 Ching-Yao Tsai1,2,3†
Ching-Yao Tsai1,2,3† Tao-Hsin Tung
Tao-Hsin Tung Wei-Cheng Chen
Wei-Cheng Chen
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health , 04 November 2021
Sec. Aging and Public Health
Volume 9 - 2021 | https://doi.org/10.3389/fpubh.2021.665985
This article is part of the Research Topic Falls Prevention for Older People in Primary Care Settings View all 9 articles
Purpose: This study examined the association between storey of building and fall risk in older adults' residences and residents' level of fear of falling.
Methods: The National Health and Ageing Trends Study (NHATS) collected information that would provide an understanding of basic trends people aged 65 years and older. Using a longitudinal survey, the present study employed the first round of NHATS data that was collected in 2011. In the first round, 12,411 participants were enrolled, and 8,077 interviews were completed. The study sample sizes for falling and worry about falling are 6,153 and 6,142, respectively.
Results: Unadjusted analysis revealed that storey of building was a risk factor for fall and worry about falling. There was a higher prevalence for fall and worry about falling when subjects lived in single storey of building compared with the subjects live in multi-storey. Logistic regression analysis showed no highly significant between storey of building and the fall/fear of falling.
Conclusion: Several clinical factors independently were indicated pertaining to the fall and worry about falling in older adult's residences.
- The finding of this paper indicated that the storey of building may be a risk factor for falling and develop worry about falling among elderly.
- Why does this paper matter? The results of this study could be a suggestion when arranging the living environment of elderly.
Falls are a major public health concern in the older adult population. For elderly people who have fallen, the fear of more falls can lead to a vicious cycle as well as result in various health problems. Millions of older people aged 65 years or older fall every year, and such incidents can cause fatal and non-fatal injuries. According to research conducted by the Centres of Disease Control and Prevention (CDC), 2.8 million older people were treated in emergency departments in the United States (US) for fall injuries in 2014. In addition, more than 27,000 older adults died from falls. In addition, annual fall injury-related costs were approximately US$31 billion (1).
Fall risk is a characteristic or a situation that is more likely to induce a fall event than other factors (2). Fall risk could be differentiated into three categories: intrinsic factors (including history of falls, age, gender, living alone, ethnicity, medicines, impaired mobility and gait, psychological factors, nutritional factors, impaired cognition, visual impairments, and sedentary behaviour), extrinsic factors (including environmental factors, footwear and clothing, and inappropriate walking aids or assistive devices), and exposure to the risk of falling (3). Some studies have considered certain hazards that increase the risk of falling, such as tripping hazards, clutter, poor lighting, low or high cabinets, no grab bar installed in the toilets, and seating that is too low or soft (4–6). Based our limited knowledge there is no study has focused on the relationship between the storey of a building that elderly people live on and fall risk. The hypothesis of this study is that elderly who lived in multi-storey of building are more likely to experience falling or report fear of falling than those who lived in single floor. Understanding this association could be essential for fall avoidance interventions. Therefore, the present study examined the association between storey of buildings and fall risk in older adults' residences and residents' level of fear of falling.
In the United States, the National Health and Ageing Trends Study (NHATS) collected information that would provide an understanding of basic trends people aged 65 years and older. Trained personnel collected the data including gender, education level, race, living environment, marital status, and economic level, by interviewing elderly people enrolled in Medicare. Using a longitudinal survey, the present study employed the first round of NHATS data that was collected in 2011. There were 8,077 interviews were completed the survey in the first round. The study excluded missing data including those who do not know answers, skipping the questions and information not ascertained. The sample sizes for falling and worry about falling are 6,153 and 6,142, respectively.
The NHATS is a publicly available data set accessed by registering online (access http://www.nhats.org) and downloading the data files for research proposes. Additional demographic data that were viewed as sensitive, such as age, were available through a simple application process. The University of Washington Human Subjects Division established that the current study did not meet the definition of research concerning human participants because the data were identified. In this study, all procedures were performed in accordance with the guidelines of our institutional ethics committee and adhered to the tenets of the Declaration of Helsinki. All patient information was anonymous. By using numerical codes for questionnaires and destroying the data in the study, the anonymity of participants and confidentiality of the responses was ensured.
This study examined the association between the storey of a building that elderly people live on and their fall risk. The question that “How many levels or floors are in your home?” were used to understand the storey of a building that participants lived. Meanwhile, there were several answers could be choose, including one, two, three, and more than fours. This study refined the data that elderly who live in single-floor of building when the answer was one; besides, the answer were others represented multi-storey building. The items that represented participants living in a multi-storey building included multi-unit building and other. In addition, although the NHATS did not present where falls occurred, falls defined as “any fall, slip, or trip in which you lose your balance and land on the storey or ground or at a lower level.” This study surveyed the fall or not in the past month and whether participants had worried about falling in the past month; two possible answers could be given for both items, namely yes or no.
The database in this study was used to examine the relationship between people living in single or multi-storey building vs. falling as well as the worry about falling. There were plenty of risk factors have been recognised in other studies (2–13). After refer to those studies, we conducted various independent variables are considered as potential associated factors such as gender, age, living arrangement, had knee surgery and various health condition for falling or worried about falling. Female elderly and people who were getting were more likely experienced falling and reported fear of falling. Besides, health conditions were also associated with falling or worried about falling.
All the non-response and inapplicable data are replaced in missing value. SPSS 22.0 was used for data management and to conduct statistical analysis. Chi-square (χ2-test) and an unadjusted odds ratio (OR) were estimated and 95% confidence interval (CI) was used to compare the relationship between storey residence, fall or not, and level of worry about falling in the past month in participants who chose to live on the single storey vs. those who chose to live on multi-storey. Multiple logistic regression was also performed in order to investigate the independence of risk factors associated with the falling or worry about falling. A p-value of <0.05 was considered to represent a statistically significant difference among test populations.
On one hand, the overall prevalence of fall was 10.6% (652/6,153) last month. Subjects lived in single storey of building (342/2,983 = 11.5%) had a higher prevalence for fall compared with the subjects live in multi-storey (1: 194/1,850 = 10.5%; 2: 97/1,129 = 8.6%; 3 or more: 19/191 = 9.9%). There were no statistically significant storey differences for fall among elderly (p-value = 0.06).
On the other hand, although there was no storey difference (p = 0.07) for the prevalence of worrying about the fall, elder subjects lived in single storey of building had a relative higher probability (30.1%, 896/2,980) of worrying about falling than multi-storey (1: 495/1,845 = 26.8%; 2: 310/1,126 = 27.5%; 3 or more: 51/191 = 26.7%).
Table 1 presents the unadjusted odds ratios for the association between certain relevant associated risk factors and the prevalence of fall. Compared to individuals without fall, in addition to storey (multiple vs. singles, OR = 0.83 [95%CI: 0.71–0.98]) and age (70–74 years vs. 65–69, OR = 1.83 [95%CI: 1.41–2.36], 75–79 vs. 65–69, OR = 2.10 [95%CI: 1.62–2.72], 80–84 vs. 65–69, OR = 1.65 [95%CI: 1.29–2.11], 85+ vs. 65–69, OR = 1.23 [95%CI: 0.97–1.54]), subjects featuring fall revealed a more-pronounced prevalence of: higher heart attack (yes vs. no, OR = 1.52 [95%CI: 1.23–1.86]), higher heart disease (yes vs. no, OR = 1.65, 95%CI: 1.36–1.99), higher blood pressure (yes vs. no, OR = 1.22 [95%CI: 1.02–1.46]), higher arthritis (yes vs. no, OR = 2.00 [95%CI: 1.68–2.39]), higher osteoporosis (yes vs. no, OR = 1.32 [95%CI: 1.09–1.60]), higher diabetes mellitus (yes vs. no, OR = 1.54 [95%CI: 1.29–1.83]), higher lung disease (yes vs. no, OR = 1.69 [95%CI: 1.38–2.07]), higher stroke (yes vs. no, OR = 2.10 [95%CI: 1.70–2.59]), higher dementia (yes vs. no, OR = 2.94 [95%CI: 2.28–3.80]), and higher knee surgery (yes vs. no OR = 1.53 [95%CI: 1.25–1.88]).
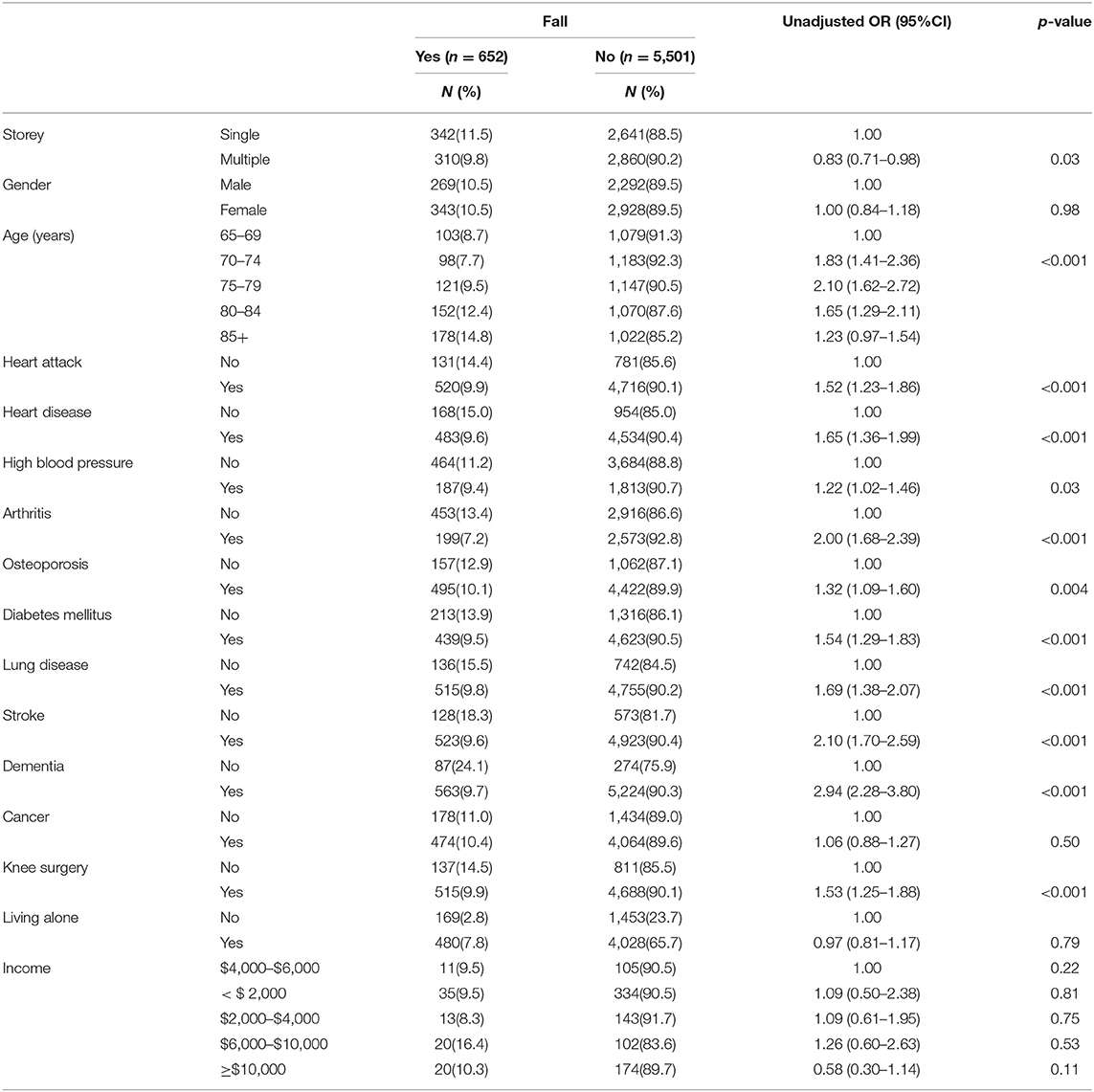
Table 1. Univariate analysis on the factors associated with fall in the past month (n = 6,153).
Table 2 indicates the unadjusted odds ratios for the association between certain relevant associated risk factors and the prevalence of worrying about fall. The significant factors related to worrying about fall included storey (multiple vs. singles, OR = 0.86 [95%CI: 0.77–0.96]), gender (female vs. male, OR = 0.57 [95%CI: 0.51–0.65]), age (70–74 years vs. 65–69, OR = 3.02 [95%CI: 2.51–3.63], 75–79 vs. 65–69, OR = 2.74 [95%CI: 2.30–3.27], 80–84 vs. 65–69, OR = 2.13 [95%CI: 1.80–2.53], 85+ vs. 65–69, OR = 1.53 [95%CI: 1.30–1.81]), heart attack (yes vs. no, OR = 1.82 [95%CI: 1.59–2.09]), heart disease (yes vs. no, OR = 1.71, 95%CI: 1.51–1.94), high blood pressure (yes vs. no, OR = 2.71 [95%CI: 2.41–3.06]), arthritis (yes vs. no, OR = 2.05 [95%CI: 1.80–2.34]), osteoporosis (yes vs. no, OR = 1.48 [95%CI: 1.31–1.68]), diabetes mellitus (yes vs. no, OR = 1.67 [95%CI: 1.44–1.94]), lung disease (yes vs. no, OR = 2.08 [95%CI: 1.77–2.45]), stroke (yes vs. no, OR = 2.42 [95%CI: 1.95–3.01]), dementia (yes vs. no, OR = 1.15 [95%CI: 1.01–1.30]), cancer (yes vs. no, OR = 1.48 [95%CI: 1.27–1.71]), and knee surgery (yes vs. no OR = 1.39 [95%CI: 1.20–1.61]).
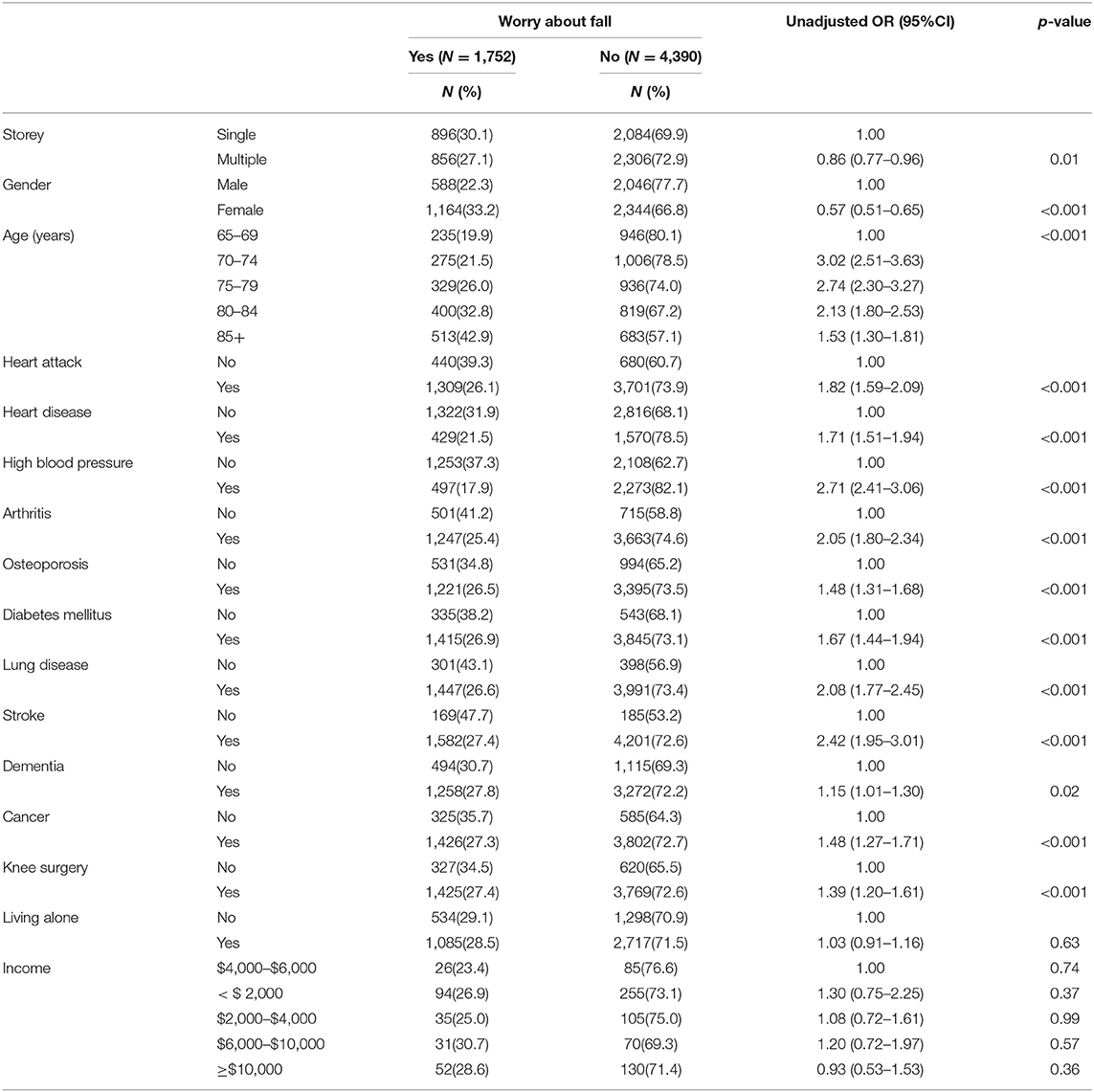
Table 2. Univariate analysis on the factors associated with worry about fall (n = 6,142).
The effect of independent associated risk factors on fall was examined using a multiple logistic regression model. As depicted in Table 3, subsequent to adjustment for confounding factors, the following appeared to be significantly related to fall prevalence: age (85+ years vs. 65–69 years, adjusted OR = 1.43 [95 CI: 1.09–1.88]), arthritis (yes vs. no, adjusted OR = 1.64 [95%CI: 1.37–1.97]), diabetes mellitus (yes vs. no, adjusted OR = 1.45 [95%CI: 1.20–1.74]), lung disease (yes vs. no, adjusted OR = 1.51 [95%CI: 1.22–1.87]), stroke (yes vs. no, adjusted OR = 1.54 [95%CI: 1.23–1.93]), dementia (yes vs. no, adjusted OR = 2.17 [95%CI: 1.64–2.85]), and knee surgery (yes vs. no, adjusted OR = 1.38 [95%CI: 1.12–1.71]).

Table 3. Multiple logistic regression model of fall in the past month (n = 6,153).
The effects of the independent associated factors of worry about fall were also examined by the multiple logistic regression model (Table 4). Independent factors of worry about fall included gender (female vs. male, adjusted OR = 0.71 [95%CI: 0.62–0.81]), age (80–84 years vs. 65–69 years, adjusted OR = 1.65 [95 CI: 1.35–2.01], 85+ years vs. 65–69 years, adjusted OR = 2.48 [95 CI: 2.03–3.02]), heart attack (yes vs. no, adjusted OR = 1.36 [95%CI: 1.16–1.58]), heart disease (yes vs. no, adjusted OR = 1.35 [95%CI: 1.18–1.55]), high blood pressure (yes vs. no, adjusted OR = 2.10 [95%CI: 1.85–2.39]), arthritis (yes vs. no, adjusted OR = 1.51 [95%CI: 1.30–1.75]), osteoporosis (yes vs. no, adjusted OR = 1.40 [95%CI: 1.22–1.61]), diabetes mellitus (yes vs. no, adjusted OR = 1.41 [95%CI: 1.20–1.65]), lung disease (yes vs. no, adjusted OR = 1.53 [95%CI: 1.28–1.83]), stroke (yes vs. no, adjusted OR = 1.45 [95%CI: 1.15–1.84]), and knee surgery (yes vs. no, adjusted OR = 1.20 [95%CI: 1.02–1.41]) after adjustment for confounding factors.
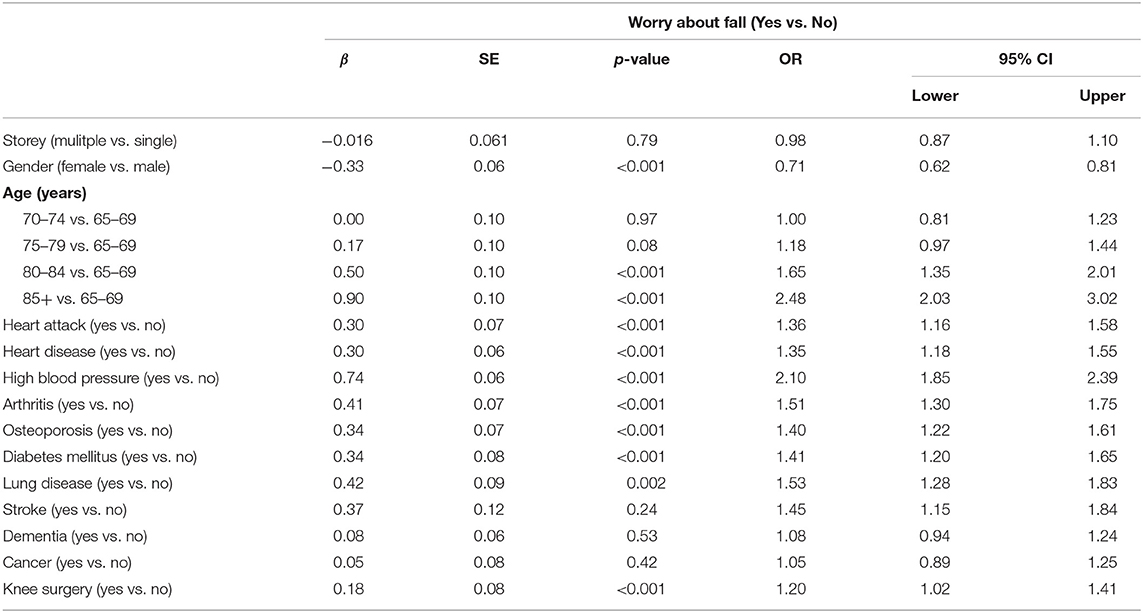
Table 4. Multiple logistic regression model of worry about fall (n = 6,142).
Falls are the leading cause of injury in the elderly population. A serious fall could result in decreased independent function and quality of life. Hip fractures in particular are a serious consequence of falling that could be devastating in older subjects. Table 5 presents the outcome evaluation of fall in older adults' residences in various populations (7–14). In this study, the results revealed that older adults who lived in multi-storey of buildings were not more worried about falling than lived in single-storey. Although the reason why older adults would not worry about the fall when they living in more than one storey of building was not clear, we supposed that disabled elderly who were inclined to experience falling or reported fear of falling were more likely to live in one storey of building. On the other hand, the barriers and safety conditions were difference between single-storey and multi-storey houses.
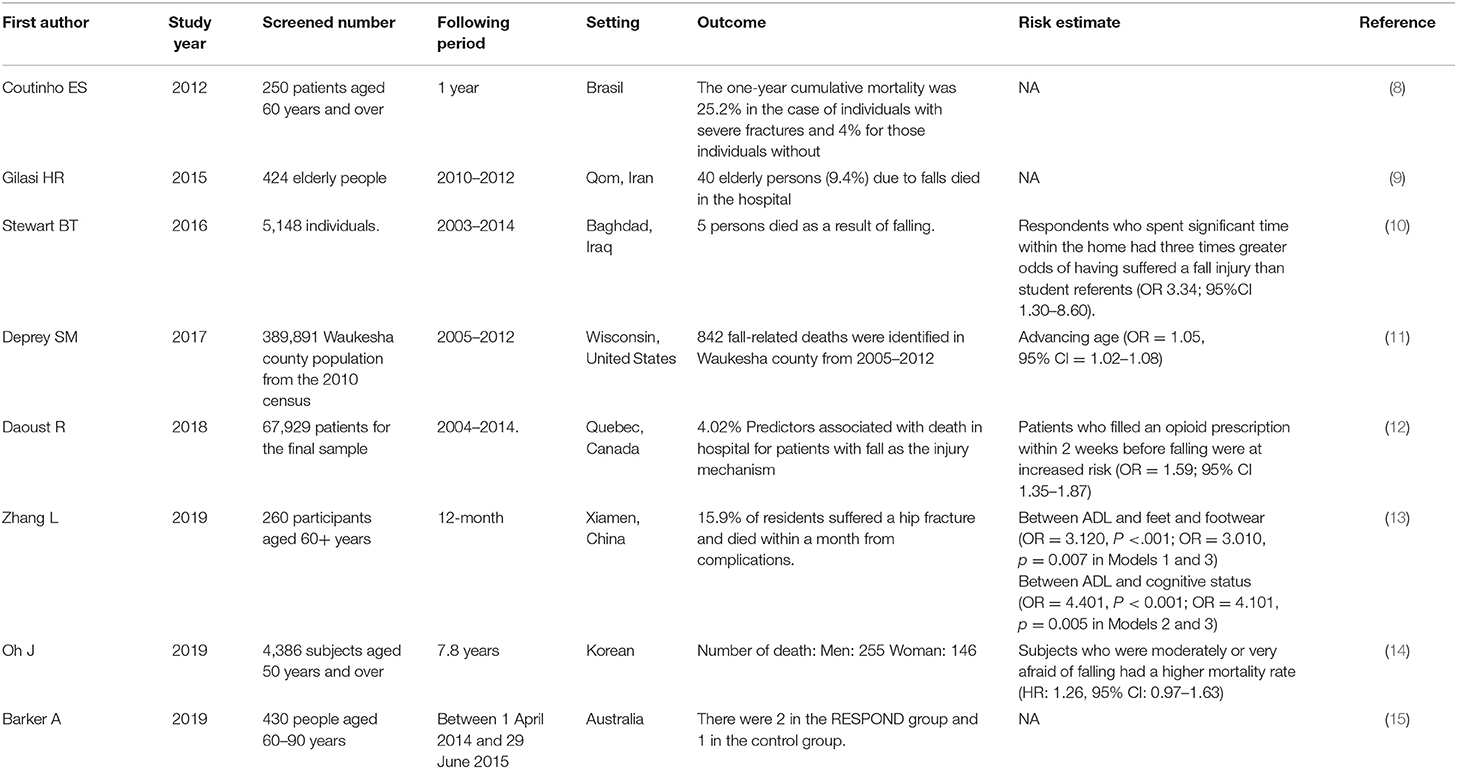
Table 5. The outcome evaluation of fall in older adults' residences in various populations.
From the clinical viewpoint, previous studies reported that physical inactivity can increase depressive symptoms and a significant association between physical inactivity and major non-communicable diseases, such as coronary heart disease, type 2 diabetes, breast cancers and colon cancers, which can also shorten life expectancy (15, 16). There were several risk factors for falls in older adults has been recognised (17–25). However, no study has assessed the relationship between the storey on which elderly people live on and other fall-related variables such as fall risks and level of worry about falls. The results of this study revealed trend between storey number and falling, but it was not highly significant (p-value = 0.06). In addition, the association between storey number and participants' level of worry about falling also was not significant (p-value = 0.07). The results indicated that no significant relationship between the storey of a building, the risk of falling, and level of worry about fall compared with other related factors. Elderly peoples' physical ability could become increasingly restricted. In this study, we did not prove our hypothesis that elderly people who lived on higher storey worry more about falling because of the fear of going up and down stairs.
Although this study provided new insights into the relationship between the storey number of a building and level of worry about falling in elderly people, it still had several limitations. This study evaluated an extensive array of fall risk factors, however, some restrictions existed in the NHATS investigation, such as the lack of data on environmental factors, footwear and clothing, inappropriate walking aids or assistive devices, and gait. Secondly, the misclassification bias of on floor number from 0 to 3, etc. could be occurred. In this study, to get classified as living in a multi-storey building, it is clear to form this that participants would be classified as multi-storey, even if they lived on the ground floor of a multi-storey building. While one possibility for being classified as single-storey living was that participants lived in a “free-standing single house”: this mean it would have to be a bungalow with only one storey, or could this term include two storey houses with bedrooms upstairs, a standard house in the UK. If single storey does include two storey houses, then some of the participants in the single storey group would have to climb stairs to get to bed. Hence, the results detailed may differ if applied to specific floors. Thirdly, the missing response of fall or worry about fall are not only low it strengthens study results, but also if the numbers drop off considerably it is an indication of potential selection bias. Fourthly, no information about stair lifts does indicate a another weakness of the study, as whether or not a multi-storey home has an elevator, is clearly important in relation to fall risk and fear of fall in the home and the lack of this information may explain why we failed to find an association. Fifthly, the data from NHATS were secondary that may deduce the link between each risk factor, including the storey of building. Besides, this was a cross-sectional study, which limited its ability to draw causal inferences. To conduct a number of prospective longitudinal analogous studies could solute such a quandary would best be accomplished. The results of which would be also expected to complement the cross-sectional findings of this study. However, one key variable that could be collected over time is falling. In a different type of study, they could have asked participants to complete falls diaries. It is not clear whether residence is likely to change greatly over time, that is their status in relation to the floor they live on might not change. A change in residence (to institutional care) would for many people indicate a deterioration in the condition, and this might be picked up as a move from a house to multi-storey accommodation, which could confound a floor of residence analysis.
Several clinical factors independently were indicated pertaining to the falling and worry about falling in older adult's residences. Further studies not only are needed to evaluate the temporal sequence of events that typically lead to falling, but also studies should assess how gender-related differences are related of falling in older adult's residences.
The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number(s) can be found below: https://nhats.org/researcher/nhats.
C-YT, E-SL, T-HT, and W-CC conducted the study and drafted the manuscript. E-SL, Y-TL, T-HT, and W-CC participated in the design of the study and performed data analysis. C-YT, T-HT, and W-CC conceived the study and participated in its design and coordination. All of the authors read and approved the final manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Centers for Disease Control and Prevention (CDC). Home and Recreational Safety. (2016). Available from: https://www.cdc.gov/homeandrecreationalsafety/falls/adultfalls.html (accessed December 12, 2020).
2. Rubenstein LZ, Josephson KR. Risk factors for falls: a central role in prevention. Generations: J Am Soc Aging. (2002) 26:15–21. Available online at: https://www.jstor.org/stable/26555172
3. Todd C, Skelton D. What are the Main Risk Factors for Falls Amongst Older People and what are the Most Effective Interventions to Prevent These Falls? Geneva, Switzerland: World Health Organization (2004).
4. Sattin RW, Rodriguez JG, DeVito CA, Wingo PA. Home environmental hazards and the risk of fall injury events among community-dwelling older persons. J Am Geriatr Soc. (1998) 46:669–76. doi: 10.1111/j.1532-5415.1998.tb03799.x
5. Northridge ME, Nevitt MC, Kelsey JL, Link B. Home hazards and falls in the elderly: the role of health and functional status. Am J Public Health. (1995) 85:509–15. doi: 10.2105/AJPH.85.4.509
6. Kamei T, Kajii F, Yamamoto Y, Irie Y, Kozakai R, Sugimoto T, et al Effectiveness of a home hazard modification program for reducing falls in urban community-dwelling older adults: A randomized controlled trial. Jpn J Nurs Sci. (2015) 12:184–97. doi: 10.1111/jjns.12059
7. Coutinho ESF, Bloch KV, Coeli CM. One-year mortality among elderly people after hospitalization due to fall-related fractures: comparison with a control group of matched elderly. Cadernos de Saúde Pública. (2012) 28:801–5. doi: 10.1590/S0102-311X2012000400019
8. Gilasi HR, Soori H, Yazdani S, Tenjani PT. Fall-related injuries in community-dwelling older adults in Qom Province, Iran, 2010-2012. Arch Trauma Res. (2015) 4:e22925. doi: 10.5812/atr.22925
9. Stewart BT, Lafta R, Esa Al Shatari SA, Cherewick M, Flaxman A, Hagopian A, et al. Fall injuries in Baghdad from 2003 to 2014: results of a randomised household cluster survey. Injury. (2016) 47:244–9. doi: 10.1016/j.injury.2015.11.006
10. Deprey SM, Biedrzycki L, Klenz K. Identifying characteristics and outcomes that are associated with fall-related fatalities: multi-year retrospective summary of fall deaths in older adults from 2005–2012. Injury Epidemiol. (2017) 4:21. doi: 10.1186/s40621-017-0117-8
11. Daoust R, et al., Recent opioid use and fall-related injury among older patients with trauma. CMAJ, 2018. 190(16): p. E500–E506. doi: 10.1503/cmaj.171286
12. Zhang L, Zeng Y, Weng C, Yan J, Fang Y. Epidemiological characteristics and factors influencing falls among elderly adults in long-term care facilities in Xiamen, China. Medicine. (2019) 98:e14375. doi: 10.1097/MD.0000000000014375
13. Oh J, Choi CK, Kim SA, Kweon SS, Lee YH, Nam HS, et al. Association of falls and fear of falling with mortality in Korean adults: the Dong-gu study. Chonnam Med J. (2019) 55:104–8. doi: 10.4068/cmj.2019.55.2.104
14. Barker A, Cameron P, Flicker L, Arendts G, Brand C, Etherton-Beer C, et al., Evaluation of RESPOND, a patient-centred program to prevent falls in older people presenting to the emergency department with a fall: a randomised controlled trial. PLoS Med. (2019) 16:e1002807. doi: 10.1371/journal.pmed.1002807
15. Galper DI, Trivedi MH, Barlow CE, Dunn AL, Kampert JB. Inverse association between physical inactivity and mental health in men and women. Med Sci Sports Exer. (2006) 38:173–8. doi: 10.1249/01.mss.0000180883.32116.28
16. Lee I-M, Shiroma EJ, Lobelo F, Puska P, Blair SN, Katzmarzyk PT, et al. Effect of physical inactivity on major non-communicable diseases worldwide: an analysis of burden of disease and life expectancy. Lancet. (2012) 380:219–29. doi: 10.1016/S0140-6736(12)61031-9
17. Stevens JA, Sogolow ED. Gender differences for non-fatal unintentional fall related injuries among older adults. Injury Prev. (2005) 11:115–9. doi: 10.1136/ip.2004.005835
18. Peel NM, Kassulke D, McClure RJ Population based study of hospitalised fall related injuries in older people. Injury Prev. (2002) 8:280–3. doi: 10.1136/ip.8.4.280
19. Wei F, Hester AL. Gender difference in falls among adults treated in emergency departments and outpatient clinics. J Gerontol Geriatr Res. (2014) 3:152. doi: 10.4172/2167-7182.1000152
20. jin Choi E, Kim SA, Kim NR, Rhee JA, Yun YW, Shin MH. Risk factors for falls in older Korean adults: the 2011 Community Health Survey. J Korean Med Sci. (2014) 29:1482–7. doi: 10.3346/jkms.2014.29.11.1482
21. Sun DQ, Huang J, Varadhan R, Agrawal Y. Race and fall risk: data from the National Health and Aging Trends Study (NHATS). Age Ageing. (2016) 45:120–7. doi: 10.1093/ageing/afv173
22. Ashburn A, Hyndman D, Pickering R, Yardley L, Harris S. Predicting people with stroke at risk of falls. Age Ageing. (2008) 37:270–6. doi: 10.1093/ageing/afn066
23. Kerse N, Parag V, Feigin VL, McNaughton H, Hackett ML, Bennett DA, et al., Falls after stroke: results from the Auckland Regional Community Stroke (ARCOS) Study, 2002 to 2003. Stroke. (2008) 39:1890–3. doi: 10.1161/STROKEAHA.107.509885
24. Maggio D, Ruggiero C, Ercolani S, Macchiarulo MC, Palmari N, Luccioli F, et al. A multi-dimensional questionnaire quantifying quality of life in elderly osteoporotic women: the Italian triple-Q osteoporosis study. Aging Clin Exp Res. (2010) 22:330–9. doi: 10.1007/BF03324937
Keywords: fall, fear of fall (FOF), risk factors, older adults, storey of building
Citation: Tsai C-Y, Lin E-S, Li Y-T, Tung T-H and Chen W-C (2021) The Relationship Between Storey of Buildings and Fall Risk. Front. Public Health 9:665985. doi: 10.3389/fpubh.2021.665985
Received: 09 February 2021; Accepted: 13 October 2021;
Published: 04 November 2021.
Edited by:
Maw Pin Tan, University of Malaya, MalaysiaReviewed by:
Angela M. Goins, University of Houston–Downtown, United StatesCopyright © 2021 Tsai, Lin, Li, Tung and Chen. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Tao-Hsin Tung, Y2gyODc2QGdtYWlsLmNvbQ==; Wei-Cheng Chen, Z2V2aW43N0Bob3RtYWlsLmNvbQ==
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.