
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Public Health, 20 September 2021
Sec. Infectious Diseases: Epidemiology and Prevention
Volume 9 - 2021 | https://doi.org/10.3389/fpubh.2021.580102
 Anna J. Henningsson1,2,3*†
Anna J. Henningsson1,2,3*† Audun Aase4
Audun Aase4 Herjan Bavelaar1
Herjan Bavelaar1 Signe Flottorp5Pia Forsberg6Ingvild Kirkehei7Matilda Lövmar3Kenneth Nilsson8
Signe Flottorp5Pia Forsberg6Ingvild Kirkehei7Matilda Lövmar3Kenneth Nilsson8 Dag Nyman9†Katharina Ornstein10†
Dag Nyman9†Katharina Ornstein10† Johanna Sjöwall3,11Barbro H. Skogman12,13Ivar Tjernberg3,14Ingeborg Aaberge4
Johanna Sjöwall3,11Barbro H. Skogman12,13Ivar Tjernberg3,14Ingeborg Aaberge4Background: For the most important and well-known infections spread by Ixodes ticks, Lyme borreliosis (LB) and tick-borne encephalitis (TBE), there are recommendations for diagnosis and management available from several health authorities and professional medical networks. However, other tick-borne microorganisms with potential to cause human disease are less known and clear recommendations on diagnosis and management are scarce. Therefore, we performed a systematic review of published studies and reviews focusing on evaluation of laboratory methods for clinical diagnosis of human tick-borne diseases (TBDs), other than acute LB and TBE. The specific aim was to evaluate the scientific support for laboratory diagnosis of human granulocytic anaplasmosis, rickettsiosis, neoehrlichiosis, babesiosis, hard tick relapsing fever, tularemia and bartonellosis, as well as tick-borne co-infections and persistent LB in spite of recommended standard antibiotic treatment.
Methods: We performed a systematic literature search in 11 databases for research published from 2007 through 2017, and categorized potentially relevant references according to the predefined infections and study design. An expert group assessed the relevance and eligibility and reviewed the articles according to the QUADAS (diagnostic studies) or AMSTAR (systematic reviews) protocols, respectively. Clinical evaluations of one or several diagnostic tests and systematic reviews were included. Case reports, non-human studies and articles published in other languages than English were excluded.
Results: A total of 48 studies fulfilled the inclusion criteria for evaluation. The majority of these studies were based on small sample sizes. There were no eligible studies for evaluation of tick-borne co-infections or for persistent LB after antibiotic treatment.
Conclusions: Our findings highlight the need for larger evaluations of laboratory tests using clinical samples from well-defined cases taken at different time-points during the course of the diseases. Since the diseases occur at a relatively low frequency, single-center cross-sectional studies are practically not feasible, but multi-center case control studies could be a way forward.
The European tick Ixodes ricinus is the vector of several potential human pathogens, of which Borrelia burgdorferi sensu lato (s.l.) and tick-borne encephalitis virus (TBEV) are the most important and well-known in human medicine. The diagnosis of the diseases they may cause, Lyme borreliosis (LB) and tick-borne encephalitis (TBE), is based on the patients' medical history and clinical signs and symptoms together with laboratory support, which mainly consists of serology, sometimes supplemented with molecular detection by PCR. Both for LB and for TBE, clinical case definitions and recommendations for management are available from several health authorities and professional medical networks [e.g., (1–5)], with the exception of diagnostic methods for detection of possible persisting Borrelia infection in patients with remaining symptoms after antibiotic treatment of LB. Other tick-borne microorganisms with potential to cause human disease are less known and clear recommendations on diagnosis and management are scarce. Potential human pathogens that have been found in I. ricinus in northern or central Europe are for example Anaplasma phagocytophilum (6–8), Rickettsia spp. (6, 9, 10), Neoehrlichia mikurensis (11–13), Babesia species (spp.) (14, 15), Borrelia miyamotoi (16–18), Francisella tularensis (19–21) and Bartonella spp. (22–24). Several of these have the potential to cause severe disease, especially in immunocompromised patients [A. phagocytophilum: (25, 26); Babesia spp.: (27–30); B. miyamotoi: (31, 32); N. mikurensis: (33); Rickettsia spp.: (34, 35)], while their medical importance in immunocompetent individuals is more uncertain. Reports on seropositivity in tick-exposed populations without a known history of disease [A. phagocytophilum: (7, 36); Babesia spp.: (37, 38); B. miyamotoi: (39); multiple tick-borne pathogens: (40); Bartonella spp.: (41); N. mikurensis: (42); F. tularensis: (43); Rickettsia spp.: (44, 45)] indicate that exposure to several of these microorganisms does not always entail symptoms, or perhaps only causes mild and self-limiting symptoms. On the other hand, signs and symptoms like fever, skin rash, neutropenia, leukopenia, elevated liver enzymes, lymphadenopathy and even CNS infection, have also been reported in immunocompetent patients [A. phagocytophilum: (26, 46); Babesia spp.: (47); B. miyamotoi: (48–50); N. mikurensis: (51, 52); F. tularensis: (53); Rickettsia spp.: (54)], and consequently, a certain under-diagnosis of these infections must be suspected. Co-infections with more than one tick-borne pathogen have been reported [e.g., (28, 55–57)], but are probably in most cases overlooked in clinical practice. Recommendations regarding clinical and laboratory investigation of possible tick-borne co-infections are scarce and general guidelines are lacking. The scarcity of well-established guidelines for diagnosis and management of several of the tick-borne diseases (TBDs) contribute to the existing medical controversies in this field.
In 2015, the Norwegian Directorate of Health initiated a Nordic consensus collaboration focusing on diagnosis and management of TBDs other than LB and TBE, led by the Norwegian National Advisory Unit on Tick-borne Diseases. The Nordic consensus network consisted of physicians and researchers from Norway, Sweden, Denmark and Finland, as well as representatives from patient organizations. As part of this work, the Norwegian Institute of Public Health was engaged to perform a systematic literature search on clinical studies evaluating laboratory methods for diagnosis of human TBDs other than LB and TBE, and a group of physicians from the Nordic countries, all with clinical and research experience of TBDs, were assigned the task of reviewing the relevant references. The review process was observed by representatives from the Public Health Agency of Sweden, the Swedish Medical Products Agency, and the National Board of Health and Welfare in Sweden.
The purpose of this present systematic review was to provide an overview of published research from 2007 through 2017 on the performance of laboratory tests evaluated on clinical samples (i.e., using authentic patient samples) for the diagnosis of human TBDs, other than untreated LB and TBE, including laboratory diagnosis of tick-borne co-infections and post-treatment persisting LB, with the objective to elucidate the following clinical questions:
a) In patients with complaints possibly related to previous tick bite(s) and with negative laboratory diagnostic tests for LB and TBE, or previously antibiotic-treated LB, what diagnostic tests are relevant for diagnosing or excluding other TBDs, including tick-borne co-infections?
b) Are there any laboratory tests that can reliably support the diagnosis of persistent LB in spite of recommended standard antibiotic treatment?
This systematic review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Protocols (PRISMA-P) guidelines (58). Protocols were developed both for the search and the review process.
We divided the work into two parts: (1) laboratory diagnosis of (single) TBDs, and (2) laboratory diagnosis of tick-borne co-infections. In both parts, we performed a systematic literature search and screened through the search results according to predefined selection criteria. In the first scientific literature search, we included references comprising research on adults, young people and children with symptoms of the following infections:
- human granulocytic anaplasmosis (Anaplasma phagocytophilum)
- rickettsiosis (Rickettsia helvetica or Rickettsia conorii)
- neoehrlichiosis (Neoehrlichia mikurensis)
- babesiosis (Babesia spp.)
- hard tick relapsing fever (Borrelia miyamotoi)
- tularemia (Francisella tularensis)
- bartonellosis (Bartonella spp.)
or with persisting symptoms after antibiotic treatment of LB (“chronic Lyme disease” or “post treatment Lyme disease syndrome”).
All laboratory methods identified in the literature search were considered as relevant, e.g., enzyme-linked immunosorbent assays (ELISA), immunofluorescent assays (IFA), immunoblotting, polymerase chain reaction (PCR), microscopy and culture. The following study designs were included: systematic reviews, cross sectional studies and case control studies. We also included case series and case studies mentioning diagnosis or diagnostic tests in the abstract. The search was limited to the publication years 2007–2017 to focus on more recent methods such as PCR. We excluded studies on tests for the diagnosis of early localized and early/late disseminated LB and TBE. We excluded studies on infections in ticks and domestic or wild animals.
In the second literature search, we included all studies reporting prevalence of or diagnostic methods for identifying co-infections between two or more of the ten infections included in the first search. In addition, we included studies on all stages of LB as well as TBE. This search was also limited to publication years 2007–2017. Studies on patients with other co-infections than TBDs, e.g., HIV, were excluded.
We searched the following databases: MEDLINE (Ovid), Embase (Ovid), Cochrane Database of Systematic Reviews (Cochrane Library), Database of Abstracts of Reviews of Effects (CRD DARE), Health Technology Assessments Database (CRD HTA), Epistemonikos, ISI Web of Science, Scopus, Prospero, ClinicalTrials.gov, WHO International Clinical Trials Registry Platform (ICTRP). In the first search, all databases mentioned above were searched by Kirkehei in January 2018, and in the second search, Kirkehei searched the following databases in August 2018: MEDLINE (Ovid), Embase (Ovid), Epistemonikos and ISI Web of Science.
A research librarian (Kirkehei) performed systematic searches based on the eligibility criteria (Table 1). All searches were described in detail in a separate report from the Norwegian Institute of Public Health (59). Another librarian, the project group at the Norwegian Institute of Public Health and the Nordic group of physicians (hereafter called “the Nordic expert group”) assured the quality of the search strategies.
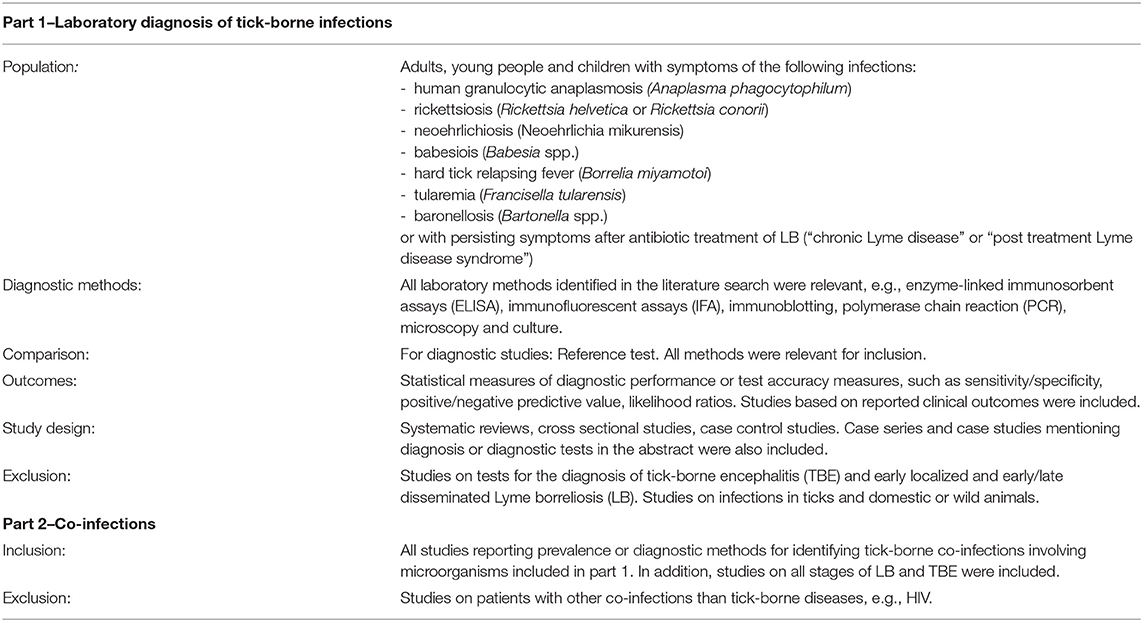
Table 1. Eligibility criteria used for the systematic literature search.
Kirkehei performed the searches in January 2018. The searches consisted of subject headings and free text terms describing the included TBDs and terms typically used when describing diagnostics (for instance diagnostic performance, sensitivity, specificity) or relevant study designs (for instance cross-sectional studies). The first search was limited to studies mentioning “ticks” (and other terms describing tick-bites) in the title or abstract. In a second supplementary search, this limitation was removed. Studies on animals or ticks (without mentioning humans) were also excluded from the search.
References from the literature search were exported to the online screening tool Covidence (60). Two of the following persons independently screened all references (Kirkehei, Flottorp, Aaberge or Aase), and disagreements were resolved through discussion. The references were screened based on title and abstract, full texts were not read at this stage.
Included references were exported to the reference management system EndNote X9 (Clarivate Analytics, Philadelphia, PA, USA) where one person (Kirkehei) sorted the references into categories by infection type and publication year. The project group at the Norwegian Institute of Public Health checked the final sorting result.
In the first broad search (diagnostic tests), Kirkehei extracted information on diagnostic methods provided only in the abstracts. To ascertain relevance and to assess methodological quality, the Nordic expert group read the studies in full text. At this point, references where only abstract and no full text was available were excluded as well as case reports, case series and papers written in other languages than English. After assessment of the full-text articles, non-systematic reviews and studies of methods not intended for clinical diagnostics in humans were also excluded.
Two reviewers from the Nordic expert group independently extracted data on authors, scientific journal and year of publication, country where the study was conducted, number of participants in study population, type of method that was studied, antigen or target gene used in the studied method, if the index test had been compared with a reference test/standard, diagnostic accuracy (i.e., sensitivity, specificity, negative predictive value, positive predictive value), and study findings. The expert reviewers independently assessed the risk of bias in each individual study. For the assessment of diagnostic studies, the QUADAS (61) checklist was used, whereas the AMSTAR (62) checklist was applied for systematic reviews. Each study obtained an over-all classification of high, medium, or low risk of bias. Disagreements between the reviewers were discussed and resolved through consensus or, if needed, by an extra expert reviewer. In some cases, a risk classification of low/medium or medium/high were considered appropriate. In case a reviewer had co-authored an article, the review task was given to another independent reviewer.
A descriptive analysis stratified by each TBD was used to summarize studies included in this systematic review. Themes for analysis included types of diagnostic methods, test performance, applicability, relevance and usefulness in clinical practice.
The study selection process and reasons for exclusion are shown in Figure 1. The search retrieved 4, 440 unique references. A total of 3, 864 references were excluded through an initial screening of the titles and/or the abstracts by two independent persons using Covidence as described above. We included 576 references and sorted them according to the type of TBD. One hundred forty-eight full-text articles were assessed for eligibility by the expert reviewers; 48 were included for quality assessment according to the QUADAS or AMSTAR checklists (Table 2). References that were excluded at this point are listed in Table 3. The results of the in-depth expert review (QUADAS/AMSTAR) are summarized below and in Table 2.
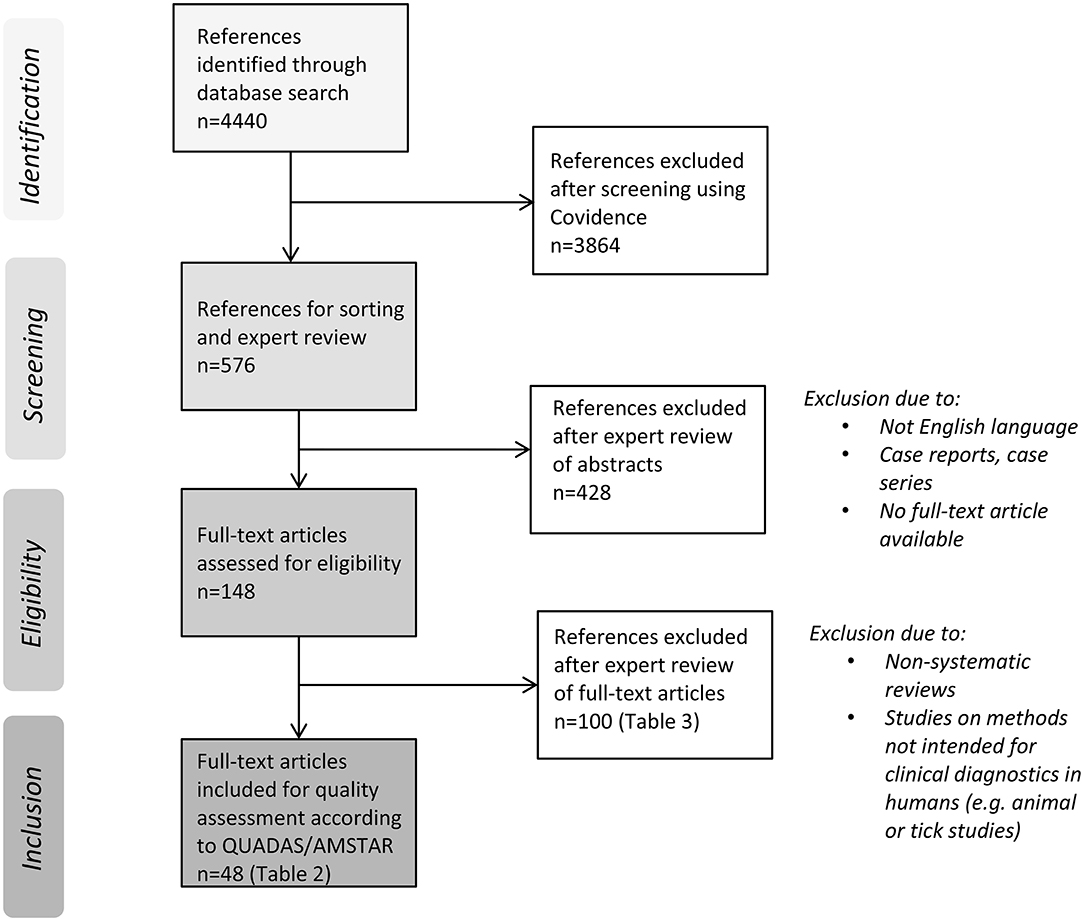
Figure 1. Flow diagram of literature search and study selection process.

Table 2. General information on the 48 publications that were included for quality assessment according to the QUADAS (diagnostic studies) or AMSTAR (systematic reviews) checklists.
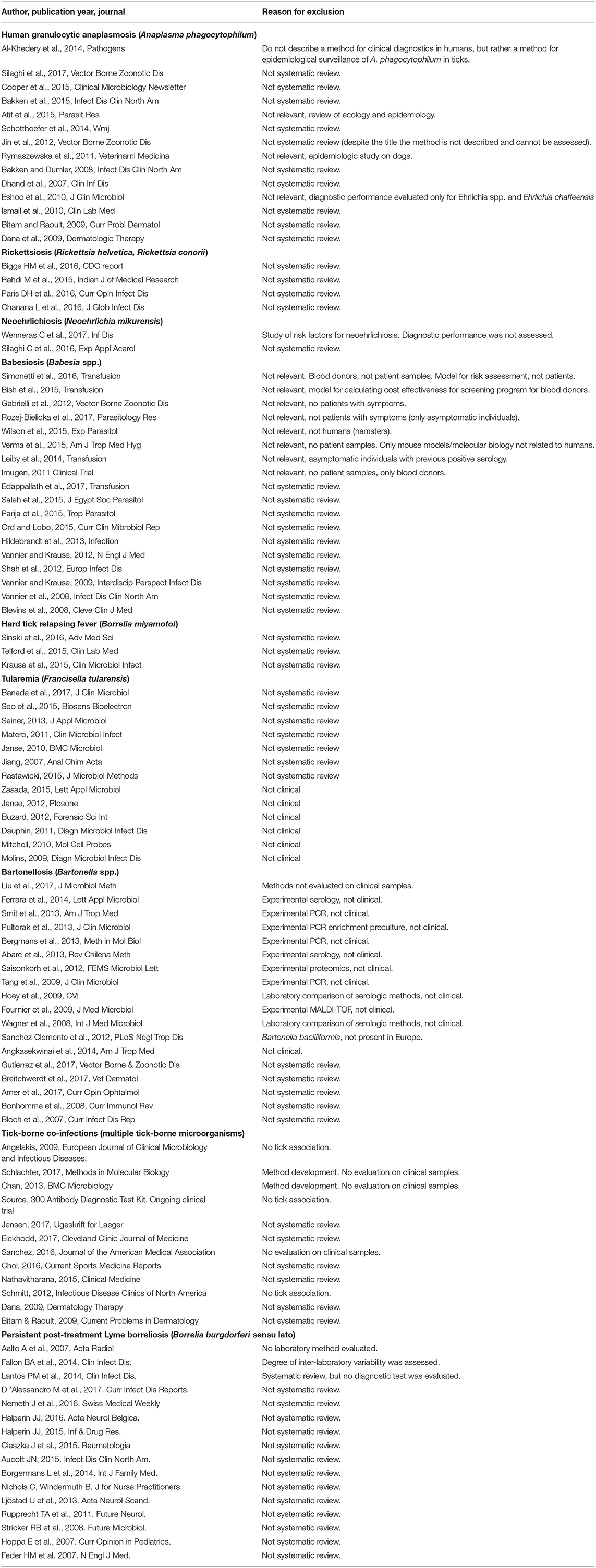
Table 3. Full-text publications reviewed but excluded from further quality assessment by QUADAS/AMSTAR.
Regarding laboratory methods evaluated for diagnosis of human granulocytic anaplasmosis (HGA), two studies on molecular detection (real-time PCR and loop-mediated isothermal amplification) vs. serology or blood smear microscopy and one systematic review were assessed according to the checklists.
Nine studies were reviewed, five regarding molecular detection and quantification (PCR, qPCR), of which one compared reverse line blot hybridization vs. qPCR. Four were serological studies [IFA, Western blot (WB), ELISA], one of which compared an epifluorescence immunoassay vs. conventional IFA and another compared ELISA vs. IFA.
One study using PCR for laboratory diagnosis of neoehrlichiosis in humans fulfilled the inclusion criteria for publications evaluating diagnostic tests and was reviewed according to the QUADAS checklist. Another publication did not contain information about diagnostic performance and one review was not systematic, and thus, these publications were excluded (Table 3).
For Babesia spp., 14 studies fulfilled the criteria for review according to the QUADAS checklist, eight studies on PCR, four on serology (IFA, multiplex IgG and EIA), one on CellaVision and one on modified microscopy. One systematic review was also included.
For B. miyamotoi, four studies fulfilled the criteria for in-depth review; two studies on serological methods (ELISA and Luminex), one on nested PCR and one aiming primarily at optimizing culture procedures from clinical samples.
Seven diagnostic studies regarding F. tularensis qualified for review according to the QUADAS protocol; all of them on serological methods (ELISA, immunochromatography and Western blot).
Out of 33 abstracts, ten diagnostic studies were included for further review. Five studies presented evaluations of serologic assays (ELISA, IFA), one of immunohistochemistry, and four studies of PCR methods.
Two publications (Schlachter, Chan, Table 3) from the same group of researchers described the same multiplex PCR assay targeting Borrelia spp. (recA gene), A. phagocytophilum (APH1387 gene) and Bab. microti (BmTPK gene). Human blood spiked with cultured B. burgdorferi and plasmids containing the target genes from A. phagocytophilum and Bab. microti added to the extracted DNA were used for developing the method but it was not evaluated on clinical patient samples, and the studies were therefore not included in the review. No other studies fulfilled the inclusion criteria.
None of the published articles assessed for eligibility (n = 16) met the inclusion criteria and all were consequently excluded from the review. No laboratory method useful for clinical diagnostic support of persisting post-treatment LB symptoms was found in this present systematic review. Five publications were primarily included, but later excluded (Table 3). Two out of five publications did not study any laboratory method and one did not focus on persisting LB after antibiotic treatment. In the last two studies, one focusing on serologic response and the other being a review on culture, the authors found the methods not useful for supporting persistent B. burgdorferi s.l. infection.
In this systematic review we performed a broad, thorough, and systematic literature search in an attempt to identify all studies mentioning diagnostic methods of TBD, regardless of study design. Nonetheless, we may still have lost some relevant studies. We limited the search to studies mentioning tick or tick bite in the title or abstract. However, not all studies on TBD explicitly mention “ticks,” and therefore we performed a supplementary search without this limitation. Instead, we limited the search to those described as cross-sectional studies or diagnostic accuracy studies. This supplementary search gave some additional references, mainly about diagnostics of tularemia and babesiosis. Due to the study design criteria applied in the supplementary search, we may have missed some relevant publications, i.e., case reports and case series. On the other hand, a major aim of this review was to investigate to what extent the different diagnostic methods described or mentioned in the scientific literature have been evaluated in comparative studies using authentic human clinical samples. The search for Lyme disease (borreliosis) was limited to studies on so called “chronic Lyme disease” according to the initial aim. To find as many relevant studies as possible, we also used search terms as “chronic or persistent or lingering or long-term.” However, it is possible that studies that have used other descriptions for this condition may have been missed.
Only few studies of high quality comparing two laboratory methods have been published (Pan; Schotthoefer). One systematic review was published suggesting all three methods; microscopy of blood smear/buffy coat, PCR of blood and serology (Sanchez). However, in the acute phase of the disease, molecular detection by PCR in blood seems to have a higher sensitivity than microscopy of blood smear, and in later phase (>4 days) of disease, serology with paired samples could be preferred. In a non-systematic review (Silaghi, Table 3) it was concluded that molecular methods are preferred for direct detection of Anaplasma spp. in blood and tissue samples, but the sensitivity of PCR is only 68.2% in European HGA. Diagnostic methods have also been summarized in a more recent non-systematic review on eco-epidemiology and clinical management of anaplasmosis (63). Further comparative studies on evaluation of laboratory diagnostics are needed in order to be able to recommend evidence-based diagnostic methods in each phase of the disease in humans.
Of the various serological tests available for laboratory diagnostics of rickettsial infection, microimmunofluorescence (MIF) or IFA for detection of IgG and IgM in acute and convalescent sera are widely used (Bizzini, Kantsö) and accepted as the reference method (64). A major disadvantage includes poor sensitivity during early infection, and this is a limitation when using single sera for diagnosis. Another limitation is that the interpretation of serological data can be confused by cross-reactions with other Rickettsia spp. and similar to that, the species of Rickettsia chosen as antigen source also affects the outcome. The utility of protein immunoblots or ELISA with recombinant antigen may be an alternative (Kowalczewska, Do), but is not yet sufficiently validated (65). Molecular methods are both sensitive and specific. Real-time PCR is often used for detection, while conventional and nested PCR also have the potential for sequencing, and a number of equally useful gene targets are reported, and unique gene regions can be targeted for species identification (Boretti, Mouffok, Renvoise, Znazen). The most useful specimens, often during early infection, are swabs or skin biopsies from the “eschar” or blood (buffy coat) (66).
One high quality study with low risk of bias compared two different laboratory methods: a multiplex PCR and a singleplex real-time PCR (Quarsten). It showed a low sensitivity (6%) for the multiplex PCR and a slightly higher, but still low, sensitivity (10%) for the singleplex PCR. Plasma was found to be superior to whole blood for detection of N. mikurensis DNA in human samples. So far, no serologic tests have been developed for neoehrlichiosis. Further high-quality studies are needed before any recommendation for laboratory evaluation of patients with suspected neoehrlichiosis can be stated.
Golden standard for babesiosis diagnostics is still conventional blood smear. IFA serology and/or PCR can be used for confirmation of the blood smear results. Four studies (three on Bab. microti and one on Bab. microti and Bab. divergens) were included where serology was compared to microscopy. In all of these the serology was also compared to either PCR and/or IFA (Table 2). The sensitivity of the serological tests in three of the studies varied between 84.5 and 97.4%. In the fourth study, diagnostic accuracy could not be calculated due to the low number of samples included. Specificity varied between 97.6 and 99.5%, but was only calculated in two of the four studies. However, in all four studies the risk of bias was graded as medium to high, making it difficult to draw any firm conclusions.
Four studies compared PCR to blood smear and two studies compared PCR to blood smear and serology or conventional PCR. Most of the studies focused on Bab. microti, possibly because they were conducted in the US where this species is most prevalent (30). In the studies where sensitivity of the PCR assays was reported it was 100% (Table 2). In one study, the sensitivity was reported as 5–10 parasites/μl. Furthermore, two studies compared different methods of microscopy with conventional blood smear. In one of the studies (Aase), a modified microscopy protocol, called the LM method, was compared with PCR and serology. This study had a low risk of bias but no positive samples other than the positive controls, and the conclusion in the study was that the modified microscopy method was unreliable. The other study (Racsa) evaluated CellaVision, but only six samples from patients with babesiosis were included, making conclusions regarding its usefulness difficult. Taken together, there is not sufficient scientific support to change the golden standard of conventional blood smear microscopy, but PCR and IFA serology can be used as a complement when the results from the microscopy are uncertain.
According to the systematic review by Sanchez et al. microscopy on thin blood smear is the most reliable method for diagnosis of active babesiosis, evidence grading I-B (American Evidence-Based Scoring System). PCR should be considered early in the infection when parasites are few and difficult to visualize in blood smears, but should be used with caution when monitoring response to therapy since DNA can be detected for a long time after parasites are no longer visualized in blood smears (IIb-B). Serology can confirm the diagnosis (I-B), but cannot replace microscopy and PCR.
B. miyamotoi was discovered as a potential human pathogen as recently as 2011 (49), and so far the disease has been described in case reports and case series from Asia, Europe and North America (31, 32, 49, 50, 67, 68), and consequently, larger evaluations of diagnostic methods are lacking. The experience of clinical diagnostics originates from limited case series and case reports and have recently been summarized in a non-systematic review by Cutler et al. (69). Laboratory methods for diagnosis mainly employ PCR and serology, even though positive microscopy findings have been reported in cerebrospinal fluid (CSF) from immunocompromised patients with B. miyamotoi-associated meningoencephalitis (31, 32, 67). Culture in modified Kelly-Pettenkorfer medium as described by Koetsveld et al. (Table 2) is laborious, time-consuming and has a rather low sensitivity in clinical samples and is therefore mainly suited for research purposes. PCR methods targeting the 16S rRNA, glpQ or flagellin genes have been able to detect B. miyamotoi-specific DNA in CSF and blood samples from meningoencephalitis cases, and from blood samples from patients with systemic illness (31, 70, 71). Commercially available ELISAs based on the C6 peptide, as evaluated by Molloy et al. (Table 2), may be positive in B. miyamotoi disease, but are not able to distinguish between infections caused by B. miyamotoi and B. burgdorferi s.l. causing Lyme borreliosis. In contrast, glycerophosphodiester phosphodieasterase (GlpQ) antigen is present in relapsing fever Borrelia but not in B. burgdorferi s.l. and can therefore discriminate between the two (72). In a more recent study, combinations of GlpQ and Variable major proteins (Vmps) from B. miyamotoi increased sensitivity and/or specificity compared to single antigens (73). However, GlpQ and Vmps assays are still experimental and not yet widely available. It appears that PCR is the most suitable diagnostic method in early systemic disease, i.e., the first 1–2 (4) weeks, as the development of specific antibodies may be delayed (49). Also, development of antibody responses may be generally compromised in immunosuppressed individuals, for example patients treated with rituximab (31, 32, 50, 67). However, establishment of more precise recommendations for laboratory testing in suspected B. miyamotoi disease will need further evaluation.
Tick bites are the most common mode of transmission for F. tularensis subsp. tularensis to humans in the USA (74). The presence of the less virulent F. tularensis subsp. holarctica in European ticks has been described (19–21), but transmission of tularemia via ticks is relatively uncommon (53, 75, 76). Laboratory confirmation of tularemia consists of detecting the bacteria in a biological sample and/or detecting a specific antibody response. The seven articles included in this review were on serological methods, including one in conjunction with PCR. All studies were assessed as having a medium risk of bias regarding clinical materials. The performance of serology is adequate for diagnosis in cases with a typical presentation (ulceroglandular tularemia), with caution for serological cross-reactions. The varying specificity of serological tests should, whenever possible, prompt confirmation with PCR of biological material in atypical presentations, especially in a low-prevalence setting.
In I. ricinus ticks, Bartonella spp. are found variably in 0–30% (18, 77–79). However, tick-borne transmission of Bartonella spp. to humans has not definitely been established, despite the detection of specific antibodies in 15–33% of individuals with LB (80, 81).
Among the 25 articles evaluating diagnostic methods, there was none assessed as being of high quality. Most of them were non-clinical laboratory comparisons of methods, either serological or PCR. The recommendation from the European Centre for Disease Prevention and Control regarding diagnostics in suspected bartonellosis consists of bacterial culture, PCR and serology in combination, but has not been consequently applied.
The lack of eligible articles focusing on human tick-borne co-infections highlights the need for further studies.
The terms post-treatment Lyme borreliosis/disease, chronic Lyme borreliosis/disease and persisting post-treatment Lyme borreliosis/disease are interchangeably used in the scientific contexts to describe a heterogenous patient population with mainly unspecific symptoms, either attributable to LB or not, following recommended antibiotic treatment of LB (82–85). In this systematic literature search, we included several search terms usually used to describe the phenomenon, to cover the whole scientific spectrum of published papers. Following the first broad search, 16 review articles and four articles comparing one or more methods were assessed for eligibility. However, none of the papers fulfilled the inclusion criteria. We conclude that to date, science has no alternative diagnostic tests to offer patients with persisting symptoms post-treatment besides the well-established ones recommended for investigation of LB. In a recently published report, however, it has been shown that symptoms that are often categorized as chronic LB in the general debate could not be uniquely linked to LB (86). Instead, ~20% of the total group of patients showed signs of autoimmunity. Further studies are needed to confirm these results, but the findings may provide an alternative explanation for this medical controversy and indicate that diagnostic tests for these conditions need a different focus.
Taken together, the number of published studies and systematic reviews regarding the accuracy of diagnostic tests for TBDs, other than LB and TBE, evaluated on clinical samples, were unexpectedly limited. Many of the studies have been performed on a small number of study participants using a case control study design. When assessing these studies according to the QUADAS checklist, many of them were classified as having a medium to high risk of bias. This is of course a highly relevant problem when evaluating patients with complaints possibly related to tick bite(s). Which microbes should be tested for and what laboratory methods should be used? Unfortunately, our systematic review reveals that high quality clinical evaluations of which laboratory methods to use for diagnosis of most of the listed TBDs are scarce. However, one should also realize that cross sectional studies, that are often considered to be of higher quality than case control studies, are difficult to perform on infectious diseases that occur with low frequency in the population. Consequently, we need to accept case control studies together with epidemiological studies and case series. Admittedly, one needs to keep in mind that a medium to high risk of bias according to the QUADAS checklist does not necessarily imply poor quality of the study with regard to evaluation of test performance, since major factors of importance are inclusion of well-defined clinical cases and relevant controls.
For diagnosis of TBDs other than LB and TBE, a number of different laboratory techniques have been used, such as blood smear microscopy, immunohistochemistry, culture, serology and PCR. Which method that is most suitable partly depends on during which phase of the disease the samples are taken. Two or three methods are preferably combined in order to achieve higher sensitivity. For most of the TBDs covered in this systematic review, only few studies fulfilled the inclusion criteria for in-depth evaluation, and several of them were based on small study populations. There were no eligible evaluation studies for tick-borne co-infections or for persistent LB after antibiotic treatment. Our findings highlight the need for larger evaluations of laboratory tests using clinical samples from well-defined cases taken at different time-points during the course of the diseases. Since the TBDs occur with low frequency in the population, single-center cross-sectional studies are practically not possible, but multi-center case control studies using well-defined clinical cases and relevant controls could be a way forward.
The original contributions presented in the study are included in the article, further inquiries can be directed to the corresponding author.
All authors listed have made a substantial, direct and intellectual contribution to the work, and approved it for publication.
This work was supported by the Norwegian Directorate of Health and by grants of the European Union through the European Development fund and the Interreg Öresund-Kattegat-Skagerrak and the Interreg NorthSea Region Programmes 2014-2020 as part of the ScandTick Innovation project (reference number 2015-29 000167) and the NorthTick project (reference number J-No: 38-2-7-19).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The authors would especially like to thank Thomas Åkerlund, microbiologist and advisor at the Unit for laboratory surveillance of bacterial pathogens, Public Health Agency of Sweden, for valuable advice during the review process. The work of the Nordic expert group was also supported by Karin Söderberg Löfdal, M.D. and Ph.D., Swedish Medical Products Agency, and Ulf Törnebladh, M.D., medical advisor at the National Board of Health and Welfare, Sweden.
1. Stanek G, Fingerle V, Hunfeld KP, Jaulhac B, Kaiser R, Krause A, et al. Lyme borreliosis: clinical case definitions for diagnosis and management in Europe. Clin Microbiol Infect. (2011) 17:69–79. doi: 10.1111/j.1469-0691.2010.03175.x
2. Mygland A, Ljostad U, Fingerle V, Rupprecht T, Schmutzhard E, Steiner I, et al. EFNS guidelines on the diagnosis and management of European Lyme neuroborreliosis. Eur J Neurol. (2010) 17:8–16. doi: 10.1111/j.1468-1331.2009.02862.x
3. National Institute for Health and Care Excellence. Lyme disease (NICE guideline NG95). (2018). Available online at: https://www.nice.org.uk/guidance/NG95 (accessed June 29, 2019).
4. Taba P, Schmutzhard E, Forsberg P, Lutsar I, Ljostad U, Mygland A, et al. EAN consensus review on prevention, diagnosis and management of tick-borne encephalitis. Eur J Neurol. (2017) 24:1214–e61. doi: 10.1111/ene.13356
5. Lantos PM, Rumbaugh J, Bockenstedt LK, Falck-Ytter YT, Aguero-Rosenfeld ME, Auwaerter PG, et al. Clinical practice guidelines by the Infectious Diseases Society of America (IDSA), American Academy of Neurology (AAN), and American College of Rheumatology (ACR), 2020 guidelines for the prevention, diagnosis and treatment of Lyme disease. Arthritis Rheumatol. (2021) 73:12–20. doi: 10.1002/art.41562
6. Severinsson K, Jaenson TG, Pettersson J, Falk K, Nilsson K. Detection and prevalence of Anaplasma phagocytophilum and Rickettsia Helvetica in Ixodes ricinus ticks in seven study areas in Sweden. Parasit Vectors. (2010) 3:66. doi: 10.1186/1756-3305-3-66
7. Henningsson AJ, Wilhelmsson P, Gyllemark P, Kozak M, Matussek A, Nyman D, et al. Low risk of seroconversion or clinical disease in humans after a bite by an Anaplasma phagocytophilum-infected tick. Ticks Tick Borne Dis. (2015) 6:787–92. doi: 10.1016/j.ttbdis.2015.07.005
8. Jaarsma RI, Sprong H, Takumi K, Kazimirova M, Silaghi C, Mysterud A, et al. Anaplasma phagocytophilum evolves in geographical and biotic niches of vertebrates and ticks. Parasit Vectors. (2019) 12:328. doi: 10.1186/s13071-019-3583-8
9. Wallménius K, Pettersson JHO, Jaenson TG, Nilsson K. Prevalence of Rickettsia spp., Anaplasma phagocytophilum, and Coxiella burnetii in adult Ixodes ricinus ticks from 29 study areas in central and southern Sweden. Ticks Tick Borne Dis. (2012) 3:100–6. doi: 10.1016/j.ttbdis.2011.11.003
10. Klitgaard K, Kjaer LJ, Isbrand A, Hansen MF, Bodker R. Multiple infections in questing nymphs and adult female Ixodes ricinus ticks collected in a recreational forest in Denmark. Ticks Tick Borne Dis. (2019) 10:1060–5. doi: 10.1016/j.ttbdis.2019.05.016
11. Andersson M, Bartkova S, Lindestad O, Raberg L. Co-infection with “Candidatus Neoehrlichia Mikurensis” and Borrelia afzelii in Ixodes ricinus ticks in southern Sweden. Vector Borne Zoonotic Dis. (2013) 13:438–42. doi: 10.1089/vbz.2012.1118
12. Kjelland V, Paulsen KM, Rollum R, Jenkins A, Stuen S, Soleng A, et al. Tick-borne encephalitis virus, Borrelia burgdorferi sensu lato, Borrelia miyamotoi, Anaplasma phagocytophilum and Candidatus Neoehrlichia mikurensis in Ixodes ricinus ticks collected from recreational islands in southern Norway. Ticks Tick Borne Dis. (2018) 9:1098–102. doi: 10.1016/j.ttbdis.2018.04.005
13. Larsson C, Hvidsten D, Stuen S, Henningsson AJ, Wilhelmsson P. “Candidatus Neoehrlichia mikurensis” in Ixodes ricinus ticks collected near the Arctic Circle in Norway. Parasit Vectors. (2018) 11:620. doi: 10.1186/s13071-018-3168-y
14. Karlsson ME, Andersson MO. Babesia species in questing Ixodes ricinus, Sweden. Ticks Tick Borne Dis. (2016) 7:10–2. doi: 10.1016/j.ttbdis.2015.07.016
15. Laaksonen M, Klemola T, Feuth E, Sormunen JJ, Puisto A, Makela S, et al. Tick-borne pathpgens in Finland: comparison of Ixodes ricinus and I. persulcatus in sympatric and parapatric areas. Parasit Vectors. (2018) 11:556. doi: 10.1186/s13071-018-3131-y
16. Wilhelmsson P, Fryland L, Borjesson S, Nordgren J, Bergstrom S, Ernerudh J, et al. Prevalence and diversity of Borrelia species in ticks that have bitten humans in Sweden. J Clin Microbiol. (2010) 48:4169–76. doi: 10.1128/JCM.01061-10
17. Kjelland V, Rollum R, Korslund L, Slettan A, Tveitnes D. Borrelia miyamotoi is widespread in Ixodes ricinus ticks in southern Norway. Tick Tick Borne Dis. (2015) 6:516–21. doi: 10.1016/j.ttbdis.2015.04.004
18. Sormunen JJ, Penttinen R, Klemola T, Hanninen J, Vuorinen I, Laaksonen M, et al. Tick-borne bacterial pathogens in southwestern Finland. Parasit Vectors. (2016) 9:168. doi: 10.1186/s13071-016-1449-x
19. Gehringer H, Schacht E, Maylaender N, Zeman E, Kaysser P, Oehme R, et al. Presence of an emerging subclone of Francisella tularensis holarctica in Ixodes ricinus ticks from south-western Germany. Ticks Tick Borne Dis. (2013) 4:93–100. doi: 10.1016/j.ttbdis.2012.09.001
20. Wittwer M, Altpeter E, Pilo P, Gygli SM, Beuret C, Foucault F, et al. Population genomics of Francisella tularensis subsp. holarctica and its implication on the eco-epidemiology of tularemia in Switzerland. Front Cell Infect Microbiol. (2018) 8:89. doi: 10.3389/fcimb.2018.00089
21. Tomaso H, Otto P, Peters M, Süss J, Karger A, Schamoni H, et al. Francisella tularensis and other bacteria in hares and ticks in North Rhine-Westphalia (Germany). Ticks Tick Borne Dis. (2018) 9:325–9. doi: 10.1016/j.ttbdis.2017.11.007
22. Schouls LM, van de Pol I, Rijpekema SG, Schot CS. Detection and identification of Ehrlichia, Borrelia burgdorferi sensu lato, and Bartonella species in Dutch Ixodes ricinus ticks. J Clin Microbiol. (1999) 37:2215–22. doi: 10.1128/JCM.37.7.2215-2222.1999
23. Podsiadly E, Chmielewski T, Sochon E, Tylewska-Wiertzbanovska S. Bartonella henselae in Ixodes ricinus ticks removed from dogs. Vector Borne Zoonotic Dis. (2007) 7:189–92. doi: 10.1089/vbz.2006.0587
24. Stensvold CR, Al Marai D, Andersen LO, Krogfelt KA, Jensen JS, Larsen KS, et al. Babesia spp. and other pathogens in ticks recovered from domestic dogs in Denmark. Parasit Vectors. (2015) 8:262. doi: 10.1186/s13071-015-0843-0
25. Bakken JS, Krueth J, Wilson-Nordskog C, Tilden RL, Asanovich K, Dumler JS. Clinical and laboratory characteristics of human granulocytic ehrlichiosis. JAMA. (1996) 275:199–205. doi: 10.1001/jama.1996.03530270039029
26. Bjoersdorff A, Berglund J, Kristiansen BE, Soderstrom C, Eliasson I. Varying clinical picture and course of human granulocytic ehrlichiosis. Twelve Scandinavian cases of the new tick-borne zoonosis are presented. Lakartidningen. (1999) 96:4200–4.
27. Uhnoo I, Cars O, Christensson D, Nystrom-Rosander C. First documented case of human babesiosis in Sweden. Scand J Infect Dis. (1992) 24:541–7. doi: 10.3109/00365549209052642
28. Haapasalo K, Suomalainen P, Sukura A, Siikamaki H, Jokiranta TS. Fatal babesiosis in man, Finland, 2004. Emerg Infect Dis. (2010) 16:1116–8. doi: 10.3201/eid1607.091905
29. Bläckberg J, Lazarevic VL, Hunfeld KP, Persson KEM. Low-virulent Babesia venatorum infection masquerading as hemophagocytic syndrome. Ann Hematol. (2018) 97:731–3. doi: 10.1007/s00277-017-3220-6
30. Krause PJ. Human babesiosis. Int J Parasitol. (2019) 49:165–74. doi: 10.1016/j.ijpara.2018.11.007
31. Hovius JW, de Wever B, Sohne M, Brouwer MC, Coumou J, Wagemakers A, et al. A case of meningoencephalitis by the relapsing fever spirochaete Borrelia miyamotoi in Europe. Lancet. (2013) 382:658. doi: 10.1016/S0140-6736(13)61644-X
32. Boden K, Lobenstein S, Hermann B, Margos G, Fingerle V. Borrelia miyamotoi-associated neuroborreliosis in immunocompromised person. Emerg Infect Dis. (2016) 22:1617–20. doi: 10.3201/eid2209.152034
33. Welinder-Olsson C, Kjellin E, Vaht K, Jacobsson S, Wenneras C. First case of human “Candidatus Neoehrlichia mikurensis” infection in a febrile patient with chronic lymphocytic leukemia. J Clin Microbiol. (2010) 48:1956–9. doi: 10.1128/JCM.02423-09
34. Nilsson K, Lindquist O, Pahlson C. Association of Rickettsia helvetica with chronic perimyocarditis in sudden cardiac death. Lancet. (1999) 354:1169–73. doi: 10.1016/S0140-6736(99)04093-3
35. Nilsson K, Elfving K, Pahlson C. Rickettsia helvetica in patient with meningitis, Sweden, 2006. Emerg Infect Dis. (2010) 16:490–2. doi: 10.3201/eid1603.090184
36. Wittesjo B, Bjoersdorff A, Eliasson I, Berglund J. First long-term study ofthe seroresponse to the agent of human granulocytic ehrlichiosis amongresidents of a tick-endemic area of Sweden. Eur J Clin Microbiol Infect Dis. (2001) 20:173–8. doi: 10.1007/s100960100463
37. Hunfeld KP, Lambert A, Kampen H, Albert S, Epe C, Brade V, et al. Seroprevalence of Babesia infections in humans exposed to ticks in midwestern Germany. J Clin Microbiol. (2002) 40:2431–6. doi: 10.1128/JCM.40.7.2431-2436.2002
38. Svensson J, Hunfeld KP, Persson KEM. High seroprevalence of Babesia antibodies among Borrelia burgdorferi-infected humans in Sweden. Ticks Tick Borne Dis. (2019) 10:186–90. doi: 10.1016/j.ttbdis.2018.10.007
39. Jahfari S, Herremans T, Platonov AE, Kuiper H, Karan LS, Vasilieva O, et al. High seroprevalence of Borrelia miyamotoi antibodies in forestry workers and individuals suspected of human granulocytic anaplasmosis in the Netherlands. New Microbes New Infect. (2014) 2:144–9. doi: 10.1002/nmi2.59
40. Rigaud E, Jaulhac B, Garcia-Bonnet N, Hunfeld KP, Féménia F, Huet D, et al. Seroprevalence of seven pathogens transmitted by the Ixodes ricinus tick in forestry workers in France. Clin Microbiol Infect. (2016) 22:735.e1-9. doi: 10.1016/j.cmi.2016.05.014
41. McGill S, Wesslén L, Hjelm E, Holmberg M, Auvinen MK, Berggren K, et al. Bartonella spp. seroprevalence in healthy Swedish blood donors. Scand J Infect Dis. (2005) 37:723–30. doi: 10.1080/00365540510012152
42. Welc-Faleciak R, Siński E, Kowalec M, Zajkowska J, Pancewicz SA. Asymptomatic “Candidatus Neoehrlichia mikurensis” infections in immunocompetent humans. J Clin Microbiol. (2014) 52:3072–4. doi: 10.1128/JCM.00741-14
43. Rossow H, Ollgren J, Hytonen J, Rissanen H, Huitu O, Henttonen H, et al. Incidence and seroprevalence of tularaemia in Finland, 1995 to 2013: regional epidemics with cyclic pattern. Euro Surveill. (2015) 20:21209. doi: 10.2807/1560-7917.ES2015.20.33.21209
44. Nielsen H, Fournier PE, Pedersen IS, Krarup H, Ejlertsen T, Raoult D. Serological and molecular evidence of rickettsia helvetica in Denmark. Scand J Infect Dis. (2004) 36:559–63. doi: 10.1080/00365540410020776
45. Elfving K, Lindblom A, Nilsson K. Seroprevalence of Rickettsia spp. infection among tick-bitten patients and blood donors in Sweden. Scand J Infect Dis. (2008) 40:74–7. doi: 10.1080/00365540701509907
46. Karlsson U, Bjoersdorff A, Massung RF, Christensson B. Human granulocytic ehrlichiosis - a clinical case in Scandinavia. Scand J Infect Dis. (2001) 33:73–4. doi: 10.1080/003655401750064130
47. Moniuszko-Malinowska A, Swiecicka I, Dunaj J, Zajkowska J, Czupryna P, Zambrowski G, et al. Infection with Babesia microti in humans with non-specific symptoms in North East Poland. Infect Dis. (2016) 48:537–43. doi: 10.3109/23744235.2016.1164339
48. Hoornstra D, Koetsveld J, Sprong H, Platonov AE, Hovius JW. Borrelia miyamotoi disease in an immunocompetent patient, Western Europe. Emerg Infect Dis. (2018) 24:1770–2. doi: 10.3201/eid2409.180806
49. Platonov AE, Karan LS, Kolyasnikova NM, Makhneva NA, Toporkova MG, Maleev VV, et al. Humans infected with relapsing fever spirochete Borrelia miyamotoi, Russia. Emerg Infect Dis. (2011) 17:1816–23. doi: 10.3201/eid1710.101474
50. Henningsson AJ, Asgeirsson H, Hammas B, Karlsson E, Parke Å, Hoornstra D, et al. Two cases of Borrelia miyamotoi meningitis, Sweden, 2018. Emerg Infect Dis. (2019) 25:1965–8. doi: 10.3201/eid2510.190416
51. Grankvist A, Sandelin LL, Andersson J, Fryland L, Wilhelmsson P, Lindgren PE, et al. Infections with candidatus neoehrlichia mikurensis and cytokine responses in 2 persons bitten by ticks, Sweden. Emerg Infect Dis. (2015) 21:1462–5. doi: 10.3201/eid2108.150060
52. Quarsten H, Grankvist A, Høyvoll L, Myre IB, Skarpaas T, Kjelland V, et al. Candidatus Neoehrlichia mikurensis and Borrelia burgdorferi sensu lato detected in the blood of Norwegian patients with erythema migrans. Ticks Tick Borne Dis. (2017) 8:715–20. doi: 10.1016/j.ttbdis.2017.05.004
53. Borde JP, Zange S, Antwerpen MH, Georgi E, von Buttlar H, Kern WV, et al. Five cases of vector-borne Francisella tularensis holarctica infections in south-western Germany. Ticks Tick Borne Dis. (2017) 8:808–12. doi: 10.1016/j.ttbdis.2017.06.009
54. Lindblom A, Wallménius K, Sjowall J, Fryland L, Wilhelmsson P, Lindgren PE, et al. Prevalence of Rickettsia spp. in ticks and serological and clinical outcomes in tick-bitten individuals in Sweden and on the Aland Islands. PLoS ONE. (2016) 11:e0166653. doi: 10.1371/journal.pone.0166653
55. Swanson SJ, Neitzel D, Reed KD, Belongia EA. Coinfections acquired from Ixodes ticks. Clin Microbiol Rev. (2006) 19:798–27. doi: 10.1128/CMR.00011-06
56. Lotric-Furlan S, Petrovec M, Avsic-Zupanc T, Nicholson WL, Sumner JW, Childs JE, et al. Prospective assessment of the etiology of acute febrile illness after a tick-bite in Slovenia. Clin Infect Dis. (2001) 33:503–10. doi: 10.1086/322586
57. Moniuszko A, Dunaj J, Swiecicka I, Zambrowski G, Chmielewska-Badora J, Zukiewicz-Sobczak W, et al. Co-infections with Borrelia species, Anaplasma phagocytophilum and Babesia spp. in patients with tick-borne encephalitis. Eur J Clin Microbiol Infect Dis. (2014) 33:1835–41. doi: 10.1007/s10096-014-2134-7
58. Moher D, Shamseer L, Clarke M, Ghersi D, Liberati A, Petticrew M, et al. Preferred reporting items for systematic reviews and meta-analyses protocols (PRISMA-P) 2015 statement. Syst Rev. (2015) 4:1. doi: 10.1186/2046-4053-4-1
59. Kirkehei I, Flottorp S, Aaberge I, Aase A. Laboratory Diagnosis of Tick-Borne Infections: A Systematic Literature Search With a Sorted Reference List. [Laboratoriadiagnostikk ved flåttbårne infeksjoner: Systematisk litteratursøk med sortering]. Oslo: Norwegian Institute of Public Health (2019).
60. Covidence. World-Class Systematic Review Management. (2018) Available online at: https://www.covidence.org/
61. Whiting P, Rutjes AW, Reitsma JB, Bossuyt PM, Kleijnen J. The development of QUADAS: a tool for the quality assessment of studies of diagnostic accuracy included in systematic reviews. BMC Med Res Methodol. (2003) 3:25. doi: 10.1186/1471-2288-3-25
62. Shea BJ, Grimshaw JM, Wells GA, Boers M, Andersson N, Hamel C, et al. Development of AMSTAR: a measurement tool to assess the methodological quality of systematic reviews. BMC Med Res Methodol. (2007) 7:10. doi: 10.1186/1471-2288-7-10
63. Matei AI, Estrada-Pena A, Cutler SJ, Vayssier-Taussat M, Varela-Castro L, Potkonjak A, et al. A review of the eco-epidemiology and clinical management of human granulocytic anaplasmosis and its agent in Europe. Parasit Vectors. (2019) 12:599. doi: 10.1186/s13071-019-3852-6
64. Brouqui P, Bacellar R, Baranton G, Birtles RJ, Bjoersdorff A, Blanco JR, et al. Guidelines for the diagnosis of tick-borne diseases in Europe. Clin Microbiol Infect. (2004) 10:1108–32. doi: 10.1111/j.1469-0691.2004.01019.x
65. Paris DH, Dumler JS. State of the art of diagnosis of rickettsial diseases: the use of blood specimens for diagnosis of scrub typhus, spotted fever group rickettsioses, murine typhus. Curr Opin Infect Dis. (2016) 29:433–9. doi: 10.1097/QCO.0000000000000298
66. Bechah Y, Socolovschi C, Raoult D. Identification of rickettsial infections by using cutaneous swab specimens and PCR. Emerg Inf Dis. (2011) 17:83–6. doi: 10.3201/eid1701.100854
67. Gugliotta JL, Goethert HK, Berardi VP, Telford SR. Meningoencephalitis from Borrelia miyamotoi in an immunocompromised patient. N Engl J Med. (2013) 368:240–5. doi: 10.1056/NEJMoa1209039
68. Sato K, Takano A, Konnai S, Nakao M, Ito T, Koyama K, et al. Human infections with Borrelia miyamotoi, Japan. Emerg Infect Dis. (2014) 20:1391–3. doi: 10.3201/eid2008.131761
69. Cutler S, Vayssier-Taussat M, Estrada-Pena A, Potkonjak A, Mihalca AD, Zeller H. A new Borrelia on the block: Borrelia miyamotoi - a human health risk? Euro Surveill. (2019) 24:1800170. doi: 10.2807/1560-7917.ES.2019.24.18.1800170
70. Karan L, Makenov M, Kolyasnikova N, Stukolova O, Toporkova M, Olenkova O. Dynamics of spirochetemia and early PCR detection of Borrelia miyamotoi. Emerg Infect Dis. (2018) 24:860–7. doi: 10.3201/eid2405.170829
71. Franck M, Ghozzi R, Pajaud J, Lawson-Hogban NE, Mas M, Lacout A, et al. Borrelia miyamotoi: 43 cases diagnosed in France by real-time PCR in patients with persistent polymorphic signs and symptoms. Front Med. (2020) 7:55. doi: 10.3389/fmed.2020.586694
72. Molloy PJ, Telford SR, Chowdri HR, Lepore TJ, Gugliotta JL, Weeks KE, et al. Borrelia miyamotoi disease in the Northeastern United States: a case series. Ann Intern Med. (2015) 163:91–8. doi: 10.7326/M15-0333
73. Koetsveld J, Kolyasnikova NM, Wagemakers A, Stukolova OA, Hoornstra D, Sarksyan DS, et al. Serodiagnosis of Borrelia miyamotoi disease by measuring anitbodies against GlpQ and variable major proteins. Clin Microbiol Infect. (2018) 24:1338.e1–1338.e7. doi: 10.1016/j.cmi.2018.03.009
74. Zellner B, Huntley JF. Ticks and Tularemia: Do We Know What We Don't Know? Front Cell Infect Microbiol. (2019) 9:146. doi: 10.3389/fcimb.2019.00146
75. Mailles A, Vaillant V. 10 years of surveillance of human tularaemia in France. Euro Surveill. (2014) 19:20956. doi: 10.2807/1560-7917.ES2014.19.45.20956
76. Haulrig MB, Mathiasen G, Nielsen RM, Kromann CB, Krogfelt KA, Wiese L. Two cases of tick-borne transmitted tularemia on Southern Zealand, Denmark. APMI. (2020) 128:61–4. doi: 10.1111/apm.13008
77. Dietrich F, Schmidgen T, Maggi RG, Richter D, Matuschka FR, Vonthein R, et al. Prevalence of Bartonella henselae and Borrelia burgdorferi sensu lato DNA in Ixodes ricinus ticks in Europe. Appl Environment Microbiol. (2010) 76:1395–8. doi: 10.1128/AEM.02788-09
78. Zajac V, Wójcik-Fatla A, Dutkiewicz J, Szymańska J. Bartonella henselae in eastern Poland: the relationship between tick infection rates and the serological response of individuals occupationally exposed to tick bites. J Vector Ecol. (2015) 40:75–82. doi: 10.1111/jvec.12135
79. Müller A, Reiter M, Schötta AM, Stockinger H, Stanek G. Detection of Bartonella spp. in Ixodes ricinus ticks and Bartonella seroprevalence in human populations. Ticks Tick Borne Dis. (2016) 7:763–7. doi: 10.1016/j.ttbdis.2016.03.009
80. Telford SR, Wormser GP. Bartonella spp. transmission by ticks not established. Emerg Infect Dis. (2010) 16:379–84. doi: 10.3201/eid1603.090443
81. Chmielewska-Badora J, Moniuszko A, Sobczak W, Zwoliński J, Piatek J, Pancewicz S. Serological survey in persons occupationally exposed to tick-borne pathogens in cases of co-infections with Borrelia burgdorferi, Anaplasma phagocytophilum, Bartonella spp. and Babesia microti. Ann Agric Environ Med. (2012) 19:271–4.
82. Dersch R, Sommer H, Rauer S, Meerpohl JJ. Prevalence and spectrum of residual symptoms in Lyme neuroborreliosis after pharmacological treatment: a systematic review. J Neurol. (2016) 263:17–24. doi: 10.1007/s00415-015-7923-0
83. Lacout A, El Hajjam M, Marcy PY, Perronne C. The persistent Lyme disease: “Tre chronic Lyme disease” rather than “Post-treatment Lyme disease syndrome”. J Glob Infect Dis. (2018) 10:170–1. doi: 10.4103/jgid.jgid_152_17
84. Nemeth J, Bernasconi E, Heininger U, Abbas U, Nadal D, Strahm C, et al. Update of the Swiss guidelines on post-treatment Lyme disease syndrome. Swiss Med Wkly. (2016) 146:w14353. doi: 10.4414/smw.2016.14353
85. Wormser GP, Dattwyler RJ, Shapiro ED, Halperin JJ, Steere AC, Klempner MS, et al. The clinical assessment, treatment, and prevention of Lyme disease, human granulocytic anaplasmosis, and babesiosis: clinical practice guidelines by the Infectious Diseases Society of America. Clin Infect Dis. (2006) 43:1089–134. doi: 10.1086/508667
Keywords: systematic review, tick-borne infections, co-infections, human, laboratory, diagnostic, clinical evaluation
Citation: Henningsson AJ, Aase A, Bavelaar H, Flottorp S, Forsberg P, Kirkehei I, Lövmar M, Nilsson K, Nyman D, Ornstein K, Sjöwall J, Skogman BH, Tjernberg I and Aaberge I (2021) Laboratory Methods for Detection of Infectious Agents and Serological Response in Humans With Tick-Borne Infections: A Systematic Review of Evaluations Based on Clinical Patient Samples. Front. Public Health 9:580102. doi: 10.3389/fpubh.2021.580102
Received: 08 July 2020; Accepted: 20 August 2021;
Published: 20 September 2021.
Edited by:
Marc Jean Struelens, Université libre de Bruxelles, BelgiumReviewed by:
Christian Perronne, Assistance Publique Hopitaux De Paris, FranceCopyright © 2021 Henningsson, Aase, Bavelaar, Flottorp, Forsberg, Kirkehei, Lövmar, Nilsson, Nyman, Ornstein, Sjöwall, Skogman, Tjernberg and Aaberge. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Anna J. Henningsson, YW5uYS5qb25zc29uLmhlbm5pbmdzc29uQHJqbC5zZQ==
†Members of the ESCMID Study Group for Lyme Borreliosis—ESGBOR, part of the European Society for Clinical Microbiology and Infectious Diseases
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.