 Kris Pui Kwan Ma
Kris Pui Kwan Ma Adrian Matias Bacong
Adrian Matias Bacong Simona C. Kwon3
Simona C. Kwon3 Stella S. Yi
Stella S. Yi Lan N. Ðoàn
Lan N. Ðoàn- 1Department of Family Medicine, University of Washington School of Medicine, Seattle, WA, United States
- 2Department of Community Health Sciences, Fielding School of Public Health, University of California, Los Angeles, Los Angeles, CA, United States
- 3Department of Population Health, Section for Health Equity, New York University Grossman School of Medicine, New York, NY, United States
Structural racism manifests as an historical and continued invisibility of Asian Americans, whose experiences of disparities and diverse needs are omitted in research, data, and policy. During the pandemic, this invisibility intersects with rising anti-Asian violence and other persistent structural inequities that contribute to higher COVID-19 mortality in older Asian Americans compared to non-Hispanic whites. This perspective describes how structural inequities in social determinants of health—namely immigration, language and telehealth access, and economic conditions—lead to increased COVID-19 mortality and barriers to care among older Asian Americans. Specifically, we discuss how the historically racialized immigration system has patterned older Asian immigrant subpopulations into working in frontline essential occupations with high COVID-19 exposure. The threat of “public charge” rule has also prevented Asian immigrants from receiving eligible public assistance including COVID-19 testing and vaccination programs. We highlight the language diversity among older Asian Americans and how language access remains unaddressed in clinical and non-clinical services and creates barriers to routine and COVID-19 related care, particularly in geographic regions with small Asian American populations. We discuss the economic insecurity of older Asian immigrants and how co-residence in multigenerational homes has exposed them to greater risk of coronavirus transmission. Using an intersectionality-informed approach to address structural inequities, we recommend the disaggregation of racial/ethnic data, meaningful inclusion of older Asian Americans in research and policy, and equitable investment in community and multi-sectoral partnerships to improve health and wellbeing of older Asian Americans.
Introduction
The disproportionate impact of COVID-19 among racially and ethnically diverse older adults has shed light on the persistent inequities against these marginalized populations (1). Asian Americans aged 45 years and older had higher COVID-19 attributable mortality compared to non-Hispanic whites (2), and Asian Americans had 35% more deaths in 2020 than their average for the last 5 years, the second-highest percent increase in excess deaths from COVID-19 and other causes (3). Older age and the presence of underlying chronic illnesses increases the risk of hospitalization and mortality from COVID-19 infection (4). However, age alone cannot fully explain COVID-19-related health disparities and the mortality gap, or the pre-pandemic health disadvantages, between minoritized older adults and their white counterparts (5, 6). Instead, the confluence of structural inequities amplifies the invisibility and exclusion of older Asian Americans in research and policy and contribute to the differential outcomes and unequal impact of COVID-19.
Emerging research literature has demonstrated that structural inequalities underlie COVID-19 disparities among Black and Latinx older adults (7, 8) but few have included older Asian Americans (6). Intersecting social processes and structures distinguish the older Asian American COVID-19 experience from younger Asian Americans, other minoritized populations, and by Asian American subgroup (9). We describe how structural inequities exacerbate existing vulnerabilities of older Asian Americans and make recommendations, using an intersectionality approach, to address the unequal brunt of COVID-19 on older Asian Americans communities (9).
Invisibility, Masked Heterogeneity, and Scapegoating of Asian Americans
Asian Americans are the fastest growing racial/ethnic group in the general population and older adult population aged 65 years and above in the United States (U.S.) (10, 11). Structural racism for Asian Americans manifests as historical and continued invisibility of their health and service disparities in scientific research, health data, and public policy (12, 13). Asian American narratives and needs remain ignored in decision-making, with insufficient resources to address the longstanding health disparities that have worsened during the pandemic. The invisibility of Asian Americans and continued masked heterogeneity of Asian subgroups is reinforced by the lack of standardized racial/ethnic data collection, which is a manifestation of structural inequity in public health surveillance. In practice, this means there is a paucity of health data on older Asian Americans, and data that are further disaggregated by ethnic subgroups (13, 14). Public health surveillance systems have been intentionally designed to mask disparities in health and healthcare use among Asian subgroups compared to the broader Asian American group and how health vary within each Asian subgroup (14). Without meaningful data collection of Asian American subgroups, there remains a poor evidence-base to demand action from policymakers and research priorities to address the inequitable distribution of health risks and outcomes (12).
The model minority is the stereotype that Asian Americans have achieved educational and economic success relative to other racial/ethnic minority groups and has created a false perception that Asian Americans do not need help, when in fact disaggregated data demonstrate the disproportionate COVID-19 impact on Asian Americans, with variation by Asian subgroup and demographic characteristics (15). For example, South Asians had the highest COVID-19 infection rates and Chinese Americans had the greatest mortality of all Asian groups (16). Vietnamese Americans with hypertension and who worked in high-contact industries and South Asians with diabetes and who worked in healthcare/gig economy were are increased risk of infection (17).
Asian Americans have been blamed for the pandemic (18). A survey from June 2020 reported that 31% of Asian Americans had experienced racial/ethnic slurs or jokes since the beginning of the pandemic, compared to Black (21%), Latinx (15%), and white (8%) adults (19). Between March 2020 to March 2021, Stop AAPI Hate received 6,603 anti-Asian hate incident reports (i.e., verbal harassment, shunning, physical assault), with the greatest reporting among Chinese, Korean, Filipino and Vietnamese adults, and 7% of reports were from Asians aged 60 years and older (20). We suspect the number of hate incidents are underreported due to digital access and literacy to report and general fears of reporting due to retribution and immigration status. The spike in anti-Asian discrimination negatively impacted the physical and mental health of Asian Americans and revealed the structural inequities faced by older Asian Americans (21).
Structural Inequities Faced by Older Asian Americans
The media's negative portrayal (e.g., #BoomerRemover) of older adults and discriminatory healthcare practices have reinforced ageist stereotypes that older adult lives are less valuable. The unprovoked targeting of older Asian Americans in anti-Asian hate incidents has placed them at increased risk of physical and emotional harm (22). Fear of going out to public spaces decreases social and health resources (e.g., ethnic grocery stores or seeking care) available to older adults and prevents them from leaving home for regular needs or seeking healthcare (21). The economic downturn in neighborhoods (e.g., Chinatowns) has contributed to social and linguistic isolation (23). Limited policy attention to the social determinants of health among older adults in communities of color, including Asian American communities, create barriers in access to healthcare and social services (17). The cultural norm of familial collectivism has been used to dismiss the need for culturally- and linguistically-appropriate resources for older Asian Americans and their families. The following sections describe how key determinants of health in older Asian American communities—immigration, language and telehealth access, and economic conditions—contribute to COVID-19 risk and barriers to care.
Older Asian Immigrant Workers in Frontline Industries
About 85% of older Asian Americans are foreign-born, more than any other U.S. racial/ethnic group (10), with the highest rates of foreign-born among South Asian, Vietnamese, Korean, Filipino, and Chinese older adults (Table 1). Asian immigration to the United States has historically been influenced by the demand for a constant labor supply, especially after the 1965 Immigration and Nationality Act and establishment of work visas. This has patterned certain Asian immigrant subpopulations into working in frontline essential occupations with high COVID-19 exposure or inadequate protection (25). About one in five Asian American and Pacific Islander adults aged 55 years and older work in frontline service job, compared to only 15% of the total U.S. population (26).
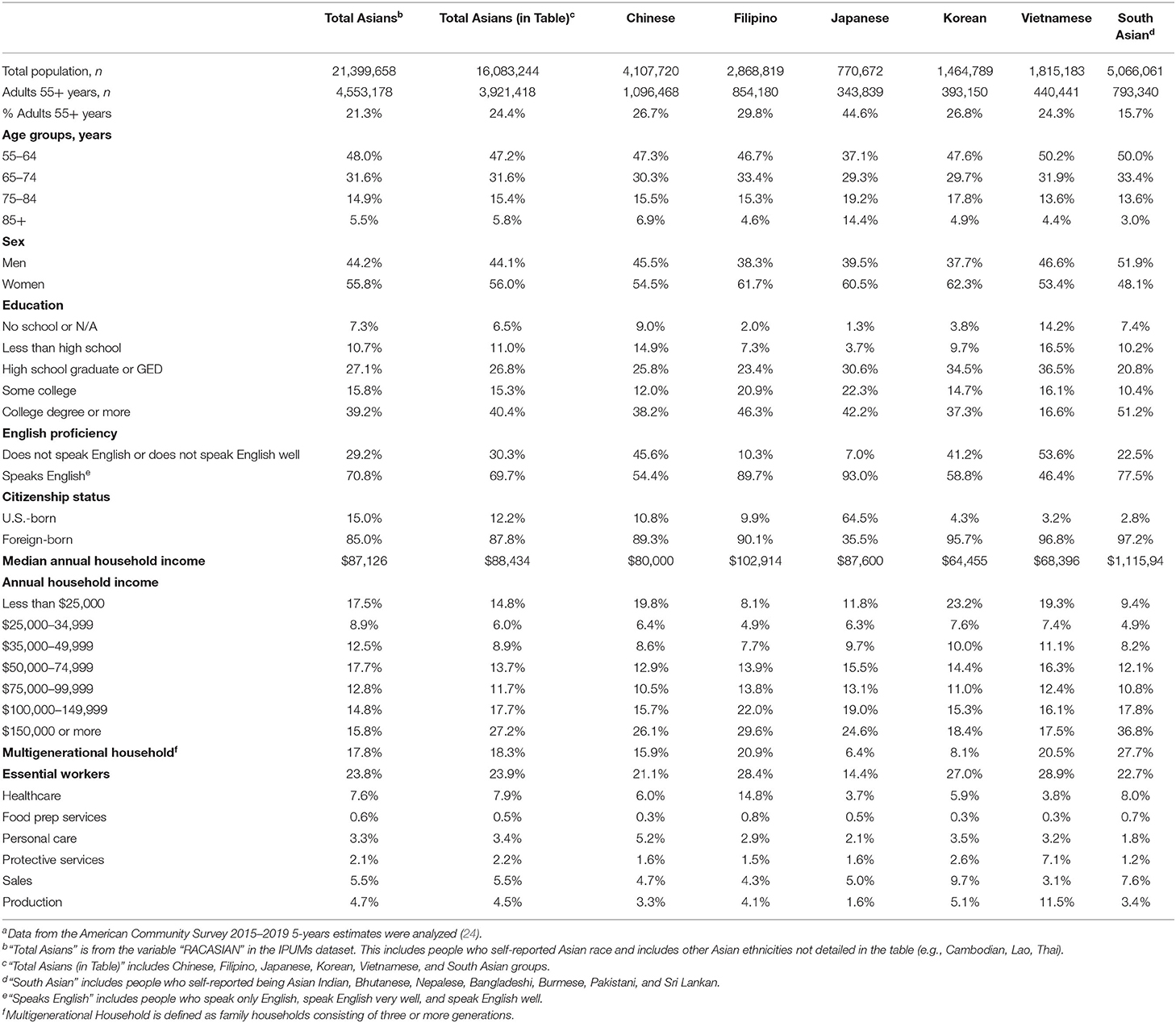
Table 1. Characteristics of Asian American adults aged 55 years and over, American Community Survey 2015–2019a.
There is an alarming rate of COVID-19 infection and deaths among Filipinx Americans (27), who have a high proportion of frontline healthcare workers (15%) relative to other Asian subgroups (Table 1). Filipinx make up 4% of the nursing workforce but comprised 31% of all COVID-19 nursing fatalities as of September 2020 (28). Many Filipinx healthcare workers were recruited to high-risk frontline positions through the establishment of U.S.-style medical schools in the Philippines during the U.S. occupation (25). Older age, high burden of comorbidities, and employment in frontline/essential industries have contributed to disproportionate COVID-19 infection and mortality in Filipinx American healthcare workers (27). Smaller Asian subgroups like Nepalese and Thai adults are also highly represented in frontline/essential industries but there is limited information the COVID-19 impact on these communities (29).
Economic Disparities Faced by Older Asian Immigrants
Contrary to the public perception of Asian Americans as the socioeconomically successful model minority, older Asian American immigrants are more likely to be poor, have fewer assets and are less likely to own a home and vehicle than older white and Hispanic/Latinx immigrants (30). Older Asian immigrants are economically worse off than their U.S.-born Asian counterparts, and the U.S.-born vs. immigrant-born wealth gap is the largest of any racial/ethnic group (30). Some reasons for this gap are that Asian American immigrants experience financial barriers and discrimination in the labor market. Older Asian immigrants are also susceptible to economic consequences (e.g., business closure) during the pandemic, and may lack generational wealth and the financial ability to bounce back from the decline (23).
Individuals with economic insecurity are at higher risk of infection and adverse consequences of COVID-19 infection, partially due to inability to socially distance because of crowded housing conditions (31). For example, about 66% of Asian older adults living in poverty resided with family, compared to 40% of non-Asian older adults in New York City (32). More than 20% of South Asian, Filipinx, and Vietnamese American older adults live in multigenerational homes (Table 1). Physical and social distancing during the pandemic is especially difficult in crowded housing conditions, where there is increased risk of intra-household transmission of coronavirus (33, 34), especially in households with high-risk older adults, frontline workers, and individuals without insurance. Although the national vaccination guidelines prioritized older adults, only a few states have flexed their plans to include prioritization for household members living with older adults to ensure adequate protection against intra-household COVID-19 transmission (35).
Threat of Public Charge as a Barrier to Eligible Public Assistance
Many immigrants, including Asian Americans, arriving in the U.S. are often of older age due to long waiting times for visas and have delayed access to public benefits like Medicare due to ineligibility based on citizenship status. The threats of being labeled as a “public charge” or becoming inadmissible for lawful permanent residence (LPR) or citizenship have hindered low-income immigrants including LPR to seek for public benefits and COVID-19 related support (36–38). Despite the recent removal of public charge criteria, fears about losing eligibility for citizenship by using public services persist. The increased xenophobic and anti-immigrant rhetoric has also prevented many permanent immigrants from utilizing public social and healthcare services, like getting COVID-19 tests or vaccination. For example, citizens and LPR were prioritized ahead of undocumented immigrants in Nebraska, despite citizenship not being a requirement for vaccination. Conflicting comments from government officials increases confusion about eligibility for COVID-19 testing and vaccination among immigrants and further strokes fears of public charge, despite the public health need to vaccinate (39).
Language and Digital Barriers to COVID-19 and Routine Care
Older Asian Americans with diverse language needs and limited digital access have difficulties seeking care in healthcare systems that have not accommodated patients with limited English proficiency (LEP) nor provided age-friendly remote services. Asian Americans include more than 40 ethnicities and 100 different languages and dialects (40). Higher percentages of LEP (not speaking English or not speaking English well) are found in Vietnamese (51%), Chinese (46%), and Korean (41%) adults aged 55 years and older, compared to the average of 29% among all Asians aged 55 and older (Table 1). Having LEP is associated with greater COVID-19 infection risk and presents barriers to accessing health services/insurance and understanding health information, especially when interpreters, culturally and linguistically matched providers, and in-language information are not available (41). Compared to their counterparts who are fluent in English, Asian Americans with LEP are more likely to not have a usual source for care, not have regular check-ups, have unmet medical needs and experience patient-provider communication problems, resulting in underutilization of healthcare services and diminished quality of care (40, 42, 43). For older Asian Americans with LEP and chronic conditions, the linguistic barriers have placed them at a disadvantage and unequal burden of morbidity and mortality.
With the rapid shift to remote and telehealth services during the pandemic, telehealth systems that do not accommodate a variety of languages and technological proficiencies are inaccessible to older Asian Americans with LEP, limited digital access and literacy. Many older Asian Americans who live in ethnic enclaves have substandard broadband Internet access due to historical place-based racism (44). They have been experiencing difficulties in obtaining accurate and timely information in their native language about COVID-19 safety precautions, testing and vaccines; locating testing or vaccination sites; scheduling physician and vaccine appointments; maintaining communication with providers; and applying for public assistance programs that support individuals impacted by the coronavirus (e.g., rental and unemployment assistance) (45). Given these barriers, fewer Asian Americans have been tested and fully vaccinated compared to non-Hispanic whites (25.6 vs. 27%) (46, 47), which potentially lead to greater COVID-19 attributable mortality in older Asian Americans (2).
Recommendations
We call for an intersectionality-informed approach to public health research, policy and decision making when addressing COVID-19 disparities, and to improve health and well-being of older Asian Americans. An intersectionality framework highlights how power and inequalities differentially impact historically marginalized groups based on their intersecting identities – identifying as an older adult and minoritized group (9).
Collect and Disaggregate Asian American Health Data
Intersectionality analysis requires race/ethnicity data to be available and disaggregated by subgroup, which is particularly important for the diverse Asian American population (48). “Asian American” and “Native Hawaiians and Other Pacific Islanders” must be collected and reported as two separate racial groups in accordance with federal guidelines (49). Detailed ethnic group data needs to be collected for Asian Americans, and if disaggregated data are not available, there should be explicit explanations to characterize the representativeness of the sample (50). More data is needed especially for Asian subgroups with smaller populations in the U.S. but with greater percentages of working or unemployed older adults (e.g., Sri Lankan, Bangladeshi, Nepalese) or rapidly growing populations in the U.S. (26). Future data collection and reporting should consider the multiple intersecting identities of Asian Americans – age, gender, socioeconomic status, disability, immigration status, sexual orientation and religion. Leveraging innovative data resources, employing both qualitative and quantitative methods, and meaningful inclusion of Asian American subgroups in research could generate more comprehensive data that capture people's lived experiences.
When reporting the disparate effects of COVID-19, older Asian Americans' experiences need to be interpreted in the context of structural inequities, with special consideration to immigration factors, language and digital access, and economic conditions. Of note, the intersecting effects in these structural inequities can look different for various Asian American subgroups. Therefore, centering research on the community from the beginning, building mutually beneficial academic-community partnerships, and engaging communities during the research process can generate findings that are most relevant to the Asian American subgroup experiences.
Meaningful Inclusion of Older Asian Americans
Intentional inclusion of older Asian Americans and other historically excluded populations in clinical research directly aligns with the National Institutes of Health policies and guidelines (51). Representation of older Asian Americans in clinical trials is necessary to end the longstanding ageist practice of conducting clinical trials with miniscule numbers of older adults and expecting to extrapolate results to be generalizable to all older adults (14). Successful methods of engagement with older Asian Americans would require linguistically- and culturally-relevant resources (i.e., bilingual researchers and materials), partnering with community-based organizations to recruit and retain participants, and using on- and offline modes of information transfer and exchange that are accessible to older Asian Americans (52, 53). In parallel, improving workforce diversity, training, and research with an intersectional lens to understanding health disparities in older adults will promote a more equitable response to advancing health for the aging population (48). Representation and equitable funding for older Asian Americans in clinical research is important because funding provides the needed resources for preliminary research, which determines funding priorities, interventions, and translating research into policy and practices that are equitable (12, 54, 55).
Investment in Community Initiatives and Uplift Cross-Sector Partnerships
Eliminating structural inequities in determinants of health will require commitment to and investment in Asian American-serving organizations, grassroot efforts, and multisectoral partnerships. Asian American-serving organizations require investments to scale up culturally- and linguistically-concordant resources, such as multilingual helpline and interactive maps, for disseminating COVID-19 vaccine information (47, 56). Training community health workers can help facilitate clinic-community linkages and assistance with clinical and social services (i.e., emergency relief benefits, food pantry programs) (57). Minimizing older adults' barriers to COVID-19 or routine care will require involving family members and bilingual community health workers in care teams, plus multi-sectoral partnerships that can provide transportation and/or internet services for in-person and telehealth visits (58).
We must reconsider the immigration pathways that are heavily linked to essential worker industries and ensure that immigrants have the appropriate occupational health and safety protections. Often times, older Asian immigrants have limited job options and have to work in low-wage, physically-demanding and high exposure industries (25). Relaxing the restrictions for the occupational industries immigrants on work visas can be employed and increasing job opportunities could better support immigrants (59). The U.S. federal government and local administrations could also increase the minimum wage and employee salaries, provide hazard pay, reduce the number of exposure hours at work, and increase paid sick leave for symptomatic or at-risk workers. Similarly, removing barriers related to eligibility for public benefits and rental/home ownership assistance programs could improve the economic security and overall well-being for older immigrant adults. Expanding the vaccine prioritization to include all members living in a multigenerational home could lower the risk of coronavirus transmission in the household (34). We also need to combat ageism at workplace and promote meaningful job opportunities that uplift the agency of older Asian Americans.
The U.S. federal government and local administrations should prioritize collaborations with community-based organizations to protect marginalized populations, including older Asian Americans adults and immigrants. Public health messaging must be clear, timely and consistent in communicating with individuals with limited English proficiency. For example, there should be explicit statements that COVID-19 vaccination and testing is available at no-cost to everyone, regardless of their citizenship status or health insurance (60). Implementing universal healthcare that cover all individuals regardless of immigration and citizenship status could relieve fears related to detention or deportation and increase the national vaccination rate (59). Federal, state, local, and philanthropic resources and funding should be equitable allocated to support multi-pronged and multi-level approaches to meet the needs of diverse older Asian Americans (12, 47, 61), and will require commitment, action and accountability to advance health equity.
Conclusion
The scenarios presented are not insurmountable but will require innovative reimagining of the public health infrastructure to address health disparities during the COVID-19 pandemic and in the future. This article focused on older Asian Americans and we acknowledge that there is overlap with the experiences of other older adults of color (7). The recommendations present immediate and long-term measures that can mitigate existing disparities and advance a health equity agenda for Asian American communities and other historically marginalized groups, including Black, Indigenous, Hispanic/Latinx, Native Hawaiian, and Pacific Islander older adults.
Data Availability Statement
Publicly available datasets were analyzed in this study. This data can be found here: Ruggles et al. (24).
Author Contributions
KM, AB, and LÐ contributed to the conceptualization, drafting and editing of the manuscript. All authors provided critical feedback and helped shape the final version of the manuscript.
Funding
This work is supported by the National Institutes of Health (NIH) National Institute on Minority Health and Health Disparities (NIMHD) Award Number U54MD000538 and the preparation of this manuscript supported in part by U.S. Department of Health & Human Services, Centers for Disease Control and Prevention (CDC) Award Numbers NU38OT2020001477, CFDA number 93.421 and 1NH23IP922639-01-00, CFDA number 93.185. Adrian M. Bacong was funded through the Eugene V. Cota-Robles Graduate Fellowship and benefited from facilities and resources provided by the California Center for Population Research at UCLA (CCPR), which receives core support (P2C-HD041022) from the Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD). Lan N. Ðoàn was supported by the NIH Resource Centers for Minority Aging Research (RCMAR) Award Number 5P30AG059302. The contents of this publication are solely the responsibility of the authors and do not necessarily represent the official views of the funders.
Author Disclaimer
The contents of this publication are solely the responsibility of the authors and do not necessarily represent the official views of the funders.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
The authors would like to extend gratitude to Drs. Kari Stephens and Anna Ratzliff for their support of this publication.
References
1. Webb Hooper M, Nápoles AM, Pérez-Stable EJ. COVID-19 and racial/ethnic disparities. JAMA. (2020) 323:2466. doi: 10.1001/jama.2020.8598
2. Chu JN, Tsoh JY, Ong E, Ponce NA. The hidden colors of coronavirus: the burden of attributable COVID-19 deaths. J Gen Intern Med. (2021) 36:1463–1465. doi: 10.1007/s11606-020-06497-4
3. Flagg A, Sharma D, Fenn L, Stobbe M. COVID-19's Toll on People of Color Is Worse Than We Knew. The Marshall Project. (2020). Available online at: https://www.themarshallproject.org/2020/08/21/covid-19-s-toll-on-people-of-color-is-worse-than-we-knew (accessed March 28, 2021).
4. Centers for Disease Control and Prevention. COVID-19 Mortality Overview - Provisional Death Counts for COVID-19. Washington, DC: Centers for Disease Control and Prevention (2021). Available online at: https://www.cdc.gov/nchs/covid19/mortality-overview.htm (accessed March 24, 2021).
5. Calderón-Larrañaga A, Dekhtyar S, Vetrano DL, Bellander T, Fratiglioni L. COVID-19: risk accumulation among biologically and socially vulnerable older populations. Ageing Res Rev. (2020) 63:1–5. doi: 10.1016/j.arr.2020.101149
6. Guerrero LR, Wallace SP. The impact of COVID-19 on diverse older adults and health equity in the United States. Front Public Health. (2021) 9:1–9. doi: 10.3389/fpubh.2021.661592
7. Chatters LM, Taylor HO, Taylor RJ. Older Black Americans during COVID-19: race and age double jeopardy. Health Educ Behav. (2020) 47:855–60. doi: 10.1177/1090198120965513
8. Garcia M, Homan P, García C, Brown T. The color of COVID-19: structural racism and the pandemic's disproportionate impact on older Black and Latinx adults. J Gerontol Series B Psychol Sci Soc Sci. (2020) 76:e75–e80. doi: 10.1093/geronb/gbaa114
9. Bowleg L. We're not all in this together: on COVID-19, intersectionality, and structural inequality. Am J Public Health. (2020) 110:917. doi: 10.2105/AJPH.2020.305766
10. Blacher K. Asian Americans and Pacific Islanders in the United States Aged 65 Years and Older: Population, Nativity, and Language. National Asian Pacific Center on Aging (2013). Available online at: https://www.napca.org/wp-content/uploads/2017/10/65-population-report-FINAL.pdf (accessed March 28, 2021).
11. Lopez G, Ruiz NG, Patten E. Key Facts About Asian Americans, a Diverse and Growing Population. Pew Research Center (2017). Available online at: https://www.pewresearch.org/fact-tank/2017/09/08/key-facts-about-asian-americans/ (accessed March 28, 2021).
12. Ðoàn LN, Takata Y, Sakuma K-LK, Irvin VL. Trends in clinical research including Asian American, Native Hawaiian, and Pacific Islander participants funded by the US National Institutes of Health, 1992 to 2018. JAMA Netw Open. (2019) 2:e197432. doi: 10.1001/jamanetworkopen.2019.7432
13. Dong X. Achieving health equity in Asian populations. Gerontol Geriatr Med. (2018) 4:1–4. doi: 10.1177/2333721418778169
14. Holland AT, Palaniappan LP. Problems with the collection and interpretation of Asian-American health data: omission, aggregation, and extrapolation. Ann Epidemiol. (2012) 22:397–405. doi: 10.1016/j.annepidem.2012.04.001
15. Gee GC, Ro A, Shariff-Marco S, Chae D. Racial discrimination and health among Asian Americans: evidence, assessment, and directions for future research. Epidemiol Rev. (2009) 31:130–51. doi: 10.1093/epirev/mxp009
16. Marcello RK, Dolle J, Tariq A, Kaur S, Wong L, Curcio J, et al. Disaggregating Asian race reveals COVID-19 disparities among Asian Americans at New York City's public hospital system. medRxiv [Preprint]. (2020). doi: 10.1101/2020.11.23.20233155
17. Chin M, Ðoàn LN, Chong SK, Wong JA, Kwon SC, Yi SS. Asian American Subgroups and the COVID-19 Experience: What We Know and Still Don't Know. Health Affairs Blog (2021). Available online at: https://www.healthaffairs.org/do/10.1377/hblog20210519.651079/full/ (accessed May 27, 2021)
18. Hswen Y, Xu X, Hing A, Hawkins JB, Brownstein JS, Gee GC. Association of “#covid19” versus “#chinesevirus” with anti-Asian sentiments on Twitter: March 9–23, 2020. Am J Public Health. (2021) 111:956–64. doi: 10.2105/AJPH.2021.306154
19. Ruiz NG, Horowitz JM, Tamir C. Many Black, Asian Americans Say They Have Experienced Discrimination Amid Coronavirus. Pew Research Center's Social & Demographic Trends Project (2020). Available online at: https://www.pewresearch.org/social-trends/2020/07/01/many-black-and-asian-americans-say-they-have-experienced-discrimination-amid-the-covid-19-outbreak/ (accessed May 22, 2021).
20. Jeung R, Horse AY, Popovic T, Lim R. 2020–2021 National Report. Stop AAPI Hate (2021). Available online at: https://stopaapihate.org/reports/ (accessed March 24, 2021).
21. Chen JA, Zhang E, Liu CH. Potential impact of COVID-19–related racial discrimination on the health of Asian Americans. Am J Public Health. (2020) 110:1624–7. doi: 10.2105/AJPH.2020.305858
22. Turton N. Stop AAPI Hate: New Data on Anti-Asian Hate Incidents Against Elderly and Total National Incidents in 2020. Stop AAPI Hate (2021). Available online at: https://stopaapihate.org/pressreleases/ (accessed March 24, 2021).
23. Ong P, Comandom A, DiRago N, Harper L. COVID-19 Impacts on Minority Businesses and Systemic Inequality. Los Angeles, CA: UCLA Center for Neighborhood Knowledge, Ong & Associates. (2020).
24. Ruggles S, Flood S, Foster S, Goeken R, Pacas J, Schouweiler M, et al. IPUMS USA: Version 11.0 [dataset]. Minneapolis, MN: IPUMS (2021).
25. Nazareno J, Yoshioka E, Adia AC, Restar A, Operario D, Choy CC. From imperialism to inpatient care: work differences of Filipino and White registered nurses in the United States and implications for COVID-19 through an intersectional lens. Gender Work Org. (2021) 28:1426–46. doi: 10.1111/gwao.12657
26. Lee EJ, Blacher K. Asian American and Pacific Islander Older Workers: Employment Trends. National Asian Pacific Center on Aging (2013). Available online at: https://www.napca.org/wp-content/uploads/2017/10/older-worker-data-FINAL.pdf (accessed March 28, 2021).
27. Escobedo LA, Morey BN, Ponce NA. Lost on the Frontline, and Lost in the Data: COVID-19 Deaths Among Filipinx Healthcare Workers in the United States. Rochester, NY: Social Science Research Network (2021).
28. National Nurses United. Sins of Omission: How Government Failures to Track COVID-19 Data Have Led to More Than 1,700 Health Care Worker Deaths and Jeopardize Public Health. (2020). Available online at: https://www.nationalnursesunited.org/sites/default/files/nnu/graphics/documents/0920_Covid19_SinsOfOmission_Data_Report.pdf (Accessed May 27, 2021).
29. Edlagan C, Kopparam R. Disaggregated Data on Asian Americans, Native Hawaiians, and Pacific Islanders Is Crucial Amid the Coronavirus Pandemic. Washington Center for Equitable Growth (2020). Available online at: http://www.equitablegrowth.org/disaggregated-data-on-asian-americans-native-hawaiians-and-pacific-islanders-is-crucial-amid-the-coronavirus-pandemic/ (accessed May 22, 2021).
30. Nam Y. Immigration and economic conditions among older Asian Americans. Race Soc Probl. (2014) 6:15–24. doi: 10.1007/s12552-014-9118-1
31. Cavalhieri KE. Economic insecurity as a risk factor during the COVID-19 pandemic. J Health Disparities Res Pract. (2021) 14:79–93. doi: 10.20944/preprints202012.0599.v2
32. Asian American Federation. Hidden in Plain Sight: Asian Poverty in New York City. New York, NY (2018). Available online at: https://www.aafederation.org/doc/AAF_poverty_2018.pdf (accessed May 27, 2021).
33. Aparicio Fenoll A, Grossbard S. Intergenerational residence patterns and Covid-19 fatalities in the EU and the US. Econ Hum Biol. (2020) 39:100934. doi: 10.1016/j.ehb.2020.100934
34. Harris JE. Los Angeles county SARS-CoV-2 epidemic: critical role of multi-generational intra-household transmission. J Bioecon. (2021) 23:55–83. doi: 10.1007/s10818-021-09310-2
35. Simpson A, Ferris S, Johnston T, Rebala P. One Home, Many Generations: States Addressing COVID Risk Among Families. The Center for Public Integrity (2021). Available online at: https://publicintegrity.org/health/coronavirus-and-inequality/one-home-many-generations-covid-risk-families/ (accessed April 1, 2021).
36. Bacong AM, Menjívar C. Recasting the immigrant health paradox through intersections of legal status and race. J Immigrant Minority Health. (2021). doi: 10.1007/s10903-021-01162-2. [Epub ahead of print].
37. Morales JF. Aging and undocumented: the sociology of aging meets immigration status. Sociol Compass. (2021) 15:e12859. doi: 10.1111/soc4.12859
38. U.S. Citizenship and Immigration Services. Public Charge. (2021). Available online at: https://www.uscis.gov/green-card/green-card-processes-and-procedures/public-charge (accessed April 1, 2021).
39. Burbach C. US Citizenship Not a Requirement for COVID Vaccine in Nebraska. Omaha Word Herald (2021). Available online at: https://omaha.com/news/state-and-regional/us-citizenship-not-a-requirement-for-covid-vaccine-in-nebraska/article_4da1d138-4fac-11eb-89a9-c3052b2306d2.html (accessed May 27, 2021).
40. Jang Y, Kim MT. Limited English proficiency and health service use in Asian Americans. J Immigr Minor Health. (2019) 21:264–70. doi: 10.1007/s10903-018-0763-0
41. Rozenfeld Y, Beam J, Maier H, Haggerson W, Boudreau K, Carlson J, et al. A model of disparities: risk factors associated with COVID-19 infection. Int J Equity Health. (2020) 19:1–10. doi: 10.1186/s12939-020-01242-z
42. Jang Y, Yoon H, Kim MT, Park NS, Chiriboga DA. Preference for patient–provider ethnic concordance in Asian Americans. Ethn Health. (2018) 26:448–59. doi: 10.1080/13557858.2018.1514457
43. Clough J, Lee S, Chae DH. Barriers to health care among Asian immigrants in the United States: a traditional review. J Health Care Poor Underserved. (2013) 24:384–403. doi: 10.1353/hpu.2013.0019
44. Hong E. Digital inequality and racialized place in the 21st century: a case study of San Francisco's Chinatown. First Monday. (2016) 21. doi: 10.5210/fm.v21i1.6196
45. della Cava M. Asian Americans in San Francisco are dying at alarming rates from COVID-19: racism is to blame. USA TODAY. (2020). Available online at: https://www.usatoday.com/in-depth/news/nation/2020/10/18/coronavirus-asian-americans-racism-death-rates-san-francisco/5799617002/ (accessed March 28, 2021).
46. Centers for Disease Control and Prevention. Demographic Trends of People Receiving COVID-19 Vaccinations in the United States. Washington, DC: Centers for Disease Control and Prevention (2020). Available online at: https://covid.cdc.gov/covid-data-tracker (accessed May 22, 2021).
47. Quach T, Ð*oàn LN, Liou J, Ponce NA. A rapid assessment of the impact of COVID-19 on Asian Americans: cross-sectional survey study. JMIR Public Health Surveil. (2021) 7:e23976. doi: 10.2196/23976
48. Poteat T. Navigating the storm: how to apply intersectionality to public health in times of crisis. Am J Public Health. (2020) 111:91–92. doi: 10.2105/AJPH.2020.305944
49. Office of Management and Budget. Revisions to the standards for the classification of federal data on race and ethnicity. Federal Reg. (1997) 62:58781–90.
50. Yi SS. Taking action to improve Asian American health. Am J Public Health. (2020) 110:435–7. doi: 10.2105/AJPH.2020.305596
51. National Institutes of Health. Revision: NIH Policy and Guidelines on the Inclusion of Individuals Across the Lifespan as Participants in Research Involving Human Subjects. National Institutes of Health (2017). Available online at: https://grants.nih.gov/grants/guide/notice-files/NOT-OD-18-116.html (accessed March 28, 2021).
52. Ma KPK, Saw A. An international systematic review of dementia caregiving interventions for Chinese families. Int J Geriatr Psychiatry. (2020) 35:1263–84. doi: 10.1002/gps.5400
53. Saw A, Stewart SL, Cummins SE, Kohatsu ND, Tong EK. Outreach to California Medicaid smokers for Asian language quitline services. Am J Prevent Med. (2018) 55:S196–S204. doi: 10.1016/j.amepre.2018.08.008
54. Borno HT, Zhang S, Gomez S. COVID-19 disparities: an urgent call for race reporting and representation in clinical research. Contemp Clin Trials Commun. (2020) 19:100630. doi: 10.1016/j.conctc.2020.100630
55. Dong X. Advancing Asian health equity: multimodal approach to translate research into practice and policy. J Am Geriatr Soc. (2019) 67:S476–8. doi: 10.1111/jgs.16110
56. National Asian Pacific Center on Aging. NAPCA Launches a National COVID-19 Vaccine Resource Map and In-Language Support to Book Vaccination Appointments. National Asian Pacific Center on Aging (2021). Available online at: https://napca.org/news/press-releases/napca-launches-a-national-covid-19-vaccine-resource-map-and-in-language-support-to-book-vaccination-appointments/ (accessed May 22, 2021).
57. Peretz PJ, Islam N, Matiz LA. Community health workers and Covid-19 — addressing social determinants of health in times of crisis and beyond. New Engl J Med. (2020) 383:e108. doi: 10.1056/NEJMp2022641
58. National Asian Pacific Center on Aging. Lyft and National Asian Pacific Center on Aging (NAPCA) Partner to Help Provide Access to Free or Discounted Rides to Vaccine Appointments. National Asian Pacific Center on Aging (2021). Available online at: https://www.napca.org/news/press-releases/lyft-and-national-asian-pacific-center-on-aging-napca-partner-to-help-provide-access-to-free-or-discounted-rides-to-vaccine-appointments/ (accessed May 22, 2021).
59. Hill J, Rodriguez DX, McDaniel PN. Immigration status as a health care barrier in the USA during COVID-19. J Migr Health. (2021) 4:100036. doi: 10.1016/j.jmh.2021.100036
60. Hussain M, Qureshi S, Suryanarayanan S, Sridaran L, Howard R. Unequal Consequences - The Disparate Impact of COVID-19 Across South Asian American Communities. South Asian Americans Leading Together (SAALT) (2020). Available online at: https://saalt.org/wp-content/uploads/2020/09/Unequal-Consequences_SAALT-2020.pdf (accessed May 22, 2021).
61. Karthick RS, Do M, Shao S, Patricia E, Hadi B, Kan LM. State of Philanthropy Among Asian Americans and Pacific Islanders: Findings and Recommendations to Strengthen Visibility and Impact. Riverside, CA: AAPI Data (2020). Available online at: https://aapip.org/sites/default/files/publication/files/2020_state_of_aapi_philanthropy_report.pdf (accessed March 28, 2021).
Keywords: COVID-19, Asian Americans, racism, intersectionality, aging, older adults
Citation: Ma KPK, Bacong AM, Kwon SC, Yi SS and Ðoàn LN (2021) The Impact of Structural Inequities on Older Asian Americans During COVID-19. Front. Public Health 9:690014. doi: 10.3389/fpubh.2021.690014
Received: 01 April 2021; Accepted: 21 July 2021;
Published: 16 August 2021.
Edited by:
Emily Joy Nicklett, University of Texas at San Antonio, United StatesReviewed by:
Ahmad Khanijahani, Duquesne University, United StatesArnab Mukherjea, California State University, East Bay, United States
Copyright © 2021 Ma, Bacong, Kwon, Yi and Ðoàn. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Kris Pui Kwan Ma, a3Jpc21hQHV3LmVkdQ==