
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
BRIEF RESEARCH REPORT article
Front. Public Health , 20 May 2021
Sec. Public Health Education and Promotion
Volume 9 - 2021 | https://doi.org/10.3389/fpubh.2021.662313
 Cynthia Mikolas1,2†
Cynthia Mikolas1,2† Hope Winfield2,3†
Hope Winfield2,3† Lorraine Smith-MacDonald2,4†
Lorraine Smith-MacDonald2,4† Ashley Pike2,5
Ashley Pike2,5 Chelsea Jones2,4,6
Chelsea Jones2,4,6 Melina Lee7
Melina Lee7 Jennifer Griffiths2
Jennifer Griffiths2 Ryan Perry2David M. Olson8Alexandra Heber9,10Joanne Olson7‡
Ryan Perry2David M. Olson8Alexandra Heber9,10Joanne Olson7‡ Phillip R. Sevigny2,11‡
Phillip R. Sevigny2,11‡ Suzette Brémault-Phillips2,5*‡
Suzette Brémault-Phillips2,5*‡Introduction: A new vision of resilience and well-being for Canadian military service members (SMs), Veterans and their families has been championed by the Canadian Armed Forces (CAF) and Veterans Affairs Canada (VAC). Operationalizing this vision, which aims to support those who serve/have served and their families as they navigate life during and post-service, requires the support of service providers (SPs). Training SPs to deliver complementary resilience-training programs Reaching In… Reaching Out (RIRO; for adults working with parents of young children) and Bounce Back and Thrive! (BBT; for parents of children aged 0–8 years of age) may support this vision.
Objective: To assess the appropriateness of RIRO/BBT trainer training for SPs, and RIRO and BBT resilience-training for military populations and families.
Methods: This qualitative descriptive study involved the delivery of RIRO/BBT trainer training to SPs (n = 20), followed by focus groups (n = 6) with SPs and organisational leaders (n = 4). Focus groups were recorded, and data were transcribed and thematically-analysed.
Results: Several themes emerged: (1) RIRO/BBT trainer training enabled SPs to model resilience and deliver the resilience-training programs, (2) training was appropriate and adaptable for the CAF and SMs/CMFs, and (3) training could support the development of resilient communities.
Discussion: RIRO/BBT trainer training and RIRO and BBT resilience-training programs use a holistic, integrated, experiential, and community approach to resilience-building and align with CAF and VAC initiatives. Once contextualised, such programs could support resilience-building in the military context.
A new vision of resilience for Canadian military service members (SMs), Veterans and their families has been championed by the Canadian Armed Forces (CAF) and Veterans Affairs Canada (VAC). CAF has clearly indicated that “well-supported, diverse and resilient people and families” ((1), p. 19) are its first priority. Resilience, a process through which individuals adapt to or recover from adversity (2), enables service members (SM) to be operationally-ready for domestic and international peace-keeping and combat and disaster response missions, and for Canadian military families (CMFs) to support them. Resilience across multiple domains (i.e., physical, mental, ethical/spiritual, social/cultural, familial, financial) and environments (i.e., psychosocial work, physical work, and physical home) is therefore foundational to CAF operational readiness (3) (Table 1).
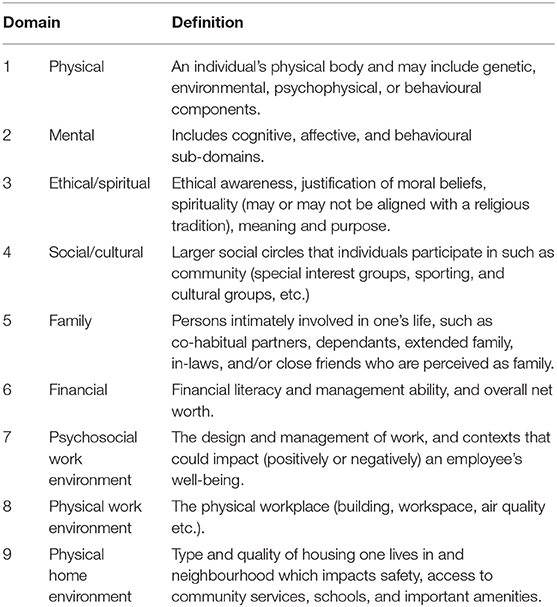
Table 1. Total health and wellness domains (3).
While the majority of CMFs manage stressors well, ~10% struggle (4–6) as they navigate military life challenges (e.g., mobility and relocation, risk of injury and illness and absence/separations). Prolonged or cumulative stressors heightens risk of family disruption and poorer health and well-being outcomes (5, 7). These stressors can impact family processes, parent–child attachment and (co)parenting during critical early childhood development (8). SMs/CMFs may benefit from resiliency programs informed by attachment and developmental–ecological frameworks that foster resilience across individual, family, and cultural contexts (8). For example, evidence indicates that resilience can be improved through programs that foster positive attachment and parent-child interactions, provide a safe, structured environment, and shift parenting attitudes and skills (8, 9). Moreover, resilience-training that is strength-based, trauma-informed, and peer-supported, and enables individuals to better navigate and thrive amidst adversity, model resilience, and contribute to building strong and resilient communities, can be powerful.
A community's sustained ability to mobilise, respond, and positively adapt to stress (individual, family, community), is affected by its resilience (10, 11). Facilitative environments that increase capacity, provide informal/formal support and resources, and decrease risks, unhealthy communication and trauma can contribute to community resilience (10, 12). According to Patel, core elements of community resilience include local knowledge, community networks and relationships, communication, health, governance/leadership, resources, economic investment, preparedness, and mental outlook (Table 2). Consideration of such elements is important when determining resilience-training programs that might foster community resilience.
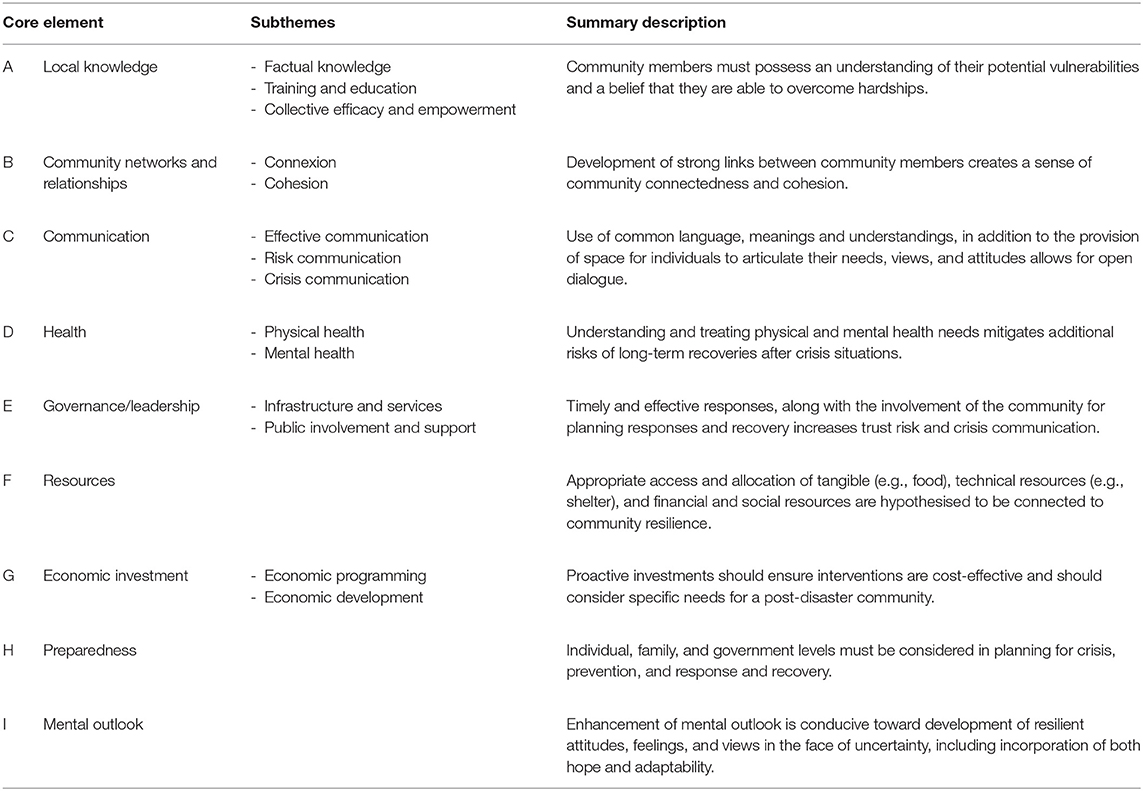
Table 2. Elements of community resilience as proposed by Patel et al. (12).
Within the military, community resilience is built through a “Triad of Responsibility” between the Chain of Command, care provider/team, and SMs/CMFs [(13), p. 11] characterises CAF's approach to health and wellness. Organisationally, CAF deploys tools, programs, and actions to enhance resilience at each stage of a SM's career and provides support for CMFs (1). Program delivery is tasked to service providers (SPs) associated with, for example, CAF Health Promotions [Strengthening the Forces Health Program (14)], military Chaplains (spiritual and familial support for SMs/CMFs), Personnel Support Services (PSP; fitness centres, libraries, camps), and Military Family Resource Centres (MFRCs; social and family services/programs).
A scan, however, of available programs and resources across diverse locations reveals SM/CMF service gaps regarding resilience-building (15).
Within the Canadian military context, potential resilience-training programs for future use with SMs/CMFs would need to be selected and evaluated using criteria such as relevance, efficiency, effectiveness, accessibility, fit, and usability. Other resilience-oriented programs are available in the CAF—most notably the Road to Mental Readiness (R2MR) program. The purpose of the R2MR program is to build awareness of mental illness and operational stress injuries (OSIs) through education, reduce stigma associated with mental illness, and increase understanding and support for these conditions (16). Two complementary made-in-Canada family-focused resilience programs are also being explored. Developed by Kordich-Hall and Pearson (17), Reaching In… Reaching Out (RIRO) is for SPs working with those engaging with parents of young children, and Bounce Back and Thrive! (BBT) is for parents of children 0–8 years of age (18).
RIRO and BBT are standardised, evidenced-informed programs based on the gold standard University of Pennsylvania's Resiliency Program (19). Group psychoeducational peer-supported programs, RIRO and BBT include topics such as fostering calming and focusing, thought-catching and reframing, challenging core beliefs, understanding thinking habits, and generating alternatives (see Table 3 for session topics and objectives of BBT and RIRO). BBT consists of 10, 2-h weekly sessions, while RIRO training is 12-h. RIRO and BBT are trauma-informed, and available in French, English and other languages. The programs have been introduced at one MFRC, utilised with trauma-affected populations, and delivered in person and online. RIRO and BBT have been found to enhance individual and community resilience and foster a culture of resilience (18).
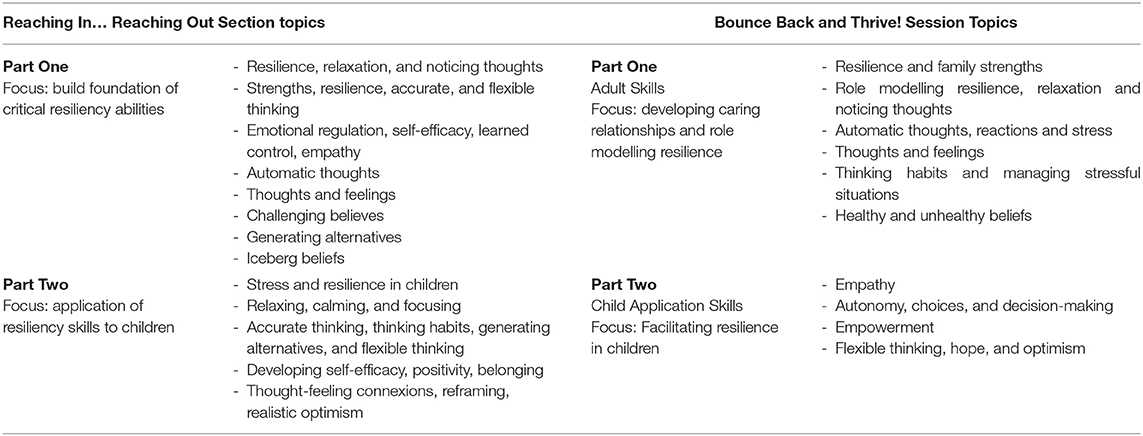
Table 3. Reaching In… Reaching Out and Bounce Back and Thrive! Sessions and objectives.
SPs can receive 40 h of RIRO/BBT trainer training to deliver RIRO and BBT that aims to familiarise them with the material, resources and skills, enhance their understanding of resilience and ability to model resilience, and prepare them to deliver the RIRO and BBT (18).
This study aims to capture the perspectives of SPs post-RIRO/BBT trainer training regarding (1) the impact of the training on their ability to model resilience and deliver RIRO and BBT; and the appropriateness of the RIRO and BBT programs for use with SMs/CMFs and military communities. Specifically, we will determine whether these programs might (2) address service/training gaps regarding resilience-building (3) lend themselves to contextualisation for military populations, and (4) foster a culture of resilience.
This study employed a qualitative descriptive research design. Following RIRO/BBT trainer training, audio-recorded focus groups (FGs) were conducted with trainees, the RIRO/BBT Master Trainer and organisational leaders. Ethical approval from a Research Ethics Board and CAF Surgeon General Endorsement were received prior to study initiation.
Study participants included SPs (n = 20) recruited from a local military base, MFRC, health authority, and University who were invited to participate in RIRO/BBT trainer training due to their roles supporting SMs/CMFs with children 0–8 years of age: MFRCs (n = 8; social workers, early child care workers), the Royal Canadian Chaplain Service (RCChS) (n = 5; chaplains, mental health chaplains), CAF transition unit (n = 1, SM), a family (n = 1; parent), the local health authority (n = 1; social worker), university-based researchers/clinician-scientists (n = 4; nurse, occupational therapist, psychologist, social worker). Organisational leaders from the MFRC (n = 2) and RCChS (n = 1), and the RIRO/BBT Master Trainer (n = 1), also participated in FGs.
RIRO/BBT trainer training was delivered in-person at the local MFRC for 5 days (September 9–13, 2019) by a RIRO/BBT Master Trainer to 20 trainees. RIRO-specific training occurred on Days 1–3 and BBT training on Days 4–5.
Data were collected during six FGs following RIRO/BBT trainer training using semi-structured interview questions. FG questions were based on study objectives and purposely broad and iterative so as to facilitate discussion (20). Questions included, “What was your experience of the program? What aspects of the program were the most/least helpful/impactful/effective? How might the program be improved/contextualised for CMFs?” FGs were facilitated by three research team members with 10 years' experience conducting FGs, while a fourth member recorded field notes. The facilitators actively engaged participants and encouraged sharing of opinions and experiences, while the observer monitored engagement, participation, and verbal and non-verbal cues (21, 22). Qualitative analysis occurred during and following the FGs through reflection and discussion (21, 22).
A FG with trainees and the Master Trainer was held at the end of training Day 5 (FG1; n = 21), followed in the 2 weeks thereafter with MFRC and RCChS leadership (FG2; n = 3), and a CMF member, transition unit SM, and research team members (FG3; n = 5). Organisation-specific FGs were conducted with trainees later in September and October 2019 (FG4 and FG5; n = 20) and in November 2020 (FG6; n = 3). In instances where participants were unable to attend due to operational commitments, participants provided feedback by email. The FGs were conducted in a private setting at the MFRC, lasted ~2 h, and were digitally recorded and transcribed verbatim by a transcriptionist. As participant identifiers were intentionally removed during the transcription process, quotes are identified by FG rather than participant.
The FG data were analysed using thematic analysis as described by Braun and Clarke (23). Braun and Clarke (23) argued that thematic analysis provides a flexible method for identifying, analysing, and reporting themes in rich detail. To ensure the validity, reliability, and conformability of the analysis, the data were thematically-analysed (inductively and deductively) by four research team members. This also ensured inter-rater reliability and bracketing of researcher bias (24). An audit trail was used to review and examine decisions and maintain credibility and rigour (25).
Initial coding was completed independently and by hand by two team members who had not conducted the FGs. Initial inductive open codes were then combined into preliminary themes focused on similarities and differences within and between FGs. Preliminary themes then underwent a secondary round of collective analysis by two other team members focused on deductive coding informed by study objectives, resilience domains, core community resilience elements (12) and the aforementioned evaluation criteria. Regular meetings enabled discussion, code verification, resolution of discrepancies and determination of final themes and supporting quotes.
Thematic analysis revealed several salient themes related to participants' experiences: (1) RIRO/BBT trainer training enhanced SPs' abilities to model resilience and deliver RIRO and BBT programs. RIRO and BBT programs (2) are useful for families and communities, (3) could assist in developing resilient environments, and (4) could be adapted for use with military populations. Themes support several of the total health and wellness domains and core elements of community resilience, with the potential for enhancement of local knowledge, community networks and relationships, communication, preparedness, and mental outlook being evident in participant feedback. Further discussion of themes follows, in addition to a table of prominent themes, subthemes, and supportive quotes, resilience domain and core elements (Table 4).
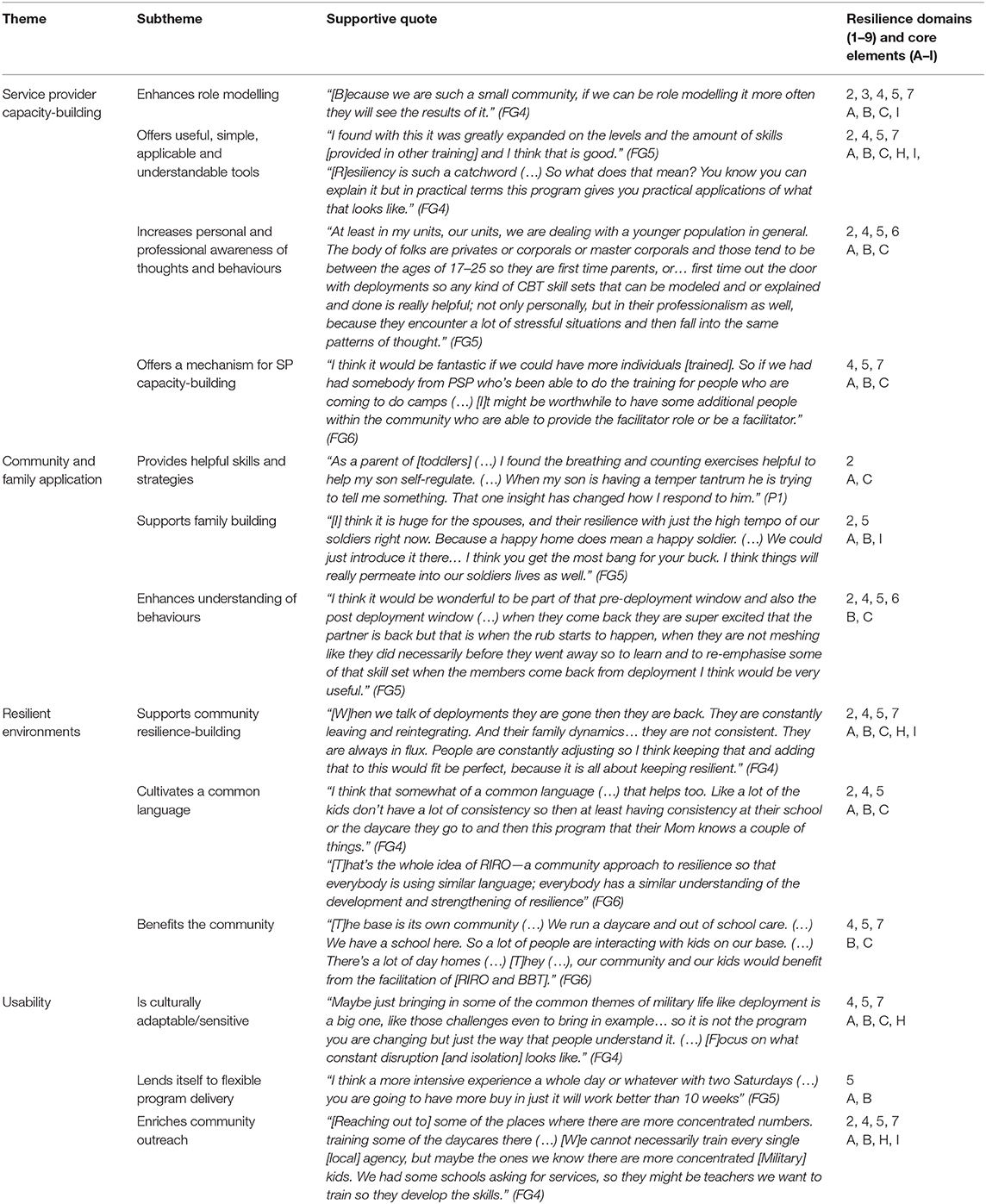
Table 4. Themes, subthemes, and supportive quotes and resilience domains/core elements.
Participants noted that resilience programs fostering adult modelling of resilience skills is currently lacking across bases and MFRCs. RIRO/BBT trainer training inspired them to more intentionally model resilience in their homes and workplaces: “[B]ecause we are such a small community, if we can be role modelling it more often they will see the results of it.” (FG4)
Participants found that the training offered relevant, useful, simple, applicable and understandable tools across resilience domains (i.e., physical, mental, ethical/spiritual, social/cultural, familial, financial) and the psychosocial work environment that, “everybody could use.” (FG5) The training expanded their knowledge and offered ways to alter tools, including using “[An aide memoire] like a cheat sheet or a quick refresher that you carry with you (…) the first page could be the 3Rs [or another learned tool] (…) After a while it becomes muscle memory and you don't need it.” (FG1) “[A]ctive breathing (…) is not necessarily a skill that everyone wants or practises (…) Fair enough. Here is another thing you can try.” (FG5) They also identified times, such as pre- and post-deployment, during which increased resilience skills may support CMFs, younger CAF members, and SMs across all ranks.
Participants indicated that the training enhanced their self-awareness, “Personal awareness… to understand my strengths and weaknesses. In terms of understanding different styles of thinking,” (FG5) and their own parenting: “[I]t was helpful to (…) pause and spend time thinking about your reaction as a parent and thinking about the children's reactions, and how that maybe we are not managing them in the best way.” (FG5)
The training offered participants an opportunity to gain insight into areas that they and others may need to develop: “I am trying to understand what might be struggles for people, (…) [and how and] when (…) to help (…) people improve their resiliency and (…) see that in-depth journey.” (FG5) It also equipped them with new strategies to “approach some topics… to help families and the members, (…) understand thought traps [thinking habits].” (FG5)
Participants saw benefit to involving SPs from various community partners to ensure widespread use of skills: “[I]t would be fantastic if we could have (…) additional people within the community who are able to (…) be a facilitator.” (FG6)
Participants believed that the training could “[H]elp [SMs] to recognise their emotions, how they think and then give them the necessary tools to correct and adjust their behaviour and thought processes.” (P1) They recommended that the tools be taught in basic training as it would, “[S]et a healthy thought pattern and provide each member with coping skills.” (P1) Another participant noted, “Chapters 1–3 of RIRO should be mandatory for all ranks. The information in it is probably some of the best building blocks I've seen.” (FG3) In addition to providing regulation tools, they recognised the impact of equipping adults with resilience skills that can be used across all domains with their children and across the lifespan.
Strengthening CMFs is important to developing community resilience. Participants related that BBT supports family-building as it is, “[V]ery family-oriented (…) and is presented in a language that speaks well to that demographic.” (FG6) It could be useful in “[T]eaching parents to know themselves and self-regulate. And then in turn help their kids to self-regulate and express when they are having difficulty.” (FG5)
Participants noted improvements in their own families as a result of role modelling, “[A]s my wife would say, I often would (…) dad-splain (…) to help [my children] through whatever they are feeling. (…) [RIRO] provided me with a language and the avenue for engagement with my children that I was lacking (…) and it has made a very positive impact on my relationship with my kids.” (FG5)
Participants identified specific periods of time, such as pre- and post-deployment windows, where increased resilience skills may be beneficial in supporting families to understand patterns of behaviour: “[I]t would be wonderful (…) pre-deployment (…) and (…) post deployment (…) when they are not meshing like they did necessarily before they went away.” (FG5)
“[The CMF community] is the environment that the kids are in and the people who are with them all the time.” (FG6) As community members often support each other amidst frequent change, uncertainty, relocation, deployments, extended absences of a parent/caregiver, and lack of SP and program continuity from one location to the next, equipping CMF communities with resilience tools is essential. Participants noted that families have been struggling to cope with the increased tempo of operations, indicating that, “[W]e are to support our families to figure out tools to help them to survive the military profession or at least until the tempo comes down and they are not so busy.” (FG5) Participants noted that access to resilience programs addressing adult modelling of resilience skills to children and child resilience skill-building is currently needed across bases and MFRCs: “[C]hildren are constantly adjusting. (…) So building up resiliency skills for children is a good thing.” (FG4)
The benefits that standard evidence-based resilience programs offer regarding use of a common language were also noted: “It would be good to have all the staff trained in it so we have the same style or the same verbiage with children that come into our care. Or even families that we're trying to help them build their resiliency skills.” (FG4)
Participants recognised the benefits that RIRO/BBT trainer training might have for other SPs, “[PSP] staff at the library, (…) they see enough [children/CMFs] that it would be great to have some of those people [trained]” (FG6), and the ways in which RIRO and BBT might complement other programs: “We have health promotions here. They run a lot of programs. [T]here's bits and pieces (…) but not a complete program like [RIRO/BBT].” (FG6) RIRO and BBT appear to align with existing CAF and MRFC program offerings and would address a service gap.
Participants noted that RIRO and BBT content would need to be contextualised for the military populations: “[T]he language, (…), some of the examples, need to change for it to communicate better to our soldiers.” (FG5) “Examples I think would be worthwhile because it may be easier for someone to pick it up, but outside of that they've tested this all across trauma, significant trauma communities. Why would we be any different? (…) It's the nominal changes to update the program vs. militarise it.” (FG2). Additionally, participants noted that, “[A]ctivities could be altered so they are a little bit more (…) military-friendly.” (FG4) Changes training content and material to neutralise gender could also be helpful: “If men are in the group, some male perspectives, changing the colour scheme might be helpful, because for me, it's feminine to a core (…) some guys might be turned off by that.” (FG1) It was further noted that, “[I]f [RIRO] doesn't emphasise separations, deployments… it will just be seen as another [civilian] course that is trying to make its way into a military context.” (FG5).
Some participants cautioned against too much militarization during contextualisation as, “People are people. When you grieve because your dad died, it doesn't matter that I wear a green uniform (…) I grieve the same way whether I wear a green uniform or I don't, but ‘we have to put it in the context because we’re separate across the country' but a lot of people are separate across the country.” (FG2) Additionally, “Some spouses want nothing to do with the military, so if you give them too many military examples they won't get it. So it's making sure there's enough of both.” (FG2)
Participants noted a need for reduced time commitment, “We have to summarise it to make it in a military context. It might be hard to get the people 1 week off from what they do.” (FG5) Participants recommended providing condensed or intensive versions of RIRO and BBT. “My concern is the longevity. Ten weeks is a long time. I kind of wish it were 6 or 8.” (FG1) Despite the length, participants indicated, “From an educator perspective, the lesson plans are very clear, could be delivered in a simplistic manner. (…) [Y]ou could open up the book and know what you needed to teach.” (FG3)
Participants suggested several potential collaboration options: “Some units have a family cell so finding out who the member is that runs that cell within a unit is a good connexion.” (FG4) “Sentinels (peer supports embedded) in the various units. RIRO offers useful tools to help them help others,” (FG5) and, “We do have a school liaison coordinator who (…) may be a good person to get that out to the school newsletters.” (FG4) The RIRO and BBT programs could be expanded to other SPs throughout the CAF and MFRCs.
The development of resilient SMs/CMFs is essential to fulfiling the vision and priorities of CAF and VAC. Offering resilience training to SPs and SMs/CMFs within the CAF community and through MFRCs can foster resilient behaviours, attitudes, and mindsets, enhance individual, family and community resilience and have intergenerational impacts. Currently, evidence-informed resilience-building programs that foster resilience within the CAF, VAC, and MFRC communities are lacking.
Trainees related that the RIRO and BBT resilience training programs, with their holistic, integrated, experiential learning and community approach, were likely to facilitate resilience-building in military and CMF communities. Skills and tools crossed resilience domains (i.e., physical, mental, ethical/spiritual, social/cultural, familial) and the psychosocial work environment. The programs also addressed many core elements of community resilience (i.e., local knowledge, community networks and relationships, communication, preparedness, and mental outlook). Participants perceived program content to be relevant, effective, useful, and accessible. Alignment and fit with CAF and VAC initiatives was also noted, although contextualisation and inclusion of military-specific scenarios would greatly enhance usability and reflect the lived experiences of SMs/CMFs. Trainees indicated that the programs would address a service gap and be complementary to current CAF and MFRC programs.
Intentional-capacity building across SPs, SMs/CMFs, MFRCs, and the CAF, together with clear and supported implementation efforts, would be required to integrate resilience-building programs such as RIRO and BBT in military, Veteran and CMF populations. Selection and contextualisation of a particular program(s), facilitator training, and embedding of training into existing program offerings and routine training cycles would also be needed. Master trainers, authorized to train others in the delivery of RIRO and BBT, would need to be credentialed to support widespread program implementation. It would also be of benefit for sufficient numbers of SPs and SMs/CMFs (25%) to receive RIRO and BBT resilience training so as to enhance the likelihood of effecting culture change at the individual, family and organisational levels (26). Making the program available in differing formats (in-person, online), length, and language specific to target audiences would also enhance uptake. This would be especially helpful for reaching SMs and CMFs who reside off base [currently 85% of CMFs (27)], or are geographically dispersed, living abroad, or separated due to duty-related activities. Online delivery would make it possible for simultaneous program participation by co-parents. Virtual RIRO/BBT peer support groups would also have the benefit of facilitating community connexion and resilience. Overarching resilience networks and hubs could create a greater sense of community and increase capacity and support, allowing SMs, Veterans, CMFs and communities to flourish during and following life in military service.
This study lays a foundation for future research regarding resilience-training programs and capacity-building within a Canadian military context. It also contributes to the much-needed evidence-base regarding culturally-specific and sensitive resilience-building programs. Further research is yet needed to assess the impact of RIRO and BBT training on SPs, SMs and Veterans, CMFs, and the CAF at large, and the effectiveness of RIRO and BBT. Consideration of programs for CMFs with older children and family members is also needed. Additionally, the implementation, spread and sustainability of RIRO and BBT programs in the CAF and VAC communities, and establishment of community resilience networks and hubs, has not been explored. Various training and program delivery formats (online and in-person formats in various languages) is also warranted.
This study had several strengths and limitations. Participation of multidisciplinary SPs and leaders who support SMs/CMFs and are familiar with the military culture, as well as SMs themselves, was a strength, as was capturing trainee perspectives immediately upon completion of RIRO/BBT trainer training. Limitations include the small sample size and lack of VAC representation, although SPs working specifically with Veterans were included. Findings were also based on discussions with the trainees prior to them delivering RIRO and BBT programs, with the exception of FG6 participants who delivered BBT training to a sample of CMFs. Additionally, not all participants who attended the RIRO and BBT training were able to join the FGs, and instead sent email responses to the questions; these responses may have been less detailed and rich. Further, due to the unforeseen circumstances of a global pandemic (COVID-19), exploration of opportunities and plans for RIRO/BBT trainees to offer either RIRO or BBT programs was not possible.
The resilience and operational readiness of SMs/CMFs is essential to CAF's ability to fulfil its missions. Resilience-training can enhance the resilience of SPs and SMs/CMFs and military communities. Preparing SPs to model resilience and deliver evidenced-based resilience-training programs such as RIRO and BBT has the potential to build capacity at the individual, family, community, SP and organisational levels, and support a resilient and ready defense team. Widespread use of standardised resilience programs could enable use of a common language and skill set in the military community and growth of a culture of resilience. This study contributes to research regarding evidence-based culturally-specific and -sensitive resilience-training programs and capacity-building within the Canadian military context.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by University of Alberta Research Ethics Board. The patients/participants provided their written informed consent to participate in this study.
SB-P, AP, AH, JO, PS, and CM conceived, designed, and conducted the study. All authors drafted, revised, and approved the final manuscript submitted for publication.
This pilot study was funded by a Glenrose Rehabilitation Hospital Clinical Research Grant and Kule Institute for Advanced Study (KIAS) Dialogue Grant. In-kind support was provided by the local MFRC, RCChS, CAF, and the academic institution with which the research team members are affiliated.
CM was employed by the MFRC.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The research team would like to thank study participants for sharing their time and experiences, the funders for enabling the study, and the MFRC, RCChS, and CAF leadership and staff for their continued support.
1. Government of Canada and Department of National Defence. Strong Secure Engaged: Canada's Defence Policy. Ottawa, ON: National Defence (2017).
2. Pfefferbaum B, Pfefferbaum RL, Van Horn RL. Community resilience interventions: Participatory, assessment-based, action-oriented processes. Am Behav Sci. (2015) 59:238–53. doi: 10.1177/0002764214550298
3. Doherty G, Knight EC, Dobreva-Martinova T. Defence team total health and wellness strategic framework. In: Paper Submitted to the 43rd HFM Panel Business Meeting. (2019). p. 8–11. Available online at: https://scholar.googleusercontent.com/scholar?q=cache:R4ZFl9Vdz4sJ:scholar.google.com/+Defence+Team+Total+Health+and+Wellness+Strategic+Frameworkandhl=enandas_sdt=0,5
4. Wang Z, Aitken N. Impacts of Military Lifestyle on Military Families: Results From the Quality of Life Survey of Canadian Armed Forces Spouses. DRDC-RDDC-2016-R012. Ottawa, ON: Defence Research and Development Canada (2016).
5. Manser L. State of Military Families in Canada: Issues Facing Regular Force Members and Their Families. Ottawa, ON: Canadian Forces Morale and Welfare Services (2018).
6. Manser L. The state of military families in Canada: a scoping review. J Mil Vet Fam Health. (2020) 6:120–8. doi: 10.3138/jmvfh-2019-0001
7. Walsh F. Family resilience: a developmental systems framework. Euro J Dev Psych. (2016) 13:313–24. doi: 10.1080/17405629.2016.1154035
8. DeVoe ER, Paris R, Acker M. Prevention and treatment for parents of young children in military families. In: Gewirtz AH, Youssef AM, editors. Parenting and Children's Resilience in Military Families. Cham: Springer (2016). p. 213–27.
9. Bradley RH, Corwyn RF. Infant temperament, parenting, and externalizing behavior in first grade: a test of the differential susceptibility hypothesis. J Child Psychol Psychiatry. (2008) 49:124–31. doi: 10.1111/j/1469-7610.2007.01829.x
10. Ungar M. Resilience, trauma, context, and culture. Trau Viol Abus. (2013) 14:255–66. doi: 10.1177/1524838013487805
11. Fisher DM, Ragsdale JM, Fisher ECS. The importance of definitional and temporal issues in the study of resilience. Appl Psych Inter Rev. (2019) 68:583–620. doi: 10.1111/apps.12162
12. Patel SS, Rogers MB, Amlôt R, Rubin GJ. What do we mean by 'community resilience'? A systematic literature review of how it is defined in the literature. PLoS Curr. (2017) 9. doi: 10.1371/currents.dis.db775aff25efc5ac4f0660ad9c9f7db2
13. Government of Canada and Department of National Defence. Surgeon General's Integrated Health Strategy - 2017 - Integration for Better Health. Ottawa, ON, CA: National Defence (2017).
14. Government of Canada and Department of National Defence. Strengthening the Forces Health Promotion Program. (2019). Available online at: https://www.canada.ca/en/department-national-defence/programs/strengthening-forces.html
15. Chartier A. The Mapping and Gaps Analysis of Services for Military Families Report. Comprehensive Military Family Plan. Canadian Forces Morale and Welfare Services, Ottawa, ON (2019).
16. Government of Canada. Road to Mental Readiness (R2MR). (2017). Available online at: https://www.canada.ca/en/department-national-defence/services/guide/dcsm/r2mr.html
17. Kordich Hall D, Pearson J. Introducing Thinking Skills to Promote Resilience in Young Children. Reaching In…Reaching Out Project (RIRO), Child and Family Partnership, Toronto, ON (2004). Available online at: https://www.reachinginreachingout.com/documents/RIRO-Thinking_skills_and_resilience.pdf
18. Pearson J, Kordich Hall D. Reaching In … Reaching Out Resiliency Guidebook “Bounce Back” Skills for Adults and Young Children. Toronto, ON (2017). Available online at: http://www.reachinginreachingout.com/resources-guidebook.htm
19. Seligman MEP, Reivich K, Jaycox L, Gillham J. The Optimistic Child. New York, NY: Harper Perennial (1995).
22. Then KL, Rankin JA, Ali E. Focus group research: what is it and how can it be used?. Can J Cardiovasc Nurs. (2014) 24:16–22.
23. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. (2006) 3:77–101. doi: 10.1191/1478088706qp063oa
25. Koch T. Establishing rigor in qualitative research: the decision trail. J Adv Nurs. (2006) 53:91–100. doi: 10.1111/j.1365-2648.2006.03681.x
26. Centola D, Becker J, Brackbill D, Baronchelli A. Experimental evidence for tipping points in social convention. Science. (2018) 360:6393. doi: 10.1126/science.aas8827
Keywords: military, families, resilience, well-being, program evaluation (MeSH), community, mental health—related quality of life
Citation: Mikolas C, Winfield H, Smith-MacDonald L, Pike A, Jones C, Lee M, Griffiths J, Perry R, Olson DM, Heber A, Olson J, Sevigny PR and Brémault-Phillips S (2021) Enhancing Resilience in Canadian Military Families and Communities: A Qualitative Analysis of the Reaching In… Reaching Out and Bounce Back and Thrive! Resiliency Skills Training Programs. Front. Public Health 9:662313. doi: 10.3389/fpubh.2021.662313
Received: 15 February 2021; Accepted: 07 April 2021;
Published: 20 May 2021.
Edited by:
Sunjoo Kang, Yonsei University, South KoreaReviewed by:
SeunYoung Joe, Korea Armed Forces Nursing Academy, South KoreaCopyright © 2021 Mikolas, Winfield, Smith-MacDonald, Pike, Jones, Lee, Griffiths, Perry, Olson, Heber, Olson, Sevigny and Brémault-Phillips. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Suzette Brémault-Phillips, c3V6ZXR0ZS5icmVtYXVsdC1waGlsbGlwc0B1YWxiZXJ0YS5jYQ==
†These authors have contributed equally to this work and share first authorship
‡These authors have contributed equally to this work and share last authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.