 Aisha Khan1,2
Aisha Khan1,2 Haroon Ahmed1*Shaheera Amjad1
Haroon Ahmed1*Shaheera Amjad1 Muhammad Sohail Afzal3
Muhammad Sohail Afzal3 Waseem Haider1
Waseem Haider1 Sami Simsek4Mudassar Rashid Khawaja5Danish Hassan Khan6
Sami Simsek4Mudassar Rashid Khawaja5Danish Hassan Khan6 Shumaila Naz6
Shumaila Naz6 Anna Durrance-Bagale7
Anna Durrance-Bagale7 Rana Muhammad Kamran Shabbir3Raja Zoq Ul Arfeen8Shahzad Ali9
Rana Muhammad Kamran Shabbir3Raja Zoq Ul Arfeen8Shahzad Ali9 Jianping Cao2,10,11,12*
Jianping Cao2,10,11,12*- 1Department of Biosciences, COMSATS University Islamabad, Islamabad, Pakistan
- 2Key Laboratory of Parasite and Vector Biology, National Health Commission of the People's Republic of China, Shanghai, China
- 3Department of Lifesciences, School of Science, University of Management and Technology, Lahore, Pakistan
- 4Department of Parasitology, Firat University, Elâziğ, Turkey
- 5Department of Economics, COMSATS University Islamabad, Islamabad, Pakistan
- 6Department of Biological Sciences, National University of Medical Sciences, Rawalpindi, Pakistan
- 7Faculty of Public Health and Policy, London School of Hygiene and Tropical Medicine, London, United Kingdom
- 8School of Food and Agricultural Sciences, University of Management and Technology (UMT), Lahore, Pakistan
- 9Department of Wildlife and Ecology, University of Veterinary and Animal Sciences, Lahore, Pakistan
- 10National Institute of Parasitic Diseases, Chinese Center for Disease Control and Prevention, Shanghai, China
- 11The School of Global Health, Chinese Center for Tropical Diseases Research, Shanghai Jiao Tong University School of Medicine, Shanghai, China
- 12WHO Collaborating Centre for Tropical Diseases, Shanghai, China
Background: The parasitic disease, cystic echinococcosis (CE), is a serious health problem in Pakistan. Risk of disease transmission is increased by economic and political instability, poor living conditions, and limited awareness of hygienic practices. The current study aimed to investigate the community perception and awareness regarding the risk factors of CE in Pakistan, from a One Health perspective.
Methods: We conducted a community-based survey involving 454 participants in the major cities of Pakistan. Quantitative data based on knowledge, attitude, and practices (KAP), the One Health concept, risk factors, and community perception of CE among the general population of the major cities of Pakistan were collected. The questions included those related to knowledge, attitude, practices, One Health concept, risk factors, and community perception. The Chi-squared test was applied to determine the associations regarding KAPs across socio-demographic parameters.
Results: KAPs had no significant associations with sociodemographic aspects such as age, sex, religion, ethnicity, education, marital status, occupation, or financial status of the participants. The findings indicated a lack of awareness about CE among the participants. Respondents were unaware of the risk factors and the One Health concept of CE. However, the community attitude and perception were positive toward the control of CE.
Conclusion: Illiteracy, deficient sanitation systems and lack of awareness are the contributing factors to CE in Pakistan. It is necessary to make the community aware regarding CE and its importance. Increasing this awareness represents an important step toward the eradication and control of CE.
Introduction
Zoonotic diseases spread between animals (usually vertebrates) and humans via direct or indirect contact (1), and represent about one-fifth of parasitic infections in nature (2). Echinococcosis is one of the most significant and widespread chronic diseases worldwide (3, 4). It is caused by taeniid Echinococcus spp. tapeworms at their larval stages, the life cycle of which involves two vertebrate hosts: definitive and intermediate (5). Humans are occasional intermediate hosts, and are infected via ingestion of contaminated food or water, or through contact with infected definitive hosts (6). Echinococcus multilocularis (causing alveolar echinococcosis) and E. granulosus sensu lato (causing cystic echinococcosis) are of major public health importance (7).
Cystic echinococcosis (CE) is a serious public health problem around the world (8) and is listed as one of the 20 neglected tropical diseases (NTDs) in the Neglected Zoonotic Diseases (NZDs) sub-group by the World Health Organization (WHO) (9, 10). CE is more common in sheep-raising countries (8, 11–14). Human CE has the highest prevalence in the eastern part of the Mediterranean region, southern and eastern Europe, and the least half of South America, Northern Africa, Australia, Russia, Western China, Siberia, and in Central Asia, where approximately 2–3 million people are infected and 200,000 new cases are reported annually (9, 14, 15). Central Asia, including Afghanistan, Kazakhstan, Kyrgyzstan, Iran, Tajikistan, Turkmenistan, Mongolia, Uzbekistan, Western China, and Pakistan, is a highly endemic region for CE, with ~58% of the population at being at risk (16).
Pakistan is an agricultural country, in which about 47% of the population are involved in agriculture. Livestock, the backbone of the agricultural sector, has a significant role in the economy of Pakistan, contributing almost 56.3% of the agricultural value and 11% of the GDP (17, 18). However, parasitic infections (including echinococcosis) cause economic losses of around 26.5 million rupees or $354000US annually to the livestock sector (19). Many reasons, including insufficiently equipped abattoirs located in the vicinity of residential areas, the proximity of animals (especially dogs and livestock) to humans, poor public awareness, and unhygienic lifestyles favor the lifecycle of E. granulosus (20).
Human health is strongly related to a country's socioeconomic status. However, various aspects of socioeconomic status (education, ethnicity, and financial resources) are disproportionately linked to health. Some aspects promote health, some are aspects are promoted by health, some are mutually determined with health, and some fall in all three categories (21). Pakistan is a country with low socioeconomic status, where aspects of socioeconomic status generally have a negative impact on health, because it is highly populated (around 200 million inhabitants) with poor living standards, and most of the population lives in underdeveloped, rural settings. Lifestyle in these areas, where humans and animals often share the same residences, and poor health and hygiene practices are followed, is a major risk for disease transmission (22). According to a Pakistan economic survey, 38% of the population was declared poor during in 2015/2016, with 41% in rural areas and 32% in urban areas. Only around 5% of households have access to clean water, proper sanitation, electricity, and cooking fuel. E. granulosus s.s (G1–G3 genotypes) has already been reported in livestock in Pakistan, and all factors are likely to contribute to its further spread among the population (23).
Over time, the livestock sub-sector in Pakistan has surpassed the crops sub-sector as the primary contributor to agriculture. During 2019-20, livestock contributed 60.6% to overall agriculture and 11.7% to GDP. The value of the livestock sector can be gauged by the fact that it accounts for around 3.1% of total exports and provides 35-40% of income for more than 8 million rural households. Goats (78.2 million), cattle (49.6 million), buffalo (41.2 million), and sheep make up the majority of Pakistan's livestock (31.2 million). The goat population in Pakistan ranks third in the world, after India and China, in livestock farming. Sheep and goats contribute significantly to the economy of the country by providing milk, meat, beef, and hides. Agriculture contributes 19.3% to Pakistan's GDP and employs 42.3% of the population. Despite a large population of sheep and goats, Pakistan's low volume ruminant production is severely hampered by a number of factors, including a lack of acaricides (24).
Few studies have examined the drivers of CE. Between 1990 and 2018, 15 retrospective survey-based studies and 19 case studies reported 1,611 cases of CE in Pakistan. The absence of a surveillance system or a national database to identify and record CE cases has resulted in a substantial data gap (16). As an infectious disease, the success of CE prevention and control programmes depends on community cooperation. Understanding all the disease-related aspects is an important determinant of community participation in programme implementation. In the present study, we investigated community knowledge, attitudes, and the One Health approach toward CE in Pakistan, particularly related to health and risk factors.
Materials and Methods
Study Design, Sampling and Selection Criteria
Pakistan is one of the most suitable countries for studying CE because the livestock sector is a major contributor to the economy. Many geographical and demographical features also promote the onset and spread of CE. This study aimed to evaluate the level of awareness of CE among residents of Pakistan; therefore, we interviewed people in major cities, including Rawalpindi, Islamabad, Chakwal, Jhelum (including Kalar Kahar), Quetta, Karachi, Hyderabad, Lahore, Peshawar, and Northern Areas (Figure 1). Urban and rural areas around or within these cities were included. We used convenience sampling to select the participants. Pakistan is an ethnically diverse country with many different communities, e.g., Punjabi, Pathan, and Kashmiri; therefore, a diverse sample is possible even in one city. Individuals with or without any kind of animal association and of any occupational and educational background were considered for sampling. All participants were aged at least 15 years old.
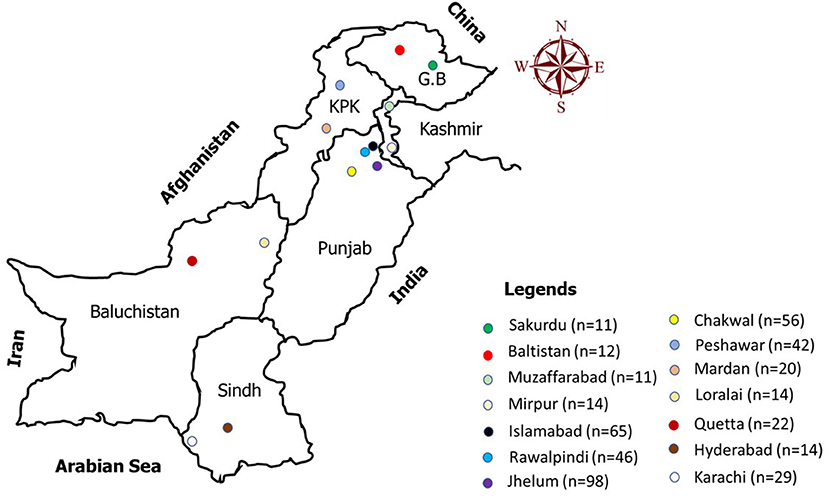
Figure 1. Map of Pakistan with multiple dots depicting the sampling sites where the data were collected.
A total of 454 people participated in the study (Table 1). Hospital staff; those in educational institutions, markets, and homes; and transport passengers were surveyed using face to face interview.
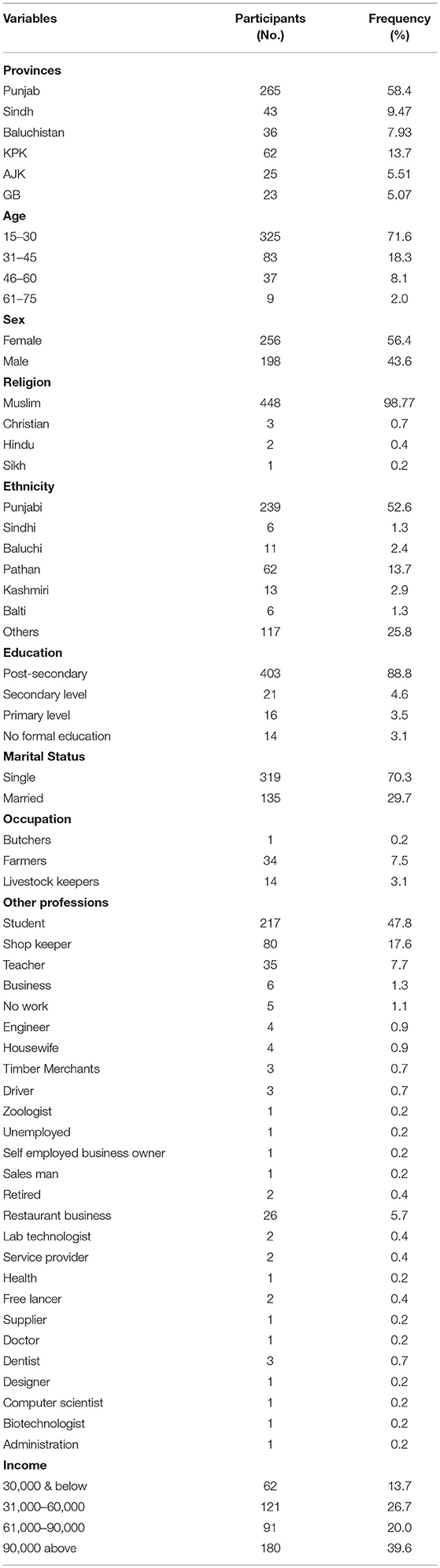
Table 1. Sociodemographic characteristics of the participants.
Community Questionnaire Survey
A community-based, cross-sectional study was designed to collect the data. An easy descriptive questionnaire was designed for both rural and urban participants. For participants not able to read or write, face-to-face interviews were conducted using the same questionnaire to obtain the data.
The questionnaire was divided into six major categories:
(1) Knowledge regarding CE, such as general awareness of the disease and its mode of transmission.
(2) Attitude, such as views on symptoms, treatment, and diagnosis.
(3) Practices related to the disease, such as the feed given to dogs, hand washing, and proximity to dogs.
(4) Risk factors regarding CE in the surveyed areas, such as the consumption of contaminated food and water, and slaughtering systems
(5) Social, political, and economic instability commonly observed in the surveyed areas.
(6) Questions related to the One Health concept (animal-environment-human) of CE and the community perception of prevention and control.
All these questions had either a Yes or No answer (see Supplementary Material).
Data Management and Statistical Analysis
This was a multivariate analysis, including dependent and independent variables.
Dependent Variables
These included: (1) knowledge about CE, (2) attitude toward treatment of infection or exposure to animals, (3) practices and factors associated with the spread of CE, (4) the One Health concept related to CE, (5) risk factors of CE, and (6) community perception in general toward CE.
Independent Variables
These were sex, age, occupation, level of education, religion, ethnicity, marital status, and income.
A database was established using MS Excel (Microsoft, Redmond, WA, USA) and then analyzed statistically using SPSS (v. 23 Version; IBM Corp., Armonk, NY, USA). Bivariate correlation was checked with the help of the Chi-squared test, where one dependent variable was weighed against one independent variable. The relationships of the different sociodemographic factors to knowledge, attitudes, practices, the One Health concept, risk factors, and community perception were analyzed. Statistically significant results were recorded at p < 0.05.
Results
Sociodemographic Background
Men (n = 198; 44%) and women (n = 256; 56%) ranged in age from 16 to 75 years. Most participants were of Punjabi ethnicity (53%), followed by Pathans (14%), Kashmiri (3%), Baloch (2%), Sindhi and Balti (1%), with 26% from other ethnicities. About 11% worked directly or indirectly with livestock, including farmers (8%), livestock owners (3%), and butchers (0.2%). Approximately 89% of the participants had other professions. Regarding the level of education, 5% were educated up to secondary level and 3% had no formal education (Table 1).
KAP Analysis
Regarding knowledge, 68% (309/454) of participants had never heard about zoonoses and 80% (361/454) were unaware of CE. The majority had never seen the disease in any individual or animal. Approximately 90% (410/454) of the respondents did not know that they could get infected with the disease. The attitude of participants was quite positive: 62% (283/454) would accept CE inspection, treatment, or surgery (if required). Stray dogs were reported by 58% (265/454) of participants; 85% (385/454) of participants washed their hands after handling cattle and 90% (407/454) washed their hands before eating. Only 58% (262/454) reported that slaughter areas were well-managed, while 64% (288/454) reported meat inspection before consumption (Table 2).
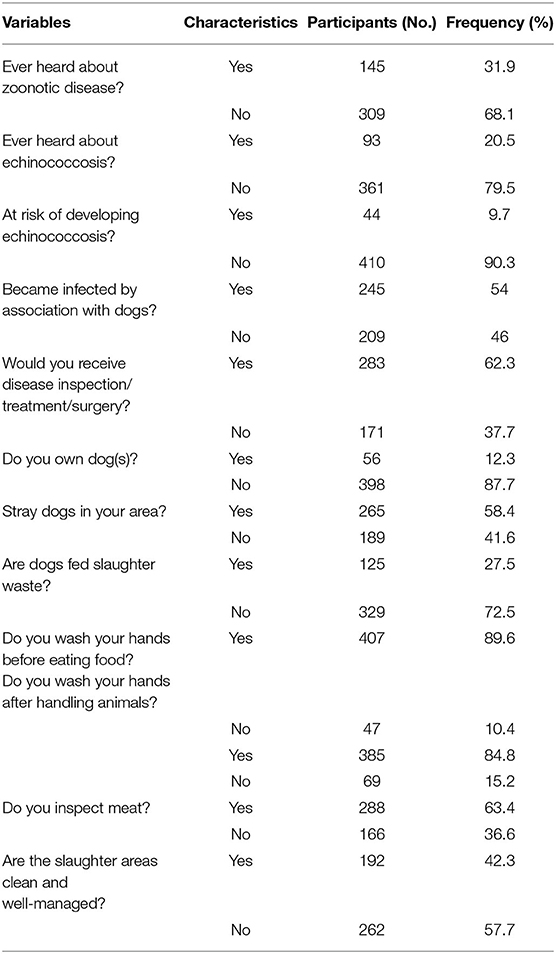
Table 2. Knowledge, attitude, and practices (KAPs) toward CE among the study respondents.
The One Health Concept of Cystic Echinococcosis
Despite low awareness of the disease, the response of participants toward the concept of One Health was positive. For all seven questions about One Health, most stated that all the suggested steps were important to ensure a healthy environment for animals and thus promote human health. Highest support (94%) was seen for the requirement of proper treatment facilities, followed by awareness and vaccination campaigns (91%). There was a positive response for the suggestion of proper waste disposal systems (93%) and food inspection (92%; Table 3).

Table 3. Representation of one health concept of CE across different variables.
Risk Factors of Cystic Echinococcosis
Regarding the risk factors surveyed, most (86%) of the participants considered lack of awareness as an important risk factor for the disease. Others identified unchecked systems of animal keeping (80%), contaminated water/food consumption (74%), and social, political, and economic instability (82%; Table 4).
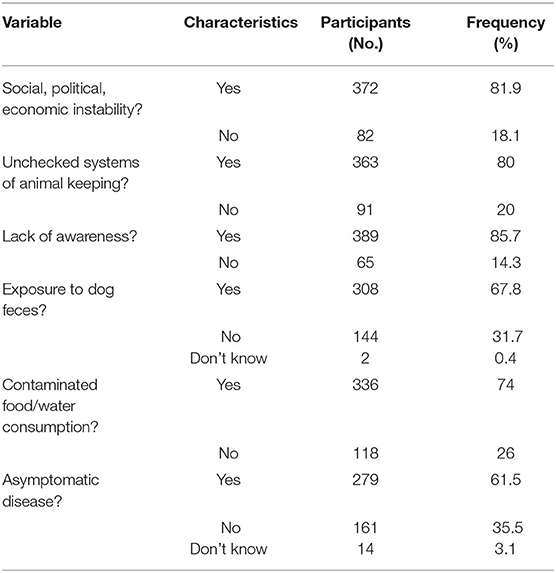
Table 4. Representation of Risk factors of CE across different variables.
Community Perceptions of Cystic Echinococcosis
We suggested 10 preventive or precautionary measures people could take to reduce, avoid, or eliminate CE. For each measure, two options were provided: one in favor of the measure and the other against it. Only 17% of participants favored the option of killing all dogs, while 47.6% thought only stray dogs should be killed. Sixty two point eight percentage thought reducing dogs' access to slaughter areas would be enough to eliminate the disease. Almost 50:50 ratios were found for prevention and treatment, with respondents considering each to be a disease control measure (Table 5).
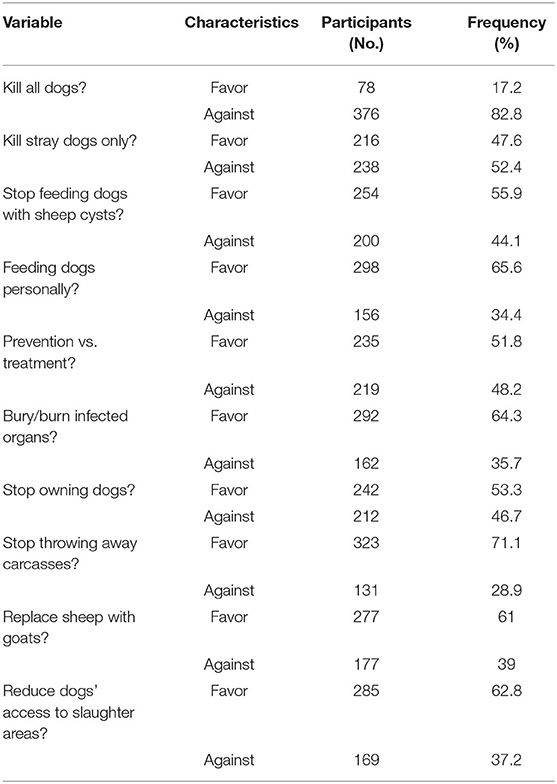
Table 5. Representation of Community perception about CE across different variables.
Analysis of the One Health Concept, Risk Factors, and Community Perception of CE Based on Various Sociodemographic Factors
We analyzed all data with reference to sociodemographic factors to ascertain whether CE awareness and views vary according to age, sex, ethnicity, religion, education, marital status, occupation, and income (Tables 6–8). While testing for the One Health concept, Q3 had significant associations (p < 0.05) with sex and religious orientation. The response to Q1 was different in various ethnic groups. The responses to Q2, Q6, and Q7 (Table 6) varied by different educational backgrounds. For the risk factors (Table 7), different age groups had different responses to Q4 (p < 0.05), while the different sexes had significantly different responses to Q2 and Q6. The various ethnic groups had different responses to Q2, Q3, Q4, Q5, and Q6. People with various educational levels responded differently to Q, Q4, Q5, and Q6 while people with different occupations responded similarly except for Q3 and Q4. Income levels did not seem to have much influence on people perception of risk. In community perception (Table 8), marital status had a significant effect on opinion (response to Q1, Q2, Q8, and Q10) while the responses to Q10 were associated with age, education and ethnicity, Q3 was associated with sex and Q4 was associated with education (p < 0.05).
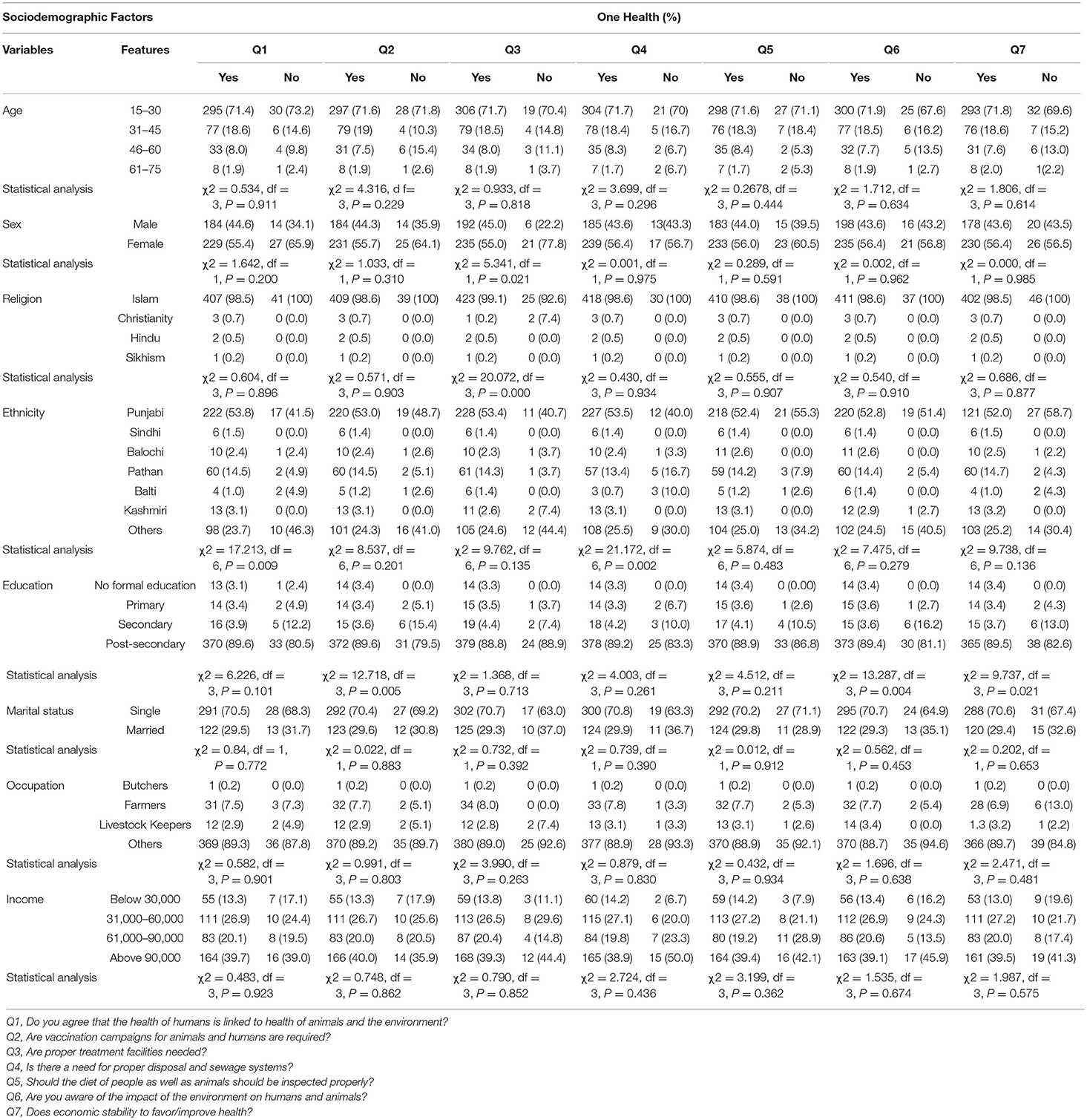
Table 6. Representation of Sociodemographic factors across One Health concept of CE questions.
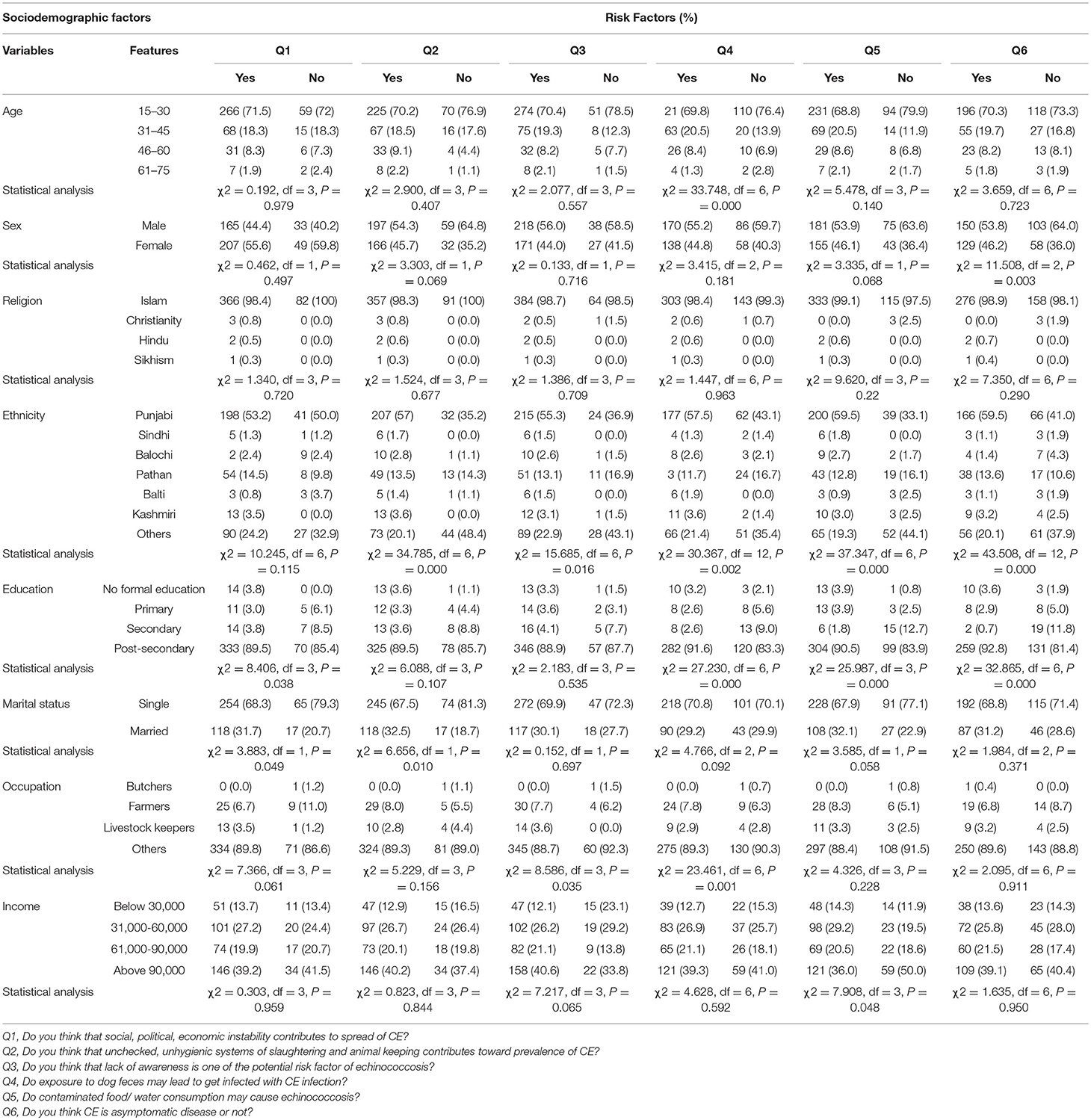
Table 7. Representation of Sociodemographic factors based on risk factors of CE questions.
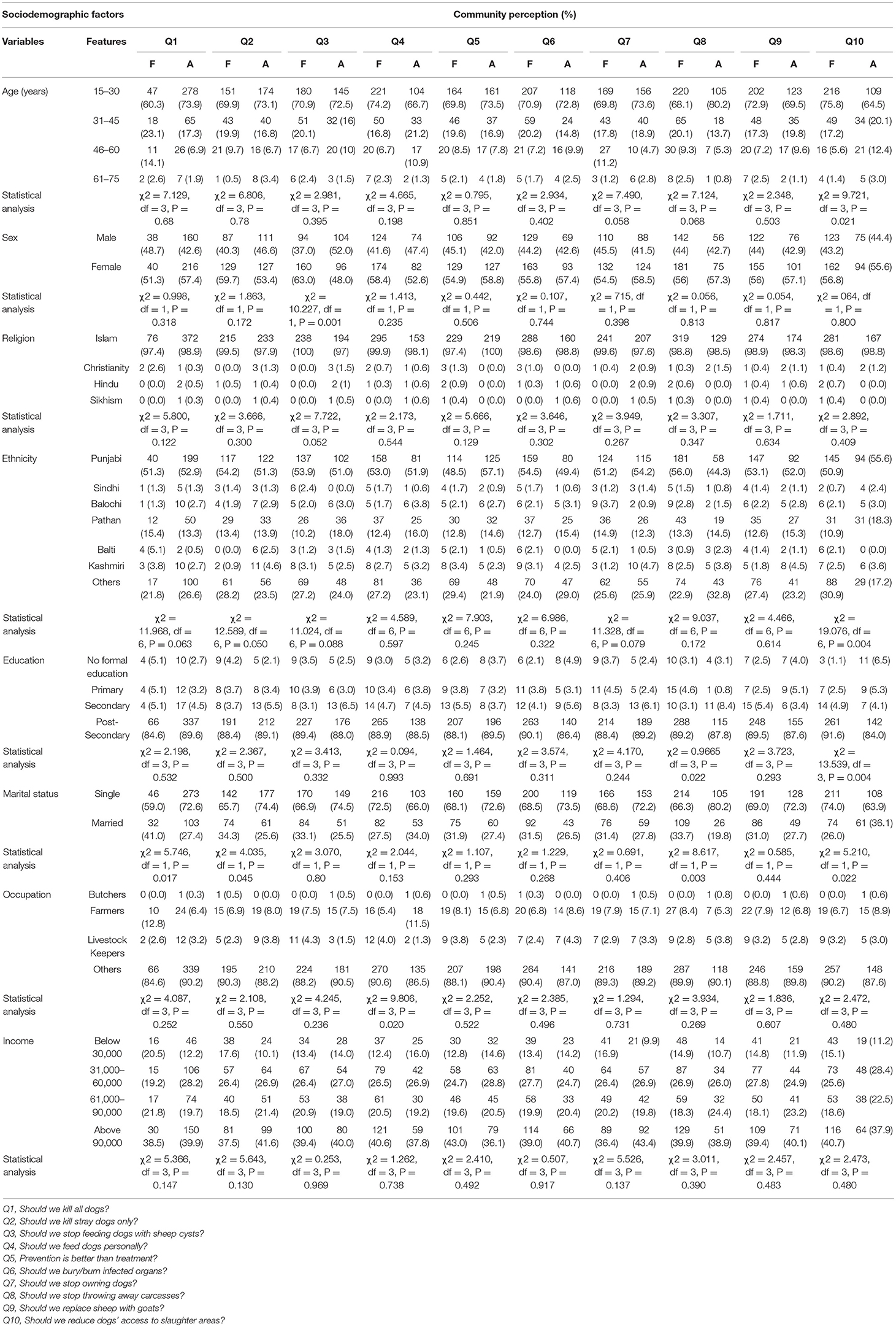
Table 8. Presentation of Community perception across sociodemographic factors.
Statistical Analysis for Knowledge, Attitude, Practices, One Health Concept, Risk Factors, and Community Perception of Cystic Echinococcosis
The factors that determine views on KAP, One Health, risk factors, and community perception (dependent variables) about CE included age, sex, religion, ethnicity, education, marital status, occupation, and income (independent variables). The results of the analysis demonstrated that only ethnicity (p < 0.05) within a section of knowledge was significant, while sex (p = 0.05) was close to significance. Among practices, significant differences were only demonstrated for sex (p < 0.05; Tables 9, 10).
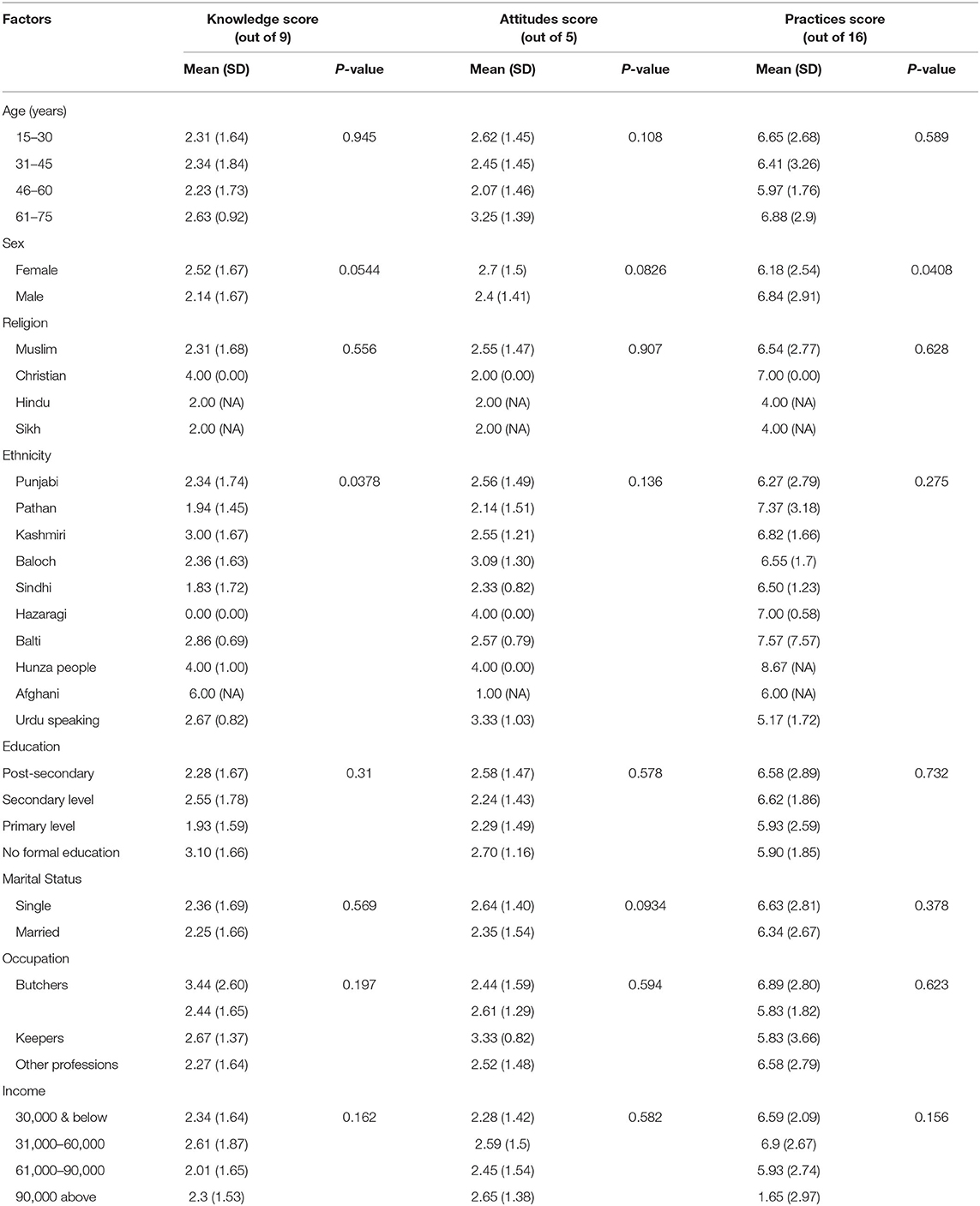
Table 9. Statistical analysis of knowledge, attitude, and practices across different socio-demographic variables.
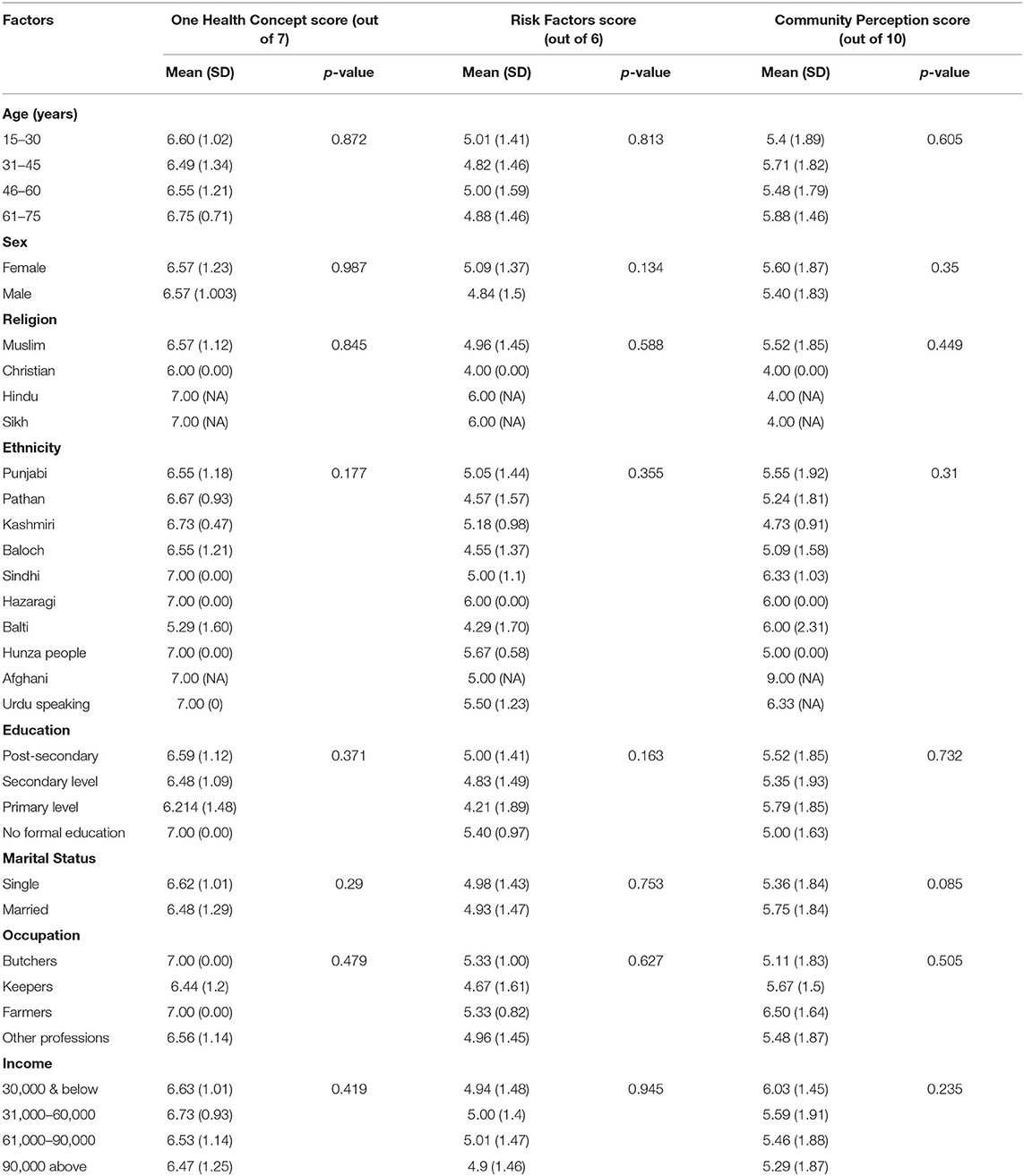
Table 10. Statistical analysis of one health concept, risk factors, and community perceptions.
Discussion
The Sociodemographic Background of the Participants
Age, sex, religion, ethnicity, education, marital status, occupation, and income were included as key sociodemographic factors in the analysis to examine their role and association with the spread of CE in Pakistan. A previous study has shown that moving from high to low on any socioeconomic aspect, income, or education results in a decline in health (21).
More highly educated individuals reported better health and lower mortality risks in various studies conducted in different countries (25–27). Among 454 surveyed individuals in the current study, very few people were illiterate (3.1%; 14/454), while 3.5% (16/454) had experienced primary education and 4.6% (21/454) had secondary level education. Most, 88.8% (403/454), had post-secondary education. All participants had little knowledge of zoonotic infections. Participants showed no significant difference in their level of knowledge, despite belonging to varying educational backgrounds. This scenario is not unusual for neglected tropical diseases such as CE, where even the educated population is unaware of the disease. However, education does have a role in other factors associated with CE, such as hand washing, water boiling, and perception of the disease. This highlights the role of education in the control of disease transmission and better education is expected to reduce transmission of the disease (28).
Many public health researchers state that income and associated resources are the most influential factors on health and mortality (29). In one study, an increase in household income from $20,000 to $70,000 reduced the odds of mortality by 50% (30). An interesting finding in our study was that participants were reluctant to seek treatment for financial reasons.
Much research has linked health to occupational rank. Higher mortality rates in servants with low prestige jobs were associated with daily practices and behaviors, whereas officials with a higher rank had a lower obesity rate, fewer were addicted to tobacco, and they had a good diet, better health care practices, and less stress (31, 32). We observed similar findings: people belonging to livestock-related occupations, where they have contact with animals, such as butchers, keepers, and farmers, have higher chances of getting CE because of their occupation. Many other studies have reported the same observation, with a higher incidence of CE in a pastoral community in than participants with other occupations (33–36). In a survey among hunters in China, few cases were found (37). This low disease frequency in hunters and higher frequency in farmers proves that occupational activity contributes to the disease, not only because of the association with animals, but by certain behaviors, attitudes, perceptions, and practices, such as hand washing.
Different ethnic groups were included in the study to ascertain whether there are certain cultural practices that could promote the transmission of the disease and make it more common in a particular group. The results of suggested that there were no significant differences, indicating that CE is equally prevalent in all ethnic groups. This could be because, in Pakistan, the livestock-related practices are similar in all regions.
KAP Analysis of CE
KAP questions were included to better analyse the major variables (risk factors, One Health, community perception) among participants, prompting them to link, compare, and evaluate these variables based on their knowledge and attitude toward the disease and the practices they follow.
The results of our survey corresponded well with those from one performed in 2018 in Pakistan (16), with participants in both studies demonstrating a clear lack of knowledge. Frequencies of familiarity with zoonoses now and in 2018 were 31.9 and 30%, respectively, while awareness of CE was 20.5 and 4.2%, indicating contrasting results compared with those of the previous study.
The participants were not familiar with the disease and its mode of transmission; therefore, they did not consider themselves at risk of developing the disease or getting infected by animals or other people.
A mixture of good and bad practices were found in both studies, based primarily on knowledge and perception of health in general and not about CE in particular. The frequency of people washing their hands before eating (90%) and after handling cattle (85%) demonstrated the general awareness of the population about cleanliness and the belief that not following these practices might affect their health and lifestyle. However, some specific practices, such as inspection of meat before consumption, either by themselves or by their animals (32%−2018, 63%–current) and the presence of stray dogs (70%−2018, 58%–current) demonstrated that people are not aware of the disease being spread by animals.
The One Health Concept of CE
The concept that human health is linked to that of animals and the environment was well-known to the participants. Reservoirs of Echinococcus species and an increase in disease transmission are outcomes of urbanization. Anthropogenic environmental changes, such as those caused by deforestation and urbanization, affect wildlife and can lead to zoonotic disease transmission in humans (38).
Increased host range and enhanced parasitic transmission between definitive and intermediate hosts, caused by environmental changes, might put humans at risk of increased echinococcosis transmission (38). Intermediate hosts of zoonotic diseases feed on vegetation, and their numbers will increase because of improvements in the quality and quantity of their food source, thus increasing the potential for disease spread to humans (39–42).
Natural or anthropogenic ecological changes for migratory host species, such as lack of food, deforestation, and urbanization, have adverse effects on host migratory behaviors, and thus preventing migration would have a substantial impact on the transmission of species causing echinococcosis. Less or no migration would end up concentrating the entire population of wildlife in human settlements and would create competition for resources for their survival, ultimately transmitting the disease. For example, in Australia, deforestation was reported as the main cause of an outbreak of Hendra virus, a result of migration of flying foxes from forested areas to human settlements in search of food, thus transmitting the virus (43).
Assessment of Risk Factors for CE
As mentioned earlier, the economy of Pakistan is highly dependent on livestock. This population is at high risk of developing CE because no proper hygiene practices are followed while dealing with animals (22). Most of the participants in this study also saw this as a major risk factor of CE in Pakistan.
Similar findings were recorded from rural households in Algeria. More cases were recorded from rural communities (71%), the reason being their dependence on livestock for the earnings, without awareness of prevention and curative measures. The association of disease with livestock contact was described in a study where the population associated with animal husbandry was more at risk of disease, with at least one case of CE per house in Algeria. A study from Algeria also recorded at least one case (p < 0.001) in 14.6% of rural and 4.6% of urban houses, suggesting that migration and urbanization are also risk factors, carrying the disease to the cities (44).
The socioeconomic and political situation is a risk factor for promoting this disease, similar to China (45). The same factor may also be a major reason for disease spread in Pakistan, as no policies, budget support for health issues, education, or other awareness programs exist to control the disease.
Human CE infection is mainly associated with contact with dogs. In a study in Algeria, 29.8% of participants reported that dogs had access to their homes and 9.3% reported access to kitchens, posing a major threat of disease transmission via food contamination with dog feces. Owning more than one dog was associated with hydatidosis (p < 0.1) in urban areas in Algeria. Moreover, the disease was also reported to be caused by the presence of stray dogs in the district (44). The scenario in Pakistan is similar, as the population of stray dogs is uncontrolled; therefore, human settlements are likely to be contaminated with their feces. Poor community awareness of CE and knowledge about modes of transmission were stated to be major risks in the present study. Similarly, in a study of CE in Algeria, disease awareness was about 50%, with only 21% of respondents aware of disease transmission from dogs to other animals and humans (44). Many other studies have reported similar findings, such as those in Morocco (46–49).
Community Perception Toward CE
In the current study, several control measures related to CE were highlighted to ascertain how aware the participants were of the disease. Participants had mixed or ambiguous views, showing a lack of awareness about the disease: most of them (71%) disagreed with throwing carcasses in open areas, but 48% stated that prevention should not be preferred over treatment because it needs a high level of awareness. Almost 63% of them were in favor of keeping dogs away from slaughter areas; however, in Pakistan the slaughter areas are privately owned property and are not managed by government authorities. We concluded that in a country where people face health-related issues every day, they are willing to support any program promising to improve their living standard, but are not capable of identifying exactly what should be done.
A study in Morocco found that participants were willing to support suggested control measures, such as waste disposal systems, hygiene conditions, and management of slaughter areas (47). However, the specific cultural practices in the community, including offal and waste disposal systems, home slaughtering, and keeping animals are risk factors that hinder disease control. Despite acknowledging CE as a serious health risk, the community was not aware of the parasite, its life cycle, and other associated mechanisms. This highlights the significance of providing knowledge and awareness of the disease to the public (50).
Conclusion
Our study demonstrated a low awareness of CE in Pakistan, despite the prevalence of the disease in the country. The population showed positive responses toward the treatment of the disease and to suggested risk factors and community perception aspects. Improving these could help to control the disease. The participants were unaware of the factors associated with the disease, such as its mode of transmission, practices favoring its spread, control, and other associated factors. However, the current practices being followed by them, directly or indirectly, can predispose them to parasitic infection and transmission of CE. The results of the present study add to the existing knowledge regarding KAPs of cystic echinococcosis One Health perspective and is the representative of a South Asian population (Pakistan). This study will also pave the way for further studies at national and international level. However, the current study also had some limitations such as the data from major cities may not present the clearer picture regarding CE in provinces or national level. Respondents with different origins, ages, ethnic groups, and professions should be equally participated in the study to provide deeper insights and true information about CE KAPs in Pakistan.
Publisher Notes
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Data Availability Statement
The original contributions generated for this study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author/s.
Ethics Statement
The studies involving human participants were reviewed and approved by the Ethics Committee of COMSATS University (CIIT/Bio/ERB/21/01). Written informed consent to participate in this study was provided by the participants' legal guardian/next of kin.
Author Contributions
AK and SAm collected the data and wrote the paper following discussions with MA, SN, and SS. HA and MK designed the study. DK, SAl, and WH helped in the analysis. RS, RA, JC, and AD-B revised the paper and improved the technical quality of the manuscript. HA supervised the study. All authors approved the final version of the paper.
Funding
This study was supported by the National Natural Science Foundation of China (No. 81772225 to JC), the Laboratory of Parasite and Vector Biology, National Health Commission of the People's Republic of China, China (No. WSBKFKT2017-01 to AK), and the Fifth Round of 3-Year Public Health Action Plan of Shanghai (No. GWV-10.1-XK13 to JC). The funders had no role in the study design, the data collection and analysis, the decision to publish, or the preparation of the manuscript.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
The authors were thankful to community members for their support which aided the completion of this study.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2021.648900/full#supplementary-material
Abbreviations
WHO, World Health Organization; NZDs, Neglected Zoonotic Diseases; CE, Cystic Echinococcosis; DALYs, Disability Adjusted Life Years.
References
1. Carmena D, Cardona GA. Echinococcosis in wild carnivorous species: epidemiology, genotypic diversity, and implications for veterinary public health. Vet Parasitol. (2014) 202:69–94. doi: 10.1016/j.vetpar.2014.03.009
2. Torgerson PR, Macpherson CN. The socioeconomic burden of parasitic zoonoses: global trends. Vet Parasitol. (2011) 182:79–95. doi: 10.1016/j.vetpar.2011.07.017
3. Zhang W, Ross AG, McManus DP. Mechanisms of immunity in hydatid disease: implications for vaccine development. J Immunol. (2008) 181:6679–85. doi: 10.4049/jimmunol.181.10.6679
4. McManus DP, Zhang W, Li J, Bartley PB. Echinococcosis. Lancet. (2003) 362:1295–304. doi: 10.1016/S0140-6736(03)14573-4
5. Eckert J, Gemmell MA, Meslin FX, Pawlowski ZS. World Health Organization and World Organization for Animal Health. WHO/OIE Manual on Echinococcosis in Humans and Animals: A Public Health Problem of Global Concern. Geneva: World Health Organization (2001).
6. Ito A, Budke CM. The echinococcoses in Asia: the present situation. Acta Trop. (2017) 176:11–21. doi: 10.1016/j.actatropica.2017.07.013
7. Thompson RC. The taxonomy, phylogeny and transmission of Echinococcus. Exp Parasitol. (2008) 119:439–46. doi: 10.1016/j.exppara.2008.04.016
8. Craig PS, Budke CM, Schantz PM, Tiaoyin L. Human Echinococcosis: a neglected disease. Trop Med Health. (2007) 35:283–92. doi: 10.2149/tmh.35.283
9. World Health Organization. Accelerating Work to Overcome the Global Impact of Neglected Tropical Diseases: A Roadmap for Implementation. Geneva: World Health Organization (2011).
10. Piseddu T, Brundu D, Stegel G, Loi F. The disease burden of human cystic echinococcosis based on HDRs from 2001 to 2014 in Italy. PLOS Negl Trop Dis. (2017) 11:e0005771. doi: 10.1371/journal.pntd.0005771
11. Hernandez A, Cardozo G, Dematteis S, Baz A. Cystic echinococcosis: analysis of serological profile related to the risk factors in individuals without ultrasound liver changes living in an endemic area of Tacuarembo, Uruguay. Parasitology. (2005) 130:455–60. doi: 10.1017/S0031182004006717
12. Romig T, Thoma D, Weible AK. Echinococcus multilocularis–a zoonosis of anthropogenic environments? J Helminthol. (2006) 80:207–12. doi: 10.1079/JOH2006347
13. Dakkak A. Echinococcosis/hydatidosis: a severe threat in Mediterranean countries. Vet Parasitol. (2010) 174:2–11. doi: 10.1016/j.vetpar.2010.08.009
14. McManus DP. Echinococcosis with particular reference to Southeast Asia. Adv Parasitol. (2010) 72:267–303. doi: 10.1016/S0065-308X(10)72010-8
15. Eckert J, Gemmell MA, Meslin FX. WHO/OIE Manual on Echinococcosis in Humans and Animals: A Public Health Problem of Global Concern. Paris: World Organisation for Animal Health (2010). p. 100–42.
16. Khan A, Ahmed H, Simsek S, Gondal MA. Poverty-associated emerging infection of Cystic Echinococcosis in population of Northern Pakistan: a hospital-based study. Trop Biomed. (2019) 36:324–34.
17. Simon JL Resources population environment: an oversupply of false bad news. Science. (1980) 208:1431–7. doi: 10.1126/science.7384784
18. Raza SH. Role of draught animals in the economy of Pakistan, Center for Tropical Veterinary. Medicine. (2000) 30:17–21.
19. Mustafa I, Ahmed H, Saeed U, Sadiq F. Availability, cyst characteristics and hook morphology of Echinococcus granulosus isolates from livestock (Cattle, Sheep and Goats) in central Punjab, Pakistan. Kafkas Univ Vet Fak. (2015) 21:849–54. doi: 10.9775/kvfd.2015.13755
20. Battelli G. Echinococcosis: costs, losses and social consequences of neglected zoonoses. Vet Res Commun. (2009) 33:47–52. doi: 10.1007/s11259-009-9247-y
21. Cutler DM, Lleras-Muney A, Vogl T. Socioeconomic Status, and Health: Dimensions and Mechanisms (No. w14333). London: National Bureau of Economic Research (2008). doi: 10.1093/oxfordhb/9780199238828.013.0007
22. Ahmed H, Ali S, Afzal MS, Khan AA, Raza H, Shah ZH, et al. Why more research needs to be done on echinococcosis in Pakistan. Infect Dis Poverty. (2017) 6:90. doi: 10.1186/s40249-017-0309-z
23. Khan A, Naz K, Ahmed H, Simsek S. Knowledge, attitudes and practices related to cystic echinococcosis endemicity in Pakistan. Infect Dis Poverty. (2018) 7:4. doi: 10.1186/s40249-017-0383-2
24. Government of Pakistan (GOP). 2019-20. Pakistan Economic Survey. Ministry of Finance. Available online at: www.finance.gov.pk (assessed April 7, 2021).
25. Cutler DM, Lleras-Muney A. Education, and health: evaluating theories and evidence. In: House JS, Schoeni RF, Kaplan GA, Pollack H, editors. The Health Effects of Social and Economic Policy. New York, NY: Russell Sage Foundation (2007). doi: 10.3386/w12352
26. Grossman M. Education, non-market outcomes. In: Hanushek E, Welch F, editors. Handbook of the Economics of Education. Amsterdam: North-Holland, Elsevier Science, forthcoming (2008).
27. Oreopoulos P. Do dropouts drop out too soon? Wealth, health and happiness from compulsory schooling. J Public Econ. (2007) 91:2213–29. doi: 10.1016/j.jpubeco.2007.02.002
28. Ozcelik S, Kengec L. Cystic echinococcosis: a study of consciousness and creating awareness. Turkish J Parasitol. (2007) 31:313–7.
29. Wilkinson R. Income distribution, and mortality: a ‘natural' experiment, Sociol. Sociol Health Illn. (1990) 12:391–412. doi: 10.1111/1467-9566.ep11340405
30. McDonough P, Duncan GJ, Williams D, House J. Income dynamics and adult mortality in the United States, 1972 through 1989. Am. J Public Health. (1999) 87:1476–83. doi: 10.2105/AJPH.87.9.1476
31. Marmot MG, Rose G, Shipley M, Hamilton PJS. Employment grade and coronary heart disease in British civil servants. J Epidemiol Commun Health. (1978) 32:244–9. doi: 10.1136/jech.32.4.244
32. Marmot MG, Smith GD, Stansfeld S, Patel C. Health inequalities among British civil servants: the Whitehall II study. Lancet. (1991) 337:1387–93. doi: 10.1016/0140-6736(91)93068-K
33. Nyakarahuka L, Lalobo-Oryema M, Kankya C, Siefert L, Ocaido M, Ejobi F. Knowledge, attitudes and practices towards CE in Pastoral communities in Kasese district, Uganda. Adv Trop Med Public Health Int. (2012) 2:32–9. doi: 10.1007/s11250-017-1394-5
34. Macpherson CN, Craig PS. Observations on human echinococcosis (hydatidosis) and evaluation of transmission factors in the Maasai of northern Tanzania. Ann Trop Med Parasitol. (1989) 83:489–97. doi: 10.1080/00034983.1989.11812377
35. Wang YH, Rogan MT, Vuitton DA, Wen H. Cystic Echinococcossis in semi-nomadic pastoral communities in north-west China. Trans Royal Soc Trop Med Hygiene. (2001) 95:153–8. doi: 10.1016/S0035-9203(01)90142-7
36. Craig PS, Larrieu E. Control of cystic echinococcosis/hydatidosis: 1863-2002. Adv Parasitol. (2006) 61:443–508. doi: 10.1016/S0065-308X(05)61011-1
37. Rausch RL. Cystic echinococcosis in the Arctic and Sub-Arctic. Parasitology. (2003) 127:73–85. doi: 10.1017/S0031182003003664
38. Reperant LA. Applying the theory of island biogeography to emerging pathogens: toward predicting the sources of future emerging zoonotic and vector-borne diseases. Vector Borne Zoonotic Dis. (2010) 10:105–10. doi: 10.1089/vbz.2008.0208
39. Barbour AG, Fish D. The biological, and social phenomenon of Lyme disease. Science. (1993) 260:1610–6. doi: 10.1126/science.8503006
40. Epstein JH, Field HE, Luby S, Pulliam JRC, Daszak P. Nipah virus: Impact, origins, and causes of emergence. Curr Infect Dis Rep. (2006) 8:59–65. doi: 10.1007/s11908-006-0036-2
41. Ruedas LAJ, Salazar-Bravo DS. Tinnin, community ecology of small mammal populations in Panama following an outbreak of Hantavirus pulmonary syndrome. J Vector Ecol. (2004) 29:177–91.
42. Mills JN, Gage KL, Khan AS. Potential influence of climate change on vector borne and zoonotic diseases: a review and proposed research plan, Environ. Health Perspect. (2010) 118:1507–14. doi: 10.1289/ehp.0901389
43. Altizer S, Bartel R, Han BA. Animal migration, and infectious disease risk. Science. (2011) 331:296–302. doi: 10.1126/science.1194694
44. Kayouèche F, Chassagne M, Benmakhlouf A. Socio-ecological factors associated with risk of family hydatidosis in the wilaya of Constantine (Algeria) through interviews of urban and rural households. Rev Med Vet. (2009) 3:119–26.
45. Yang YR, Sun T, Li Z, Zhang J. Community surveys, and risk factor analysis of human alveolar and cystic echinococcosis in Ningxia Hui Autonomous Region, China. Bull World Health Organ. (2006) 84:714–21. doi: 10.2471/BLT.05.025718
46. Khayat R. Contribution au développement d'un modèle intégré de lutte contre l'hydatidose/échinococcose au Maroc. Rabat: Thèse Doct Vét IAV Hassan II (2006).
47. Tair A. Le chien dans la région d'Ouezzane: investigations sur sa vie, ses mœurs et son rôle dans la transmission de l'hydatidose et de la leishmaniose. Rabat: Thèse Doct Vét IAV Hassan II (2009).
48. Oudni M, M'rad S, Gorcii M, Mekki M. L'échinococcose hydatique de l'enfant en Tunisie: fertilité et localisation des kystes. Bull Soc Pathol Exot. (2006) 100:10–3.
49. Thys S, Sahibi H, Gabriël S, Rahali T. Community perception, and knowledge of cystic echinococcosis in the High Atlas Mountains, Morocco. BMC Public Health. (2019) 19:v118. doi: 10.1186/s12889-018-6372-y
Keywords: cystic echinococcosis, community perception, one health concept, risk factors, Pakistan
Citation: Khan A, Ahmed H, Amjad S, Afzal MS, Haider W, Simsek S, Khawaja MR, Khan DH, Naz S, Durrance-Bagale A, Shabbir RMK, Arfeen RZU, Ali S and Cao J (2021) Community Based Assessment of Behavior and Awareness of Risk Factors of Cystic Echinococcosis in Major Cities of Pakistan: A One Health Perspective. Front. Public Health 9:648900. doi: 10.3389/fpubh.2021.648900
Received: 02 January 2021; Accepted: 28 April 2021;
Published: 04 June 2021.
Edited by:
Jiufeng Sun, Guangdong Provincial Center for Disease Control and Prevention, ChinaReviewed by:
Hongbin Yan, Chinese Academy of Agricultural Sciences, ChinaCesar Gavidia, National University of San Marcos, Peru
Copyright © 2021 Khan, Ahmed, Amjad, Afzal, Haider, Simsek, Khawaja, Khan, Naz, Durrance-Bagale, Shabbir, Arfeen, Ali and Cao. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Haroon Ahmed, aGFyb29uYWhtYWQxMkB5YWhvby5jb20=; Jianping Cao, Y2FvanBAeWFob28uY29t