
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health, 17 June 2021
Sec. Disaster and Emergency Medicine
Volume 9 - 2021 | https://doi.org/10.3389/fpubh.2021.601375
This article is part of the Research TopicImproving Disaster Health Outcomes and Resilience through Rapid Research: Implications for Public Health Policy and PracticeView all 17 articles
 Ashley Hyde1
Ashley Hyde1 Barbara S. E. Verstraeten2
Barbara S. E. Verstraeten2 Joanne K. Olson3
Joanne K. Olson3 Suzanne King4,5
Suzanne King4,5 Suzette Brémault-Phillips6
Suzette Brémault-Phillips6 David M. Olson7*
David M. Olson7*Introduction: Data show that maternal stress triggered by exposure to a natural disaster before, during or just after pregnancy is associated with adverse pregnancy and newborn outcomes. In this paper, the first aim is to describe our efforts to test a simple, low-cost intervention to large numbers of women following a major natural disaster. The second aim is to outline the challenges faced and lessons learned during the execution of this natural disaster study.
Methods: The setting was the May 2016 Fort McMurray Wood Buffalo wildfire in northern Alberta, Canada. Women who were pregnant or preconception at the time of the disaster were invited to participate via social media. This prospective cohort study included a randomized controlled trial to test the effectiveness of an expressive writing intervention on the levels of prenatal maternal stress and maternal, birth, and early childhood outcomes. At recruitment and at multiple timepoints postpartum, a battery of questionnaires was administered to evaluate objective and subjective stress exposure to the fire as well as maternal mental health, resilience and its contributing factors as well as infant developmental milestones. Qualitative content analysis of the expressive writing was conducted.
Discussion: There is an increasing need to develop effective, wide-spread, rapid, and low-cost interventions to reduce prenatal maternal stress, increase resilience, and improve pregnancy outcomes following a natural disaster. Though analysis of data is ongoing, we highlight the strengths of this study which include strong community participation, rapid recruitment of eligible participants, low-cost intervention and data acquisition, and successful testing of the intervention. We acknowledge the challenges we encountered including the high rate of participant disqualifications or losses due to incomplete collection of online data; evacuation, dispersal, and inconsistent return to homes; and the high levels of stress accumulated post-disaster which led to inability to complete the study. Despite potential challenges, there remains a need for such research amid natural disasters.
Climate change is causing more natural disasters. Their frequent worldwide occurrences wreak havoc upon families, particularly at-risk pregnant women. Hurricanes, floods, and wildfires have been linked with increased rates of preterm birth, low birth weight, and other adverse birth outcomes (1–3). Not only can natural disasters and their subsequent prenatal maternal stress (PNMS) have substantial impact on maternal and birth outcomes, they can also significantly impact child developmental outcomes.
On May 1st, 2016, a wildfire started in the northern Albertan region of Fort McMurray Wood Buffalo (FMWB). Within 3 days, the fire had massively multiplied in size and approached the town of Fort McMurray and nearby municipalities, forcing a mass evacuation of 88,000 people. This natural disaster became Canada's worst in every respect with an estimated cost of $9 billion (4). Twenty-four hundred buildings (10% of total), mostly family houses, were destroyed. Many structures left intact experienced significant smoke damage or ash contamination (5). During the height of the fire, the air pollution index rose to 38 on a 10-point scale (6–8). The town's water supply was contaminated and the large amount of residual ash and soil contained 19 different toxic metals and compounds reaching levels 20 times above recommended limits (5, 9). Residents were not allowed to return to the city until June 1, and then only limited numbers were permitted access. Over the next 2 weeks, about half of the evacuees returned, and it would take until September for the remainder with intact homes to return (10). It took much longer for those whose homes were destroyed to return, and some never did. Even before the wildfire, many FMWB families were experiencing economic difficulties due to layoffs or decreased working hours owing to lower oil prices and demand affecting community mental health (11). Psychologists and other experts predicted that after families returned to their homes, cases of domestic abuse and interpersonal violence would likely increase due to the stressors and uncertainties brought on by this natural disaster (12).
The Developmental Origins of Health and Disease (DOHaD) theory posits that multiple environmental factors operating on the mother before, during, and after pregnancy and while breastfeeding can influence the development of the child in ways that may favor survival in the short-term but may also compromise health in the longer-term (13). Increasing attention has been paid to the environment and experiences of the mother during pregnancy; consequently, PNMS has become an important subject of research. Animal (14–16) and human (17–19) research on PNMS suggest that exposure of the pregnant or preconception individual to stress is associated with a host of negative maternal health and pregnancy outcomes (e.g., preterm birth, gestational diabetes, preeclampsia, fetal growth restriction) as well as adverse developmental trajectories for the offspring - especially on the neurodevelopmental (20) and metabolic level, such as obesity (21), diabetes (22, 23), and cardiovascular issues (24). In addition, past maternal experiences with depression, exposure to adverse life events prior to pregnancy or environmental stressors in the woman's previous generations are thought to have similar adverse consequences as do immediate stressors (25–27).
Previous research studying pregnant women exposed to sudden-onset natural disasters such as the 1998 Quebec Ice Storm (28), the 2009 Iowa Floods (29), and the 2011 Queensland Floods (30) have attempted to disentangle the effects of maternal objective stress exposure, their cognitive appraisal, and their subjective distress due to the disasters on their own mental health and their children's development. These studies demonstrate significant effects of one or more of these aspects of the mothers' stress experience on maternal mood (29, 31), birth outcomes (32, 33), the cognitive (34, 35), behavioral (36–38), and motor (39, 40) development of their children, as well as immune (41, 42) and metabolic health (43, 44). Many of these outcomes have been shown to be mediated by epigenetic effects, still visible at age 13 (45, 46). The results of these disaster studies often suggest that the sex of the child, or the timing of the stressor in utero, moderates the impact of the stressor (32, 40).
Beyond prenatal exposure, stress either before conception or soon after birth may also have programming effects. Because an individual's hypothalamic-pituitary-adrenal (HPA) axis can be disrupted for months or even years after a severe disaster (47–49), maternal exposure to a disaster in the months before conception could conceivably influence the earliest moments of embryonic development (50, 51). As for postnatal effects, although the fetal programming hypothesis is based on the connection between the maternal HPA axis and fetal development via the placenta and umbilical cord, maternal stress may also be directly communicated to the young infant via breast milk and maternal behavior (52–54).
Whereas a natural disaster is most often limited in time, its resulting stress factors are not. Traumatic events add a considerable amount of stress to the stress load an individual has amassed over the course of its lifetime. Moreover, a short-term natural disaster is often followed by a host of stressors in its aftermath among which are physical and/or environmental, psychological, social, and financial factors. The wear and tear on the body due to the accumulation of life stressors is called allostatic load (AL) (55, 56). AL is the totality of the stressors acting on the body at any given time, both psychological and physical stressors, and how the body attempts to maintain homeostasis in the face of stress. When a threshold is reached at which the body can no longer cope with the AL, the risk increases to develop numerous disease processes associated with allostatic load including preterm birth, susceptibility to infection, and adverse newborn neurodevelopment (57, 58).
Resilience can be defined at the personal or individual level as well as from a socio-ecological perspective. At the individual level, resilience includes physiological, biological, individual, social, and environmental protective factors (59). It is thought of as a dynamic process, the capacity to bounce back, cope with, and recover from adverse events and trauma in order to maintain health and well-being (60). Psychological resilience is considered a major moderator of the relationship between the experience of trauma and the development of posttraumatic psychopathology (61, 62). Social-ecological resilience on the other hand is defined by Folke et al. (63) as the “capacity to adapt or transform in the face of change in socio-ecological systems, particularly unexpected change, in ways that continue to support human well-being (p. 41)” (63). Resilience can also be interpreted in relation to posttraumatic growth, focussing more on “bounce forward” than “bounce back” after experiencing traumatic events.
Cumulatively, the increased allostatic load due to a natural disaster and consequent uncertainty and disruption of lives, toxic chemical ingestion, and the pro-inflammatory stimulus of pollutants in air, water, and soil have the potential to accumulate to the point where individual resilience is overcome and people lose the ability to cope. In this situation they become vulnerable to adverse health outcomes and disease. Hence stress-related adverse outcomes in the case of pregnancy are the difference between an individual's (or a community's) allostatic load and resilience. Improving outcomes requires reducing allostatic load and/or increasing resilience.
Several studies indicate that interventions with highly anxious mothers, including reassurance of the fetus' health using additional ultrasound sessions (64, 65), group prenatal care (66), and prenatal education on preparing for childbirth and motherhood (67), may improve perinatal outcomes. However, although a systematic review found that web-based programs for perinatal mental health appear promising, significant gaps in the literature remain (68). The challenge to which we responded was to provide a simple, inexpensive, timely intervention to a large number of women who had experienced the FMWB disaster while pregnant or shortly preconception.
The first aim of this paper is to describe our efforts to develop a protocol to deliver and test a rapid intervention to a large number of women following a disaster. The second goal is to outline the challenges faced and lessons learned during the execution of this natural disaster study. It is important to share how challenges were dealt with because the protocol with modifications has been applied in other natural disaster research to date (Houston's Hurricane Harvey) and may be used in future studies.
As this study had a number of objectives, we conceptualized unique objectives and measures for each of the overall aims of this study.
We aimed to determine the extent to which a brief, online expressive writing intervention supports maternal resilience. The research questions guiding this project were: (1) Does expressive writing support resilience, reduce stress, and improve outcomes? (2) What thoughts, feelings, themes, experiences, actions, relationships, and factors do the women write about that reflect aspects of resilience? (3) In their post-writing reflections, how effective do the women find expressive writing to be?
Since the 1980's James W. Pennebaker has developed, tested, and refined a simple intervention to help people deal with stressors utilizing expressive writing (69, 70). Narratives or stories reveal both the individual and collective resilience strategies (71). Short bursts of expressive writing (i.e., 15–20 min) were shown to be sufficient to allow for emotional disclosure, the active ingredient in the intervention (70, 72–74), and to improve biochemical markers of physical and immune functioning as well as other physical health outcomes and healthcare utilization (75–83). Each subject in this study was randomly assigned to one of three treatment groups developed in consultation with J. Pennebaker: (1) the expressive writing group, writing about their innermost feelings (active group), (2) a writing group addressing non-emotional issues of healthy lifestyle (non-expressive writing group), and (3) women who did not receive any writing instructions (control or no-intervention group). Expressive writing accesses innermost thoughts and feelings and is a self-reflective learning activity that allows for review and cognitive processing of what has been written and thereby relieves anxiety and builds resilience (73, 74, 81, 84). The format makes participant involvement easy and convenient, even at a distance (85).
Our second goal was to determine the effect that maternal exposure to the FMWB wildfire had on birth outcomes, maternal psychopathology, and infant developmental outcomes. We also aimed to ascertain the effectiveness of the effective writing intervention and its impact on these same outcomes. We hypothesized that maternal objective stress exposure, cognitive appraisal, and subjective stress from the fires would have significant effects on birth outcomes, maternal psychopathology (at 12 months post-wildfire), and infant outcomes (at 18 months of age). In addition, we posited that the effects of PNMS would be moderated by the timing of maternal exposure to the wildfire (from 6 months preconception to 9 months gestation). Finally, we proposed that the PNMS effects from the wildfire would be significantly greater in the no-intervention group and the non-expressive writing group than in the active expressive writing group and that the strength of the buffering effect of the intervention would vary according to the perinatal timing of exposure to the wildfire as well as the intervention.
The study was designed as a prospective cohort study with a randomized controlled trial to test the effectiveness of an expressive writing intervention. The Fort McMurray Wood Buffalo region has around 1,250 births per year such that ~1,850 women were estimated to be pregnant or about to conceive at the time of the evacuation. Eligible participants included English-speaking women who were pregnant or within 6 months of conception when evacuated due to the 2016 Fort McMurray Wood Buffalo wildfire. Although it was a requirement that participants were residents of the FMWB region at the time of the wildfire, we recognized that some would not return to the community and indeed were not planning on returning at the time we commenced recruitment, which occurred between November 2016 and October 2018. Therefore, women who had temporarily or permanently moved away from the community of FMWB were still welcome to participate.
Study recruitment occurred primarily via social media platforms such as Facebook using targeted advertising. Additionally, we promoted the study and its potential benefits through television and radio features, which encouraged interested mothers to visit the study website1 and join the study. Women with multiple pregnancies or with fetuses diagnosed with congenital anomalies were not eligible to participate while women who did not complete the consent and recruitment questionnaires did not receive the intervention. In addition, mothers who experienced a perinatal death or stillbirth after recruitment were withdrawn from the study such that no further questionnaires were administered.
Of the 339 records in the database, 309 were individual participants of which 222 participants filled out sufficient recruitment questionnaires to be included in at least part of the analyses. The other records were removed because of ineligibility or not containing sufficient data. A total of 204 women completed the recruitment stage and were randomized for the expressive writing intervention. The numbers of participants in each of the intervention and control groups were as follows: 69 participants in the expressive writing group, 68 participants in the non-expressive writing group, and 67 in the control group. Of these, 110 ultimately completed the objective stress questionnaire 24 months after the fire (Figure 1).

Figure 1. Flow chart illustrating the sample size and attrition in the Fort McMurray Mommy Baby study. Completion of all recruitment questionnaires was not a requirement for inclusion in at least part of the data analyses but was necessary for randomization for the writing intervention into the expressive writing group, non-expressive writing group, and non-writing or control group. The number of participants who completed the McMurray Objective Maternal Stress Scale (MOMSS) approximately 24 months after the fire is indicated.
This research protocol was reviewed and received ethical approval from the Health Research Ethics Board Health Panel at the University of Alberta (PRO-000067510). Eligible women were given information outlining the study purpose, benefits and risks of participating, and methods for withdrawal, prior to consenting to participate. They were also provided telephone contact information for the study coordinator should they wish to ask further questions about the study.
All data are stored in an online secure REDCap (Research Electronic Data Capture) database, hosted by the Women and Children's Health Research Institute at the University of Alberta, Edmonton, AB, Canada (86). Except for the 18-month postpartum evaluation, study consent, questionnaires, and the intervention were delivered electronically, although participants were given the opportunity to complete the MOMSS questionnaire by phone or to receive a paper copy in the mail. Data from the face-to-face assessment was entered manually. Upon completing the consent form, women were asked to supply their name, email address, and date of birth. This information was used to automatically send personalized invitations to complete the surveys and as login information for the participants for the questionnaires. Personal identifying information was solely available within the REDCap database and only accessible by selected team members. For analyses, the REDCap data were converted into Microsoft Word, Microsoft Excel, and SPSS documents using anonymous participant identifiers and date shifting, which were stored on a separate secure research drive and/or password protected.
After completing the recruitment questionnaires, participants were randomized for the expressive writing intervention into one of three writing groups as discussed above. The two active writing groups (expressive and non-expressive) were asked to write each day for four consecutive days with the following instructions: “In narrative form, please write constantly without stopping for 15 minutes about the topic. Provide as much factual detail and description as possible.” After each writing session, participants were asked to indicate to what extent, on a scale from 1 to 4, they were experiencing stress-related symptoms and emotions. Invitations to complete the writing tasks were sent out via email, containing a link to the writing exercise. Participants were asked to complete one exercise per day within 24 h of receiving the email invitation. Supplementary Table 1 provides an overview of the questions and topics included in the intervention.
All women recruited into the Fort McMurray Mommy Baby study were administered the same questionnaires. Upon completion of the study consent, women were asked to fill in a demographics questionnaire providing socioeconomic data (parental education, job classification, and estimated income), relationship status, obstetric history, and delivery date of the index pregnancy. The study protocol also included psychometric questionnaires as discussed below. An overview of the timing of the questionnaires is available in Table 1.
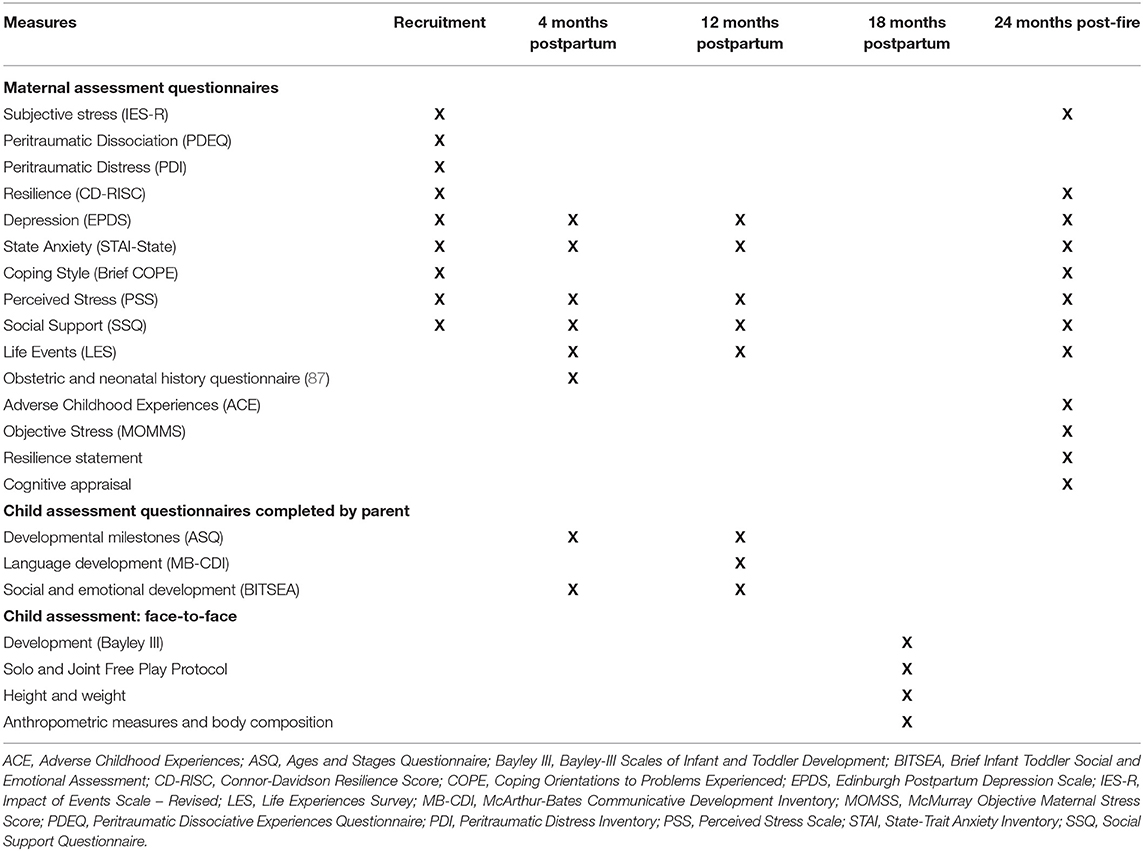
Table 1. Fort McMurray Mommy Baby Study data collection tools and timing.
The degree of objective hardship due to the fire was measured by a questionnaire tapping into four categories of trauma exposure: Threat (e.g., threat to life or physical integrity), Loss (e.g., of persons or property), Scope (e.g., length of evacuation and interruption of communication), and Change (e.g., amount of displacement, change in routine). The McMurray Objective Maternal Stress Score (MOMSS) is based on similar questionnaires developed for previous natural disaster studies examining the objective stress experienced by participants in the Quebec ice storm as well as Iowa and Queensland floods (28–30). As this was the first post-wildfire population the team approached, a new questionnaire was developed. Because each disaster is different, the MOMSS includes questions about threat, loss, scope, and change that were tailored specifically to the FMWB wildfire. Responses on each category are scored to a maximum of 50 points/category for Change and Scope but −4 to 50 for Loss (−2/−4 for increase in household income in 2016), for a total possible score of 200. For Threat, a possible 5 additional points were given for injuries to partner and/or children and for witnessing flames touching the mother's own home. A fifth category, Thwart, consists of elements impeding or slowing the mother's ability to leave the city as well as external barriers to get all family members to safety, but was not included in the overall score. The invitation to complete the questionnaire was sent out 24 months after the fire to all women who had completed recruitment questionnaires.
Subjective distress is at least in part determined by peritraumatic distress and dissociation. Peritraumatic distress, assessed with the 13-item Peritraumatic Distress Inventory (PDI), is the degree of distress experienced at the time of or immediately after the disaster as recalled at a later point in time (88). Peritraumatic dissociation on the other hand is measured using the 10-item Peritraumatic Dissociative Experiences Questionnaire (PDEQ) and estimates the severity of dissociative-like experiences such as amnesia, derealization, depersonalization, altered perception of time, and out-of-body experiences (89). Both questionnaires are scored on a 5-point Likert scale from “Not at all” to “Extremely true.” Together, these measures serve as a predictor of which participants may be at increased risk of developing posttraumatic stress disorder (PTSD).
The Impact of Event Scale-Revised (IES-R) is used to assess the severity of PTSD symptoms in relation to traumatic events, as experienced in the 7 days preceding completion of the questionnaire (90). This 22-item questionnaire, with scores ranging from “Not at all” (0) to “Extremely” (4), yields a total score as well as scores for three categories of PTSD symptoms: intrusive thoughts, avoidance, and hyperarousal. This particular scale was chosen for our study as it enables comparisons to previous disaster studies including Project Ice Storm, the Iowa Flood Study, and Queensland Flood Study (35, 91, 92).
Maternal anxiety was measured using the State-Trait Anxiety Inventory (STAI) (93), which asks participants how they generally feel, i.e., trait anxiety such as “I am content; I am a steady person,” or currently feel, assessing state anxiety with statements including “I feel tense; I feel frightened,” and is rated on a 4-point Likert scale from “Almost Never” to “Almost Always.” Internal consistency and test-retest reliability coefficients have been shown to range between 0.69 and 0.95 (93, 94).
The Edinburgh Postnatal Depression Scale (EPDS) was used to measure maternal depression (95, 96). The EPDS is a 10-item questionnaire that indicates whether a woman has depressive symptoms including guilt, sleep disturbance, low energy, and suicidal ideations. It has been validated for antenatal and postpartum mothers as well as in women who have delivered more than 1 year prior to administration (95, 97). In English-speaking mothers, a cut-off score of 13 or more is suggested for probable major depression in postpartum women whereas 15 or more may be used antenatally (98). The EPDS, rated on a 4-point Likert scale (0–3), has high test-retest reliability and good internal consistency (Cronbach's alpha > 0.8) (99).
The Coping Orientations to Problems Experienced (COPE) and the abbreviated version Brief COPE identify coping strategies participants use when experiencing stress (100). The latter is a 28-item questionnaire that measures the way participants have been coping with stress in their lives over the last month with answers ranging from “Not true at all” to “True nearly all of the time” (101). It assesses 14 means of coping such as self-distraction, denial, substance use, positive reframing, humor, religion, and acceptance, which can be categorized into emotion and problem-focused coping as well as dysfunctional coping (102).
The Life Experiences Survey (LES) used in this study is a 24-item score, derived from the original 57-item self-report questionnaire designed to inventory life changes participants experienced in the last year (103). Here, we asked about life events since conception of the child in the study, outside of the wildfire. It lists life changes in love and relationships such as marital status, health including pregnancy, pregnancy complications, and major illness of self as well as death and illness of loved ones, work-related and financial changes, and crime-related events. In addition to indicating whether the event occurred, participants are asked to rate the perceived impact of the event on a 7-point Likert scale ranging from “Extremely Negative (−3)” to “Extremely Positive (+3).”
The Connor-Davidson Resilience Scale-25 (CD-RISC) is a 25-item questionnaire that measures resilience by asking participants how they may have felt over the preceding month (60). The scale covers several aspects of resilience including self-efficacy, sense of humor, attachment to others, the ability to adapt to change, optimism, and faith rated on a 5-point Likert scale ranging from “Not true at all” to “True nearly all the time.” The total score is used in analyses with low scores indicating low levels of resilience.
At the 24 month post-fire timepoint, participants were also asked to respond to the following statement: “When things go wrong in my life it generally takes me a long time to get back to normal,” scored from “Don't agree at all (1)” to “Agree a lot (5).” Thus, for this statement, a lower score indicates higher levels of resilience. At the same time, cognitive appraisal of the fire was assessed by a single question, as follows: “Taking into account all of the effects of the Fort McMurray and Alberta wildfires on you and your family, what would you say have been the overall consequences of the event?” The consequences were also rated on a 5-point scale, from “Very negative,” over “Neutral, there were no consequences at all” to “Very positive.”
The Social Support Questionnaire (Short Form) (SSQ) is a 6-item survey that asks participants about both the social support they have available to them as well as their level of satisfaction with the support available (104). The SSQ is a two-part survey, with part 1 asking participants to name their social supports in specific circumstances, if any, and the relationship to them while the second part asks participants to indicate their satisfaction with these supports, ranging from “Very satisfied” (6) to “Very dissatisfied” (1).
The Perceived Stress Scale (PSS) was designed to evaluate the extent to which certain situations in the participant's life were considered stressful and thus how these situations affect individual feelings and the levels of perceived stress (105). It is a 14-item measure asking about thoughts and feelings in the past month, rated on a 5-point scale ranging from “Never” to “Very often.” Multiple items are stated in a positive way, e.g., “how often have you felt that you were on top of things” and are reverse coded such that higher scores indicate higher stress levels.
The Adverse Childhood Experiences (ACE) questionnaire, consisting of 10 questions, asks participants about personal experiences of abuse (psychological, physical, and sexual), as well as dysfunctionality within the household including mental illness, criminal behavior, violence against the participant's mother (106). The number of ACEs have been associated with increased risk of preterm birth (25) as well as risk behaviors and disease in adulthood (107, 108).
The Ages and Stages Questionnaire (ASQ) is a 30-item survey that asks mothers to assess five domains of infant development: communication, gross motor, fine motor, problem solving, and personal-social (109). It allows for the evaluation of developmental progress across these areas and is intended to catch delays in young children. Mothers are supplied with age-appropriate questionnaires and asked to answer questions using a 3-point Likert scale ranging from “Yes” to “Sometimes” to “Not yet.” At the end of the questionnaire, a list of overall questions is included assessing concerns regarding development noted by the parents. Examples are “Has your baby had any medical problems in the last several months?”, “Do you have concerns about your baby's behavior?” and “Does anything about your baby worry you?”. In the current study the ASQ-III 6 months and ASQ-III 12 months were used (110).
The MacArthur-Bates Communicative Development Inventories (MB-CDI) are instruments for assessing the communicative skills of infants (Words and Gestures) and toddlers (Words and Sentences) (111). We used the Infant form (Level 1), intended for 8- to 18-month-old children, limited to an 89-word vocabulary checklist for parents to indicate words that their child “understands” or “says.”
The Brief Infant- Toddler Social Emotional Assessment (BITSEA) is a 42-item questionnaire that asks mothers about social-emotional and behavioral competencies and problems in their infants (112). It assesses behavior as observed over the last month, scored on a 3-point Likert scale (“Not true/rarely; Somewhat true/sometimes; Very true/often”). In addition, parents are asked to respond to two questions with possible answers ranging from “Not at all” to “Very worried,” i.e., “How worried are you about your child's behavior, emotions, and relationships?” and “How worried are you about your child's language development?” The different areas evaluated are then combined into two separate scales. The Competencies scale covers 11 items reflecting social-emotional abilities (e.g., empathy, imitation/play skills) whereas the Problems scale reflects internalizing and externalizing problems, maladaptive and atypical behaviors as well as dysregulation. A third scale, the BITSEA Autism score, combines 19 problem and competence items associated with Autism Spectrum Disorders (113, 114).
At the children's age of ~18 months, parents were offered a face-to-face assessment with a trained experimenter. The child's body composition was evaluated, examining height, weight, head circumference as well as anthropometric measurements including mid-upper arm, waist, and calf circumferences, and triceps and subscapular skinfolds. In addition, maternal height, weight, and pregnancy status were recorded.
Cognitive, fine and gross motor abilities were assessed using the Bayley-III Scales of Infant and Toddler Development (115). Cognitive development is assessed through examination of thinking and problem solving, while motor development is assessed through examination of fine and gross motor skills.
During the face-to-face sessions, these were assessed and videotaped.
We conducted an analysis of study participants' expressive writing entries using qualitative methodology to elucidate both their resilience factors and the effectiveness of expressive writing on their resilience. Findings from this qualitative analysis were compared and contrasted with data from other study measures including the Connor-Davidson Resilience Scale (CD-RISC) (60) and with qualitative data from other disasters. Since the expressive writing intervention was administered electronically only using online journals, transcription for data analysis was not required. The Word documents containing the writing entries linked to a numeric participant identifier were uploaded into NVivo 12 (QSR International, Melbourne, Australia) to facilitate coding according to the six phases of thematic analysis (116). These are (1) familiarization; (2) coding; (3) theme generation; (4) review of themes; (5) theme definition and naming; and (6) writing up with data analysis using an inductive approach.
All quantitative data are/were analyzed using Microsoft Excel and IBM SPSS (IBM Corp, Armonk, NY, USA) after thorough data cleaning and checking. Imputation of missing values was performed using the expectation-maximization method (117). The timing of the fire in relation to the stage of pregnancy at exposure (preconception, first, second, and third trimester), was determined by calculating the number of days between the start of the fire (May 1, 2016) and the best estimated due date. Preconception exposure was defined as having a due date more than 280 days after the fire and evacuation. First trimester exposure corresponded to due dates falling 187–279 days following May 1, second trimester between 94 and 186 days, and third trimester 0–93 days. Statistical tests conducted and planned for these data include demographic statistics using parametric and non-parametric tests according to normality of distribution and homogeneity of variance; Pearson and Spearman correlations; structural equation modeling; multiple linear regression with interaction terms in moderation models; repeated measures regression models. Timing of the fire will be/was included as one of the covariates in the moderation analyses. Significant interactions are further investigated using the PROCESS macro v3.4 for SPSS (118). Probing the interaction reveals the magnitude and significance of simple or conditional effects of a predictor according to the level of the moderator. Furthermore, using the Johnson-Neyman procedure, it indicates the region of significance, the moderator transition points at which the conditional effects of the predictor achieve or lose significance. The coordinates provided by PROCESS can then be used to graph interaction figures.
Data collection was finalized by October 2018, with data analyses ongoing. During the study, preliminary results were shared with the FMWB community as well as policy makers on several occasions. Data resulting from this study have been presented at local, national, and international meetings. Two papers have been published (119, 120) while several others are under review or in preparation.
The Fort McMurray Mommy Baby study was designed to test the effectiveness of an expressive writing intervention on a vulnerable population, i.e., pregnant and preconception women exposed to a natural disaster, and its effects on maternal, birth, and child developmental outcomes. We employed a low-cost intervention that was widely deployed electronically or by traditional mail. It required a small commitment in terms of time, physical or mental involvement from participants over 4 days. This was enough input to allow for emotional disclosure, the active ingredient of the intervention. As time passes for the participants, the tool could be re-used by them to manage stress and build personal resilience. Since upwards of 1.5 billion people have been affected by natural disasters in the last decade alone (121), it is more than likely that the need for such tools will increase. This is imperative to assure the health of future generations.
In the development and execution of this protocol for a prospective randomized controlled trial in the aftermath of a natural disaster, we faced many challenges. While we were able to overcome some, others were insurmountable. Nevertheless, we feel it is important to share the lessons we learned so disaster research and the development of interventions for preconception and pregnant women and their children can move forward, even in these challenging research environments.
Throughout this study, we employed community-based participatory research principles (122) which acknowledged the unique knowledge needs of the FMWB community, the need for involvement throughout the research process, and importance of dissemination of study findings on an ongoing basis. In the months following the wildfire, prior to establishing formal study funding, we met with several leaders within the community to co-design the study protocol including participant recruitment and retention strategies. We also invited a participant, a local mother who was pregnant during the wildfire, to be a member of our research team. She provided valuable insight into the social structure of the community, suggestions on recruitment strategies, and feedback on the study measures. Furthermore, despite the extensive distance between the research institution and the community (450 km), the research team made several trips to refine recruitment strategies and monitor the progress of the study. We also organized “forums” for key stakeholders in the community (i.e., study participants, policy makers, and community leaders) to share preliminary findings, strengthen the relationship with the community, and inquire about any modifications that needed to be made to the protocol.
In addition to the strong relationships with the FMWB community that were built during the development of the protocol, other strengths of this study included the rapid recruitment of eligible participants, low-cost intervention and data acquisition, and successful testing of the intervention. We were able to recruit approximately one-sixth (n = 309) of all estimated eligible women (n = 1,850) who were pregnant or within 6 months preconception at the time of the wildfire. As there were a number of other studies occurring within the community during the same time frame and our participants experienced significant disruptions to their personal lives with many leaving the geographical area, we consider this sample size and recruitment successful given the circumstances. The use of REDCap limited the costs associated with the collection of the study data. As well, the expressive writing intervention was simple and low-cost largely because it was administered via REDCap. Given the university's extensive experience with REDCap, the establishment of the database for the Fort McMurray Mommy Baby Study facilitated the rapid rollout of a subsequent disaster study (Hurricane Harvey in Texas, USA). A final strength of this study involved the successful testing of an expressive writing intervention in the context of a natural disaster. To our knowledge, this had not been previously carried out.
What makes populations who have gone through natural disasters interesting, i.e., experiencing a sudden severe stressor in a quasi-random manner that impacts a large community, inherently also creates limitations. Protocols for a post-disaster study are unique and, in most cases, not immediately available. Developing the protocol, acquiring funding, and setting up the study takes time, which causes delays in data collection and introduces the risk of recall bias. Furthermore, due to the nature of disasters, such protocols cannot be executed in controlled environments. Even when carefully planned, actually carrying out the study is difficult, not in the least because of the time-sensitivity. In fact, the circumstances of the Fort McMurray Wood Buffalo wildfire and its aftermath required us to modify the protocol and be flexible and creative as the project unfolded in order to ensure sufficient quality data collection. Adequate funds only became available ~one year after the fire. As such, we were not able to hire a research coordinator and research assistant, take on an aggressive recruitment strategy or offer incentives until Spring 2017. This, at least in part, resulted in a major revision of the envisioned sample size. Another adjustment that was required was a revision of the timeline to perform the in-person developmental assessment. In accordance with our previous disaster studies, this evaluation was initially planned for when the infants were 16 months old (30). Because of the delay in funding as well as difficulties in finding a qualified research nurse, this evaluation had to be postponed for 2 months. Moreover, we were only able to assess 33 children.
The objective stress questionnaire was distributed to the participants later than scheduled as well. As this was our first post-fire study, a new survey needed to be designed. The development of the questionnaire requires an in-depth understanding of the complex geographic, social, and economic environment, with a need for extensive examination and preparation. This was hindered by the fact that none of the members of the research team lived in the community as well as the distance.
The obvious need for quick development of a protocol and application for funding may also hinder the quality of the study in the long term. In the time frame available to design the study and apply for funding, it may not be possible to set up an optimal multidisciplinary research team or contact experts. This may lead to important questions not being asked. Another consideration is how participants interact with the online secure database because there is not enough time for beta testing. For example, some individuals participated more than once, and the database should have prevented this. A number of data entry mistakes required extensive data cleaning. This is an inherent problem when participants enter data on mobile devices. Also, email invitations are easy to overlook or forget as there is no physical reminder of the questionnaire. Participants received up to five reminder emails with the link to the appropriate questionnaire.
Careful thought also needs to be given to the time required to complete the questionnaires. The initial batch of surveys in this study took over 1 h to complete. Moreover, often when there is no immediate tangible benefit to participants, they will not continue completing the questionnaires. In an effort to minimize this problem and in recognition of the significant time commitment required to complete the surveys, we decided while the study was ongoing to compensate participants for their time with $50 gift cards for online purchases. To further encourage completion of the questionnaires, the order of the surveys was changed, partly in recognition of the fact that several of the questions may have been perceived as difficult or sensitive and could have caused participants to drop out. Aside from the number and length of the questionnaires, another element to keep in mind is to not overly study the community undergoing significant stress as this can lead to research fatigue. At the time of the current study, multiple others were being conducted, several funded through the same government agency, each with their own demands. When individuals participate in different studies at the same time, it may be possible that these demands increase stress and that potential positive effects of participation may be canceled out.
In addition, disentangling the effects of exposure to a disaster from the alterations in mental health that are inherently associated with the reproductive period without overwhelming participants with numerous questionnaires is very difficult. Although pregnancy and childbirth are physiological processes and not illnesses, they can be associated with negative psychological experiences related to unexpected pregnancy, loss of a pregnancy, challenging obstetric history, and maternal and fetal complications. Moreover, one needs to consider other traumatic events in a woman's life, ranging from adverse childhood experiences to other life events and difficult environmental circumstances, i.e., racism, violence, unemployment, substance abuse, and socioeconomic struggles, prior to, during, and after pregnancy and childbirth (25, 123–125). The latter is especially the case in disaster research since recruitment is often only possible after a considerable time lag, during which much in addition to the disaster could have occurred in a woman's life. The Adverse Childhood Experiences questionnaire and Life Experiences Survey were included in the protocol but were only completed by a limited number of participants, preventing us from correcting for these events in analyzing the data.
A limitation of disaster-related studies is that the stress is not limited to the event itself; it continues to accumulate due to the consequences of the event and may therefore affect who participates in the study. This leads to two problems inherent in such studies: that some participants may not be able to have the time or the focus to participate in the study due to being overwhelmed by stress, and that it may be the least affected by stress who are disproportionately represented in the study. Ongoing stress may derive from temporary housing or relocation issues, fear for the safety, health, and well-being of loved ones, economic and/or food insecurities, and in the case of the FMWB disaster, longer-term disputes with insurance agencies.
Our recommendations for future studies that test interventions to improve pregnancy outcomes in the midst of disasters are: (1) recruit in larger communities where many more participants live so that the power of the study is maintained in spite of the participant attrition due to all the reasons described here. (2) Recruit the most stressed participants into your study in order to create a robust effect size so that your intervention has the largest effect possible. For instance, during the current coronavirus pandemic there are many pregnant women, some of whom are highly stressed. Focus your recruitment on those you consider to be the most stressed. (3) Prepare in advance for a disaster intervention study. It is possible for investigative teams to obtain ethical approval (or at least in a draft form), develop their protocols, interventions, and database tools in advance of a natural disaster. Then, when a significant disaster strikes a community, the team can quickly implement their study. The costs for this preparedness are surprisingly low; it is the analysis phase of the study that is more expensive due to research staff costs. However, once the data are gathered, it is easier to obtain funding for these analyses.
The first purpose of this paper was to describe the development of a protocol to test an intervention offered to pregnant and preconception women following a disaster. The Fort McMurray Mommy Baby Study was the first study attempting to reduce stress in preconception and pregnant women after a catastrophic natural disaster. Previous studies largely documented the degree of stress women experiencing a natural disaster had and the effects of that stress on their pregnancy outcomes and the developmental trajectories of their children. Similar studies evaluate the impact of these events at both the community and the individual level, but none have attempted to reduce stress, increase resilience, and thereby improve outcomes. These are the problems the research in this field needs to address.
The second purpose was to outline the challenges encountered in the context of this research. As a first study in this regard, we experienced several challenges. These included the a priori study design not conforming to the realities of a post-disaster environment in a remote community. There were challenges with participant recruitment and retention that led to consequent loss of data, reduced sample size, and gaps in the data. There might also have been selection and recall biases. Last, even though we started organizing the study as soon as the disaster occurred, it took 6 months to obtain ethical approval, funding, and to initiate the study. This time lag may have led to some of the problems encountered. Fortunately, this is an iterative process whereby improvements will occur with repeated attempts to respond to future natural disasters with studies that test interventions to improve outcomes.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
This study involving human participants was reviewed and approved by Health Research Ethics Board Health Panel, University of Alberta. The participants provided their written informed consent to participate in this study.
Each author contributed to the design of the study. AH drafted the manuscript, which was revised and completed by AH, BV, JO, and DO. All authors contributed to the article and approved the submitted version.
This study was funded by a grant from the Canadian Institutes of Health Research No. 151029 (DO). It also received support from the Women and Children's Health Research Institute No. 2475 (DO), the Faculty of Medicine and Dentistry, University of Alberta, through the WCHRI CIHR Bridge Program, FoMD Portion (DO), and the O'Brien Institute for Public Health. This study was also funded by the Worldwide Universities Network as part of the Optimal Pregnancy Environment Risk Assessment (OPERA) program.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The authors would sincerely like to thank Melissa Meeres for providing local logistical support and performing the in-person assessments. We also extend our gratitude to all FMWB mothers who participated in this study.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2021.601375/full#supplementary-material
1. Xiong X, Harville EW, Mattison DR, Elkind-Hirsch K, Pridjian G, Buekens P. Exposure to Hurricane Katrina, post-traumatic stress disorder and birth outcomes. Am J Med Sci. (2008) 336:111–5. doi: 10.1097/MAJ.0b013e318180f21c
2. Oyarzo C, Bertoglia P, Avendano R, Bacigalupo F, Escudero A, Acurio J, et al. Adverse perinatal outcomes after the February 27th 2010 Chilean earthquake. J Matern Fetal Neonatal Med. (2012) 25:1868–73. doi: 10.3109/14767058.2012.678437
3. Torche F. The effect of maternal stress on birth outcomes: exploiting a natural experiment. Demography. (2011) 48:1473–91. doi: 10.1007/s13524-011-0054-z
4. Alam R, Islam S, Mosely E, Thomas S, Dodell V, Doel D. Rapid Impact Assessment of the Fort McMurray wildfire. Edmonton, AB: MacEwan University and the Institute for Catastropic Loss Reduction (2017). Available online at: https://www.iclr.org/wp-content/uploads/2019/08/Rapid-Impact-Assessment-of-Fort-McMurray-Wildfire.pdf (accessed August 18, 2020)
5. Slaughter G. Fort McMurray Wildfire: Arsenic Found in Ash, Delaying Re-entry for 2,000 Residents. CTVNews.ca (2016). Available online at: https://www.ctvnews.ca/canada/fort-mcmurray-wildfire-arsenic-found-in-ash-delaying-re-entry-for-2-000-residents-1.2922761 (accessed August 18, 2020).
6. Vice News. On a Scale of 1 to 10, the Air Pollution in Fort McMurray is 38. (2016). Available online at: https://news.vice.com/article/on-a-scale-of-one-to-ten-the-air-pollution-in-fort-mcmurray-is-38 (accessed August 19, 2020).
7. Landis MS, Edgerton ES, White EM, Wentworth GR, Sullivan AP, Dillner AM. The impact of the 2016 Fort McMurray horse river wildfire on ambient air pollution levels in the Athabasca Oil Sands Region, Alberta, Canada. Sci Total Environ. (2018) 618:1665–76. doi: 10.1016/j.scitotenv.2017.10.008
8. Wentworth GR, Aklilu Y-A, Landis MS, Hsu Y-M. Impacts of a large boreal wildfire on ground level atmospheric concentrations of PAHs, VOCs and ozone. Atmos Environ. (2018) 178:19–30. doi: 10.1016/j.atmosenv.2018.01.013
9. Giovannetti J. Tests Reveal Toxic Levels of Contaminants in Fort Mac Soil and Ash. The Globe and Mail, Toronto, ON: Phillip Crawley (2016). Available online at: http://www.theglobeandmail.com/news/alberta/tests-reveal-toxic-levels-of-contaminants-in-fort-mac-soil-and-ash/article30346538 (accessed Augest 19, 2020).
10. Alberta Government. Home Again: Recovery After the Wood Buffalo Wildfire. (2016). Available online at: https://open.alberta.ca/dataset/9781460131350/resource/147e872d-10a1-491f-826a-10e803c40bfe (accessed August 19, 2020).
11. Ritchie A, Hrabok M, Igwe O, Omeje J, Ogunsina O, Ambrosano L, et al. Impact of oil recession on community mental health service utilization in an oil sands mining region in Canada. Int J Soc Psychiatry. (2018) 64:563–9. doi: 10.1177/0020764018785401
12. CBC News. Domestic Abuse Concerns in Aftermath of Fort McMurray Fire. (2016). Available from: http://www.cbc.ca/news/canada/edmonton/domestic-abuse-concerns-in-aftermath-of-fort-mcmurray-fire-1.3629228 (accessed August 19, 2020).
13. Gluckman PD, Hanson MA, Buklijas T. A conceptual framework for the developmental origins of health and disease. J Dev Orig Health Dis. (2010) 1:6–18. doi: 10.1017/S2040174409990171
14. Charil A, Laplante DP, Vaillancourt C, King S. Prenatal stress and brain development. Brain Res Rev. (2010) 65:56–79. doi: 10.1016/j.brainresrev.2010.06.002
15. Weinstock M. Alterations induced by gestational stress in brain morphology and behaviour of the offspring. Prog Neurobiol. (2001) 65:427–51. doi: 10.1016/S0301-0082(01)00018-1
16. Weinstock M. Prenatal stressors in rodents: effects on behavior. Neurobiology of Stress. (2017) 6:3–13. doi: 10.1016/j.ynstr.2016.08.004
17. Glover V. Annual research review: prenatal stress and the origins of psychopathology: an evolutionary perspective. J Child Psychol Psychiatry. (2011) 52:356–67. doi: 10.1111/j.1469-7610.2011.02371.x
18. Talge NM Neal C Glover V Early Stress Translational Research and Prevention Science Network: Fetal and Neonatal Experience on Child and Adolescent Mental Health. Antenatal maternal stress and long-term effects on child neurodevelopment: how and why? J Child Psychol Psychiatry. (2007) 48:245–61. doi: 10.1111/j.1469-7610.2006.01714.x
19. Graignic-Philippe R, Dayan J, Chokron S, Jacquet AY, Tordjman S. Effects of prenatal stress on fetal and child development: a critical literature review. Neurosci Biobehav Rev. (2014) 43:137–62. doi: 10.1016/j.neubiorev.2014.03.022
20. van den Bergh BRH, Dahnke R, Mennes M. Prenatal stress and the developing brain: risks for neurodevelopmental disorders. Dev Psychopathol. (2018) 30:743–62. doi: 10.1017/S0954579418000342
21. Lamichhane N, Olsen NJ, Mortensen EL, Obel C, Heitmann BL, Händel MN. Associations between maternal stress during pregnancy and offspring obesity risk later in life—A systematic literature review. Obes Rev. (2020) 21:e12951. doi: 10.1111/obr.12951
22. Paxman EJ, Boora NS, Kiss D, Laplante DP, King S, Montina T, et al. Prenatal maternal stress from a natural disaster alters urinary metabolomic profiles in project ice storm participants. Sci Rep. (2018) 8:12932. doi: 10.1038/s41598-018-31230-x
23. Kajantie E, Strang-Karlsson S, Hovi P, Wehkalampi K, Lahti J, Kaseva N, et al. Insulin sensitivity and secretory response in adults born preterm: the Helsinki Study of Very Low Birth Weight Adults. J Clin Endocrinol Metab. (2015) 100:244–50. doi: 10.1210/jc.2014-3184
24. Plana-Ripoll O, Li J, Kesmodel US, Olsen J, Parner E, Basso O. Maternal stress before and during pregnancy and subsequent infertility in daughters: a nationwide population-based cohort study. Hum Reprod. (2016) 31:454–62. doi: 10.1093/humrep/dev309
25. Christiaens I, Hegadoren K, Olson DM. Adverse childhood experiences are associated with spontaneous preterm birth: a case-control study. BMC Med. (2015) 13:124. doi: 10.1186/s12916-015-0353-0
26. Painter RC, Osmond C, Gluckman P, Hanson M, Phillips DI, Roseboom TJ. Transgenerational effects of prenatal exposure to the Dutch famine on neonatal adiposity and health in later life. BJOG. (2008) 115:1243–9. doi: 10.1111/j.1471-0528.2008.01822.x
27. Nesari M, Olson JK, Vandermeer B, Slater L, Olson DM. Does a maternal history of abuse before pregnancy affect pregnancy outcomes? A systematic review with meta-analysis. BMC Pregnancy Childb. (2018) 18:404. doi: 10.1186/s12884-018-2030-8
28. King S, Laplante DP. The effects of prenatal maternal stress on children's cognitive development: Project Ice Storm. Stress. (2005) 8:35–45. doi: 10.1080/10253890500108391
29. Brock RL, O'Hara MW, Hart KJ, McCabe JE, Williamson JA, Laplante DP, et al. Partner support and maternal depression in the context of the Iowa floods. J Fam Psychol. (2014) 28:832–43. doi: 10.1037/fam0000027
30. King S, Kildea S, Austin MP, Brunet A, Cobham VE, Dawson PA, et al. QF2011: a protocol to study the effects of the Queensland flood on pregnant women, their pregnancies, and their children's early development. BMC Pregn Childbirth. (2015) 15:109. doi: 10.1186/s12884-015-0539-7
31. Brock RL, O'Hara MW, Hart KJ, McCabe-Beane JE, Williamson JA, Brunet A, et al. Peritraumatic distress mediates the effect of severity of disaster exposure on perinatal depression: The Iowa Flood Study. J Trauma Stress. (2015) 28:515–22. doi: 10.1002/jts.22056
32. Dancause KN, Laplante DP, Oremus C, Fraser S, Brunet A, King S. Disaster-related prenatal maternal stress influences birth outcomes: Project Ice Storm. Early Hum Dev. (2011) 87:813–20. doi: 10.1016/j.earlhumdev.2011.06.007
33. Dancause KN, Mutran D, Elgbeili G, Laplante DP, Kildea S, Stapleton H, et al. Dietary change mediates relationships between stress during pregnancy and infant head circumference measures: the QF2011 study. Matern Child Nutr. (2017) 13:1–14. doi: 10.1111/mcn.12359
34. Laplante DP, Brunet A, Schmitz N, Ciampi A, King S. Project Ice Storm: prenatal maternal stress affects cognitive and linguistic functioning in 5 1/2-year-old children. J Am Acad Child Adolesc Psychiatry. (2008) 47:1063–72. doi: 10.1097/CHI.0b013e31817eec80
35. Laplante DP, Hart KJ, O'Hara MW, Brunet A, King S. Prenatal maternal stress is associated with toddler cognitive functioning: The Iowa Flood Study. Early Hum Dev. (2018) 116:84–92. doi: 10.1016/j.earlhumdev.2017.11.012
36. Laplante DP, Zelazo PR, Brunet A, King S. Functional play at 2 years of age: effects of prenatal maternal stress. Infancy. (2007) 12:69–93. doi: 10.1111/j.1532-7078.2007.tb00234.x
37. Simcock G, Laplante DP, Elgbeili G, Kildea S, Cobham V, Stapleton H, et al. Infant neurodevelopment is affected by prenatal maternal stress: the QF2011 Queensland Flood Study. Infancy. (2017) 22:282–302. doi: 10.1111/infa.12166
38. St-Hilaire A, Steiger H, Liu A, Laplante DP, Thaler L, Magill T, et al. A prospective study of effects of prenatal maternal stress on later eating-disorder manifestations in affected offspring: preliminary indications based on the Project Ice Storm cohort. Int J Eat Disord. (2015) 48:512–6. doi: 10.1002/eat.22391
39. Simcock G, Kildea S, Elgbeili G, Laplante DP, Stapleton H, Cobham V, et al. Age-related changes in the effects of stress in pregnancy on infant motor development by maternal report: The Queensland Flood Study. Dev Psychobiol. (2016) 58:640–59. doi: 10.1002/dev.21407
40. Cao X, Laplante DP, Brunet A, Ciampi A, King S. Prenatal maternal stress affects motor function in 5(1/2)-year-old children: Project Ice Storm. Dev Psychobiol. (2014) 56:117–25. doi: 10.1002/dev.21085
41. Veru F, Dancause K, Laplante DP, King S, Luheshi G. Prenatal maternal stress predicts reductions in CD4+ lymphocytes, increases in innate-derived cytokines, and a Th2 shift in adolescents: Project Ice Storm. Physiol Behav. (2015) 144:137–45. doi: 10.1016/j.physbeh.2015.03.016
42. Turcotte-Tremblay AM, Lim R, Laplante DP, Kobzik L, Brunet A, King S. Prenatal maternal stress predicts childhood asthma in girls: Project Ice Storm. Biomed Res Int. (2014) 2014:201717. doi: 10.1155/2014/201717
43. Dancause KN, Laplante DP, Hart KJ, O'Hara MW, Elgbeili G, Brunet A, et al. Prenatal stress due to a natural disaster predicts adiposity in childhood: The Iowa Flood Study. J Obes. (2015) 2015:570541. doi: 10.1155/2015/570541
44. Dancause KN, Veru F, Andersen RE, Laplante DP, King S. Prenatal stress due to a natural disaster predicts insulin secretion in adolescence. Early Hum Dev. (2013) 89:773–6. doi: 10.1016/j.earlhumdev.2013.06.006
45. Cao-Lei L, Dancause KN, Elgbeili G, Massart R, Szyf M, Liu A, et al. DNA methylation mediates the impact of exposure to prenatal maternal stress on BMI and central adiposity in children at age 13(1/2) years: Project Ice Storm. Epigenetics. (2015) 10:749–61. doi: 10.1080/15592294.2015.1063771
46. Cao-Lei L, Veru F, Elgbeili G, Szyf M, Laplante DP, King S. DNA methylation mediates the effect of exposure to prenatal maternal stress on cytokine production in children at age 131/2 years: Project Ice Storm. Clin Epigenet. (2016) 8:54. doi: 10.1186/s13148-016-0219-0
47. Bowler RM, Mergler D, Huel G, Cone JE. Psychological, psychosocial, and psychophysiological sequelae in a community affected by a railroad chemical disaster. J Trauma Stress. (1994) 7:601–24. doi: 10.1002/jts.2490070408
48. Dallman MF, Akana SF, Scribner KA, Bradbury MJ, Walker CD, Strack AM, et al. Stress, feedback and facilitation in the hypothalamo-pituitary-adrenal axis. J Neuroendocrinol. (1992) 4:517–26. doi: 10.1111/j.1365-2826.1992.tb00200.x
49. Goenjian AK, Yehuda R, Pynoos RS, Steinberg AM, Tashjian M, Yang RK, et al. Basal cortisol, dexamethasone suppression of cortisol, and MHPG in adolescents after the 1988 earthquake in Armenia. Am J Psychiatry. (1996) 153:929–34. doi: 10.1176/ajp.153.7.929
50. Hohwu L, Li J, Olsen J, Sorensen TI, Obel C. Severe maternal stress exposure due to bereavement before, during and after pregnancy and risk of overweight and obesity in young adult men: a Danish National Cohort Study. PLoS ONE. (2014) 9:e97490. doi: 10.1371/journal.pone.0097490
51. Virk J, Li J, Vestergaard M, Obel C, Lu M, Olsen J. Early life disease programming during the preconception and prenatal period: making the link between stressful life events and type-1 diabetes. PLoS ONE. (2010) 5:e11523. doi: 10.1371/journal.pone.0011523
52. Glynn LM, Davis EP, Schetter CD, Chicz-Demet A, Hobel CJ, Sandman CA. Postnatal maternal cortisol levels predict temperament in healthy breastfed infants. Early Hum Dev. (2007) 83:675–81. doi: 10.1016/j.earlhumdev.2007.01.003
53. Cao Y, Rao SD, Phillips TM, Umbach DM, Bernbaum JC, Archer JI, et al. Are breast-fed infants more resilient? Feeding method and cortisol in infants. J Pediatr. (2009) 154:452–4. doi: 10.1016/j.jpeds.2008.09.025
54. Lester BM, Conradt E, LaGasse LL, Tronick EZ, Padbury JF, Marsit CJ. Epigenetic programming by maternal behavior in the human infant. Pediatrics. (2018) 142:e20171890. doi: 10.1542/peds.2017-1890
55. Sterling P, Eyer J. Allostasis: a new paradigm to explain arousal pathology. In: Fisher S, Reason J, editors. Handbook of Life Stress, Cognition and Health. New York, NY: JohnWiley & Sons (1988). p. 629–49.
56. McEwen BS. Stress, adaptation, and disease. Allostasis and allostatic load. Ann N Y Acad Sci. (1998) 840:33–44. doi: 10.1111/j.1749-6632.1998.tb09546.x
57. Olson DM, Severson EM, Verstraeten BS, Ng JW, McCreary JK, Metz GA. Allostatic load and preterm birth. Int J Mol Sci. (2015) 16:29856–74. doi: 10.3390/ijms161226209
58. Rich-Edwards JW, Grizzard TA. Psychosocial stress and neuroendocrine mechanisms in preterm delivery. Am J Obstet Gynecol. (2005) 192(5 Suppl.):S30–5. doi: 10.1016/j.ajog.2005.01.072
59. Fergus S, Zimmerman MA. Adolescent resilience: a framework for understanding healthy development in the face of risk. Annu Rev Public Health. (2005) 26:399–419. doi: 10.1146/annurev.publhealth.26.021304.144357
60. Connor KM, Davidson JR. Development of a new resilience scale: the Connor-Davidson Resilience Scale (CD-RISC). Depress Anxiety. (2003) 18:76–82. doi: 10.1002/da.10113
61. Powers MB, Warren AM, Rosenfield D, Roden-Foreman K, Bennett M, Reynolds MC, et al. Predictors of PTSD symptoms in adults admitted to a Level I trauma center: a prospective analysis. J Anxiety Disord. (2014) 28:301–9. doi: 10.1016/j.janxdis.2014.01.003
62. Pietrzak RH, Johnson DC, Goldstein MB, Malley JC, Rivers AJ, Morgan CA, et al. Psychosocial buffers of traumatic stress, depressive symptoms, and psychosocial difficulties in veterans of Operations Enduring Freedom and Iraqi Freedom: the role of resilience, unit support, and postdeployment social support. J Affect Disord. (2010) 120:188–92. doi: 10.1016/j.jad.2009.04.015
63. Folke C, Biggs R, Norström AV, Reyers B, Rockström J. Social-ecological resilience and biosphere-based sustainability science. Ecol Soc. (2016) 21. doi: 10.5751/ES-08748-210341
64. Field T, Sandberg D, Quetel TA, Garcia R, Rosario M. Effects of ultrasound feedback on pregnancy anxiety, fetal activity, and neonatal outcome. Obstet Gynecol. (1985) 66:525–8.
65. Nabhan AF, Aflaifel N. High feedback versus low feedback of prenatal ultrasound for reducing maternal anxiety and improving maternal health behaviour in pregnancy. Cochr Database Syst Rev. (2015) 2015:CD007208. doi: 10.1002/14651858.CD007208.pub3
66. Heberlein EC, Picklesimer AH, Billings DL, Covington-Kolb S, Farber N, Frongillo EA. The comparative effects of group prenatal care on psychosocial outcomes. Arch Womens Ment Health. (2016) 19:259–69. doi: 10.1007/s00737-015-0564-6
67. Consonni EB, Calderon IMP, Consonni M, De Conti MHS, Prevedel TTS, Rudge MVC. A multidisciplinary program of preparation for childbirth and motherhood: maternal anxiety and perinatal outcomes. Reprod Health. (2010) 7:28. doi: 10.1186/1742-4755-7-28
68. Ashford MT, Olander EK, Ayers S. Computer- or web-based interventions for perinatal mental health: a systematic review. J Affect Disord. (2016) 197:134–46. doi: 10.1016/j.jad.2016.02.057
69. Pennebaker JW, Beall SK. Confronting a traumatic event: toward an understanding of inhibition and disease. J Abnorm Psychol. (1986) 95:274–81. doi: 10.1037/0021-843X.95.3.274
70. Pennebaker JW, Smyth JM. Opening up by Writing it Down: How Expressive Writing Improves Health and Eases Emotional Pain. 3rd ed. New York, NY: Guilford Press (2016). 210 p.
71. Kirmayer LJ, Dandeneau S, Marshall E, Phillips MK, Williamson KJ. Rethinking resilience from indigenous perspectives. Can J Psychiatry. (2011) 56:84–91. doi: 10.1177/070674371105600203
72. Lange A, Van De Ven J-P, Schrieken B. Interapy: treatment of post-traumatic stress via the internet. Cogn Behav Ther. (2003) 32:110–24. doi: 10.1080/16506070302317
75. Petrie KJ, Booth RJ, Pennebaker JW, Davison KP, Thomas MG. Disclosure of trauma and immune response to a hepatitis B vaccination program. J Consult Clin Psychol. (1995) 63:787–92. doi: 10.1037/0022-006X.63.5.787
76. Petrie KJ, Fontanilla I, Thomas MG, Booth RJ, Pennebaker JW. Effect of written emotional expression on immune function in patients with human immunodeficiency virus infection: a randomized trial. Psychosom Med. (2004) 66:272–5. doi: 10.1097/01.psy.0000116782.49850.d3
77. Baddeley JL, Pennebaker JW. A postdeployment expressive writing intervention for military couples: a randomized controlled trial. J Trauma Stress. (2011) 24:581–5. doi: 10.1002/jts.20679
78. Esterling BA, L'Abate L, Murray EJ, Pennebaker JW. Empirical foundations for writing in prevention and psychotherapy: mental and physical health outcomes. Clin Psychol Rev. (1999) 19:79–96. doi: 10.1016/S0272-7358(98)00015-4
79. Pennebaker JW, Kiecolt-Glaser JK, Glaser R. Disclosure of traumas and immune function: health implications for psychotherapy. J Consult Clin Psychol. (1988) 56:239–45. doi: 10.1037/0022-006X.56.2.239
80. Booth RJ, Petrie KJ, Pennebaker JW. Changes in circulating lymphocyte numbers following emotional disclosure: evidence of buffering? Stress Med. (1997) 13:23–9. doi: 10.1002/(SICI)1099-1700(199701)13:1<23::AID-SMI714>3.0.CO;2-E
81. Francis ME, Pennebaker JW. Putting stress into words: the impact of writing on physiological, absentee, and self-reported emotional well-being measures. Am J Health Promot. (1992) 6:280–7. doi: 10.4278/0890-1171-6.4.280
82. Frisina PG, Borod JC, Lepore SJ. A meta-analysis of the effects of written emotional disclosure on the health outcomes of clinical populations. J Nerv Ment Dis. (2004) 192:629–34. doi: 10.1097/01.nmd.0000138317.30764.63
83. Zachariae R, O'Toole MS. The effect of expressive writing intervention on psychological and physical health outcomes in cancer patients—a systematic review and meta-analysis. Psychooncology. (2015) 24:1349–59. doi: 10.1002/pon.3802
84. Baddeley JL, Daniel GR, Pennebaker JW. How Henry Hellyer's use of language foretold his suicide. Crisis. (2011) 32:288–92. doi: 10.1027/0227-5910/a000092
85. Hiemstra R. Uses and benefits of journal writing. In: English LM, Gillen MA, editors. Promoting Journal Writing in Adult Education (New Directions for Adult and Continuing Education). San Francisco, CA: Jossey-Bass (2001). p. 19–26.
86. Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap)–a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. (2009) 42:377–81. doi: 10.1016/j.jbi.2008.08.010
87. Jacobsen B, Kinney DK. Perinatal complications in adopted and non-adopted schizophrenics and their controls: preliminary results. Acta Psychiatr Scand. (1980) 62:337–46. doi: 10.1111/j.1600-0447.1980.tb07709.x
88. Brunet A, Weiss DS, Metzler TJ, Best SR, Neylan TC, Rogers C, et al. The peritraumatic distress inventory: a proposed measure of PTSD criterion A2. Am J Psychiatry. (2001) 158:1480–5. doi: 10.1176/appi.ajp.158.9.1480
89. Birmes P, Brunet A, Benoit M, Defer S, Hatton L, Sztulman H, et al. Validation of the peritraumatic dissociative experiences questionnaire self-report version in two samples of French-speaking individuals exposed to trauma. Eur Psychiatry. (2005) 20:145–51. doi: 10.1016/j.eurpsy.2004.06.033
90. Weiss DS, Marmar CR. The impact of event scale—revised. In: Wilson JP, Keane TM, editors. Assessing Psychological Trauma and PTSD. New York, NY: Guilford Press (1997). p. 399–411.
91. Dancause KN, Laplante DP, Fraser S, Brunet A, Ciampi A, Schmitz N, et al. Prenatal exposure to a natural disaster increases risk for obesity in 5(1/2)-year-old children. Pediatr Res. (2012) 71:126–31. doi: 10.1038/pr.2011.18
92. Simcock G, Kildea S, Kruske S, Laplante DP, Elgbeili G, King S. Disaster in pregnancy: midwifery continuity positively impacts infant neurodevelopment, QF2011 study. BMC Pregn Childbirth. (2018) 18:309. doi: 10.1186/s12884-018-1944-5
93. Spielberger CD, Gorsuch RL, Lushene PR, Vagg PR, Jacobs AG. Manual for the State-Trait Anxiety Inventory. Palo Alto, CA: Consulting Psychologists Press (1983).
94. Spielberger CD. State-Trait Anxiety Inventory: Bibliography. 2nd ed. Palo Alto, CA: Consulting Psychologists Press (1989).
95. Cox JL, Chapman G, Murray D, Jones P. Validation of the Edinburgh Postnatal Depression Scale (EPDS) in non-postnatal women. J Affect Disord. (1996) 39:185. doi: 10.1016/0165-0327(96)00008-0
96. Cox JL, Holden JM, Sagovsky R. Detection of postnatal depression. Development of the 10-item Edinburgh Postnatal Depression Scale. Br J Psychiatry. (1987) 150:782–6. doi: 10.1192/bjp.150.6.782
97. Kozinszky Z, Dudas RB. Validation studies of the Edinburgh Postnatal Depression Scale for the antenatal period. J Affect Disord. (2015) 176:95–105. doi: 10.1016/j.jad.2015.01.044
98. Matthey S, Henshaw C, Elliott S, Barnett B. Variability in use of cut-off scores and formats on the Edinburgh Postnatal Depression Scale: implications for clinical and research practice. Arch Womens Ment Health. (2006) 9:309–15. doi: 10.1007/s00737-006-0152-x
99. Smith-Nielsen J, Matthey S, Lange T, Vaever MS. Validation of the Edinburgh Postnatal Depression Scale against both DSM-5 and ICD-10 diagnostic criteria for depression. BMC Psychiatry. (2018) 18:393. doi: 10.1186/s12888-018-1965-7
100. Carver CS, Scheier MF, Weintraub JK. Assessing coping strategies: a theoretically based approach. J Pers Soc Psychol. (1989) 56:267–83. doi: 10.1037/0022-3514.56.2.267
101. Carver CS. You want to measure coping but your protocol's too long: consider the brief COPE. Int J Behav Med. (1997) 4:92–100. doi: 10.1207/s15327558ijbm0401_6
102. Wong PTP, Reker GT, Peacock EJ. A resource-congruence model of coping and the development of the coping schema inventory. In: Wong PTP, Wong LCJ, editors. Handbook of Multicultural Perspectives on Stress and Coping. International and Cultural Psychology Series. Dallas, TX: Spring Publications (2006). p. 223–83.
103. Sarason IG, Johnson JH, Siegel JM. Assessing the impact of life changes: development of the Life Experiences Survey. J Consult Clin Psychol. (1978) 46:932–46. doi: 10.1037/0022-006X.46.5.932
104. Sarason IG, Sarason BR, Shearin EN, Pierce GR. A brief measure of social support: practical and theoretical implications. J Soc Person Relat. (1987) 4:497–510. doi: 10.1177/0265407587044007
105. Cohen S, Kamarck T, Mermelstein R. A global measure of perceived stress. J Health Soc Behav. (1983) 24:385–96. doi: 10.2307/2136404
106. Felitti VJ, Anda RF, Nordenberg D, Williamson DF, Spitz AM, Edwards V, et al. Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults. The Adverse Childhood Experiences (ACE) Study. Am J Prev Med. (1998) 14:245–58. doi: 10.1016/S0749-3797(98)00017-8
107. Exley D, Norman A, Hyland M. Adverse childhood experience and asthma onset: a systematic review. Eur Respir Rev. (2015) 24:299–305. doi: 10.1183/16000617.00004114
108. Bellis MA, Hughes K, Leckenby N, Perkins C, Lowey H. National household survey of adverse childhood experiences and their relationship with resilience to health-harming behaviors in England. BMC Med. (2014) 12:72. doi: 10.1186/1741-7015-12-72
109. Bricker D, Squires J, Mounts L, Potter L, Nickel R, Twombly E. Ages & Stages Questionnaire: A Parent-Completed Monitoring System. Baltimore, MD: Paul H. Brookes Publishing Co. (1999).
110. Squires J, Bricker D. Ages & Stages Questionnaires®, Third Edition (ASQ®-3): A Parent-Completed Child Monitoring System. Baltimore, MD: Paul H. Brookes Publishing Co., Inc. (2009).
111. Fenson L, Dale P, Reznich J, Thal D, Bates E, Hartung J, et al. MacArthur Communicative Development Inventories: User's Guide and Technical Manual. San Diego, CA: Singular Publishing Group (1993).
112. Briggs-Gowan MJ, Carter AS, Irwin JR, Wachtel K, Cicchetti DV. The Brief Infant-Toddler Social and Emotional Assessment: screening for social-emotional problems and delays in competence. J Pediatr Psychol. (2004) 29:143–55. doi: 10.1093/jpepsy/jsh017
113. Kruizinga I, Visser JC, van Batenburg-Eddes T, Carter AS, Jansen W, Raat H. Screening for autism spectrum disorders with the Brief Infant-Toddler Social and Emotional Assessment. PLoS ONE. (2014) 9:e97630. doi: 10.1371/journal.pone.0097630
114. Giserman Kiss I, Feldman MS, Sheldrick RC, Carter AS. Developing autism screening criteria for the Brief Infant-Toddler Social and Emotional Assessment (BITSEA). J Autism Dev Disord. (2017) 47:1269–77. doi: 10.1007/s10803-017-3044-1
115. Bayley N. Bayley Scales of Infant and Toddler Development. 3rd ed. Toronto, ON: Pearson Canada Inc (2005).
116. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. (2006) 3:77–101. doi: 10.1191/1478088706qp063oa
117. Gold MS, Bentler PM. Treatments of missing data: a Monte Carlo comparison of RBHDI, iterative stochastic regression imputation, and expectation-maximization. Struct Equ Model. (2000) 7:319–55. doi: 10.1207/S15328007SEM0703_1
118. Hayes AF, Rockwood NJ. Regression-based statistical mediation and moderation analysis in clinical research: observations, recommendations, and implementation. Behav Res Ther. (2017) 98:39–57. doi: 10.1016/j.brat.2016.11.001
119. Verstraeten BSE, Elgbeili G, Hyde A, King S, Olson DM. Maternal mental health after a wildfire: effects of social support in the Fort McMurray Wood Buffalo Study. Can J Psychiatry. (2020) 1–9. doi: 10.1177/0706743720970859
120. Brémault-Phillips S, Pike A, Olson J, Severson E, Olson D. Expressive writing for wildfire-affected pregnant women: themes of challenge and resilience. Int J Disast Risk Reduct. (2020) 50:101730. doi: 10.1016/j.ijdrr.2020.101730
121. Centre for Research on the Epidemiology of Disasters. EM-DAT: Emergency Events Database Brussels. Belgium: Universite Catholique de Louvain, School of Public Health (2020). Available from: https://www.emdat.be/database (accessed August 19, 2020).
122. Minkler M, Wallerstein N. Community-Based Participatory Research for Health: From Process to Outcomes. 2nd ed. San Francisco, CA: Jossey-Bass (2008).
123. Dominguez TP, Dunkel-Schetter C, Glynn LM, Hobel C, Sandman CA. Racial differences in birth outcomes: the role of general, pregnancy, and racism stress. Health Psychol. (2008) 27:194–203. doi: 10.1037/0278-6133.27.2.194
124. Abdou CM, Schetter CD, Jones F, Roubinov D, Tsai S, Jones L, et al. Community perspectives: mixed-methods investigation of culture, stress, resilience, and health. Ethn Dis. (2010) 20(1 Suppl. 2):S2–41–8. Available online at: https://www.ethndis.org/priorsuparchives/ethn-20-01s2-s41.pdf
Keywords: natural disaster, wildfire, pregnancy, prenatal maternal stress, maternal mental health, resilience, developmental origins of health and disease, child development
Citation: Hyde A, Verstraeten BSE, Olson JK, King S, Brémault-Phillips S and Olson DM (2021) The Fort McMurray Mommy Baby Study: A Protocol to Reduce Maternal Stress Due to the 2016 Fort McMurray Wood Buffalo, Alberta, Canada Wildfire. Front. Public Health 9:601375. doi: 10.3389/fpubh.2021.601375
Received: 31 August 2020; Accepted: 06 May 2021;
Published: 17 June 2021.
Edited by:
Arthur Chan, University of Toronto, CanadaReviewed by:
Emily Harville, Tulane University, United StatesCopyright © 2021 Hyde, Verstraeten, Olson, King, Brémault-Phillips and Olson. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: David M. Olson, ZGF2aWQub2xzb25AdWFsYmVydGEuY2E=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.