 Rosario Foti
Rosario Foti Elisa Visalli
Elisa Visalli
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
OPINION article
Front. Public Health, 09 November 2020
Sec. Digital Public Health
Volume 8 - 2020 | https://doi.org/10.3389/fpubh.2020.558838
This article is part of the Research TopicPersonalized Digital Health and Patient-Centric ServicesView all 21 articles
In March 2020, a new disease called COVID-19 caused by a novel member of the Coronaviridae family named SARS-CoV-2 (severe acute respiratory coronavirus 2 syndrome) was declared pandemic (1).
In this context, the management of patients with immune-rheumatic diseases is absolutely crucial. These conditions share treatments with immunosuppressive agents such as corticosteroids and synthetic or biological disease-modifying drugs (2, 3), but despite a slight increase in infections is documented, unjustified discontinuation of immunosuppressants in rheumatic disorders is not recommended (4). Discontinuation of therapy may lead to disease flares (2) with systemic inflammation and immunological disruption that can potentially increase susceptibility to infections in rheumatic diseases (5). Therefore, a medical reassessment could be necessary, and it may further increase the patient's infectious risk due to moving around and being in the hospital.
In response to these needs, profound changes have been introduced in our organization (6), and telemedicine could play an important role in public health emergencies (7). Telemedicine is the remote delivery of healthcare services and clinical practices through medical data transmission via information and communication technologies. Furthermore, it has been proved useful to a remarkable increase in published randomized controlled trials and, consequently, to an improved quality of available data (8).
It can represent an additional and potentially suitable tool for follow-up monitoring of patients especially during the pandemic lockdown, and through it, we were able to ensure continuity of specific treatments for the management of inflammatory pathologies by identifying urgent remote situations, such as an infectious complication or a serious onset of the disease that requires physical consultation (8, 9).
From March 11, 2020, all patients affected by rheumatic diseases and treated with biological disease-modifying drugs afferent to Rheumatology Unit of Policlinico S. Marco in Catania were contacted.
The synchronous telemedicine application is meant to offer a virtual alternative to the in-person rheumatologist's visit, and it requires a live interaction between health professionals and patients; this activity has been provided by telephone follow-up visits and by fax and e-mail usage in order to send reports to the patient. Technological improvements, combined with the high-speed internet and the massive spread of smartphones, enable the possibility to apply this framework and quickly deploy video teleconsultations from a patient's home.
Patients were called to evaluate the state of health and the presence of any adverse events; laboratory test reports, such as acute phase reactants (erythrocyte sedimentation rate and C-reactive protein), have been examined. All patients with symptoms of infection temporarily withdrew biological disease-modifying antirheumatic drugs (DMARDs) or traditional DMARDs at the time of symptoms onset. A nurse administered the clinimetric questionnaires assessment to evaluate the disease activity, the impact of rheumatic disease on the health status, and the presence of anxiety, depression, and fibromyalgia. In addition to disease activity and any adverse events, with particular regard to infectious events, the assessment of the psychological situation will be important. Indeed, COVID-19 has also a serious impact on mental health, and Huang and Zhao (10) demonstrated a significantly higher incidence of anxiety disorders and depressive symptoms (DSs) especially in younger people. Depression and anxiety are frequently associated with fibromyalgia (11), which is one of the numerous comorbidities that may accompany inflammatory rheumatic with possible interference with symptomatology, disease activity and overall management plan (12).
In particular, the following scales, described in Table 1, have been used:
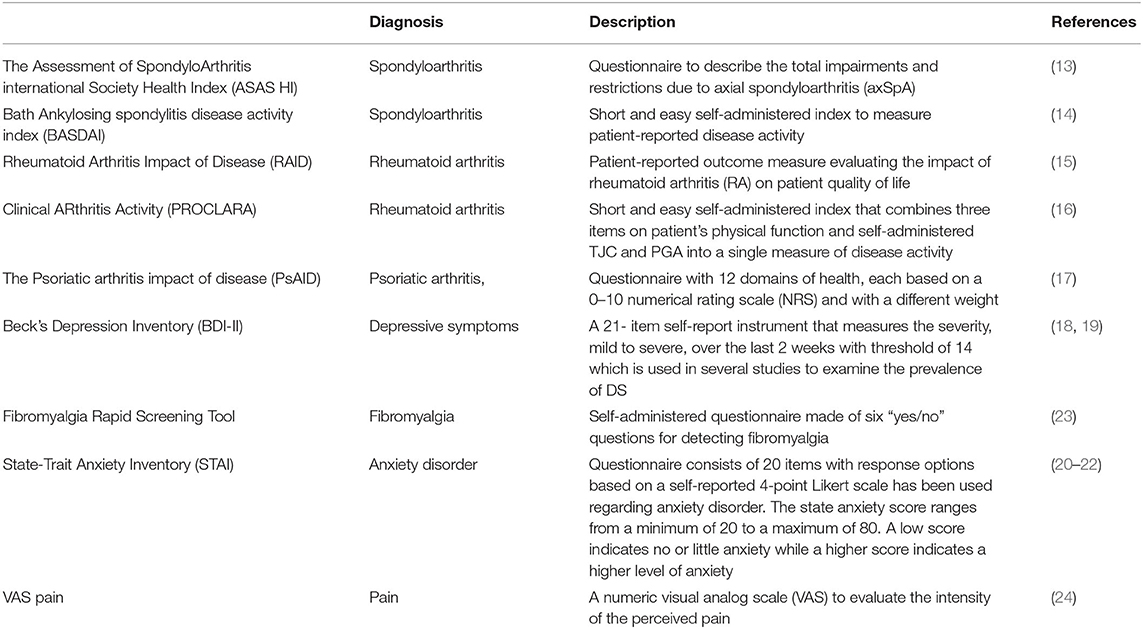
Table 1. Clinimetric questionnaires assessment.
The Assessment of SpondyloArthritis international Society Health Index to describe the total impairments and restrictions due to axial spondyloarthritis and Bath Ankylosing Spondylitis Disease Activity Index to measure patient-reported disease activity for patients with spondyloarthritis (13, 14).
For patients with rheumatoid arthritis (RA), the following evaluations have been used: the Rheumatoid Arthritis Impact of Disease, a patient-reported outcome measure evaluating the impact of RA on patient quality of life (15); the Clinical ARthritis Activity (PRO-CLARA), a short and easy self-administered index that combines three items on patient's physical function and self-administered tender joints count (TJC) and patient global assessment (PGA) into a single measure of disease activity (16). For patients with psoriatic arthritis, The Psoriatic Arthritis Impact of Disease questionnaire with 12 domains of health, each based on a 0- to 10-point numerical rating scale and with a different weight (17), has been used. There is not a clinimetric index to evaluate physical function for psoriatic arthritis; therefore, we used self-administered TJC such as PRO-CLARA for RA for the part related to joint count.
The presence of DSs has been assessed using the beck's depression inventory (BDI)-II, a 21-item self-report instrument that measures the severity, mild to severe, over the last 2 weeks with threshold of 14, which is used in several studies to examine the prevalence of DSs (18, 19).
The STAI, state–anxiety scale, which consists of 20 items with response options based on a self-reported 4-point Likert scale, has been used regarding anxiety disorder. The state-anxiety score ranges from a minimum of 20 to a maximum of 80. A low score indicates no or little anxiety while a higher score indicates a higher level of anxiety (20–22).
The Fibromyalgia Rapid Screening Tool questionnaire is a brief, self-administered questionnaire made of six yes/no questions for detecting fibromyalgia that has demonstrated high sensitivity and specificity among patients with chronic diffuse pain conditions and has been used in this study (23).
The visual analog scale for the assessment of pain (24) has been used for measurement of pain perception. Comorbidities may have an important impact on the health status of our patients; therefore, we used the Charlson comorbidity index to evaluate this important aspect as well (25).
We are working on the correlation of the results obtained to have more information that can guide us to a correct clinical evaluation because questionnaires assess different aspects and could provide us an additional element in our diagnostic evaluation (flare disease or fibromyalgia) and affect the therapeutic choices.
As being in the Rheumatology Department, we have switched ~80% of outpatient appointments to synchronous telemedicine. This has worked surprisingly well, and patients have been very understanding. Outpatient clinic face-to-face consultations are limited to urgent patients. Patient management through telemedicine has allowed us to carry out a remote assessment of the state of health and of the psychological implications that the changes related to the pandemic from COVID-19 have been determined in our patients without exposing them to an increased infectious risk. Regarding the day-hospital patients, intravenous treatment was postponed if patient condition allowed it; however, treatments were maintained during COVID-19 pandemic. Regarding rituximab treatment, we know that this therapy induces B-cell depletion, and it reduces the immunogenicity of several vaccines; similarly, the immunological memory following SARS-CoV-2 infection will probably be impaired by this biologic, making patients sensitive to a reinfection (26). In this case, there is not an unequivocal strategy to be suggested; instead, it is an individual strategy, considering that these drugs can often be lifesaving. The usage of subcutaneous administration could be suggested when the same mechanism of the drug is available, with a limited risk for the patients mainly in terms of possible loss of efficacy. Human contact in the care of patients and face-to-face questioning and physical examination are important for a careful analysis of the clinical situation, perhaps for acceptance of care and for ensuring good compliance as well (9). Most aspects of rheumatology practice have changed since the onset of the COVID-19 pandemic, and new modes of care delivery may reshape practices and help with workforce shortages and asymmetric distribution of providers; furthermore, our challenge will also be to get information about the effect of rheumatic disease therapies on dysregulated inflammatory responses that may be associated with the morbidity and mortality that are seen with COVID-19. Even though the evidence for a superior or equal effectiveness of telemedicine compared to the standard face-to-face approach was weakened preventing to draw definitive conclusions, we continue to work modifying our approach to try to ensure the necessary care while respecting safety, and optimistically, this tool will become an important part of management in rheumatic diseases.
All Authors contributed to the writing of the manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
1. Zhou P, Yang XL, Wang XG, Hu B, Zhang L, Zhang W. A pneumonia outbreak associated with a new coronavirus of probable bat origin. Nature. (2020) 579:270–3. doi: 10.1038/s41586-020-2012-7
2. Coletto LA, Favalli EG, Caporali R. Psoriasis and psoriatic arthritis: how to manage immunosuppressants in COVID-19 days. Dermatol Ther. (2020) 14:e13415. doi: 10.1111/dth.13415
3. Favalli EG, Biggioggero M, Meroni PL. Methotrexate for the treatment of rheumatoid arthritis in the biologic era: still an “anchor” drug? Autoimmun Rev. (2014) 13:1102–8. doi: 10.1016/j.autrev.2014.08.026
4. Kalb RE, Fiorentino DF, Lebwohl MG, Toole J, Poulin Y, Cohen AD, et al. Risk of serious infection with biologic and systemic treatment of psoriasis: results from the psoriasis longitudinal assessment and registry (PSOLAR). JAMA Dermatol. (2015) 151:961–9. doi: 10.1001/jamadermatol.2015.0718
5. Listing J, Gerhold K, Zink A. The risk of infections associated with rheumatoid arthritis, with its comorbidity and treatment. Rheumatology. (2013) 52:53–61. doi: 10.1093/rheumatology/kes305
6. Hollander JE, Carr BG. Virtually perfect? Telemedicine for covid-19. N Engl J Med. (2020) 382:1679–81. doi: 10.1056/NEJMp2003539
7. Lurie N, Carr BG. The role of telehealth in the medical response to disasters. JAMA Intern Med. (2018) 178:745–6. doi: 10.1001/jamainternmed.2018.1314
8. Piga M, Cangemi I, Mathieu A, Cauli A. Telemedicine for patients with rheumatic diseases: systematic review and proposal for research agenda. Semin Arthritis Rheum. 47:121–8. doi: 10.1016/j.semarthrit.2017.03.014
9. Richez C, Lazaro E, Lemoine M, Truchetet ME, Schaeverbeke T. Implications of COVID19 for the management of patients with inflammatory rheumatic diseases. Joint Bone Spine. (2020) 87:187–9. doi: 10.1016/j.jbspin.2020.03.010
10. Huang Y, Zhao N. Generalized anxiety disorder, depressive symptoms and sleep quality during COVID-19 outbreak in China: a web-based cross-sectional survey. Psychiatry Res. (2020) 288:112954. doi: 10.1016/j.psychres.2020.112954
11. Kremer M, Becker LJ, Barrot M, Yalcin I. How to study anxiety and depression in rodent models of chronic pain? Eur J Neurosci. (2020). doi: 10.1111/ejn.14686. [Epub ahead of print].
12. Benlidayi C. Fibromyalgia interferes with disease activity and biological therapy response in inflammatory rheumatic diseases. Rheumatol Int. (2020) 40:849–58. doi: 10.1007/s00296-019-04506-2
13. Di Carlo M, Lato V, Di Matteo A, Carotti M, Salaffi F. Defining functioning categories in axial spondyloarthritis: the role of the ASAS health index. Rheumatol Int. (2017) 37:713–8. doi: 10.1007/s00296-016-3642-9.
14. Zochling J1. Measures of symptoms and disease status in ankylosing spondylitis: ankylosing spondylitis disease activity score (ASDAS), ankylosing spondylitis quality of life scale (ASQoL), bath ankylosing spondylitis disease activity index (BASDAI), bath ankylosing spondylitis functional index (BASFI), bath ankylosing spondylitis global score (BAS-G), bath ankylosing spondylitis metrology index (BASMI), dougados functional index (DFI), and health assessment questionnaire for the spondylarthropathies (HAQ-S). Arthritis Care Res. (2011) 63(Suppl. 11):S47–58. doi: 10.1002/acr.20575
15. Dougados M, Brault Y, Logeart I, van der Heijde D, Gossec L, Kvien T. Defining cut-off values for disease activity states and improvement scores for patient-repor ted outcomes: the example of the rheumatoid arthritis impact of disease (RAID) Dougados et al. Arthritis Res Ther. (2012) 14:R129. doi: 10.1186/ar3859
16. Salaffi F1, Migliore A, Scarpellini M, Corsaro SM, Laganà B, Mozzani F, et al. Psychometric properties of an index of three patientreported outcome (PRO) measures, termed the clinical arthritis activity (PRO-CLARA) in patients with rheumatoid arthritis. The NEW INDICES study. Clin Exp Rheumatol. (2010) 28:186–200.
17. Salaffi F, Di Carlo M, Carotti M, Farah S, Gutierrez M. The psoriatic arthritis impact of disease 12-item questionnaire: equivalence, reliability, validity, and feasibility of the touch-screen administration versus the paper-and-pencil version Ther Clin Risk Manag. (2016) 12:631–42. doi: 10.2147/TCRM.S101619
18. Beck A, Steer R, Brown G. Beck Depression Inventory-II. San Antonio, TX: The Psychological Corporation Harcourt Brace & Company (1996).
19. Tam W, Lo K, Pacheco J. Prevalence of depressive symptoms among medical students: overview of systematic reviews. MedEduc. (2019) 53:345–54. doi: 10.1111/medu.13770
20. Rotenstein LS, Ramos MA, Torre M, Segal JB, Peluso MJ, Guille C, et al. Prevalence of depression, depressive symptoms, and suicidal ideation among medical students. JAMA. (2016) 316:2214–36. doi: 10.1001/jama.2016.17324
21. Julian LJ. Measures of anxiety: state-trait anxiety inventory (STAI), beck anxiety inventory (BAI), and hospital anxiety and depression scale- anxiety (HADS-A). Arthritis Care Res. (2011) 63(Suppl. 11):S467–72. doi: 10.1002/acr.20561
22. Vagg PR, Spielberger CD, O'Hearn TP. Is the state-trait anxiety inventory multidimensional? Personal Individ Differ. (1980) 1:207–14. doi: 10.1016/0191-8869(80)90052-5
23. Cho SJ, Perrot S, Sohn JH, Bae JS, Chu MK. Validity and reliability of the fibromyalgia rapid screening tool among individuals with chronic daily headache: a clinic-based study. Pain Med. (2019) 20:1193–201. doi: 10.1093/pm/pny216
24. Fries JF, Spitz PW, Young DY. The dimensions of health outcomes: the health assessment questionnaire, disability and pain scales. J Rheumatol. (1982) 9:789–93.
25. Brusselaers N, Lagergren J. The charlson comorbidity index in registry-based research. Methods Inf Med. (2017) 56:401–6. doi: 10.3414/ME17-01-0051
Keywords: COVID-19, immune-rheumatic diseases, immunosuppressive agents, clinical practice, telemedicine
Citation: Foti R, Amato G, Foti R and Visalli E (2020) Management of Patients With Inflammatory Rheumatic Diseases: Telemedicine and Rheumatologists Challenged in the Era of COVID-19. Front. Public Health 8:558838. doi: 10.3389/fpubh.2020.558838
Received: 04 May 2020; Accepted: 14 September 2020;
Published: 09 November 2020.
Edited by:
Maria Hägglund, Uppsala University, SwedenReviewed by:
Charles Doarn, University of Cincinnati, United StatesCopyright © 2020 Foti, Amato, Foti and Visalli. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Elisa Visalli, ZWxpdmlzYTIxQGdtYWlsLmNvbQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.