 Rasheed Omobolaji Alabi1,2*
Rasheed Omobolaji Alabi1,2* Päivi Hietanen3Mohammed Elmusrati2
Päivi Hietanen3Mohammed Elmusrati2 Omar Youssef1,4Alhadi Almangush1,4,5
Omar Youssef1,4Alhadi Almangush1,4,5 Antti A. Mäkitie1,6,7
Antti A. Mäkitie1,6,7- 1Research Program in Systems Oncology, Faculty of Medicine, University of Helsinki, Helsinki, Finland
- 2Department of Industrial Digitalization, School of Technology and Innovations, University of Vaasa, Vaasa, Finland
- 3Docrates Cancer Center, Helsinki, Finland
- 4Department of Pathology, University of Helsinki, Helsinki, Finland
- 5University of Turku, Institute of Biomedicine, Pathology, Turku, Finland
- 6Department of Otorhinolaryngology – Head and Neck Surgery, University of Helsinki and Helsinki University Hospital, Helsinki, Finland
- 7Division of Ear, Nose and Throat Diseases, Department of Clinical Sciences, Intervention and Technology, Karolinska Institute and Karolinska University Hospital, Stockholm, Sweden
Objectives: The purpose of this study was to provide a scoping review on how to address and mitigate burnout in the profession of clinical oncology. Also, it examines how artificial intelligence (AI) can mitigate burnout in oncology.
Methods: We searched Ovid Medline, PubMed, Scopus, and Web of Science, for articles that examine how to address burnout in oncology.
Results: A total of 17 studies were found to examine how burnout in oncology can be mitigated. These interventions were either targeted at individuals (oncologists) or organizations where the oncologists work. The organizational interventions include educational (psychosocial and mindfulness-based course), art therapies and entertainment, team-based training, group meetings, motivational package and reward, effective leadership and policy change, and staff support. The individual interventions include equipping the oncologists with adequate training that include—communication skills, well-being and stress management, burnout education, financial independence, relaxation, self-efficacy, resilience, hobby adoption, and work-life balance for the oncologists. Similarly, AI is thought to be poised to offer the potential to mitigate burnout in oncology by enhancing the productivity and performance of the oncologists, reduce the workload and provide job satisfaction, and foster teamwork between the caregivers of patients with cancer.
Discussion: Burnout is common among oncologists and can be elicited from different types of situations encountered in the process of caring for patients with cancer. Therefore, for these interventions to achieve the touted benefits, combinatorial strategies that combine other interventions may be viable for mitigating burnout in oncology. With the potential of AI to mitigate burnout, it is important for healthcare providers to facilitate its use in daily clinical practices.
Conclusion: These combinatorial interventions can ensure job satisfaction, a supportive working environment, job retention for oncologists, and improved patient care. These interventions could be integrated systematically into routine cancer care for a positive impact on quality care, patient satisfaction, the overall success of the oncological ward, and the health organizations at large.
Introduction
The oncologists are confronted with important decisions daily due to their dealings with patients with cancer (1). This makes this specialty inherently challenging as cancer is capable of inflicting devastation on the life of the person diagnosed with it. The individuals diagnosed with cancer usually experience psychological trauma, overwhelming emotions, and social and economic burden due to the effects of this deadly disease (2). As a result, oncologists are often exposed to long hours of direct patient care (3), medical counseling of the families of the patients, cumbersome electronic documentation, ever-changing medical environments, feeling of loss of control over daily responsibilities, and dissatisfaction in the provided resources by the health facilities to deal with emotional reactions of patients and their families (4, 5).
Despite the significant advances in the field of oncology, many patients with cancer still face long-suffering and die of the disease. This constantly exposes oncologists to difficult feelings of grief and compassion fatigue. At the same time, they have to use their cognitive and intellectual capacities to administer complex treatments to patients who are seriously ill. These aforementioned factors make them vulnerable to burnout syndrome (5). Following the first time that the term was described by psychologist Herbert Freudenberger, several attempts have been made to properly put this phenomenon into perspective (6–9). For instance, the WHO considered burnout as a syndrome that includes feelings of energy depletion, job dissatisfaction, and reduced professional performance (10). Likewise, it was construed as a form of chronic job stress that is characterized by three principal constructs, which include emotional exhaustion, cynicism and depersonalization, and reduced personal and professional efficacy (7, 11). Although, later definitions have eschewed personal and professional accomplishment as it was found that it overlaps with individual traits such as self-efficacy (12). Other forms of burnout manifestations include physical exhaustion, frequent oncology-related ethical mistakes, ineffectiveness, decreasing professional competence, unexplainable mood swing and absenteeism, and a sense of detachment toward colleagues and patients (13–15).
The challenge of burnout in oncology has a mean prevalence of 70% in Europe (16) and varies between 20 and 70% around the world (17, 18). Additionally, it is a multifaceted phenomenon with negative impacts on oncologists, colleagues, patients, and healthcare institutions (19). For oncologists, it affects personal well-being and increases the possibility of medical errors (17, 18). Consequently, these have profound effects on the patients as it affects their adherence to treatment recommendations and reduces the overall satisfaction of the medical care provided (20–23). Furthermore, these negative consequences underscore the long-term success of healthcare establishments (5, 24, 25).
In the absence of adequate well-being of oncologists, there is a significant chance for the oncologists to leave in search of a more conducive working environment or decrease the working hours (26, 27). Similarly, an increasing number of chemical dependence [alcoholism, drug addiction, and cigarette smoking (15)], and frequent disagreement between colleagues have been reported among oncologists (28). Also, the recent increase in suicide rates among junior doctors suggests the need to properly examine the issue of burnout in healthcare facilities (29). These observations are pointers that a holistic approach is important to understand the well-being of oncologists. Of note, in the current economic situation due to the COVID-19 pandemic, many institutions will have to deal with a decrease in staff numbers and other resources. It is expected that work may become increasingly stressful which may lead to burnout.
Therefore, understanding how to address oncologist burnout may offer an insightful step toward improving the quality of care offered to patients with cancer. As a result of this, we aim to conduct a scoping review of the published articles to identify the evidence-based approaches that focused on how to address and mitigate burnout in the oncology medical profession. Furthermore, we identify and analyze how artificial intelligence (AI) can assist to mitigate burnout in this field. The aforementioned research questions are important to map the current state of research in this subject area (oncology) when planning future research. Burnout in oncology was specifically considered as oncologists have been touted to be frequently affected by burnout syndrome and thus becoming one of the most vulnerable professionals (4, 30).
Materials and Methods
Search Protocol
In this study, we systematically retrieved all studies that addressed burnout in oncology. The systematic search included databases of Ovid Medline, PubMed, Scopus, and Web of Science from inception until the end of July 2021. The framework that informed the search strategy was guided by the population (participants), concept, and context framework (PCC) (31). With the PCC paradigm, the questions of “who,” “what,” and “with what qualifiers” questions were answered. That is, the population (who: oncologists), concept (what: burnout), and context (what qualifiers: mitigate burnout) paradigm was used to formulate the research questions. Thus, the search approach was developed by combining search keywords: [(“addressing AND burnout AND oncology”) OR (“mitigating AND burnout AND oncology”)]. The search terms were extended to consider other related terms such as [(“emotional exhaustion” OR “cynicism” OR “depersonalization” OR “professional inefficacy” AND “mitigating” AND “oncology”)]. The search term extension was necessary to capture all possible studies. The retrieved hits were further analyzed for possible duplicates and irrelevant studies. Also, to further minimize the omission of any study, the reference lists of all the eligible articles were manually searched to ensure that all the relevant studies were duly included. In addition, experts were contacted and a Google search (Google Scholar) for relevant articles or PhD theses relating to this scoping review was done. To avoid selection bias due to selective publication, and most importantly, to enrich the scoping review process and reduce research waste, unpublished studies were also considered. The Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) was used in the searching and screening processes (Figure 1).
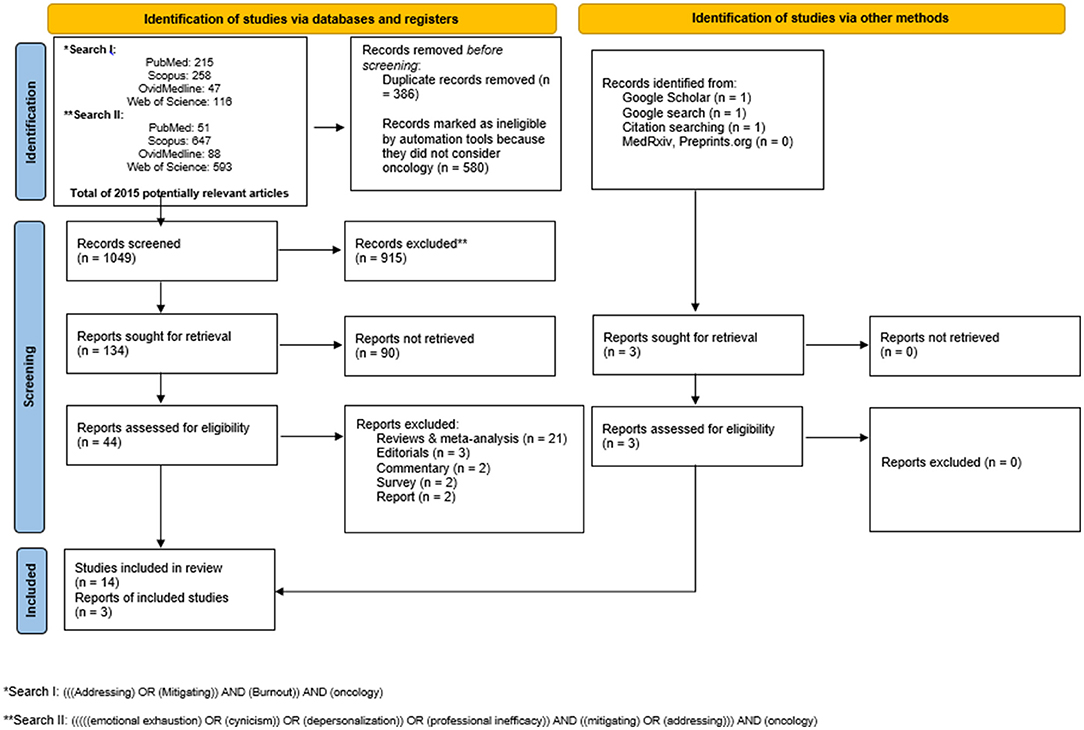
Figure 1. The Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) flow diagram highlighting the search strategy and the search results.
Inclusion and Exclusion Criteria
All studies that had examined how to address or mitigate burnout in oncology were included in this study. However, studies that considered ways of mitigating or addressing burnout among radiation therapists, physician assistants, medical assistants, graduate medical trainees, radiologists, physicians, nurses, infusion center professionals, and nursing oncology were excluded. Additionally, studies that considered burnout interventions in other fields such as social sciences, psychology, environmental science, biochemistry, genetics, molecular biology, neuroscience, doctors, pharmacology, toxicology, and pharmaceutical; arts and humanities, business, management, and accounting were excluded. Similarly, to further enhance the quality of this study, comments, opinions, perspectives, editorials, reviews, abstracts only, and articles in languages other than English were excluded (Figure 1). As this study was aimed at a scoping review, a meta-analysis of the included studies was not performed.
Screening
The screening was done in two distinct stages. In the first stage, two independent reviewers (RA and OY) used a data extraction sheet to examine the titles and abstracts of the retrieved and potentially relevant articles. The data extraction sheet was used to minimize the omission of possible eligible studies. The interobserver reliability was measured using Cohen's Kappa coefficient (κ = 0.83). In the second stage, possible discrepancies regarding the studies considered relevant were resolved by a consensus meeting and discussion between the two independent reviewers. The relevant information regarding the study characteristics of each of these potentially relevant articles was extracted (summarized in Table 1).
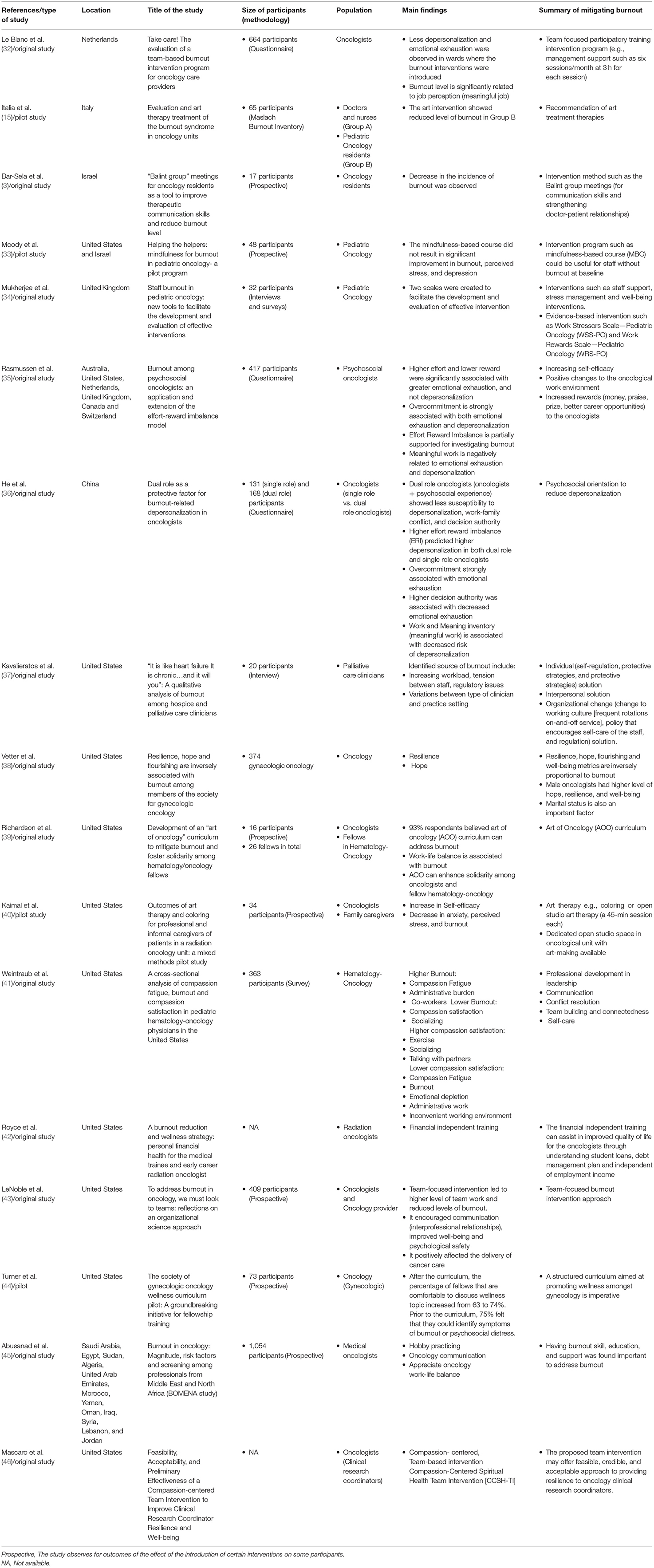
Table 1. The main findings from the included studies.
Quality Appraisal
The preliminary quality appraisal was done using the quality guideline for systematic review as recommended by the National Institute of Health Quality Assessment tools (47). The included studies in this review were subjected to four quality criteria informed by a similar study that used the same quality assessment tool (48). These criteria were modified to include design, methodology, interventions, and statistical analysis (Supplementary Table 1). The studies that showed reasonable quality (≥50%) were further subjected to the main quality assessment using the Agency for Health Research and Quality (AHRQ) tool. The AHRQ quality assessment tool was chosen as this scoping review aims at identifying means of burnout mitigation in oncology. The AHRQ has a total of 11 items for the methodological quality assessment (Supplementary Table 1) (49). The AHRQ has been scaled with score 0 for “NO” and “Unclear” and score 1 for “Yes.” An overall score of >8 indicated a “high” quality. Conversely, an AHRQ score between four and seven was defined as “medium” while a score of <4 was defined as “low” quality (49, 50). The score disagreements were resolved by consensus discussion between the two independent reviewers (RA and OY). The result of the quality assessment is presented in Table 2.
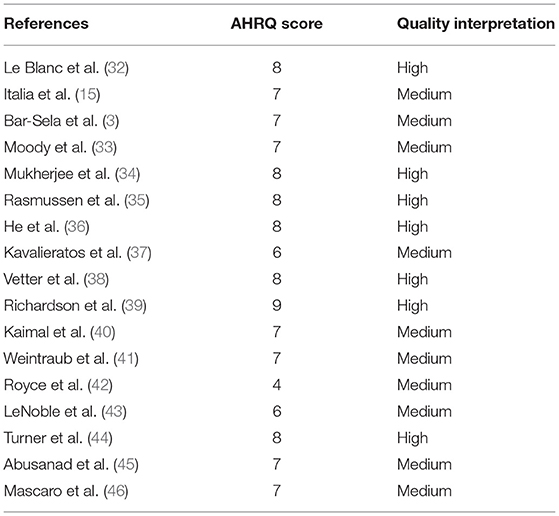
Table 2. Summary of quality assessment.
Data Extraction
In each eligible study, the name of the first author, year of publication, country, the title of studies, results of the interventions, and summary of the strategies to address burnout in oncology were extracted (Table 1). A detailed explanation of the strategic interventions to mitigating burnout in oncology was discussed collectively in the discussion section.
Results
Results of the Database Search
The selection of eligible studies for this study is presented with the PRISMA flowchart (Figure 1). A total of 2015 hits were retrieved. After deleting duplicates (N = 386), irrelevant papers (N = 580), and exclusions (N = 915), we found 17 studies eligible to be included in this scoping review as shown in Figure 1 (3, 15, 32–46).
Characteristics of Relevant Studies
All the articles included were published in the English language. Of the 17 included studies, 9 (52.9%) studies were conducted only in the United States (37–44, 46), 3 (17.6%) studies carried out in Europe (15, 32, 34), 2 (11.8%) studies each from Asia (3, 36), and 3 (17.6%) studies were from the international multicenter (33, 35, 45). From the included studies, 6 (35.3%) studies recommended individual interventions (how to address burnout) that include self-efficacy, self-regulation, and protective strategies for the oncologists (35–38, 41, 45). Furthermore, in addition to the individual intervention, 12 (70.5%) studies suggested organizational interventions that include organizing team-based participatory training such as group meetings, staff support, review policies, positive changes to the working environment, leadership and communication skills training for the staff, stress management, psychosocial education (mindfulness-based course, career development, resiliency training, and conflict resolution), motivational and encouragement (reward, prizes, and appreciation of efforts), and art treatment therapies (3, 15, 32–37, 39, 43, 44, 46) (summarized in Table 1). In terms of the quality assessment of the included studies, 7 (41.2%) of the included studies showed high-quality assessment scores. Conversely, 10 (58.8%) of the included studies were of medium-quality scores study (Table 2).
Summary of the Findings From the Studies
The findings of these studies (summarized in Table 1) indicated that burnout is a substantial issue associated with oncology as a medical profession. The included articles contained several recommendations of interventions that could serve as the impetus for addressing and mitigating burnout in the oncological ward. These interventions were broadly categorized into seven divisions: individual, organizational, educational, art and entertainment, team-based, motivational, and disruptive technology. The risk factors found for the prevalence, expression, and manifestations of burnout in the oncological unit are presented in Figure 2 (Box 1).
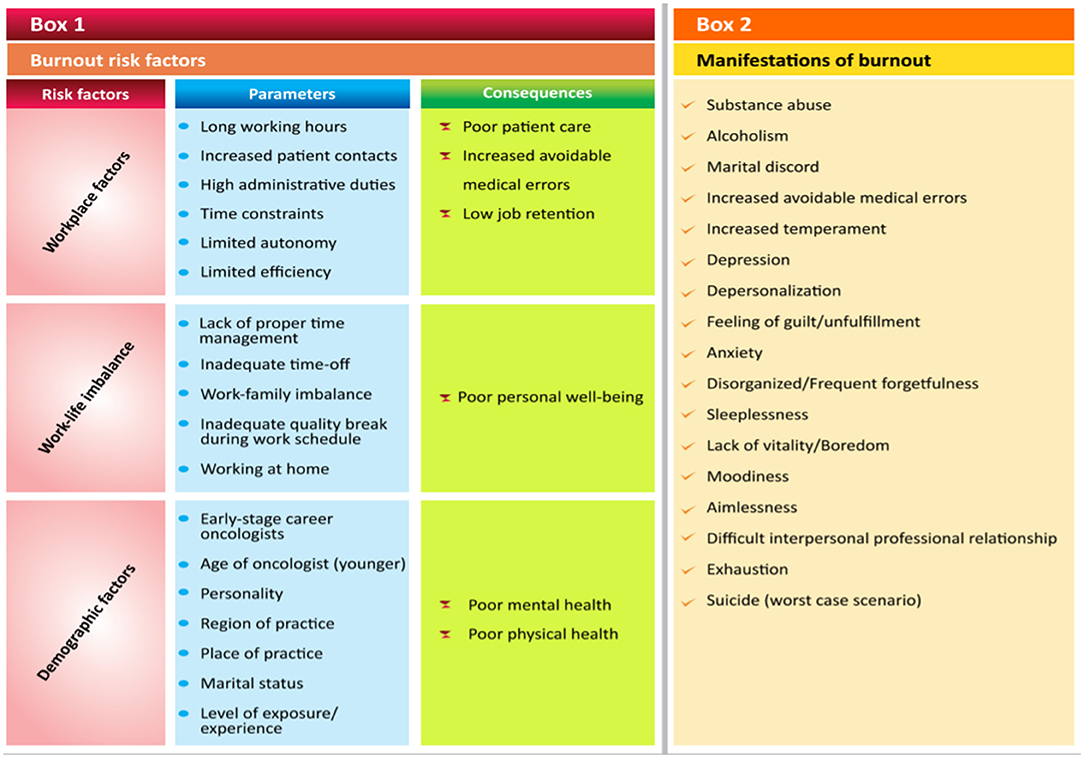
Figure 2. The prevalence, expression, and manifestations of burnout in the oncological unit.
The results also indicated that these interventions are poised to offer self-care, personal well-being (less depersonalization and emotional exhaustion), resilience and reduction to burnout, and job satisfaction and retention for the oncologists (3, 15, 32, 36, 39, 43). It was found that the burnout level is strongly associated with job satisfaction (32, 34). Considering the effort-reward imbalance model, higher efforts and a lower reward were reported to be associated with emotional exhaustion (35) and depersonalization (36). Meanwhile, overcommitment is strongly linked to both emotional exhaustion and depersonalization (35, 36). Having trained in psychosocial education was found to show a higher impact on work-family balance and reduce depersonalization (36). Similarly, creating a conducive working environment for meaningful work was associated with decreased risk of depersonalization (36).
Discussion
In this scoping review, we examined the published studies on how to address or mitigate burnout in oncology as a medical profession. In terms of prevalence, specifically in the United States, it was reported that around 62% of the oncologists have reported experiencing specific symptoms of this burdensome phenomenon called burnout. In Europe and Australia, it varies significantly, ranging from 52 to 78% (5). Thus, without proper measures to address and mitigate burnout in oncology, the pool of available resources for proper cancer management may not achieve the desired objectives due to stress, depression, burnout, and tragically even suicide among the oncologists.
The stressor that causes burnout can be generic, work-related stressors such as monotonous, wearisome and unexciting tasks, significant workload, and poor interpersonal relationships with colleagues (34). In addition, excessive interruptions, meaningless documentation and regulatory specifications, cumbersome electronic health record (EHR) systems, and increasing pressure on the oncologists to attend to more patients without consideration on quality and oncologists-patients relationships are posited to putting the oncologists in morally compromising situations (51). Thus, increasing the possibility of stress and burnout (51). Also, there are job-specific stressors that are inherent to each job such as oncology (34, 52). An example of such stressors includes administering and managing complex treatment regimens for patients with cancer. Several work-related stressors in oncological settings have been published (27, 32, 53). Overcommitment has also posed as an individual stressor that is capable of causing emotional exhaustion and depersonalization which may eventually lead to burnout (35, 36).
Therefore, from the aforementioned, it becomes a shared responsibility between the oncologists and the organizations where they work to be determined in their approach toward reducing burnout and further cultivate resilience and career satisfaction (5, 54–56). This means that effective interventions that are poised to address and mitigate burnout may require that it is multifaceted, i.e., addressing organizational and personnel stressors that lead to burnout (33, 57). That is, individual oncologists are expected to identify burnout in themselves and their colleagues (5, 58). Similarly, organizations should be ready to offer systematic interventions (5, 58, 59).
Individual interventions for oncologists include self-efficacy, self-regulation, and protective strategies against stress and burnout (35–37, 41). However, the lack of confidentiality, stigmatization, and the trepidation of professional repercussions are some of the factors affecting medical staff such as the oncologists from help-seeking attempts on challenges such as behavioral health issues (burnout, depression, and suicide) (60). Therefore, the need for an inflection point to transparent and appropriate help-seeking behavior from the oncologists to address behavioral health issues such as burnout becomes imperative (60). To this end, the organization should provide the necessary help-seeking platforms and staff support (including psychological and bereavement support, working hours limitation, resiliency training, and team role clarifications) to avoid burnout (34).
Furthermore, it is important for organizations to carefully and critically develop an evidence-based and appropriate type of training for medical team leaders (24). It has been reported that good leadership skills and qualities are capable of reducing burnout, increases staff well-being, and position the organization in which they function for success (24). Also, the cordial relationship between the staff and their team leader or supervisor is a critical aspect of professional satisfaction (61). Therefore, the leadership types, skills, and qualities have a significant impact on well-being, degree of burnout, and professional satisfaction (24). The organizational factors that impact well-being include the nature of the practice environment (work-life balance), the level of autonomy offered to the staff, and the amount of workload assigned to the staff (54–56, 62). These interventions can replete oncologists and offset their emotional exhaustion (33).
Team-based interaction and group meetings improve communication skills, keep the team members informed, engage them through sharing ideas for improvements in their practice environments, discussions about career development, and provides constructive feedback to team members (24). Likewise, organizational interventions in the form of education, training, and short-term courses such as stress management, psychosocial education, mindfulness-based course, and conflict-resolution training. However, the level of stress and burnout within the oncological unit should be accessed before the introduction of any course or training for optimum results (33, 34). Similarly, the courses and training should be carefully structured to avoid adding another stress to the already busy professional schedule of the oncologists (33).
The use of context-specific measures to access work-related stressors and rewards as the reliance on generic measures may provide an incomplete picture of the level of stress among staff (34, 52). Thereby, this might lead to a recommendation of inappropriate burnout interventions. An example of the widely used measure is the effort-reward imbalance model. Of note, effort corresponds to the obligations and responsibilities that the employee is saddled with, while the rewards are not necessarily financial but may include esteem (respect), prizes and awards, job well-done appreciation, job security, and career opportunities and progression (34, 35). Thus, higher efforts and lower reward are strongly associated with emotional exhaustion (35) and both emotional exhaustion and depersonalization (36). Though, overcommitment predicts both emotional exhaustion and depersonalization. This is because, overcommitted individuals have a set of attitudes, behaviors, and emotions that make them strive to be approved (35, 63). To this end, they are usually prone to stress and burnout (35, 64).
It has been reported that the use of art treatment therapies in the form of coloring, dedicated open art studio with therapeutic support within the oncological unit, psychodrama, and relaxation increase the oncologist in self-care and decreases anxiety, perceived stress, and burnout in both oncologist and family caregivers (15, 40). Interestingly, participants with interest (or experience) in art-making were found to benefit more from this intervention (40). The motive behind the art-making intervention is to shift the attention of the stressed personnel away from their worries (40). Therefore, this brings to mind that various interventions should be offered on a personal level. This is because people benefit from different types of these interventions.
Although burnout and stress shared almost similar symptomatology, they are however different concepts. While stress is short-term and disappears once the situation becomes conducive, burnout is a long-term and complex phenomenon that gradually develops over an extended period of time (9, 65). Of note, untreated and unaddressed burnout may lead to personal chronic health consequences such as heart disease, stroke, obesity, or mental health consequences such as depressions, anxiety, substance and chemical use, and suicide (1, 66–71). Professionally, it may lead to reduced professional accomplishment and satisfaction (1, 66). Other closely related concepts (but with overlapping features) such as compassion fatigue, moral distress, and empathy fatigue captured different aspects of burnout (5). In general, this study provides background information for further research in this field, especially in surgical oncology.
Artificial Intelligence as an Intervention to Mitigate Burnout in Oncology
With advancements in technology, the application of AI in medicine continues to grow significantly. In terms of mitigating burnout, AI is thought to be poised to offer a potential to mitigate burnout in oncology by enhancing the productivity and performance of the oncologists, reduce the workload and provide job satisfaction, and foster teamwork between the caregivers of patients with cancer (72).
There are arrays of studies that have been published regarding the potential of machine learning and AI for the prognostication of cancer which suggested that the performance and productivity of oncologists can be improved (72). For example, the prediction of recurrences and overall survival (73–75). Thus, AI technology such as deep learning is poised to enhance precision medicine (76–79) and improved clinical decisions (73, 74). With the improved clinical decisions, the oncologists may experience emotional satisfaction, reduced depersonalization, and increased professional efficacy. Hence, the it offers the potential to increase job satisfaction and reduce burnout of oncologists (80, 81).
In addition, the high workload has been reported as an important factor that contributes to occupational stress (82, 83). This has a negative effect on the quality of care offered to the patients. It has been reported that administrative tasks contribute to the workload of clinicians and significantly limit the time for direct clinical face time between the clinicians and patients (84). For example, it was found that physicians spend 49% of their work time on administrative tasks (desk work and EHRs) and 33% of their work time on direct clinicians-patient interaction (84). Thus, AI has been touted to significantly reduce this administrative burden (72).
Natural language processing, a branch of AI offers the potential for detailed and informative summarization of EHRs. It offers cognitive systems that can interpret, augment, and transform free text contained in the EHR and clinical notes in a format that can be represented for computation (85). This might be an instrument to reduce the workload and stress for the oncologists in terms of the onerous tasks of navigating and engagement with the EHR. With the aid of natural language processing, the structured data fields can be autopopulated from the notes of clinicians (72). Similarly, it can assist in the proper querying of relevant data of patients and transcribe past patient encounters. For example, it was reported that transcription (voice-to-text) can enhance work time savings of 17% for doctors (72).
Finally, the use of AI may aid through the optimized billing codes, and quality outcome reporting for hospital records and regulatory purposes (85). It also has the potential to integrate unstructured and structured data from different sources (72). This provides more cohesive, faster, and convenient access to information of patients across the multidisciplinary team in the oncological unit. This can greatly foster teamwork, easy collaboration, strong communication for shared decision making, and coordinated actions on the evaluation of the progress of the patients by the caregivers of patients with cancer (72). Therefore, the aforementioned benefits of AI intervention have the potential to further reduce workload and create a relaxed working environment for the oncologist and thus avoid stress. With these AI-based interventions, the oncologists may be well-positioned to perform with greater efficiency, engagement, and effectiveness (85).
Conclusion
In conclusion, many oncological wards would have to deal with increasing admission of patients with cancer. This might be even more emphasized due to the recent outbreak of coronavirus pandemic. It is expected that work will become increasingly stressful and the possibility of burnout remains high. Therefore, healthcare management should recognize and seek to address this problem in oncology. Finding ways to ameliorate burnout is important for creating a conducive working environment for oncologists and to increase the well-being of oncologists and reduce medical errors. The interventions presented in this study will not achieve the required touted objectives without recognition of burnout as a problem by the healthcare institutions and professional bodies. This ensures that individual interventions are considered important, and consequently combinatorial strategies that include other interventions presented in this study offer the most viable hope to mitigating burnout among oncologists and positively affect the delivery of cancer care.
Clinical Implications
The physical and emotional well-being of the clinical oncologists is important to enhance the quality of care, patient satisfaction, and overall success of the organizations where the oncologists work (5). The physical and mental distress resulting from burnout adversely affects clinical oncologists-patients relationships (51), poorer patient outcomes (40), increases inefficacy, errors, chronic health conditions, and decreased productivity of the clinical oncologists (5, 51). Consequently, their personal engagements outside work such as family life and lifestyles are usually affected (5, 13). Due to the increasing prevalence of burnout in oncology, some of the oncologists have tragically left their practice or retired early (after decades of specialized training) (86, 87) or even committed suicide in some cases (60). Thereby, an increasing shortage of oncologists is evident. Based on these implications, the oncologists need to recognize the stress and burnout symptoms, acquire mindfulness training, learn resilience and cognitive-behavioral psychotherapy skills, reiterate their professional objectives, and improve communications and interpersonal skills to ensure the quality of care offered to the patients. The burnout interventions listed in this study are targeted at effective wellness strategies for the clinical oncologists and to improve their professional environment.
Strength and Limitations
Strengths of this study include: (a) a systematic scoping review of all the published studies that have examined burnout intervention in clinical oncology. It maps the current state of research in this subject area (oncology medical profession) and aids in future planning of research; (b) these interventions were broadly categorized into seven divisions, namely, individual, organizational, educational, team-based, art and entertainment, motivational, and disruptive technology; and (c) furthermore, the possibility of disruptive technology such as AI and its subfield, machine learning as a possible intervention for addressing burnout in a medical profession was examined. There are certain limitations relating to this scoping review. First, the quality assessment score of all the included studies was not significantly high. Additionally, there are a few concerns about some of the interventions mentioned in the articles included in this study. Most of these interventions were thought of as those that were targeted at either oncologists (individuals) or the organization. Rarely were the interventions aimed at targeting both the oncologists and the organizations (88). Considering interventions (how to address burnout) that target both individuals and organizations may be pertinent for an effective burnout reduction strategy. Of note, it is important to include more participants (oncologists) in the evaluation of the benefits of these interventions to evaluate their efficacy. Moreover, some of these interventions require significant evidence-based support and strategies needed for institutions to introduce them to their organizational structures. Thus, it is important to avoid generalizing the reviewed interventions. Also, some challenges must be addressed by policymakers, healthcare providers, industry, and patients before AI can safely be used in an oncological unit.
Author Contributions
RA and AM: study concepts and study design. RA and OY: studies extraction. PH and AA: acquisition and quality control of included studies. RA, ME, AA, AM, and PH: data analysis and interpretation. RA, OY, AA, AM, and PH: manuscript preparation. AA, ME, and PH: manuscript review. AA, RA, and OY: manuscript editing. All authors approved the final manuscript for submission.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
We thank the Sigrid Jusélius Foundation, the Helsinki University Hospital Research Fund, the Turku University Hospital Fund, and the Helsinki University Hospital Research Fund.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2021.677915/full#supplementary-material
References
1. Shanafelt T, Dyrbye L. Oncologist burnout: causes, consequences, and responses. J Clin Oncol Off J Am Soc Clin Oncol. (2012) 30:1235–41. doi: 10.1200/JCO.2011.39.7380
2. Jaiswal A. Integrative Bioinformatics of Functional and Genomic Profiles for Cancer Systems Medicine, Finland: University of Helsinki (2018). p. 82.
3. Bar-Sela G, Lulav-Grinwald D, Mitnik I. Balint group” meetings for oncology residents as a tool to improve therapeutic communication skills and reduce burnout level. J Cancer Educ. (2012) 27:786–9. doi: 10.1007/s13187-012-0407-3
5. Hlubocky FJ, Back AL, Shanafelt TD. Addressing burnout in oncology: why cancer care clinicians are at risk, what individuals can do, and how organizations can respond. Am Soc Clin Oncol Educ Journal Am Soc Clin Oncol Annu Meet. (2016) 35:271–9. doi: 10.1200/EDBK_156120
6. Freudenberger HJ. Staff burn-out. J Soc Issues. (1974) 30:159–65. doi: 10.1111/j.1540-4560.1974.tb00706.x
7. Maslach C, Jackson S, Leiter M. Maslach Burnout Inventory Manual. 3rd ed. Palo Alto, CA: Consulting Psychologists Press (1996).
8. National Academy of Medicine. Validated Instruments to Assess Work-Related Dimensions of Well-Being. (2020). Available online at: https://nam.edu/valid-reliable-survey-instruments-measure-burnout-well-work-related-dimensions/ (accessed April 30, 2020).
9. Bährer-Kohler S. Burnout for Experts. Boston, MA: Springer US (2013). doi: 10.1007/978-1-4614-4391-9
10. World Health Organization. ICD-11 for Mortality and Morbidity Statistics, QD85 Burn-out. International Classification of Disease. (2019). Available online at: https://icd.who.int/browse11/l-m/en#/http://id.who.int/icd/entity/129180281 (accessed April 30, 2020).
12. Demerouti E, Bakker AB, Nachreiner F, Schaufeli WB. A model of burnout and life satisfaction amongst nurses. J Adv Nurs. (2000) 32:454–64. doi: 10.1046/j.1365-2648.2000.01496.x
13. Spickard A, Gabbe SG, Christensen JF. Mid-career burnout in generalist and specialist physicians. J Am Med Assoc. (2002) 288:1447–50. doi: 10.1001/jama.288.12.1447
14. Meier DE, Back AL, Morrison RS. The inner life of physicians and care of the seriously ill. J Am Med Assoc. (2001) 286:3007–14. doi: 10.1001/jama.286.23.3007
15. Italia SC, Favara-Scacco A, Di Cataldo A, Russo G. Evaluation and art therapy treatment of the burnout syndrome in oncology units. Psychooncology. (2008) 17:676–80. doi: 10.1002/pon.1293
16. Banerjee S, Califano R, Corral J, de Azambuja E, De Mattos-Arruda L, Guarneri V, et al. Professional burnout in European young oncologists: results of the European Society for Medical Oncology (ESMO) Young Oncologists Committee Burnout Survey. Ann Oncol Off J Eur Soc Med Oncol. (2017) 28:1590–6. doi: 10.1093/annonc/mdx196
17. Murali K, Makker V, Lynch J, Banerjee S. From burnout to resilence: an update for oncologists. Am Soc Clin Oncol Educ Journal. (2018) 38:862–72. doi: 10.1200/EDBK_201023
18. Murali K, Banerjee S. Burnout in oncologists is a serious issue: what can we do about it? Cancer Treat Rev. (2018) 68:55–61. doi: 10.1016/j.ctrv.2018.05.009
19. van Wyk BE, Pillay-Van Wyk V. Preventive staff-support interventions for health workers. In: The Cochrane Collaboration, editors, Cochrane Database Syst. Rev. Chichester: John Wiley & Sons, Ltd (2010). doi: 10.1002/14651858.CD003541.pub2
20. Shanafelt TD, Balch CM, Bechamps G, Russell T, Dyrbye L, Satele D, et al. Burnout and medical errors among American surgeons. Ann Surg. (2010) 251:995–1000. doi: 10.1097/SLA.0b013e3181bfdab3
21. West CP, Dyrbye LN, Erwin PJ, Shanafelt TD. Interventions to prevent and reduce physician burnout: a systematic review and meta-analysis. Lancet. (2016) 388:2272–81. doi: 10.1016/S0140-6736(16)31279-X
22. Haas JS, Cook EF, Puopolo AL, Burstin HR, Cleary PD, Brennan TA. Is the professional satisfaction of general internists associated with patient satisfaction? J Gen Intern Med. (2000) 15:122–8. doi: 10.1046/j.1525-1497.2000.02219.x
23. Girgis A, Hansen V, Goldstein D. Are Australian oncology health professionals burning out? A view from the trenches. Eur J Cancer. (2009) 45:393–9. doi: 10.1016/j.ejca.2008.09.029
24. Shanafelt TD, Gorringe G, Menaker R, Storz KA, Reeves D, Buskirk SJ, et al. Impact of organizational leadership on physician burnout and satisfaction. Mayo Clin Proc. (2015) 90:432–40. doi: 10.1016/j.mayocp.2015.01.012
25. Chiu SF, Tsai MC. Relationships among burnout, job involvement, and organizational citizenship behavior. J Psychol. (2006) 140:517–30. doi: 10.3200/JRLP.140.6.517-530
26. Grunfeld E, Whelan TJ, Zitzelsberger L, Willan AR, Montesanto B, Evans WK. Cancer care workers in Ontario: prevalence of burnout, job stress and job satisfaction. CMAJ Can Med Assoc J J Assoc Medicale Can. (2000) 163:166–9.
27. Ramirez AJ, Graham J, Richards MA, Cull A, Gregory WM, Leaning MS, et al. Burnout and psychiatric disorder among cancer clinicians. Br J Cancer. (1995) 71:1263–9. doi: 10.1038/bjc.1995.244
28. Creagan ET. Stress among medical oncologists: the phenomenon of burnout and a call to action. Mayo Clin Proc. (1993) 68:614–5. doi: 10.1016/S0025-6196(12)60378-4
29. Verghis S. Wounded Healers. (2018). Available online at: http://sharonverghis.com/stories/doctorsSuicide.html (accessed April 30, 2020).
30. Ramirez A, Graham J, Richards M, Timothy A. Stress at work for the clinical oncologist. Clin Oncol. (1996) 8:137–9. doi: 10.1016/S0936-6555(96)80036-7
31. University of South Australia. Apply Population, Concept, and Context (PCC). What PCC. (2021). Available online at: https://guides.library.unisa.edu.au/ScopingReviews (accessed August 24, 2021).
32. Le Blanc PM, Hox JJ, Schaufeli WB, Taris TW, Peeters MCW. Take care! The evaluation of a team-based burnout intervention program for oncology care providers. J Appl Psychol. (2007) 92:213–27. doi: 10.1037/0021-9010.92.1.213
33. Moody K, Kramer D, Santizo RO, Magro L, Wyshogrod D, Ambrosio J, et al. Helping the helpers: mindfulness training for burnout in pediatric oncology—a pilot program. J Pediatr Oncol Nurs. (2013) 30:275–84. doi: 10.1177/1043454213504497
34. Mukherjee S, Beresford B, Tennant A. Staff burnout in paediatric oncology: new tools to facilitate the development and evaluation of effective interventions. Eur J Cancer Care. (2014) 23:450–61. doi: 10.1111/ecc.12176
35. Rasmussen V, Turnell A, Butow P, Juraskova I, Kirsten L, Wiener L, et al. IPOS Research Committee, Burnout among psychosocial oncologists: an application and extension of the effort-reward imbalance model. Psychooncology. (2016) 25:194–202. doi: 10.1002/pon.3902
36. He Y, Pang Y, Zhang Y, Fielding R, Tang L. Dual role as a protective factor for burnout-related depersonalization in oncologists. Psychooncology. (2017) 26:1080–6. doi: 10.1002/pon.4425
37. Kavalieratos D, Siconolfi DE, Steinhauser KE, Bull J, Arnold RM, Swetz KM, et al. It is like heart failure. it is chronic … and it will kill you”: a qualitative analysis of burnout among hospice and palliative care clinicians. J Pain Symptom Manage. (2017) 53:901–10.e1. doi: 10.1016/j.jpainsymman.2016.12.337
38. Vetter MH, Vetter MK, Fowler J. Resilience, hope and flourishing are inversely associated with burnout among members of the Society for Gynecologic Oncology. Gynecol Oncol Rep. (2018) 25:52–5. doi: 10.1016/j.gore.2018.06.002
39. Richardson DR, Tan X, Winzelberg G, Rosenstein DL, Collichio FA. Development of an art of oncology curriculum to mitigate burnout and foster solidarity among hematology/oncology fellows. JCO Oncol Pract. (2020) 16:e384–94. doi: 10.1200/JOP.19.00529
40. Kaimal G, Carroll-Haskins K, Mensinger JL, Dieterich-Hartwell RM, Manders E, Levin WP. Outcomes of art therapy and coloring for professional and informal caregivers of patients in a radiation oncology unit: a mixed methods pilot study. Eur J Oncol Nurs. (2019) 42:153–61. doi: 10.1016/j.ejon.2019.08.006
41. Weintraub AS, Sarosi A, Goldberg E, Waldman ED. A cross-sectional analysis of compassion fatigue, burnout, and compassion satisfaction in pediatric hematology-oncology physicians in the United States. J Pediatr Hematol Oncol. (2020) 42:e50–5. doi: 10.1097/MPH.0000000000001548
42. Royce TJ, Davenport KT, Dahle JM. A burnout reduction and wellness strategy: personal financial health for the medical trainee and early career radiation oncologist. Pract Radiat Oncol. (2019) 9:231–8. doi: 10.1016/j.prro.2019.02.015
43. LeNoble CA, Pegram R, Shuffler ML, Fuqua T, Wiper DW. To address burnout in oncology, we must look to teams: reflections on an organizational science approach. JCO Oncol Pract. (2020) 16:e377–83. doi: 10.1200/JOP.19.00631
44. Turner TB, Kushner DM, Winkel AF, McGwin G, Blank SV, Fowler JM, et al. The Society of Gynecologic Oncology wellness curriculum pilot: a groundbreaking initiative for fellowship training. Gynecol Oncol. (2020) 156:710–4. doi: 10.1016/j.ygyno.2019.12.005
45. Abusanad A, Bensalem A, Shash E, Mula-Hussain L, Benbrahim Z, Khatib S, et al. Burnout in oncology: magnitude, risk factors and screening among professionals from Middle East and North Africa (BOMENA study). Psychooncology. (2021) 30:736–46. doi: 10.1002/pon.5624
46. Mascaro JS, Palmer PK, Ash MJ, Peacock C, Sharma A, Escoffery C, et al. Feasibility, acceptability, and preliminary effectiveness of a compassion-centered team intervention to improve clinical research coordinator resilience and well-being. JCO Oncol Pract. (2021) 17:e936–46. doi: 10.1200/OP.21.00120
47. National Institute of Health. Study quality assessment tools, United States. (2020). Available online at: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools (accessed May 13, 2020).
48. Phillips CS, Becker H. Systematic Review: expressive arts interventions to address psychosocial stress in healthcare workers. J Adv Nurs. (2019) 75:2285–98. doi: 10.1111/jan.14043
49. Rostom A, Dubé C, Cranney A, Saloojee N, Sy R, Garritty C, et al. Celiac disease. Evid Rep Technol Assess. Jun (2004) 104:1–6.
50. Xie W, Wang J, Zhang Y, Zuo M, Kang H, Tang P, et al. The levels, prevalence and related factors of compassion fatigue among oncology nurses: a systematic review and meta-analysis. J Clin Nurs. (2021) 30:615–32. doi: 10.1111/jocn.15565
51. Hlubocky FJ, Rose M, Epstein RM. Mastering resilience in oncology: learn to thrive in the face of burnout. Am Soc Clin Oncol Educ Journal Am Soc Clin Oncol Annu Meet. (2017) 37:771–81. doi: 10.1200/EDBK_173874
52. Demerouti E, Bakker AB. The job demands–resources model: challenges for future research. SA J Ind Psychol. (2011) 37:974. doi: 10.4102/sajip.v37i2.974
53. Shanafelt TD, Novotny P, Johnson ME, Zhao X, Steensma DP, Lacy MQ, et al. The well-being and personal wellness promotion strategies of medical oncologists in the north central cancer treatment group. Oncology. (2005) 68:23–32. doi: 10.1159/000084519
54. Shanafelt TD, Sloan JA, Habermann TM. The well-being of physicians. Am J Med. (2003) 114:513–9. doi: 10.1016/S0002-9343(03)00117-7
55. Shanafelt TD. Enhancing meaning in work: a prescription for preventing physician burnout and promoting patient-centered care. J Am Med Assoc. (2009) 302:1338. doi: 10.1001/jama.2009.1385
56. Egener B, McDonald W, Rosof B, Gullen D. Perspective: organizational professionalism. Acad Med. (2012) 87:668–74. doi: 10.1097/ACM.0b013e31824d4b67
57. Cox T, Griffiths A, Barlowe C, Randall R, Rial-Gonzalez E. Organisational Interventions for Work Stress: A Risk Management Approach. Norwich: HSE Journals (2020).
58. Hlubocky FJ, Taylor LP, Marron JM, Spence RA, McGinnis MM, Brown RF, et al. A call to action: ethics committee roundtable recommendations for addressing burnout and moral distress in oncology. JCO Oncol Pract. (2020) 16:191–9. doi: 10.1200/JOP.19.00806
59. Hlubocky FJ, Shanafelt TD, Back AL, Paice JA, Tetzlaff ED, Friese CR, et al. Creating a blueprint of well-being in oncology: an approach for addressing burnout from ASCO's clinician well-being taskforce. Am Soc Clin Oncol Educ Journal. (2021) 2021:e339–53. doi: 10.1200/EDBK_320873
60. Nagy C, Schwabe D, Jones W, Brown A, Shupe M, Mancone A, et al. Time to talk about it: physician depression and suicide” video/discussion session for interns, residents, and fellows. J Teach Learn Resour. (2016) 12:10508. doi: 10.15766/mep_2374-8265.10508
61. Demmy TL, Kivlahan C, Stone TT, Teague L, Sapienza P. Physicians' perceptions of institutional and leadership factors influencing their job satisfaction at one academic medical center. Acad Med. (2002) 77:1235–40. doi: 10.1097/00001888-200212000-00020
62. Wallace JE, Lemaire JB, Ghali WA. Physician wellness: a missing quality indicator. Lancet. (2009) 374:1714–21. doi: 10.1016/S0140-6736(09)61424-0
63. van Vegchel N, de Jonge J, Meijer T, Hamers JPH. Different effort constructs and effort-reward imbalance: effects on employee well-being in ancillary health care workers. J Adv Nurs. (2001) 34:128–36. doi: 10.1046/j.1365-2648.2001.3411726.x
64. Bakker AB, Killmer CH, Siegrist J, Schaufeli WB. Effort-reward imbalance and burnout among nurses. J Adv Nurs. (2000) 31:884–91. doi: 10.1046/j.1365-2648.2000.01361.x
65. Schaufeli WB, Leiter MP, Maslach C. Burnout: 35 years of research and practice. Career Dev Int. (2009) 14:204–20. doi: 10.1108/13620430910966406
66. Shanafelt TD, Raymond M, Kosty M, Satele D, Horn L, Pippen J, et al. Satisfaction with work-life balance and the career and retirement plans of US oncologists. J Clin Oncol. (2014) 32:1127–35. doi: 10.1200/JCO.2013.53.4560
67. Alarcon G, Eschleman KJ, Bowling NA. Relationships between personality variables and burnout: a meta-analysis. Work Stress. (2009) 23:244–63. doi: 10.1080/02678370903282600
68. Shanafelt TD, Bradley KA, Wipf JE, Back AL. Burnout and self-reported patient care in an internal medicine residency program. Ann Intern Med. (2002) 136:358. doi: 10.7326/0003-4819-136-5-200203050-00008
69. Shanafelt TD. Special report: suicidal ideation among American surgeons. Arch Surg. (2011) 146:54. doi: 10.1001/archsurg.2010.292
70. Oreskovich MR, Shanafelt T, Dyrbye LN, Tan L, Sotile W, Satele D, et al. The prevalence of substance use disorders in American physicians: the prevalence of substance use disorders in American. Am J Addict. (2015) 24:30–8. doi: 10.1111/ajad.12173
71. Tyssen R, Hem E, Vaglum PN, Grønvold T, Ekeberg Ø. The process of suicidal planning among medical doctors: predictors in a longitudinal Norwegian sample. J Affect Disord. (2004) 80:191–8. doi: 10.1016/S0165-0327(03)00091-0
72. Hazarika I. Artificial intelligence: opportunities and implications for the health workforce. Int Health. (2020) 12:241–5. doi: 10.1093/inthealth/ihaa007
73. Alabi RO, Elmusrati M, Sawazaki-Calone I, Kowalski LP, Haglund C, Coletta RD, et al. Machine learning application for prediction of locoregional recurrences in early oral tongue cancer: a Web-based prognostic tool. Virchows Arch. (2019) 475:489–97. doi: 10.1007/s00428-019-02642-5
74. Alabi RO, Elmusrati M, Sawazaki-Calone I, Kowalski LP, Haglund C, Coletta RD, et al. Comparison of supervised machine learning classification techniques in prediction of locoregional recurrences in early oral tongue cancer. Int J Med Inf. (2019) 2019:104068. doi: 10.1016/j.ijmedinf.2019.104068
75. Karadaghy OA, Shew M, New J, Bur AM. Development and assessment of a machine learning model to help predict survival among patients with oral squamous cell carcinoma. J Am Med Assoc Otolaryngol Neck Surg. (2019) 145:1115. doi: 10.1001/jamaoto.2019.0981
76. Fröhlich H, Balling R, Beerenwinkel N, Kohlbacher O, Kumar S, Lengauer T, et al. From hype to reality: data science enabling personalized medicine. BMC Med. (2018) 16:7. doi: 10.1186/s12916-018-1122-7
77. Shrager J, Tenenbaum JM. Rapid learning for precision oncology. Nat Rev Clin Oncol. (2014) 11:109–18. doi: 10.1038/nrclinonc.2013.244
78. J.-Bibault E, Giraud P, Burgun A. Big Data and machine learning in radiation oncology: state of the art and future prospects. Cancer Lett. (2016) 382:110–7. doi: 10.1016/j.canlet.2016.05.033
79. Ding MQ, Chen L, Cooper GF, Young JD, Lu X. Precision oncology beyond targeted therapy: combining omics data with machine learning matches the majority of cancer cells to effective therapeutics. Mol Cancer Res. (2018) 16:269–78. doi: 10.1158/1541-7786.MCR-17-0378
80. Zakhem GA, Motosko CC, Ho RS. How should artificial intelligence screen for skin cancer and deliver diagnostic predictions to patients? J Am Med Assoc Dermatol. (2018) 154:1383. doi: 10.1001/jamadermatol.2018.2714
81. Murali K, Banerjee S. Let's address burnout in oncologists and reimagine the way we work. Nat Rev Clin Oncol. (2019) 16:1–2. doi: 10.1038/s41571-018-0097-9
82. Marine A, Ruotsalainen JH, Serra C, Verbeek JH. Preventing occupational stress in healthcare workers. In: The Cochrane Collaboration, editors, Cochrane Database Syst. Rev. Chichester: John Wiley & Sons, Ltd (2006). doi: 10.1002/14651858.CD002892.pub2
83. Nieuwenhuijsen K, Bruinvels D, Frings-Dresen M. Psychosocial work environment and stress-related disorders, a systematic review. Occup Med. (2010) 60:277–86. doi: 10.1093/occmed/kqq081
84. Erickson SM, Rockwern B, Koltov M, McLean RM, Medical Practice and Quality Committee of the American College of Physicians. Putting patients first by reducing administrative tasks in health care: a position paper of the American College of Physicians. Ann Intern Med. (2017) 166:659. doi: 10.7326/M16-2697
85. Haddad TC. Artificial Intelligence as a solution to burnout in oncology. Artif Intell Oncol Curr Appl Future Dir. (2019). Available online at: https://www.cancernetwork.com/view/artificial-intelligence-oncology-current-applications-and-future-directions (accessed July 15, 2020).
86. Balch CM, Copeland E. Stress and burnout among surgical oncologists: a call for personal wellness and a supportive workplace environment. Ann Surg Oncol. (2007) 14:3029–32. doi: 10.1245/s10434-007-9588-0
87. Campbell DA, Sonnad SS, Eckhauser FE, Campbell KK, Greenfield LJ. Burnout among American surgeons. Surgery. (2001) 130:696–705. doi: 10.1067/msy.2001.116676
Keywords: burnout—professional, mitigate, compassion fatigue, address, job satisfaction, oncology, artificial intelligence, stress
Citation: Alabi RO, Hietanen P, Elmusrati M, Youssef O, Almangush A and Mäkitie AA (2021) Mitigating Burnout in an Oncological Unit: A Scoping Review. Front. Public Health 9:677915. doi: 10.3389/fpubh.2021.677915
Received: 08 March 2021; Accepted: 24 August 2021;
Published: 01 October 2021.
Edited by:
Caterina Ledda, University of Catania, ItalyReviewed by:
Michele Teodoro, University of Messina, ItalyDelia Virga, West University of Timișoara, Romania
Copyright © 2021 Alabi, Hietanen, Elmusrati, Youssef, Almangush and Mäkitie. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Rasheed Omobolaji Alabi, cmFzaGVlZC5hbGFiaUBoZWxzaW5raS5maQ==