 Rajesh Melaram
Rajesh Melaram
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
MINI REVIEW article
Front. Public Health , 24 June 2021
Sec. Environmental Health and Exposome
Volume 9 - 2021 | https://doi.org/10.3389/fpubh.2021.683719
Liver disease is a global health issue, resulting in about two million deaths per year. It encompasses a wide spectrum of varied or unknown etiologies, ranging from lifestyle choices to pre-existing comorbidities. In recent decades, exposure to environmental toxins and subsequent liver health outcomes have captured public interest, due to the extensive application of pesticides, consumption of aflatoxin contaminated foodstuff, and cyanobacterial harmful algae blooms in endemic regions of liver disease. Hepatocellular carcinoma is a serious and debilitating condition of the liver, characterized by abdominal pain and unexplained weight loss. Established risk factors for hepatocellular carcinoma include alcohol consumption, cigarette smoking, and viral infections of hepatitis B and C. However, mounting evidence suggests that environmental toxins may represent an important contributing factor in hepatocellular carcinoma development. This mini-review synthesizes epidemiological investigations, providing evidence for environmental toxins as one potential risk factor for liver disease.
Liver disease is a global health problem causing approximately two million deaths annually, owing to cirrhosis, hepatocellular carcinoma, and viral hepatitis. One million liver disease deaths occur from cirrhosis complications, while another million results from viral hepatitis and hepatocellular carcinoma (1). Despite strides in antiviral and vaccine developments, liver disease represents a significant burden to society and continues to worsen as life expectancy grows with sedentary lifestyles and overnutrition (2). The largest burden of liver disease rests in Europe, with cirrhosis and liver cancer increasing throughout most European countries. Liver disease epidemiology varies across Europe due to the prevalence of modifiable risk factors, including heavy alcohol consumption, obesity, and viral hepatitis (3). In the United States of America (USA), chronic liver disease and cirrhosis are responsible for >44,000 deaths each year, regardless of underestimates in liver deaths (4). Alcohol-related liver disease, chronic hepatitis B virus, hepatitis C virus, and non-alcoholic fatty liver disease are common etiologies of chronic liver disease and cirrhosis (5). Global estimates on chronic liver disease and cirrhosis indicate non-alcoholic fatty liver disease (60%) as the most common etiology, followed by hepatitis B virus (29%), hepatitis C virus (9%), and alcoholic-related liver disease (2%) (6). Moreover, China, a developing country where >20% of population is affected by countless liver diseases, is experiencing an upsurge in liver disease burden (2). Important causes of liver morbidity and mortality in China include alcohol-related liver disease, drug-induced liver injury, hepatitis B and C virus infections, liver cancer, liver cirrhosis, and non-alcoholic fatty liver disease. Although heavy alcohol consumption, viral hepatitis, and non-alcoholic liver disease are major risk factors for liver disease worldwide (7), recent evidence indicates that environmental toxins (organochlorine pesticides, aflatoxins, microcystins) contribute to liver disease.
Pesticides, chemicals used to manage and treat pests, have been linked to human cancers (8). The agricultural and horticultural industries widely employ pesticides, and human exposure primarily occurs via diet (9, 10). Some factors prevent degradation among household pesticides, such as lack of moisture, microorganisms, and sunlight (10, 11), which may facilitate human exposure through dermal contact and ingestion (12). Experimental studies have demonstrated that organochlorine exposure, specifically dichlorodiphenyltrichloroethane (DDT) and dichlorodiphenyldichloroethylene (DDE), results in liver tumors and hepatocellular carcinoma development in rodents (9, 13–15). Yet, epidemiological studies examining pesticide exposure and human hepatocellular carcinoma have produced mixed results, particularly in the USA. For example, one study determined that farmers were at an increased risk for HCC compared to non-farmers (16), while three other studies indicated a non-significant increased risk for HCC among farmers (17–19).
Aside from pesticides, aflatoxins have shown to increase the risk of liver disease. Aflatoxins comprise a group of mycotoxins produced by the toxigenic species, Aspergillus flavus and Aspergillus parasiticus. Aflatoxin B1, a contaminant of dietary staples (groundnuts, maize, rice, and sorghum) in tropical and subtropical regions (20), is the main aflatoxin of concern to humans. High temperatures and humidity, in conjunction with plant moisture content, are factors of fungal growth and toxin production (21). Globally, risk of aflatoxin exposure is estimated to affect 4.5 to 5.5 billion people (22). Southeast Asia, sub-Saharan Africa, and some parts of South America experience the highest risk of exposure to aflatoxins. Aflatoxin B1 exposure may be responsible for approximately between 25,200 and 155,000 HCC cases worldwide, and an estimated 40% live in sub-Saharan Africa (22).
Liver disease incidence is reportedly high in places enduring cyanobacterial harmful algae blooms (23–26). These phenomena result from photosynthetic cyanobacteria multiplying within freshwater systems given favorable environmental factors, such as light intensity, nutrients, pH, short-wavelength radiations, and temperature (27–29). Cyanobacterial harmful algae blooms can release several cyanotoxins into surrounding waters, including anatoxins, cylindrospermopsins, microcystins, nodularins, and saxitoxins (30). However, the microcystins constitute an important and prevalent cyanotoxin in surface waters globally, posing environmental and health hazards (31). Many cyanobacterial genera synthesize microcystins, including colonial Microcystis spp. and filamentous Anabaena spp., Anabaenopsis spp., Aphanizomenon, Nostoc, and Planktothrix/Oscillatoria (32). Their mode of action entails the inhibition of protein phosphatases 1A and 2B in hepatocytes, where they accumulate to induce liver damage (33, 34). Acute poisoning can interfere with liver function, promoting hemorrhage formation, and ultimately, hemorrhagic shock (35, 36). Also, liver toxicity caused by microcystin has shown to induce apoptosis, cytoskeletal disruption, DNA damage, inflammation, necrosis, and oxidative stress (37, 38).
Ingestion of contaminated drinking water is a frequent source of human exposure, although microcystins can taint aquatic organisms for consumption, harbor waters where dermal contact occurs, and drift as aerosol sprays during recreational activity (39). Acute exposure causes dermatitis, fever, headache, increased liver enzyme activity, and stomachache (40). Signs and symptoms of chronic exposure are less clear, regardless of a possible connection with an increased liver disease risk. Several epidemiological studies identified potential linkages between microcystin exposure and liver disease (23–26, 40). Fatal intoxications rarely happen, as recounted in Brazil, where cyanotoxin exposure was considered a contributing factor for the death of hemodialysis patients (41).
This mini-review investigates the linkage between environmental toxin exposure and liver disease in endemic regions. Hepatocellular carcinoma, a major cause of primary liver disease, is examined in the context of human environmental exposure. Therefore, we review and analyze pertinent epidemiological data on hepatocellular carcinoma, supporting environmental toxins as an emergent risk factor.
Hepatocellular carcinoma (HCC), a predominant form of primary liver cancer, is the third leading cause of cancer mortality worldwide. In the USA, HCC incidence has increased in recent decades and is expected to rise in the next 20 years as more individuals are diagnosed with hepatitis C virus and non-alcoholic steatohepatitis (42). From 2000 to 2012, adjusted incident rates for HCC increased by an average annual percentage change of 4.5% (95% CI 4.3–4.7) (43). The main risk factors for HCC in the USA, starting with the greatest burden for HCC, include non-alcoholic fatty liver disease, alcoholic liver disease, and hepatitis C and B viruses (44). In China, HCC is the major histological type of liver cancer, comprising 83.9–92.3% of liver cancer cases (45). Approximately 19% of the world's population resides in China, and liver cancer incidence is higher compared to other nations (46).
Primary liver cancer is a widespread disease of different varieties, with HCC accounting for about 75–85% of primary liver cancers (47). Chronic infection with hepatitis B virus (HBV) or hepatitis C virus (HCV) is a major risk factor for HCC, and HBV is the major risk factor in high incident areas of HCC (48). For instance, approximately 55% of HCC cases worldwide are due to chronic HBV infection, whereas an estimated 89% of HCC cases occur in regions endemic or hyperendemic to HBV (49, 50). In the USA, HCV is a major risk factor for HCC, where roughly 2% of the population has the disease (48). HCC in China is largely attributed to chronic hepatitis B infection, which is acquired early in life. Behavior intervention and vaccination have shown to reduce liver cancer incidence in endemic China (51). Universally, the availability of the HBV vaccine has resulted in fewer infections and resultant HCC cases. Similarly, the development of an HCV vaccine is key to a global control and elimination of HCV (52, 53).
Alcohol consumption is a recognized risk factor for liver cirrhosis and HCC. In developed nations, such as the USA and Europe, alcohol consumption is frequent and regarded as one common etiology of HCC. Depending on the country and geographic area, the ratio of alcohol abuse to all HCC etiologies varies, and roughly 15–30% of HCC is attributed to alcohol abuse (54). Multiple studies demonstrated an association between a high alcohol consumption and an increased HCC risk. For example, as reviewed in (55), an alcohol intake of >60–100 g/day increases the risk for HCC, while an alcohol intake of >600,000 ml over a person's lifespan significantly increases their risk for HCC. Furthermore, the dose-effect relationship between alcohol consumption and HCC incidence has been studied in males and females, individually, with chronic HBV infection. Individuals with a high alcohol consumption and HBV (OR 48.6 CI 95% 24.1–98.0), or HCV (OR 109 CI 95% 50.9–233.0), had an increased risk for HCC than individuals with a low alcohol consumption and without chronic viral infection (56).
The role of cigarette smoking has been examined in relation to HCC mortality, but its effects remain uncertain. Cigarette smoking is known to induce toxicity and serves as initiators and promoters of various cancers (57). A large cohort study in China demonstrated an association between cigarette smoking and HCC mortality in females, accounting for alcohol consumption and dietary habits (58). Similarly, a large cohort study in Japan determined that cigarette smoking (past and present) was an important risk factor for HCC mortality. The study conducted a univariate analysis, meaning potential confounders and interactive effects potentially altered the observed association (59).
A meta-analysis of 38 cohort and 58 case-control studies explored the association of cigarette smoking with an increased risk in liver cancer development. The adjusted meta-analysis risk ratio for liver cancer among current smokers and former smokers was 1.51 (95% CI 1.37–1.67) and 1.12 (CI 95% 0.78–1.60), respectively. Irrespective of location, publication time, sample size, and study design, epidemiological studies within the meta-analysis concluded an increased risk for liver cancer among current smokers. The number of cigarettes smoked per day also positively correlated with liver cancer (60). In Hawaii, a retrospective study concluded a non-significant association between smoking and HCC survival. However, significant associations were reported for alcohol consumption and hepatitis B. Using a multivariable model, another retrospective study confirmed cigarette smoking as a non-significant independent predictor of HCC mortality. Unlike previous studies, the study evaluated the interaction between alcohol consumption and cigarette smoking, which was statistically significant (p = 0.02) (61).
Pesticides are chemical agents used to control animals, plants, and microorganisms. Pesticide use in agricultural settings, commerce, individual households, and public health is large, increasing the likelihood of human exposures. Diet is a primary source of exposure in the USA as pesticides are routinely used in agriculture and horticulture. Alternative sources of exposure include occupation and residential proximity to agricultural pesticide applications (9, 10). It has been hypothesized that pesticide exposure contributes to hepatic carcinogenesis via genotoxic and immunotoxic mechanisms, in addition to hormonal action and tumor promotion (9). Additionally, epidemiological studies in the USA and China support an association between pesticide exposure and HCC risk. Case-control studies from China documented significant increased risks for HCC and organochlorine pesticides (62–64). Studies in the USA reported inconclusive results on pesticide exposure and HCC risk. Three studies indicated a non-significant increased risk for HCC among farmers (17–19), whereas one study revealed a higher increased risk of HCC among farmers compared to non-farmers (16). A more recent case-control study using a geographic information system demonstrated a significant association between organochlorine pesticides and increased HCC risk in males (OR 2.76 95% CI 1.58–4,82), but not in females (OR 0.83 95% CI 0.35–1.93) (65). Collectively, epidemiological studies in China and the USA provide evidence that pesticide exposure in agriculturally concentrated areas increases HCC risk in farmers.
Aflatoxins are mycotoxins produced by Aspergillus flavus and Aspergillus parasiticus. These fungi thrive in hot and humid environments, which is promising for mycotoxin production. Aflatoxin B1 (AFB1), a potent mycotoxin of Aspergillus spp., is carcinogenic to experimental animals (66). Following its ingestion, AFB1 is metabolized by the hepatic cytochrome P-450-dependent monooxygenase system to a potent AFB1-8,9 oxide (67). This metabolite forms DNA and protein adducts through covalent interactions, for example, AFB1-guanine and AFB1-albumin (68). Research on aflatoxin metabolism and toxicology has resulted in the development of exposure biomarkers to assess its role in hepatocarcinogenicity. Many of these biomarkers involve aflatoxin metabolites in urine, DNA and protein adducts in blood and tissue, and excreted urinary guanine adduct (48).
AFB1 frequently contaminates food items, including corn, legumes, and peanuts, and human exposure results from consuming such products (69). Moreover, aflatoxins have been implicated in HCC incidence, predominantly in sub-Saharan Africa, Southeast Asia, and China. These regions include developing countries with tropical and subtropical climates, which favor Aspergillus spp. growth, thus increasing aflatoxin exposure (22). Many African and Asian diets involve staples of groundnuts and maize, two crops prone to aflatoxin infection. Many epidemiological studies documented associations between AFB1 exposure biomarkers and HCC risk, and data show that dietary AFB1 exposure may explain the high incidence of HCC in sub-Saharan Africa (70).
HBV is problematic in developing countries where chronic aflatoxin exposure occurs, and both risk factors affect rural populations more significantly than urban populations. The disparity may result from fewer dietary options in rural areas compared to urban areas. In rural areas, HBV prevalence is generally high, and viral infection is greater among males than females (71). AFB1 exposure and HBV infection often co-occur, making it difficult to measure individual exposure to AFB1, considering variations in toxin concentrations of food samples. Consequently, published studies report inconsistent findings concerning dietary AFB1 exposure and HCC risk. Collecting AFB1 biomarkers before a diagnosis of HBV or HCV may benefit prospective studies, allowing researchers to examine the interaction between AFB1 exposure and HBV or HCV infections relative to HCC development.
The microcystins (MCs) represent a large group of cyanotoxins in the environment. These bioactive metabolites are low in molecular weight and can reach micromolar concentrations in bloom-infested waters. Various environmental parameters influence MC production within freshwater ecosystems, including pH, nitrogen and phosphorus, stochiometric ratio of available nitrogen to phosphorus, and water temperature (72). MCs contain a unique molecular substructure, 3-amino-9-methoxy-2,6,8-trimethyl-10-phenyl-deca-4,6-dienoic acid (Adda). Two variable sites (2 and 4) within the heptapeptide differentiates individual congeners (73). With over 250 congeners identified to date, MC-LR (leucine, arginine) is the most studied and toxic variant of MCs (74). Oral consumption of contaminated drinking water is the primary route of exposure to MCs. Uptake is dependent on a bile acid transporter facilitated by organic anion-transporting proteins expressed in hepatocytes. Once in the liver, MCs inactivate protein phosphatases types 1 and 2A, triggering liver failure (33–35). Thus, MCs are classified as hepatotoxins, and human exposure is vastly a concern in areas with a high endemicity of liver cancer (Table 1).
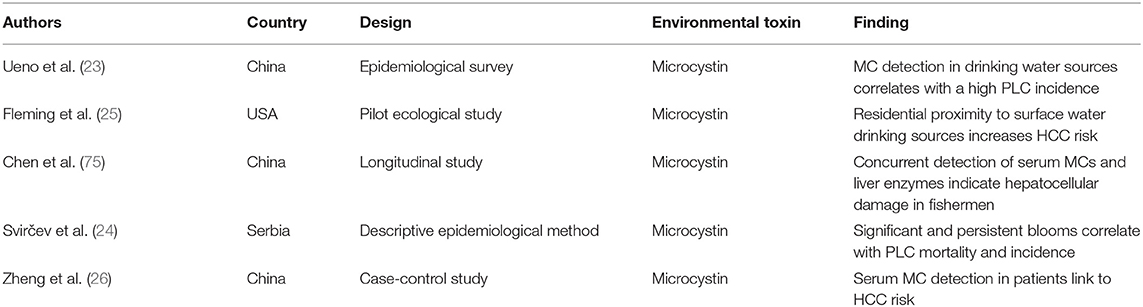
Table 1. Summary of epidemiological investigations on microcystins and liver disease.
An epidemiological survey containing three trials evaluated MC exposure and PLC in endemic China (23). The first trial discovered blue-green algal hepatotoxins in ditch/pond samples (21%), ranging from 90 to 460 pg/ml. In a second trial, MC concentrations increased from June to September (62–296 pg/ml). The third trial revealed MCs in drinking water sources of ditches/ponds, rivers, and shallow wells. Most contamination occurred in river samples (32%), followed by ditch/pond samples (17%) and shallow well samples (4%). Results of the epidemiology survey supported blue-green algal hepatotoxins in drinking water as one potential risk factor for China's high PLC incidence.
Previous findings on MC exposure and PLC incidence prompted hepatotoxin analysis in human serum. Daily chronic exposure to MCs and ensuing health effects were studied in fishermen at Lake Chaohu (75). Liquid chromatography-mass spectrometry detected MCs in 35 samples, averaging 0.389 ng/mL. Compared to the World Health Organization's tolerable daily intake for lifetime daily exposure of 2.0–3.0 μg/person, a range of 2.2–3.9 μg MC-LR equivalents was estimated as the daily intake of MCs. Multivariable analyses characterized a positive relationship between serum liver enzymes and MCs, indicating hepatocellular damage in fisherman from chronic exposure to MCs. The study demonstrated a biochemical biomarker for MC exposure via serum liver enzyme measurement. Several years later, a positive correlation was discovered for serum MC-LR and HCC risk in southwest China (7). Statistical analyses were controlled for the established risk factors, including HBV, alcohol, and aflatoxin. The odds ratio for HCC risk increased by 2.3 (95% CI 1.5–5.5) as an elevated serum MC-LR was detected in patients. Binary logistic regression determined a positive interaction with alcohol (synergism index = 4.0 95% CI 1.7–9.5) and HBV (synergism index = 3.0 95% CI 2.0–4.5), but a negative interaction with aflatoxin (synergism index = 0.4 95% CI 0.3–0.7). The results confirmed serum MC-LR as an independent risk factor for HCC risk.
Besides China, liver cancer is a malignant disease in Central Serbia and the southeastern region of the USA. Two investigation periods (1980–1990 and 2000–2002) were conducted on cyanotoxin exposure and PLC mortality and incidence in Central Serbia (24). Heavy cyanobacterial blooms occurred in regions with a high PLC mortality (11.6 for 1980–1990) and PLC incidence (34.7 for 2000–2002). A drinking water reservoir contained an elevated MC-LR concentration of 650 μg/L compared to 2.5 μg/L from tap water. Based on descriptive epidemiological data, persistent and significant blooms correlated with PLC morality and incidence. The study lacked statistical models, which could strengthen the argument that hepatotoxins in drinking water reservoirs correlate with PLC mortality and incidence. Following the detection of MCs in surface water drinking sources, a pilot ecological study in Florida assessed the proximity to a surface water treatment plant and HCC risk (25). Environmental databases connected HCC cancers diagnosed between 1981 and 1998. Residents who lived within service zones had an increased risk for HCC than residents who lived in neighboring zones. Study results limited to the population level as the design was ecological, a limitation of ecological studies. Conversely, exposure assessments can identify toxicants and their effects to determine whether a causal relationship exists between environmental exposure and adverse health outcome. The validity and variability of MC biomarkers, however, may present a challenge in defining an exposure measurement.
Liver disease is a multifactorial disease of identified factors, including alcohol consumption, cigarette smoking, and hepatitis B and C virus infections. Limited epidemiological investigations speculate the association between environmental toxin exposure and hepatocellular carcinoma development in endemic regions. Hepatocellular carcinoma, a regular cause of cancer death across the world, is continuing to grow in developing and developed nations. Herein, environmental exposure constitutes a public health hazard due to the increased usage of organochlorine pesticides in occupational settings, dietary staples perpetually contaminated with aflatoxin B1, and continued presence of hepatotoxic microcystins in drinking water sources. This mini-review examined multiple epidemiological studies on hepatocellular carcinoma in an effort to illuminate human exposure to environmental toxins as one emergent risk factor for liver disease. We found that most epidemiological data support the potential association between environmental toxins and hepatocellular cancer in the developing world. Notably, microcystin pollution in drinking water sources appears to greatly influence liver cancer, a problem worth researching due to changes in climate and personal lifestyle behaviors. Findings can be used to assist health and medical professionals in all levels of prevention, including the diagnosis and treatment of liver disease patients.
RM wrote and edited all components of the manuscript.
The author declares that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
1. Asrani SK, Devarbhavi H, Eaton J, Kamath PS. Burden of liver disease in the world. J Hepatol. (2019) 70:151–71. doi: 10.1016/j.jhep.2018.09.014
2. Xiao J, Wang F, Wong N, He J, Zhang R, Sun R, et al. Global liver disease burdens and research trends: analysis from a Chinese perspective. J Hepatol. (2019) 71:212–21. doi: 10.1016/j.jhep.2019.03.004
3. Pimpin L, Cortez-Pinto H, Negro F, Corbould E, Lazarus JV, Webber L, et al. Burden of liver disease in Europe: epidemiology and analysis of risk factors to identify prevention policies. J Hepatol. (2018) 69:718–35. doi: 10.1016/j.jhep.2018.05.011
4. Mokdad AA, Lopez AD, Shahraz S, Lozano R, Mokdad AH, Stanaway J, et al. Liver cirrhosis mortality in 187 countries between 1980 and 2010: a systematic analysis. BMC Med. (2014) 12:145. doi: 10.1186/s12916-014-0145-y
5. Moon AM, Singal AG, Tapper EB. Contemporary epidemiology of chronic liver disease and cirrhosis. Clin Gastroenterol Hepatol. (2020) 18:2650–66. doi: 10.1016/j.cgh.2019.07.060
6. GBD 2017 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancelet. (2018) 392:1789–858.
7. Ruhl CE, Everhart JE. Determinants of the association of overweight with elevated serum alanine aminotransferase activity in the United States. Gastroenterology. (2003) 124:71–9. doi: 10.1053/gast.2003.50004
8. Blair A, Ritz B, Wesseling C, Freeman LB. Pesticides and human health. Occup Environ Med. (2015) 72:81–2. doi: 10.1136/oemed-2014-102454
9. Dich J, Zahm SH, Hanberg A, Adami HO. Pesticides and cancer. Cancer Causes Control. (1997) 8:420–43. doi: 10.1023/A:1018413522959
10. Ritz B, Rull RP. Assessment of environmental exposures from agricultural pesticides in childhood leukaemia studies: challenges and opportunities. Radiat Prot Dosimetry. (2008) 132:148–55. doi: 10.1093/rpd/ncn268
11. Gunier RB, Ward MH, Airola M, Bell EM, Colt J, Nishioka M, et al. Determinants of agricultural pesticide concentrations in carpet dust. Environ Health Perspect. (2011) 119:970–6. doi: 10.1289/ehp.1002532
12. Gunier RB, Harnly ME, Reynolds P, Hertz A, Von Behren J. Agricultural pesticide use in California: pesticide prioritization, use densities, and population distributions for a childhood cancer study. Environ Health Perspect. (2001) 109:1071–8. doi: 10.1289/ehp.011091071
13. Gomaa AI, Khan SA, Toledano MB, Waked I, Taylor-Robinson SD. Hepatocellular carcinoma: epidemiology, risk factors and pathogenesis. World J Gastroenterol. (2008) 14:4300–8. doi: 10.3748/wjg.14.4300
14. Jin X, Chen M, Song L, Li H, Li Z. The evaluation of p,p'-DDT exposure on cell adhesion of hepatocellular carcinoma. Toxicology. (2014) 322:99–108. doi: 10.1016/j.tox.2014.05.002
15. Jin XT, Song L, Zhao JY, Li ZY, Zhao MR, Liu WP. Dichlorodiphenyltrichloroethane exposure indices the growth of hepatocellular carcinoma via Wnt/beta-catenin pathway. Toxicol Lett. (2014) 225:158–66. doi: 10.1016/j.toxlet.2013.12.006
16. Stemhagen A, Slade J, Altman R, Bill J. Occupational risk factors and liver cancer: a retrospective case-control study of primary liver cancer in New Jersey. Am J Epidemiol. (1983) 117:443–54. doi: 10.1093/oxfordjournals.aje.a113562
17. Austin H, Delzell E, Grufferman S, Levine R, Morrison AS, Strolley PD, et al. Case-control study of hepatocellular carcinoma, occupation, and chemical exposures. J Occup Med. (1987) 29:665–9.
18. Brownson RC, Reif JS, Chang JC, Davis JR. Cancer risks among Missouri farmers. Cancer. (1989) 64:2381–6.
19. Suarez L, Weiss NS, Martin J. Primary liver cancer death and occupation in Texas. Am J Ind Med. (1989) 15:167–75. doi: 10.1002/ajim.4700150205
20. Strosnider H, Azziz-Baumgartner E, Banziger M, Bhat RV, Breiman R, Brune M, et al. Workgroup report: public health strategies for reducing aflatoxin exposure in developing countries. Environ Health Perspect. (2006) 114:1898–903. doi: 10.1289/ehp.9302
21. Kew MC. Aflatoxins as a cause of hepatocellular carcinoma. J Gastrointestin Liver Dis. (2013) 22:305–10.
22. Williams JH, Phillips TD, Jolly PE, Stiles JK, Jolly CM, Aggarwal D. Human aflatoxicosis in developing countries: a review of toxicology, exposure, potential health consequences, and interventions. Am J Clin Nutr. (2004) 80:1106–22. doi: 10.1093/ajcn/80.5.1106
23. Ueno Y, Nagata S, Tsutsumi T, Hasegawa A, Watanabe MF, Park HD, et al. Detection of microcystins, a blue-green algal hepatotoxin, in drinking water sampled in Haimen and Fusui, endemic areas of primary liver cancer in China, by highly sensitive immunoassay. Carcinogenesis. (1996) 17:1317–21. doi: 10.1093/carcin/17.6.1317
24. Svirčev Z, Drobac D, Tokodi N, LuŽanin Z, Munjas AM, Nikolin B, et al. Epidemiology of cancers in Serbia and possible connection with cyanobacterial blooms. J Environ Sci Health C. (2014) 32:319–37. doi: 10.1080/10590501.2014.967053
25. Fleming LE, Rivero C, Burns J, Williams C, Bean JA, Shea KA, et al. Blue green algal (cyanobacterial) toxins, surface drinking water, and liver cancer in Florida. Harmful Algae. (2002) 1:157–68. doi: 10.1016/S1568-9883(02)00026-4
26. Zheng C, Zeng H, Lin H, Wang J, Feng X, Qiu Z, et al. Serum microcystin levels positively linked with risk of hepatocellular carcinoma: a case-control study in southwest China. Hepatology. (2017) 66:1519–28. doi: 10.1002/hep.29310
27. Neilan BA, Pearson LA, Muenchhoff J, Moffitt MC, Dittmann E. Environmental conditions that influence toxin biosynthesis in cyanobacteria. Environ Microbiol. (2013) 15:1239–53. doi: 10.1111/j.1462-2920.2012.02729.x
28. Häder DP, Villafañe VE, Helbling EW. Productivity of aquatic primary producers under global climate change. Photochem Photobiol Sci. (2014) 13:1370–92. doi: 10.1039/C3PP50418B
29. Rastogi RP, Sinha RP, Incharoensakdi A. The cyanotoxin-microcystins: current overview. Rev Environ Sci Bio/Technol. (2014) 13:215–49. doi: 10.1007/s11157-014-9334-6
30. Stewart I, Carmichael WW, Backer LC. Toxic cyanobacteria. In: Selendy JMH, editor. Water and Sanitation-Related Diseases and the Environment: Challenges, Interventions, and Preventive Measures. Oxford, UK: John Wiley and Sons (2011). p. 95–110.
31. Backer LC, Miller M. Sentinel animals in a one health approach to harmful cyanobacterial and algal blooms. Vet Sci. (2016) 3:8. doi: 10.3390/vetsci3020008
32. de Figueiredo DR, Azeiteiro UM, Esteves SM, Goncalves FJM, Pereira MJ. Microcystin-producing blooms-a serious global public health issue. Ecotoxicol Environ Saf. (2004) 59:151–63. doi: 10.1016/j.ecoenv.2004.04.006
33. Wiegand C, Pflugmacher S. Ecotoxicological effects of selected cyanobacterial secondary metabolites: a short review. Toxicol Appl Pharmacol. (2005) 203:201–18. doi: 10.1016/j.taap.2004.11.002
34. Runnegar M, Berndt N, Kong SM, Lee EY, Zhang L. In vivo and in vitro binding of microcystin to protein phosphatase 1 and 2A. Biochem Biophys Res Commun. (1995) 216:162–9. doi: 10.1006/bbrc.1995.2605
35. MacKintosh C, Beattie KA, Klumpp S, Cohen P, Cood GA. Cyanobacterial microcystin-LR is a potent and specific inhibitor of protein phosphatases 1 and 2A from both mammals and higher plants. FEBS Lett. (1990) 264:187–92. doi: 10.1016/0014-5793(90)80245-E
36. Dawson RM. The toxicology of microcystins. Toxicon. (1998) 36:953–62. doi: 10.1016/S0041-0101(97)00102-5
37. Liu J, Sun Y. The role of associated proteins and signal pathways in microcystin-LR toxicity. Toxicol Lett. (2015) 236:1–7. doi: 10.1016/j.toxlet.2015.04.010
38. Zhou M, Tu W, Xu J. Mechanisms of microcystin-LR induced cytoskeletal disruption in animal cells. Toxicon. (2015) 101:92–100. doi: 10.1016/j.toxicon.2015.05.005
39. Bell SG, Codd GA. Cyanobacterial toxins and human health. Rev Med Microbiol. (1994) 5:256–64. doi: 10.1097/00013542-199410000-00005
40. Zhao Y, Yan Y, Xie L, Wang L, He Y, Wan X, et al. Long-term environmental exposure to microcystins increases the risk of nonalcoholic fatty liver disease in humans: a combined fisher-based investigation and murine model study. Environ Int. (2020) 138:105648. doi: 10.1016/j.envint.2020.105648
41. Azevedo SMFO, Carmichael WW, Jochimsen EM, Rinehart KL, Lau S, Shaw G. R. Human intoxication by microcystins during renal dialysis treatment in Caruaru-Brazil. Toxicology. (2002) 181–2:441–6. doi: 10.1016/S0300-483X(02)00491-2
42. McGlynn KA, London WT. The global epidemiology of hepatocellular carcinoma, present and future. Clin Liver Dis. (2011) 15:223–43. doi: 10.1016/j.cld.2011.03.006
43. White DL, Thrift AP, Kanwal F, Davila J, El-Serag HB. Incidence of hepatocellular carcinoma in all 50 United States, from 2000 through 2012. Gastroenterology. (2017) 152:812–20. doi: 10.1053/j.gastro.2016.11.020
44. Singal AG, El-Serag HB. Hepatocellular carcinoma from epidemiology to prevention: translating knowledge into practice. Clin Gastroenterol Hepatol. (2015) 13:2140–51. doi: 10.1016/j.cgh.2015.08.014
45. Wang M, Wang Y, Feng X, Wang R, Wang Y, Zeng H, et al. Contribution of hepatitis B virus and hepatitis C virus of liver cancer in China north areas: experience of the Chinese National Cancer Center. Int J Infect Dis. (2017) 65:15–21. doi: 10.1016/j.ijid.2017.09.003
46. Torre LA, Bray F, Siegel RL, Ferlay J, Lortet-Tieulent J, Jemal A. Global cancer statistics, 2012. CA Cancer J Clin. (2015) 65:87–108. doi: 10.3322/caac.21262
47. Rawla P, Sunkara T, Muralidharan P, Raj JP. Update in global trends and aetiology of hepatocellular carcinoma. Contemp Oncol. (2018) 22:141–50. doi: 10.5114/wo.2018.78941
48. Santella RM, Wu HC. Environmental exposures and hepatocellular carcinoma. J Clin Transl Hepatol. (2013) 1:138–43. doi: 10.14218/JCTH.2013.008XX
49. Bosch FX, Ribes J, Díaz M, Cléries R. Primary liver cancer: worldwide incidence and trends. Gastroenterology. (2004) 127:5–16. doi: 10.1053/j.gastro.2004.09.011
50. Kew M. Epidemiology of chronic hepatitis B virus infection, hepatocellular carcinoma, and hepatitis B virus-induced hepatocellular carcinoma. Pathol Biol. (2010) 58:273–77. doi: 10.1016/j.patbio.2010.01.005
51. Nelson NP, Easterbrook PJ, McMahon BJ. Epidemiology of hepatitis B virus infection and impact of vaccination on disease. Clin Liv Dis. (2016) 20:607–28. doi: 10.1016/j.cld.2016.06.006
52. Zanetti AR, Van Damme P, Shouval D. The global impact of vaccination against hepatitis B: a historical overview. Vaccine. (2008) 26:6266–73. doi: 10.1016/j.vaccine.2008.09.056
53. Chen JY, Feeney ER, Chung RT. HCV and HIV co-infection: mechanisms and management. Nat Rev Gastroenterol Hepatol. (2014) 11:362–71. doi: 10.1038/nrgastro.2014.17
54. Jepsen P, Ott P, Andersen PK, Sørensen HT, Vilstrup H. Risk for hepatocellular carcinoma in patients with alcoholic cirrhosis. Ann Intern Med. (2012) 156:841–7. doi: 10.7326/0003-4819-156-12-201206190-00004
55. McGlynn KA, London WT. Epidemiology and natural history of hepatocellular carcinoma. Best Pract Res Clin Gastroenterol. (2005) 19:3–23. doi: 10.1016/j.bpg.2004.10.004
56. Donato F, Tagger A, Gelatti U, Parrinello G, Boffetta P, Albertini A, et al. Alcohol and hepatocellular carcinoma: the effect of lifetime intake and hepatitis virus infections in men and women. Am J Epidemiol. (2002) 155:323–31. doi: 10.1093/aje/155.4.323
57. Taioli E. Gene-environment interaction in tobacco-related cancers. Carcinogenesis. (2008) 29:1467–74. doi: 10.1093/carcin/bgn062
58. Evans AA, Chen EA, Ross FM, Shen WY, Lin WT, London WT. Eight-year follow-up of the 90,000-person Haimen City cohort: I. Hepatocellular carcinoma mortality, risk factors, and gender differences. Cancer Epidemiol Biomarkers Prev. (2002) 11:369–76.
59. Ogimoto I, Shibata A, Kurozawa Y, Nose T, Yoshimura T, Suzuki H, et al. Risk of death due to hepatocellular carcinoma among smokers and ex-smokers. Univariate analysis of JACC study data. Kurume Med J. (2004) 51:71–81. doi: 10.2739/kurumemedj.51.71
60. Lee YCA, Cohet C, Yang YC, Stayner L, Hashibe M, Straif K. Meta-analysis of epidemiologic studies on cigarette smoking and liver cancer. Int J Epidemiol. (2009) 38:1497–511. doi: 10.1093/ije/dyp280
61. Wong LL, Limm WM, Tsai N, Severino R. Hepatitis B, and alcohol affect survival of hepatocellular carcinoma patients. World J Gastroenterol. (2005) 11:3491–7. doi: 10.3748/wjg.v11.i23.3491
62. McGlynn KA, Abnet CC, Zhang M, Sun XD, Fan JH, O'Brien TR, et al. Serum concentrations of 1,1,1-trichloro-2,2-bis(p-chlorophenyl)ethane (DDT) and 1,1-dichloro-2,2-bis(p-chlorophenyl)ethylene (DDE) and risk of primary liver cancer. J Natl Cancer Inst. (2006) 98:1005–1110. doi: 10.1093/jnci/djj266
63. Zhao B, Shen H, Liu F, Liu S, Niu J, Guo F, Sun X. Exposure to organochlorine pesticides is an independent risk factor of hepatocellular carcinoma: A case–control study. J Expo Sci Environ Epidemiol. (2011) 22:541–8. doi: 10.1038/jes.2011.29
64. Persson EC, Graubard BI, Evans AA, London WT, Weber JP, Leblanc A, et al. Dichlorodiphenyltrichloroethane and risk of hepatocellular carcinoma. Int J Cancer. (2012) 131:2078–84. doi: 10.1002/ijc.27459
65. VoPham T, Brooks MM, Yuan JM, Talbott EO, Ruddell D, Hart JE, et al. Pesticide exposure and hepatocellular carcinoma risk: a case-control study using a geographic information system (GIS) to link SEER-Medicare and California pesticide data. Environ Res. (2015) 143:68–82. doi: 10.1016/j.envres.2015.09.027
66. Roebuck BD, Liu YL, Rogers AE, Groopman JD, Kensler TW. Protection against aflatoxin B1-induced hepatocarcinogenesis in F344 rats by 5-(2-pyrazinyl)-4-methyl-1,2-dithiole-3-thione (oltipraz): predictive role for short-term molecular dosimetry. Cancer Res. (1991) 51:5501–6.
67. Forrester LM, Neal GE, Judah DJ, Glancey MJ, Wolf CR. Evidence for involvement of multiple forms of cytochrome P-450 in aflatoxin B1 metabolism in human liver. Proc Natl Acad Sci USA. (1990) 87:8306–10. doi: 10.1073/pnas.87.21.8306
68. Gallagher EP, Wienkers LC, Stapleton PL, Kunze KL, Eaton DL. Role of human microsomal and human complementary DNA expressed cytochromes P4501A2 and P4503A4 in the bioactivation of aflatoxin B1. Cancer Res. (1994) 54:101–8.
69. Kensler TW, Roebuck BD, Wogan GN, Groopman JD. Aflatoxin: a 50-year odyssey of mechanistic and translational toxicology. Toxicol Sci. (2011) 120:28–48. doi: 10.1093/toxsci/kfq283
70. Wu HC, Santella R. The role of aflatoxins in hepatocellular carcinoma. Hepat Mon. (2012) 12:e7238. doi: 10.5812/hepatmon.7238
71. Liu Y, Wu F. Global burden of aflatoxin-induced hepatocellular carcinoma: a risk assessment. Environ Health Perspect. (2010) 118:818–24. doi: 10.1289/ehp.0901388
72. Xie L, Rediske RR, Gillett ND, O'Keefe JP, Scull B, Xue Q. The impact of environmental parameters on microcystin production in dialysis bag experiments. Sci Rep. (2016) 6:38722. doi: 10.1038/srep38722
73. Henao E, Rzymski P, Waters M. N. A review on the study of cyanotoxins in paleolimnological research: current knowledge and future needs. Toxins. (2020) 12:6. doi: 10.3390/toxins12010006
74. Dietrich D, Hoeger S. Guidance values for microcystins in water and cyanobacterial supplement products (blue-green algal supplements): a reasonable or misguided approach. Toxicol Appl Pharmacol. (2005) 203:273–89. doi: 10.1016/j.taap.2004.09.005
Keywords: aflatoxin, environmental, hepatocellular, carcinoma, liver disease, microcystin, pesticide
Citation: Melaram R (2021) Environmental Risk Factors Implicated in Liver Disease: A Mini-Review. Front. Public Health 9:683719. doi: 10.3389/fpubh.2021.683719
Received: 22 March 2021; Accepted: 17 May 2021;
Published: 24 June 2021.
Edited by:
Md. Mozammel Hoq, University of Dhaka, BangladeshReviewed by:
M. Jahangir Alam, University of Houston, United StatesCopyright © 2021 Melaram. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Rajesh Melaram, cmFqZXNoLm1lbGFyYW1Ad2FsZGVudS5lZHU=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.