 Chunhong Shao
Chunhong Shao Wei Wang2
Wei Wang2 Meijie Jiang
Meijie Jiang
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health, 20 May 2021
Sec. Infectious Diseases – Surveillance, Prevention and Treatment
Volume 9 - 2021 | https://doi.org/10.3389/fpubh.2021.669173
This article is part of the Research TopicInfectious Disease Surveillance: Applying Cooperative Research to Recent Outbreaks including COVID-19View all 50 articles
Infection by carbapenem-resistant Klebsiella pneumoniae (CRKp) hampers the treatment of elderly patients with lower respiratory tract infection (LRTI); however, relevant data with respect to the characteristics of CRKp in elderly patients with LRTIs are limited. In the present study, K. pneumoniae isolated from elderly patients with LRTIs was collected and identified by VITEK-MS. VITEK 2 compact was used for drug sensitivity test to screen CRKps, and broth dilution method was used for drug sensitivity of tigecycline and colistin. The resistance genes, virulence genes, and serotypes of CRKps were detected via polymerase chain reaction. The homology of CRKps was analyzed via PFGE and MLST. Moreover, plasmid conjugation experiment was carried out to determine the transferability of carbapenem resistance. PCR-based replicon typing (PBRT) and S1 nuclease-PFGE were conducted for plasmid profiling. From January 2019 to August 2019, 258 elderly patients with LRTIs caused by K. pneumoniae were observed; of these, 31 (12.02%) infections were caused by CRKp strains. Majority of the patients were admitted to the intensive care unit and neurosurgery wards. Intracranial hemorrhage and pneumonia were the most common underlying diseases. Furthermore, 29 patients infected by CRKp had been exposed to various antimicrobial drugs before the positive culture. All isolates exhibited high resistance to β-lactam antibiotics. The predominant carbapenem resistance gene was blaKPC−2, and CRKps carrying blaKPC−2 were all ST11 type. Two blaNDM−5 carrying isolates were assigned to ST307 and ST1562, respectively. Conjugative assays revealed that plasmids harboring blaNDM−5 gene were self-transmissible. Plasmid analysis suggested that two blaNDM−5 were located on a ~45 kb IncX3 type plasmid. The high incidence of CRKp in elderly patients with LRTIs indicates the urgent need for further surveillance and strict infection control measures.
Carbapenem-resistant Enterobacteriaceae (CRE) presents an urgent public health concern worldwide due to rapidly rising resistance rates and subsequent high mortality. Report from China CRE Network revealed that most CRE cases were caused by Klebsiella pneumoniae (73.9%) (1). K. pneumoniae is a common causative pathogen of various nosocomial infections, including pneumonia, urinary tract infection, abdominal infection, and bacteremia. Despite improvements in hospital infection control and antimicrobial scientific stewardship, carbapenem-resistant K. pneumoniae (CRKp) is still on the rise (2, 3). Surveillance of antibiotic resistance by CHINET in China revealed that 3.0 and 2.9% of Klebsiella spp. were resistant to imipenem and meropenem, respectively, in 2005, compared to 25.3 and 26.8%, respectively, in 2019 (http://chinets.com/Data/GermYear). This antibiotic resistance poses a greater challenge in clinical treatment of infection caused by CRKp.
Lower respiratory tract infections (LRTIs) are a leading cause of mortality and morbidity worldwide (4). Community- or hospital-acquired LRTIs are highly prevalent in the elderly. In developing countries, the situation is more complicated, and management is often difficult due to the identification of etiological agents and administration of an appropriate treatment in cases requiring antibiotic therapy. K. pneumoniae is an important pathogen causing LRTIs in the elderly (5). A report from China CRE Network revealed that 65.4% of the CRE patients presented LRTIs, and it is more serious in the elderly (1). Infection by CRKp makes the treatment of elderly patients with LRTIs face greater challenges.
Although CRKp has led to wide global disseminations and serious clinical outcomes, limited data is available on the molecular epidemiology of this pathogen in elderly patients with LRTIs. Therefore, we conducted this study to investigate the resistance profiles, molecular epidemiology, and clinical characteristics of CRKp isolates obtained from elderly patients with LRTIs.
K. pneumoniae strains were collected from lower respiratory tract specimens, including bronchoalveolar lavage fluid, sputum, and pleural effusion, obtained from individual elderly patients (age ≥ 60 years) admitted to Taian City Central Hospital in China from January 2019 to August 2019. Elderly patients who presented at least two of the following symptoms were included in the study: fever, cough, dyspnoea, wheezing, chest pain, or sore throat. Any prior antimicrobial treatment taken by the patient was also recorded before microbiological investigations. Patients diagnosed with pulmonary tuberculosis or with infections other than LRTIs were excluded. Patient information including age, gender, diagnosis, treatment, and outcomes was obtained from the Electronic Medical Records. The methods in this study were approved by the Ethics Committee of Taian City Central Hospital and were carried out in accordance with the approved guidelines. The VITEK-MS (bioMérieux, France) was used to identify the bacterial strains. CRKp was defined as the minimal inhibition concentration (MIC) of ertapenem ≥2 μg/mL or the MIC of imipenem and meropenem ≥ 4 μg/mL (6). Only the first episode of CRKp-associated LRTIs was included.
Antimicrobial susceptibility testing was performed by VITEK 2 compact system using GN13 cards (bioMérieux, France) according to the manufacturer's instructions. The MICs of imipenem, meropenem, and ertapenem were determined by an E-test (bioMérieux); whereas, MICs of tigecycline and colistin were determined by broth microdilution method (Bio-kont, China). Escherichia coli ATCC25922 and K. pneumoniae ATCC700603 (American Type Culture Collection Center, Manassas, VA, USA) acted as the quality controls. All antibiotics were administered according to the 2019 European Committee on Antimicrobial Susceptibility Testing breakpoint (www.eucast.org/clinical_breakpoint). Susceptibility data were analyzed using WHONET 5.6 software recommended by the World Health Organization.
Samples were screened for the presence of carbapenem resistance genes (blaKPC, blaSME, blaIMI, blaNMC, blaGES, blaIMP, blaVIM, blaGIM, blaSIM, blaSPM, blaNDM, and blaOXA−48like), other β-lactamase genes (blaCTX−M, blaTEM, blaSHV, blaMOX, blaFOX, blaDHA, blaCIT, and blaEBC), and integron structures (Int1, Int2, Int3) (7, 8). For CRKp isolates that were resistant to quinolones or aminoglycoside, plasmid-mediated quinolone resistance genes [qnrA, qnrB, qnrC, qnrD, qnrS, qepA, and aac(6)-Ib-cr] or 16S rRNA methyase gene (rmtA, rmtB, rmtC, rmtD, npmA, and armA) were screened (9, 10). Primers used in the present study were listed in Supplementary Table 1.
The isolates were serotyped for serotypes K1, K2, K5, K20, K54, and K57, and moreover, 12 virulence-associated genes, including rmpA, aerobactin, wcaG, ybtA, iucB, iroNB, ureA, uge, kfuBC, fim, wabG, and allS, were screened using PCR as previously reported (11). Nucleotide sequences were analyzed and compared using BLAST (http://www.ncbi.nlm.nih.gov/blast).
An overnight bacterial culture was suspended in cell suspension buffer [100 mM EDTA, 100 mM Tris-HCl (pH 8.0)] and adjusted to an optical density of 4.0 at a wave length of 600 nm. The suspension was mixed with equal volumes 2% solution of low-melting agarose in Tris-EDTA [TE: 1 mM EDTA, 10 mM Tris-HCl (pH 8.0)]. After cooling, the agarose sections were incubated for 4 h at 54°C in cell lysis buffer [50 mM Tris-HCl, 50 mM EDTA (pH 8.0), 0.01 g/ml N-lauroyl-sarcosine, sodium salt, 0.1 mg/ml proteinase K]. Thereafter, the sections were washed thoroughly with TE buffer and digested overnight with XbaI restriction endonuclease (Takara Bio, Inc., Otsu, Japan). Genomic DNA was separated in 0.5× Tris/borate/EDTA (TBE) buffer in a PFGE system (CHEF Mapper; Bio-Rad Laboratories, Inc., Hercules, CA, USA) at 14°C, using a voltage of 6 V/cm, a switch angle of 120°, and a switch ramp of 6–36 s for 21 h.
MLST of K. pneumoniae was performed according to protocols available on the MLST Pasteur website (http://www.pasteur.fr/recherche/genopole/PF8/mlst/Kpneumoniae.html). Seven conserved housekeeping genes (gapA, infB, mdh, pgi, phoE, rpoB, and tonB) were amplified, sequenced, and compared with those in the MLST databases.
Conjugation was performed using the mixed broth method. Briefly, E. coli J53 AziR was used as the recipient strain and 31 clinical CRKps served as the donors. Transconjugants were selected on Mueller Hinton agar supplemented with meropenem (0.5 μg/mL) and sodium azide (100 μg/mL). The transconjugants were identified by VITEK-MS. Antimicrobial susceptibility test of the transconjugant was carried out as described for the clinical strain.
Plasmid incompatibility types of the transconjugants were identified via PCR-based replicon typing, as reported previously (8). The size and amount of plasmids carried by the 31 clinical isolates and transconjugants were evaluated using S1-pulsed-field gel electrophoresis (S1-PFGE), as previously described (12). The genome of Salmonella H9812 digested with XbaI was used as the marker.
From January 2019 to August 2019, 258 elderly patients with LRTIs caused by K. pneumoniae were observed; of these, 31 (12.02%) were caused by CRKp strains. The median age of 31 patients was 75.38 years (range: 60–92 years), and 58.06% (18/31) were male patients. Moreover, 13 patients (41.94 %) were hospitalized in the intensive care unit, and 9 patients in the neurosurgery ward. Intracranial hemorrhage and pneumonia were the most common underlying diseases. Furthermore, 22 (70.97%) patients received endotracheal intubation. The baseline clinical characteristics of the patients are presented in Table 1.
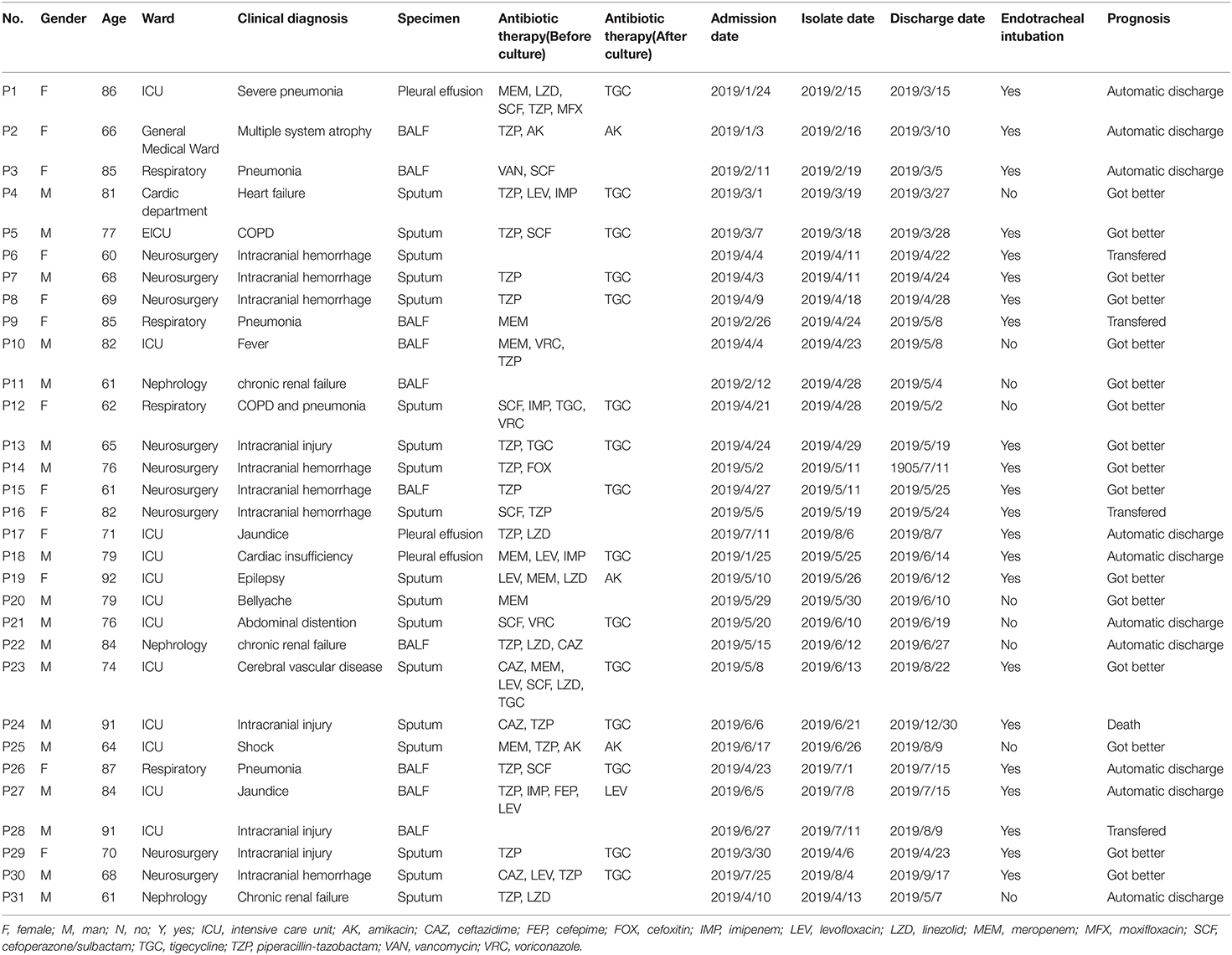
Table 1. Clinical characteristics of 31 elderly patients with LRTIs by CRKp.
Additionally, 29 patients were exposed to various antimicrobial drugs before the positive culture (Table 1). The main antibiotics used included β-lactam/β-lactamase inhibitor combinations, cephalosporins, carbapenems, quinolones, vancomycin, and linezolid. Based on in vitro susceptibility testing results, 80.65% (25/31) of the patients received inappropriate empirical treatment. Of these, 41.94% (13/31) switched to appropriate drugs such as tigecycline, levofloxacin, and amikacin after susceptibility results were available. Antimicrobial treatment adjustment and outcomes are presented in Table 1. Eventually, 16 patients improved, 14 patients were discharged automatically or transferred to other hospitals, and only one patient died.
The antimicrobial susceptibility profiles of the CRKp isolates are listed in Table 2. Only Kp22 was sensitive to aztreonam. Other isolates exhibited high resistance to cephalosporin, β-lactam/β-lactamase inhibitor combinations, and carbapenems. Kp27 was sensitive to levofloxacin and ciprofloxacin. The resistance rate of 31 isolates to gentamicin and amikacin was 19.35%. Among the 31 isolates, 27 strains (87.10%) were susceptible to trimethoprim-sulfamethoxazole and all isolates were susceptible to colistin and tigecycline (100%).
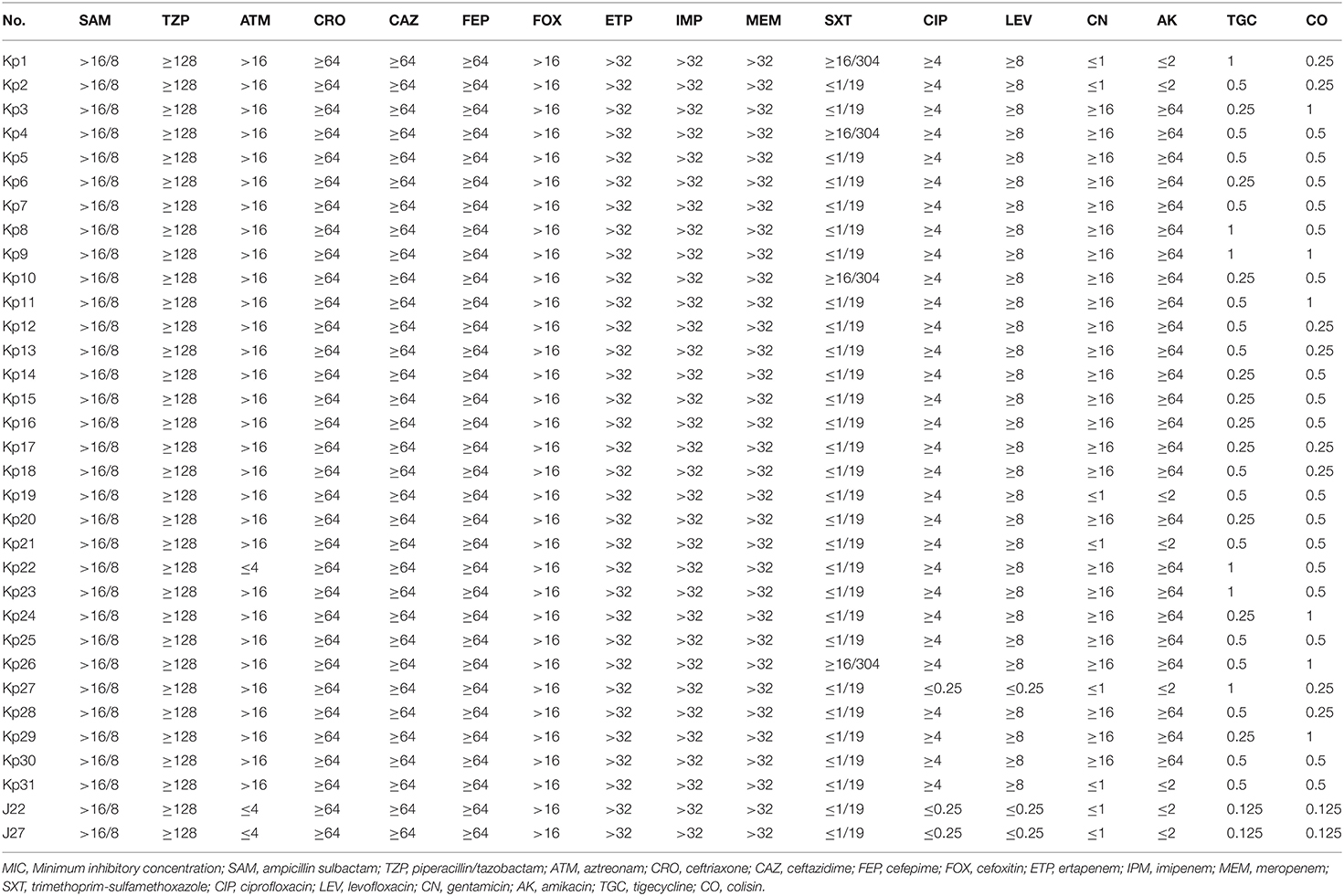
Table 2. The MIC of 31 CRKp isolates and two transconjugants (μg/mL).
The predominant carbapenem resistance gene was blaKPC−2 (93.55%, 29/31). Two isolates carried blaNDM−5. In addition to carbapenem resistance genes, we examined other types of β-lactamase genes, including ESBLs and AmpC genes. The distribution patterns of resistance genes in these strains are listed in Table 3. We identified blaTEM−1, blaSHV−1, and blaCTX−M−1group in 31 (100%), 28 (90.32%), and 27 (87.10%) isolates, respectively. Moreover, 30 isolates carried class I integron. Among the 25 aminoglycoside resistant CRKps, 23 isolates carried the rmtB gene, and Kp23 also carried armA. Kp3 and Kp9 carried only armA.
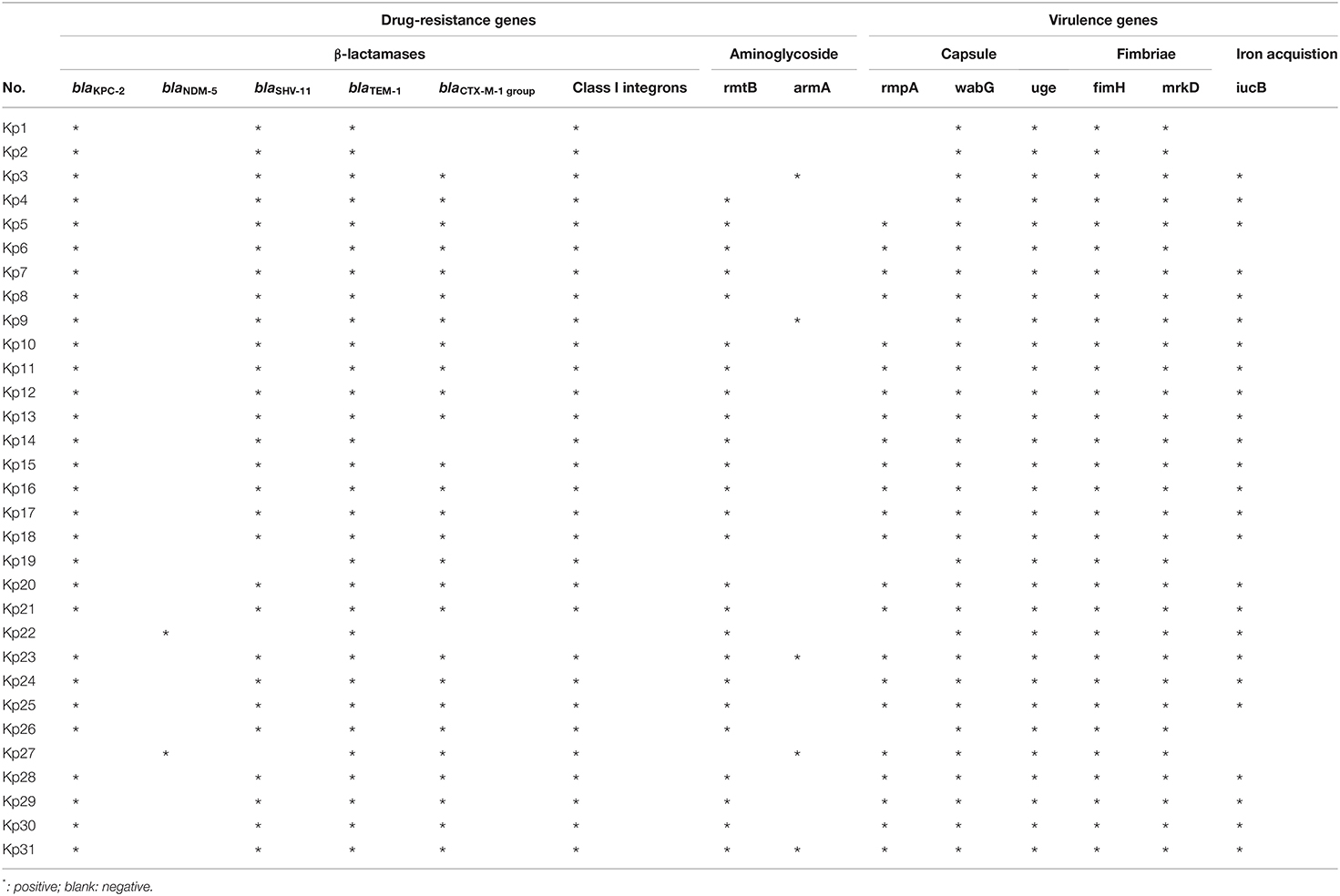
Table 3. The drug-resistance genes and virulence genes of 31 CRKp isolates.
The serotype and 12 virulence-associated genes of CRKp isolates were analyzed. For the six serotypes closely related to hypervirulent K. pneumoniae, all strains exhibited negative results. Among the 12 virulence-associated genes, fim, uge, mrkD, and wabG were harbored by all 31 isolates. In addition, rmpA and iucB were also harbored by 74.19% (23/31) and 80.65% (25/31) of the strains, respectively; however, the other six genes including, aerobactin, wcaG, ybtA, iroNB, ureA, kfuBC, and allS were not detected in any of the 31 isolates. The detailed results are listed in Table 3.
MLST analysis revealed that 29 CRKps carrying blaKPC−2 were ST11 type, which was the most common type of CRKp found in China. Moreover, blaNDM−5 carrying Kp22 and Kp27 was assigned to ST307 and ST1562, respectively. For PFGE, a cluster was defined as strains with homology >80%. The results revealed that the homology of 29 isolates of ST11 was more than 80%, indicating a cluster; however, no homology between the two strains carrying blaNDM−5 (Figure 1). Notably, the eight CRKps from neurosurgery, between April 6, 2019 and May 19, 2019, showed high homology (≥95%).
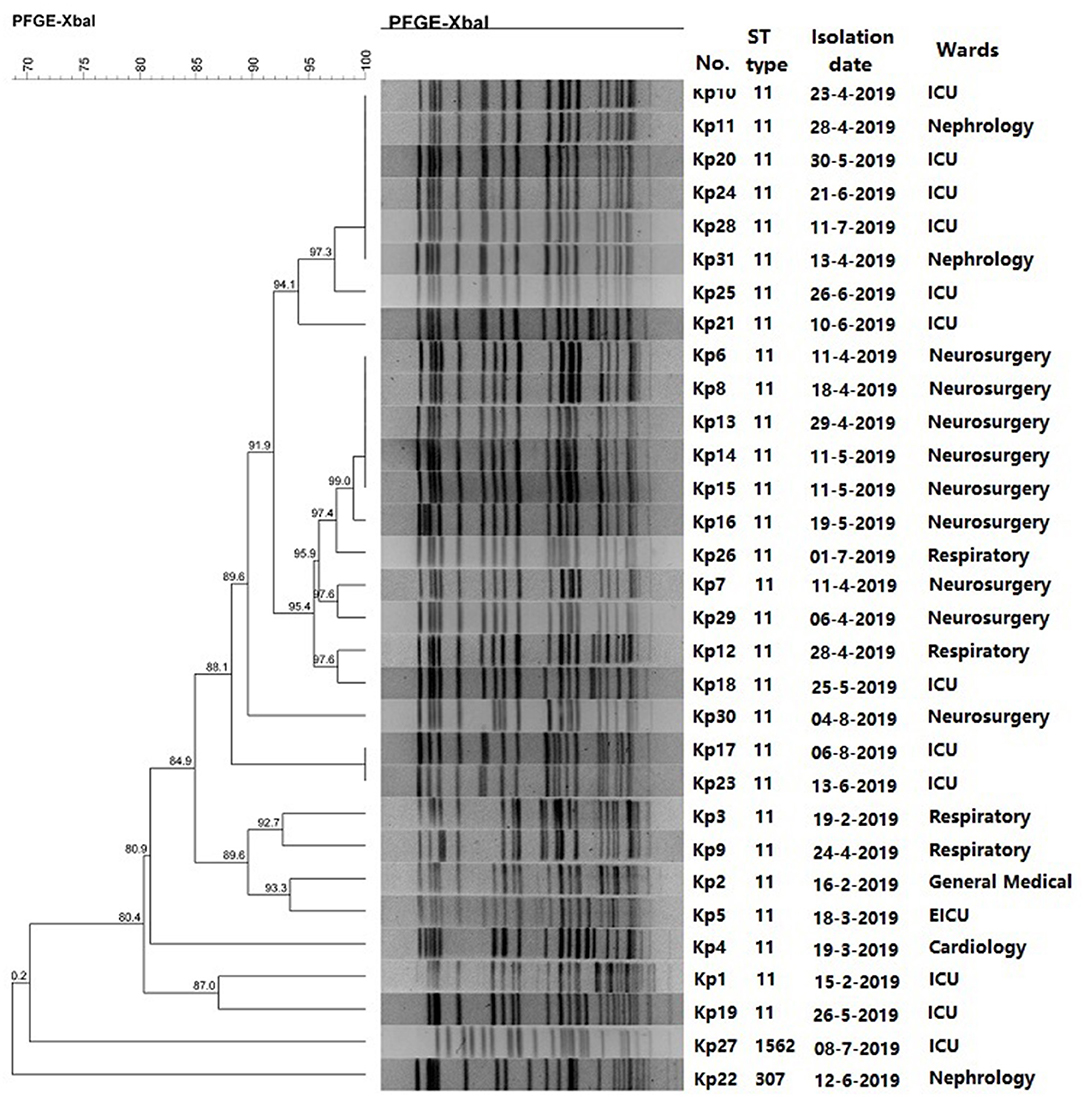
Figure 1. PFGE results and MLST typing for 31 CRKp isolates.
Our results revealed that blaNDM−5 was successfully transferred to E. coli J53 from Kp22 and Kp27 isolates. The corresponding transconjugants are termed J22 and J27, respectively. Regrettably, the blaKPC−2 gene failed to be transferred. Compared to the recipient strain E. coli J53, J22, and J27 exhibited significantly reduced carbapenem susceptibility (Table 2). The sensitivities of cephalosporin, β-lactam/β-lactamase inhibitor combinations, and carbapenems were similar to those of the donor strains, and the sensitivity of J22 and J27 to aztreonam, trimethoprim-sulfamethoxazole, quinolones, aminoglycosamines, tigecycline, and colistin were similar to those of E. coli J53. Moreover, S1-PFGE revealed that 31 CRKp isolates carried 1–4 plasmids (Supplementary Figure 1). Both Kp22 and Kp27 contained two plasmids. After conjugation, J22 and J27 contained only one plasmid, about 45 kb in size (Figure 2). Furthermore, PCR-based replicon typing revealed that these two plasmids belong to the IncX3 incompatibility group.
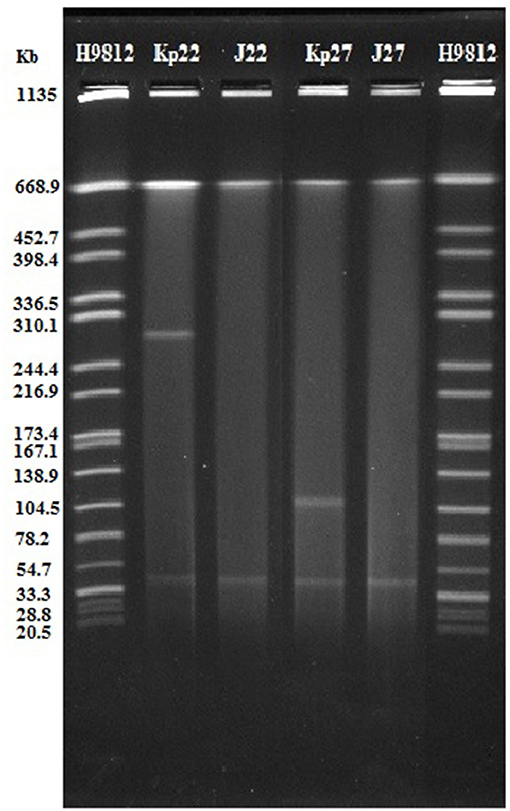
Figure 2. S1-PFGE results for Kp22 and Kp27 and their transconjugants.
Respiratory tract infections can occur at any age; however, LRTIs is more common in the elderly people. Moreover, pneumonia is a leading cause of illness and death in the elderly (13). Viruses are responsible for a large proportion of LRTIs but antibiotics are often unnecessarily prescribed for their treatment without any laboratory testing and can contribute to the emergence of antimicrobial resistance (14). K. pneumoniae is the predominant bacterial pathogen of LRTIs, and the positive rate of CRKp is increasing year by year, particularly for elderly patients (15, 16). Analysis of the molecular characteristics and drug resistance mechanism of CRKp from elderly patients with LRTIs can prove beneficial in treating this kind of infection.
In China, KPC-2 is the predominant carbapenemase in CRKp, and ST11 is the major sequence type of CRKp (17, 18). Similarly, the majority (93.55%) of CRKp isolates in the present study were KPC-2-producing ST11. We isolated two strains of blaNDM−5 carrying K. pneumoniae in the present study. In addition to blaKPC-2 and blaNDM−5, all the 31 isolates harbored blaTEM-1. Moreover, majority of these isolates carried blaSHV−11 and blaCTX−M−1, which was in accordance to the results of the previous reports (19, 20). These resistance genes led to the resistance of 31 isolates to β-lactams. Furthermore, most isolated strains were resistant to aminoglycosides and quinolones, which made the clinical fewer antibiotics choice. Fortunately, all strains were sensitive to tigecycline and colistin.
The emergence and spread of New Delhi metallolactamase (NDM)-producing Enterobacteriaceae has posed a serious public health concerns. The NDM-5 carbapenemase differs from NDM-1 by only two amino acid substitutions (Val88Leu and Met154Leu) and exhibits increased resistance to carbapenems and expanded-spectrum cephalosporins (21). NDM-5 has been identified mostly in E. coli but has rarely been described in K. pneumoniae and other Enterobacteriaceae isolates. In the present study, two K. pneumoniae isolates carrying blaNDM−5 came from different wards. They were assigned to be ST307 and ST1562. NDM-5 carried ST307 K. pneumoniae has been reported previously (21, 22). To the best of our knowledge, this is the first report of ST 1562 types with blaNDM−5. The blaNDM−5 gene was located on a conjugative IncX3 plasmid. In 2019, Ziyan Kong reported a nosocomial outbreak of NDM-5-producing K. pneumoniae in a neonatal unit in China (8). They demonstrated that all blaNDM−5 genes were located on a ~45 kb IncX3 type plasmid. The study of Zhu et al. (21) showed that the IncX3 plasmid facilitated the dissemination of blaNDM−5 among multiclonal K. pneumoniae strains and that conjugal transfer contributed significantly to IncX3 plasmid stability within K. pneumoniae. Hence, there is an urgent need for effective infection control measures to prevent blaNDM−5 variants from causing epidemic in the future.
Over the past decade, carbapenem-resistant hypervirulent K. pneumoniae (CR-hvKP) has gained immense attention (23). In this study, the serotypes closely related to hypervirulent K. pneumoniae and 12 virulence-associated genes of 31 CRKp isolates were analyzed. Six virulence-associated genes, fim, uge, mrkD, wabG, rmpA, and iucB were harbored by almost 31 isolates. These virulence genes are related to capsule synthesis, flagella movement, and iron acquisition, which are virulence factors of K. pneumonia (24). Fortunately, several serotypes of hypervirulent K. pneumoniae remained undetected. Eventually, 31 patients revealed good prognosis, and only one patient died.
The main risk factors of CRKp infection include immunosuppression, ICU admission, antibiotics exposure, surgery, mechanical ventilation, and central venous catheterization (25, 26). Elderly patients with LRTI often present non-specific symptoms, which are often covered by primary diseases, leading to irrational use of antibiotics (27). In the present study, 29 patients were exposed to various antimicrobial drugs before the positive culture. Piperacillin/tazobactam was the most commonly used antibiotic in 31 patients. Based on in vitro susceptibility testing results, majority of these patients changed to appropriate drugs such as tigecycline, levofloxacin, and amikacin. Importantly, nervous system diseases including intracranial hemorrhage and injury are the most common underlying diseases in this study. Most of these patients are unconscious and were subjected to mechanical ventilation. This is in accordance with the results of previous studies (26). Admission to neurosurgery is also a risk factor for CRKp infection. In addition, CRKp strains from neurosurgical patients have high homology, which indicates that there may be an outbreak of nosocomial infection of CRKps in neurosurgery; however, as this study was retrospective, we could not perform in-depth analysis of the patient's surrounding environment and the source of the strain.
In summary, we reported the characteristics of CRKp isolates collected from elderly patients with LRTIs. The high incidence of CRKp highlights the urgent need for further surveillance and strict infection control measures, particularly for ICU patients and immune-compromised elderly patients. One blaNDM−5 carrying CRKp with ST1562 were first reported.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author/s.
The studies involving human participants were reviewed and approved by the Ethics Committee of Taian City Central Hospital. Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
MJ and FZ designed the experiments and revised the manuscript. CS carried out the experiments and wrote the manuscript. WW and SL analyzed the data. ZZ contributed to experiment conception. All authors contributed to the article and approved the submitted version.
This study was supported by the National Natural Science Foundation of China (no. 81401696) and the Shandong Provincial Natural Science Foundation of China (no. ZR2016HL44).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2021.669173/full#supplementary-material
Supplementary Figure 1. S1-PFGE results for 31 CRKp isolates.
Supplementary Table 1. Primers used in the present study.
1. Zhang Y, Wang Q, Yin Y, Chen H, Jin L, Gu B, et al. Epidemiology of carbapenem-resistant Enterobacteriaceae infections: report from the china CRE network. Antimicrob Agents Chemother. (2018) 62:e01882-17. doi: 10.1128/AAC.01882-17
2. Viaggi V, Pini B, Tonolo S, Luzzaro F, Principe L. In vitro activity of ceftazidime/avibactam against clinical isolates of ESBL-producing Enterobacteriaceae in Italy. J Chemother. (2019) 31:195-201. doi: 10.1080/1120009X.2019.1620406
3. Cristina ML, Alicino C, Sartini M, Faccio V, Spagnolo AM, Bono VD, et al. Epidemiology, management and outcome of carbapenem-resistant Klebsiella pneumoniae bloodstream infections in hospitals within the same endemic metropolitan area. J Infect Public Health. (2018) 11:171-7. doi: 10.1016/j.jiph.2017.06.003
4. GBD 2016 Lower Respiratory Infections Collaborators. Estimates of the global, regional, and national morbidity, mortality, and aetiologies of lower respiratory infections in 195 countries, 1990-2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Infect Dis. (2018) 18:1191-210. doi: 10.1016/S1473-3099(18)30310-4
5. Khan S, Priti S, Ankit S. Bacteria etiological agents causing lower respiratory tract infections and their resistance patterns. Iran Biomed J. (2015) 19:240-6. doi: 10.7508/ibj.2015.04.008
6. Clinical and Laboratory Standards Institute. Performance Standards for Antimicrobial Susceptibility Testing Twentieth Informational Supplement. Wayne, PA: CLSI (2020) p. M100-S30.
7. Jin Y, Song X, Liu Y, Wang Y, Zhang B, Fan H, et al. Characteristics of carbapenemase-producing Klebsiella pneumoniae as a cause of neonatal infection in Shandong, China. Exp Ther Med. (2017) 13:1117-26. doi: 10.3892/etm.2017.4070
8. Kong Z, Cai R, Cheng C, Zhang C, Kang H, Ma P, et al. First reported nosocomial outbreak of NDM-5-producing Klebsiella pneumoniae in a neonatal unit in China. Infect Drug Resist. (2019) 12:3557-66. doi: 10.2147/IDR.S218945
9. Domokos J, Damjanova I, Kristof K, Ligeti B, Kocsis B, Szabo D. Multiple benefits of plasmid-mediated quinolone resistance determinants in Klebsiella pneumoniae ST11 high-risk clone and recently emerging ST307 clone. Front Microbiol. (2019) 10:157. doi: 10.3389/fmicb.2019.00157
10. Yeganeh Sefidan, F, Mohammadzadeh-Asl Y, Ghotaslou R. High-level resistance to aminoglycosides due to 16S rRNA methylation in Enterobacteriaceae isolates. Microb Drug Resist. (2019) 25:1261-5. doi: 10.1089/mdr.2018.0171
11. Shao C, Hao Y, Wang Y, Jiang M, Jin Y. Genotypic and phenotypic characterization of blaNDM-7-Harboring IncX3 plasmid in a ST11 Klebsiella pneumoniae isolated from a pediatric patient in China. Front Microbiol. (2020) 11:576823. doi: 10.3389/fmicb.2020.576823
12. Hao Y, Shao C, Bai Y, Jin Y. Genotypic and phenotypic characterization of IncX3 plasmid carrying blaNDM-7 in Escherichia coli sequence type 167 isolated from a patient with urinary tract infection. Front Microbiol. (2018) 9:2468. doi: 10.3389/fmicb.2018.02468
13. Meyer KC. The role of immunity and inflammation in lung senescence and susceptibility to infection in the elderly. Semin Respir Crit Care Med. (2010) 31:561-74. doi: 10.1055/s-0030-1265897
14. Tchatchouang S, Nzouankeu A, Kenmoe S, Ngando L, Penlap V, Fonkoua MC, et al. Bacterial aetiologies of lower respiratory tract infections among adults in Yaoundé, Cameroon. Biomed Res Int. (2019) 2019:4834396. doi: 10.1155/2019/4834396
15. Ojha CR, Rijal N, Khagendra KC, Palpasa K, Kansakar P, Gupta BP, et al. Lower respiratory tract infections among HIV positive and control group in Nepal. Virusdisease. (2015) 26:77-81. doi: 10.1007/s13337-015-0254-z
16. Uzoamaka M, Ngozi O, Johnbull OS, Martin O. Bacterial etiology of lower respiratory tract infections and their antimicrobial susceptibility. Am J Med Sci. (2017) 354:471-5. doi: 10.1016/j.amjms.2017.06.025
17. Gu B, Bi R, Cao X, Qian H, Hu R, Ma P. Clonal dissemination of KPC-2-producing Klebsiella pneumoniae ST11 and ST48 clone among multiple departments in a tertiary teaching hospital in Jiangsu Province, China. Ann Transl Med. (2019) 7:716. doi: 10.21037/atm.2019.12.01
18. Xu M, Fu Y, Fang Y, Xu H, Kong H, Liu Y, et al. High prevalence of KPC-2-producing hypervirulent Klebsiella pneumoniae causing meningitis in Eastern China. Infect Drug Resist. (2019) 12:641-53. doi: 10.2147/IDR.S191892
19. Zhao Y, Zhang X, Torres VVL, Liu H, Rocker A, Zhang Y, et al. An outbreak of carbapenem-resistant and hypervirulent Klebsiella pneumoniae in an intensive care unit of a Major Teaching Hospital in Wenzhou, China. Front Public Health. (2019) 7:229. doi: 10.3389/fpubh.2019.00229
20. Zhan L, Wang S, Guo Y, Jin Y, Duan J, Hao Z, et al. Outbreak by hypermucoviscous Klebsiella pneumoniae ST11 isolates with carbapenem resistance in a Tertiary Hospital in China. Front Cell Infect Microbiol. (2017) 7:182. doi: 10.3389/fcimb.2017.00182
21. Zhu W, Wang X, Qin J, Liang W, Shen Z. Dissemination and stability of the blaNDM−5-carrying IncX3-Type plasmid among multiclonal Klebsiella pneumoniae isolates. mSphere. (2020) 5:e00917-20. doi: 10.1128/mSphere.00917-20
22. Poirel L, Goutines J, Aires-de-Sousa M, Nordmann P. High rate of association of 16S rRNA methylases and carbapenemases in Enterobacteriaceae recovered from hospitalized children in Angola. Antimicrob Agents Chemother. (2018) 62:e00021-18. doi: 10.1128/AAC.00021-18
23. Lee CR, Lee JH, Park KS, Jeon JH, Kim YB, Cha CJ, et al. Antimicrobial resistance of hypervirulent Klebsiella pneumoniae: epidemiology, hypervirulence-associated determinants, and resistance mechanisms. Front Cell Infect Microbiol. (2017) 7:483. doi: 10.3389/fcimb.2017.00483
24. Walker KA, Miller VL. The intersection of capsule gene expression, hypermucoviscosity and hypervirulence in Klebsiella pneumoniae. Curr Opin Microbiol. (2020) 54:95-102. doi: 10.1016/j.mib.2020.01.006
25. Li J, Li Y, Song N, Chen Y. Risk factors for carbapenem-resistant Klebsiella pneumoniae infection: a meta-analysis. J Glob Antimicrob Resist. (2020) 21:306-13. doi: 10.1016/j.jgar.2019.09.006
26. Candevir Ulu A, Kurtaran B, Inal AS, Kömür S, Kibar F, Yapici Ç, et al. Risk factors of carbapenem-resistant Klebsiella pneumoniae infection: a serious threat in ICUs. Med Sci Monit. (2015) 21:219-24. doi: 10.12659/MSM.892516
Keywords: K. pneumoniae, carbapenemase, elderly, drug resistance, lower respiratory tract infection
Citation: Shao C, Wang W, Liu S, Zhang Z, Jiang M and Zhang F (2021) Molecular Epidemiology and Drug Resistant Mechanism of Carbapenem-Resistant Klebsiella pneumoniae in Elderly Patients With Lower Respiratory Tract Infection. Front. Public Health 9:669173. doi: 10.3389/fpubh.2021.669173
Received: 18 February 2021; Accepted: 26 April 2021;
Published: 20 May 2021.
Edited by:
Roger Hewson, Public Health England, United KingdomReviewed by:
Qiucheng Shi, Zhejiang University, ChinaCopyright © 2021 Shao, Wang, Liu, Zhang, Jiang and Zhang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Meijie Jiang, eHRpbmd3QDEyNi5jb20=; Fusen Zhang, aWN1emhhbmdmdXNlbkAxMjYuY29t
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.