
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health , 11 December 2020
Sec. Life-Course Epidemiology and Social Inequalities in Health
Volume 8 - 2020 | https://doi.org/10.3389/fpubh.2020.604385
This article is part of the Research Topic Social Inequality in Cancer Screening View all 5 articles
 M. Solís-Ibinagagoitia1
M. Solís-Ibinagagoitia1 S. Unanue-Arza2
S. Unanue-Arza2 M. Díaz-Seoane3
M. Díaz-Seoane3 L. Martínez-Indart1
L. Martínez-Indart1 A. Lebeña-Maluf1I. Idigoras1,4I. Bilbao4
A. Lebeña-Maluf1I. Idigoras1,4I. Bilbao4 I. Portillo1,4*
I. Portillo1,4*Background: Despite the high participation rates in the Basque Country, colorectal cancer screening programme (Spain), there is still a part of the population that has never participated. Since it is essential to ensure equal access to health services, it is necessary to identify the determinants of health and socio-economic factors related to non-participation in the screening programme.
Methods: Cross sectional descriptive study including all invited population in a complete round between 2015 and the first trimester of 2017. Health risk factors available in medical records and their control have been analyzed using univariate and multivariate analyses.
Results: 515,388 people were invited at the programme with a 71.9% of fecal immunochemical test participation rate. Factors that increase the risk of non-participation are: being men (OR = 1.10, 95% CI 1.09–1.12); younger than 60 (OR = 1.18, 95% CI 1.17–1.20); smoker (OR = 1.20, 95% CI 1.18–1.22); hypertensive (OR = 1.14, 95% CI 1.12–1.15) and diabetic (OR = 1.40, 95% CI 1.36–1.43); having severe comorbidity (OR = 2.09, 95% CI 2.00–2.19) and very high deprivation (OR = 1.15, 95% CI 1.12–1.17), as well as making <6 appointments to Primary Care in 3 years (OR = 2.39, 95% CI 2.33–2.45). Still, the area under the curve (AUC) indicates that there are more factors related to non-participation.
Conclusions: The participation in the Basque Country colorectal cancer-screening Programme is related to some risk factors controlled by Primary Care among others. Therefore, the involvement of these professionals could improve, not only the adherence to the CRC screening, but also other health styles and preventive interventions.
After 10 years of implementation, the Bowel Cancer Screening Programme (BCSP) of the Basque Country has progressively achieved a significant increase in participation, from 58.1% in 2009 to 72.3% in 2017 surpassing European Guidelines recommendations (65%) (1, 2). Literature suggests that high levels of regular participation are required for screening programmes to be effective (3–6).
The BCSP is based on Primary Health Care (PHC), where most of the preventive and health promotion activities are carried out. A full description of this programme can be found as reported by Portillo et al. (7).
The main results after the first invitation indicate higher colorectal cancer (CRC) detection; however, the incidence has been progressively descending over time according with successive rounds participation. In addition, more than 70% of the cancerous lesions detected by screening were in earlier stages (I and II) than CRC detected in non-participants and survival at 5 years was significantly higher (90.1 vs. 60.5%) (3).
Despite our high participation rate, there are people who having been invited by the programme have never participated, even though all the process is completely free of charge without appointment to get and drop off the screening test. CRC screening participation could be influenced by several factors (socio-economic factors, lifestyles, comorbidities, health preventive actions...). Some of these factors may be related to the determinants of health or to the relationship that the population has with the health system. Therefore, knowledge of determinants of health inequality involved is necessary to address the problem.
Some of the socio-economic factors that could be related to participation have been studied in the literature. Regarding sex, data show consistently lower levels of participation in men than in women (5), even though advanced adenoma and CRC detection rates are higher in men (8–11). Moreover, the benefits of participation increase in men showing a pronounced decrease in mortality (4.3% in men vs. 1.9% in women) (1, 3).
Furthermore, according to the European Code Against Cancer, there are behaviors that help reduce the risk of developing cancer such as not smoking, reducing alcohol consumption, exercising, and eating healthy (12). Despite this, the literature studying the relationship between these factors and non-participation is scarce, as it focuses mainly on socio-economic inequalities (13).
The aim of the present study is to identify socio-demographic and lifestyle factors related to non-participation in the CRC Screening Programme of the Basque Country (Spain).
A cross sectional descriptive study was conducted between May and June 2019. The CRC screening programme of the Basque Country procedures consists of an immunochemical test [fecal occult blood test (FOBT), OC-Sensor®] every 2 years, followed by a colonoscopy under deep sedation in positive cases as confirmatory test (≥20 μg hemoglobin/g feces).
All invited population between 2015 and the first trimester of 2017 was included, covering the target population between 50 and 69 years of age in the Basque Country (a complete round). Persons were totally excluded if they had previously been diagnosed with a CRC, or temporarily excluded if a colonoscopy was performed in the last 5 years. People with unknown addresses were considered invalid invitees. Finally, 515,388 people were invited appropriately.
Based on the literature, age, sex, smoking, and obesity (before the invitation) were considered risk factors for development of CRC (14) and diabetes mellitus and arterial hypertension as prevalent chronic conditions. Sex, not gender, was considered due to available data from medical records.
Furthermore, we also included the use of the health services [any type of general practitioner (GP) or nurse consultation apart from those for administrative purposes], participation in preventive activities (influenza vaccine), control of certain risk factors (diabetes, obesity, and arterial hypertension) by PHC following a protocol. Comorbidity and deprivation indexes were calculated using five socio-economic indicators selected from each small area: unemployment, insufficient instruction, insufficient instruction in young people, manual workers, and temporary wage-earners (see Additional File 1 in Supplementary Material) (15, 16). The sample population was also categorized into five groups according to their participation in previous rounds.
The variables were categorized as shown in the Additional File 2 (Supplementary Material).
Non-participation was considered the main outcome in this study. An invited person was considered non-participant if they did not have an FOBT valid result. If the FOBT result was erroneous and no other valid sample had been delivered, it was also considered a non-participant. The database was cleaned eliminating duplicates, leaving us only with the last invitation.
After that, if the result of the FOBT was positive, the adherence of a consequent colonoscopy or another complementary imaging test is required. This variable was measured taking into account that a person with a positive FOBT has subsequently undergone a colonoscopy or conclusive alternative test, so that the quality of the preparation is adequate and the entire colon is observed until cecum. Lesions detected in colonoscopy are coded following the European Guidelines as normal (including hyperplastic polyps), low risk adenoma (LRA), medium risk adenoma (MRA), high-risk adenoma (HRA), other intestinal pathologies, and CRC (2). The most severe result was considered for each participant. Quality indicators and complications on the colonoscopy are described as well.
Information was obtained from the Basque Country BCSP Database, which has a system of encryption and access in accordance with the current data protection laws, and standardized medical record (Osabide), that belongs to the Basque Health Service (Osakidetza) and permits an effective coordination between PHC and specialized care. Moreover, PHC has some specific facilities included in the medical record to prioritize the detection and control of risk factors and follow-up preventive interventions such as diabetes, hypertension, tobacco consumption, alcohol, and obesity among others (17). All data were systematically anonymized for analysis and subsequent publication.
The study population was described using frequencies and percentages for categorical variables and means and standard deviations (SDs) for continuous variables. For categorical variables, χ2-test was used or Fisher's test when the expected frequencies were <5. Univariate and multivariate logistic regression were conducted to estimate Odds Ratios (ORs) with 95% confidence intervals (CIs), considering statistical significance at the 5% level (p ≤ 0.05). Models were systematically adjusted by sex. Discrimination was measured by the area under the receiver operating characteristic curve (AUC).
In addition, each subpopulation with the risk factor (hypertensive, obese, and diabetic) was considered and checked to see if the control of this factor influences non-participation. The same was done with participation in other preventive activities measured by flu vaccination in ≥65-year olds for whom it is recommended.
If a patient had not visited a GP or nurse in the last 3 years, the absence of information in certain variables (tobacco consumption, arterial hypertension, diabetes, and obesity) was considered as missing data and it was excluded from the analysis.
The analysis was carried out using the statistical program SPSS 23.0, IBM (Armonk, New York, USA).
515,388 people were invited in the study period. The participation rate was 71.9% (74.1% women, 69.4% men), 5.3% were positive and the adherence for colonoscopy was 93.8%. A flow-chart with all details is shown in Additional File 3 (Supplementary Material).
The invited people were 52% women and their mean age was 58.7 (SD = 5.8). The characteristics of the invited population by sex are shown in Table 1. Non-participation levels were significantly higher in men than in women (30.6 vs. 25.9%) as well as advanced adenomas (44 vs. 26.2%) and carcinoma findings (4.6 vs. 3.5%). About half of the population was a regular participant (53.2%). However, a 23.1% of people had never participated (women 22%, men 26.7%).
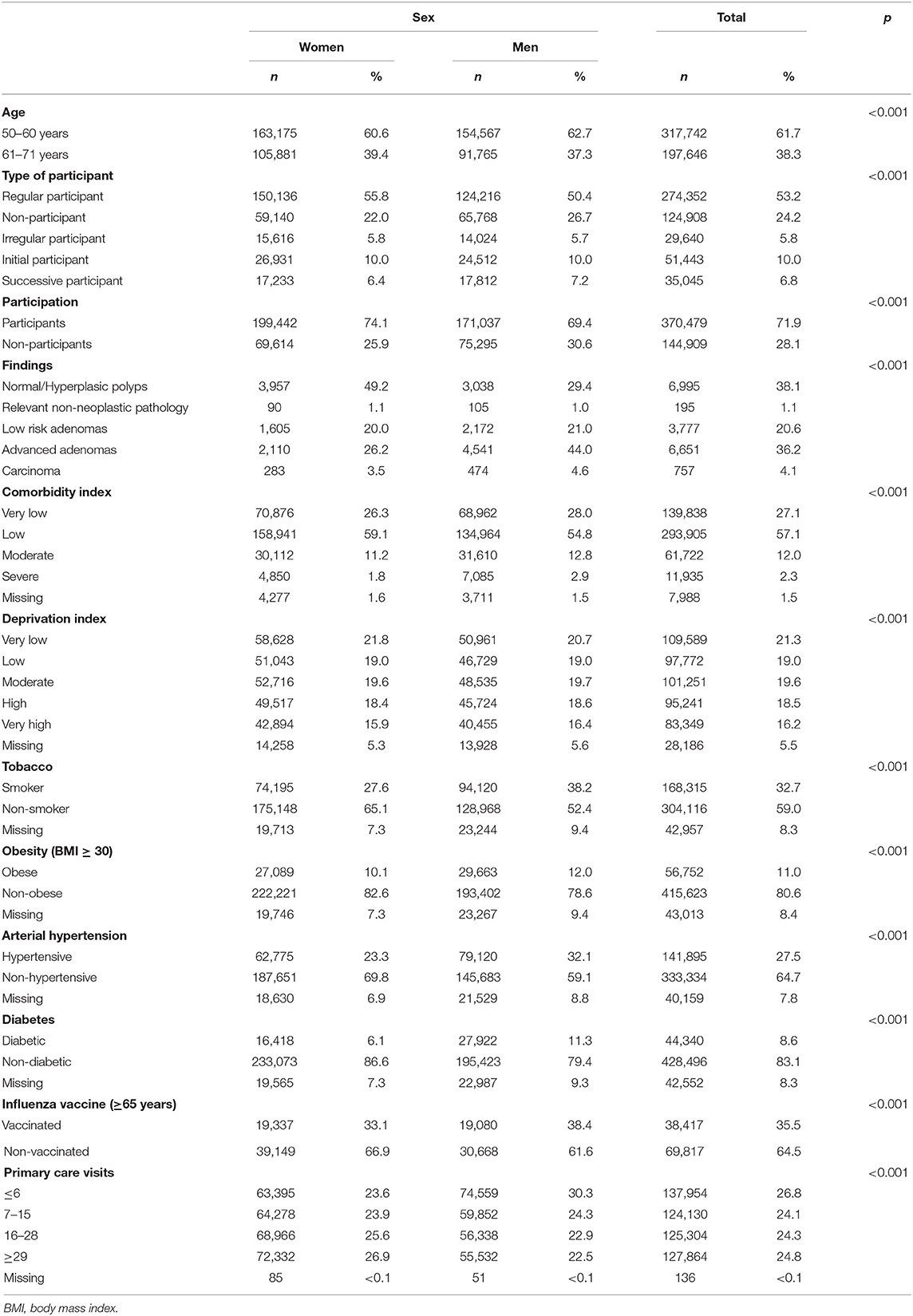
Table 1. Characteristics of the invited population for CRC screening program by sex.
In terms of health risk factors of the invited population, we observed that men had a higher proportion of smokers (38.2 vs. 27.6%), obese (12.0 vs. 10.1%), hypertensive (32.1 vs. 23.3%), and diabetics (11.3 vs. 6.1%) than women. However, men use less PHC services than women, in fact, 45.4% of men visit PHC 16 times or more, compared to 52.5% of women. On the contrary, influenza vaccination was superior in men (38.4 vs. 33.1%).
A multivariate analysis was performed including the previously mentioned statistically significant variables in the univariate analysis. First, it was made with all the population and then the disaggregated analysis by sex was repeated. The results of global analysis are shown in Table 2. Regarding the analysis by sex the results showed the same trend as the global analysis, except obesity that shows to be protective in men (OR = 0.96, 95% CI 0.93–0.99, p = 0.015) (see Additional File 4 in Supplementary Material).
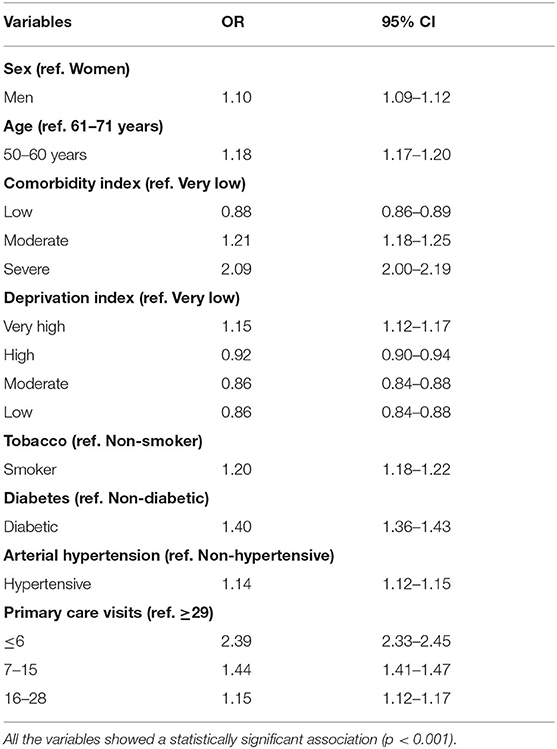
Table 2. Multivariate logistic regression.
Adjusting for the other variables, men were more likely not to participate in the screening programme (OR = 1.10, 95% CI 1.09–1.12). With regard to age, it was observed that people in the younger group have a higher risk of not participating than those older than 60 years old (OR = 1.18, 95% CI 1.17–1.20). When it comes to lifestyle, smokers are also at greater risk (OR = 1.20, 95% CI 1.18–1.22). Having hypertension (OR = 1.14, 95% CI 1.12–1.15) or diabetes (OR = 1.40, 95% CI 1.36–1.43) means an increase in the probability of not participating.
Comorbidity and deprivation index as well as PHC visits were classified in more than two categories and are represented in Figure 1. Studying comorbidity index, the risk of non-participation increased as the index descended, and this drop was more pronounced in both moderate to severe. Deprivation index showed the same trend but the differences between categories were slighter. After a slight decrease in the risk of non-participation of those who have a low deprivation with respect to those who have a very low index, the risk increases as the deprivation index increases.
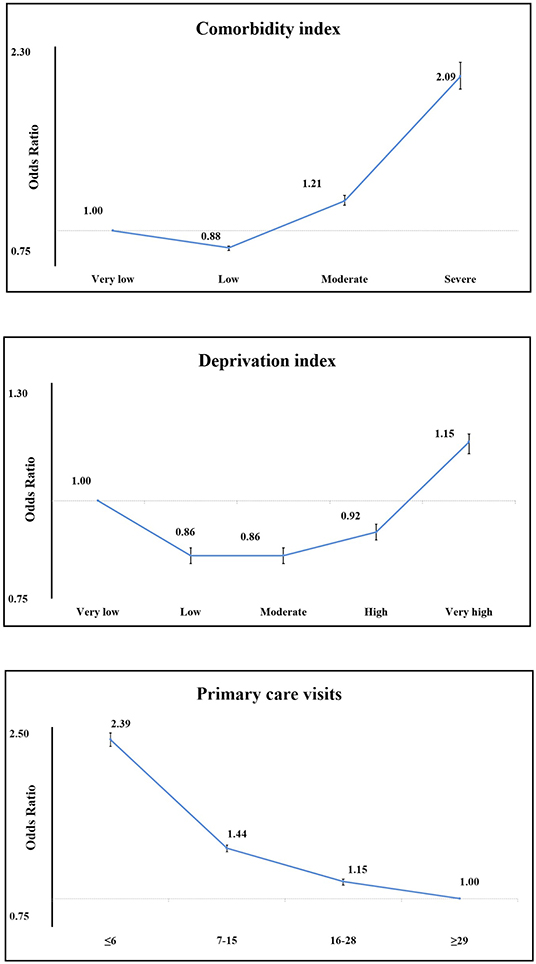
Figure 1. ORs for non-participation in CRC screening by comorbidity, deprivation index, and PHC visits.
Finally, PHC visits reflected a marked gradient (Figure 1), so that the group of the least number of visits (≤6 visits) had double the risk of not participating (OR = 2.4, 95% CI 2.33–2.45) in comparison to the reference category (≥29).
The area under the curve was 0.611 (95% CI 0.609–0.613, p < 0.001).
Another analysis was performed on subpopulations that presented each risk factor or preventive activity studied (Table 3). The results showed that people with inadequate control of these risk factors or non-participation in preventive activities have an increased risk of not participating in the screening.
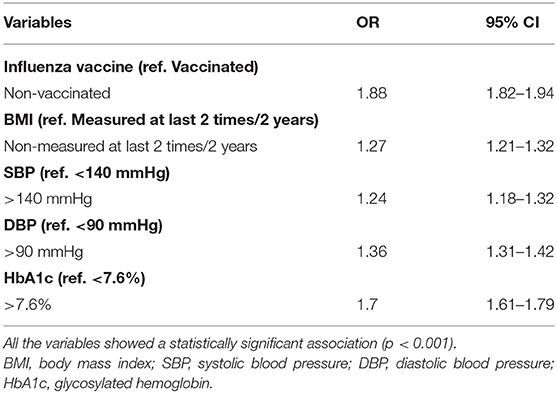
Table 3. Sub-analysis (univariate) of risk factors control.
First, the hypertensive with a systolic blood pressure (SBP) higher than 140 mmHg have a 24% higher risk of not participating (OR = 1.24, 95% CI 1.18–1.32) and those with a diastolic blood pressure (DBP) higher than 90 mmHg have a 36% increased risk of not participating (OR = 1.36, 95% CI 1.31–1.42).
For diabetics, having a Hemoglobin A1c (HbA1c) level higher than 7.6% increased the risk of not participating by 70% (OR = 1.7, 95% CI 1.61–1.79).
Among obese people, we observed that not having at least two body mass index (BMI) measurements in the last 2 years increases the risk of non-participation by 27% (OR = 1.27, 95% CI 1.21–1.32). Finally, in subjects over 65 years old who are recommended for influenza vaccination, the risk of not participating was 88% higher in non-vaccinated people (OR = 1.8, 95% CI 1.82–1.94). All the results were statistically significant (p < 0.001).
Sex must be considered as one of the main factors that can determine participation in cancer screening programmes. It has been widely studied, and our results agree with a vast majority of studies that have evidenced that participation in CRC screening programmes around the world is greater in women than in men (18–23).
The literature suggests that men may have worse self-care awareness, which could be reflected by being less active in preventive activities or taking care of themselves (24). This could be explained by the fact that traditional models of masculinity have a higher risk of not participating in CRC screening (25–27). In addition, men are at greater risk of developing CRC so they represent a sector of the population to be taken into consideration in screening. In this study we have seen that older men have a lower risk of not participating. According to Moss et al., one explanation could be that screening becomes more acceptable in successive rounds, which reduced the differences in participation between the sexes in their study (28).
On the other hand, both the comorbidity index and the deprivation index are also important factors to consider. Hall et al. (2013) concluded in a qualitative study that having other health problems is a barrier to participating, as participation in screening is not a priority, due to the fact that they do not consider the risk of cancer in the moment they are invited (29). Probably it may be due to their serious health status that they not consider participating (29, 30). However, van Dam et al. reported that worse physical health reduces the possibility of non-participation due to high use of the health system (31). Moreover, in this relation it is necessary to emphasize that the risk of non-participation of those who had a very low index—those with less comorbidity—was slightly higher than those with a low index. Perhaps because the perception of a healthy status may cause individuals to underestimate the risk of becoming ill and consequently they do not take the test, which is also shown in other studies (32).
Deprivation index shows a similar trend to the comorbidity index, thus the groups of very low and very high deprivation index have the highest risk of non-participation. In the Basque Country, people with a high socio-economic status usually have access to and use private health insurance, even with a health system that provides universal coverage. This could mean that many of these people are being screened outside the public system (33) and they may also have the perception of a lower risk of cancer. On the contrary, those with a high level of deprivation could be focused on problems arising from a precarious situation or have personal difficulties to deliver the sample (34–36). In fact, Dawidowicz et al. found a strong association between social deprivation and non-participation (37).
Furthermore, the relationship between a high deprivation index and an unhealthy lifestyle has been demonstrated, which causes a major proportion of individuals with health risk factors (38) like smoking (39, 40), obesity (41, 42), or diabetes (43–45).
Finally, missing values correspond to people who have not visited the health system in the last 3 years before the invitation, so we were not able to register this data. Nevertheless, this exclusion was random, so there is no bias in the analysis and it does not affect the results.
The sample size is the main strength of our study. Literature that relates health risk factors to non-participation in screening is scarce. Our study is novel because we are not aware of any study that analyses the influence of the control of these factors. For this reason, subsequent studies and design interventions are needed in this area.
Besides, the main limitation of this study could be that well-known health risk factors such as alcohol consumption or an unhealthy diet have not been included as they are not properly registered in the medical records. Moreover, isolation and unwanted loneliness is another factor that we have not been able to register and may encourage non-participation. Probably the value of the area under the curve was insufficient because there must be more factors that we have not analyzed in this study that influence non-participation and they should be explored in future. In addition to this, comparing participation in CRC screening with breast and cervix screening programmes has not been possible. With regard to gender, it has not been possible to analyze its relationship with non-participation because both medical records and most of the literature consider only sex although “gender” and “sex” are commonly used equally when they are not really equivalent. In future, it would be interesting to take gender into account when analyzing people's behavior and its effect on their health.
Adherence to colonoscopy has not been addressed in this study because the factors involved could be widely different. Further investigation in this area is needed.
To conclude, it can be said that PHC has an important role in health prevention, promotion, and control of risk factors. Encouraging PHC to take part by actively giving advice for CRC screening can lead to an increase in participation.
Being men, young, smoker, diabetic, hypertensive, or under-frequented in PHC increases the risk of being a non-participant in the Basque Country's CRC screening programme. Having poor control of health risk factors, or not actively taking part in preventive activities further increases the chances of not participating.
Non-statistically significant sex differences have been observed in factors affecting non-participation, except for obesity. Non-obese men are at higher risk of not participating than those who are obese.
A higher index of deprivation increases the risk of non-participation. However, people with the lowest deprivation also have high non-participation rates. This implies a social inequality that needs to be considered and that probably requires affirmative action measures.
PHC is a basic pillar when it comes to improving the recruitment of people who do not participate in CRC screening. Higher involvement of PHC would be necessary.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethical approval for this study was obtained (08/08/2018) from the Research with Drugs Ethics Committee of the Basque Country (CEIm).
SU-A, II, IB, and IP were involved in the conception and design of the study. MS-I, LM-I, AL-M, and IP collected the data, MS-I, AL-M, LM-I, and IP performed the analysis. MS-I, SU-A, MD-S, and IP were primarily involved in the drafting of the manuscript. All authors participated in the interpretation of the results of this study. All authors reviewed and approved the final version of the submitted manuscript.
This study is funded by the Health Department of the Basque Government (Spain) (Internal code: 2017111126). SU-A has received funding from the Department of Education of the Basque Government through the Consolidated Research Group MATHMODE (IT1294-19).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
DESBERDINAK GROUP: Isabel Mosquera, Amaia Bacigalupe, Unai Martín, Nere Mendizabal, Montse Calvo, Eunate Arana-Arri, Jose Luis Hurtado, Jose Luis Bilbao, Maria Luz Jauregui, Edurne Marañon, Natale Imaz, Josebe Fernández-Landa, Elena Aldasoro, Erika Valero.
The collaborators involved in the study belong to the Basque Health Service and the Basque University, also the authorities of the Basque Government by their commitment with the inequalities reduction.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2020.604385/full#supplementary-material
AUC, area under the receiver operating characteristic curve; BCSP, Bowel Cancer Screening Programme; BMI, body mass index; CI, Confidence interval; CRC, colorectal cancer; DBP, diastolic blood pressure; FOBT, fecal occult blood test; GP, general practitioner; HbA1c, Hemoglobin A1c; HRA, high-risk adenoma; LRA, low risk adenoma; MRA, medium risk adenoma; OR, Odds Ratio; PHC, Primary Health Care; SBP, systolic blood pressure; SD, Standard deviation.
1. Idigoras I, Arrospide A, Portillo I, Arana-Arri E, Martínez-Indart L, Mar J, et al. Evaluation of the colorectal cancer screening Programme in the Basque Country (Spain) and its effectiveness based on the Miscan-colon model. BMC Public Health. (2017) 18:1. doi: 10.1186/s12889-017-4639-3
2. Segnan N, Patnick J, Karsa L Von. European Guidelines for Quality Assurance in Colorectal Cancer Screening. 1st ed. Luxembourg: Publications Office of the European Union (2010).
3. Idigoras Rubio I, Arana-Arri E, Portillo Villares I, Bilbao Iturribarrria I, Martínez-Indart L, Imaz-Ayo N, et al. Participation in a population-based screening for colorectal cancer using the faecal immunochemical test decreases mortality in 5 years. Eur J Gastroenterol Hepatol. (2019) 31:197–204. doi: 10.1097/MEG.0000000000001338
4. Fenton JJ, Elmore JG, Buist DSM, Reid RJ, Tancredi DJ, Baldwin LM. Longitudinal adherence with fecal occult blood test screening in community practice. Ann Family Med. (2010) 8:397–401. doi: 10.1370/afm.1133
5. Hurtado JL, Bacigalupe A, Calvo M, Esnaola S, Mendizabal N, Portillo I, et al. Social inequalities in a population based colorectal cancer screening programme in the Basque Country. BMC Public Health. (2015) 15:1021. doi: 10.1186/s12889-015-2370-5
6. Lansdorp-Vogelaar I, Goede SL, Ma J, Xiau-Cheng W, Pawlish K, Van Ballegooijen M, et al. State disparities in colorectal cancer rates: contributions of risk factors, screening, and survival differences. Cancer. (2015) 121:3676–83. doi: 10.1002/cncr.29561
7. Portillo I, Idigoras I, Bilbao I, Arana-Arri E, Fernández-Landa MJ, Hurtado JL, et al. Colorectal cancer screening program using FIT: quality of colonoscopy varies according to hospital type. Endosc Int Open. (2018) 6:E1149–56. doi: 10.1055/a-0655-1987
8. Portillo I, Idígoras I, Ojembarrena E, Arana E, Luis Hurtado J, Basurko R, et al. Lesiones detectadas en el programa de cribado de cáncer colorrectal en el País Vasco: primera ronda 2009–2011. Gastroenterol Hepatol. (2013) 36:301–8. doi: 10.1016/j.gastrohep.2013.02.004
9. Arana-Arri E, Idigoras I, Uranga B, Pérez R, Irurzun A, Gutiérrez-Ibarluzea I, et al. Population-based colorectal cancer screening programmes using a faecal immunochemical test: should faecal haemoglobin cut-offs differ by age and sex? BMC Cancer. (2017) 17:1. doi: 10.1186/s12885-017-3555-3
10. Ferlitsch M, Heinze G, Salzl P, Britto-Arias M, Waldmann E, Reinhart K, et al. Sex is a stronger predictor of colorectal adenoma and advanced adenoma than fecal occult blood test. Med Oncol. (2014) 31:151. doi: 10.1007/s12032-014-0151-0
11. Majek O, Gondos A, Jansen L, Emrich K, Holleczek B, Katalinic A, et al. Sex differences in colorectal cancer survival: population-based analysis of 164,996 colorectal cancer patients in Germany. PLoS ONE. (2013) 8:e68077. doi: 10.1371/journal.pone.0068077
12. Schüz J, Espina C, Villain P, Herrero R, Leon ME, Minozzi S, et al. European Code against Cancer 4th Edition: 12 ways to reduce your cancer risk. Cancer epidemiology. (2015) 39 Suppl 1:S10. doi: 10.1016/j.canep.2015.03.017
13. Mosquera I, Mendizabal N, Martín U, Bacigalupe A, Aldasoro E, Portillo I. Inequalities in participation in colorectal cancer screening programmes: a systematic review. Eur J Public Health. (2020) 30:558–67. doi: 10.1093/eurpub/ckz236
14. Johnson CM, Wei C, Ensor JE, Smolenski DJ, Amos CI, Levin B, et al. Meta-analyses of colorectal cancer risk factors. Cancer Causes Control. (2013) 24:1207–22. doi: 10.1007/s10552-013-0201-5
15. Domínguez-Berjón MF, Borrell C, Cano-Serral G, Esnaola S, Nolasco A, Isabel Pasarín M, et al. Construcción de un índice de privación a partir de datos censales en grandes ciudades españolas (Proyecto MEDEA). Gaceta Sanit. (2008) 22:179–87. doi: 10.1157/13123961
16. Orueta JF, Nuño-Solinis R, Mateos M, Vergara I, Grandes G, Esnaola S. Predictive risk modelling in the Spanish population: a cross-sectional study. BMC Health Serv Res. (2013) 13:1. doi: 10.1186/1472-6963-13-269
17. Cuida tu salud—Osasun Eskola—Osakidetza. Available online at: https://www.osakidetza.euskadi.eus/cuida-tu-salud/ab84-oescuida/es/ (accessed October, 2020).
18. Mansouri D, McMillan DC, Grant Y, Crighton EM, Horgan PG. The impact of age, sex and socioeconomic deprivation on outcomes in a colorectal cancer screening programme. PLoS ONE. (2013) 8:e66063. doi: 10.1371/journal.pone.0066063
19. Gupta S, Tong L, Allison JE, Carter E, Koch M, Rockey DC, et al. Screening for colorectal cancer in a safety-net health care system: access to care is critical and has implications for screening policy. Cancer Epidemiol Biomarkers Prev. (2009) 18:2373–9. doi: 10.1158/1055-9965.EPI-09-0344
20. Molina-Barceló A, Peiró-Pérez R, Vanaclocha M, Vallés G, Guaita L, Salas D. Informed participation in the Valencian Community Colorectal Cancer Screening Programme from a gender perspective. Gac Sanit. (2018) 32:72–6. doi: 10.1016/j.gaceta.2016.07.010
21. Pornet C, Dejardin O, Morlais F, Bouvier V, Launoy G. Socioeconomic determinants for compliance to colorectal cancer screening. A multilevel analysis. J Epidemiol Community Health. (2010) 64:318–24. doi: 10.1136/jech.2008.081117
22. Malila N, Hakama M, Pukkala E. A 25-year follow-up of a population screened with faecal occult blood test in Finland. Acta Oncol. (2007) 46:1103–6. doi: 10.1080/02841860701442531
23. Clarke N, Sharp L, Osborne A, Kearney PM. Comparison of uptake of colorectal cancer screening based on fecal immunochemical testing (FIT) in males and females: a systematic review and meta-analysis. Cancer Epidemiol Biomarkers Prev. (2015) 24:39–47. doi: 10.1158/1055-9965.EPI-14-0774
24. Ritvo P, Myers RE, Paszat L, Serenity M, Perez DF, Rabeneck L. Gender differences in attitudes impeding colorectal cancer screening. BMC Public Health. (2013) 13:500. doi: 10.1186/1471-2458-13-500
25. Oster C, McGuiness C, Duncan A, Turnbull D. Masculinity and men's participation in colorectal cancer screening. Psychol Men Masc. (2015) 16:254–63. doi: 10.1037/a0038154
26. Springer KW, Mouzon DM. “Macho men” and preventive health care: implications for older men in different social classes. J Health Soc Behav. (2011) 52:212–27. doi: 10.1177/0022146510393972
27. Christy SM, Mosher CE, Rawl SM. Integrating men's health and masculinity theories to explain colorectal cancer screening behavior. Am J Mens Health. (2014) 8:54–65. doi: 10.1177/1557988313492171
28. Moss SM, Campbell C, Melia J, Coleman D, Smith S, Parker R, et al. Performance measures in three rounds of the English bowel cancer screening pilot. Gut. (2012) 61:101–7. doi: 10.1136/gut.2010.236430
29. Hall NJ, Rubin GP, Dobson C, Weller D, Wardle J, Ritchie M, et al. Attitudes and beliefs of non-participants in a population-based screening programme for colorectal cancer. Health Expect. (2015). 18:1645–57. doi: 10.1111/hex.12157
30. Wools A, Dapper EA, R de LJ. Colorectal cancer screening participation: a systematic review. Eur J Public Health. (2016) 26:156. doi: 10.1093/eurpub/ckv148
31. van Dam L, Korfage IJ, Kuipers EJ, Hol L, van Roon AH, Reijerink JC, et al. What influences the decision to participate in colorectal cancer screening with faecal occult blood testing and sigmoidoscopy? Eur J Cancer. (2013) 49:2321–30. doi: 10.1016/j.ejca.2013.03.007
32. Ogedegbe G, Cassells AN, Robinson CM, Duhamel K, Tobin JN, Sox CH, et al. Perceptions of barriers and facilitators of cancer early detection among low-income minority women in community health centers. J Natl Med Assoc. (2005) 97:162–70.
33. Encuesta de salud (2018). Available online at: http://www.euskadi.eus/informacion/encuesta-de-salud-2017-2018/web01-a3osag17/es/ (accessed November 10, 2019)
34. Pornet C, Denis B, Perrin P, Gendre I, Launoy G. Predictors of adherence to repeat fecal occult blood test in a population-based colorectal cancer screening program. Br J Cancer. (2014) 111:2152–5. doi: 10.1038/bjc.2014.507
35. von Wagner C, Good A, Wright D, Rachet B, Obichere A, Bloom S, et al. Inequalities in colorectal cancer screening participation in the first round of the national screening programme in England. Br J Cancer. (2009) 101(Suppl. 2):S60–3. doi: 10.1038/sj.bjc.6605392
36. Le Breton J, Journy N, Attali C, Le CP, Brixi Z, Bastuji-Garin S, et al. Improving participation in colorectal cancer screening: targets for action. Prev Med. (2012) 55:488–92. doi: 10.1016/j.ypmed.2012.08.004
37. Dawidowicz S, Le Breton J, Moscova L, Renard V, Bercier S, Brixi Z, et al. Predictive factors for non-participation or partial participation in breast, cervical and colorectal cancer screening programmes. Fam Pract. (2019) 37:15–24. doi: 10.1093/fampra/cmz031
38. Klabunde CN, Lanier D, Breslau ES, Zapka JG, Fletcher RH, Ransohoff DF, et al. Improving colorectal cancer screening in primary care practice: innovative strategies and future directions. J Gen Intern Med. (2007) 22:1195–205. doi: 10.1007/s11606-007-0231-3
39. Menvielle G, Dugas J, Richard JB, Luce D. Socioeconomic and healthcare use-related determinants of cervical, breast and colorectal cancer screening practice in the French West Indies. Eur J Cancer Prev. (2018) 27:269–73. doi: 10.1097/CEJ.0000000000000329
40. Brose LS, McEwen A. Neighbourhood deprivation and outcomes of stop smoking support—an observational study. PLoS ONE. (2016) 11:1–10. doi: 10.1371/journal.pone.0148194
41. Nau C, Schwartz BS, Bandeen-roche K, Liu A, Pollak J, Hirsch A, et al. Community socioeconomic deprivation and obesity trajectories in children using electronic health records. Obesity. (2015) 23:207–12. doi: 10.1002/oby.20903
42. Poulsen MN, Glass TA, Pollak J, Bandeen-Roche K, Hirsch AG, Bailey-Davis L, et al. Associations of multidimensional socioeconomic and built environment factors with body mass index trajectories among youth in geographically heterogeneous communities. Prev Med Rep. (2019) 15:100939. doi: 10.1016/j.pmedr.2019.100939
43. Carrillo-Vega MF, Albavera-Hernández C, Ramírez-Aldana R, García-Peña C. Impact of social disadvantages in the presence of diabetes at old age. BMC Public Health. (2019) 19:1–10. doi: 10.1186/s12889-019-7348-2
44. Green PM, Kelly BA. Colorectal cancer knowledge, perceptions, and behaviors in African Americans. Cancer Nurs. (2004) 27:206–17. doi: 10.1097/00002820-200405000-00004
Keywords: social inequalities, colorectal cancer, screening programme, risk factors, prevention, non-participation
Citation: Solís-Ibinagagoitia M, Unanue-Arza S, Díaz-Seoane M, Martínez-Indart L, Lebeña-Maluf A, Idigoras I, Bilbao I and Portillo I (2020) Factors Related to Non-participation in the Basque Country Colorectal Cancer Screening Programme. Front. Public Health 8:604385. doi: 10.3389/fpubh.2020.604385
Received: 09 September 2020; Accepted: 11 November 2020;
Published: 11 December 2020.
Edited by:
Guido Van Hal, University of Antwerp, BelgiumReviewed by:
Ivana Kulhánová, Charles University, CzechiaCopyright © 2020 Solís-Ibinagagoitia, Unanue-Arza, Díaz-Seoane, Martínez-Indart, Lebeña-Maluf, Idigoras, Bilbao and Portillo. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: I. Portillo, bWFyaWFpc2FiZWwucG9ydGlsbG92aWxsYXJlc0Bvc2FraWRldHphLmV1cw==; orcid.org/0000-0002-3871-3423
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.