 Xia Wang
Xia Wang Yan Wang1†
Yan Wang1†- 1Hospital of Chengdu University of Traditional Chinese Medicine, Chengdu, China
- 2Department of Clinical Medicine, Chengdu University of Traditional Chinese Medicine, Chengdu, China
Background: Currently, more and more subfertility couples are opting for combined acupuncture to improve the success rate of in vitro fertilization and embryo transfer (IVF-ET). However, the efficacy and safety of acupuncture in IVF-ET is still highly controversial.
Objectives: The purpose of this overview is to summarize evidence of essential outcomes of systematic reviews (SRs) of acupuncture in IVF-ET and evaluate their methodological quality.
Methods: We conducted a comprehensive literature search for relevant SRs in eight databases from inception to July 31, 2020, without language restriction. We evaluated the methodological quality of the included SRs by using A Measurement Tool to Assess Systematic Reviews 2 (AMSTAR-2), which was the latest available assessment tool. The Risk of Bias in Systematic Review (ROBIS) tool was used to assess the risk of bias in SRs. We assessed the Grades of Recommendation, Assessment, Development, and Evaluation (GRADE) score to determine the strength of evidence. We excluded the overlapping randomized controlled trials (RCTs) and performed a re-meta-analysis of the primary RCTs.
Results: This review included 312 original RCT studies and 65,388 participants. By using AMSTAR-2, we found that the methodological quality of 16 SRs was critically low, because they had more than one critical weakness. Our reviews showed that although the GRADE for quality of evidence profile was suboptimal, acupuncture seemed to be beneficial in increasing the pregnancy rate. Our re-meta-analysis suggested that acupuncture was superior to sham acupuncture in improving the clinical pregnancy rate (CPR) of IVF-ET with substantial heterogeneity (RR = 1.31, 95% CI: 1.13–1.52, p = 0.0004, I2 = 66%). No statistical difference was observed regarding the outcomes of live birth rate (LBR), ongoing pregnancy rate (OPR), biochemical pregnancy rate (BPR), and miscarriage rate (MR) between two groups. When compared with no adjunctive treatment groups, acupuncture improved CPR (RR = 1. 25, 95% CI: 1.11–1.42, p = 0.0003) and OPR (RR = 1. 38, 95% CI: 1.04–1.83, p = 0.03). Acupuncture was more superior than no adjunctive treatment in reducing MR (OR = 1.42, 95% CI: 1.03–1.95, p = 0.03) and BPR (RR = 1.19, 95% CI: 1.02–1.37, p = 0.02).
Conclusions: Although the evidence of acupuncture in IVF-ET is insufficient, acupuncture appears to be beneficial to increase the clinical pregnancy rate in women undergoing IVF-ET. However, there are severe heterogeneity and methodological quality defects, which limit the reliability of results. Further, high-quality primary studies are still needed.
Introduction
Infertility is defined as failure to establish a clinical pregnancy after 12 months of regular, unprotected sexual intercourse (1, 2). The prevalence rate of infertility is 15% in the reproductive period (3). Among couples who are trying to conceive at reproductive age in China, 25% may encounter infertility (4). According to the report, female factors account for 40% of overall infertility (5). In vitro fertilization and embryo transfer (IVF-ET) is an effective treatment method for subfertility couples (6, 7). Worldwide, 7,079,145 cycles were carried out between 2004 and 2013, and successfully resulted in the birth of approximately 1.45 million children (8). Currently, the average success rates per IVF cycle remain low, although live birth rate gradually improved in most regions, some demonstrated declines. Fresh cycle live birth rate was highest in the USA (29%) and lowest in Japan (5%) between 2012 and 2013 (8). For many women, cycles need to be repeated to succeed. The IVF-ET cycle is time-consuming and costly. The direct and indirect costs of one cycle of IVF-ET are equivalent to $10,000 to 25,000 (9, 10), so it is essential to enhance the success rate of IVF-ET. Therefore, many patients try to seek alternative therapies to improve IVF-ET outcomes, including acupuncture. Acupuncture involves the insertion of metallic needles into the body. The application of acupuncture through stimulating certain acupoints on the human body is to activate the meridians and to regulate the function of qi and blood so as to prevent and treat disease. In the USA, 47% of infertile women engaged in acupuncture during IVF-ET treatment (11). The mechanisms of acupuncture in IVF-ET have been reported to enhance hormonal balance (12), inhibit uterine motility (13), increase blood flow to uterine and ovarian areas (14), and downregulate various stress responses (15–17).
Nowadays, some systematic reviews (SRs) of acupuncture in IVF-ET have been published to evaluate its effectiveness and safety. However, no consensus has been reached. Some reviews indicated that acupuncture might provide benefits in improving reproductive outcomes (18–29). Others found no statistically significant difference in clinical pregnancy or live birth when compared with a control (30–33). The quality of evidence is unclear. Therefore, our study aims to assess the methodological and reporting quality of SRs concerning the effectiveness of acupuncture for infertile women undergoing IVF-ET, and to provide beneficial recommendations for the implementation of SRs.
Method
Protocol and Registration
The protocol of this study was registered in PROSPERO with the registration number CRD42020201238 (https://www.crd.york.ac.uk/PROSPERO/).
Search Strategy for Identification of Studies
Electronic literature was searched in the following databases from inception to July 31, 2020, without language restrictions: including four international electronic databases (Pubmed, EMBASE, Cochrane Library, and Web of Science) and four Chinese electronic databases (CNKI, Sino, Wan Fang, and VIP database). Unpublished conference proceedings relevant to infertile women undergoing IVF-ET were reviewed, if available. MeSH items or free words included: (In vitro fertilization OR Intracytoplasmic sperm injection OR Embryo transfer OR Assisted reproductive techniques) AND (systematic review OR Meta-analysis) AND (Acupuncture OR Acupuncture therapy OR Acupuncture points OR Electroacupuncture OR Acupuncture Analgesia). The search strategy of EMBASE is shown in Appendix and modified to suit other databases.
Inclusion and Exclusion Criteria
Study Participants
Female patients diagnosed with infertility and undergoing IVF-ET would be included. There were no restrictions in diagnosis criteria or participant age. IVF-ET with intracytoplasmic sperm injection (ICSI) was allowed.
Study Intervention
Treatment with acupuncture must be used as the primary intervention measure. All types of acupuncture (i.e., traditional acupuncture, electro-acupuncture, auricular acupuncture, laser acupuncture) were included. It could be treated with acupuncture alone, or combined with medicine, or with other treatments, regardless of the frequency or duration of the treatment.
Study Comparison
The control interventions included placebo (sham) acupuncture or no adjunctive treatment, or western medicine treatment, or rehabilitation exercise, or Chinese herb medicine, or Tui-na massage, or other convenient controls. Systematic reviews comparing different types of needle were excluded.
Study Outcome Measures
The primary outcomes were clinical pregnancy rate (CPR), live birth rate (LBR), biochemical pregnancy rate (BPR), ongoing pregnancy rate (OPR), and miscarriage rate (MR). The secondary outcomes were adverse events.
Study Design
Systematic reviews containing more than one randomized controlled trial (RCT) were included. Non-RCT SRs, review comments, overviews of SRs, editorials, and guidelines were excluded.
Selection of Studies and Data Extraction
According to the intended inclusion and exclusion criteria, the articles were screened independently by two reviewers (XW and YW). Another reviewer (SBW) was involved and made a decision when two authors showed a difference of opinion. One reviewer (XW) used a standardized form to extract the following information from the included articles; another author (YW) reviewed the extracted document. Data extraction included researcher, publication time, number of RCTs enrolled, data synthesis methods, quality assessment tool for RCTs, adverse effects, characteristics of interventions and control groups, primary and secondary outcomes, evaluation criteria of methodology, main results, and conclusions.
Assessment of Systematic Reviews
Two independent reviewers (XW and YW) evaluated the quality of the included SRs. Before the evaluation, each topic of the assessment tools was intensively discussed to reach a consensus.
Assessment of Methodological Quality
The methodological quality of the included reviews was assessed by using A Measurement Tool to Assess Systematic Reviews 2 (AMSTAR-2), which was the latest available assessment tool. The AMSTAR-2 contains 16 domains, of which domains 2, 4, 7, 9, 11, 13, and 15 were the critical items, and the items should not be used to derive an overall score (34). We adopted the rating process based on the identification of critical domains. AMSTAR-2 domains are shown in Supplementary Figure 2.
Assessment of Bias
Risk of Bias in Systematic Review (ROBIS) is a new tool for assessing the risk of bias in systematic reviews (35). The four critical elements were “study eligibility criteria,” “identification and selection of studies,” “data collection and study appraisal” and “synthesis and findings.” Each domain was evaluated as “high risk,” “low risk,” or “unclear risk.”
The Quality of Evidence
For each significant result, we gave a score of 4 because these were based on randomized trials and assessed limitations that might have reduced the evidence's quality (36). We deducted points if there were: study limitations; sparse data on an outcome of interest, inconsistent results, indirectness of evidence, or imprecision. According to the Grades of Recommendation, Assessment, Development, and Evaluation (GRADE) score, the quality of evidence was classified into high, moderate, low, and very low (36, 37).
Strategy for Data Synthesis
To assess the combined effects of the included reviews, we performed a re-meta-analysis of the main outcomes. The effects of acupuncture on CPR, LBR, BPR, OPR, and MR were observed in women undergoing IVF-ET. Considering the overlap of some primary RCTs, the two reviewers listed the trials for each SR and then excluded the overlapping trials. All data were dichotomous. When no significant heterogeneity could be observed (I2 < 50%), a fixed-effects model was applied and results were pooled. If there was significant heterogeneity (I2 ≥ 50%), the random-effects model was applied correctly, and expressed as relative risk (RR). The Forest plots were performed with RevMan5.3 software.
We also performed a subgroup analysis of several factors that might influence the CPR of acupuncture. This included: (1) age (≥35 or <35 years); (2) duration of infertility (≥4 or <4 years); (3) number of embryos transferred (≥2 or <2); (4) type of sham (invasive vs. non-invasive); and (5) sham points (yes or no). The information of the variables for subgroup analysis are shown in Supplementary Table 1. Sensitivity analysis was performed to explore whether the overall conclusions were affected.
Results
Results on Literature Search and Selection
A total of 265 records were collected from electronic databases. In total, 120 duplicates were excluded by filtration; 114 of the remaining citations were excluded by title and abstract screening, and 31 studies were assessed through the full texts. After being reviewed by two reviewers independently, 16 SRs about acupuncture for infertile women undergoing IVF-ET were included (Figure 1). The reasons for exclusion are shown in Supplementary Figure 2.
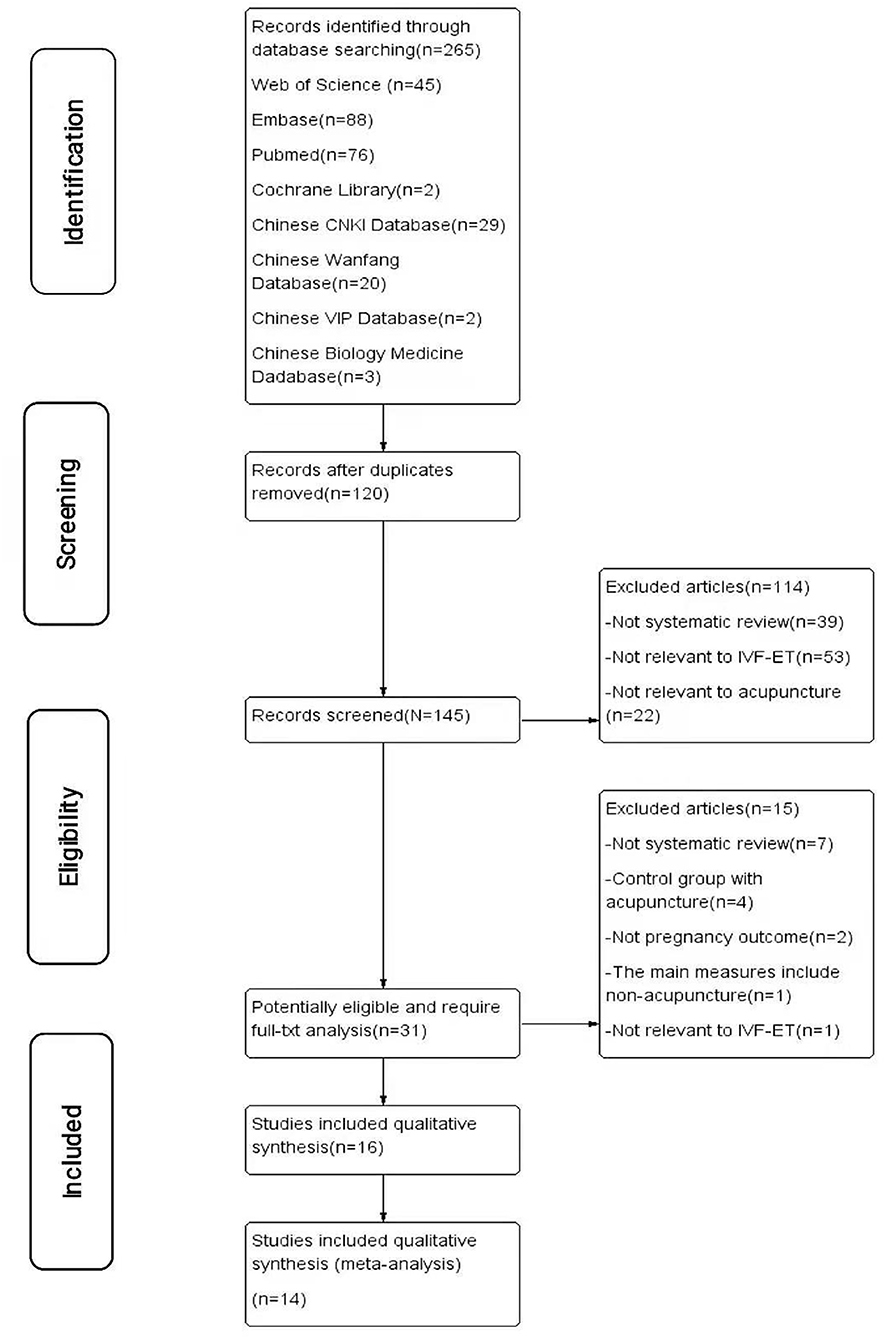
Figure 1. The PRISMA flow diagram of study selection.
Characteristics of Included Reviews
The sixteen included reviews (18–33) were published between 2008 and 2020. Fourteen reviews were published in English, two in Chinese. This overview included 312 original RCTs and 65,388 participants. The number of RCTs of included SRs ranged from 3 to 32 studies. As for intervention, all reviews compared acupuncture with no adjunctive treatment or sham (placebo) acupuncture. Eight reviews (20, 22, 25, 28–32) included traditional acupuncture as the main intervention. Twelve reviews (18–28, 32, 33) used electroacupuncture as an intervention measure. Eight SRs (18, 19, 21, 23, 24, 26, 27, 33) used manual acupuncture as a therapeutic intervention. Five SRs (20, 22, 26, 27, 32) included auricular acupuncture as an intervention measure. Five reviews (20–22, 25, 32) used transcutaneous electrical acupoint stimulation or laser acupuncture as the intervention. One review (30) used sham acupuncture as the control group, while others used sham acupuncture or no adjunctive treatment. Only one review (28) applied the Jadad scale for methodological quality assessment of original RCTs, and thirteen SRs (18–25, 29–33) used the Cochrane Handbook, but two reviews (26, 27) did not report the methodological tool. Table 1 shows the basic characteristics of the included SRs.
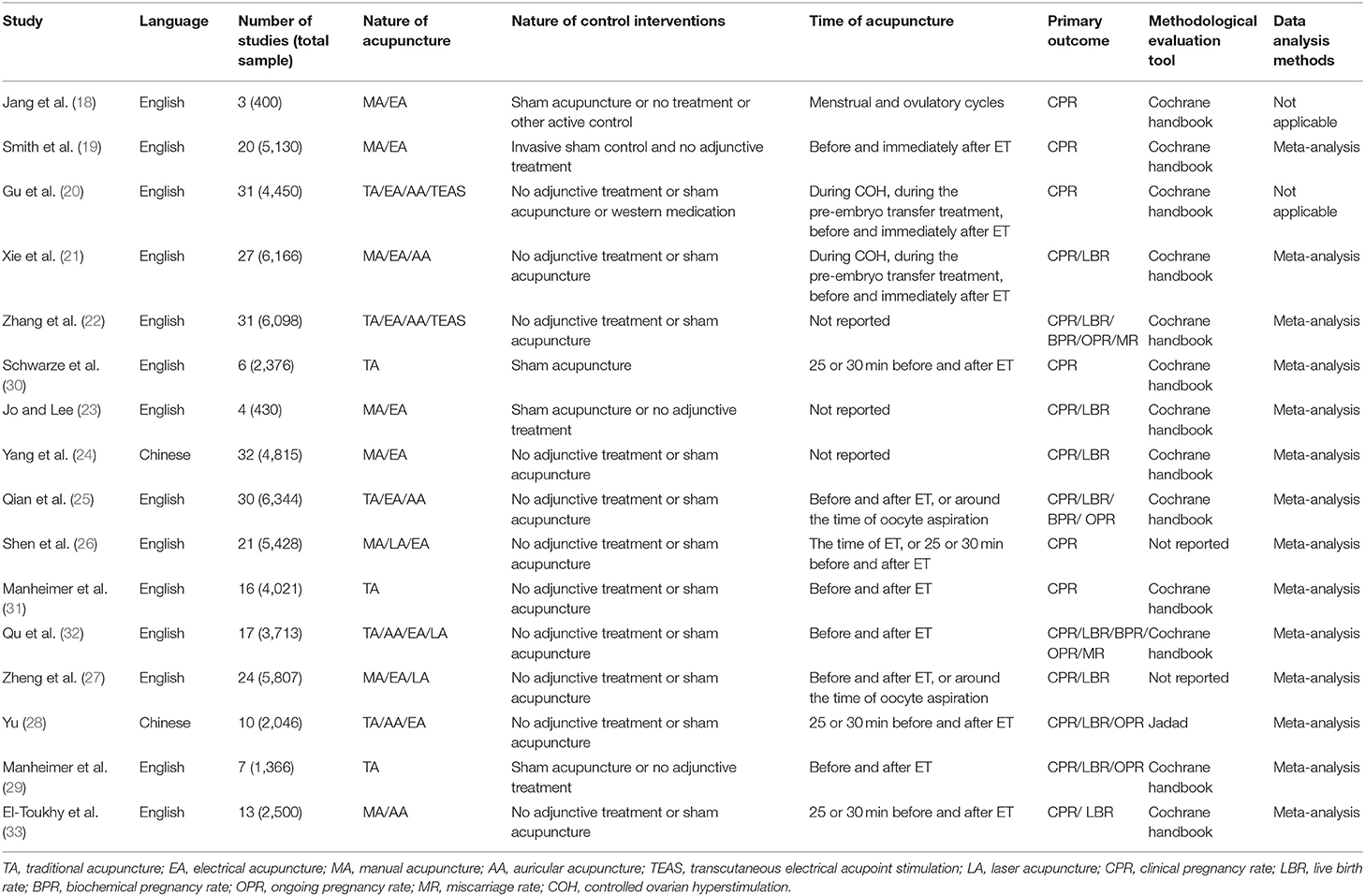
Table 1. Basic characteristics of the included SRs.
Methodological Appraisal
AMSTAR-2 was used to assess the methodological quality of studies. The qualities of sixteen reviews were considered critically low, because they had more than one critical flaw (items 2, 4, 7, 9, 11, 13, and 15) with multiple non-critical weaknesses. Fourteen SRs (19–30, 32, 33) were not registered in advance, and we could not judge whether the review methods were established in advance. Only one author (19) explained their selection of the study designs for inclusion in the review. Eleven reviews (19, 22–25, 27–29, 31–33) described a comprehensive literature search strategy. Only one review (21) provided a list of excluded studies. None of the SRs described the funding sources of included RCTs. Fourteen reviews (19, 21–33) applied meta-analytical methods, and all of them explained reasons for heterogeneity reasonably. Nine studies did not declare the conflicts of interest or provide a source of funding. The details of the assessment of the quality of the included SRs are shown in Table 2.
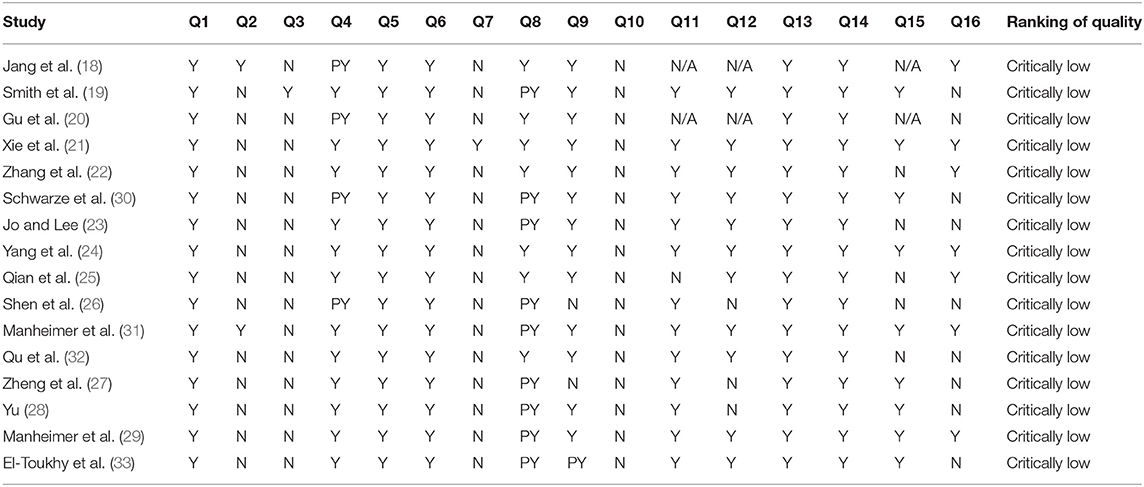
Table 2. AMSTAR-2 for methodological quality of the included SRs.
Risk of Bias of Included Systematic Reviews
The assessment of the risk of bias of each review is shown in Table 3 and Figure 2. The final phase considered the overall risk of bias of SRs, and nine SRs (56.25%) were rated with a low-risk of bias. Seven SRs (43.75%) were rated with a high-risk of bias, and the main reason for the risk of bias in SRs was the failure to adequately explain and deal with the risk of bias in their results.
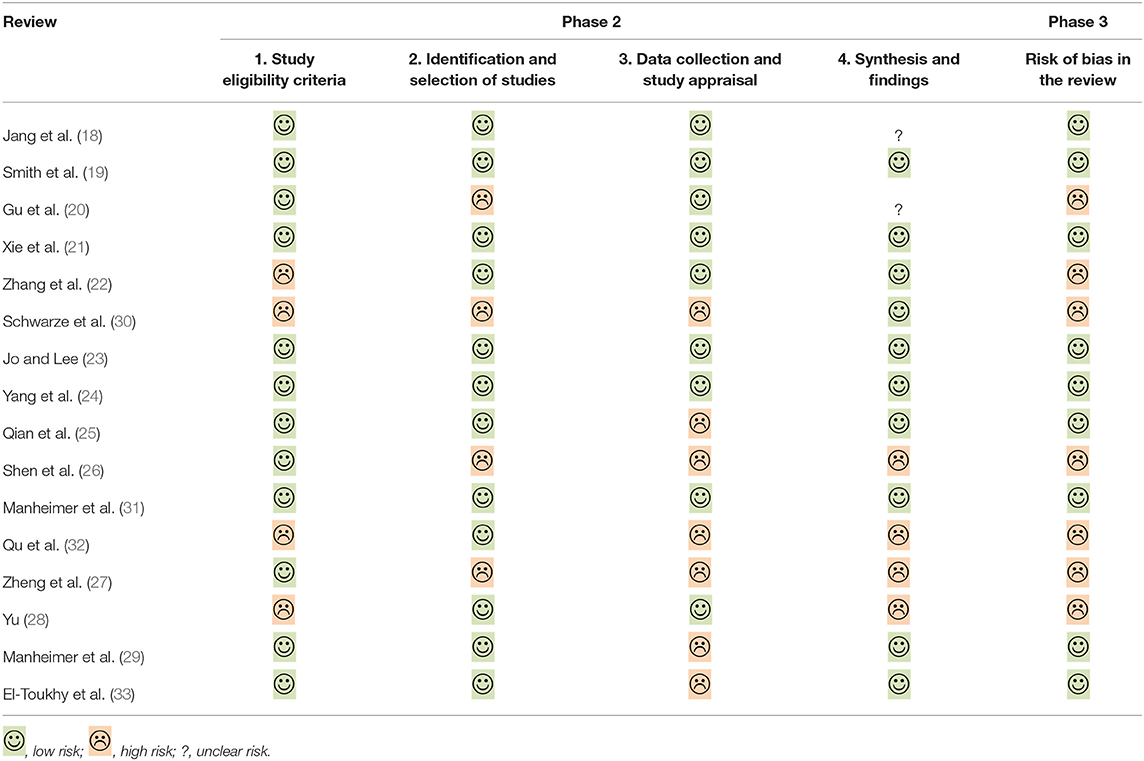
Table 3. Suggested tabular presentation for ROBIS results.
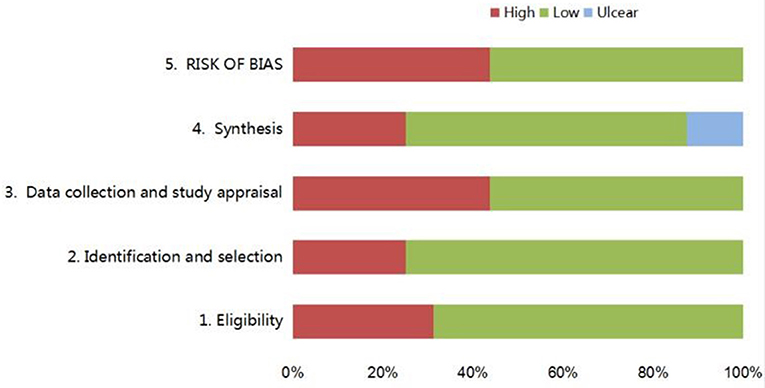
Figure 2. Graphical presentation of risk of bias of the included SRs.
GRADE for Quality of Evidence Profile
Fourteen reviews (19, 21–33) included 35 outcomes that were related to the effectiveness of acupuncture for IVF-ET. The risk of bias, imprecision, and reporting bias were the main reasons for downgrading. There was high or moderate or low or very low-grade evidence to indicate that acupuncture might improve the CPR and LBR when acupuncture was performed on the day of ET. The qualities of the evidence are shown in Table 4.
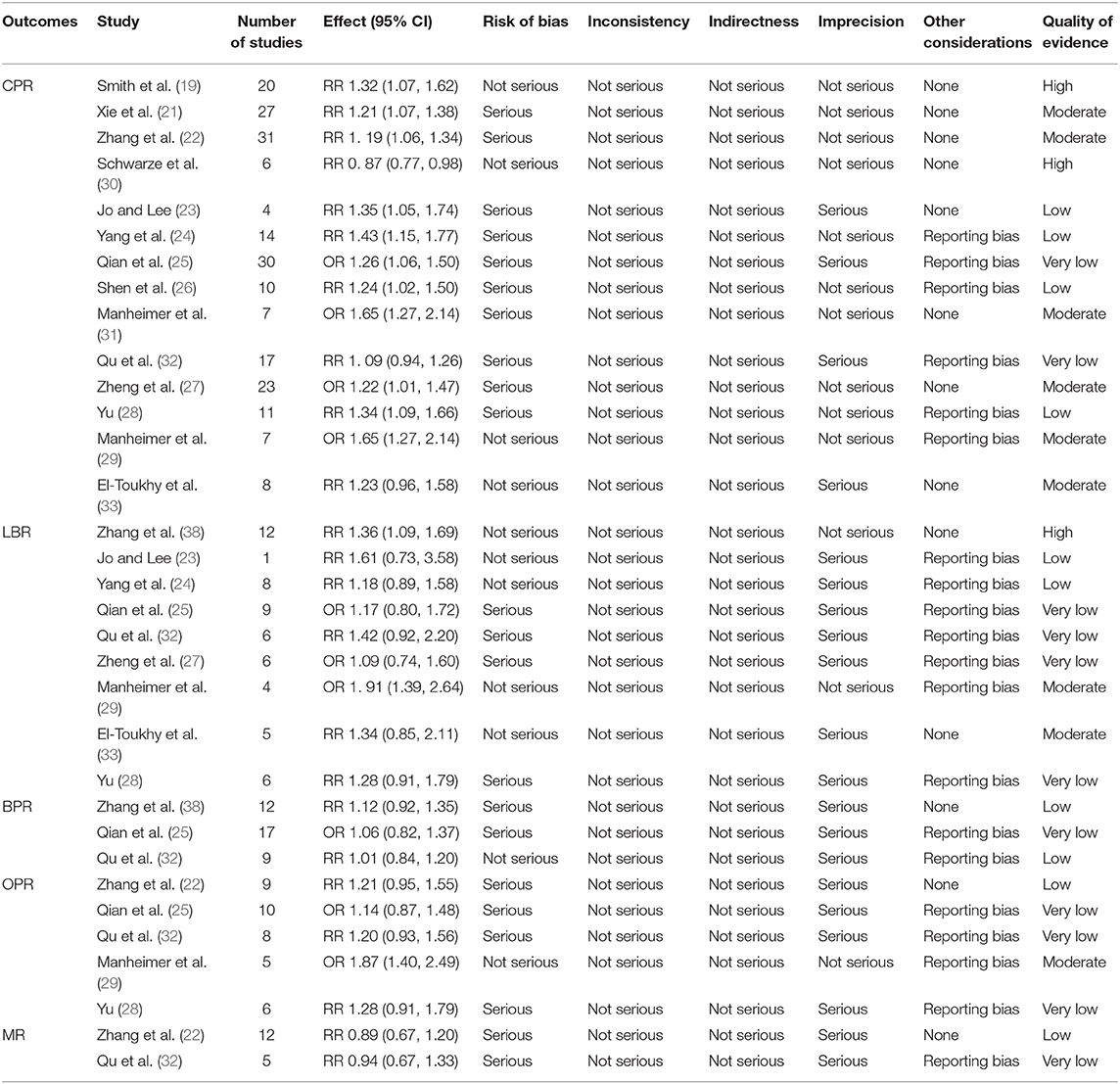
Table 4. GRADE for quality of evidence profile.
Effect of the Interventions
Acupuncture vs. Sham Acupuncture
Fourteen reviews (19, 21–33) encompassing 21 primary RCTs (4,899 participants) suggested that acupuncture was superior to sham acupuncture in increasing the CPR of IVF-ET (RR = 1.31, 95% CI: 1.13–1.52, p = 0.0004). However, there was substantial heterogeneity for the CPR (I2 = 66%) (Figure 3). There was no statistical difference between the acupuncture and sham acupuncture groups for improving LBR (RR = 0.92, 95% CI: 0.83–1.00, p = 0.06, 10 RCTs, 3,171 participants) or OPR (RR = 1.13, 95% CI: 0.90–1.41, p = 0.30, 8 RCTs, 2,793 participants) (Figures 5, 6). The benefits for reducing MR (OR = 1.20, 95% CI: 0.87–1.65, p = 0.28, 7 RCTs, 2,698 participants) or BPR (RR = 1.08, 95% CI: 0.87–1.32, p = 0.49, 8 RCTs, 2,581participants) were not significant between the acupuncture and control groups (Figures 7, 8).
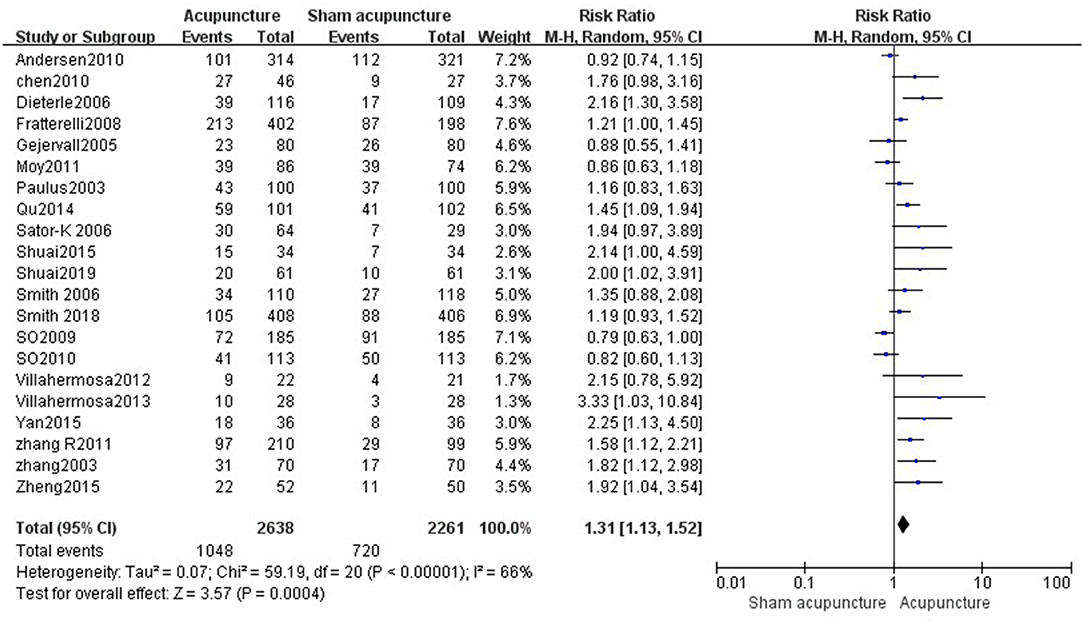
Figure 3. Acupuncture vs. sham acupuncture on the clinical pregnancy rate.
Acupuncture vs. No Adjunctive Treatment
Data were obtained from 22 RCTs (3,658 participants) out of the 14 included reviews. When using the random-effects model, the pooled results showed that acupuncture groups were significantly better than no adjunctive treatment group in improving the CPR (RR = 1.25, 95% CI: 1.11–1.42, p = 0.0003; Figure 4). The results of 11 RCTs (2,196 participants) suggested that acupuncture was not better than no adjunctive treatment in the LBR (RR = 0.89, 95% CI: 0.82–0.97, p = 0.007; Figure 5). OPR data from 7 RCTs out of the 14 included reviews were available (1,418 participants). A significant difference in the OPR was observed when the random-effects model was used (RR = 1.38, 95% CI: 1.04–1.83, p = 0.03; Figure 6). Moreover, acupuncture was more superior than no adjunctive treatment on MR reduction (OR = 1.42, 95% CI: 1.03–1.95, p = 0.03, 12 RCTs, 2,465 participants) (Figure 7). The pooled results showed a significant difference in reducing the BPR (RR = 1.19, 95% CI: 1.02–1.37, p = 0.02) between acupuncture groups and no adjunctive treatment groups (Figure 8).
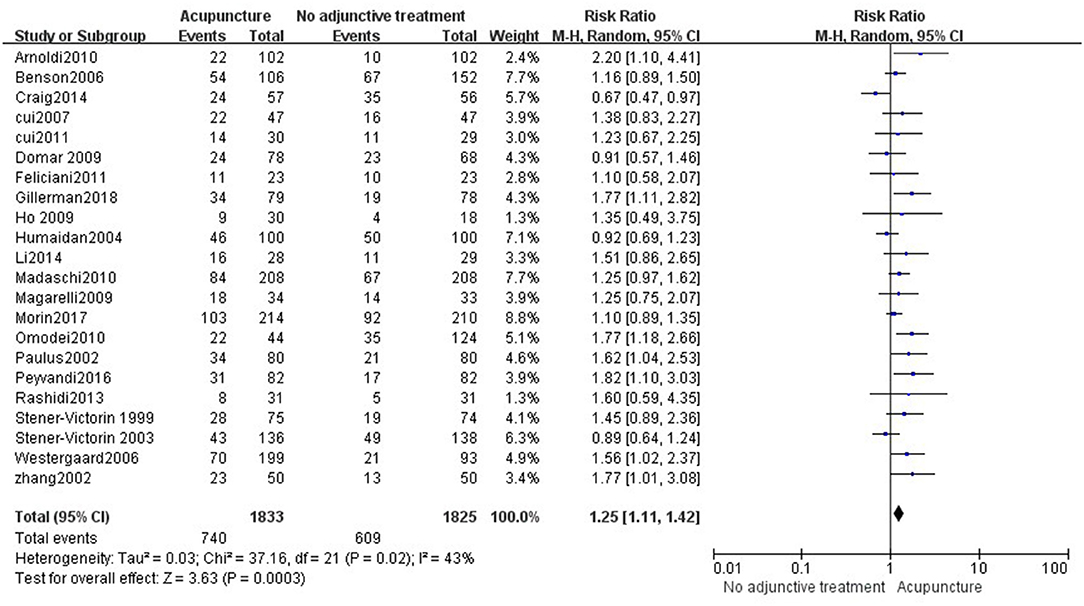
Figure 4. Acupuncture vs. no adjunctive treatment on the clinical pregnancy rate.
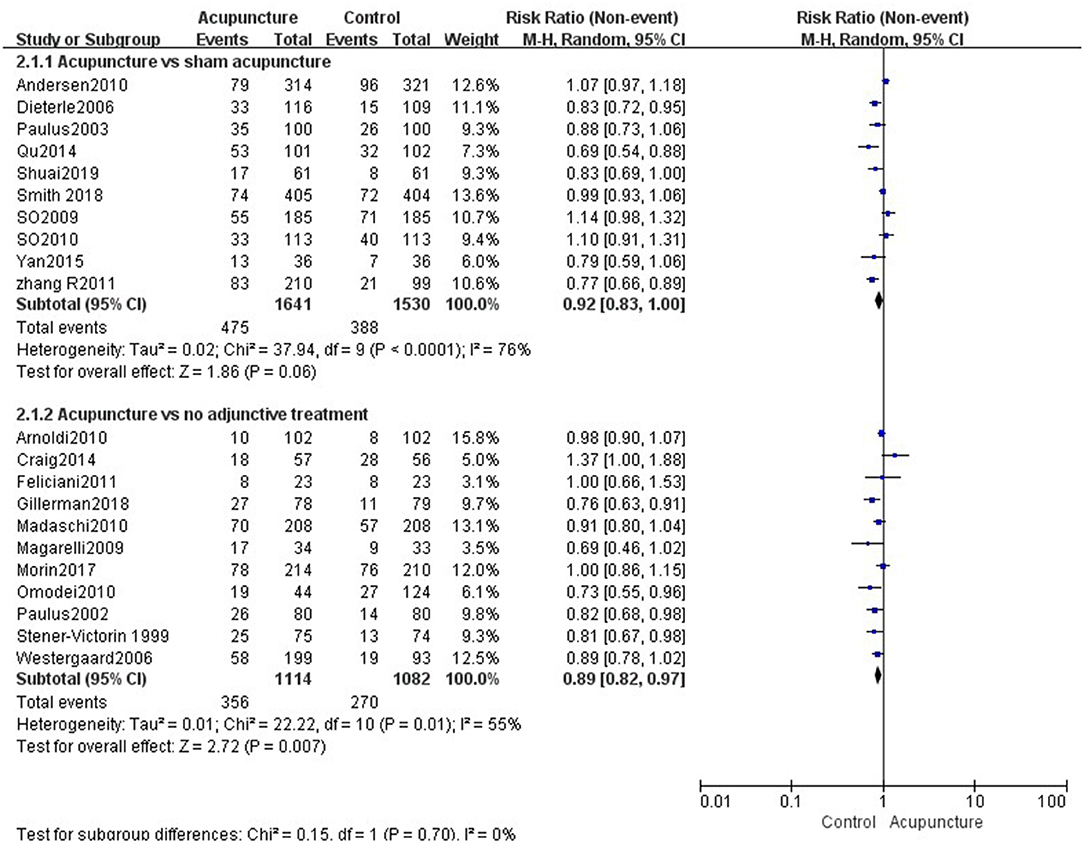
Figure 5. Effects of acupuncture on the live birth rate.
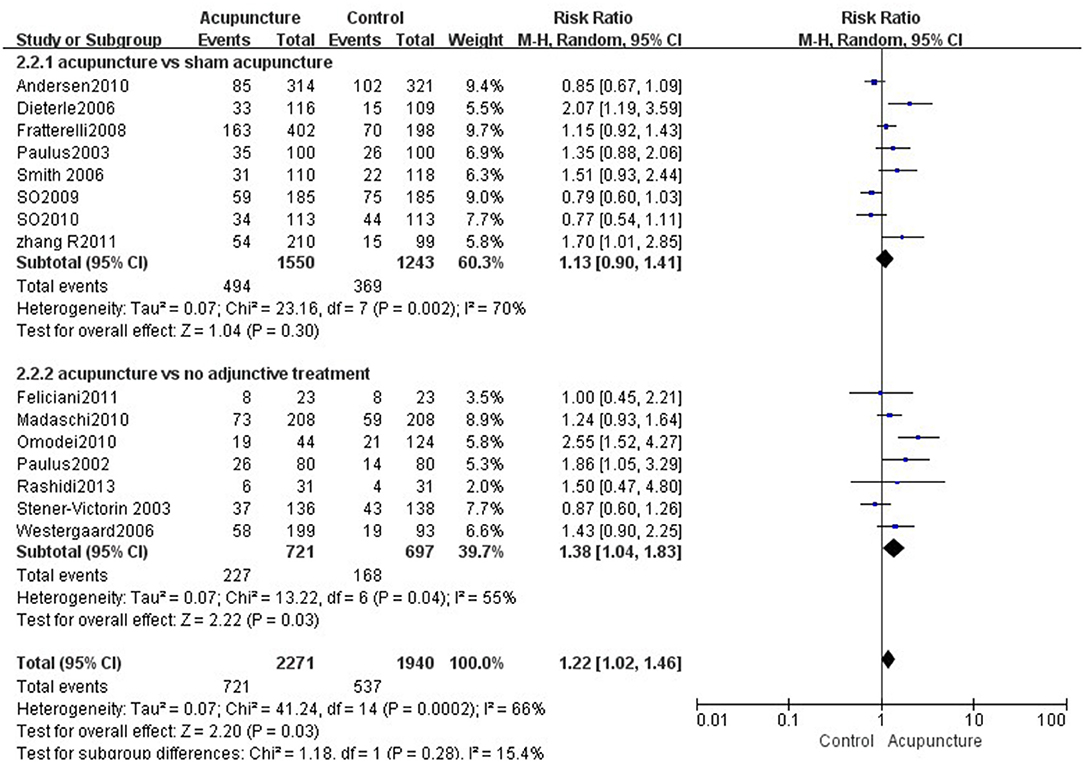
Figure 6. Effects of acupuncture on the ongoing pregnancy rate.
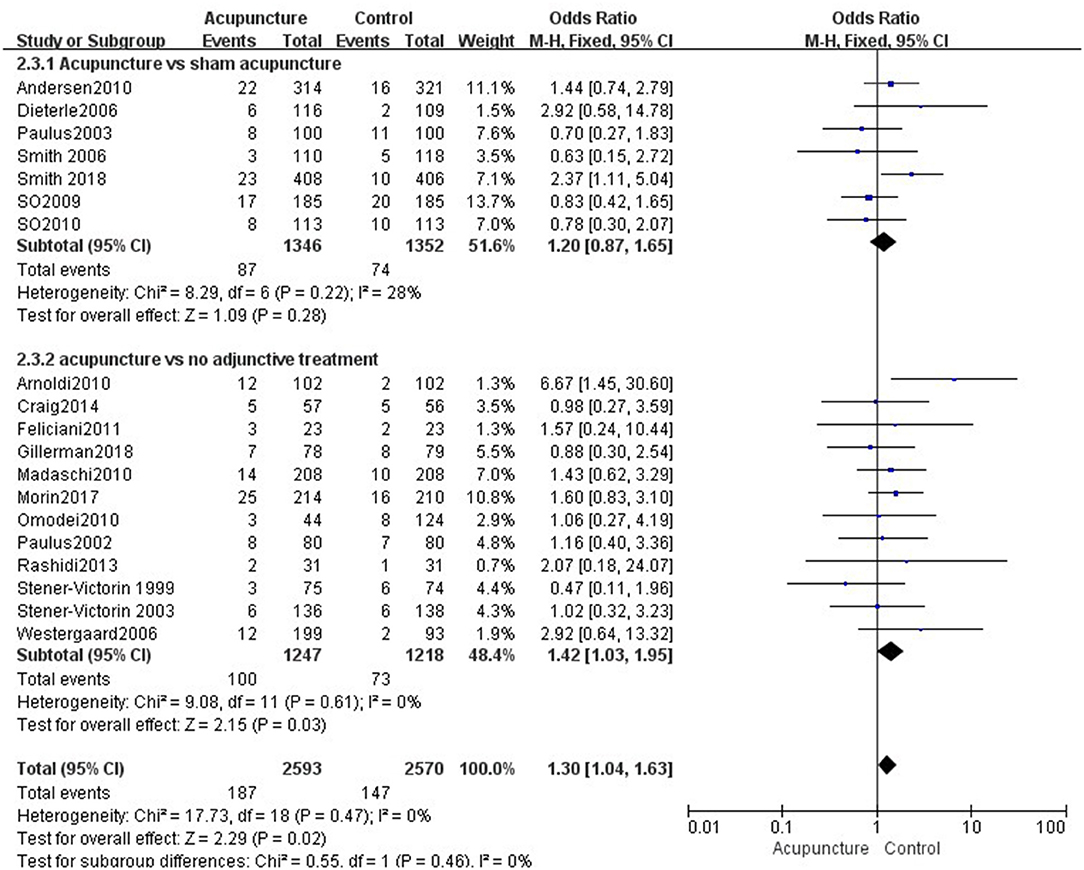
Figure 7. Effects of acupuncture on the miscarriage rate.
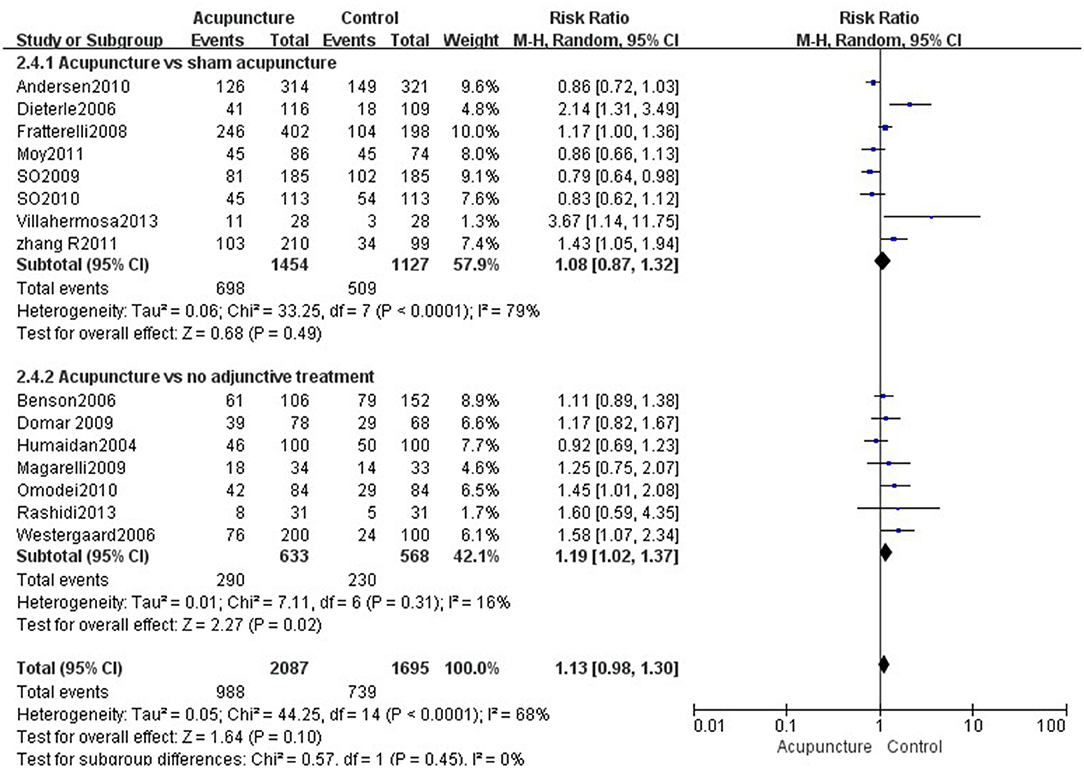
Figure 8. Effects of acupuncture on the biochemical pregnancy rate.
Subgroup Analysis on Clinical Pregnancy Rate
Sensitivity analysis was conducted by examining individual studies, the pooled results were not affected. Age below 35 years was a significant factor in the CPR (RR = 1.41, 95% CI: 1.15–1.74). Studies that used the invasive sham control showed a significant difference in the CPR (RR = 1.77, 95% CI: 1.09–2.86), and non-invasive sham control also significantly improved the CPR (RR = 1.28, 95% CI: 1.06–1.53). The duration of infertility over 4 years was not conducive to improving the CPR (RR = 0.81, 95% CI: 0.71–0.93). The number of transplanted embryos more than two (RR = 0.79, 95% CI: 0.70–0.88) and the absences of sham acupoint controls (RR = 0.82, 95% CI: 0.74–0.92) were detrimental to the CPR. Age over 35 years, duration of infertility <4 years, and sham points were not significant modifiers of the CPR. Table 5 shows the results of the subgroup analysis of outcomes regarding the CPR.
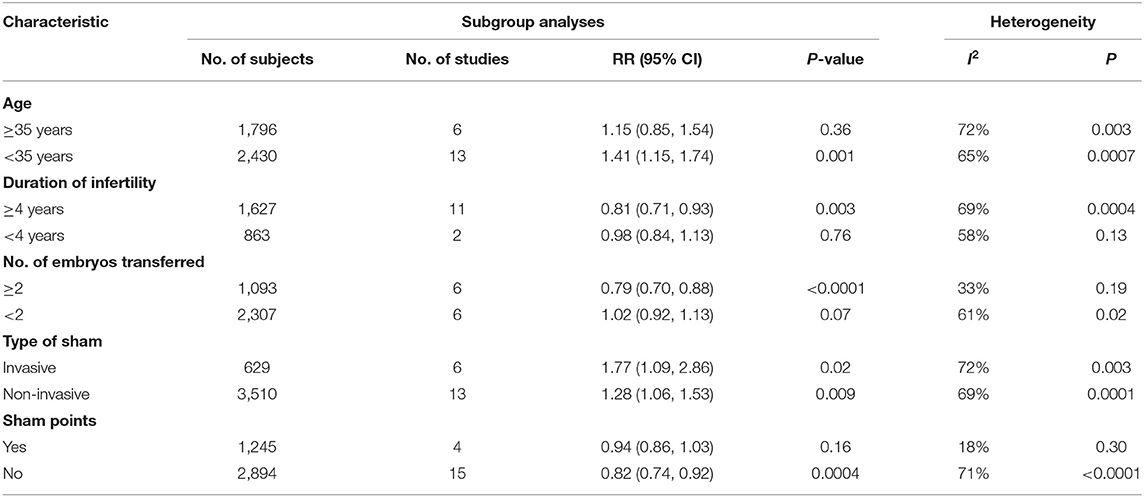
Table 5. Subgroup analysis on clinical pregnancy rate.
Adverse Effects
A total of five reviews (18, 19, 22, 29, 31) mentioned adverse events. Only three SRs (18, 19, 22) reported adverse events, including mild allergy, nausea, drowsiness, headache, chest pain, dizziness, and fatigue, while the other two SRs (29, 31) reported no serious adverse events.
Discussion
Summary of Main Findings
This updated overview of 16 SRs summarized the clinical evidence on the effectiveness and safety of acupuncture for infertile women undergoing IVF-ET from 312 primary studies that included 65,388 participants, and evaluated the methodological quality and quality of evidence. The current evidence indicated that acupuncture appeared to be superior to the control group in improving the CPR of IVF-ET. However, the methodological qualities of SRs were critically low, and the GRADE for the quality of evidence profile was suboptimal. By using the ROBIS tool, seven SRs were rated with a high-risk bias. Some SRs showed that acupuncture might be increasing LBR and OPR, but the sample was insufficient. No significant difference was found in reducing BPR and MR between groups. High-quality RCTs with large sample sizes were necessary to demonstrate the clinical effectiveness of acupuncture for IVF-ET.
In this overview, we used AMSTAR-2 to assess the methodological quality of SRs. The confidence of the overview was critically low. In some reviews using AMSTAR-2, we also found that the overall confidence in the results was rated as critically low (38–40). AMSTAR-2 was updated in 2017, so previous SRs might not have covered some items of AMSTAR-2. It might be one reason why most of the SRs were critically low as assessed by AMSTAR-2. The methodological quality of SRs was limited by the lack of data on registration and funding, comprehensive search strategy, a list and justification of excluded articles, and explanation of the risk of bias. Future research should pay attention to the above issues. The GRADE system was used to assess the evidence quality of the included SRs. The strength of evidence was moderate or low or very low for most outcomes. Most of the outcome indicators were demoted because of the bias in random, distributive hiding, or blind studies. Due to the characteristics of acupuncture, it was difficult for patients to achieve blinding, so it was important to separate researchers.
Our re-meta-analysis finds that acupuncture in IVF-ET trials appears to increase CPR, OPR, and LBR compared with no adjunctive treatment. The differences are not significant compared with sham acupuncture in increasing OPR and LBR. Since the quality of the methodology of all the SRs included is critically low, there is a high probability that the result of the re-meta-analysis is biased. There is significant heterogeneity in these clinical studies of acupuncture. Almost every trial has a different approach design in terms of interventions, the timing of treatments, controls, and outcome measures. Subgroup analysis is used to explore the factors that may affect the CPR of acupuncture. Age below 35 years is a significant factor on reproductive outcomes. Non-invasive sham control also shows a significant difference, so it is also important to estimate the placebo effect of sham acupuncture in acupuncture IVF-ET trials. Currently, most trials adopt the protocol of Paulus (41), involving acupuncture treatments before and after ET. However, the quality of the embryo is essential, but acupuncture only before and after ET has significant limitations.
Strengths and Limitations
To reduce the risk of bias, we only included the SRs of randomized trials. We evaluated the methodological quality of the included SRs by using the AMSTAR-2 tool, which was the latest available assessment tool. We assessed the GRADE score to determine the strength of evidence. We excluded the overlapping RCTs and performed a re-meta-analysis of the primary RCTs. To minimize potential bias in the overview process, we used more than two reviewers in the literature screening, data extraction, and quality assessment.
The latest RCTs were unlikely to be included in the recently published SRs, so there was some publication bias. Almost every IVF-ET trial had a different methodological design, which tended to cause severe heterogeneity, which limited the ability to interpret aggregate estimates. We collected evidence for acupuncture in IVF-ET, but we could not separate the different types of acupuncture intervention and timing of treatments.
Opportunities for Future Research
There is some debate about the effectiveness of acupuncture to treat infertile women undergoing IVF-ET. Acupuncture appears to be superior to the control group in improving the CPR of IVF-ET, but the evidence should be treated cautiously because of the methodological flaws. Recommendations for further studies are as follows: Most RCTs are considered to have an unclear risk of bias in the domains of allocation concealment and selective outcome reporting due to poor reporting, so RCTs should comply with the relevant guidelines. In most of the included studies, acupuncture was performed within a few days or hours before and after ET. So we can perform acupuncture during COH to observe the effect of acupuncture on the number of eggs obtained and oocyte quality. The duration of acupuncture may also influence the efficacy of acupuncture. Increasing the duration of insertion may increase the cumulative effect of acupuncture. Some reviews found that women with a history of multiple IVF-ET failures would benefit more from the effect of acupuncture, so more relevant RCTs should be conducted to estimate the effectiveness of acupuncture in the future. Acupuncture and placebo acupuncture touching the skin would evoke activity in cutaneous afferent nerves and leading to the “limbic touch response,” so they were equally effective (42). Therefore, it is also necessary to estimate the clinical effects of sham acupuncture in acupuncture IVF-ET trials. The difference of non-specific effect between acupuncture and sham acupuncture can be reduced to the maximum extent through the effective blind and random method. An advance registration contributes to improving transparency and minimizes potential bias. Only two SRs reported the protocol or registration number, so advance registration should be encouraged.
Conclusion
This study reviews the SRs of acupuncture for infertile women undergoing IVF-ET. Based on the current evidence, acupuncture appears to be beneficial to increase the CPR in women undergoing IVF-ET. However, there are severe heterogeneity and methodological quality defects, which limit the reliability of results. Further, high-quality primary studies are still needed.
Data Availability Statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author/s.
Author Contributions
XW and YW participating in study design, critical dialogue, data analysis, and article writing. SW contributed to the design of this study, participated in critical dialogue, and revised the manuscript. BH, YC, and NZ contributed to the literature search and extracted data. ML proofread the manuscript. All authors contributed to the article and approved the submitted version.
Funding
This work was supported by grants from the National Administration of Traditional Chinese Medicine (201729).
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2021.651811/full#supplementary-material
References
1. Datta J, Palmer MJ, Tanton C, Gibson LJ, Jones KG, Macdowall W, et al. Prevalence of infertility and help seeking among 15 000 women and men. Hum Reprod. (2016) 31:2108–18. doi: 10.1093/humrep/dew123
2. Irvine DS. Epidemiology and aetiology of male infertility. Hum Reprod. (1998) 13 (Suppl. 1):33–44. doi: 10.1093/humrep/13.suppl_1.33
4. Zheng D, Zhou Z, Li R, Wu H, Xu S, Kang Y, et al. Consultation and treatment behaviour of infertile couples in China: a population-based study. Reprod Biomed Online. (2019) 38:917–25. doi: 10.1016/j.rbmo.2018.11.034
5. Koroma L, Stewart L. Infertility: evaluation and initial management. J Midwifery Women Health. (2012) 57:614–21. doi: 10.1111/j.1542-2011.2012.00241.x
6. Buckett W, Sierra S. The management of unexplained infertility: an evidence-based guideline from the Canadian fertility and andrology society. Reprod Biomed Online. (2019) 39:633–40. doi: 10.1016/j.rbmo.2019.05.023
7. European IVF-monitoring Consortium, European Society of Human Reproduction Embryology, Calhaz-Jorge C, De Geyter C, Kupka MS, de Mouzon J, et al. Assisted reproductive technology in Europe, 2013: results generated from European registers by ESHRE. Hum Reprod. (2017) 32:1957–73. doi: 10.1093/humrep/dex264
8. Kushnir VA, Barad DH, Albertini DF, Darmon SK, Gleicher N. Systematic review of worldwide trends in assisted reproductive technology 2004-2013. Reprod Biol Endocrinol. (2017) 15:6. doi: 10.1186/s12958-016-0225-2
9. Mandrik O, Knies S, Severens JL. Economic value of in vitro fertilization in Ukraine, Belarus, and Kazakhstan. Clinicoecon Outcomes Res. (2015) 7:347–56. doi: 10.2147/CEOR.S79513
10. Bahadur G, Homburg R, Bosmans JE, Huirne JAF, Hinstridge P, Jayaprakasan K, et al. Observational retrospective study of UK national success, risks and costs for 319,105 IVF/ICSI and 30,669 IUI treatment cycles. BMJ Open. (2020) 10:e034566. doi: 10.1136/bmjopen-2019-034566
11. Domar AD, Conboy L, Denardo-Roney J, Rooney KL. Lifestyle behaviors in women undergoing in vitro fertilization: a prospective study. Fertil Steril. (2012) 97:697–701.e1. doi: 10.1016/j.fertnstert.2011.12.012
12. Cavalla H. Acupuncture and electroauriculo-therapy treatment for infertility. Med Acu Punct. (2010) 22:49–52. doi: 10.1089/acu.2009.0715
13. Cakmak YO. Electroacupuncture reduces uterine artery blood flow impedance. Taiwan J Obstet Gynecol. (2010) 49:390. doi: 10.1016/S1028-4559(10)60084-8
14. Napadow V, Ahn A, Longhurst J, Lao L, Stener-Victorin E, Harris R, et al. The status and future of acupuncture mechanism research. J Altern Complement Med. (2008) 14:861–9. doi: 10.1089/acm.2008.SAR-3
15. Balk J, Catov J, Horn B, Gecsi K, Wakim A. The relationship between perceived stress, acupuncture, and pregnancy rates among IVF-ET patients: a pilot study. Complement Ther Clin Pract. (2010) 16:154–7. doi: 10.1016/j.ctcp.2009.11.004
16. Han JS. Acupuncture and endorphins. Neurosci Lett. (2004) 361:258–61. doi: 10.1016/j.neulet.2003.12.019
17. Sniezek DP, Siddiqui IJ. Acupuncture for treating anxiety and depression in women: a clinical SR. Med Acupuncture. (2013) 25:164–72. doi: 10.1089/acu.2012.0900
18. Jang S, Kim KH, Jun JH, You S. Acupuncture for in vitro fertilization in women with poor ovarian response: a systematic review. Integr Med Res. (2020) 9:100395. doi: 10.1016/j.imr.2020.02.003
19. Smith CA, Armour M, Shewamene Z, Tan HY, Norman RJ, Johnson NP. Acupuncture performed around the time of embryo transfer: a systematic review and meta-analysis. Reprod Biomed Online. (2019) 38:364–79. doi: 10.1016/j.rbmo.2018.12.038
20. Gu YE, Zhang X, Zhang Q, Dai MC, Wu Y, Zhou Y, et al. The effects of acupuncture on pregnancy outcomes of in vitro fertilization with embryo transfer: an interdisciplinary systematic review. J Gynecol Obstet Hum Reprod. (2019) 48:677–84. doi: 10.1016/j.jogoh.2019.07.008
21. Xie Z, Peng Z, Yao B. The effects of acupuncture on pregnancy outcomes of in vitro fertilization: a systematic review and meta-analysis. Complem Alter Med. (2019) 19:131. doi: 10.1186/s12906-019-2523-7
22. Zhang X, Lee M, Smith CA. Effects of acupuncture during in vitro fertilization or intracytoplasmic sperm injection: an updated systematic review and meta-analysis. Eur J Integrat Med. (2018) 23:14–25. doi: 10.1016/j.eujim.2018.09.001
23. Jo J, Lee YJ. Effectiveness of acupuncture in women with polycystic ovarian syndrome undergoing in vitro fertilisation or intracytoplasmic sperm injection: a systematic review and meta-analysis. Acupunct Med. (2017) 35:162–70. doi: 10.1136/acupmed-2016-011163
24. Yang HS, Fang YG, Li XT. Effects of acupuncture on pregnancy in patients undergoing in vitro fertilization and embryo transfer: a systematic review of RCTs. Chin J Tradition Chin Med Pharm. (2017) 32:5591–8.
25. Qian Y, Xia XR, Ochin H, Huang C, Gao C, Gao L, et al. Therapeutic effect of acupuncture on the outcomes of in vitro fertilization: a systematic review and meta-analysis. Arch Gynecol Obstet. (2017) 295:543–58. doi: 10.1007/s00404-016-4255-y
26. Shen C, Wu M, Shu D, Zhao X, Gao Y. The role of acupuncture in in vitro fertilization: a systematic review and meta-analysis. Gynecol Obstet Invest. (2015) 79:1–12. doi: 10.1159/000362231
27. Zheng CH, Huang GY, Zhang MM, Wang W. Effects of acupuncture on pregnancy rates in women undergoing in vitro fertilization: a systematic review and meta-analysis. Fertil Steril. (2012) 97:599–611. doi: 10.1016/j.fertnstert.2011.12.007
28. Jie Y. Systematic Review of Acupuncture in In-Vitro Fertilization and Embryo Transfer. Master's thesis. Heilongjiang university of Chinese medicine, Haerbin (China) (2009).
29. Manheimer E, Zhang G, Udoff L, Haramati A, Langenberg P, Berman BM, et al. Effects of acupuncture on rates of pregnancy and live birth among women undergoing in vitro fertilisation: systematic review and meta-analysis. BMJ. (2008) 336:545–9. doi: 10.1136/bmj.39471.430451.BE
30. Schwarze JE, Ceroni JP, Ortega-Hrepich C, Villa S, Crosby J, Pommer R. Does acupuncture the day of embryo transfer affect the clinical pregnancy rate? Systematic review and meta-analysis. JBRA Assist Reprod. (2018) 22:363–8. doi: 10.5935/1518-0557.20180057
31. Manheimer E, van der Windt D, Cheng K, Stafford K, Liu J, Tierney J, et al. The effects of acupuncture on rates of clinical pregnancy among women undergoing in vitro fertilization: a systematic review and meta-analysis. Hum Reprod Update. (2013) 19:696–713. doi: 10.1093/humupd/dmt026
32. Qu F, Zhou J, Ren RX. Effects of acupuncture on the outcomes of in vitro fertilization: a systematic review and meta-analysis. J Altern Complement Med. (2012) 18:429–39. doi: 10.1089/acm.2011.0158
33. El-Toukhy T, Sunkara SK, Khairy M, Dyer R, Khalaf Y, Coomarasamy A. A systematic review and meta-analysis of acupuncture in in vitro fertilisation. BJOG. (2008) 115:1203–13. doi: 10.1111/j.1471-0528.2008.01838.x
34. Shea BJ, Reeves BC, Wells G, Thuku M, Hamel C, Moran J, et al. AMSTAR-2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. (2017) 358:j4008. doi: 10.1136/bmj.j4008
35. RoBIS tool. Bristol Medical School: Population Health Sciences. Available online at: http://www.bristol.ac.uk/population-health-sciences/projects/robis/robis-tool/ (accessed January 31, 2021).
36. Guyatt GH, Oxman AD, Vist GE, Kunz R, Falck-Ytter Y, Alonso-Coello P, et al. GRADE: an emerging consensus on rating quality of evidence and strength of recommendations. BMJ. (2008) 336:924–6. doi: 10.1136/bmj.39489.470347.AD
37. Brozek JL, Akl EA, Alonso-Coello P, Lang D, Jaeschke R, Williams JW, et al. Grading quality of evidence and strength of recommendations in clinical practice guidelines. Part 1 of 3. An overview of the GRADE approach and grading quality of evidence about interventions. Allergy. (2009) 64:669–77. doi: 10.1111/j.1398-9995.2009.01973.x
38. Zhang F, Sun M, Han S, Shen X, Luo Y, Zhong D, et al. Acupuncture for primary dysmenorrhea: an overview of systematic reviews. Evid Based Complement Alternat Med. (2018) 2018:8791538. doi: 10.1155/2018/8791538
39. Li M, Xing X, Yao L, Li X, He W, Wang M, et al. Acupuncture for treatment of anxiety, an overview of systematic reviews. Complement Ther Med. (2019) 43:247–52. doi: 10.1016/j.ctim.2019.02.013
40. Dettori JR, Skelly AC, Brodt ED. Critically Low confidence in the results produced by spine surgery systematic reviews: an AMSTAR-2 evaluation from 4 spine journals. Global Spine J. (2020) 10:667–73. doi: 10.1177/2192568220917926
41. Paulus WE, Zhang M, Strehler E, El-Danasouri I, Sterzik K. Influence of acupuncture on the pregnancy rate in patients who undergo assisted reproduction therapy. Fertil Steril. (2002) 77:721–4. doi: 10.1016/S0015-0282(01)03273-3
42. Lund I, Näslund J, Lundeberg T. Minimal acupuncture is not a valid placebo control in randomised controlled trials of acupuncture: a physiologist's perspective. Chin Med. (2009) 4:1. doi: 10.1186/1749-8546-4-1
Appendix
The following search strategy was used for EMBASE and was modified to suit other databases.
#1. “in vitro fertilization”/exp OR “in vitro fertilization” (94,173)
#2. “intracytoplasmic sperm injection” (22,292)
#3. “embryo transfer” (34,983)
#4. “assisted reproductive techniques” (2,769)
#5. #1 OR #2 OR #3 OR #4 (9,7692)
#6. acupuncture (51,982)
#7. “acupuncture therapy” (1,780)
#8. “acupuncture points” (2,067)
#9. “electroacupuncture” (8,057)
#10. “acupressure” (2,405)
#11. “acupuncture analgesia” (2,164)
#12. #6 OR #7 OR #8 OR #9 OR #10 OR #11 (54,401)
#13. “review it” (2,912)
#14. “systematic review” (330,910)
#15. “meta analysis” (290,000)
#16. “systematic* review*” (357,380)
#17. “meta analy*” (307,640)
#18. #13 OR #14 OR #15 OR #16 OR #17 (504,371)
#19. #5 AND #12 AND #18 (88).
Keywords: acupuncture, in vitro fertilization, systematic reviews, overview, methodological quality
Citation: Wang X, Wang Y, Wei S, He B, Cao Y, Zhang N and Li M (2021) An Overview of Systematic Reviews of Acupuncture for Infertile Women Undergoing in vitro Fertilization and Embryo Transfer. Front. Public Health 9:651811. doi: 10.3389/fpubh.2021.651811
Received: 11 January 2021; Accepted: 19 March 2021;
Published: 20 April 2021.
Edited by:
Kevin Lu, University of South Carolina, United StatesReviewed by:
Nan Huo, Mayo Clinic, United StatesXiaomo Xiong, University of South Carolina, United States
Copyright © 2021 Wang, Wang, Wei, He, Cao, Zhang and Li. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Shaobin Wei, d2Vpc2hhb2JpbjU2MjBAMTYzLmNvbQ==
†These authors have contributed equally to this work and share first authorship