
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health, 25 November 2020
Sec. Infectious Diseases: Epidemiology and Prevention
Volume 8 - 2020 | https://doi.org/10.3389/fpubh.2020.601961
 Ali Akhtar1†
Ali Akhtar1† Amer Hayat Khan1*
Amer Hayat Khan1* Hadzliana Zainal1
Hadzliana Zainal1 Mohamed Azmi Ahmad Hassali2Irfhan Ali3Long Chiau Ming4
Mohamed Azmi Ahmad Hassali2Irfhan Ali3Long Chiau Ming4Background: Unnecessary antimicrobial use is an emerging problem throughout the world. To design future interventions to ensure rational antimicrobial use and decrease the risk of antimicrobial resistance, physician's knowledge and prescribing practices of antimicrobials should be assessed. Therefore, the main objective of this study is to investigate the physician's knowledge along with their prescribing patterns of antimicrobials in their health care system.
Methods: The present qualitative study was conducted in a tertiary care public hospital located at Penang island, situated in Northwest of Malaysia. A total of 12 semi-structured, face to face interviews were conducted with purposive sampling technique. Physicians recruited had different specialties. All interviews were audio recorded, then transcribed into English language and analyze by thematic content analysis.
Results: Four major themes were identified: (1) prescribing patterns of physicians regarding antimicrobials; (2) physician's knowledge about antimicrobials; (3) antimicrobial resistance; (4) satisfaction with management of infections. Physicians believed in regular educational activities and updates about the latest antimicrobial guidelines may change the prescribing behavior of physicians to optimize the use of antimicrobials. This may lead to decrease in burden of antimicrobial resistance in their health care system. Physicians emphasized that stricter rules and regular monitoring of antimicrobial use should be implemented to overcome the main challenges of antimicrobial resistance.
Conclusion: Different factors were identified to assist optimized use of antimicrobials and decrease the risk of antimicrobial resistance. The present study helps to design targeted future interventions to ensure rational antimicrobial use and decrease the impact of antimicrobial resistance in Malaysia.
Antimicrobials have reduced the death rate due to infectious diseases for the past 70 years when they were first introduced. Whereas, inappropriate use of these antimicrobials made many micro-organisms resistant to them (1). Antimicrobial resistance (AMR) is an emerging problem throughout the world that cause increased mortality, morbidity, and cost of the treatment (2). In Europe, more than 25,000 deaths have been recorded annually due to AMR and around €1.5 billion is the cost to cope with these drug-resistant infections due to increase in the healthcare expenses and low treatment outcomes (1).
To increase the rational use of antimicrobials, the prescribing pattern of physicians should be changed (3). Antimicrobial stewardship programs (ASP) play a significant role to rationalize the use of antimicrobials in health care settings. Educating health care professionals by ASPs can decrease unnecessary prescribing of antimicrobials, cost of therapy and hospital stay (4). Health care providers are in support of ASPs because they can improve their knowledge, practice, and care of their patients more efficiently (5). Previous studies reported that physicians agreed on the excessive use of antimicrobials all over the world but denied this issue in their own health care settings (6, 7). Appropriate use of antimicrobials solely depends on the knowledge of physicians toward the antimicrobial usage guidelines which vary from country to country (3, 8). Adherence to antimicrobial guidelines by the physicians should be monitored to evaluate their prescribing behavior is the best way to increase the rational use of antimicrobials and reduce the risk of AMR (9).
Countries in South East Asia contribute substantially to inappropriate antimicrobial use which leads to higher risk of AMR (10). Many South East Asian countries collaborated with WHO to conduct national situational analyses of antimicrobial management to evaluate the use of antimicrobials in their respective countries to assess the inappropriate use of antimicrobials and educate the health care providers about the rational use of antimicrobials. Regular auditing of antimicrobials increases the rational use of antimicrobials and decreases the risk of AMR (10).
Ministry of Health (MoH) in Malaysia creates awareness about rational use of antimicrobials by publishing guidelines, however, the prescription rates of antimicrobials remain at high level (70–80%) in primary care settings and hospitals (11, 12). Some studies conducted in Malaysia reported the high rate of antimicrobial prescription are due to upper respiratory infections and acute gastroenteritis which contributes for around 49.2 and 20.5% of the antimicrobials prescription respectively (13). Therefore, it can be concluded that only publishing the guidelines alone is not enough to change the prescribing habits of health care professionals. Education of physicians regarding the published guidelines and reminders at regular intervals may have some positive impact to change their prescribing patterns and increase the rational use of antimicrobials (11, 14).
Hence, the objective of current study is to explore and compare physician's prescribing patterns and perceptions about antimicrobial use and resistance in relation to the management of common infections at a tertiary care hospital.
By in-depth reviewing the published literature regarding antimicrobials, a semi-structured interview guide was prepared attached as a Supplementary Material (1, 3–8, 15, 16). Prior to conducting interviews, the reliability and validity of this interview guide has been evaluated to strengthen the findings of the study. Experts from School of Pharmaceutical Sciences, Universiti Sains Malaysia with substantial experience in qualitative research, reviewed the initial interview guide and validated it. Three independent physicians working as head of their departments in Hospital Pulau Pinang, Malaysia reviewed and approved all the questions in interview guide to increase the appropriateness of the interview guide. Before conducting interviews, a pilot study was carried out to improve the interview guide accordingly. Face to face interviews were conducted by recording with the physicians in hospital during office hours to assure the reliability of findings of the present study.
This study was conducted in a tertiary care hospital in Penang Island, which is a Malaysian state located in the northwest of Malaysia. By using purposive sampling technique in qualitative research, physicians registered with Malaysian Medical Council were included in this study after obtaining their written consent. The prescribing patterns and perceptions of physicians regarding antimicrobials practices in big cities could be different from those in small cities or villages.
The objectives of the study were explained to the participant physicians before starting prior to signing the consent form. Physicians had the right to withdraw from the interview at any stage of the study. Interviews were conducted in the physicians' offices during office hours. To ensure privacy of the respondents, identity of the physicians was kept anonymous. Interviews were audio recorded and then transcribed into different codes against the views of the physicians to assure the confidentiality and privacy by the principal investigator (AA). Interviews were conducted with the physicians until the saturation point has been achieved. English language was used for interviews and their duration of an interview was ~15–35 min. Physicians had the freedom to add their additional views and share experiences related to their antimicrobial practices. Saturation point had been achieved by the tenth interview; however, two more interviews were conducted to confirm saturation. All these twelve interviews were conducted from November 2019 to February 2020.
All recorded interviews were transcribed precisely, and the language used to write transcripts was English. To avoid grammatical errors, slight changes have been done in transcripts in the process of data extraction. Firstly, thematic content analysis was carried out independently by three researchers (AA, AHK, and HZ) in which similar views of physicians related to general questions were highlighted. Secondly, different opinions of physicians related to same research questions were compared to find out any differences between them. Emerging themes from the transcripts were identified. All the transcribed interviews were analyzed by the research team repeatedly before categorizing into the themes and sub-themes. In this way, similar themes were categorized collectively to avoid the repetition of the data.
A detailed description of all the interviewees is presented in Table 1. Out of 12 respondents, 7 were male physicians and 5 were female. Mean age of physicians were 37 ± 8 years. Following are the four major themes including sub-themes emerged from the analysis of transcribed interviews:
1. Prescribing patterns of physicians regarding antimicrobials;
2. Physician's knowledge about antimicrobials;
3. Antimicrobial Resistance (AMR);
4. Satisfaction with management of infections.
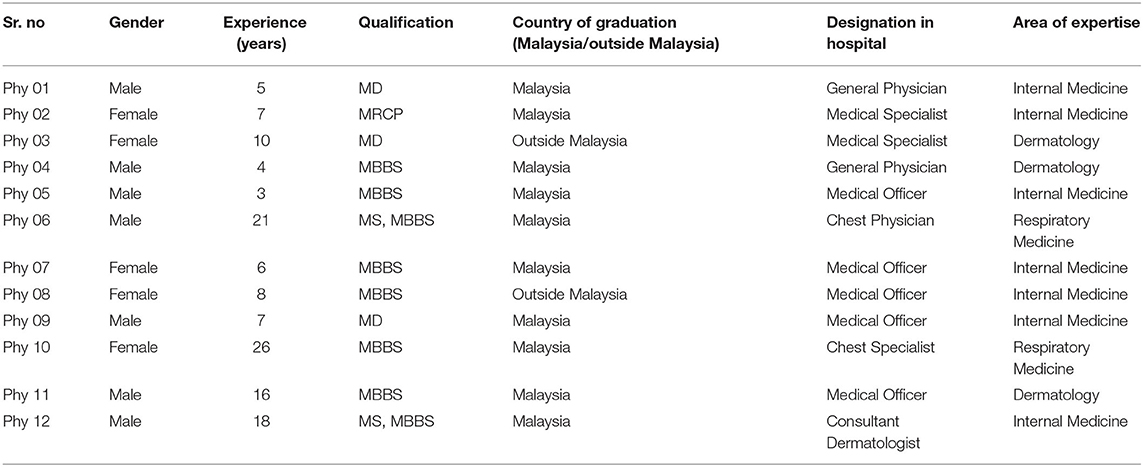
Table 1. Demographics of physicians.
Theme 1: Prescribing patterns of physicians regarding antimicrobials
i) Decision of antimicrobial prescribing
The majority of physicians stated that the decision to prescribe antimicrobials is solely based on the clinical condition of the patients.
“Based on the clinical features of the patients whether they are in infected state, risk factors of the patients or they are immunocompromised, or weather is there any history of recent hospitalization.” (Phy 02)
“Firstly, it depends on the hospital guidelines and then go through clinically depending on the severity of the infections.” (Phy 08)
“By assessing the patient's condition like if a patient got fever, sign of infection, inflammation, pain and start antimicrobials.” (Phy 11)
ii) Difference in prescribing patterns among physicians
Most of the physicians explained that their prescribing patterns depends on the guidelines given by the hospital and slightly different from each other due to the experience in their respective fields.
“Yes, because of new antibiograms coming, new microorganisms and new culture sensitivity results then we adjust accordingly to what is the most predominant bug we have.” (Phy 06)
“Yes, I do. I think I get more experience so based on clinical symptoms then you can expect the kind of bacteria that the patient may have then you will prescribe antibiotic accordingly.” (Phy 08)
“Yes, based on the changes in the guidelines so it's changed according to antibiogram of the hospital as well.” (Phy 10)
“Yes, is ever changing because of the change of guidelines and emergence of new resistance strains.” (Phy 04)
iii) Prescribe antimicrobial or wait and watch approach
Respondents included in current study said that wait and watch approach for prescribing antimicrobials depends on condition of the patients whether to start antimicrobials immediately or wait for the culture and sensitivity results.
“Usually those are referred to our specialist clinics they are more severe cases, they are more resistance and expensive so most of them they have systemic symptoms so we most likely to start antimicrobials rather than wait and see.” (Phy 12)
“Most important is the clinical features how the patient is presenting, if the patient is very ill or looks like it's a bacterial infection, we won't wait.” (Phy 06)
“Usually this one we will see the patient's general conditions or the blood parameters then only we will decide.” (Phy 05)
“Normally we wait and see if there is no other worsening of the symptoms, we just treat accordingly to whatever symptoms he came in with but should there be anything while he admitted or we think he is having infection then we will start antimicrobials.” (Phy 06)
“We must closely monitor the condition of patient, suggest investigation and then decide what to prescribe.” (Phy 03)
iv) Alternatives to antimicrobials
Interviewed physicians stated that they use alternatives to antimicrobials by examining the condition of the patients, give symptomatic treatment and suggests further investigations.
“Symptomatic relief for example a patient is having fever we can give hydration, peptic sponging, encourage oral intake.” (Phy 08)
“I think if antimicrobial is not indicated then we will give symptomatic treatment.” (Phy 04)
“Then I will suggest that patient use those antiseptics wash and to monitor the patient and follow up more closely for the signs of infection.” (Phy 02)
Theme 2: Physician's knowledge about antimicrobials
Most of the physicians have the access to the latest guidelines on antimicrobials published all over the world alongside the local guidelines by the Ministry of Health, Malaysia. Organization of CMEs by the hospital administration at regular intervals helps health care providers with latest education on antimicrobials. Detailed views of physicians regarding knowledge of antimicrobials and its related factors can be seen in Table 2.
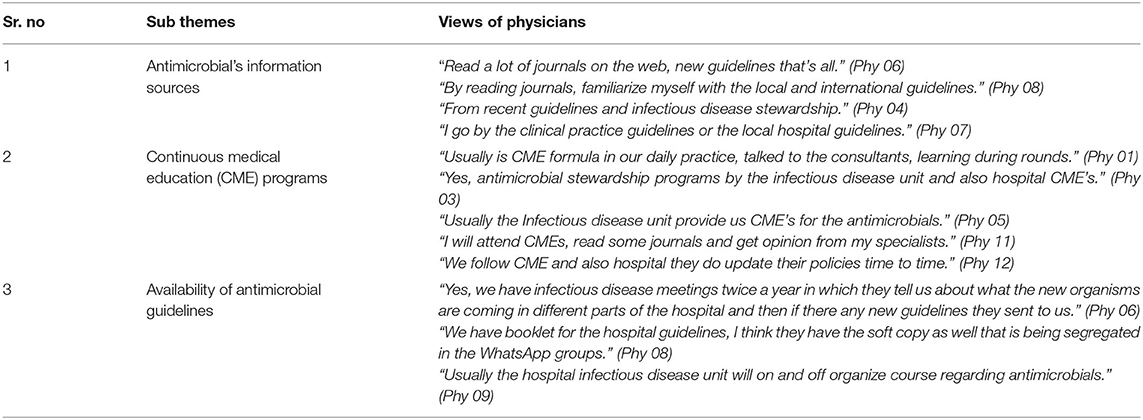
Table 2. Physician's antimicrobial knowledge.
Theme 3: Antimicrobial Resistance (AMR)
i) AMR being a problem
Most of the physicians interviewed in the study admit that AMR is an emerging problem all over the world and if this problem persists it would be life threatening and may increase the cost of treatment. Moreover, it may decrease the treatment outcomes of the patients prescribed with antimicrobials.
“Yes, there has been risk for the incidence of antimicrobial resistance over the years and I think probably due to a lot of patients who are resistant to some form of antibiotics prior to admission in the hospital.” (Phy 02)
“Yes, we are definitely seeing an increase in the more resistant organism specially those coming from ICU, they are so resistant sometimes that we run out of antimicrobials to use so we definitely seeing an increase in the last few years.” (Phy 06)
“Yes definitely, I think it happens because people are very liberal with antibiotic usage even for viral issues, they start prescribing antimicrobials and this leads to antimicrobial resistance.” (Phy 07)
“Yes, because some people are resistant towards antibiotics that they need to be on antimicrobial for a long period of time and sometimes patient die because of antimicrobial resistance.” (Phy 11)
ii) Future with AMR
Respondents included in the present study stated that if AMR is not controlled now, it will result in very drastic circumstances in the future which may lead to higher mortality rate due to infections.
“Currently the antimicrobial resistance is increasing in trend but I think so far it is still under control.” (Phy 02)
“I think it will increase mortality because there are more infections that are not treatable if AMR is an issue in the future.” (Phy 04)
iii) Intensity of AMR
Physicians shared their experiences about the intensity of AMR and stated that if the burden of AMR is not controlled now, it will egregiously affect the health care system all over the world.
“If we do not use our antimicrobial correctly, definitely the resistance will become more and more, this may become a major and serious problem in the future.” (Phy 01)
“So, the antimicrobial should be carefully prescribed or there will be an increase in the antimicrobial resistance in the future.” (Phy 02)
“I think if we are not careful, we will reach that stage where we might not have any antibiotics to prescribe, so we have to become a bit more vigilant with what we use now.” (Phy 06)
“It depends on doctor's practice; some doctors like to give antibiotics first due to patient's request so the antibiotic resistance is increasing.” (Phy 11)
Theme 4: Satisfaction with management of infections
Many physicians admit that there are unnecessary prescriptions of antimicrobials in their health care system, but it can be reduced by regularly educating the health care providers with the latest guidelines and ASP. Educational activities for patients and the general public regarding antimicrobial usage and preventive measures should be initiated for the better control of infections. Table 3 shows the detailed views of physicians regarding their infection management satisfaction and their related factors.
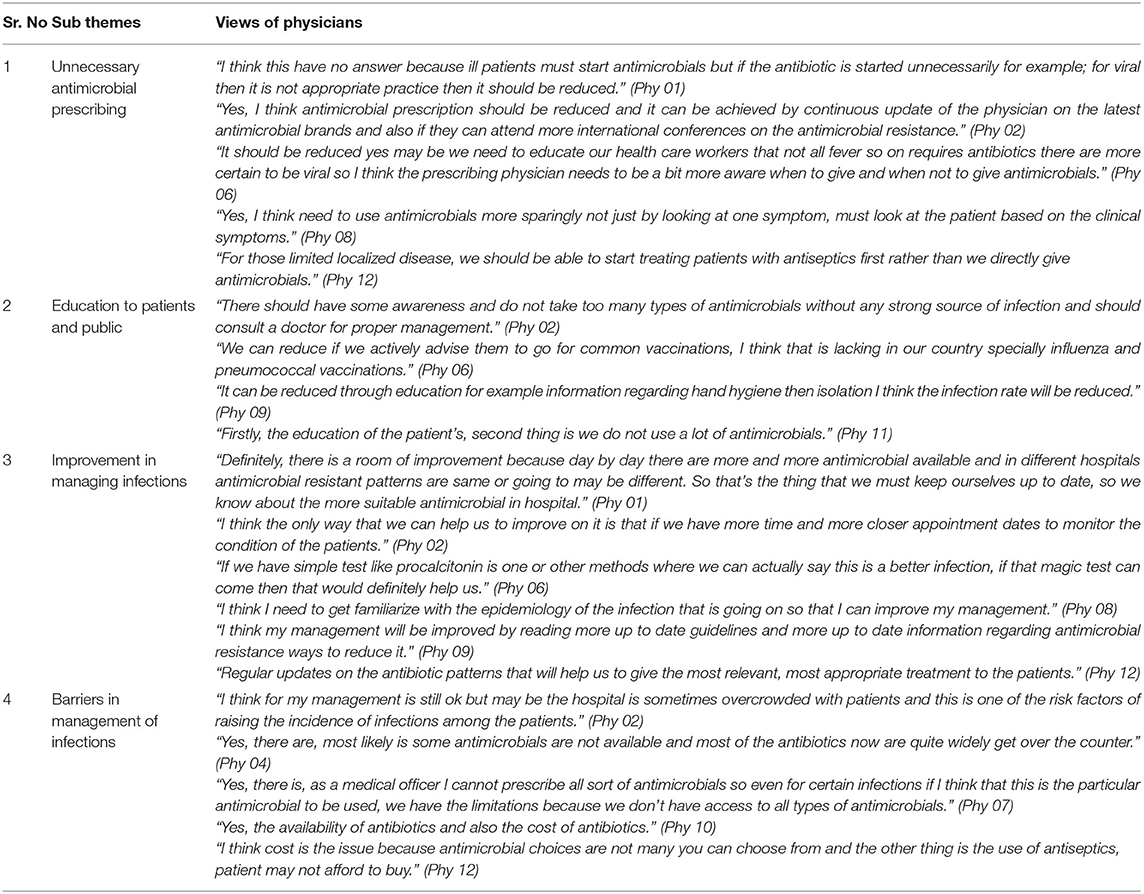
Table 3. Physician's infection management satisfaction.
Our findings show that physicians working in a large public hospital of Malaysia were well-aware of the fact about the overuse of antimicrobials. A majority of the physicians admits that antimicrobials are sometimes unnecessary or over prescribed nationally in their country but some of them also shared their experience that in their own hospital the use of antimicrobials should be rationalized. Previous literature reported the emergence of antimicrobial resistance among their own health care system as well as over all the world as reported in present study (6, 17).
Many studies emphasize the relation of overuse of antimicrobials with the prescribing behavior of the physicians. Physicians should change their prescribing patterns of antimicrobials according to the latest guidelines for antimicrobial usage to overcome the risk of AMR which is an emerging problem all over the world (8, 18). Healthcare providers should update their knowledge in their respective fields by reading the official guidelines of their country rather than to depend on the knowledge given by representatives of different pharmaceutical industries, whose main concern is to sell their products and make profit (19). Other educational activities should be implemented in hospitals to empower the knowledge of physicians and decrease the risk of over prescribing of antimicrobials and AMR as reported in current study and previous literature (8, 9).
Many physicians in current study stated that other health care providers over prescribe antimicrobials, but their own prescribing behavior is not in a category of over prescribing, which supports the findings of previous studies (3, 7, 17). Unnecessary use and over prescribing of antimicrobials ultimately leads to AMR. Moreover, majority of the physicians included in current study believed that they can reduce the risk of AMR by reducing the use of unnecessary antimicrobials. As reported in previous studies (6, 20), many physicians agreed that updated antimicrobial knowledge is very important in their respective fields but they also need regular educational activities related to antimicrobials, feedback on their prescribing behavior and there should be an appropriate guideline on restricted agents which require a preapproval before prescribing, helping them to reduce the unnecessary prescription of antimicrobials which leads to decrease the risk of AMR.
Almost all the physicians interviewed are well-aware of the fact that AMR is not just a national problem but a global issue which is prevailing day by day. In addition, all our interviewed physicians admit that reduction in unnecessary antimicrobial usage decreases the risk of AMR in their own country as well as all over the world as compared to only 66% respondents who agreed in the study conducted by Wester et al. (15). Regular ASP conducted in the hospital of included physicians may contribute to these differences by creating more knowledge and providing updated antimicrobial guidelines for the better use of antimicrobials and reducing the risk of AMR.
Most of the physicians believed that if emergence of AMR is not controlled now, it may lead to failure of treatment and increase the therapy cost in the near future. Physicians should take advice from their seniors about the optimal use of antimicrobials because senior physicians have more knowledge about the rational use of antimicrobials due to their vast experience in their respective fields as compared to junior physicians or fresh graduates. These findings are comparable with previous studies which also reported that senior physicians are more confident for the rational use of antimicrobials as compared to junior physicians (6, 8).
The current study found that physicians have access to a wide variety of resources regarding antimicrobials for reading and updating their knowledge to improve their antimicrobial prescribing practices. A majority of the physicians emphasize regular training on antimicrobials in their hospital that provides them latest knowledge and training to change their antimicrobial prescribing behavior to promote the rational use of antimicrobials and make strategies to overcome the burden of AMR in their local health care settings. Our study also indicates the relation of junior physicians with their seniors regarding teaching and training for the better use of antimicrobials, as senior staff shared their vast knowledge with junior physicians to improve their decision making.
Physicians included in the present study also shared many useful suggestions during the interview session to enhance the rationale use of antimicrobials locally as well as globally. These includes that strict regulations should be implemented regarding the use of antimicrobials and monitor the usage of antimicrobials at regular intervals to ensure its rationale use all over the country. A majority of the participating physicians also indicated that if they have better and accurate diagnostic equipment, the excessive use of antimicrobials could be minimized. Moreover, updated knowledge of antimicrobials and regular antimicrobial stewardship programmes in the hospital reduced the overuse of antimicrobials. Physicians appreciate the regular availability of local guidelines by the hospital management which provides updated knowledge which is consistent with an Australian survey (5). Physicians knowledge could be improved if hospital pharmacists had a heightened role in educating as well as monitoring antimicrobial utilization, which is implemented in many countries of the world. Developing ASP and implementing them is also included in the role of hospital pharmacists (21).
There are few limitations in our study. Firstly, our study was conducted in one public sector hospital, so the generalizability of the results must be viewed with caution. Secondly, physicians who do not wish to take part in our study may have different views and opinions regarding the use of antimicrobials and antimicrobial resistance, which may lead to unmeasured bias. Nevertheless, our comprehensive methodology and results investigate different aspects of all the themes which can reduce this bias. Thirdly, there is a possibility that physicians gave socially accepted answers but not their true opinions. This issue was addressed by assuring the physicians about the privacy of their opinions. Despite of these above said limitations, the objectives of current study have been achieved, as we identified different factors involved in prescribing behavior and perceptions of physicians regarding the use of antimicrobials and risk of antimicrobial resistance in their own health care system and all over the world.
Physicians working in included health care setting were well-aware of the problems of unnecessary usage of antimicrobials and different factors involved in the emergence of antimicrobial resistance and they strongly believed that regular efforts may decrease the impact of these problems. Our study compares different views of physicians regarding their practices, which may be used to design targeted interventions in future. Ongoing educational activities should continue to update the physician's knowledge and latest updates on antimicrobials, which helps to decrease the risk of antimicrobial resistance which is an emerging problem throughout the world.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Current Study was conducted after the approval from National Institute of Health and Medical Research and Ethics Committee, Malaysia (NMRR-19-1037-46721). The patients/participants provided their written informed consent to participate in this study.
AA conceptualized and designed the study, conducted the statistical analyses, interpreted the data, and drafted the manuscript. AK, HZ, and MA revised the manuscript for intellectual content, read, and approved the final version of the manuscript. IA and LM helped in conducted the interviews and supervised the drafting of the manuscript, supported in interpreting the data, and revised the manuscript for intellectual content. All authors read and approved the final manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
We would like to thank the Director General of Health Malaysia for his permission to publish this article. The authors are thankful to Institute of Postgraduate Studies (IPS) of Universiti Sains Malaysia (USM) for fellowship support.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2020.601961/full#supplementary-material
1. Kaae S, Malaj A, Hoxha I. Antibiotic knowledge, attitudes and behaviours of Albanian health care professionals and patients–a qualitative interview study. J Pharm Policy Pract. (2017) 10:1–8. doi: 10.1186/s40545-017-0102-1
2. Gandra S, Barter D, Laxminarayan R. Economic burden of antibiotic resistance: how much do we really know? Clin Microbiol Infect. (2014) 20:973–80. doi: 10.1111/1469-0691.12798
3. Pulcini C, Williams F, Molinari N, Davey P, Nathwani D. Junior doctors' knowledge and perceptions of antibiotic resistance and prescribing: a survey in France and Scotland. Clin Microbiol Infect. (2011) 17:80–7. doi: 10.1111/j.1469-0691.2010.03179.x
4. Ashiru-Oredope D, Sharland M, Charani E, McNulty C, Cooke J. Improving the quality of antibiotic prescribing in the NHS by developing a new Antimicrobial Stewardship Programme: Start Smart—Then Focus. J Antimicrob Chemother. (2012) 67(Suppl. 1):i51–63. doi: 10.1093/jac/dks202
5. Bannan A, Buono E, McLaws ML, Gottlieb T. A survey of medical staff attitudes to an antibiotic approval and stewardship programme. Intern Med J. (2009) 39:662–8. doi: 10.1111/j.1445-5994.2009.01936.x
6. Srinivasan A, Song X, Richards A, Sinkowitz-Cochran R, Cardo D, Rand C. A survey of knowledge, attitudes, and beliefs of house staff physicians from various specialties concerning antimicrobial use and resistance. Arch Intern Med. (2004) 164:1451–6. doi: 10.1001/archinte.164.13.1451
7. Abbo L, Sinkowitz-Cochran R, Smith L, Ariza-Heredia E, Gómez-Marín O, Srinivasan A, et al. Faculty and resident physicians' attitudes, perceptions, and knowledge about antimicrobial use and resistance. Infect Control Hosp Epidemiol. (2011) 32:714–8. doi: 10.1086/660761
8. Md Rezal RS, Hassali MA, Alrasheedy AA, Saleem F, Md Yusof FA, Godman B. Physicians' knowledge, perceptions and behaviour towards antibiotic prescribing: a systematic review of the literature. Expert Rev Anti Infect Ther. (2015) 13:665–80. doi: 10.1586/14787210.2015.1025057
9. Nakwatumbah S, Kibuule D, Godman B, Haakuria V, Kalemeera F, Baker A, et al. Compliance to guidelines for the prescribing of antibiotics in acute infections at Namibia's national referral hospital: a pilot study and the implications. Expert Rev Anti Infect Ther. (2017) 15:713–21. doi: 10.1080/14787210.2017.1320220
10. Tay KH, Ariffin F, Sim BL, Chin SY. Multi-faceted intervention to improve the antibiotic prescriptions among doctors for acute URI and acute diarrhoea cases: the green zone antibiotic project. Malay J Med Sci. (2019) 26:101. doi: 10.21315/mjms2019.26.4.12
11. Teng CL, Tong SF, Khoo EM, Lee V, Zailinawati AH, Mimi O, et al. Antibiotics for URTI and UTI: prescribing in Malaysian primary care settings. Aust Fam Physician. (2011) 40:325. Available online at: https://www.racgp.org.au/download/documents/AFP/2011/May/201105teng.pdf
12. Lim V, Cheong Y, Suleiman A. Pattern of antibiotic usage in hospitals in Malaysia. Singapore Med J. (1993) 34:525–8.
13. Ab Rahman N, Teng CL, Sivasampu S. Antibiotic prescribing in public and private practice: a cross-sectional study in primary care clinics in Malaysia. BMC Infect Dis. (2016) 16:208. doi: 10.1186/s12879-016-1530-2
14. Arnold SR, Straus SE. Interventions to improve antibiotic prescribing practices in ambulatory care. Cochrane Database Syst Rev. (2005) 2005:CD003539. doi: 10.1002/14651858.CD003539.pub2
15. Wester CW, Durairaj L, Evans AT, Schwartz DN, Husain S, Martinez E. Antibiotic resistance: a survey of physician perceptions. Arch Intern Med. (2002) 162:2210–6. doi: 10.1001/archinte.162.19.2210
16. Velasco E, Ziegelmann A, Eckmanns T, Krause G. Eliciting views on antibiotic prescribing and resistance among hospital and outpatient care physicians in Berlin, Germany: results of a qualitative study. BMJ Open. (2012) 2:e000398. doi: 10.1136/bmjopen-2011-000398
17. Guerra CM, Pereira CAP, Neto ARN, Cardo DM, Correa L. Physicians' perceptions, beliefs, attitudes, and knowledge concerning antimicrobial resistance in a Brazilian teaching hospital. Infect Control Hosp Epidemiol. (2007) 28:1411–4. doi: 10.1086/523278
18. Cabana MD, Rand CS, Powe NR, Wu AW, Wilson MH, Abboud P-AC, et al. Why don't physicians follow clinical practice guidelines? A framework for improvement. JAMA. (1999) 282:1458–65. doi: 10.1001/jama.282.15.1458
19. Fadare JO, Oshikoya KA, Ogunleye OO, Desalu OO, Ferrario A, Enwere OO, et al. Drug promotional activities in Nigeria: impact on the prescribing patterns and practices of medical practitioners and the implications. Hosp Pract. (2018) 46:77–87. doi: 10.1080/21548331.2018.1437319
20. Giblin TB, Sinkowitz-Cochran RL, Harris PL, Jacobs S, Liberatore K, Palfreyman MA, et al. Clinicians' perceptions of the problem of antimicrobial resistance in health care facilities. Arch Intern Med. (2004) 164:1662–8. doi: 10.1001/archinte.164.15.1662
Keywords: antimicrobials, interviews, Malaysia, physicians, qualitative study, resistance
Citation: Akhtar A, Khan AH, Zainal H, Ahmad Hassali MA, Ali I and Ming LC (2020) Physicians' Perspective on Prescribing Patterns and Knowledge on Antimicrobial Use and Resistance in Penang, Malaysia: A Qualitative Study. Front. Public Health 8:601961. doi: 10.3389/fpubh.2020.601961
Received: 02 September 2020; Accepted: 27 October 2020;
Published: 25 November 2020.
Edited by:
Marco Cassone, University of Michigan, United StatesReviewed by:
Fahad Saleem, University of Balochistan, PakistanCopyright © 2020 Akhtar, Khan, Zainal, Ahmad Hassali, Ali and Ming. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Amer Hayat Khan, ZHJhbWVyMjAwNkBnbWFpbC5jb20=
†ORCID: Ali Akhtar orcid.org/0060-10-4231157
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.