 Alessio Arrivi
Alessio Arrivi Marcello Dominici1,2
Marcello Dominici1,2 Mauro Truglio
Mauro Truglio Gaetano Vaudo
Gaetano Vaudo Giacomo Pucci
Giacomo Pucci
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
BRIEF RESEARCH REPORT article
Front. Public Health , 24 June 2021
Sec. Environmental Health and Exposome
Volume 9 - 2021 | https://doi.org/10.3389/fpubh.2021.683683
This article is part of the Research Topic Insights in Environmental Health and Exposome: 2021 View all 7 articles
Background: During the lockdown for COVID-19, a massive decrease in hospital admissions for acute coronary syndrome (ACS) and a drop in air pollution were both detected in Italy. Our aim was to investigate the possible association between these two events at the Province of Terni, one of the most polluted urban and industrial area in Central Italy.
Methods: We analyzed data of daily 24-h urban air concentrations of particulate matter (PM)10 and PM2.5 from fixed station monitoring network located in the main city centers of the Terni province, and accesses for ACS at the catheterization laboratory of the Cardiological Hub Center of the Terni University Hospital during lockdown. A comparison was made with data corresponding to the same lockdown time period of years 2019, 2018, and 2017.
Results: Invasive procedures for ACS decreased in 2020 (n = 49) as compared with previous years (n = 93 in 2019, n = 109 in 2018, and n = 89 in 2017, p < 0.001). Conversely, reductions in average PM10 (20.7 μg/m3) and PM2.5 (14.7 μg/m3) in 2020 were consistent with a long-term decreasing trend, being comparable to those recorded in 2019 and 2018 (all p > 0.05) and slightly lower than 2017 (p < 0.05). The Granger-causality test demonstrated the lack of association between time-varying changes in air pollution and the number of procedures for ACS.
Conclusions: Our results did not support the hypothesis that reduction in invasive procedures for ACS during lockdown was linked to an air cleaning effect. Reasons other than reduced air pollution should be sought to explain the observed decrease in ACS procedures.
The coronavirus disease 19 (COVID-19) drastically reduced access to healthcare in 2020. Specifically, during the lockdown period, hospital admissions for acute coronary syndrome (ACS) suddenly decreased in Italy. This decrease was found significant for ST-elevation myocardial infarction (STEMI) (27%) and Non-ST-elevation myocardial infarction (NSTEMI) (65%), both in the north and in the central/south of Italy (1). Similarly, an air cleaning effect was observed by NASA and European Space Agency pollution monitoring satellites (2).
Air pollution is a sophisticated mixture of gases and particulate components (PM10 and PM2.5 with aerodynamic diameter ≤10 and ≤2.5 μM, respectively), whose concentration may change depending on the source, emission rate, and climate conditions (3). In most medical research, air pollution had a significant relationship with the occurrence of ACS (4, 5). Data from systematic reviews and meta-analyses showed that short-term exposure to particulate matter (PM2.5 and PM10) is a significant risk factor for myocardial infarction (6). A 13% relative increase in non-fatal acute coronary events was observed over the long term following a 5 μg/m3 increase in estimated annual mean PM2.5 and a 10 μg/m3 increase in estimated annual mean PM10 (7). In a study carried out in the urban areas of Utah (USA), the exposure to fine particulate matter air pollution contributed to trigger acute coronary events in patients with CAD (8). Nevertheless, the accuracy, completeness, and representativeness of data largely vary across studies (5, 9, 10) and the matter remains controversial, given also the presence of discordant results showing no association (11–13). Therefore, examining this interplay during a unique and unprecedented social upheaval, such as lockdown for COVID-19 pandemic (14), may contribute to clarify the debate on the topic.
In this research report, we aimed at analyzing the relationship between the number of invasive procedures for ACS performed at the Cardiological Hub Center of Terni, one of the most polluted urban and industrial areas in Central Italy (15), and atmospheric air pollution trends measured during the lockdown period in comparison with previous years. The main hypothesis was to find evidence of an association between variations in air quality and the number of invasive procedures for ACS through the analysis of time series data that included the lockdown period.
We retrospectively collected data related to admissions to the emergency service of the Cardiological Hub Center of the Terni University Hospital, which is equipped with catheterization laboratory providing the 24-h 7-days-a-week primary PCI (24/7 pPCI) service. This latter fully covers the cardiological emergencies of Terni and its province, a basin with about 226,000 inhabitants. We selected the number of patients who received a diagnosis of any ACS including unstable angina (UA, ICD-9 code 411.1), NSTEMI (ICD-9 code 410.7) and STEMI (ICD-9 code 410.9), and related invasive procedures, during the time period corresponding to the national lockdown, going from March 9, 2020, to May 3, 2020. To make comparison between years and to avoid running into a seasonality bias, we collected the same data during the same time period for the years 2019, 2018, and 2017. People residing outside the province of Terni and accessing the Cardiology Hub service for ACS during the periods under examination were excluded from the overall analysis. For this particular research project, individual data were not collected; data were protected for privacy purposes by rendering it anonymous prior to analysis.
We collected, on a daily basis and for the same period of time as described above, data about the average 24-h air concentration of air pollutants. Two particulate matter (PM) pollutants, PM10 and PM2.5, were selected for this analysis because they were shown to have a significant relationship with the occurrence of ACS in previous research (4, 5). These data were extracted from the data made public on the service website (www.arpa.umbria.it), and corresponded to the average value recorded from the entire network of fixed public monitoring stations, consisting of six units located within the main city centers of the province of Terni with more than 10,000 inhabitants (Terni = 3, Narni = 1, Amelia = 1, Orvieto = 1, total population 161,771 people, representing the 72% of inhabitants of the Province of Terni, Figure 1). The two PM measures (PM10 and PM2.5) were standardized and averaged out.
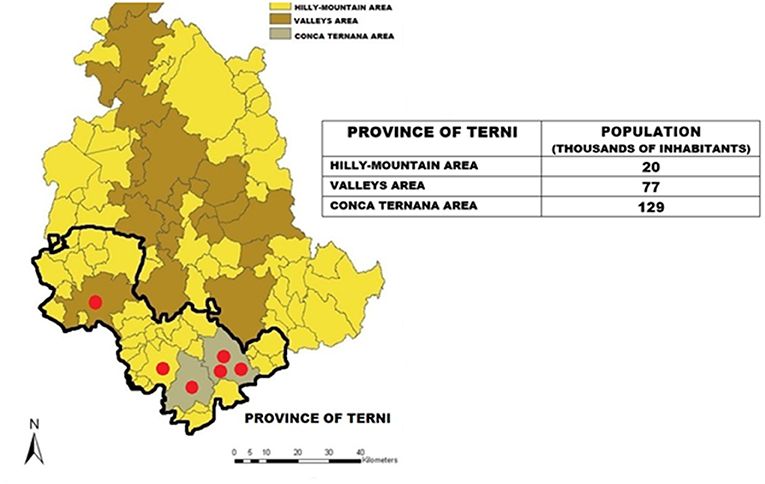
Figure 1. Geographical map of the province of Terni showing the distribution of the network of fixed public monitoring stations, consisting of six units located within the main city centers of the Terni province with more than 10,000 inhabitants (Terni = 3, Narni = 1, Amelia = 1, Orvieto = 1, total population 161,771 people, representing the 72% of the province of Terni).
We first tested the normality of the distribution of pollutants (PM10 and PM2.5) through appropriate statistics (Kolmogorov–Smirnov test) and performed an analysis of variance for repeated measures (Repeated Measures ANOVA) to evaluate an overall difference in the distribution of average values across years. This test was combined with the appropriate post-hoc paired t-tests for further pairwise comparisons. The distribution of the daily number of procedures for ACS was analyzed through a Generalized Linear Model, which was checked for over- and underdispersion. The Iteratively Reweighted Least Squares (IRLS) algorithm was used in order to find the maximum likelihood estimate for the model (16), while the pairwise Wald test was used for post-hoc comparisons.
We performed an analysis of the significance between time series of both pollutants and number of procedures, based on three main steps: (1) a time/count analysis, to evaluate possible interactions between yearly time series of pollution and the number of procedures, by testing for at-a-glance visual similarities in slopes; (2) a dynamic time warping (17) (DTW), which measures a smart distance between two curves, taking any possible lags into account, from which it is possible to build dendrograms showing possible relations between all the elements under analysis; (3) the Granger causality test (18), which was run to evaluate possible causation relationships between the two object variables, properly treated as times series data whose stationarity was verified by the Augmented Dickey-Fuller method (19). According to its original formulation, a time series X(t) Granger-causes Y(t), if the past values of X(t) help in predicting the future values of Y(t). Similarly to the DTW, the Granger causality test takes into account possible lags between the two series under analysis. The optimal number of lags under study is usually a compromise between bias and power: using too few lags, there is a risk of a biased test because of residual auto-correlation; using too many could lead to potentially spurious rejections of the null hypothesis (i.e., random correlations). For this study, an interval of lags between 1 and 10 was tested. We carried out two sensitivity analyses: one after taking PM10 and PM2.5 separately, the second after restriction of the time span to 2019 and 2020, in order to find if a causation started during this time period.
The total number of invasive procedures for ACS, PM10 and PM2.5 levels and their average value, divided per years, are all reported in Table 1. Average PM2.5 and PM10 air concentrations recorded in 2020 were consistent with a long-term decreasing trend, being comparable with levels recorded during 2019 (15.9 mg/m3) and 2018 (20.1 mg/m3, p vs. 2020 >0.05). A slight, although significant, reduction was observed when levels recorded in 2020 were compared with 2017 (20.2 mg/m3, p vs. 2020 <0.05). PM10 and PM2.5 levels recorded during 2019 were also significantly lower than during 2018 and 2017 (both p < 0.001, Figure 2A).

Table 1. Average levels of particulate matter (PM)2.5 and PM10 (μg/m3), their average, and the number of invasive procedures for acute coronary syndromes (ACS) recorded during the lockdown period in 2020 and during the same time period in 2019, 2018, and 2017.
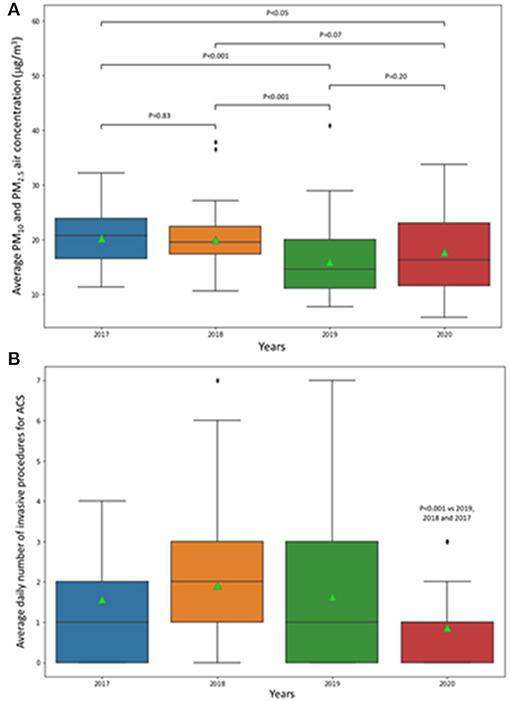
Figure 2. Box and whiskers plot representing (A) the distribution of particulate matter (PM)10 and PM2.5 air concentration and (B) the distribution of the number of invasive procedures for acute coronary syndromes (ACS) recorded between March 9 and May 3 of 2020, 2019, 2018, and 2017. The ends of the box are the upper and lower quartiles; the horizontal line inside the box represents the median, and the green triangle denotes the mean. The end of the whiskers represents the upper and lower extremes; data beyond those values are outliers.
Regarding the number of urgent invasive procedures for ACS, the GLM using further affirmation with IRLS algorithm revealed no signs of overdispersion (Pearson χ2/DF residuals = 1.32); accordingly, a significant reduction in procedures in 2020 as compared with the other years at the pairwise Wald test was found (p < 0.001, Figure 2B).
The analysis of the time series divided by years did not reveal any possible at-a-glance similarity in slopes of the time series for both procedures and air pollution during the whole time period explored (Figure 3).
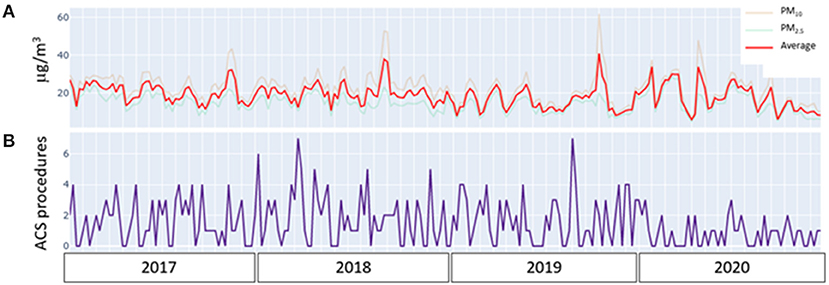
Figure 3. (A) Time/counts analysis plot of time series of air concentration of particulate matter (PM)2.5 (blue), PM10 (pink) air pollutants, and their average (red), in the examined periods from 2017 to 2020. (B) Time/counts analysis plot of time series of the number of invasive procedures for acute coronary syndromes (ACS procedures) in the examined periods from 2017 to 2020. The visual inspection of the graph excludes any at-a-glance similarity in slopes of the time series by years.
In order to perform the Granger causality test, the stationarity of the time series was successfully tested with the Augmented Dickey–Fuller method (p = 0.005 for pollution, p < 0.000001 for invasive procedures count). The Granger test did not reveal any significant correlation between the time series describing the changes in air pollution and the number of procedures performed. This result demonstrated the absence of any relationship between changes in air pollution and the number of urgent procedures performed for ACS. In a sensitivity analysis, no differences were found when PM10 and PM2.5 air concentrations were analyzed separately, neither when the analysis was conducted considering the different ACS phenotypes (unstable angina, NSTEMI, and STEMI). Moreover, we did not find any significant difference in the overall results when the time series analysis was restricted only to years 2019 and 2020.
The main aim of our study was to assess possible associations between changes in particulate air components (PM10 and PM2.5) and the number of urgent invasive procedures for ACS managed at the Hub Center of the Terni University Hospital, covering the entire province of Terni (about 226,000 inhabitants), by analyzing the changes that took place during the time of the lockdown period imposed by the Italian government to contrast the consequences of the COVID-19 pandemic, compared to the same periods of time during the previous years. We decided to compare the same calendar period (March 9 to May 3) across the different years to avoid running into a seasonality bias: although the exact trigger of ACS may not always be readily apparent, seasonal variations in their incidence are well-known (20), with highest ACS events from March to May (21).
Our data showed only slight changes in air pollution levels of PM10 and PM2.5 recorded in 2020 across the Terni province. This trend was more consistent with a long-term improvement in air quality instead of a sudden decrease caused by restrictions imposed by the Italian government. Conversely, the reduction in urgent invasive procedures for ACS in 2020 was massive (n = 49, −47%), as compared with 2019 (n = 93) and with previous years. Using at our best all the appropriate statistical approaches evaluating possible interactions between yearly time series of the two variables, our analysis failed to demonstrate a possible relationship between these two events. Our results, therefore, refuse the initial hypothesis of a possible causative role for the reduction of air particulate matter as a determinant of the decrease in ACS during the lockdown period.
Short- and long-term exposure to air pollutants (especially PM2.5, but also PM10) has been associated with an increased risk of ACS, particularly STEMI, in previous research (4, 5). There is consistent pathophysiological background in support of such association. Indeed, fine PM incentivize inflammatory response predisposing to atherosclerosis (22), enhance thrombosis/coagulation (23), and impair endothelial function increasing plaque rupture vulnerability (24) and vessel vasoconstriction (25, 26). Mustafic et al. demonstrated a significant correlation between the rise of the most frequently evaluated components of air pollution and the occurrence of AMI (27). Subsequent studies in Europe and USA confirmed this hypothesis (4, 8, 28). Whereas, much of the recent literature supports this association, there are also studies rejecting this causal link (11–13). Different geographical context and inaccuracies in the representation of time series for both pollutants and health outcomes may have contributed in previous research to such discrepancy (5, 9, 10). We believe that the analysis of time series data including the unprecedented social upheaval represented by the lockdown measures for COVID-19 pandemic could have offered a unique chance to get further insights into this topic.
The choice to consider all the ACS in the manuscript was dictated by their common pathophysiological thread: it is actually known from previous literature data how air pollution is associated with key markers of the atherothrombotic burden, including systemic inflammatory response, oxidative stress, and endothelial dysfunction (29); this evolving process may lead to instability of vulnerable plaque, with its consequent rupture/erosion; the last one is the common hallmark of all ACS (30). Based on evidence of heart muscle damage, ACS clinically manifests as unstable angina and non-ST-elevated or ST-elevated myocardial infarction (MI) (31).
Terni is recognized as one of the most polluted cities in Central Italy (32). This is due to its particular geographical location: in fact, its basin is surrounded by the Apennine mountains; this geophysical configuration limits the dispersion and enhances the accumulation of atmospheric pollutants. The main sources of pollution are vehicular traffic, domestic heating, and industrial emissions such as a power plant for waste treatment and an active steel plant (33). More importantly, people residing in the province of Terni were found to be characterized by a very low rate of long-distance and short-distance internal migration, a situation that is completely different to the larger urban areas, such as Rome and Milan (34).
During the initial period of COVID-19 pandemic, an unprecedented massive decrease in hospital admissions for ACS (specifically −27% of STEMI and −65% of NSTEMI) was described in Italy as well as in other parts of the world (1). The real determinants of such reduction remains, to date, a matter of debate. The short-term improvement in air pollution observed during the COVID-19 crisis has been hypothesized as one of the reasons for such decrease (35). Results from our study argue against the hypothesis that the reduction in invasive procedures for ACS was at least in part explained by an improvement in air quality. Indeed, we failed to find a causative relationship between the two events even when accounting for possible associations occurring in previous years. The Granger causality test proved to be a powerful ally in this scenario, as it is aimed at identifying directed functional (“causal”) interactions from time-series data (18). Granger causality implements a statistical, predictive notion of causality whereby causes precede, and help predict, their effects; it is defined in both the time and frequency domains, and it allows for the conditioning out of common causal influences. One of its known limitations (36) is that reducing the number of observations causes uncertainty in the Granger estimates, possibly leading to rejection of the null hypothesis (no causation) due to lack of power. Therefore, we cannot exclude that the absence of any significant association between PM2.5 and PM10 air exposure and the number of invasive procedures for ACS, as observed in our single-center study, was partially driven by a low sample size (a basin of about 226,000 citizens). Moreover, given the low number of public monitoring stations for air pollutants (n = 6) scattered throughout the territory of the province of Terni, we acknowledge that an increased number and a more spread out distribution of such stations could ideally provide more robust data about the real distribution of air pollution determinants. However, as previously reported, the particular geographical context, the specific migration characteristics that tend to keep the population relatively stable over years, and the high levels of exposure to air pollutants could, at least in part, counterbalance such limitations.
Since data of PM2.5 and PM10 concentrations were the only air pollutants expressed in absolute terms from the list of pollutants made publicly available on the public website, we cannot exclude that other air pollutants could reflect a different behavior. Moreover, individual exposures to other sources of air pollution, such as indoor exposure and distance from busy roads, were not analyzed in this particular research project. We cannot also exclude that the air cleaning time was too short to lead to a significant causal drop in ACS during lockdown or, in parallel, that the real incidence of ACS during the COVID-19 outbreak was underestimated. Indeed, this latter finding may be caused by the fact that some patients did not make use of hospital care during the pandemic due to fear of contagion from COVID-19 (37). Due to its retrospective nature, any relationship of causation between a variable exposure and events cannot be definitely drawn from our study. Nevertheless, we adopted rather robust statistical methodology that could represent an appropriate and up-to-date analytical approach on a topic that is not yet clear, provided that further longitudinal studies are needed to better clarify this point. The lack of association between air pollution and ACS in our manuscript may be explained considering other factors; in fact, apart from environmental conditions, different triggers of acute myocardial infarction have been examined in several studies; among these, intense exercise or physical exertion, emotional stress, and inadequate control of cardiovascular risk factors can be taken into account (38). Therefore, it is plausible that some behaviors seen during the lockdown (a slight increased physical activity, especially for bodyweight training, more relaxation and family time, adherence to the Mediterranean diet and therapy, and a mild percentage reduction in smokers) may have played a role in the minor incidence of ACS (37, 39, 40).
In conclusion, we failed to find an association between an air cleaning effect observed during lockdown and a concomitant reduction in invasive procedures for ACS in the province of Terni. Reasons other than reduced air pollution should be sought to explain the observed decrease in ACS procedures.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
AA, MD, NB, MT, GV, and GP: made substantial contributions to the conception or design of the work to the acquisition, analysis and interpretation of data for the work, drafted the work and revised it critically for important intellectual content, gave final approval of the version to be published, and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
1. De Rosa S, Spaccarotella C, Basso C, Calabrò MP, Curcio A, Perrone Filardi P, et al. Reduction of hospitalizations for myocardial infarction in Italy in the COVID-19 era. Eur Heart J. (2020) 41:2083–8. doi: 10.1093/eurheartj/ehaa409
2. Barthels M. Europe's Air Pollution Drop Continues Amid Coronavirus Closures. Space. com (2020). Available online at: https://www.space.com/italy-coronavirus-outbreak-response-reduces-emissions-satellite-images.html (accessed May 24, 2021).
3. Hamanaka RB, Mutlu GM. Particulate matter air pollution: effects on the cardiovascular system Front Endocrinol (Lausanne). (2018) 9:680. doi: 10.3389/fendo.2018.00680
4. Argacha JF, Collart P, Wauters A, Kayaert P, Lochy S, Schoors D, et al. Air pollution and ST-elevation myocardial infarction: a case-crossover study of the Belgian STEMI registry 2009-2013. Int J Cardiol. (2016) 223:300–5. doi: 10.1016/j.ijcard.2016.07.191
5. Akbarzadeh MA, Khaheshi I, Sharifi A, Yousefi N, Naderian M, Namazi MH, et al. The association between exposure to air pollutants including PM 10, PM 2.5, ozone, carbon monoxide, sulfur dioxide, and nitrogen dioxide concentration and the relative risk of developing STEMI: a case-crossover design. Environ Res. (2018) 161:299–303. doi: 10.1016/j.envres.2017.11.020
6. Luo C, Zhu X, Yao C, Hou L, Zhang J, Cao J, et al. Short-term exposure to particulate air pollution and risk of myocardial infarction: a systematic review and metaanalysis. Environ Sci Pollut Res. (2015) 22:14651–62. doi: 10.1007/s11356-015-5188-x
7. Cesaroni G, Forastiere F, Stafoggia M, Andersen ZJ, Badaloni C, Beelen R, et al. Long term exposure to ambient air pollution an dincidence of acute coronary events: prospective cohort study and meta-analysis in 11 European cohorts from the ESCAPE Project. BMJ. (2014) 348:f7412. doi: 10.1136/bmj.f7412
8. Pope CA, Muhlestein JB, Anderson JL, Cannon JB, Hales NM, Meredith KG, et al. Short-term exposure to fine particulate matter air pollution is preferentially associated with the risk of ST-segment elevation acute coronary events. J Am Heart Assoc. (2015) 4:e002506. doi: 10.1161/JAHA.115.002506
9. Collart P, Dramaix M, Lev∧eque A, Coppieters Y. Short-term effects of air pollution on hospitalization for acute myocardial infarction: age effect on lag pattern. Int J Environ Health Res. (2017) 27:68–81. doi: 10.1080/09603123.2016.1268678
10. Ho AFW, Zheng H, Earnest A, Cheong KH, Pek PP, Seok JY, et al. Time-stratified case crossover study of the association of outdoor ambient air pollution with the risk of acute myocardial infarction in the context of seasonal exposure to the Southeast Asian Haze problem. J Am Heart Assoc. (2019) 8: e011272. doi: 10.1161/JAHA.118.011272
11. Berglind N, Ljungman P, Möller J, Hallqvist J, et al. Air pollution exposure: a trigger for myocardial infarction? Int J Environ Res Public Health. (2010) 7:1486–99. doi: 10.3390/ijerph7041486
12. Peters A, von Klot S, Heier M, Trentinaglia I, Cyrys J, Hormann A, et al. Particulate air pollution and nonfatal cardiac events. Part I. Air pollution, personal activities, and onset of myocardial infarction in a case-crossover study. Res Rep Health Eff Inst. (2005) 124:1–66.
13. Sullivan J, Sheppard L, Schreuder A, Ishikawa N, Siscovick D, Kaufman J. Relation between short-term fine-particulate matter exposure and onset of myocardial infarction. Epidemiology. (2005) 16:41–8. doi: 10.1097/01.ede.0000147116.34813.56
14. Gorini F, Chatzianagnostou K, Mazzone A, Bustaffa E, Esposito A, Berti S, et al. “Acute myocardial infarction in the time of COVID-19”: a review of biological, environmental, and psychosocial contributors. Int J Environ Res Public Health. (2020) 17:7371. doi: 10.3390/ijerph17207371
15. Moroni B, Ferrero L, Crocchianti S, Perrone MG, Sangiorgio G, Bolzacchini E, et al. Aerosol dynamics upon Terni basin (Central Italy): results of integrated vertical profile measurements and electron microscopy analysis. Rendiconti Lincei Sci Fisiche Nat. (2013) 24:319–28. doi: 10.1007/s12210-013-0230-8
16. Burrus CS. Iterative Reweighted Least Squares. OpenStax CNX, (2012). Available online at: http://cnx.org/contents/92b90377-2b34-49e4-b26f-7fe572db78a1@12
17. Meert W, Hendrickx K, Van Craenendonck T. wannesm/dtaidistance (Version v2.0.0). Zenodo. (accessed May 24, 2021).
18. Granger C. Investigating causal relations by econometric models and cross-spectral methods. Econometrica. (1969) 37:424–38. doi: 10.2307/1912791
19. Dickey DA, Fuller WA. Distribution of the estimators for autoregressive time series with a unit root. J Am Stat Assoc. (1979) 74:427–31. doi: 10.1080/01621459.1979.10482531
20. Stewart S, Keates AK, Redfern A, McMurray JJV. Seasonal variations in cardiovascular disease. Nat Rev Cardiol. (2017) 14:654–64. doi: 10.1038/nrcardio.2017.76
21. Sharif Nia H, Chan YH, Froelicher ES, Pahlevan Sharif S, Yaghoobzadeh A, Jafari A, et al. Weather fluctuations: predictive factors in the prevalence of acute coronary syndrome. Health Promot Perspect. (2019) 9:123–30. doi: 10.15171/hpp.2019.17
22. Newby DE, Mannucci PM, Tell GS, Baccarelli AA, Brook RD, Donaldson K, et al. Expert position paper on air pollution and cardiovascular disease. Eur Heart J. (2015) 36:83–93b. doi: 10.1093/eurheartj/ehu458
23. Mills NL, Törnqvist H, Gonzalez MC, Vink E, Robinson SD, Söderberg S, et al. Ischemic and thrombotic effects of dilute diesel-exhaust inhalation in men with coronary heart disease. N Engl J Med. (2007) 357:1075–82. doi: 10.1056/NEJMoa066314
24. Suwa T, Hogg JC, Quinlan KB, Ohgami A, Vincent R, van Eeden SF. Particulate air pollution induces progression of atherosclerosis. J Am Coll Cardiol. (2002) 39:935–42. doi: 10.1016/S0735-1097(02)01715-1
25. Bouthillier L, Vincent R, Goegan P, Adamson IY, Bjarnason S, Stewart M, et al. Acute effects of inhaled urban particles and ozone: lung morphology, macrophage activity, and plasma endothelin-1. Am J Pathol. (1998) 153:1873–84. doi: 10.1016/S0002-9440(10)65701-X
26. Brook RD, Brook JR, Urch B, Vincent R, Rajagopalan S, Silverman F. Inhalation of fine particulate air pollution and ozone causes acute arterial vasoconstriction in healthy adults. Circulation. (2002) 105:1534–6. doi: 10.1161/01.CIR.0000013838.94747.64
27. Mustafic H, Jabre P, Caussin C, Murad MH, Escolano S, Tafflet M, et al. Main air pollutants and myocardial infarction: a systematic review and meta-analysis. JAMA. (2012) 307:713–21. doi: 10.1001/jama.2012.126
28. Goldberg MS, Burnett RT, Stieb DM, Brophy JM, Daskalopoulou SS, Valois M, et al. Associations between ambient air pollution and daily mortality among elderly persons in Montreal, Quebec. Sci Total Environ. (2013) 464:931–42. doi: 10.1016/j.scitotenv.2013.06.095
29. Vaudrey B, Mielcarek M, Sauleau E, Meyer N, Marchandot B, Moitry M, et al. Short-term effects of air pollution on coronary events in Strasbourg, France-Importance of seasonal variations. Med Sci (Basel). (2020) 8:31. doi: 10.3390/medsci8030031
30. Torbicki A, Kastrati A, Vahanian A, Auricchio A, Hoes A, Merkely, et al. ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation: The Task Force for the management of acute coronary syndromes (ACS) in patients presenting without persistent ST-segment elevation of the European Society of Cardiology (ESC). Eur Heart J. (2011) 32:2999–3054. doi: 10.1093/eurheartj/ehr236
31. Fanaroff AC, Rymer JA, Goldstein SA. Acute coronary syndrome. JAMA. (2015) 314:1990. doi: 10.1001/jama.2015.12743
32. Guerrini R. Qualità dell'aria nella provincia di Terni tra il 2002 e il 2011. Quad. ARPA Umbria XXXIII (2012). p. 81–7.
33. Folli S. Covid-19 e Qualità dell'aria nel Bacino Padano. Available online at: https://www.snpambiente.it/2020/06/19/covid-19-e-qualita-dellaria-nel-bacino-padano-2/ (accessed July 4, 2020).
34. Bonifazi C, Heins F, Licari F, Tucci E. The regional dynamics of internal migration intensities in Italy. Popul Space Place. (2020) e2331. doi: 10.1002/psp.2331
35. Picano E. Where have all the myocardial infarctions gone during lockdown? The answer is blowing in the less-polluted wind. Eur Heart J. (2020) 41:2146–7. doi: 10.1093/eurheartj/ehaa411
37. Mamas M. What Impact Has COVID-19 Had on ACS Presentations? (2020). Available online at: https://www.medscape.com/viewarticle/928083#vp/2 (accessed April 12, 2020).
38. Nawrot TS, Perez L, Künzli N, Munters E, Nemery B. Public health importance of triggers of myocardial infarction: a comparative risk assessment. Lancet. (2011) 377:732–40. doi: 10.1016/S0140-6736(10)62296-9
39. Di Renzo L, Gualtieri P, Pivari F, Soldati L, Attinà A, Cinelli G, et al. Eating habits and lifestyle changes during COVID-19 lockdown: an Italian survey. J Transl Med. (2020) 18:229. doi: 10.1186/s12967-020-02399-5
Keywords: air pollution, acute coronary syndromes, invasive procedures, COVID-19, lockdown, particulate matter
Citation: Arrivi A, Dominici M, Bier N, Truglio M, Vaudo G and Pucci G (2021) Association Between Air Pollution and Acute Coronary Syndromes During Lockdown for COVID-19: Results From the Terni Hub Center. Front. Public Health 9:683683. doi: 10.3389/fpubh.2021.683683
Received: 21 March 2021; Accepted: 14 May 2021;
Published: 24 June 2021.
Edited by:
Sonia Dagnino, Imperial College London, United KingdomReviewed by:
Ka Hung Chan, University of Oxford, United KingdomCopyright © 2021 Arrivi, Dominici, Bier, Truglio, Vaudo and Pucci. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Giacomo Pucci, Z2lhY29tby5wdWNjaUB1bmlwZy5pdA==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.