 Grace E. Patterson
Grace E. Patterson K. Marie McIntyre
K. Marie McIntyre Helen E. Clough
Helen E. Clough Jonathan Rushton
Jonathan Rushton
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
PERSPECTIVE article
Front. Public Health , 12 April 2021
Sec. Health Economics
Volume 9 - 2021 | https://doi.org/10.3389/fpubh.2021.630449
COVID-19 has disrupted everyday life worldwide and is the first disease event since the 1918 H1N1 Spanish influenza (flu) pandemic to demand an urgent global healthcare response. There has been much debate on whether the damage of COVID-19 is due predominantly to the pathogen itself or our response to it. We compare SARS-CoV-2 against three other major pandemics (1347 Black Death, 1520's new world smallpox outbreaks, and 1918 Spanish Flu pandemic) over the course of 700 years to unearth similarities and differences in pathogen, social and medical context, human response and behavior, and long-term social and economic impact that should be used to shape COVID-19 decision-making. We conclude that <100 years ago, pandemic disease events were still largely uncontrolled and unexplained. The extensive damage wreaked by historical pandemics on health, economy, and society was a function of pathogen characteristics and lack of public health resources. Though there remain many similarities in patterns of disease spread and response from 1300 onwards, the major risks posed by COVID-19 arise not from the pathogen, but from indirect effects of control measures on health and core societal activities. Our understanding of the epidemiology and effective treatment of this virus has rapidly improved and attention is shifting toward the identification of long-term control strategies that balance consideration of health in at risk populations, societal behavior, and economic impact. Policymakers should use lessons from previous pandemics to develop appropriate risk assessments and control plans for now-endemic COVID-19, and for future pandemics.
COVID-19 has disrupted everyday life worldwide. It is the first disease event since the 1918–20 H1N1 Spanish influenza (flu) pandemic to demand an urgent global healthcare response, propagated by the speed and likelihood of potential transmission. An understanding of how much disruption is caused by the pathogen, and how much is caused by our reaction to its potential presence, is essential. We compare SARS-CoV-2 against three other pathogens known for the magnitude of their impact. Yersinia pestis, causative agent of the 1347 Black Death, is among the most destructive pathogens in human history. Variola major, cause of the 1520s smallpox outbreaks in the New World, exemplifies how disease impacts vary by population. Spanish flu is most similar to the current pathogen, yet major differences exist regarding scientific advancements and pre-existing immunity.
We compare across these four major disease events the rates of infection, likelihood of dying, and available diagnostics, therapeutics and vaccines (Table 1). We examine the historical impact of these largely unchecked pathogens upon populations and economies. We discuss how culture and society's collective memory affect the response to pandemics and identify important lessons for decision-making as we adapt to a new normal.
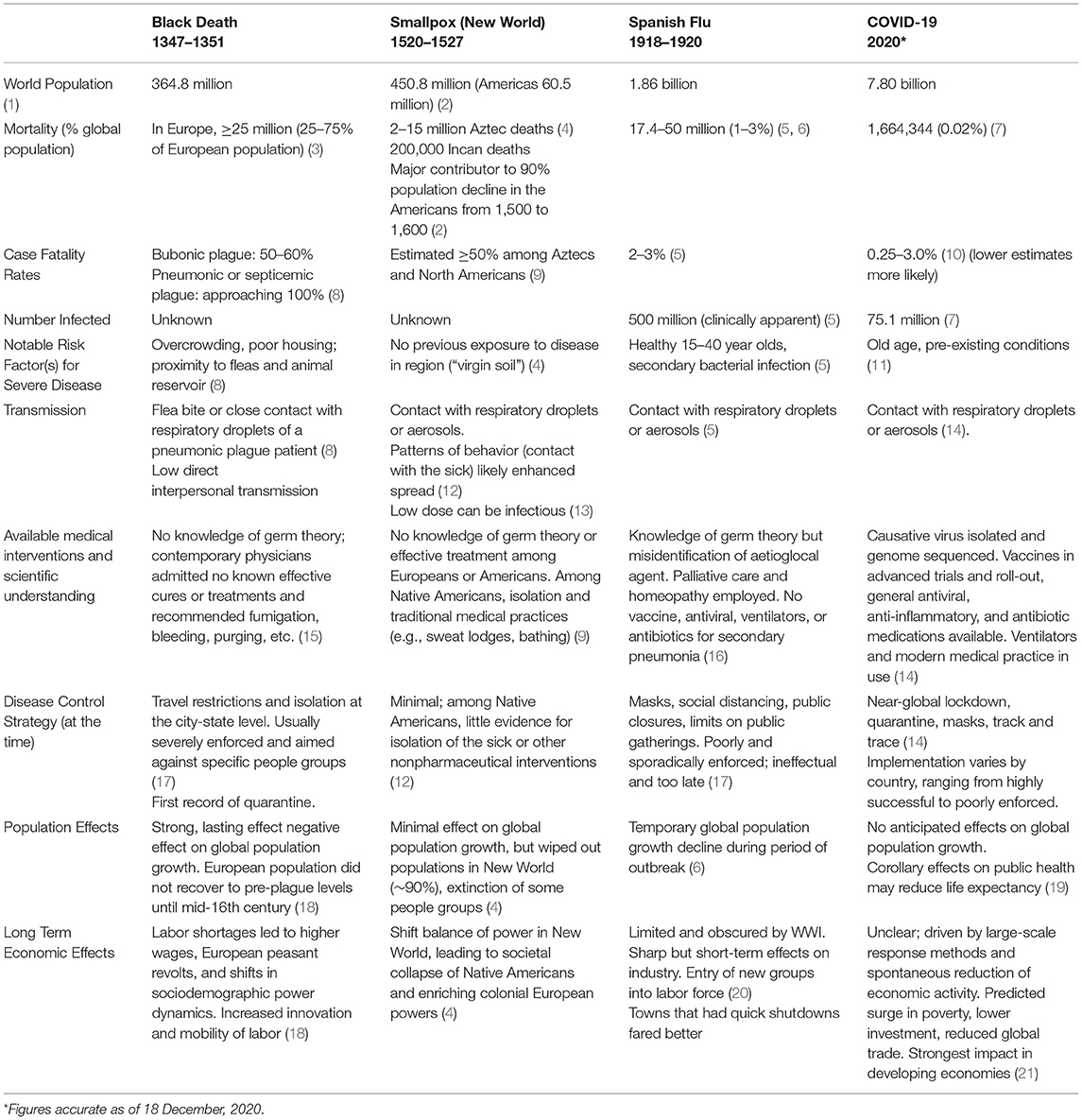
Table 1. Context and impacts of major pandemics.
SARS-CoV-2 differs from Y. pestis, V. major and Spanish flu in terms of disease transmission and pathophysiology. Of these four, it is the least deadly, and poses the lowest risk to otherwise healthy people; however increasing evidence suggests significant long-term sequelae for a proportion of individuals who have symptoms. The Black Death had exceedingly high case fatality rates (CFRs), approaching 100% for septicemic and pneumonic plague and 50–60% for the bubonic form of the disease (8). Over a third of the European population died during the 1347 outbreak, with some regions experiencing up to 75% mortality (22). CFRs for smallpox amongst immunologically naïve native Americans in the 1520s were estimated at 50% (9), and many survivors were left disfigured or blinded. Smallpox (and other European diseases) drove an estimated 90% decrease in indigenous populations in the Americas from 1500 to 1600 (2). Spanish flu had a CFR estimated at 2–3% (23) and few known long-term effects, other than occasional extended convalescence and limited instances of neuropsychiatric disorders (24). Current COVID-19 CFR estimations range from 0.3 to 3.0%, with lower estimates more likely to be accurate (10). There are growing reports of secondary and long-term impacts from COVID-19, typically among hospitalized patients but also among less severe cases. These include poor cardiovascular functioning (25), wide-ranging neurological symptoms (26), chronic fatigue (27), and others, with some patients needing long-term convalescence. While it is too early to fully understand the long-term impacts of COVID-19, similar post-viral syndromes have also been observed among those infected with SARS (28).
It is unknown how many people were infected during the Black Death and 1520s smallpox outbreaks. An estimated 500 million people (1 in 3 worldwide) were infected with Spanish flu and 1–3% of the global population died from the disease (5). Thus far, 75.1 million people have been confirmed to have COVID-19 (~1 in 104), killing 0.02% of the global population (7).
Disease susceptibility and immunological naivety influence the outcome of pandemic disease events. Both plague and smallpox are highly infectious and affect people of all ages, though smallpox exhibits a significantly higher mortality rate amongst children compared to adults (9). Spanish flu had severe impacts amongst the otherwise healthy 15–40 age group while also affecting typically high-risk groups (23). COVID-19 is different; it has a low attack rate (29) and severe clinical disease occurs mainly in the old and those with pre-existing health conditions (11).
Y. pestis has evolved over centuries to evade and modulate innate and adaptive immune responses (30). In 1347, naïve Europeans would have had minimal immunological protection from the plague. Conversely, pre-existing herd immunity from years of smallpox circulation spared European colonizers the widespread mortality observed among naïve populations when smallpox was introduced to the New Word (9). While Spanish flu was likely a result of a novel variant, there is evidence of cross-protection in elderly populations who were exposed to historical flu outbreaks; this was also observed among survivors of later flu epidemics (23). It is unknown if exposure to commonly circulating coronaviruses provides protection against COVID-19, but reactivity against SARS-CoV-2 has been observed in T-cells from unexposed people (31).
While much of the modern world would be unrecognizable to our ancestors, certain dynamics of disease spread remain the same. Humans and domesticated animals historically lived at close quarters, and the risk of animal to human disease transmission was intuitively minimized thousands of years before a causal relationship was established (32). Communicable diseases spread more easily where there is poverty and/or high population density (33, 34), as seen in Marseille where ~80% of the population perished in the Black Death (3). In India, Spanish flu mortality rates among members of the lowest social class were three times higher than that of other demographic groups (35). These risk factors remain relevant today: 73% of emerging infectious diseases in humans originate in animals (36), including COVID-19 (37). Large cities with international travel hubs, such as New York and London, were initially hit hard by COVID-19 and contributed to the unprecedented speed of global disease spread. Early understanding of the complex, multi-factorial role of socio-economic deprivation in COVID-19 spread, indicates that poverty remains a risk factor for poor outcome from infectious disease (38).
Science and public health advances have accelerated over the last 100 years; we should be better equipped to respond to the current pandemic. The Black Death, New World smallpox outbreaks, and Spanish flu all occurred before the discovery of antibiotics and antivirals and the development of centralized public health surveillance; even the aetiological agent of each outbreak was unidentified at the time. Early forms of quarantine and isolation were employed during the Black Death, and sanitary cordons were enforced by armed guards (17). Outbreak spread was ultimately unmitigated for both the Black Death and New World smallpox, and no effective treatment protocols were available (9, 39). The Native American custom of sleeping in close proximity to sick individuals would have spread smallpox even more efficiently (12). Mitigation tactics only slightly improved for Spanish flu, with sporadic use of non-pharmaceutical interventions such as track and trace, isolation, and social distancing (17). Late implementation, poor record-keeping, lack of a centralized global health body, and wartime priorities rendered these largely ineffectual. Public gathering spaces and schools were commonly shut down, but total lockdowns were not employed. Masks and disinfectants were used liberally, but ineffectively, and the only treatment was palliative care. Today, healthcare professionals can deploy antivirals, immune modulating drugs, antibiotics, oxygen, and ventilators to treat COVID-19 and related complications. At the time of writing (December 2020), the first doses of multiple vaccines for COVID-19 are being administered and surveillance systems have been established in many countries. Extensive lockdowns were enacted in most countries and travel restrictions, social distancing, and quarantine rules remain in place for the foreseeable future. Concern that healthcare capacity could be overwhelmed has stimulated rapid capacity building and shifting existing capacity away from day-to-day needs to help alleviate COVID-19. These modern tactics minimized harm from various infectious diseases but halted critical preventive activities, which may cause future chronic health burdens and global social and economic disruption surmounting that of COVID-19 alone (40). Countries such as Taiwan, which were able to locally eradicate the virus via swift but relatively short-lived enactment of nonpharmaceutical interventions, have suffered the least in terms of health, social and economic damage from COVID (41). Countries that have not been as successful in controlling spread of the virus (e.g., the United States - US) face long term health and economic damage from poorly coordinated and implemented control plans.
Historically, severity of disease has correlated with severity of economic outcomes. The Black Death caused a major labor shortage, providing unprecedented market power to common people and sparking a European peasant revolt (18). While trade and industry were temporarily damaged, the socio-economic structure of society was permanently redressed as wages increased. Skilled workers were increasingly mobile and spread innovative technology faster and further than before (18). Smallpox had less dramatic effects on the evolution of economic systems, but its unequal impacts on native groups paved the way for European conquest of the New World, through which mining of natural resources funded European empire-building (4). Smallpox often preceded the conquistadors, decimating populations and leading to starvation among survivors as their societal structure collapsed (9). Spanish flu closely followed World War I (WWI); both were particularly deadly for young to middle-aged men, which led to labor shortages and stalling of industry (20). These shortages were not as economically transformative as for the Black Death, perhaps as industry was less dependent upon mass labor, a smaller proportion of the overall workforce died, and more women and minors went into work outside the home (42). There is little evidence that Spanish flu caused major GDP or consumption declines or stock market volatility; major fluctuations had already occurred due to WWI (43, 44). These outbreaks contrast with COVID-19, which poses minimal physical risk to most of the labor force but major economic risk from the unprecedented lockdowns and non-pharmaceutical interventions employed to contain the virus. Early transient labor shortages were driven by shifts in demand and movement restrictions (45). Now, mitigation measures drive record unemployment. COVID-19 related stock market volatility is unprecedented (43) and national GDPs have plummeted (46). It remains to be seen what detrimental effects will persist in the global economy, though experts predict wage contraction and widespread poverty, with profound effects on emerging markets and developing economies (21).
The Black Death, smallpox, and Spanish flu no longer pose an imminent threat to the global population, but they changed global population structure and economies and prompted scientific advances in disease eradication, antibiotics, vaccines, and surveillance systems. It is too early to understand the long-term effects of SARS-CoV-2 or whether we will eradicate this pathogen, but we should seek inspiration from the past for how to move forward in control.
Bubonic plague, smallpox, and Spanish flu have been controlled by herd immunity and scientific advancements, though plague and flu still circulate. Localized hotspots of infection may be our COVID-19 future as this disease becomes endemic. Over the past 80 years, significant resources were spent developing surveillance systems, vaccines, and programs to monitor and manage flu (17). For COVID-19, it is unlikely we will develop curative treatments, and, as asymptomatic cases make up an estimated 17.9–30.8% of infections, disease eradication is unlikely (47). The best approach may be that birthed from the Spanish flu: develop vaccines, efficient monitoring systems, and an understanding the epidemiology of the virus, when endemic. The “end goal” would be high-level vaccine coverage coupled with notifiable disease status. This will potentially take a long time: until this is achieved, how can COVID-19 be managed with maximal public cooperation coupled with maximizing economic activity?
Public responses to pandemic disease are largely unchanged since the Black Death. Disbelief of disease presence, misinformation, unclear public communication, disregard for governmental proclamations, and poor personal risk assessment were and are still common. Despite the rapid onset of bubonic plague, it often took weeks for plague infection to be recognized in a population. In 1630s Italy, physicians were “insulted on the streets” for warning people about the arrival of the bubonic plague (48). Today, media touting COVID-19 conspiracy theories are amplified by prominent voices (49). Conflicting information about ongoing disease has long been spread (purposely or not) by news media, sometimes at the behest of governmental leadership. In an example of wartime censorship, the Italian government forced a Milan newspaper to stop printing daily death tolls during the Spanish flu because it was too demoralizing (17). In the US, public health officials hid the extent of disease spread and downplayed the danger it posed (20). In attempts to keep morale up, leaders inadvertently eroded trust in public institutions.
Uncertainty and desperation can drive people to use of dubious modes of protection during disease outbreaks. Physicians in the 1300s recommended bloodletting and drinking wine to ward off the plague (15). During the Spanish flu people wore camphor bags and gargled saltwater, while early in the COVID-19 pandemic, many sought protection from zinc lozenges and off-label medications (50). In a parallel to modern times, official Anti-Mask Leagues were formed in the US during the Spanish flu, citing insufficient scientific evidence for mask use and violation of constitutional rights. These examples demonstrate that public response to pandemics is driven by personal assessment of risks as shaped by individual circumstances and belief systems, not necessarily government mandates. In an attempt to save their economy during COVID-19, the Swedish government did not impose lockdown. However, Sweden still experienced economic losses similar to their neighbors, as people spontaneously reduced mobility and economic activity (51), being unconvinced by the herd immunity strategy (52), and presumably having made a decision based their individual assessment of risk.
COVID-19 poses a more targeted threat to health than previous pandemics however we have more understanding of its etiology and epidemiology than would have been possible in previous centuries. Why then has our global response been so profound? Our collective understanding of pandemics, as shaped by literature and culture, may play some role. The historical fascination with plagues is evidenced by some of the earliest surviving English literature and is observed across art and entertainment. Geoffrey Chaucer's 1386 “Canterbury Tales” describes the effects of total social upheaval that arose from the Black Death and provides insight into a world shaped by the threat of plague. Albert Camus's 1947 “The Plague” accurately captures the now familiar atmosphere of lockdown, obsession with case counts, and feelings of powerlessness. More recent movies such as Outbreak and Contagion may be a modern individual's reference point for predicting the possibilities of horrific disease outbreaks (and indeed, sales of these increased markedly at the pandemic's outset) (53). All explore the effects of pandemics on fear as well as fear on pandemics (54). A specific challenge for the modern era comes via the immediacy of social media, where genuine and “fake” information are frequently presented with apparently equal credibility. The myriad collective experiences and cognitive biases innate to humanity are further challenges that scientists, policymakers, figureheads and communicators should be aware of in themselves and their audiences when formulating and communicating response plans (55).
In the era of COVID-19, scientific and medical advances have enabled us to identify and treat disease in a way that would have been unimaginable to previous generations. Therefore, the biggest danger we face are reactions that are disproportionate to the nature of risks from COVID-19, leading to challenges in core social activities of food production, provision of education, healthcare, and basic health needs. Indeed, one legacy of COVID-19 may be the corollary deaths that stem from disease control strategies (40). Major economic downturns are correlated with chronic disease and mental disorder-associated mortalities; already in 2020 we have observed short-term excess deaths not attributed to COVID-19 and reduced healthcare uptake. To minimize long-term harm to global health targets, decision-makers must balance the direct health risks from the virus against those from the socioeconomic effects of control strategies. The underpinning evidence and reasoning must be unified across government, medicine, and media, and presented to a mistrustful public with transparency. As seen in the past, illogical decision-making and poor leadership have the potential to multiply harm caused by disease. We must minimize the impact of this pandemic by accurately assessing and proportionately responding to the true threats of COVID-19 and its legacy.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author/s.
The idea for this paper was initiated by JR and developed by GP, with input from KM and HC. GP wrote the first draft, with edits by JR, KM, and HC. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
1. World Population | An Interactive Experience - World Population. Available from: https://worldpopulationhistory.org/map/1/mercator/1/0/25/ (accessed August 11, 2020).
2. Koch A, Brierley C, Maslin MM, Lewis SL. Earth system impacts of the European arrival and great dying in the Americas after 1492. Quat Sci Rev. (2019) 207:13–36. doi: 10.1016/j.quascirev.2018.12.004
3. Scott S, Duncan CJ. The great pestilence. In: Biology of Plagues: Evidence From Historical Populations. Cambridge: Cambridge University Press (2001). p. 81–114. doi: 10.1017/CBO9780511542527.006
4. Taylor MW. Smallpox. In: Viruses and Man: A History of Interactions. Cham: Springer International Publishing (2014). p. 143–64. Available from: http://link.springer.com/10.1007/978-3-319-07758-1_9 (accessed August 18, 2020).
5. Taubenberger JK, Morens DM. 1918 Influenza: the Mother of All Pandemics. Emerg Infect Dis. (2006) 12:15–22. doi: 10.3201/eid1209.05-0979
6. The Spanish Flu (1918-20): The Global Impact of the Largest Influenza Pandemic in History - Our World in Data. Available from: https://ourworldindata.org/spanish-flu-largest-influenza-pandemic-in-history (accessed August 28, 2020).
7. COVID-19 Map - Johns Hopkins Coronavirus Resource Center. Available from: https://coronavirus.jhu.edu/map.html (accessed August 28, 2020).
8. Dennis DT, Staples JE. Plague. In: Bacterial Infections of Humans. Boston, MA: Springer US (2009). p. 597–611. Available from: https://link.springer.com/chapter/10.1007/978-0-387-09843-2_28 (accessed August 11, 2020).
9. Fenner F, Henderson DA, Arita I, Jezek Z, Ladnyi ID. The history of smallpox and its spread around the world. In: Fenner F, Henderson DA, Arita I, Jezek Z, Ladnyi ID, editors. Smallpox and Its Eradication. Geneva: World Health Organization (1988). p. 1460.
10. Wilson N, Kvalsvig A, Barnard LT, Baker MG. Case-fatality risk estimates for COVID-19 calculated by using a lag time for fatality. Emerg Infect Dis. (2020) 26:1339–41. doi: 10.3201/eid2606.200320
11. The OpenSAFELY Collaborative, Williamson E, Walker AJ, Bhaskaran KJ, Bacon S, Bates C. OpenSAFELY: factors associated with COVID-19-related hospital death in the linked electronic health records of 17 million adult NHS patients. medRxiv. (2020).
12. Riley JC. Smallpox and American Indians revisited. J Hist Med Allied Sci. (2010) 65:445–77. doi: 10.1093/jhmas/jrq005
13. Milton DK. What was the primary mode of smallpox transmission? Implications for biodefense. Front Cell Infect Microbiol. (2012) 2:150. doi: 10.3389/fcimb.2012.00150
14. Van Damme W, Dahake R, Delamou A, Ingelbeen B, Wouters E, Vanham G, et al. The COVID-19 pandemic: diverse contexts; different epidemics—how and why? BMJ Glob Heal. (2020) 5:e003098. doi: 10.1136/bmjgh-2020-003098
15. Aberth J. The Black Death: The Great Mortality of 1348-1350. New York, NY: Palgrave Macmillan US (2005). Available from: http://link.springer.com/10.1007/978-1-137-10349-9 (accessed August 26, 2020).
16. Short KR, Kedzierska K, van de Sandt CE. Back to the future: lessons learned from the 1918 influenza pandemic. Front Cell Infect Microbiol. (2018) 8:343. doi: 10.3389/fcimb.2018.00343
17. Tognotti E. Lessons from the history of quarantine, from plague to influenza A. Emerg Infect Dis. (2013) 19:254–9. doi: 10.3201/eid1902.120312
18. Pamuk S. The black death and the origins of the “great divergence” across Europe, 1300-1600. Eur Rev Econ Hist. (2007) 11:289–317. doi: 10.1017/S1361491607002031
19. Asquith BJ. What Can We Learn from the 1918 Pandemic? Careful Economics and Policy Lessons from Influenza. Policy Paper No. 2020-022. Kalamazoo, MI: W.E. Upjohn Institute for Employment Research (2020). doi: 10.17848/pol2020-022
20. How the Horrific 1918 Flu Spread Across America | History | Smithsonian Magazine. Available from: https://www.smithsonianmag.com/history/journal-plague-year-180965222/ (accessed August 21, 2020).
21. World Bank. Global Economic Prospects, June 2020. Washington, DC: World Bank (2020). doi: 10.1596/978-1-4648-1553-9
22. Alexander JT, Gottfried RS. The black death: natural and human disaster in Medieval Europe. Technol Cult. (1985) 26:831. doi: 10.2307/3105626
23. Morens DM, Fauci AS. The 1918 influenza pandemic: insights for the 21st century. J Infect Dis. (2007) 195:1018–28. doi: 10.1086/511989
24. Manjunatha N, Math S, Kulkarni G, Chaturvedi S. The neuropsychiatric aspects of influenza/swine flu: a selective review. Ind Psychiatry J. (2011) 20:83. doi: 10.4103/0972-6748.102479
25. Puntmann VO, Carerj ML, Wieters I, Fahim M, Arendt C, Hoffmann J, et al. Outcomes of cardiovascular magnetic resonance imaging in patients recently recovered from coronavirus disease 2019 (COVID-19). JAMA Cardiol. (2020) 5:1265–73. doi: 10.1001/jamacardio.2020.3557
26. Ellul MA, Benjamin L, Singh B, Lant S, Michael BD, Easton A, et al. Neurological associations of COVID-19. Lancet Neurol. (2020) 19:767–83. doi: 10.1016/S1474-4422(20)30221-0
27. Garrigues E, Janvier P, Kherabi Y, Le Bot A, Hamon A, Gouze H, et al. Post-discharge persistent symptoms and health-related quality of life after hospitalization for COVID-19. J Infect. (2020) 81:e4–e6. doi: 10.1016/j.jinf.2020.08.029
28. Moldofsky H, Patcai J. Chronic widespread musculoskeletal pain, fatigue, depression and disordered sleep in chronic post-SARS syndrome; a case-controlled study. BMC Neurol. (2011) 11:37. doi: 10.1186/1471-2377-11-37
29. Klompas M, Baker MA, Rhee C. Airborne transmission of SARS-CoV-2. JAMA. (2020) 324:441. doi: 10.1001/jama.2020.12458
30. Sebbane F, Lemaître N, Sturdevant DE, Rebeil R, Virtaneva K, Porcella SF, et al. Adaptive response of Yersinia pestis to extracellular effectors of innate immunity during bubonic plague. Proc Natl Acad Sci USA. (2006) 103:11766–71. doi: 10.1073/pnas.0601182103
31. Sette A, Crotty S. Pre-existing immunity to SARS-CoV-2: the knowns and unknowns. Nat Rev Immunol. (2020) 20:457–8. doi: 10.1038/s41577-020-0389-z
32. Weiss RA. The Leeuwenhoek Lecture 2001. Animal origins of human infectious disease at the London School of Hygiene and Tropical Medicine. Lecture. (2001) 356:957–77. doi: 10.1098/rstb.2001.0838
33. Connolly C, Keil R, Ali SH. Extended urbanisation and the spatialities of infectious disease: demographic change, infrastructure and governance. Urban Stud. (2020) 1–19. doi: 10.1177/0042098020910873
34. Semenza JC, Suk JE, Tsolova S. Social determinants of infectious diseases: a public health priority. Euro Surveill. (2010) 15:19608. Available from: http://www.eurosurveillance.org/ViewArticle.aspx?ArticleId=19608Article
35. Mills ID. The 1918-1919 influenza pandemic-the Indian experience. Indian Econ Soc Hist Rev. (1986) 23:1–40. doi: 10.1177/001946468602300102
36. Woolhouse MEJ, Gowtage-Sequeria S. Host range and emerging and reemerging pathogens. Emerg Infect Dis. (2005) 11:1842–7. doi: 10.3201/eid1112.050997
37. Zhang Y-Z, Holmes EC. A genomic perspective on the origin and emergence of SARS-CoV-2. Cell. (2020) 0:1–5. doi: 10.1016/j.cell.2020.03.035
38. Patel JA, Nielsen FBH, Badiani AA, Assi S, Unadkat VA, Patel B, et al. Poverty, inequality and COVID-19: the forgotten vulnerable. Public Health. (2020) 183:110–1. doi: 10.1016/j.puhe.2020.05.006
39. Smith PW, Watkins K, Hewlett A. Infection control through the ages. Am J Infect Control. (2012) 40:35–42. doi: 10.1016/j.ajic.2011.02.019
40. Brenner MH. Will there be an epidemic of corollary illnesses linked to a COVID-19-related recession? Am J Public Health. (2020) 110:974–5. doi: 10.2105/AJPH.2020.305724
41. Su SF, Han YY. How Taiwan, a non-WHO member, takes actions in response to COVID-19. J Glob Health. (2020) 10:010380. doi: 10.7189/jogh.10.010380
42. Karlsson M, Nilsson T, Pichler S. The impact of the 1918 Spanish flu epidemic on economic performance in Sweden. An investigation into the consequences of an extraordinary mortality shock. J Health Econ. (2014) 36:1–19. doi: 10.1016/j.jhealeco.2014.03.005
43. Baker SR, Bloom N, Davis SJ, Kost K, Sammon M, Viratyosin T. The Unprecedented Stock Market Reaction to COVID-19. Stanford. Report No.: 20112 (2020). Available from: http://www.policyuncertainty.com (accessed August 11, 2020).
44. Barro RJ, Ursua JF, Weng J. The coronavirus and the great influenza epidemic - lessons from the “Spanish Flu” for the Coronavirus's potential effects on mortality and economic activity (2020). In: CESifo Working Paper No. 8166. NBER Work Pap Ser. (2020). Available from: http://www.nber.org/papers/w26866%0ANATIONAL (accessed August 14, 2020).
45. Costa Dias M, Joyce R, Postel-Vinay F, Xu X. The challenges for labour market policy during the COVID-19 pandemic*. Fisc Stud. (2020) 41:371–82. doi: 10.1111/1475-5890.12233
46. The Global Economic Outlook During the COVID-19 Pandemic: A Changed World. Available from: https://www.worldbank.org/en/news/feature/2020/06/08/the-global-economic-outlook-during-the-covid-19-pandemic-a-changed-world (accessed August 18, 2020).
47. Moghadas SM, Fitzpatrick MC, Sah P, Pandey A, Shoukat A, Singer BH, et al. The implications of silent transmission for the control of COVID-19 outbreaks. Proc Natl Acad Sci USA. (2020) 117:17513–5. doi: 10.1073/pnas.2008373117
48. Ciulla MM. History repeating. The plague of 1630 in milan and the covid-19 pandemia. Acta Biomed. (2020) 91:234–5. doi: 10.23750/abm.v91i2.9553
49. Gruzd A, Mai P. Going viral: how a single tweet spawned a COVID-19 conspiracy theory on Twitter. Big Data Soc. (2020) 7:205395172093840. doi: 10.1177/2053951720938405
50. Adams KK, Baker WL, Sobieraj DM. Myth busters: dietary supplements and COVID-19. Annals Pharmacother. (2020) 54:820–6. doi: 10.1177/1060028020928052
51. Akkaya Y, Belfrage CJ, Corbo V, Di Casola P. GDP Growth in Sweden Relative to Other Countries in the wake of Covid-19. Sveriges Riksbank (2020). Available online at: https://www.riksbank.se/globalassets/media/rapporter/ekonomiska-kommentarer/engelska/2020/gdp-growth-in-sweden-relative-to-other-countries-in-the-wake-of-covid-19.pdf (accessed March 4, 2020).
52. Orlowski EJW, Goldsmith DJA. Four months into the COVID-19 pandemic, Sweden's prized herd immunity is nowhere in sight. J R Soc Med. (2020) 113:292–8. doi: 10.1177/0141076820945282
53. Haring B. Coronavirus Fears Spark Sales Surge For 'Contagion' Film, Dean Koontz Novel. Deadline [Internet]. Available online at: https://deadline.com/2020/03/coronavirus-fears-spark-sales-surge-contagion-film-dean-koontz-book-1202874644/ (accessed March 4, 2020).
54. Riva MA, Benedetti M, Cesana G. Pandemic Fear and Literature: Observations from Jack London's the Scarlet Plague. Emerg Infect Dis. (2014) 20:1753–7. doi: 10.3201/eid2010.130278
Keywords: plague, smallpox, Spanish flu, economic impact, pandemic control, COVID-19
Citation: Patterson GE, McIntyre KM, Clough HE and Rushton J (2021) Societal Impacts of Pandemics: Comparing COVID-19 With History to Focus Our Response. Front. Public Health 9:630449. doi: 10.3389/fpubh.2021.630449
Received: 17 November 2020; Accepted: 19 February 2021;
Published: 12 April 2021.
Edited by:
Hideki Hashimoto, The University of Tokyo, JapanReviewed by:
Tomoji Onozuka, The University of Tokyo, JapanCopyright © 2021 Patterson, McIntyre, Clough and Rushton. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jonathan Rushton, anJ1c2h0b25AbGl2ZXJwb29sLmFjLnVr
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.