 Martin C. Nwadiugwu
Martin C. Nwadiugwu
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Public Health, 25 January 2021
Sec. Clinical Diabetes
Volume 8 - 2020 | https://doi.org/10.3389/fpubh.2020.600427
Background: Diabetes is a long-term condition that can be treated and controlled but do not yet have a cure; it could be induced by inflammation and the goal of managing it is to prevent additional co-morbidities and reduce glycemic fluctuations. There is a need to examine inflammatory activities in diabetes-related angiopathies and explore interventions that could reduce the risk for future outcome or ameliorate its effects to provide insights for improved care and management strategies.
Method: The study was conducted in Embase (1946–2020), Ovid Medline (1950–2020), and PubMed databases (1960–2020) using the PICO framework. Primary studies (randomized controlled trials) on type 2 diabetes mellitus and inflammatory activities in diabetes-related angiopathies were included. Terms for the review were retrieved from the Cochrane library and from PROSPERO using its MeSH thesaurus qualifiers. Nine articles out of 454 total hits met the eligibility criteria. The quality assessment for the selected study was done using the Center for Evidence-Based Medicine Critical Appraisal Sheet.
Results: Data analysis showed that elevated CRP, TNF-α, and IL-6 were the most commonly found inflammatory indicator in diabetes-related angiopathies, while increased IL-10 and soluble RAGE was an indicator for better outcome. Use of drugs such as salsalate, pioglitazone, simvastatin, and fenofibrate but not glimepiride or benfotiamine reported a significant decrease in inflammatory events. Regular exercise and consumption of dietary supplements such as ginger, hesperidin which have anti-inflammatory properties, and those containing prebiotic fibers (e.g., raspberries) revealed a consistent significant (p < 0.05) reduction in inflammatory activities.
Conclusion: Inflammatory activities are implicated in diabetes-related angiopathies; regular exercise, the intake of healthy dietary supplements, and medications with anti-inflammatory properties could result in improved protective risk outcome for diabetes patients by suppressing inflammatory activities and elevating anti-inflammatory events.
Diabetes is a chronic condition with rising global prevalence that is associated with multimorbidity (1). It is linked with metabolic abnormalities such as increased oxidative stress, free radicals, accumulated free fatty acids in the blood, and the onset of inflammatory changes (2). There are currently no cures for diabetes and its signs and severity differ among people of different ethnic groups (2). The economic cost of treating diabetes increases with increasing age and even more so for clinically managing the disease and its associated comorbidities (3).
The clinical treatment goal in managing people with diabetes is to prevent the onset of associated co-morbidities by relieving symptoms, and controlling hyperglycemia and hypoglycemic episodes upon diagnosis (2). According to Reutrakul and Mokhlesi (4) people living with type 2 diabetes mellitus (T2DM) constitute about 90–95% of all people living with diabetes, and they often present several associations with hypertension, cardiovascular diseases, nephropathy, retinopathy, depression, inflammatory and neurodegenerative diseases, and so on, most of which are recognized when co-morbidities becomes evident (5). About 97.5% of people with T2DM have at least one co-morbid condition while about 88.5% have two or more additional disorders (6).
Although inflammation has been associated with diabetes (2), the key question remains on finding supporting strategies that prevent worsening outcome. Inflammation is a pathological process caused by diverse cytologic and chemical reactions (7). The hallmarks of inflammation are dysfunction and injury to tissues usually manifested by loss of function, heat, pain, and swelling (7). Damage to small blood vessels (diabetic microangiopathy) and to the larger vessels (diabetic macroangiopathy) generally referred to as diabetic angiopathy is the major vascular complication of diabetes (8). Diabetic microangiopathy includes diabetic retinopathy, nephropathy, and neuropathy, whereas complications from macroangiopathy include cardiovascular events such as heart attacks, strokes, and insufficient blood flow (8). Evidence from large randomized controlled trials (RCTs) have suggested that optimal metabolic control in T2DM could delay the onset of both diabetic micro and macroangiopathy (8). Moreover, changes in metabolic status such as changes in the status of cytokines in adipose tissues could increasingly alter insulin action (9). The accrual of circulating pro-inflammatory cytokines and reactive oxygen species (ROS) in prediabetes patients have been reported to disrupt intestinal barriers and compromise tight junctions between cells allowing for deleterious compounds to be increasingly absorbed (10).
Pro-inflammatory cytokine production activates myeloperoxidase enzymes and NADPH oxidase (NOX) involved in amino acid oxidation to produce advanced glycation end-product (AGE) precursors (11). Like pro-inflammatory cytokines, AGE is a biomarker for vascular complications (12); its production within the body is accelerated by oxidative stress, dyslipidemia, and hyperglycemic conditions associated with diabetes patients (13), and is particularly elevated in people who also have impaired renal function due to decreased urinary AGE excretion (14). The ability of the receptor for advanced glycation end-products (RAGE) to interact and bind with AGEs is thought to promote atherosclerosis, endothelial dysfunction, and has an inflammatory effect in diabetes complications by inducing lipid abnormalities, oxidative stress, and macrophage uptake via upregulation of inflammatory cytokines such as IL-1, IL-6, and TNF (15–17).
The objective of the study was to systematically review literature to investigate inflammatory activities in diabetes-related angiopathies and to explore beneficial interventions, as the evidence to support strategies to successfully cope with the chronic illness of T2DM is patchy, and the possibility for worsening condition or reversal substantial (18). The overarching aim of the study was to identify
1. Inflammatory activities in T2DM-related angiopathies and
2. Beneficial interventions for reducing the risk of inflammatory activities.
The remaining sessions of this study will discuss the methodology, search strategy, and quality assessment of the systematic review. Next, inflammatory activities and T2DM-related angiopathies will be overviewed in relation with findings from the selected studies. A narrative synthesis of the effect of interventions on measures of inflammation will be included. The study will conclude by summarizing the findings and how they may be beneficial for diabetes patients with co-morbid conditions.
This study reviewed only RCTs (19). Since the outcome of interest was to investigate inflammatory activities in diabetes-related angiopathies and explore beneficial interventions, articles from RCTs reporting inflammatory activities in people with diabetic angiopathies after an intervention or in comparison with an experimental group were of interest. The study was registered in PROSPERO (CRD42020204001).
Only articles from peer-reviewed journals published in English with a focus on human subjects (18+ years) and from any country were included. The timeline of study in the selected RCTs was at least 14 days. Included studies reported the outcome of an intervention on inflammatory markers, namely, drugs, dietary supplement, aerobic exercise, as well as blood glucose levels and risk for diabetic angiopathy. The significant differences in measures of inflammation after the intervention in each RCT were reported. Animal studies were excluded. The PICO framework used to define the eligibility criteria is seen below:
P—Population: type 2 diabetes patients
I—Exposure: inflammation
C—Comparison/control: healthy individuals
O—Outcome: diabetic angiopathies
Only RCTs on type 2 diabetes reporting inflammatory activities in diabetes-related angiopathies and beneficial interventions were eligible (see Table 1). Studies involving people who do not have diabetes or other types of diabetes were excluded. The search items can be seen in Table 2.
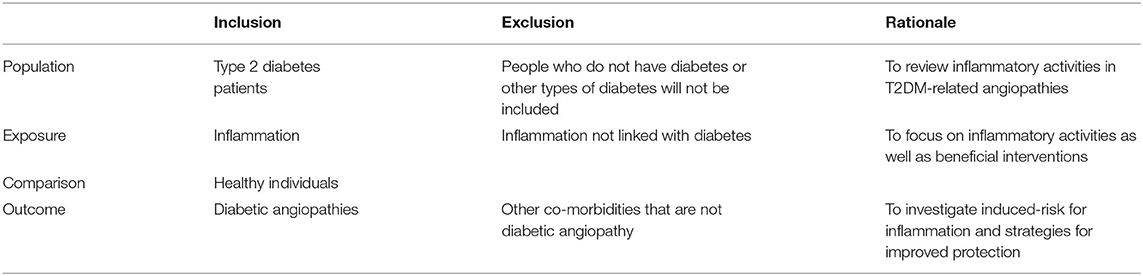
Table 1. Inclusion/exclusion criteria.
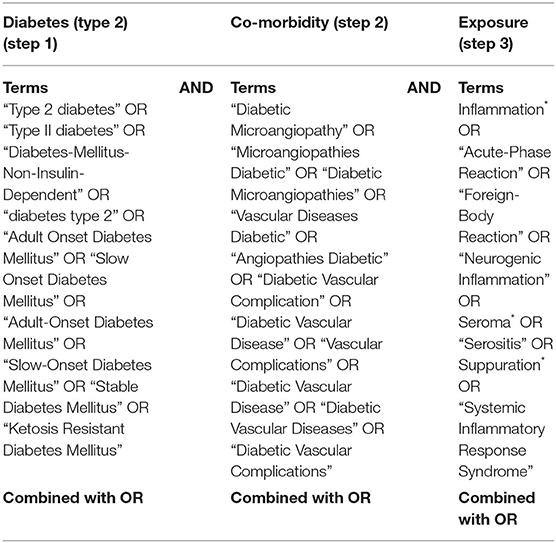
Table 2. Search items.
The review was conducted in Ovid Medline, Embase, and PubMed databases. Ovid Medline is a large database of healthcare, medicine, and scientific disciplines. PubMed is a biomedical and genomic database accessed from the National Center for Biotechnology Information (NCBI) platform, whereas Embase is a widely used biomedical and pharmacological bibliographic database hosted on Elsevier. Keywords for the population, exposure, and outcome were used to search each database. Terms for the population “type 2 diabetes patients” and outcome “diabetic angiopathies” were retrieved from the Cochrane library (20), whereas terms for the exposure “inflammation” were identified using PROSPERO MeSH thesaurus qualifiers (7). The terms can be seen in the database search history (Appendix 1: PubMed Queries; Appendix 2: Ovid Medline Queries; Appendix 3: Embase Query).
The key categories searched were diabetes (type 2), inflammation, and diabetic angiopathies. Synonyms for each key category generated were individually searched and then collectively combined with the “OR” logical operator. An intersection between the three key categories searched was done using the “AND” operator as shown in Table 2. The screening process from the three databases yielded 454 total hits and is presented in the PRISMA flow diagram in Figure 1. One hundred and ninety-one duplicates were removed after initial screening by titles and abstracts. Two-hundred and five articles were not included because they did not meet the eligibility criteria. Out of the 58 articles left, 49 were excluded for not fully meeting the selection criteria as they either only highlighted protocols or were about inflammation linked with other disorders. Nine RCTs met the inclusion criteria and were included in the narrative synthesis and quality appraisal of the findings.
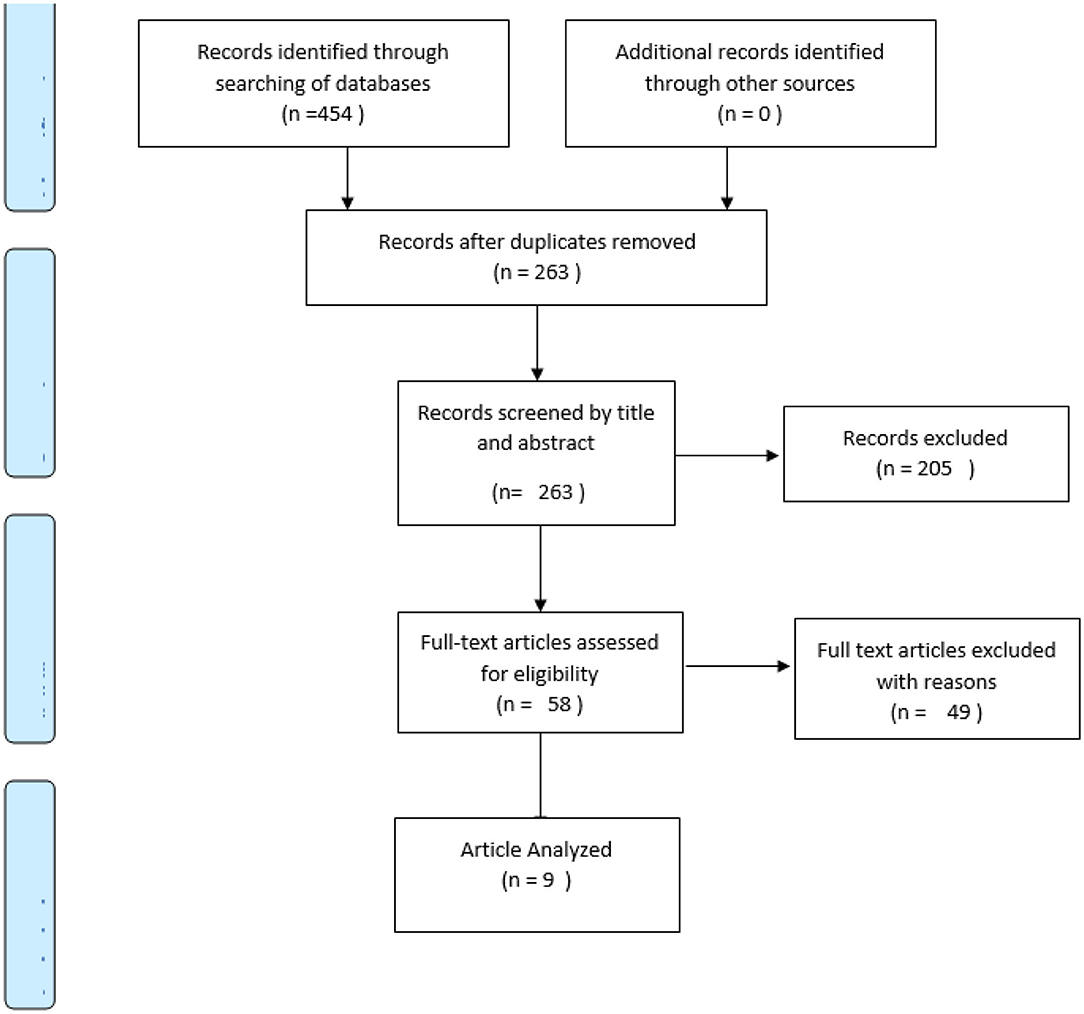
Figure 1. PRISMA flow diagram.
Data from the nine selected studies were extracted under these headings: name of author(s), year of publication, study design, co-morbidity type, inflammatory associations, methods, and intervention as seen in Table 3. The quality assessment of the selected studies was done using the Center for Evidence-Based Medicine Critical Appraisal Sheet (21). Data about the participants, interventions used for the RCTs, objectivity of the blind study, if the groups were similar and treated equally at the start of the trial, and validity of the outcome of treatment were examined using the CEBM appraisal sheet. The validity of the outcome of treatment for each study was rated “high,” “moderate,” or “low” based on the quality (22). The criteria for rating were lack of blinding, selective outcome reporting, and incomplete accounting of outcome events based on the GRADES guidelines by Guyatt et al. (22). Studies that did not meet all three criteria were considered as “high quality,” those that met only one were considered “moderate quality” while those that met two or more were considered “low quality.” Inflammatory mechanisms from the RCTs were analyzed and used in explaining the activities of inflammation in diabetes-related angiopathies.
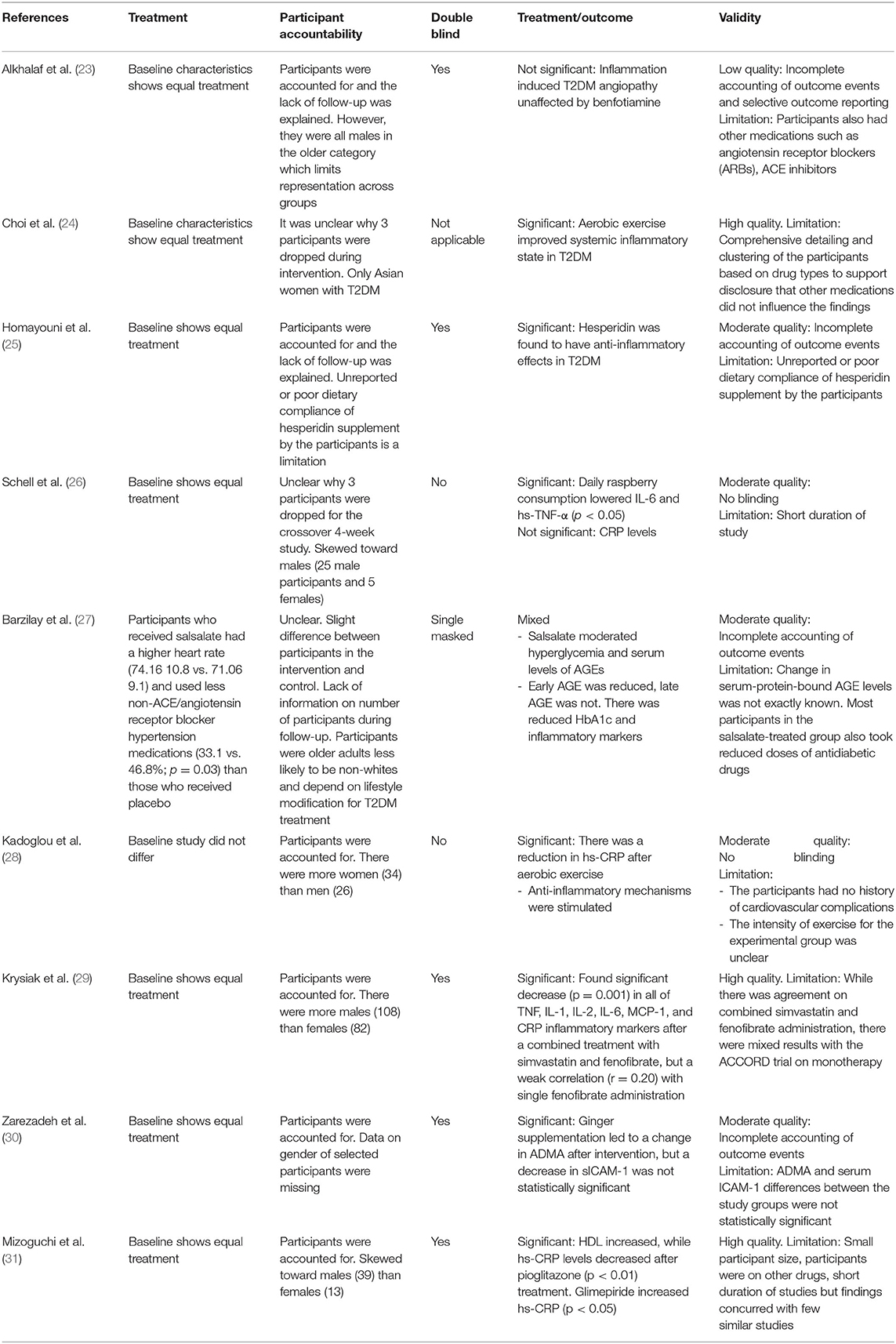
Table 3. Quality appraisal.
The result of the database search is presented in Table 4. From the selected studies in Table 5, the highlighted inflammatory activities were high-sensitivity C reactive protein (hs-CRP), myeloperoxidase (MPO), serum amyloid-A (sAA), tumor necrosis factor-alpha (TNF-α), interleukins (IL-1, IL-2, IL-6, IL-18, IL-10), soluble receptor for advanced glycation end-products (sRAGE), intercellular adhesion molecule-1 (ICAM-1), monocyte chemoattractant protein-1 (MPC-1), white blood cells (WBC), and total anti-oxidant capacity (TAC) (23). Hs-CRP was the most common inflammatory biomarker as it was measured by seven of the nine selected studies. This was closely followed by TNF-α (five times) and IL-6 (four times). TNF-α, IL-1β, IL-6, MCP-1, IL-2, and interferon-γ are some of the monocyte- and lymphocyte-derived pro-inflammatory cytokines (29). These cytokines including CRP are markers of chronic low-grade systemic inflammation and a prognostic indicator of vascular complications and increased cardiovascular risk (29). While IL-10 is an anti-inflammatory cytokine, IL-18 is a pro-inflammatory cytokine. The IL-18/IL-10 ratio represents the balance that foretells the incidence of coronary complications (32–34). The elevation of IL-18 promotes atherosclerosis by interferon-γ release which are balanced by IL-10 cytokines (32, 35). Thus, disequilibrium of IL-18/IL-10 ratio may promote atherosclerotic process.

Table 4. Database search results.
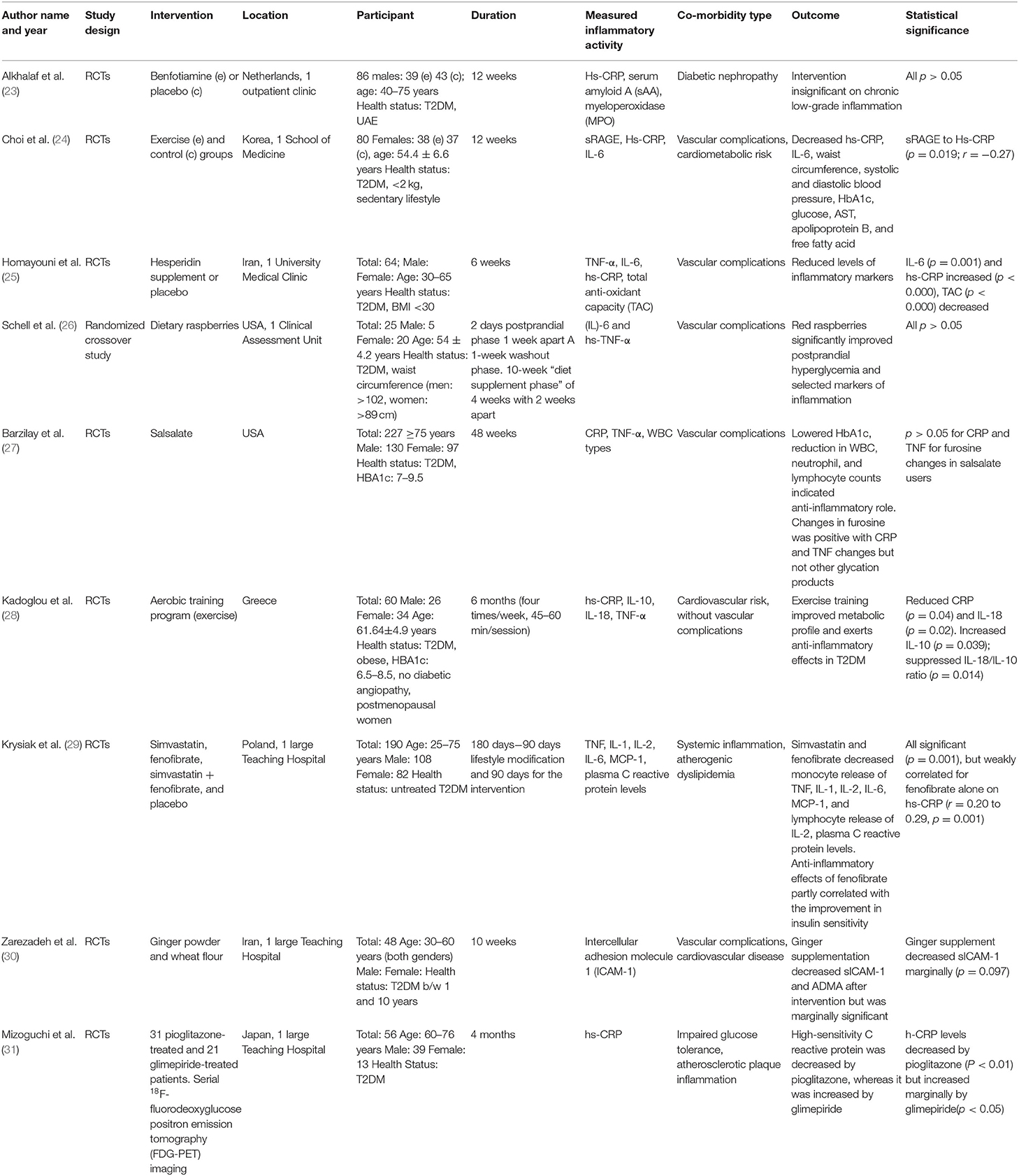
Table 5. Data extraction.
An overview of the findings from the nine selected studies (Table 5) shows that the interventions could be explained and grouped into three main categories: exercise, diet, and medication. Two studies (24, 28) investigated the effects of aerobic exercise on markers of inflammation (hs-CRP, sRAGE, IL-6, IL-10, IL-18) in T2DM participants with cardiovascular or cardiometabolic risk. Three studies (25, 26, 30) examined the effect of dietary supplements, while four studies (23, 27, 29, 31) investigated the use of medication as an intervention. A further overview and appraisal of each study under the appropriate category (exercise, diet, medication) is explored in the following section.
To understand inflammatory activities in T2DM, Choi et al. (24) explored the effects of exercise on inflammatory markers and soluble receptor for AGEs on 75 patients with T2DM for 12 weeks and found that, apart from the physical benefits of exercise that was observed such as a reduction in waist circumference, and loss of weight and body fat percentage leading to a reduction in risk factors for atherosclerosis and cardiometabolic diseases (e.g., decrease in blood pressure, free fatty acids, oxidative stress), there was a significant decrease in the levels of hs-CRP and an increase in soluble receptor for AGEs in the exercise group but not in the control group, which suggests that aerobic exercise improved systemic inflammatory state in T2DM. While the level of moderate intensity of the aerobic exercise may not be exactly quantified, the study found an independent association (R2 = 0.244) of age, glucose, cholesterol levels, and triglyceride with soluble receptor for AGEs (24). Although this is a weak association, it implies that aerobic exercise had a positive influence on glucose, cholesterol, and triglyceride levels. Similarly, Kadoglou et al. (28) found that aerobic exercise undertaken four times a week lessens the effect of inflammatory activities and improved anti-inflammatory markers after 6 months. The study reported improvement in glucose control, insulin resistance, and anti-inflammatory protection via increased IL-10 (4.14 ± 5.65 vs. −0.23 ± 4.73 pg/ml), and suppression of IL-18, and IL-18/IL-10 ratio (p > 0.05) in 60 overweight patients with T2DM who do not have vascular complications (28). Although TNF-α levels (p = 0.77) remained constant, hs-CRP was significantly decreased (p = 0.04) and was independent of significant alteration in IL-18 as the participants were reported to be on antidiabetic drugs (28). Also, systolic blood pressure was considerably improved (p < 0.05), while diastolic blood pressure decreased and IL-10 was elevated after the exercise program.
Exercise has been reported in previous studies to ameliorate cellular apoptosis, atherosclerotic plaque, tissue factor expression, and nuclear factor-κB activation (36–38). While these findings are revealing and an enhancement of IL-10 levels were reported in T2DM participants by Kadoglou et al. (28) after exercise training, the participants had no history of cardiovascular complications which limits the study conclusions for aerobic exercise as an intervention for protective risk outcome in diabetic angiopathy. Taken together, the study by Choi et al. (24) and Kadoglou et al. (28) reported a reduction in hs-CRP after an aerobic exercise; Choi et al. (24) found a statistically significant difference (p < 0.013) in the levels of hs-CRP measured at the start and end of the study, while Kadoglou et al. (28) reported a 39.6% reduction in hs-CRP (p < 0.04) at the end of the aerobic exercise. Choi et al. (24) also reported a statistically significant difference (p < 0.05) in the levels of IL-6 for the exercise group compared with the control. While participants in the study by Choi et al. (24) had both vascular and cardiometabolic risk, those in Kadoglou et al. (28) were reported to have only cardiovascular risk. The anti-inflammatory effects of exercise seemed to result in greater significant effect size as it correlated to decreased HbA1c and blood pressure, and was negatively correlated with increased soluble receptor for AGEs which suggest that aerobic exercise improved systemic inflammatory state in T2DM.
Dietary supplements such as ginger powder, dietary raspberries, and hesperidin were the intervention used by Zarezadeh et al. (30), Schell et al. (26), and Homayouni et al. (25), respectively, to investigate intervention effectiveness on inflammatory activities linked with vascular complications. Schell et al. (26) and Homayouni et al. (25) found a significant reduction (p < 0.05) in levels of IL-6, TNF-α, and hs-TNF, while Zarezadeh et al. (30) reported that ginger supplement decreased serum ICAM-1 marginally, serum ICAM-1 has previously been associated with the pathogenesis of cardiovascular disease in T2DM. Schell et al. (26) did not find a significant difference in CRP after red raspberries were consumed, but reported that daily raspberry consumption for a period of 4 weeks showed a consistently significant lowering effect (p < 0.05) on IL-6 and high-sensitivity TNF-α (hs-TNF-α) at 4 h postprandial after meal.
Furthermore, hesperidin was suggested to have anti-inflammatory effects in T2DM as there was a significant difference (p < 0.05) in TNF-α, hs-CRP, and IL-6 inflammatory markers between the control and experimental groups of the RCT that investigated the consumption of hesperidin supplement and its effect on blood pressure and inflammatory activities on 64 T2DM patients (25). A statistically significant (p = 0.001) decrease in levels of TNF-α and IL-6 (p = 0.034) markers of inflammation, respectively, was reported, but no difference in the mean hs-CRP, rather an increased serum total antioxidant capacity (TAC) at the end in comparison with baseline values was reported. In addition, the percent change of TNF-α, IL-6, and hs-CRP levels were significantly reduced in the treated group compared with the control (p < 0.05), indicating that hesperidin has anti-inflammatory effects in T2DM (25). Although the study reported repeated assessment of dietary components and showed that hesperidin may improve TAC and reduce inflammation in patients with T2DM, unreported or poor dietary compliance of hesperidin supplement by the participants, the inability to measure antioxidant enzymes and serum nitric oxide (NO) level, and lack of intention-to-treat analysis could have limited the study findings (25).
The long- and short-term hesperidin administration have been reported to have anti-hypertensive effects and to stimulate NO production via phosphorylation of enzymes that mediate its output in vascular endothelial cells (39, 40). Hesperidin probably controls vascular tone by increasing vasorelaxing factors like NO or other tone modulating products such as NADPH oxidase (41, 42). It is believed that the onset of ROS disrupts NO production and leads to an increase in prostaglandin-like compounds that are suggested to have proinflammatory actions (25). The anti-inflammatory and antioxidant benefits of hesperidin are strongly correlated with hypertension and oxidative stress; (43) and it has been reported that hesperidin represses ROS-generating enzymes (43–45). It is important that ROS are repressed because inflammation in diabetic condition is induced by elevated ROS (25) which promotes the pathogenesis of cardiovascular disease in people with T2DM, and this can be measured through changes in ICAM-1 (inter-cellular adhesion molecule-1) and ADMA (asymmetric dimethylarginine) biomarkers (30).
A significant difference in ADMA serum levels (p = 0.002) and a marginal change in serum ICAM-1 (p = 0.097) were reported in the ginger supplementation group by Zarezadeh et al. (30) in the study to determine the effect of ginger supplementation on ICAM-1 serum levels and ADMA in 45 patients with T2DM after 10 weeks. In the same study, another intervention group received wheat flour, but the ADMA and serum ICAM-1 differences between the groups were not statistically significant, giving slight credence to ginger as a possible intervention. The study by Zarezadeh et al. (30) was conducted in a University hospital in Iran and did not include information on the participant's gender (30). Similarly, the study by Homayouni et al. (25) which was also conducted in a University hospital in Iran had no information on the participant's gender, but that by Schell et al. (26) carried out in a clinical assessment unit in the USA had gender information and the selected participants consisted of more males (25) than females (5).
A handful of studies have investigated the anti-inflammatory effect of medication on measures of inflammation. Alkhalaf et al. (23) studied the outcome of benfotiamine intervention in atherosclerotic plaque inflammation. The investigation of benfotiamine and its effect on markers of low-grade inflammation in 39 T2DM patients with nephropathy who had high-normal urinary albumin excretion(UAE) and UAE in the microalbuminuric range (15–300 mg/24 h) found no significant change in hs-CRP, MPO, and sAA compared with the control group after 12 weeks (23). Markers of endothelial dysfunction and AGE yielded insignificant results, suggesting that inflammation-induced vascular complications in T2DM are unaffected by benfotiamine (23), although the patients were found to have had other medications such as angiotensin receptor blockers (ARBs) and ACE inhibitors which might have introduced confounding. While Alkhalaf et al. (23) found no significant difference in hs-CRP, sAA, and MPO between the benfotiamine or placebo-treated groups, Mizoguchi et al. (31) reported that hs-CRP levels decreased after pioglitazone (p < 0.01) treatment but increased marginally by glimepiride (p < 0.05), and the increasing hs-CRP levels were associated with atherosclerotic plaque inflammation. However, the small number of participants on pioglitazone (31 patients), some who were on other medications such as statins, aspirin, and renin–angiotensin system inhibitors, could potentially have introduced confounding variables that may interact with the efficacy of the intervention via drug–drug interaction (46). The short duration of the study and the fact that only atherothrombotic stroke was of interest is a limitation of the generalizability of the study with regards to diabetic angiopathies (31).
In a similar experiment to investigate the outcome of pioglitazone treatment, Mizoguchi et al. (31) found increased high-density lipoprotein (HDL) upon pioglitazone administration, though when compared with glimepiride, a stepwise multiple regression analysis considered this independent in association with inflammation-induced atherosclerosis. The attenuation of atherosclerotic plaque inflammation may be associated with increased HDL levels as previous findings reported increased HDL cholesterol levels after statin administration, but decreased plaque inflammation in dyslipidemic patients (47). HDL cholesterol promotes antioxidant, anti-inflammatory events attenuating atherosclerosis (31), and high level of HDL can reduce the odds of T2DM patients developing microvascular retinopathy and renal disease (48). In contrast, the AIM-HIGH clinical trial result found no cardiovascular benefit in 34% of its participants with T2DM despite a noticeable increase in HDL cholesterol level (49). The observation that atherosclerotic plaque inflammation–attenuating properties of pioglitazone could be largely ascribed to its HDL-increasing property rather than its hs-CRP-lowering property suggests a difference in systemic and plaque inflammation, and that hs-CRP, a marker for chronic systemic inflammation, may not reflect plaque inflammation (31). Nevertheless, the study suggests that pioglitazone could be a potent intervention in attenuating inflammation-induced atherosclerosis.
The findings on salsalate treatment and the outcome from combined treatment with simvastatin and fenofibrate were insightful and beneficial. Barzilay et al. (27) in a 48-week TINSAL-T2D study found that salsalate moderated hyperglycemia and serum levels of AGEs which are involved in diabetes-related vascular complications after 118 out of 207 total participants received 3.5 g/day of salsalate (27). A noticeable significant change (p > 0.05) in WBC and furosine but not in other glycation products for CRP and TNF in salsalate users was reported (27). Although Barzilay et al. (27) stated that the reasons for not detecting a change in serum-protein-bound AGE levels were not exactly known, the fact that AGE could have multiple pathways, that metformin was taken by most participants, and that the salsalate-treated participants with hypoglycemic events were receiving reduced antihyperglycemic medications were suggested as a possible explanation. Barzilay et al. (27) found that salsalate had no effect on late AGEs but reduced early AGEs and had a significant lowering effect on HbA1c; however, there was an increase in serum pentosidine (an AGE) indicating the possibility of induced oxidative stress, while changes in markers of inflammation or renal factors were independent of changes in pentosidine and glycation factors.
Interestingly, Krysiak et al. (29) in a separate study found a significant decrease (p = 0.001) in all of TNF, IL-1, IL-2, IL-6, MCP-1, and CRP inflammatory activities after a combined treatment with simvastatin and fenofibrate, but a weak correlation (r = 0.20) with single fenofibrate administration. The study, which involved 196 T2DM participants with mixed dyslipidemia, reported that the medications exerted a similar but more efficacious effect on systemic inflammation after combined administration (29). However, single administration of simvastatin reduced monocyte release of pro-inflammatory cytokines such as TNF-α, IL-1β, IL-6, and monocyte chemoattractant protein-1 (MCP-1); and lymphocyte release of IL-2, interferon-γ, and TNF-α; including a decrease in plasma CRP levels, while single administration of fenofibrate had anti-inflammatory effects that correlated with improved insulin sensitivity and downregulation of lymphocytes rather than monocytes (29). Lymphocytes and monocytic cells are present in atherosclerotic plaques and are very well associated with the progression of atherosclerosis (50–52).
Assessment of the RCTs using medication as an intervention showed that none of the four studies were multi-country and majority of the selected participants were males; for example, the RCT by Alkhalaf et al. (23) was conducted in an outpatient clinic in the Netherlands and all participants were males which limits the conclusion for females. The representation of gender was skewed toward the male in the other studies; for example, selected participants in the study by Krysiak et al. (29) had 108 males and 82 females. Also, Barzilay et al. (27) had 130 male and 97 female participants, while there were 39 males and 13 females in the study by Mizoguchi et al. (31). All participants had T2DM; however, participants in the study by Alkhalaf et al. (23) also had UAE, while those in the RCT conducted by Krysiak et al. (29) had untreated T2DM. These additional disorders may represent confounding factors which may not have been accounted for by the RCTs.
Diabetic angiopathies can be induced by low-grade inflammation, AGEs, and endothelial dysfunction which are considered intermediate pathways (23). TNF-α, IL-1β, IL-6, MCP-1, IL-2, and interferon-γ are some of the monocyte- and lymphocyte-derived pro-inflammatory cytokines (29); these cytokines as well as CRP are markers of chronic low-grade systemic inflammation and prognostic indicators of vascular complications and increased cardiovascular risk (29). The risk for vascular complications and the extent of insulin resistance have been linked with changes in the levels of these inflammatory markers (53–55). Inflammation just like hyperglycemia, is an integral process leading to atherosclerosis and increased risk of atherosclerotic cardiovascular disease (31). However, there is little evidence to suggest that a particular oral anti-diabetic medication is the preferred intervention to ameliorate inflammation-induced atherosclerosis or angiopathies (31). Drugs such as pioglitazone, simvastatin, and fenofibrate, and non-acetylated salicylate such as salsalate but not benfotiamine suggested benefits in moderating vascular complications (23, 27, 29, 31).
Benfotiamine had been previously suggested as a therapy for diabetic nephropathy and other related complications through its activation of transketolase for the inhibition of AGE precursors, low-grade inflammation, and endothelial dysfunction in an experiment using animals with diabetes (56, 57). Transketolase, an enzyme involved in the breakdown of glucose, plays a role in inhibiting vascular complications (58, 59), and although Alkhalaf et al. (23) reported a significant increase in transketolase activity (a co-factor of thiamine), no significant findings from benfotiamine administration across the two study groups were observed, suggesting that further long-term studies are needed to understand the pathway and mechanisms of its action in humans (56). The study by Alkhalaf et al. (23) was one of the few papers that reported findings on measures of inflammatory markers after benfotiamine administration.
Nonetheless, the TINSAL-T2D study found that salsalate treatment did not overly change most AGE levels (27). However, pioglitazone was found to ameliorate inflammation-induced atherosclerosis in T2DM. Mizoguchi et al. (31) evaluating the effect of 0.5–4.0 mg glimepiride and 15–30 mg pioglitazone intervention on atherosclerotic plaque inflammation after 4 months, found that both interventions decreased HbA1c, but only pioglitazone ameliorated inflammation-induced atherosclerosis. This result agreed with the PERISCOPE and CHICAGO studies that showed that when compared with glimepiride, pioglitazone prevented the continuous development of carotid or coronary atherosclerosis after 18 months of treatment (60, 61), providing evidence for pioglitazone as a protective risk factor for diabetes-related angiopathies. Furthermore, the use of simvastatin, a drug with anti-inflammatory properties (29, 62, 63), and fenofibrate was found to be a clinically relevant medication in the treatment of low-grade inflammation for the prevention of atherosclerosis (29).
Nevertheless, there are contrasting findings on fenofibrate intervention in other studies. For example, the FIELD and BIP trial studies on lowering events in diabetes found that fibrate significantly decreased cardiovascular risk by only 19 and 17%, respectively; although there was a decrease in mortality and nonfatal heart attack, the result was not significant (64). In addition, the Action to Control Cardiovascular Risk in Diabetes Lipid trial (ACCORD) after a 10-year study reported decreased cerebrovascular risks in middle-aged and older T2DM patients using simvastatin intervention alone or in combination with fenofibrate (65). The difference between the findings by Krysiak et al. (29) and the ACCORD trial was on the superior potency of the combination of simvastatin and fenofibrate compared with monotherapy. The ACCORD trial highlighted the potency of simvastatin as well as in combination with fenofibrate, while Krysiak et al. (29) reported that both combined and monotherapy administration of simvastatin and fenofibrate equally affected monocyte cytokine release, but only the combined medication decreased lymphocyte cytokine release and improved lipid profile. These differences could be associated with the characteristics of the participants as Krysiak et al. (29) included lifestyle modification and metformin in the study of a small number of newly diagnosed patients with T2DM who also had dyslipidemia, and administered the combined therapy at reduced dosage for a shorter period, unlike the ACCORD trial that was a 10-year study.
The role of systemic inflammation in T2DM-related vascular complications have been linked with low levels of soluble receptor for AGEs (24) and chronic inflammation which is correlated with increasing risk for cardiovascular events (28). Soluble RAGE was suggested to ameliorate the adverse and inflammatory action of RAGE, and patients with T2DM have been reported to have low levels of circulating soluble RAGE (66, 67). The circulating soluble RAGE has an indirect relationship with insulin resistance, HbA1c, and CRP, making it a marker and predictor for inflammation and cardiovascular events (68, 69). The report on lower systemic inflammation due to the induction of soluble RAGE in patients with T2DM by Choi et al. (24) is consistent with other studies by Arikawa et al. (70), Nadar and Lundberg (71), and Riesco et al. (72) all of whom reported significant decrease in CRP and IL-6 levels after 4–6 months of regular exercise. The precise fundamental process responsible for generating soluble RAGE via regular exercise remains unclear (24).
Accordingly, pro-inflammatory markers such as IL-18 are elevated in diabetes and strongly considered as an independent predictor of adverse cardiovascular events (73, 74). The alterations in IL-18 were positively linked with changes in insulin resistance in one of the selected studies (28), and other studies have reported changes in IL-18 levels influenced by lifestyle modification such as exercise (28, 75). The process in which exercise lowers IL-18 concentration is probably by modifying insulin signaling or downregulating cytokine production decreasing inflammatory cell infiltration of adipose tissues (76); however, determining the association of the cause and effect still remains unclear (28). In contrast, anti-inflammatory serum levels of IL-10 secreted by T cells of Th2 subtype, macrophages, and monocytes in humans have been shown to cancel out the risk of cardiac events (33).
Inflammation independently induces the risk for hypertension (25, 77, 78). Modern diets are said to be replete with AGEs which are generated during food processing and have been implicated in the pathogenesis of diabetes-related disorders due to their ability to activate chronic low-grade inflammation and insulin resistance (79). The speed at which AGEs increase in amount in the body differs among people and is dependent on lifestyle such as cigarette smoking, consumption of AGE-rich diet, age, and metabolic health of an individual (79). The consumption of AGE-rich diet (e.g., fried meats, glycated proteins, toasted wheat flakes, etc.) leads to the proliferation of pathogenic colonic bacteria; therefore, eating healthy diets low in AGE may reduce AGE accumulation from exogenous sources. Yet, the difficulty is in resisting and overcoming the temptation to consume those meals as AGE-rich diets have enhanced aroma, flavor, and color (80). One solution has been the supplementation with prebiotic fibers which improve optimal gut microbial balance to inhibit AGE in people at risk of T2DM (79). Prebiotic fibers such as inulin and raspberries could reduce the glycemic index of a diet, slow the absorption of intestinal nutrient, and delay gastric emptying (79).
Dietary interventions geared at preventing the progression of inflammatory activities are necessary to attenuate diabetes-related angiopathies. Hesperidin, ginger, and dietary raspberry supplementation from the selected studies were suggested as dietary supplements that could ameliorate the effect of inflammation and AGEs (25, 26, 30). Hesperidin inhibits the production of inflammatory cytokines that increase arterial stiffness and peripheral vascular resistance which are indications for hypertension and vascular complications (24). Raspberries are prebiotic fibers whose products may lower the absorption of exogenous AGE in the gut and inhibit circulating proinflammatory cytokines; they can also induce changes that enhance gut barrier functioning by elevating the production of glucagon-like peptide 2 (GLP-2) which promotes an increase in crypt cells (79, 81, 82). Food supplements like ginger have been reported to have anti-inflammatory and anti-oxidant properties (30) which lowers ADMA, which when elevated decreases NO production leading to decreased blood supply to peripheral tissues (30).
An increase in ADMA promotes the activation of nuclear factor kappa B (NF-κB) transcription factor which is associated with increased ICAM-1 and proinflammatory cytokine production (30). ICAM-1 is a protein expressed through NF-κB pathway in endothelial cells and leukocytes (30). ADMA makes the NF-κB pathway active, leading to increased ICAM-1 (83). ADMA and ICAM-1 play a role in diabetes-related cardiovascular complications and insulin resistance level as they are involved in pathway association with oxidative stress, NO inhibition, increased blood pressure, and inflammation (84–87). During inflammatory conditions, leukocytes produce and attach ICAM-1 protein to endothelial cells promoting macrophage production of foam cells (88). Therefore, inhibition of NF-κB transcription factor, ADMA, and ICAM-1 could prevent cardiovascular complications in T2DM (30).
Taken all together, there was limited information on participant compliance during the interventions. Also, not all studies included information on gender and disclosed the current medication in the baseline characteristics of the participants at the beginning and end of the study, especially because the participants were known T2DM patients. Most studies had more male participants and were not multi-country, implying lack of diversity in racial origin and ethnicity which could potentially limit the representation of the conclusions. It is important to note that the selected studies looked at interventions on inflammatory activities in people with diabetes. Moreover, the data selection was done by a single reviewer but verified by another reviewer for consistency. The small sample size of participants and limited RCTs on inflammatory activities in T2DM-related comorbidities is a limitation. However, the study contributes to medical knowledge and education for carers and people with diabetes-related angiopathies by reviewing information on how intake of healthy dietary supplements, aerobic exercise, and anti-inflammatory medications can improve protection from future risk by highlighting beneficial interventions that may lower the potential for negative outcomes.
Elevated inflammatory activities and its association pathways such as endothelial dysfunction and AGEs have been reported in diabetes-related vascular disorders. TNF-α and IL-6 were the most common proinflammatory cytokines from the selected studies; together with CRP, their alterations represent an important biomarker for accessing inflammatory activities in diabetic angiopathies. The activities of IL-10, an anti-inflammatory cytokine, is helpful in accessing reduced risk for induced inflammation in diabetes-related angiopathies. Regular aerobic exercise, medications that decrease proinflammatory activities, as well as diet rich in prebiotic fibers and those possessing anti-inflammatory properties were suggested as a means of attenuating the risk of increased proinflammatory events.
A summary of knowledge from the findings suggested that salsalate treatment could reduce inflammatory activity but may not change AGE levels which is linked to oxidative stress because markers of serum inflammation only indirectly reflect oxidative stress. The single administration of simvastatin was found to downregulate monocytic and lymphocytic release of proinflammatory markers, whereas fenofibrate only reduced markers of lymphocytic inflammation. The administration of both drugs were suggested to halt the progression of diabetes-related atherosclerosis because lymphocytes and monocytic cells are present in atherosclerotic plaques. Similarly, pioglitazone was found to prevent the continuous progression of inflammation-induced atherosclerosis by increasing HDL and lowering hs-CRP levels, indicating its involvement in reducing systemic and plaque inflammation.
Finally, while it is known that changes in metabolic status and cytokines could increasingly alter insulin action, and that exercise may lower cellular apoptosis and atherosclerotic plaque, not much of this has been studied with regards to people with T2DM and existing angiopathies or on the effectiveness of various food supplements. In this study, aerobic exercise was shown to reduce risk factors associated with vascular and cardiometabolic risk by increasing soluble RAGE which interacts with AGE, a known promoter of atherosclerosis in diabetes condition. Indeed, the review showed that regular exercise increases anti-inflammatory activities and reduces proinflammatory events and mediators of oxidative stress such as AGE which is high in AGE-rich diets. Prebiotic fibers such as raspberries lower the absorption of AGEs in the gut, while ginger and hesperidin lower inflammatory activities that promote cardiovascular and vascular complications by suppressing ADMA, regulating ICAM-1, and stimulating DDAH and NO production. Thus, medication and healthy dietary supplements with anti-inflammatory properties, along with regular exercise, may result in beneficial outcome for diabetes patients.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author/s.
MN devised the conceptual ideas and wrote the article.
The author declares that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author would like to acknowledge Emma France for reviewing the article.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2020.600427/full#supplementary-material
AIM-HIGH, Atherothrombosis Intervention in Metabolic Syndrome with Low HDL/High Triglycerides: Impact on Global Health Outcomes Trial; HbA1c, hemoglobin A1c; hs-CRP, high-sensitivity C reactive protein; TNF-α, umor necrosis factor-alpha; IL, interleukin; sRAGE, soluble receptor for advanced glycation end-products; sAA, serum amyloid A; ICAM-1, intercellular adhesion molecule 1; MPC-1, monocyte chemoattractant protein-1; WBC, white blood cell; TAC, total antioxidant capacity; MPO, myeloperoxidase; T2DM, type 2 diabetes mellitus; T1DM, type 1 diabetes mellitus; TINSAL-T2D, Targeting Inflammation Using Salsalate for Type 2 Diabetes.
1. Khaledi M, Haghighatdoost F, Feizi A, Aminorroaya A. The prevalence of comorbid depression in patients with type 2 diabetes: an updated systematic review and meta-analysis on huge number of observational studies. Acta Diabetologica. (2019) 56:631–50. doi: 10.1007/s00592-019-01295-9
2. Vaisman N, Mordechai K. The medical research infrastructure and health services fund of the Tel Aviv Medical Center. Tel Aviv. (2015) Novel assay for monitoring glucose balance and oxidative stress, US 2015/0299790 A1.
3. Zhuo X, Zhang P, Hoerger TJ. Lifetime direct medical costs of treating type 2 diabetes and diabetic complications. Am J Prev Med. (2013) 45:253–61. doi: 10.1016/j.amepre.2013.04.017
4. Reutrakul S, Mokhlesi B. Obstructive sleep apnea and diabetes: a state of the art review. Chest. (2017) 152:1070–86. doi: 10.1016/j.chest.2017.05.009
5. Haljas K. Depression, Daylight and Diabetes: Shared Genetic background and Genomic Moderation of Associations. (2019). Available online at: https://helda.helsinki.fi/bitstream/handle/10138/299825/DEPRESSI.pdf?sequence=1&isAllowed=y (accessed August 25, 2020).
6. Iglay K, Hannachi H, Howie P, Xu J, Li X, Engel S. Prevalence and co-prevalence of comorbidities among patients with type 2 diabetes mellitus. Curr Med Res Opin. (2016) 32:1243–52. doi: 10.1185/03007995.2016.1168291
7. National Institute for Health Research NIHR. PROSPERO MeSH Page: Inflammation. (2020). Available online at: https://www.crd.york.ac.uk/PROSPERO/MeSHPage.asp (accessed August 25, 2020).
8. WHO. Complications of Diabetes. (2020). Available online at: https://www.who.int/diabetes/action_online/basics/en/index3.html (accessed August 25, 2020).
9. Tsalamandris S, Antonopoulos AS, Oikonomou E. The role of inflammation in diabetes: current concepts and future perspectives. Eur Cardiol Rev. (2019) 14:50–9. doi: 10.15420/ecr.2018.33.1
10. Rapin JR, Wiernsperger N. Possible links between intestinal permeability and food processing: a potential therapeutic niche for glutamine. Clinics. (2010) 65:635–43. doi: 10.1590/S1807-59322010000600012
11. Anderson MM, Heinecke JW. Production of N(epsilon)-(carboxymethyl) lysine is impaired in mice deficient in NADPH oxidase: a role for phagocyte-derived oxidants in the formation of advanced glycation end products during inflammation. Diabetes. (2003) 52:2137–43. doi: 10.2337/diabetes.52.8.2137
12. Lisanne C, Joop D, Robin PF. Advanced glycation end products: an emerging biomarker for adverse outcome in patients with peripheral artery disease. Atherosclerosis. (2016) 254:291–9. doi: 10.1016/j.atherosclerosis.2016.10.012
13. Sebekova K, Boor P, Valachovicova M. Association of metabolic syndrome risk factors with selected markers of oxidative status and microinflammation in healthy omnivores and vegetarians. Mol Nutr Food Res. (2006) 50:858–68. doi: 10.1002/mnfr.200500170
14. Vlassara H, Uribarri J, Cai W. Advanced glycation end product homeostasis: exogenous oxidants and innate defenses. Ann N Y Acad Sci. (2008) 1126:46–52. doi: 10.1196/annals.1433.055
15. Thornalley PJ. Cell activation by glycated proteins AGE receptors, receptor recognition factors and functional classification of AGEs. Cell Mol Biol. (1998) 44:1013–23.
16. Neumann A, Schinzel R, Palm D. High molecular weight hyaluronic acid inhibits advanced glycation endproduct-induced NF-kB activation and cytokine expression. FEBS Lett. (1999) 453:283–7. doi: 10.1016/S0014-5793(99)00731-0
17. Cai W, He JC, Zhu L. High levels of dietary advanced glycation end products transform low-density lipoprotein into a potent redox-sensitive mitogen-activated protein kinase stimulant in diabetic patients. Circulation. (2004) 110:285–91. doi: 10.1161/01.CIR.0000135587.92455.0D
18. WHO Global repot on diabetes (2016). Available online at: https://apps.who.int/iris/bitstream/handle/10665/204871/9789241565257_eng.pdf;jsessionid=521F99636581BC06AED4E80B500BD929?sequence=1 (accessed August 25, 2020).
19. Centre for Evidence Based Medicine (CEBM) Study design (2020). Available online at: https://cebm.net/2014/04/study-designs (accessed August 25, 2020).
20. Cochrane Library. Definition: Diabetes Mellitus. (2020). Available online at: https://www.cochranelibrary.com/advanced-search/mesh (accessed August 25, 2020).
21. Centre for Evidence Based Medicine (CEBM). Randomized Controlled Trials (RCT) Critical Appraisal Sheet. (2020). Available online at: http://cebm.net/2014/06/critical-appraisal (accessed August 25, 2020).
22. Guyatt GH, Oxman AD, Vist G. GRADE guidelines: 4. rating the quality of evidence—study limitations (risk of bias). J Clin Epidemiol. (2011) 4:407–15. doi: 10.1016/j.jclinepi.2010.07.017
23. Alkhalaf A, Kleefstra N, Groenier KH. Effect of benfotiamine on advanced glycation endproducts and markers of endothelial dysfunction and inflammation in diabetic nephropathy. PLoS ONE. (2012) 7:e0040427. doi: 10.1371/journal.pone.0040427
24. Choi KM, Han KA, Ahn HJ. Effects of exercise on sRAGE levels and cardiometabolic risk factors in patients with type 2 diabetes: a randomized controlled trial. J Clin Endocrinol Metab. (2012) 97:3751–8. doi: 10.1210/jc.2012-1951
25. Homayouni F, Haidari F, Hedayati M. Blood pressure lowering and anti-inflammatory effects of hesperidin in type 2 diabetes; a randomized double-blind controlled clinical trial. Phytother Res. (2018) 32:1073–9. doi: 10.1002/ptr.6046
26. Schell J, Betts NM, Lyons TJ. Raspberries improve postprandial glucose and acute and chronic inflammation in adults with type 2 diabetes. Ann Nutr Metab. (2019) 74:165–74. doi: 10.1159/000497226
27. Barzilay JI, Jablonski KA, Fonseca V. The impact of salsalate treatment on serum levels of advanced glycation end products in type 2 diabetes. Diabetes Care. (2014) 37:1083–91. doi: 10.2337/dc13-1527
28. Kadoglou NPE, Iliadis F, Angelopoulou N. The anti-inflammatory effects of exercise training in patients with type 2 diabetes mellitus. Eur J Cardiovasc Prevent Rehabil. (2007) 14:837–43. doi: 10.1097/HJR.0b013e3282efaf50
29. Krysiak R, Gdula-Dymek A, Okopien B. Effect of simvastatin and fenofibrate on cytokine release and systemic inflammation in type 2 diabetes mellitus with mixed dyslipidaemia. Am J Cardiol. (2011) 107:1010-1018.e1. doi: 10.1016/j.amjcard.2010.11.023
30. Zarezadeh M, Saedisomeolia A, Khorshidi M. Asymmetric dimethylarginine and soluble inter-cellular adhesion molecule-1 serum levels alteration following ginger supplementation in patients with type 2 diabetes: a randomized double-blind, placebo-controlled clinical trial. J Comp Integr Med. (2019) 16. doi: 10.1515/jcim-2018-0019
31. Mizoguchi M, Tahara N, Tahara A. Pioglitazone attenuates atherosclerotic plaque inflammation in patients with impaired glucose tolerance or diabetes a prospective, randomized, comparator-controlled study using serial FDG PET/CT imaging study of carotid artery and ascending aorta. JACC Cardiovasc Imaging. (2011) 4:1110–8. doi: 10.1016/j.jcmg.2011.08.007
32. Chalikias GK, Tziakas DN, Kaski JC. Interleukin-18: interleukin-10 ratio and in-hospital adverse events in patients with acute coronary syndrome. Atherosclerosis. (2005) 182:135–43. doi: 10.1016/j.atherosclerosis.2005.02.002
33. Heeschen C, Dimmeler S, Hamm CW, Fichtlscherer S, Boersma E, Simoons ML. Serum level of the anti-inflammatory cytokine interleukin-10 is an important prognostic determinant in patients with acute coronary syndromes. Circulation. (2003) 107:2109–14. doi: 10.1161/01.CIR.0000065232.57371.25
34. Chalikias GK, Tziakas DN, Kaski JC. Interleukin-18/interleukin-10 ratio is an independent predictor of recurrent coronary events during a 1-year follow-up in patients with acute coronary syndrome. Int J Cardiol. (2007) 117:333–9. doi: 10.1016/j.ijcard.2006.05.017
35. Reddy P. Interleukin-18: recent advances. Curr Opin Hematol. (2004) 11:405–10. doi: 10.1097/01.moh.0000141926.95319.42
36. Tedgui A, Mallat Z. Anti-inflammatory mechanisms in the vascular wall. Circ Res. (2001) 88:877–87. doi: 10.1161/hh0901.090440
37. Smith DA, Irving SD, Sheldon J. Serum levels of the antiinflammatory cytokine interleukin-10 are decreased in patients with unstable angina. Circulation. (2001) 104:746–9. doi: 10.1161/hc3201.094973
38. Sriwijitkamol A, Christ-Roberts C, Berria R. Reduced skeletal muscle inhibitor of kappaB beta content is associated with insulin resistance in subjects with type 2 diabetes: reversal by exercise training. Diabetes. (2006) 55:760–7. doi: 10.2337/diabetes.55.03.06.db05-0677
39. Rizza S, Muniyappa R, Iantorno M. Citrus polyphenol hesperidin stimulates production of nitric oxide in endothelial cells while improving endothelial function and reducing inflammatory markers in patients with metabolic syndrome. J Clin Endocrinol Metab. (2011) 96:E782–92. doi: 10.1210/jc.2010-2879
40. Dobiaš L, Petrová M, Vojtko R. Long-term treatment with hesperidin improves endothelium-dependent vasodilation in femoral artery of spontaneously hypertensive rats: the involvement of NO-synthase and KV channels. Phytother Res. (2016) 30:1665–71. doi: 10.1002/ptr.5670
41. Schini-Kerth VB, Auger C, Kim JH. Nutritional improvement of the endothelial control of vascular tone by polyphenols: Role of NO and EDHF. Pflügers Arch. (2010) 459:853–62. doi: 10.1007/s00424-010-0806-4
42. Yamamoto M, Jokura H, Hashizume K. Hesperidin metabolite hesperetin-7-O-glucuronide, but not hesperetin-3′-O-glucuronide, exerts hypotensive, vasodilatory, and anti-nflammatory activities. Food Func. (2013) 4:1346–51. doi: 10.1039/c3fo60030k
43. Pradeep K, Park SH, Ko KC. Hesperidin a flavanoglycone protects against gamma-irradiation induced hepatocellular damage and oxidative stress in Sprague-Dawley rats. Eur J Pharmacol. (2008) 587:273–80. doi: 10.1016/j.ejphar.2008.03.052
44. Jain M, Parmar HS. Evaluation of antioxidative and anti-inflammatory potential of hesperidin and naringin on the rat air pouch model of inflammation. Inflamm Res. (2011) 60:483–91. doi: 10.1007/s00011-010-0295-0
45. Vaziri ND, Rodriguez-Iturbe B. Mechanisms of disease: oxidative stress and inflammation in the pathogenesis of hypertension. Nat Clin Pract Nephrol. (2006) 2:582–93. doi: 10.1038/ncpneph0283
46. Nwadiugwu MC. Frailty and the risk of polypharmacy in the older person: enabling and preventative approaches. J Aging Res. (2020) 2020:6759521. doi: 10.1155/2020/6759521
47. Tahara N, Kai H, Ishibashi M. Simvastatin attenuates plaque inflammation: evaluation by fluorodeoxyglucose positron emission tomography. J Am Coll Cardiol. (2006) 48:1825–31. doi: 10.1016/j.jacc.2006.03.069
48. Sacks FM, Hermans MP, Fioretto P, Valensi P, Davis T, Horton E. Association between plasma triglycerides and high-density lipoprotein cholesterol and microvascular kidney disease and retinopathy in type 2 diabetes mellitus: a global case-control study in 13 countries. Circulation. (2014) 9:999–1008. doi: 10.1161/CIRCULATIONAHA.113.002529
49. AIM-HIGH Investigators. The role of niacin in raising high-density lipoprotein cholesterol to reduce cardiovascular events in patients with atherosclerotic cardiovascular disease and optimally treated low-density lipoprotein cholesterol: baseline characteristics of study participants. The atherothrombosis intervention in metabolic syndrome with low HDL/high triglycerides: impact on global health outcomes (AIM-HIGH) trial. Am Heart J. (2011) 161:538–43. doi: 10.1016/j.ahj.2010.12.007
50. Hansson GK. Inflammatory mechanisms in atherosclerosis. J Thromb Haemost. (2009) 7:328–31. doi: 10.1111/j.1538-7836.2009.03416.x
51. Weyand CM, Younge BR, Goronzy JJ. T cells in arteritis and atherosclerosis. Curr Opin Lipidol. (2008) 19:469–77. doi: 10.1097/MOL.0b013e32830bfdc2
52. Wilson HM, Barker RN, Erwig LP. Macrophages: promising targets for the treatment of atherosclerosis. Curr Vasc Pharmacol. (2009) 7:234–43. doi: 10.2174/157016109787455635
53. Schroecksnadel K, Frick B, Winkler C. Crucial role of interferon-gamma and stimulated macrophages in cardiovascular disease. Curr Vasc Pharmacol. (2006) 4:205–13. doi: 10.2174/157016106777698379
54. Tedgui A, Mallat Z. Cytokines in atherosclerosis: pathogenic and regulatory pathways. Physiol Rev. (2006) 86:515–81. doi: 10.1152/physrev.00024.2005
55. Kher N, Marsh JD. Pathobiology of atherosclerosis—a brief review. Semin Thromb Hemost. (2004) 30:665–72. doi: 10.1055/s-2004-861509
56. Babaei-Jadidi R, Karachalias N, Ahmed N. Prevention of incipient diabetic nephropathy by high-dose thiamine and benfotiamine. Diabetes. (2003) 52:2110–20. doi: 10.2337/diabetes.52.8.2110
57. Hammes HP, Du X, Edelstein D. Benfotiamine blocks three major pathways of hyperglycemic damage and prevents experimental diabetic retinopathy. Nat Med. (2003) 9:294–9. doi: 10.1038/nm834
58. Karachalias N, Babaei-Jadidi R, Rabbani N. Increased protein damage in renal glomeruli, retina, nerve, plasma and urine and its prevention by thiamine and benfotiamine therapy in a rat model of diabetes. Diabetologia. (2010) 53:1506–16. doi: 10.1007/s00125-010-1722-z
59. Xue M, Qian Q, Adaikalakoteswari A. Activation of NF-E2-related factor-2 reverses biochemical dysfunction of endothelial cells induced by hyperglycemia linked to vascular disease. Diabetes. (2008) 57:2809–17. doi: 10.2337/db06-1003
60. Mazzone T, Meyer PM, Feinstein SB, Davidson MH, Kondos GT, D'Agostino RB Sr, et al. Effect of pioglitazone compared with glimepiride on carotid intima-media thickness in type 2 diabetes: a randomized trial. JAMA. (2006) 296:2572–81. doi: 10.1001/jama.296.21.joc60158
61. Nissen SE, Nicholls SJ, Wolski K, Nesto R, Kupfer S, Perez A, et al. Comparison of pioglitazone vs glimepiride on progression of coronary atherosclerosis in patients with type 2 diabetes: the PERISCOPE randomized controlled trial. JAMA. (2008) 299:1561–73. doi: 10.1001/jama.299.13.1561
62. Okopien' B, Krysiak R, Kowalski J. The effect of statins and fibrates on interferon-gamma and interleukin-2 release in patients with primary type II dyslipidemia. Atherosclerosis. (2004) 176:327–35. doi: 10.1016/j.atherosclerosis.2004.05.009
63. Kirmizis D, Papagianni A, Dogrammatzi F. Effects of simvastatin on markers of inflammation, oxidative stress and endothelial cell apoptosis in patients on chronic hemodialysis. J Atheroscler Thromb. (2010) 17:1256–65. doi: 10.5551/jat.5710
64. BIP (Bezafibrate Infarction Prevention) Study Group. Secondary prevention by raising HDL cholesterol and reducing triglycerides in patients with coronary artery disease: the Bezafibrate Infarction Prevention (BIP) study. Circulation. (2000) 102:21–7. doi: 10.1161/01.CIR.102.1.21
65. Ginsberg HN, Elam MB, Lovato LC. ACCORD study group effects of combination lipid therapy in type 2 diabetes mellitus. N Engl J Med. (2010) 362:1563–74. doi: 10.1056/NEJMoa1001282
66. Basta G, Sironi AM, Lazzerini G. Circulating soluble receptor for advanced glycation end products is inversely associated with glycemic control and S100A12 protein. J Clin Endocrinol Metab. (2006) 91:4628–34. doi: 10.1210/jc.2005-2559
67. Cipollone F, Iezzi A, Fazia M. The receptor RAGE as a progression factor amplifying arachidonate-dependent inflammatory and proteolytic response in human atherosclerotic plaques: role of glycemic control. Circulation. (2003) 108:1070–7. doi: 10.1161/01.CIR.0000086014.80477.0D
68. Koyama H, Shoji T, Yokoyama H. Plasma level of endogenous secretory RAGE is associated with components of the metabolic syndrome and atherosclerosis. Arterioscler Thromb Vasc Biol. (2005) 25:2587–93. doi: 10.1161/01.ATV.0000190660.32863.cd
69. Chiang KH, Huang PH, Huang SS. Plasma levels of soluble receptor for advanced glycation end products are associated with endothelial function and predict cardiovascular events in nondiabetic patients. Coron Artery Dis. (2009) 20:267–73. doi: 10.1097/MCA.0b013e32832c459c
70. Arikawa AY, Thomas W, Schmitz KH. Sixteen weeks of exercise reduces C-reactive protein levels in young women. Med Sci Sports Exerc. (2011) 43:1002–9. doi: 10.1249/MSS.0b013e3182059eda
71. Nader GA, Lundberg IE. Exercise as an anti-inflammatory intervention to combat inflammatory diseases of muscle. Curr Opin Rheumatol. (2009) 21:599–603. doi: 10.1097/BOR.0b013e3283319d53
72. Riesco E, Choquette S, Audet M. Effect of exercise training combined with phytoestrogens on adipokines and C-reactive protein in postmenopausal women: a randomized trial. Metabolism. (2012) 61:273–80. doi: 10.1016/j.metabol.2011.06.025
73. Blankeberg S, Tiret L, Bickel C. Interleukin-18 is a strong predictor of cardiovascular death in stable and unstable angina. Circulation. (2002) 106:24–30. doi: 10.1161/01.CIR.0000020546.30940.92
74. Blankeberg S, Luc G, Ducimetiere P. Interleukin-18 and the risk of coronary heart disease in European men (PRIME). Circulation. (2003) 108:2453–9. doi: 10.1161/01.CIR.0000099509.76044.A2
75. Esposito K, Pontillo A, Di Palo C. Effect of weight loss and lifestyle changes on vascular inflammatory markers in obese women. JAMA. (2003) 289:1799–804. doi: 10.1001/jama.289.14.1799
76. Petersen AMW, Pedersen BK. The anti-inflammatory effects of exercise. J Appl Physiol. (2005) 98:1154–62. doi: 10.1152/japplphysiol.00164.2004
77. Mahmud A, Feely J. Arterial stiffness is related to systemic inflammation in essential hypertension. Hypertension. (2005) 4:1118–22. doi: 10.1161/01.HYP.0000185463.27209.b0
78. Savoia C, Schiffrin EL. Inflammation in hypertension. Curr Opin Nephrol Hypertens. (2006) 15:152–8. doi: 10.1097/01.mnh.0000203189.57513.76
79. Kellow NJ, Coughlan MT, Savige GS. Effect of dietary prebiotic supplementation on advanced glycation, insulin resistance and inflammatory biomarkers in adults with pre-diabetes: a study protocol for a double-blind placebo-controlled randomized crossover clinical trial. BMC Endocrine Disord. (2014) 14:55. doi: 10.1186/1472-6823-14-55
80. Goldberg T, Cai W, Peppa M. Advanced glycoxidation end products in commonly consumed foods. J Am Diet Assoc. (2004) 104:1287–91. doi: 10.1016/j.jada.2004.05.214
81. Cani PD, Possemiers S, Van de Wiele T. Changes in gut microbiota control inflammation in obese mice through a mechanism involving GLP-2-driven improvement of gut permeability. Gut. (2009) 58:1091–103. doi: 10.1136/gut.2008.165886
82. Cani PD. Crosstalk between the gut microbiota and the endocannabinoid system: impact on the gut barrier function and the adipose tissue. Clin Microbiol Infect. (2012) 18:50–3. doi: 10.1111/j.1469-0691.2012.03866.x
83. Aggarwal BB. Nuclear factor-κB: the enemy within. Cancer Cell. (2004) 6:203–8. doi: 10.1016/j.ccr.2004.09.003
84. Shi Y, Hu FB. The global implications of diabetes and cancer. Lancet. (2014) 383:1947. doi: 10.1016/S0140-6736(14)60886-2
85. Kampoli AM, Tousoulis D, Briasoulis A. Potential pathogenic inflammatory mechanisms of endothelial dysfunction induced by type 2 diabetes mellitus. Curr Pharm Des. (2011) 17:4147–58. doi: 10.2174/138161211798764825
86. Vanessa FT, Prioletta A, Zuo P. Hyperglycemia-induced oxidative stress and its role in diabetes mellitus related cardiovascular diseases. Curr Pharm Des. (2013) 19:5695–703. doi: 10.2174/1381612811319320005
87. Sibal L, Agarwal SC, Home PD, Boger RH. The role of asymmetric dimethylarginine (ADMA) in endothelial dysfunction and cardiovascular disease. Curr Cardiol Rev. (2010) 6:82–90. doi: 10.2174/157340310791162659
Keywords: diabetic angiopathy, inflammation, commorbidity, intervention study, diabetes miletus
Citation: Nwadiugwu MC (2021) Inflammatory Activities in Type 2 Diabetes Patients With Co-morbid Angiopathies and Exploring Beneficial Interventions: A Systematic Review. Front. Public Health 8:600427. doi: 10.3389/fpubh.2020.600427
Received: 30 August 2020; Accepted: 14 December 2020;
Published: 25 January 2021.
Edited by:
Ilaria Barchetta, Sapienza University of Rome, ItalyReviewed by:
Željko Reiner, University Hospital Centre Zagreb, CroatiaCopyright © 2021 Nwadiugwu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Martin C. Nwadiugwu, bWFydGludG9ueTR1QGdtYWlsLmNvbQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.