellschaft-Umwelt/Bevoelkerung/Wanderungen/vorlaeufige-ergebnisse.html (accessed May 30, 2021).
52. Geißler R. Die Sozialstruktur Deutschlands. 7. Auflage. Wiesbaden: Springer-Verlag (2014). doi: 10.1007/978-3-531-19151-5
53. Kirkcaldy B, Wittig U, Furnham A, Merbach M, Siefen RG. Migration und Gesundheit. Bundesgesundheitsblatt-Gesundheitsforschung-Gesundheitsschutz. (2006) 49:873–83. doi: 10.1007/s00103-006-0021-9
54. Sangalang CC, Becerra D, Mitchell FM, Lechuga-Peña S, Lopez K, Kim I. Trauma, post-migration stress, and mental health: a comparative analysis of refugees and immigrants in the United States. J Immigr Minority Health. (2019) 21:909–19. doi: 10.1007/s10903-018-0826-2
55. Weishaar HB. Consequences of international migration: a qualitative study on stress among Polish migrant workers in Scotland. Public Health. (2008) 122:1250–6. doi: 10.1016/j.puhe.2008.03.016
56. Berry JW. Stress perspectives on acculturation. Cambridge Handbook Accultur Psychol. (2006) 1:43–56. doi: 10.1017/CBO9780511489891.007
57. Berry JW. Acculturation: living successfully in two cultures. Inter. J Inter Relat. (2005) 29:697–712. doi: 10.1016/j.ijintrel.2005.07.013
59. Lu Y, Qin L. Healthy migrant and salmon bias hypotheses: a study of health and internal migration in China. Soc Sci Med. (2014) 102:41–8. doi: 10.1016/j.socscimed.2013.11.040
60. Razum O, Zeeb H, Rohrmann S. The “healthy migrant effect”–not merely a fallacy of inaccurate denominator figures. Int J Epidemiol. (2000) 29:191–2. doi: 10.1093/ije/29.1.191
61. Friedrich K. 16 Jahre innerdeutsche Ost-West-Migration – eine Einführung in die Transformation eines geschlossenen Migrationsregimes in die Postmoderne. In: Friedrich K, Schultz A, editos. Brain drain oder brain circulation ? Konsequenzen und Perspektiven der Ost-West-Migration, Forum IFL, 8. Leipzig: Institut für Länderkunde (2008) 1–123.
62. Huinink J, Vidal S, Kley S. Individuals' openness to migrate and job mobility. Soc Sci Res. (2014) 44:1–14. doi: 10.1016/j.ssresearch.2013.10.006
63. Vidal S, Lutz K. Internal migration over young adult life courses: continuities and changes across cohorts in West Germany. Adv Life Course Res. (2018) 36:45–56. doi: 10.1016/j.alcr.2018.03.003
64. Glorius B. Go west: internal migration in Germany after reunification. Belgeo. (2010) 3:281–92. doi: 10.4000/belgeo.6470
65. Stawarz N, Sander N, Sulak H, Rosenbaum-Feldbrügge M. The turnaround in internal migration between East and West Germany over the period 1991 to 2018. Demogr Res. (2020) 43:993–1008. doi: 10.4054/DemRes.2020.43.33
66. Mund M, Nestler S. Beyond the cross-lagged panel model: next-generation statistical tools for analyzing interdependencies across the life course. Adv Life Course Res. (2019) 41:100249. doi: 10.1016/j.alcr.2018.10.002
67. Berth H, Brähler E, Zenger M, Stöbel-Richter Y. 30 Jahre ostdeutsche Transformation. In: Berth H, Brähler E, Zenger M, Stöbel-Richter Y., editors. Sozialwissenschaftliche Ergebnisse und Perspektiven der Sächsischen Längsschnittstudie. Gießen: Psychosozial-Verlag (2020), 1–357. doi: 10.30820/9783837973945
68. Franzin A, Sambo F, di Camillo B. bnstruct: an R package for Bayesian Network structure learning in the presence of missing data. Bioinformatics. (2017) 33:1250–2. doi: 10.1093/bioinformatics/btw807
69. Harrell FE Jr. Hmisc: Harrell Miscellaneous. R Package Version 4.4-1 (2020). Available online at: https://CRAN.R-project.org/package=Hmisc (accessed March 15, 2021).
70. Kassambara A. ggcorrplot: Visualization of a Correlation Matrix using “ggplot2”. R package version 0.1.3.999 (2019). Available online at: http://www.sthda.com/english/wiki/ggcorrplot (accessed March 15, 2021).
71. Rosseel Y. lavaan: an R Package for Structural Equation Modeling. J Stat Softw. (2012) 48:1–36. doi: 10.18637/jss.v048.i02
72. Schmalbach B, Irmer JP, Schultze M. ezCutoffs: Fit Measure Cutoffs in SEM. R package version 1.0.2. (2019). Available online at: https://CRAN.R-project.org/package=ezCutoffs (accessed March 15, 2021).
73. Wickham H. ggplot2: Elegant Graphics for Data Analysis. Switzerland: Springer-Verlag (2016). doi: 10.1007/978-3-319-24277-4
74. Yuan KH, Bentler PM. 5. Three likelihood-based methods for mean and covariance structure analysis with nonnormal missing data. Sociol Methodol. (2000) 30:165–200. doi: 10.1111/0081-1750.00078
75. Brosseau-Liard PE, Savalei V. Adjusting incremental fit indices for nonnormality. Multivar Behav Res. (2014) 49:460–70. doi: 10.1080/00273171.2014.933697
76. Brosseau-Liard PE, Savalei V, Li L. An investigation of the sample performance of two nonnormality corrections for RMSEA. Multivar Behav Res. (2012) 47:904–30. doi: 10.1080/00273171.2012.715252
77. Schermelleh-Engel K, Moosbrugger H, Müller H. Evaluating the fit of structural equation models: tests of significance and descriptive goodness-of-fit measures. Methods Psychol Res Online. (2003) 8:23–74.
78. Cheng C, Cheung MWL, Lo BC. Relationship of health locus of control with specific health behaviours and global health appraisal: a meta-analysis and effects of moderators. Health Psychol Rev. (2016) 10:460–77. doi: 10.1080/17437199.2016.1219672
79. Musich S, Wang SS, Slindee L, Kraemer S, Yeh CS. The impact of internal locus of control on healthcare utilization, expenditures, and health status across older adult income levels. Geriatr Nurs. (2020) 41:274–81. doi: 10.1016/j.gerinurse.2019.10.008
80. Zhang A, Jang Y. The role of internal health locus of control in relation to self-rated health in older adults. J Gerontol Soc Work. (2017) 60:68–78. doi: 10.1080/01634372.2016.1267672
81. Sarafino EP, Smith TW. Health Psychology: Biopsychosocial Interactions. New Jersey, NJ: John Wiley and Sons (2014).
82. Landis D, Albert RD. Handbook of Ethnic Conflict. Springer (2012). doi: 10.1007/978-1-4614-0448-4
83. Ghaffarian S. The acculturation of Iranian immigrants in the United States and the implications for mental health. J Soc Psychol. (1998) 138:645–54. doi: 10.1080/00224549809600419
84. Jasinskaja-Lahti I, Liebkind K, Horenczyk G, Schmitz P. The interactive nature of acculturation: perceived discrimination, acculturation attitudes and stress among young ethnic repatriates in Finland, Israel and Germany. Int J Interc Relat. (2003) 27:79–97. doi: 10.1016/S0147-1767(02)00061-5
85. Statista. Im Osten gibt es immer noch weniger Gehalt [There are still low wages in East-Germany]. (2020). Available online at: https://de.statista.com/infografik/19156/gehaltsvergleich-westdeutschland-und-ostdeutschland/ (accedded November 11, 2020).
86. Mahadea D, Rawat T. Economic growth, income and happiness: an exploratory study. South Afr J Econ. (2008) 76:276–90. doi: 10.1111/j.1813-6982.2008.00181.x
87. Ahmad F, Jhajj AK, Stewart DE, Burghardt M, Bierman AS. Single item measures of self-rated mental health: a scoping review. BMC Health Serv Res. (2014) 14:398. doi: 10.1186/1472-6963-14-398
88. Cunny KA, Perri M III. Single-item vs multiple-item measures of health-related quality of life. Psychol Rep. (1991) 69:127–30. doi: 10.2466/pr0.1991.69.1.127
89. DeSalvo KB, Jones TM, Peabody J, McDonald J, Fihn S, Fan V, et al. Health care expenditure prediction with a single item, self-rated health measure. Med Care. (2009) 47:440–7. doi: 10.1097/MLR.0b013e318190b716
90. Joshanloo M. Income satisfaction is less predictive of life satisfaction in individuals who believe their lives have meaning or purpose: a 94-nation study. Pers Individ Diff . (2018) 129:92–4. doi: 10.1016/j.paid.2018.03.018
91. Nagy MS. Using a single-item approach to measure facet job satisfaction. J Occup Organ Psychol. (2002) 75:77–86. doi: 10.1348/096317902167658
Keywords: health, migration, socio-economic status, locus of control, German reunification, German migration
Citation: Schmalbach B, Schmalbach I, Kasinger C, Petrowski K, Brähler E, Zenger M, Stöbel-Richter Y, Richter EP and Berth H (2021) Psychological and Socio-Economical Determinants of Health: The Case of Inner German Migration. Front. Public Health 9:691680. doi: 10.3389/fpubh.2021.691680
Received: 06 April 2021; Accepted: 01 June 2021;
Published: 29 June 2021.
Edited by:
Matthias Jaeger, Psychiatrie Baselland, SwitzerlandReviewed by:
Ling Wang, King's College London, United KingdomCopyright © 2021 Schmalbach, Schmalbach, Kasinger, Petrowski, Brähler, Zenger, Stöbel-Richter, Richter and Berth. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Hendrik Berth, aC5iZXJ0aEB1a2RkLmRl
†These authors share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.