 Veerle J. Verheyen1,2*
Veerle J. Verheyen1,2* Sylvie Remy1
Sylvie Remy1 Eva Govarts1Ann Colles1
Eva Govarts1Ann Colles1 Gudrun Koppen1
Gudrun Koppen1 Laura Rodriguez Martin1Flemming Nielsen3Liesbeth Bruckers4
Laura Rodriguez Martin1Flemming Nielsen3Liesbeth Bruckers4 Esmée M. Bijnens5Stijn Vos5Bert Morrens6Dries Coertjens6Ilse Loots6
Esmée M. Bijnens5Stijn Vos5Bert Morrens6Dries Coertjens6Ilse Loots6 Annelies De Decker7Carmen Franken7
Annelies De Decker7Carmen Franken7 Elly Den Hond7Vera Nelen7
Elly Den Hond7Vera Nelen7 Stefaan De Henauw8Adrian Covaci9Nicolas Van Larebeke10,11Caroline Teughels12
Stefaan De Henauw8Adrian Covaci9Nicolas Van Larebeke10,11Caroline Teughels12 Tim S. Nawrot5
Tim S. Nawrot5 Greet Schoeters1,2
Greet Schoeters1,2- 1VITO Health, Flemish Institute for Technological Research (VITO), Antwerp, Belgium
- 2Department of Biomedical Sciences, University of Antwerp, Antwerp, Belgium
- 3Institute of Public Health, Department of Environmental Medicine, University of Southern Denmark, Odense, Denmark
- 4I-BioStat, Data Science Institute, Hasselt University, Hasselt, Belgium
- 5Centre for Environmental Sciences, Hasselt University, Hasselt, Belgium
- 6Department of Sociology, Faculty of Social Sciences, University of Antwerp, Antwerp, Belgium
- 7Provincial Institute of Hygiene, Provincial Research Centre for Environment and Health, Antwerp, Belgium
- 8Department of Public Health and Primary Care, Faculty of Medicine and Health Sciences, Ghent University, Ghent, Belgium
- 9Toxicological Centre, University of Antwerp, Antwerp, Belgium
- 10Analytical, Environmental and Geo-Chemistry, Vrije Universiteit Brussel, Brussels, Belgium
- 11Department of Radiotherapy and Experimental Cancerology, Ghent University, Ghent, Belgium
- 12Flemish Planning Bureau for the Environment and Spatial Development, Brussels, Belgium
Chronic biological stress may adversely affect adolescents' physical and mental health, but insight in the personal and environmental factors that determine chronic stress is limited. We measured 3-month cumulative hair cortisol concentration (HCC) in 419 adolescents, participating in the Flemish Environment and Health Study. Adolescents' health and lifestyle characteristics, household and neighborhood socio-economic status as well as neighborhood urbanicity were assessed as potential determinants of HCC, using multiple linear regression models. We additionally explored heterogeneity of our results by sex. HCC were significantly higher in boys from densely populated neighborhoods, the association was not significant in girls. Accordingly, boys living outside cities had significantly lower HCC than boys, living in cities. HCC was significantly lower in adolescents with an optimal vitality, a measure of a positive mental health status. In adolescent girls, menarcheal status (pre-/postmenarche) was a significant determinant of HCC. Our findings are the first to suggest that residential urbanicity may have an impact on chronic biological stress in a general population of adolescent boys.
Introduction
Adolescence is characterized by many physical, emotional, social and cognitive challenges (1). Chronic biological stress during this vulnerable developmental period may have long-lasting implications for physical and mental health (2, 3). The hypothalamic–pituitary–adrenal (HPA) axis, with the hormone cortisol as its main effector, is a crucial biological stress response system (4). Acute and transient activation of the HPA axis facilitates effective coping with stressors (5). However, chronic HPA axis activation may lead to long-term physiological alterations and has been associated with respiratory and cardiovascular diseases, type 2 diabetes, cognitive disorders and depression (4, 6). A good insight in the factors that determine chronic HPA axis activation and cortisol secretion in adolescents is important, however, these factors are not yet fully established (7).
Traditional assessment of HPA axis function through measurement of cortisol levels in saliva, blood or urine, reflects cortisol concentrations over minutes to 24-h prior to sampling. Obtaining valid information on long-term cortisol secretion is difficult using these matrices (8). In the past decade, the cortisol concentration in scalp hair has emerged as a biomarker of long-term HPA-axis activity (4). Sampling is easily conducted and non-invasive, a single hair sample retrospectively captures several months of cortisol secretion (9). The number of studies using hair cortisol concentration (HCC) as a biomarker of chronic biological stress has substantially increased in the past years. However, literature on determinants of HCC in healthy adolescents is still limited. Most existing studies were conducted in the context of physical and mental diseases or in socioeconomically disadvantaged subgroups and included both children and adolescents (10). A systematic review of literature (7), identified sex, age, anthropometry and household socioeconomic status (SES) as determinants of HCC in children and adolescents. Recent studies, including only adolescents, did not find significant associations of HCC with sex; studies on HCC in relation to anthropometry yielded varying results (11–14). Gray et al. (7) identified associations of HCC with perinatal characteristics, atopic illness and mental health as important remaining knowledge gaps. The perinatal period may influence HPA functioning and disease risk later in life (15). Atopic disease and the use of corticosteroid medication may also affect HPA axis functioning (16). No significant associations of HCC with adolescents' mental health measures, including perceived stress or anxiety, have yet been reported (7, 10, 17). Interestingly, a small study among adolescents (12–18 years, n = 27) did not find a significant association of HCC with perceived stress, however, adolescents' optimism was significantly associated with lower HCC (18).
The HCC of adolescents may also be related to their residential environment. An urban, densely populated, residential environment has been hypothesized to act as a chronic stressor, regardless of a person's individual socioeconomic position (19, 20). Potential pathways are the social context of an urban neighborhood and a higher exposure to air pollution, noise and heat (21, 22). In an exploratory study among children (median age 10 years, n = 92), neighborhood urbanicity was not related to HCC (20). However, neighborhood socio-environmental influences may exert stronger effects on adolescents, compared to children (19).
The objective of this study was to gain a better insight in sociodemographic, health and lifestyle factors as well as neighborhood characteristics that contribute to chronic stress in adolescents. The selection of potential determinants of chronic biological stress was based on existing literature. To the best of our knowledge, this study is the first to explore HCC in relation to neighborhood urbanicity in adolescents. During adolescence the responsivity of the HPA axis may be sex-dependent. We therefore additionally explored effect modification of associations between HCC and potential determinants by sex (23, 24). Our study may support formal and informal initiatives to promote adolescents' health and wellbeing through chronic biological stress prevention and reduction.
Materials and Methods
Study Population and Design
This study was embedded in a human biomonitoring program, i.e., the Flemish Environment and Health Study (FLEHS), initiated by the Flemish government in 2002. The goal of FLEHS is to investigate the relationship between a broad range of environmental exposures and health effects and to support environmental health policy by identifying priorities for further action (25). This study was conducted within the fourth cycle of the FLEHS (FLEHS-4, 2016–2020), including adolescents from the general population of Flanders. One of the main objectives of FLEHS-4 was to investigate associations of residential environmental surroundings with adolescents' health. The study protocol was approved in June 2017 by the Antwerp University Hospital Ethical committee (registration number B300201732753). Between September 2017 and June 2018, a representative sample of 428 Flemish 14–15 year old adolescents was recruited and examined in schools by trained nurses. Parents and adolescents filled out extensive questionnaires that provided detailed information on health, lifestyle and household socio-economic status. A stratified clustered multi-stage sampling strategy was applied to enroll equal numbers of participant across both sexes, to represent all educational levels, to geographically represent all Flemish provinces and different degrees of urbanicity. The inclusion criteria of the FLEHS-4 study were: informed consent signed by the adolescent and a parent, having lived in Flanders for at least 5 years, adolescent and parents mastered enough Dutch to fill out questionnaires. Exclusion criteria were: data of more than one questionnaire missing, blood and urine sample missing, being held back in school for more than 1 year, attending a boarding school. One adolescent was excluded because of pregnancy. Of the 428 FLEHS-4 participants, eight could not participate in this part of the study because their hair was too short (<3 cm). One participant was excluded for following a growth hormone therapy. Thus, the final sample of this study included 419 adolescents.
Hair Cortisol Concentrations
A strand of hair of at least 3 cm was cut close to the scalp from the posterior vertex of the adolescents' head. Hair samples were stored in the dark at room temperature in paper envelopes. Analysis was performed within 18 months after collection of the first samples. HCC was determined from the scalp-near 3 cm hair segment. Human hair on the head grows at a rate of approximately 1 cm per month, HCC of 3 cm hair strands retrospectively reflect cortisol levels for the period of 3 months (26). Samples were analyzed at the Institute of Public Health, Department of Environmental Medicine of the University of Southern Denmark (SDU), using liquid chromatography combined with tandem mass spectrometry (LC-MS/MS) as described previously by (27). Briefly, hair samples were washed with methanol and dried at room temperature. The 3 cm hair strand was cut into 2–3 mm segments that weighed 20–30 mg. Aliquots of 100 μL 20 ng/mL isotope labeled cortisol-D4 were added as internal standard, together with 0.9 mL methanol. Samples were incubated in the dark at 25°C, while whirl mixed at 2,000 revolutions per minute for 5 days and subsequently centrifuged at 3,000 g for 5 min. Twenty microlitre of the supernatant was injected onto a High-Performance Liquid Chromatography (HPLC) column. HPLC was performed using an Accella 1,250 pump (Thermo Scientific, San Jose, CA) and a PAL autosampler (CTC analytics, Zwingen, Switzerland). The analytical column was a Kinete × C18 column, 100 × 4.6 mm (2.6 μm) equipped with a 2 × 4 mm C18 SecurityGuard column (Phenomenex, Torrance, CA). Isocratic elution was performed with a mobile phase system consisting of methanol and 0.1 M formic acid (80:20) at a flow rate of 400 μL/min for 6 min. After the peaks were eluted, a wash procedure was performed before the next samples was injected onto the column. The triple quadrupole mass spectrometer was a TSQ Vantage (Thermo Scientific, San Jose, CA). The calibration curve and calculation of the sample concentration were based on the area ratio of the analyte/isotope labeled internal standard. The calibration curve ranged from 0.02 up to 200 ng/mL, which corresponds to a range of 1–1000 pg/mg hair when 20 mg of hair is utilized. Quality control samples were included in the analysis with low, medium and high concentration levels (7.1, 35.9 and 91.7 pg/mg, respectively). The limit of quantification (LOQ) for cortisol was 0.3 pg/mg hair. The intra-day repeatability coefficient of variation (CV) of the assay was 8.7% and the inter-day reproducibility CV was 9.5%.
Determinants of Hair Cortisol Concentrations
Sociodemographic Variables
The country of birth of the adolescent and his or her parents was assessed as Belgium, European Union, or outside the European Union. Household socioeconomic status (SES) was evaluated, based on education and income variables. Therefore, the highest household educational attainment was assessed according to the Belgian education system as primary (no educational attainment, primary school, lower secondary school), secondary (higher secondary school) and tertiary (higher education attainment). Monthly equivalent income was calculated as the total monthly household income standardized to the number of household members, a value of one is assigned to the household head, of 0.5 to each additional adult member and of 0.3 to each child under 18 year (28). Parents also reported their perceived income adequacy, a subjective SES measure, ranging from difficult to very easy to make ends meet.
We geocoded participants' homes addresses to assess neighborhood urbanicity and neighborhood SES. We classified urbanicity of the participants' residential neighborhood, using the Eurostat definition of urbanicity that is based on a combination of geographical contiguity and population density, applied to 1 km2 population grid cells (29). Eurostat defines neighborhoods as (1) cities: densely populated areas where 50% or more of the population lives in urban Centers with a population density of at least 1,500 inhabitants per km2 and at least 50,000 inhabitants, (2) towns/suburbs: intermediate density areas where 50% or more of the population lives in urban clusters with a population density of at least 300 inhabitants per km2 and a minimum population of 5,000 inhabitants, (3) rural areas: thinly populated areas outside of city Centers and urban clusters.
In accordance with previous FLEHS studies, we assessed population density at the municipality level dichotomously as low residential population density (≤ 600 inhabitants/km2) and high residential population density (>600 inhabitants/km2) (30). We assessed neighborhood socioeconomic status (SES) using the Area Deprivation Index (ADI), which is calculated at a sub-municipality level in Flanders on a yearly basis (31). The area deprivation index of 2018 considers all children born in year 2018, 2017 and 2016 that live in deprived households in a given neighborhood in Flanders, divided by the total number of children born in this neighborhood during the same period. The ADI is documented by the Child and Family Government Agency (www.kindengezin.be). Selection criteria are the family's monthly income, the parents' educational attainment and employment situation, development of the children, housing and health. If a family fulfills at least three criteria, it is considered to be deprived.
Lifestyle, Physical and Mental Health Variables
Information on adolescents' lifestyle included smoking, frequency of alcohol use and sports (physical activity that causes sweating and/or heavy breathing). We gathered information on their hair washing frequency and hair treatment (dying, bleaching).
During sampling at school, waist circumference, body length and weight were measured by study nurses with standardized equipment and according to standardized protocols. From this information, the body mass index (BMI) was calculated as body weight in kg/(body length in m)2. Boys and girls were classified as underweight, normal weight, overweight or obese according to the sex- and age-specific 2004 Belgian growth curves (32). The parent questionnaire provided information on perinatal factors, including maternal smoking during pregnancy, low birth weight (<2500 g) and preterm birth (born before the 37th pregnancy weeks). Atopic disease (doctor-diagnosed asthma, atopic dermatitis, allergic rhinitis in the past year) was evaluated, based on questions from the International Study of Asthma and Allergy in Childhood (ISAAC) questionnaire (33). The use of corticosteroid medication in the 14 days prior to sampling was reported and information on infections in the past year was also provided. Girls provided information on their menarcheal status and use of contraceptives.
Mental health of adolescents was assessed by the following indicators:
- The Strengths and Difficulties Questionnaire (SDQ), a validated screening method that covers a broad range of mental health symptoms (34, 35). The 25-item versions of the SDQ contains four scales, each of five items, focusing on difficulties in emotional functioning, conduct, hyperactivity and interaction with peers in the past 6 months (35). The five items can be scored 0, 1, or 2, and the total score for each scale can therefore range from 0 to 10. These four scales together form the total difficulties scale (range 0–40). Additionally, the SDQ contains one 5-item scale focusing on prosocial behavior. A high score on the total difficulties scales (20–40) represents an abnormal degree of difficulties; a high score on the prosocial scale (6–10) represents normal prosocial behavior.
- The Vitality scale for positive mental health from the Short Form-36 (SF-36) Health Survey questionnaire assesses vitality based on four items: lust for life, energy level, level of exhaustion and tiredness in the past 4 weeks, with scores between 0 and 100 (best score) (36). To reflect optimal vitality, a cut-off value of 77.4 was applied to the continuous vitality score, being the study mean vitality score plus one standard deviation, in accordance to the BHIS, the Belgian Health Interview Surveys (37). Optimal vitality was evaluated dichotomously for each participant as a value above the cut-off value.
- Perceived stress in the past 3 months was assessed based on the question “Did you experience a lot of stress in the past 3 months?” and was scored as low (never, seldom), medium (sometimes), high (often, always).
- Self-rated general happiness was evaluated, based on the question “All things considered, would you say that you are happy?” and was scored as low (not happy at all, rather not happy) or high (rather happy, very happy).
Meteorological Data
Data on local ambient temperature and UV-radiation was provided by the Belgian Royal Meteorological Institute (KMI). Temperature was measured in 15 weather stations in Flanders, we used data from the weather station closest to the adolescents' home to calculate average temperature and UV-radiation over the 3-month period prior to sampling. Based on the sampling date, the season of sampling was determined.
Statistical Analysis
Statistical analysis was performed using SPSS Statistics (version 26; IBM, Armonk, NY, USA) and R version 3.5.0 (R Foundation for Statistical Computing, Vienna, Austria). HCC concentrations (pg/mg hair) were not normally distributed and were therefore transformed by the natural logarithm prior to statistical analysis. For two HCC values below the LOQ, values were imputed using a truncated lognormal distribution. First a truncated lognormal distribution was fitted for the observed values (the values above the LOQ). This resulted in an estimate of the mean and standard deviation of the lognormal distribution of all values (below and above the LOQ). For values < LOQ, random values were imputed, taken between 0 and the limit from the lognormal distribution with the estimated mean and SD. Outliers (above the mean + 3 standard deviations) were not excluded from our main analyses, since we found no analytical or biological reason for exclusion. HCC are described as the geometric mean concentrations with 95% confidence interval (95% CI), together with the median HCC, 25th, 75th and 90th percentile. HCC of boys and girls were compared using an independent samples t-test.
We first examined associations between HCC as a dependent variable and each determinant as an independent variable in linear regression models, adjusted for age and sex. A p ≤ 0.05 was used as cut-off for statistical significance. Effect modification by sex was assessed by adding the interaction term of each determinant and sex into the regression model and evaluating the p-value of the interaction term. Only significant interactions (p ≤ 0.10) were reported. The use of contraceptives and menarcheal status were evaluated as potential determinants of HCC in girls-only models.
Next, multiple linear regression models were built, including significant determinants of HCC (p ≤ 0.05), additionally adjusted for variables that were associated with HCC at a significance level of ≤ 0.20 in the former analysis. Age and sex remained in the models as fixed covariates regardless of their significance. We examined associations between the independent variables by Spearman rank correlation (ρ). Collinearity between independent variables in the models was checked by evaluating the variance inflation factor (VIF <3) (38). The R-square of the model is presented as the percentage of variation in HCC, explained by the independent variables in the final model.
In a sensitivity analysis, all associations were evaluated after winsorizing HCC values that were identified as outliers (39). In line with previous cortisol research (9, 40–42), HCC values of more than 3 standard deviations (SD) above the mean were set at 3 SD above the mean before transformation to the natural logarithm, to reduce their impact on data analysis.
Given the large selection of potential determinants that was included in this exploratory analysis, we accounted for multiple testing. We verified our results after controlling for a false discovery rate (FDR) at q = 0.10 using the Benjamini and Hochberg method (43). We included the p-values of each association between an independent variable and HCC after adjustment for age and sex in the Benjamini–Hochberg procedure. For variables that were significantly modified by sex, we included p-values of each sex separately.
Results
Study Population Characteristics
Sociodemographic, lifestyle and health characteristics of the study population are described in Table 1. Our study population consisted of 419 adolescents. Slightly more girls (n = 228, 54.4%) participated in this study compared to boys (n = 191, 45.6%), but equal distribution between the sexes is approached. The mean (SD) age of the study population was 14.8 (± 0.5) years for both sexes. For 80.4% of the adolescents, Belgium was their country of birth; this proportion reflects the general Flemish population (79.5% born in Belgium) (44). Household educational attainment was high in this study: 59.4% of the households had a parent that achieved a tertiary educational level compared to 41% in Flanders (45). This tendency was also observed in previous FLEHS studies and is due to better response rates in highly educated households (46, 47). The average ADI of 12% in our study population is slightly lower than the Flemish ADI of 14.5% (48). Almost one out of three households (28.4%) found it difficult to make ends meet with their income. Residential population density was high for 36% of participants whereas 48.9% of the Flemish population lives in densely populated municipalities (44). A minority of participants lived in cities (13.6%) and rural areas (14.1%), the majority lived in towns and suburbs (72.3%). On the national scale, a higher share of 29.5% of the population lives in cities, 55% of Belgians live in towns and suburbs, and comparable to our study population, 15.5% live in rural areas (49). BMI was normal for 77% of the participating boys and 68% of the girls, this is comparable to the fraction of Flemish adolescents (10–17 years) with a normal BMI (75.2 and 69%, respectively) (44). Vitality was optimal for 13.4% of participants, a result in line with the 14% of the Belgian population (50). More than one third of participants (33.2%) reported to perceive a lot of stress.
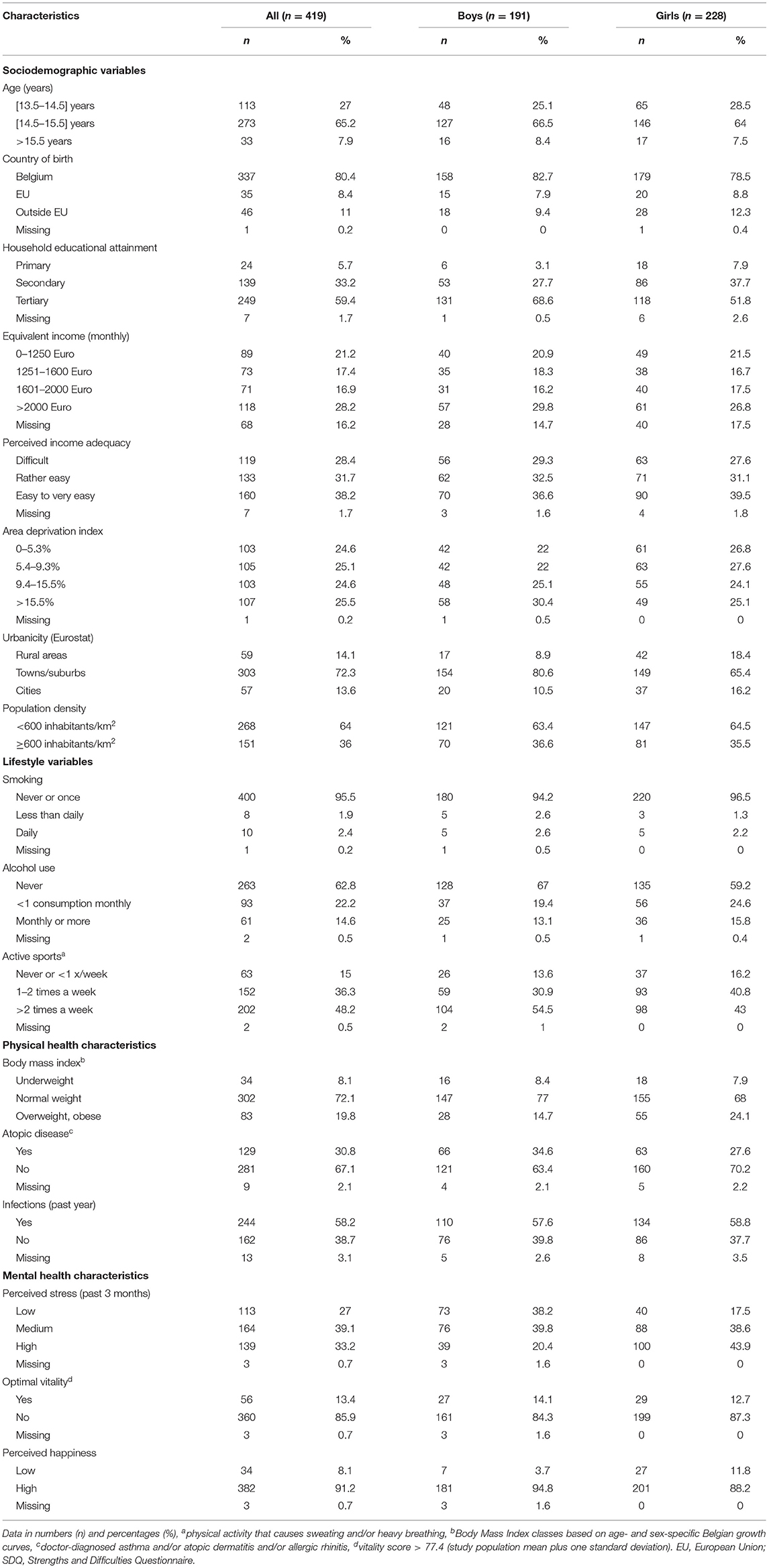
Table 1. Study population characteristics.
Hair cortisol concentrations are described in Table 2. The geometric mean HCC of all participants was 3.13 (95% CI: 2.90, 3.38) pg/mg, median HCC value was 2.98 pg/mg with an interquartile range of 2.28 pg/mg. Geometric mean HCC was higher for girls than boys [3.30 (95% CI: 2.99, 3.63) vs. 2.95 (95% CI: 2.61, 3.30) pg/mg], the difference was not statistically significant (p = 0.154).
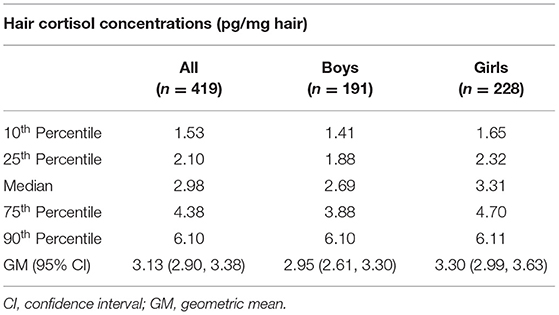
Table 2. Descriptive statistics of hair cortisol concentrations of all participants and stratified by sex.
Assessment of Determinants of Hair Cortisol Concentrations in Adolescents
Table 3 presents results of associations between HCC and potential determinants of HCC in regression models, adjusted for sex and age. Results of the univariate analysis are presented in Supplementary Table 1. Effect modification of associations between potential determinants and HCC by sex is reported when significant.

Table 3. Linear regression analyses, adjusted for sex and age, for the assessment of determinants of hair cortisol concentrations in adolescents.
Sociodemographic Determinants of HCC
We did not observe a significant association between HCC and sex (p = 0.138) nor between HCC and age (p = 0.221). HCC was not significantly associated with adolescents' country of birth (p = 0.356). There were no significant associations between HCC and household educational attainment (p = 0.835) or equivalent income (p = 0.422). Overall, HCC was not significantly associated with perceived income adequacy (p = 0.194). Between perceived income adequacy categories, we observed a tendency toward significantly lower HCC in adolescents, living in households that reported having it easy make ends meet, compared to adolescents, living in households that reported having it difficult to make ends meet (p = 0.070). The model estimated HCC of adolescents from households that reported having it easy to make ends meet on average a factor 0.84 (95% CI: 0.69, 1.01) lower, compared to their counterparts from households that reported having it difficult to make ends meet.
Living in a more densely populated neighborhood was positively associated with adolescents' HCC [p = 0.047, β = 1.18 (95% CI: 1.00, 1.38)]. The association between neighborhood population density and HCC was significantly modified by sex and was driven by boys (p-interaction = 0.024). Boys who lived in a densely populated neighborhoods, had significantly higher HCC compared to their peers from less densely populated neighborhoods [p = 0.002, β = 1.44 (95% CI: 1.14, 1.81)]. The association was not significant in girls [p = 0.934, β = 0.99 (95% CI: 0.80, 1.23)]. HCC for all adolescents taken together, was not significantly associated with neighborhood urbanicity (p = 0.177). However, this association was also significantly modified by sex (p-interaction = 0.011). Boys, living in towns/suburbs or in rural areas had significantly lower HCC compared to boys that lived in cities [p = 0.002, β = 0.56 (95% CI: 0.38, 0.80) and p = 0.002, β = 0.44 (95% CI: 0.27, 0.74), respectively]. HCC was not significantly associated with urbanicity in girls [p = 0.521, β = 1.10 (95% CI: 0.83, 1.46) and p = 0.980, β = 1.00 (95% CI: 0.70, 1.41) for towns/suburbs and for rural areas, respectively, compared to cities].
Lifestyle, Health and Meteorological Determinants of HCC
We did not observe significant associations of HCC with lifestyle characteristics. We found no significant associations of HCC with anthropometric measures or perinatal factors. The association between HCC and atopic disease tended toward significance [p = 0.071, β = 1.17 (95% CI: 0.99, 1.38)]. In girls, HCC was significantly higher in post-menarcheal girls compared to pre-menarcheal girls in an age-adjusted model [p = 0.004, β = 1.61 (95% CI: 1.17, 2.23)]. HCC was not significantly associated with mental health variables such as SDQ scores, perceived stress or general happiness. Adolescents reporting optimal vitality, however, had significantly lower HCC than adolescents that did not score optimal on vitality [p = 0.015, β = 0.76 (95% CI: 0.61, 0.95)]. There were no significant associations of HCC with meteorological factors or season of sampling.
Determinants of HCC: Accounting for Multiple Simultaneous Determinants
In the next step, significant determinants of HCC were evaluated in a multiple regression model, adjusted with all variables that showed a significance level ≤ 0.2 in the determinant assessment. Spearman rank correlations between all variables that met this criterion were first evaluated, results are presented in Supplementary Table 2. We observed a weak negative correlation between optimal vitality and atopic disease (Spearman rank ρ = −0.131), a weak positive correlation between age and menarcheal status (Spearman rank ρ = 0.166) and a moderately strong positive correlation between neighborhood urbanicity and population density (Spearman rank ρ = 0.545). Adolescents' HCC remained negatively associated with optimal vitality [p = 0.035, β = 0.78 (95% CI: 0.63, 0.98)] and population density [p = 0.036, β = 1.19 (95% CI: 1.04, 1.40)] after adjustment for sex, age, perceived income adequacy and atopic disease. The model, presented in Supplementary Table 3, explained 3% of the variance in adolescents' HCC. In this model, the association between HCC and atopic disease further attenuated [p = 0.232, β = 1.11 (95% CI: 0.94, 1.31)]. HCC was overall not significantly associated with perceived income adequacy (p = 0.120): we however observed significant lower HCC in adolescents living in a household that reported having it easy to get by with their income, compared to adolescents, living in households that reported having it difficult to get by [p = 0.040, β = 0.82 (95% CI: 0.67, 0.99)].
As population density is a criterion for urbanicity, both variables were assessed in separate models. When the interaction term of sex and population density was additionally added to the model, as presented in Supplementary Table 4, HCC of boys from a densely populated neighborhood remained significantly higher compared to HCC of those from less densely populated neighborhoods [p = 0.002, β = 1.46 (95% CI: 1.15, 1.85)] after adjustment for age, perceived income adequacy, atopic disease and optimal vitality. The model explained 4.1% in boys' variation in HCC. When the interaction term of sex and neighborhood urbanicity was included in the model, the model explained an equal proportion of 4.1% of variations in HCC of adolescent boys. Boys from towns/suburbs or rural areas exhibited significantly lower HCC compared to boys from cities [p = 0.002, β = 0.55 (95% CI: 0.38, 0.81) and p = 0.003, β = 0.45 (95% CI: 0.27, 0.76), respectively]. The estimated mean HCC for boys and girls in relation to urbanicity are illustrated in Figure 1.
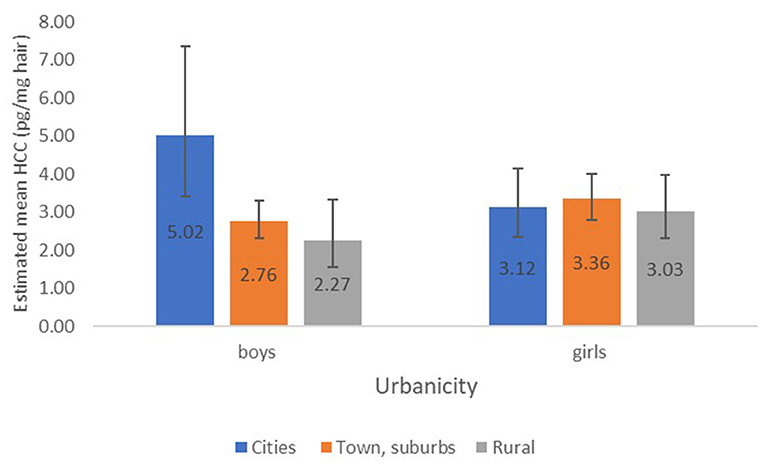
Figure 1. Estimated mean HCC (±95% CI) in relation to urbanicity for boys and girls, associations of HCC with urbanicity adjusted for age, perceived income adequacy, atopic disease and optimal vitality.
Menarcheal status remained a significant determinant of HCC in girls [p = 0.006, β = 1.59 (95% CI: 1.14, 2.23)] after adjustment for age, perceived income adequacy, population density, optimal vitality and atopic disease. The model, presented in Supplementary Table 5, explained 3.5% of variations in adolescent girls' HCC.
Sensitivity Analysis
In a sensitivity analysis, linear regressions analyses for the assessment of determinants of HCC were performed using winsorized data. In accordance with literature (8, 9, 40, 51), we observed several outliers in our data. Three participants exhibited HCC > 3 standard deviations (SD) from the mean and were winsorized to the mean + 3 SD. Results of the analyses are presented in Supplementary Table 6, winsorizing the data was of little influence on the observed associations and interactions. We found similar significant differences by sex for the association of neighborhood population density with HCC (p-interaction = 0.022), with significantly higher HCC for boys from densely populated neighborhoods [p = 0.003, β = 1.39 (95% CI: 1.12, 1.73)], but no significant difference in HCC by population density was found for girls [p = 0.989, β = 1.00 (95% CI: 0.82, 1.23)]. We also observed similar differences by sex for the association of urbanicity with HCC (p-interaction = 0.014). Boys that lived in towns and suburbs or rural areas had significantly lower HCC compared to boys that lived in cities [p = 0.003, β = 0.59 (95% CI: 0.42, 0.83) and p = 0.002, β = 0.47 (0.29, 0.76), respectively]. There was no significant difference in HCC across urbanicity for girls.
We reinterpreted our results after controlling for the false discovery rate (FDR) at q = 0.10 using the Benjamini and Hochberg method. Optimal vitality did not remain a significant determinant of HCC when we controlled for the FDR at q = 0.10, while population density, urbanicity remained significant determinants of adolescent boys' HCC and menarcheal status remained a significant determinant of adolescent girls' HCC.
Discussion
In this study, we explored potential determinants of chronic biological stress in a general population of Flemish adolescents, using hair cortisol concentrations as a novel objective biomarker of chronic stress. HCC was significantly lower in adolescents with an optimal vitality, an indicator of a positive mental health status, and significantly higher in adolescents from densely populated neighborhoods. The association of HCC with population density was driven by boys. Moreover, boys from urban neighborhoods had significantly higher HCC than those from towns, suburbs and rural areas. The associations remained significant after adjustment for age, perceived income adequacy, atopic disease and optimal vitality. This is the first study to identify neighborhood urbanicity as a determinant of chronic stress in a general population of adolescents. We identified post-menarcheal status as an important determinant of HCC in girls.
We did not observe a significant difference in HCC between adolescent boys and girls in this study. Our results are in line with a large-scale multi-country study that measured hair cortisol in adolescents using LC/MS-MS (12–17 years, n = 353) (51). Other studies, including children and adolescents, found a significant difference in HCC by sex (7). This difference seems to be predominantly present in childhood. A recent study (n = 434) observed significantly higher HCC in boys compared to girls in prepuberty, HCC values in both sexes converged after the onset of puberty (13). Similar to other recent adolescent-specific studies (10, 51), age was not a significant HCC determinant in this study. Research in broader age ranges did find significant associations of HCC with age (7, 13).
In line with previous research in adolescent populations (52, 53), we did not observe a significant relation between household educational attainment and HCC. The household equivalent income was not significantly associated with HCC. Adolescents from households that reported having it easy to very easy to get by with their income exhibited borderline significantly lower HCC compared to adolescents from households that reported having it difficult to make ends meet. Previous research has indicated that subjective income adequacy measures exhibit a positive association with health and well-being, above and beyond the health benefits associated with objective income measures (3).
In contrast to Wagner et al. (13) in the age group of 5–18 years (n = 434) (13), we found no significant associations between perinatal factors (low birth weight, preterm birth) and adolescents' HCC. Possibly, the associations attenuate over time, a prospective cohort study found maternal prenatal smoking and low birth weight to be associated with HCC in children, however, the associations did not persist in adolescence (12). We identified post-menarcheal status as an important determinant of HCC in girls. The onset of menstruation is a hallmark of female pubertal development that is associated with a marked increase in cortisol secretion (54). In accordance with previous research (55), we found no significant association of girls' contraceptive use with HCC. We observed a tendency toward a significant association of HCC with atopic diseases, which are known to be widespread among adolescents. HCC was not significantly associated with psychosocial variables such as SDQ scores or perceived stress. These results are consistent with existing literature (7, 10, 56). Adolescents may experience psychological stress when they are not stressed biologically and alternatively may be biologically stressed, but not report any psychological stress (18). Optimal vitality was significantly associated with lower HCC in our study. An exploratory study previously assessed HCC in relation to a positive mental health status in adolescents (12–18 years, n = 27) and observed an inverse association between HCC and optimism (18). According to the World Health Organization, mental health is a state of well-being in which an individual realizes his or her own abilities, can cope with the normal stresses of life and is able to make a contribution to his or her community (57). Optimal vitality did not remain a significant determinant when we controlled for multiple testing. However, our aim was to identify potential determinants of adolescents' HCC. We therefore still consider optimal vitality as a potential determinant of HCC. Possibly, vitality and coping strategies play a role in associations between stressors and biological stress. We therefore suggest future research to consider optimal vitality as a determinant of HCC in adolescence.
The observed association of HCC with a high neighborhood population density in all adolescents was driven by boys. Furthermore, urbanicity was a significant determinant of HCC in boys in this study, but not in girls. Sexually dimorphic HPA axis reactivity has previously been reported, with men showing a greater cortisol response to real-life or controlled laboratory stress compared to women (58). Flanders, our study region, is known as one of the most densely populated areas in Europe (59). Moreover, urbanization is one of the dominant demographic trends in the 21st century (22). Importantly, living in an urban area seems to be associated with an increased risk of mental health problems, compared to living in a rural area (19). Retrospective studies showed that this increased risk for mental health problems in adults may be greater for those who grew up in an urban context (60, 61). Residential urbanicity has also been associated with adverse cardio-metabolic health outcomes (62, 63). Despite the evidence of a higher incidence of health problems in urban areas, the mechanisms underlying this association are not well understood (22). Extensive research has put forward several pathways through which an urban environment may affect physical and mental health, including the socioeconomic circumstances and social context of an urban residential environment and environmental challenges such as air pollution, noise, heat and lack of greenspace (21, 22). A Flemish study, tracking 175 children during a 3-year time period between childhood and adolescence, found that higher residential exposure to semi-natural and forested areas was associated with increased feelings of happiness, while a poorer emotional status was seen with increased residential traffic exposure (56). Chronic stress through HPA axis activation has been suggested as a potential biological mechanism, underlying the association between urbanicity and health (19). In our adolescent study population, household SES and neighborhood SES were not associated with HCC, nor was psychosocial stress. Possibly, environmental factors such as air pollution and noise play a role. Animal and human studies, using salivary and serum cortisol as short-term markers of HPA axis activity, have demonstrated that air pollutants may dose-dependently increase the release of cortisol (64). Increased salivary cortisol levels have also been associated with noise exposure (65). In a recent study in Flanders, we observed a positive association between residential proximity to major roads and HCC in pregnant women (66). Further research in this study population may elucidate the relationship between air pollution, noise and participants' HCC.
This study has several strengths. First, all hair samples were collected by a small team of trained nurses, ensuring low variability in sampling method across our study population. We used a sensitive LC-MS/MS method to measure hair cortisol, as recommended. The multidisciplinary setup of the FLEHS-4 study, resulted in detailed information on physical and mental health, social and behavioral factors, as well as geographical information. This enabled us to characterize a broad range of variables that have previously been postulated as potential determinants of HCC in literature, but have not yet been explored in adolescents. We also need to address several limitations. The bidirectional relationship between stress and health outcomes makes cross-sectional studies vulnerable to reverse causation (12). Longitudinal follow-up of our study population could provide more insight in direction of associations between HCC and health. We had no information on natural hair color, which has been hypothesized to influence HCC, but previous studies found no associations of HCC with natural hair color in adolescents (7, 11). We collected information on corticosteroid medication use in a period of 14 days prior to sampling. Information on less recent medication use was not collected. We did not observe significant associations of HCC with local ambient temperature; however, participants were not examined during the warmer summer season because of school holidays. Our aim was to identify potential determinants of adolescents' HCC that need to be confirmed or underpinned in future research. We therefore assessed a broad range of potential determinants of HCC. Although we evaluated our results after correcting for multiple testing, we cannot rule out the possibility of observing significant associations due to chance. More targeted assessment of health, psychosocial variables, behavior and urban environmental exposures could help future, larger, studies to gain a deeper insight in the determinants of adolescents' chronic stress. Growing attention is currently being paid to concept of the urban exposome, the totality of environmental exposures and their endogenous response in shaping disease risk and disease development of urban dwellers (67, 68). Applying the exposome concept to stress research can provide a more holistic view of all factors that contribute to chronic stress. The emerging technology of wearable sensors can help to easily and rapidly generate the necessary information (22).
In conclusion, our results suggest that personal factors as well as residential environment significantly determine hair cortisol concentrations in adolescents, a marker of chronic biological stress. Preventing chronic stress, a known risk factor for ill health, should therefore not be limited to the personal level but should also include preventive measures at the neighborhood level. This new knowledge may support future stress research and evidence-informed public health.
Data Availability Statement
The datasets presented in this article are not readily available because access to the data can only be granted by the data owner. Requests to access these datasets should be directed to VITO, RkxFSFMuZGF0YW1hbmFnZW1lbnRAdml0by5iZQ==.
Ethics Statement
The studies involving human participants were reviewed and approved by Antwerp University Hospital. Written informed consent to participate in this study was provided by the participants' legal guardian/next of kin.
Author Contributions
VV, SR, LB, IL, ED, VN, SD, NV, AdC, CT, TN, and GS have made substantial contributions to the conception and design of the study. VV, AnC, EG, GK, LM, LB, AD, CF, DC, EB, SV, and ED contributed to acquisition of data and statistical analysis. FN contributed to design of the study, acquisition of data and biomarker analysis. VV, SR, LB, BM, and GS participated in the interpretation of the data. VV drafted the manuscript. SR and GS helped to draft the manuscript. VV, SR, EG, AnC, GK, LM, FN, LB, EB, SV, BM, DC, IL, AD, CF, ED, VN, SD, AdC, NV, CT, TN, and GS were involved in critically reviewing and editing the manuscript. GS coordinated the Flemish Environment and Health Study. All authors approved the manuscript to be published.
Funding
This paper is based on research conducted within the framework of the Flemish Center of Expertise on Environment and Health (FLEHS 2016-2020), funded by the Government of Flanders, Department of Environment & Spatial Development. VV was supported by a PhD fellowship at the University of Antwerp and VITO, funded by the Flemish Center of Expertise on Environment and Health.
Author Disclaimer
The views expressed herein are those of the author(s) and are not necessarily endorsed by the government of Flanders.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
We thank the adolescents and their families who participated in FLEHS IV. Without their effort, this study would not have been possible. We thank the field workers from the Provincial Institute of Hygiene and VITO for the sample and data collection.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2021.669022/full#supplementary-material
References
1. Romeo RD. Adolescence: a central event in shaping stress reactivity. Dev Psychobiol. (2010) 52:244–53. doi: 10.1002/dev.20437
2. Schreier HMC, Chen E. Low-grade inflammation and ambulatory cortisol in adolescents: interaction between interviewer-rated versus self-rated acute stress and chronic stress. Psychosom Med. (2017) 79:133–42. doi: 10.1097/PSY.0000000000000377
3. Hofmann M, Young C, Binz TM, Baumgartner MR, Bauer N. Contact to nature benefits health: mixed effectiveness of different mechanisms. Int J Environ Res. (2018) 15:31. doi: 10.3390/ijerph15010031
4. Iob E, Steptoe A. Cardiovascular disease and hair cortisol: a novel biomarker of chronic stress. Curr Cardiol Rep. (2019) 21:116. doi: 10.1007/s11886-019-1208-7
5. Wellen KE, Hotamisligil GS. Inflammation, stress, and diabetes. J Clin Investig. (2005) 115:1111–9. doi: 10.1172/JCI25102
6. Thomson EM. Neurobehavioral and metabolic impacts of inhaled pollutants. Endocrine Disruptors. (2013) 1:e27489. doi: 10.4161/endo.27489
7. Gray NA, Dhana A, Van Der Vyver L, Van Wyk J, Khumalo NP, Stein DJ. Determinants of hair cortisol concentration in children: a systematic review. Psychoneuroendocrinology. (2018) 87:204–14. doi: 10.1016/j.psyneuen.2017.10.022
8. Mayer SE, Lopez-Duran NL, Sen S, Abelson JL. Chronic stress, hair cortisol and depression: a prospective and longitudinal study of medical internship. Psychoneuroendocrinology. (2018) 92:57–65. doi: 10.1016/j.psyneuen.2018.03.020
9. Rietschel L, Streit F, Zhu G. Hair cortisol in twins: heritability and genetic overlap with psychological variables and stress-system genes. Sci Rep. (2017) 7:15351. doi: 10.1038/s41598-017-11852-3
10. Prado-Gascó V, de la Barrera U, Sancho-Castillo S, de la Rubia-Ortí JE, Montoya-Castilla I. Perceived stress and reference ranges of hair cortisol in healthy adolescents. PloS ONE. (2019) 14:e0214856. doi: 10.1371/journal.pone.0214856
11. de Kruijff I, Noppe G, Kieviet N, Choenni V, Lambregtse-van den Berg MP, Begijn DGA, et al. LC-MS/MS-based reference intervals for hair cortisol in healthy children. Psychoneuroendocrinology. (2020) 112:104539. doi: 10.1016/j.psyneuen.2019.104539
12. Petimar J, Rifas-Shiman SL, Hivert MF, Fleisch AF, Tiemeier H, Oken E. Prenatal and childhood predictors of hair cortisol concentration in mid-childhood and early adolescence. PloS ONE. (2020) 15:e0228769. doi: 10.1371/journal.pone.0228769
13. Wagner M, Kratzsch J, Vogel M, Peschel T, Gaudl A, Ceglarek U, et al. Hair cortisol concentration in healthy children and adolescents is related to puberty, age, gender, and body mass index. Horm Res Paediatr. (2020) 92:237–44. doi: 10.1159/000504914
14. Petimar J, Rifas-Shiman SL, Hivert MF, Fleisch AF, Tiemeier H, Oken E. Childhood hair cortisol concentration and early teen cardiometabolic outcomes. Pediatr Obes. (2020) 15:e12592. doi: 10.1111/ijpo.12592
15. Barouki R, Gluckman PD, Grandjean P, Hanson M, Heindel JJ. Developmental origins of non-communicable disease: implications for research and public health. Environ Health: Glob Access Sci Source. (2012) 11:42. doi: 10.1186/1476-069X-11-42
16. Wright RJ. Stress and atopic disorders. J Allergy Clin Immunol. (2005) 116:1301–6. doi: 10.1016/j.jaci.2005.09.050
17. Chmielewski PP, Strzelec B. Elevated leukocyte count as a harbinger of systemic inflammation, disease progression, and poor prognosis: a review. Folia Morphol. (2018) 77:171–8. doi: 10.5603/FM.a2017.0101
18. Milam J, Slaughter R, Verma G, McConnell R. Hair cortisol, perceived stress and dispositional optimism: a pilot study among adolescents. J Trauma Stress Disord Treat. (2014) 3:1000126. doi: 10.4172/2324-8947.1000126
19. Evans BE, Huizink AC, Greaves-Lord K, Tulen JHM, Roelofs K, van der Ende J. Urbanicity, biological stress system functioning and mental health in adolescents. PloS ONE. (2020) 15:e0228659. doi: 10.1371/journal.pone.0228659
20. Evans BE, Beijers R, Hagquist C, de Weerth C. Childhood urbanicity and hair steroid hormone levels in ten-year-old children. Psychoneuroendocrinology. (2019) 102:53–7. doi: 10.1016/j.psyneuen.2018.11.039
21. Robert SA. Socioeconomic position and health: the independent contribution of community socioeconomic context. Ann Rev Sociol. (1999) 25:489–516. doi: 10.1146/annurev.soc.25.1.489
22. Tonne C, Adair L, Adlakha D, Anguelovski I, Belesova K, Berger M, et al. Defining pathways to healthy sustainable urban development. Environ int. (2021) 146:106236. doi: 10.1016/j.envint.2020.106236
23. Liu J, Bisschop PH, Eggels L, Foppen E, Fliers E, Zhou JN, et al. Intrahypothalamic estradiol modulates hypothalamus-pituitary-adrenal-axis activity in female rats. Endocrinology. (2012) 153:3337–44. doi: 10.1210/en.2011-2176
24. Oyola MG, Handa RJ. Hypothalamic–pituitary–adrenal and hypothalamic–pituitary–gonadal axes: sex differences in regulation of stress responsivity. Stress. (2017) 20:476–94. doi: 10.1080/10253890.2017.1369523
25. Schoeters G, Hond E Den, Colles A, Loots I, Morrens B, Keune H, et al. Concept of the Flemish human biomonitoring programme. Int J Hyg Environ Health. (2012) 215:102–8. doi: 10.1016/j.ijheh.2011.11.006
26. Stalder T, Steudte-Schmiedgen S, Alexander N, Klucken T, Vater A, Wichmann S, et al. Stress-related and basic determinants of hair cortisol in humans: a meta-analysis. Psychoneuroendocrinology. (2017) 77:261–74. doi: 10.1016/j.psyneuen.2016.12.017
27. Verheyen VJ, Remy S, Lambrechts N, Govarts E, Colles A, Poelmans L, et al. Residential exposure to air pollution and access to neighborhood greenspace in relation to hair cortisol concentrations during the second and third trimester of pregnancy. Environ Health. (2021) 20:11. doi: 10.1186/s12940-021-00697-z
28. De Vos K, Zaidi MA. Equivalence scale sensitivity of poverty statistics for the Member States of the European Community. Rev Income Wealth. (1997) 43:319–33. doi: 10.1111/j.1475-4991.1997.tb00222.x
29. Eurostat. Methodological Manual on Territorial Typologies. (2018). Available online at: https://doi.org/10.2785/228845
30. Den Hond E, Paulussen M, Geens T, Bruckers L, Baeyens W, David F, et al. Biomarkers of human exposure to personal care products: results from the Flemish environment and health study. (FLEHS 2007-2011). Sci Total Environ. (2013) 463–464:102–10. doi: 10.1016/j.scitotenv.2013.05.087
31. Statistics Flanders. Metadata Armoede. (2018). Available online at: https://www.statistiekvlaanderen.be/nl/kansarmoede-index-van-kind-en-gezin.
32. Roelants M, Hauspie R, Hoppenbrouwers K. References for growth and pubertal development from birth to 21 years in Flanders, Belgium. Ann Hum Biol. (2009) 36:680–94. doi: 10.3109/03014460903049074
33. Asher MI, Keil U, Anderson HR, Beasley R, Crane J, Martinez F, et al. International study of asthma and allergies in childhood. (ISAAC): rationale and methods. Eur Respir J. (1995) 8:483–91. doi: 10.1183/09031936.95.08030483
34. Goodman R. Psychometric properties of the strengths and difficulties questionnaire. J Am Acad Child Adolesc Psychiatry. (2001) 40:1337–45. doi: 10.1097/00004583-200111000-00015
35. Vugteveen J, de Bildt A, Theunissen M, Reijneveld M, Timmerman M. Validity aspects of the strengths and difficulties questionnaire (SDQ). Adolescent self-report and parent-report versions among dutch adolescents. Assessment. (2019) 28:601–16. doi: 10.1177/1073191119858416
36. Brown LF, Kroenke K, Theobald DE, Wu J. Comparison of SF-36 vitality scale and fatigue symptom inventory in assessing cancer-related fatigue. Support Care Cancer. (2011) 19:1255–9. doi: 10.1007/s00520-011-1148-2
37. Braekman E, Berete F, Charafeddine R, Demarest S, Drieskens S, Gisle L, et al. Measurement agreement of the self-administered questionnaire of the belgian health interview survey: paper-and-pencil versus web-based mode. PloS ONE. (2018) 13:e0197434. doi: 10.1371/journal.pone.0197434
38. Kock N, Lynn GS. Lateral collinearity and misleading results in variance-based sem: an illustration and recommendations. JAIS. (2012) 13. doi: 10.17705/1jais.00302
39. Wilcox R. Trimming Winsorization. In: Armitage P, Colton T, editors. Encyclopedia of Biostatistics. (2nd ed.). Chichester, West Sussex, England, Hoboken, NJ: John Wiley (2005).
40. Bossé S, Stalder T, D'Antono B. Childhood trauma, perceived stress, and hair cortisol in adults with and without cardiovascular disease. Psychosom Med. (2018) 80:393–402. doi: 10.1097/PSY.0000000000000569
41. Rippe RCA, Noppe G, Windhorst DA, Tiemeier H, van Rossum EFC, Jaddoe VWV, et al. Splitting hair for cortisol? associations of socio-economic status, ethnicity, hair color, gender and other child characteristics with hair cortisol and cortisone. Psychoneuroendocrinology. (2016) 66:56–64. doi: 10.1016/j.psyneuen.2015.12.016
42. Short SJ, Stalder T, Marceau K, Entringer S, Moog NK, Shirtcliff EA, et al. Correspondence between hair cortisol concentrations and 30-day integrated daily salivary and weekly urinary cortisol measures. Psychoneuroendocrinology. (2016) 71:12–18. doi: 10.1016/j.psyneuen.2016.05.007
43. Benjamini Y, Hochberg Y. Controlling the false discovery rate: a practical powerful approach to multiple testing. J R Stat Soc Series B Stat Methodol. (1995) 57:289–300. doi: 10.1111/j.2517-6161.1995.tb02031.x
44. Steunpunt Milieu en Gezondheid. Vlaamse Humane-Biomonitoringprogramma 2016-2020: Referentiewaarden Bij Jongeren. (2020). Available online at: https://www.milieu-en-gezondheid.be/nl/onderzoeksresultaten
45. Statbel Onderwijsniveau. Available online at: https://statbel.fgov.be/nl/themas/werk-opleiding/opleidingen-en-onderwijs/onderwijsniveau.
46. Morrens B, Bruckers L, Hond E Den, Nelen V, Schoeters G, Baeyens W, et al. Social distribution of internal exposure to environmental pollution in Flemish adolescents. Int J Hyg Environ Health. (2012) 215:474–81. doi: 10.1016/j.ijheh.2011.10.008
47. Gys C, Bastiaensen M, Bruckers L, Colles A, Govarts E, Martin LR, et al. Determinants of exposure levels of bisphenols in Flemish adolescents. Environ Res. (2020) 193:110567. doi: 10.1016/j.envres.2020.110567
48. Kindengezin Lokaal dashboard kansarmoede. Available online at: https://www.opgroeien.be/cijfers-en-publicaties/kansarmoede/gemeentelijk-niveau.
49. Eurostat - Data Explorer. DEGURBA. Available online at https://appsso.eurostat.ec.europa.eu/nui/show.do?dataset=urb_ctour&lang=en (accessed January 7, 2021).
50. Gisle L, Drieskens S, Demarest S, Van der Heyden J. Geestelijke gezondheid: gezondheidsenquête 2018. Brussel, België: Sciensano; Rapportnummer: D/2020/14.440/4. Available online at: https://his.wiv-isp.be/nl/SitePages/Introductiepagina.aspx.
51. Binz TM, Rietschel L, Streit F, Hofmann M, Gehrke J, Herdener M, et al. Endogenous cortisol in keratinized matrices: systematic determination of baseline cortisol levels in hair and the influence of sex, age and hair color. Forensic Sci Int. (2018) 284:33–8. doi: 10.1016/j.forsciint.2017.12.032
52. Groeneveld MG, Vermeer HJ, Linting M, Noppe G, Van Rossum EFC, Van IJzendoorn MH. Children's hair cortisol as a biomarker of stress at school entry. Stress. (2013) 16:711–5. doi: 10.3109/10253890.2013.817553
53. Karlén J, Frostell A, Theodorsson E, Faresjö T, Ludvigsson J. Maternal influence on child HPA axis: a prospective study of cortisol levels in hair. Pediatrics. (2013) 132:e1333–e40. doi: 10.1542/peds.2013-1178
54. Kang JY, Park JY, Chun SI, Suh HS, Lee K, Ahn RS. Puberty-related changes in cortisol, dehydroepiandrosterone, and estradiol-17β secretions within the first hour after waking in premenarcheal girls. Neuroendocrinology. (2014) 99:168–77. doi: 10.1159/000363368
55. Stalder T, Kirschbaum C. Analysis of cortisol in hair – state of the art and future directions. Brain Behav Immun. (2012) 26:1019–29. doi: 10.1016/j.bbi.2012.02.002
56. Van Aart CJC, Michels N, Sioen I, De Decker A, Bijnens EM, Janssen BG, et al. Residential landscape as a predictor of psychosocial stress in the life course from childhood to adolescence. Environ Int. (2018) 120:456–63. doi: 10.1016/j.envint.2018.08.028
57. Kessler RC, Angermeyer M, Anthony JC, De Graaf R, Demyttenaere K., Gasquet I., et al. Lifetime prevalence and age-of-onset distributions of mental disorders in the World Health Organization's World Mental Health Survey Initiative. World Psychiatry. (2007) 6:168–76.
58. Kudielka BM, Kirschbaum C. Sex differences in HPA axis responses to stress: a review. Biol Psychol. (2005) 69:113–32. doi: 10.1016/j.biopsycho.2004.11.009
59. De Coster S, van Leeuwen DM, Jennen DGJ, Koppen G, Den Hond E, Nelen V, et al. Gender-specific transcriptomic response to environmental exposure in flemish adults. Environ Mol Mutagen. (2013) 54:574–88. doi: 10.1002/em.21774
60. Pedersen CB, Mortensen PB. Urbanization and traffic related exposures as risk factors for Schizophrenia. BMC psychiatry. (2006) 6:2. doi: 10.1186/1471-244X-6-2
61. Marcelis M, Navarro-Mateu F, Murray R, Selten JP, Van Os J. Urbanization and psychosis: a study of 1942-1978 birth cohorts in The Netherlands. Psychol Med. (1998) 28:871–9. doi: 10.1017/S0033291798006898
62. Lindroth M, Lundqvist R, Lilja M, Eliasson M. Cardiovascular risk factors differ between rural and urban Sweden: the 2009 Northern Sweden MONICA cohort. BMC Public Health. (2014) 14:825. doi: 10.1186/1471-2458-14-825
63. O'Neal WT, Sandesara PB, Kelli HM, Venkatesh S, Soliman EZ. Urban-rural differences in mortality for atrial fibrillation hospitalizations in the United States. Heart rhythm. (2018) 15:175–9. doi: 10.1016/j.hrthm.2017.10.019
64. Thomson EM, Christidis T, Pinault L, Tjepkema M, Colman I, Crouse DL, et al. Self-rated stress, distress, mental health, and health as modifiers of the association between long-term exposure to ambient pollutants and mortality. Environ Res. (2020) 191:109973. doi: 10.1016/j.envres.2020.109973
65. Bigert C, Bluhm G, Theorell T. Saliva cortisol - a new approach in noise research to study stress effects. Int J Hyg Environ Health. (2005) 208:227–30. doi: 10.1016/j.ijheh.2005.01.014
66. Verheyen V, Van den Eeden L, Lambrechts N, Remy S, Govarts E, Nielsen F, et al. Residential proximity to major roads and neighbourhood green space in relation to biological stress in the second trimester of pregnancy in the IPANEMA cohort. Environ Epidemiol. (2019) 3:411–2. doi: 10.1097/01.EE9.0000610608.92959.d6
67. Robinson O, Tamayo I, de Castro M, Valentin A, Giorgis-Allemand L, Hjertager Krog N, et al. The urban exposome during pregnancy and its socioeconomic determinants. Environ Health Perspect. (2018) 126:077005. doi: 10.1289/EHP2862
Keywords: adolescents, chronic biological stress, determinants, hair cortisol concentration, Flemish environment and health study (FLEHS), neighborhood urbanicity
Citation: Verheyen VJ, Remy S, Govarts E, Colles A, Koppen G, Martin LR, Nielsen F, Bruckers L, Bijnens EM, Vos S, Morrens B, Coertjens D, Loots I, De Decker A, Franken C, Den Hond E, Nelen V, De Henauw S, Covaci A, Van Larebeke N, Teughels C, Nawrot TS and Schoeters G (2021) Determinants of Chronic Biological Stress, Measured as Hair Cortisol Concentration, in a General Population of Adolescents: From Individual and Household Characteristics to Neighborhood Urbanicity. Front. Public Health 9:669022. doi: 10.3389/fpubh.2021.669022
Received: 17 February 2021; Accepted: 14 October 2021;
Published: 23 November 2021.
Edited by:
Kin Bong Hubert Lam, University of Oxford, United KingdomReviewed by:
M. Jahangir Alam, University of Houston, United StatesTheodora Katsila, National Hellenic Research Foundation, Greece
Copyright © 2021 Verheyen, Remy, Govarts, Colles, Koppen, Martin, Nielsen, Bruckers, Bijnens, Vos, Morrens, Coertjens, Loots, De Decker, Franken, Den Hond, Nelen, De Henauw, Covaci, Van Larebeke, Teughels, Nawrot and Schoeters. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Veerle J. Verheyen, dmVlcmxlLnZlcmhleWVuQHZpdG8uYmU=