
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health , 18 December 2020
Sec. Public Health Education and Promotion
Volume 8 - 2020 | https://doi.org/10.3389/fpubh.2020.530596
 Jessica D. Austin1
Jessica D. Austin1 Serena A. Rodriguez2
Serena A. Rodriguez2 Lara S. Savas3
Lara S. Savas3 Tina Megdal4Lois Ramondetta5
Tina Megdal4Lois Ramondetta5 Maria E. Fernandez3*
Maria E. Fernandez3*Introduction: A healthcare provider's ability to give a strong recommendation for the HPV vaccine is of utmost importance in increasing HPV vaccination. To reduce the burden of HPV-related cancers, there is a critical need to develop and implement theory-based interventions aimed at strengthening healthcare providers' communication about the HPV vaccine.
Methods: We used Intervention Mapping (IM) steps 1–5 to develop and implement a provider-level intervention that aligns with the priorities and needs of a large, urban Federally Qualified Health Center (FQHC).
Results: In step 1, a diverse planning group identified barriers to HPV vaccination in clinical settings and generated process maps and a logic model of the problem. Step 2 outlined outcomes and provider performance objectives of the intervention and identified knowledge, skills, self-efficacy, outcome expectations, and normative beliefs as modifiable targets that need to change for providers to deliver strong recommendations for the HPV vaccine to parents and patients. In step 3, the planning group mapped the methods of persuasive communication, information, and modeling and skills training to behavioral targets and outlined the program practical applications (strategies) components, scope, and sequence. In steps 4 and 5, the planning group produced the intervention and planned for program implementation. The iterative and participatory process of IM resulted in modifications to the initial intervention that aligned with the needs of the FQHC.
Discussion: IM provided a systematic, participatory, and iterative approach for developing a theory-based provider-level intervention aimed at strengthening healthcare providers' ability to provide a strong recommendation for the HPV vaccine to eligible patients and parents served by a large FQHC. IM assisted with the identification of behavioral targets and methods that move beyond HPV knowledge and reminders to create behavior change. IM can help researchers and planners describe the processes and rational behind developing interventions and may help to facilitate implementation in real-world clinical settings by tailoring intervention components to the needs of the population.
Human papillomavirus (HPV) is one of the most common sexually transmitted infections in the United States with an estimated 70% of individuals acquiring the infection at some point in their lifetimes (1, 2). Persistent infection with a high-risk HPV type is the leading cause of cervical cancer and associated with the development of other cancers, such as vulvar, vaginal, and anal cancers among women, and penile and anal cancers among men (3, 4). The HPV vaccine has the potential to decrease the burden of HPV-related cancers by preventing over 90% of cancers attributed to HPV infections when presented prior to exposure (5). The Centers for Disease Control (CDC) Advisory Committee for Immunization Practices recommends that healthcare providers administer the HPV vaccine series to adolescent males and females at ages 11–12 concurrent with other recommended vaccines and completing the series prior to age 13 (6–8). The CDC also recommends catch-up HPV vaccination for individuals through age 26 who are not adequately vaccinated (8). Despite national recommendations, the uptake of the HPV vaccine as an evidence-based practice remains suboptimal, resulting in underuse and missed opportunities to prevent HPV-related cancers (9). In 2017, 66% of all 13–17 year old adolescents initiated the HPV vaccine and only 51.1% received all recommended doses, well below the Healthy People 2020 benchmark of 80% (4, 10, 11). Geographic, socioeconomic, racial, and ethnic disparities in HPV vaccine initiation and completion have also emerged, further exacerbating HPV-related cancer burdens (12–17).
Studies assessing HPV vaccine uptake consistently highlight the importance of healthcare providers' recommendations (18–20). Receiving a provider recommendation is significantly associated with HPV vaccine uptake, and a provider's ability to provide a strong recommendation is considered one of the most important strategies to increase HPV vaccine coverage (11, 17–23). However, providers often fail to recommend the HPV vaccine, and they do not recommend the HPV as consistently as other vaccinations recommended for 11–12 year old adolescents (23). A number of studies have identified challenges to recommending and communicating about the HPV vaccine, such as a lack of clarity around clinical guidelines, discomfort discussing the topic with patients and parents, and a lack of confidence responding to vaccine hesitant parents (24–27). Increasing healthcare providers' knowledge, communication skills to deliver a strong recommendation, and confidence in addressing parental and patient concerns is imperative to improve uptake and coverage.
Despite being one of the strongest predictors of HPV vaccination uptake and coverage, few interventions focus on improving HPV vaccine communication. There is a need for theory-based interventions aimed at strengthening healthcare providers' communication about HPV vaccination for children. Provider-targeted interventions are often limited to delivering provider education about the vaccine or alerts in electronic medical records (20). Importantly, absent from the literature is the use of theory to inform the development and implementation of provider-level interventions. To increase HPV vaccine recommendation behaviors, intervention developers should utilize theory that supports behavior change and should make decisions about intervention components and messages using a logical and systematic approach (28–30). These interventions should also address multiple determinants, such as self-efficacy and attitudes, and align with the priority populations needs and intervention context (31–34).
IM is a theory-driven planning framework that provides a systematic process and detailed protocol for effective multi-level intervention development, implementation, and evaluation (34, 35). IM incorporates prominent health behavior theories, such of Social Cognitive Theory, to understand determinants driving a health problem and to maps methods of behavior change, such as skills training with guided practice or modeling. IM has been used to develop multiple cancer prevention and control programs to increase HPV vaccination (36, 37), and cervical, breast, and colorectal cancer screening (38–44). This paper describes the use of Intervention Mapping (IM) to systematically develop and implement a theory-based intervention to strengthen providers' recommendation for the HPV vaccine. The provider-level intervention described in this paper was one component of a larger multi-level intervention to comprehensively address factors influencing HPV vaccination in a large, urban Federally Qualified Health Center (FQHC) in Texas.
FQHC leaders collaborated with researchers to develop a multi-level intervention to increase the proportion of FQHC age-eligible patients (11–26 years) initiating and completing the HPV vaccine series in accordance with Advisory Committee on Immunization Practice Guidelines. The overall program goal was to increase the percentage of age-eligible patients initiating the HPV vaccine within 1 year to 30%. For this paper, we describe the use of IM to develop a provider-level intervention aimed at strengthening FQHC providers' recommendation for the HPV vaccine. We define providers as physicians, nurses, medical assistants, and other medical professionals who speak about vaccination with patients and/or parents during in-person clinic visits. This study was approved by the University of Texas Health Science Center at Houston Institutional Review Board.
IM provides a systematic framework for program development and planning that can help increase the use of effective practices in healthcare settings (45–48). IM guides program planners to consider, through a needs and assets assessment, the determinants, mechanisms, and strategies for effecting change, and it encourages a particpatory approach throughout intervention development, implementation, adapatation, and dissemination (35). The IM process is composed of six steps; each one involves specific tasks that guide the translation of relevant determinants into a health promotion program. We describe the first five steps where the deliverable following the completion of each step serves as a guide for the subsequent steps (35). Step 1 includes conducting a needs assessment often led by a planning group. In step 2, planners state desired health promoting behaviors and identify performance objectives, the specific sub-behaviors required to achieve the behaviors, identify determinants associated with the health promoting behaviors, and develop a matrix of change objectives. The change objectives are the changes needed in each determinant in order for an individual to complete a performance objective and ultimately the overall health promoting behavior. To develop program components in step 3, planners identify theoretical change methods targeting determinants and operationalize methods as practical applications. Change methods are theory- or evidence-based techniques meant to influence determinants, and practical applications are ways of organizing, operationalizing, and delivering the methods (35). Program materials are produced in step 4, and step 5 includes developing an implementation plan for the intervention.
In our study for step 1, we formed a planning group and stated the current behaviors and determinants associated with failures in providing strong recommendations for HPV vaccinations to parents of HPV-vaccine eligible patients. In step 2, we stated the desired intervention outcomes, specified the provider health promoting behavior (making a strong recommendation) and performance objectives necessary to achieve the behavior, and identified psychosocial factors that influence strong provider recommendations (determinants) (34, 35). Performance objectives were crossed with determinants to create a matrix of change objectives which were a blueprint for intervention materials. In step 3, we designed the provider intervention by developing program components, mapping change objectives and determinants to theoretical change methods, and selecting practical applications, or strategies, to deliver the theoretical methods. We produced program messages and materials for providers in step 4 and, in step 5, we planned for intervention implementation by identifying who would deliver the intervention, specifying tasks necessary for intervention implementation and delivery, and developing strategies to enable implementation and delivery. Throughout each IM step, we relied on behavioral and organizational theory, evidence in the literature, and new data to the guide decision-making.
We established a diverse planning group comprised of stakeholders with expertise in cancer prevention and control, intervention development, HPV, and FQHC leadership. Specifically, our planning group included FQHC program leaders, 3 intervention design experts, cancer prevention and control researchers, a gynecological oncologist, and 2 program staff. The planning group, led by a cancer prevention and control researcher, met weekly during the development phase and bi-weekly during the implementation phase of the provider-level intervention. Using facilitated discussion and synthesis of provider and staff surveys, the planning group identified barriers to HPV vaccine uptake and failures in FQHC providers delivering a strong recommendations for HPV vaccinations to eligible patients and parents. The group listed barriers to uptake identified through their previous research examining HPV vaccination among adolescents (49–53), and they developed a healthcare delivery process map unique to the FQHC. Process maps are useful tools for quality improvement that illustrate key individuals and activities in clinical processes, and they assist in identifying opportunities for improvement (54, 55). The group developed the process map by listing each step of the appointment process for patients from check-in to check-out, staff rolls and responsibilities during each step, and patient handoffs (36). FQHC providers and staff provided input via email and in-person discussions throughout the process to ensure accuracy. The group combined new data from the process map with previous research to develop a logic model of the problem (Figure 1), a graphic representation of the multilevel factors associated with a lack of HPV vaccine uptake (32).
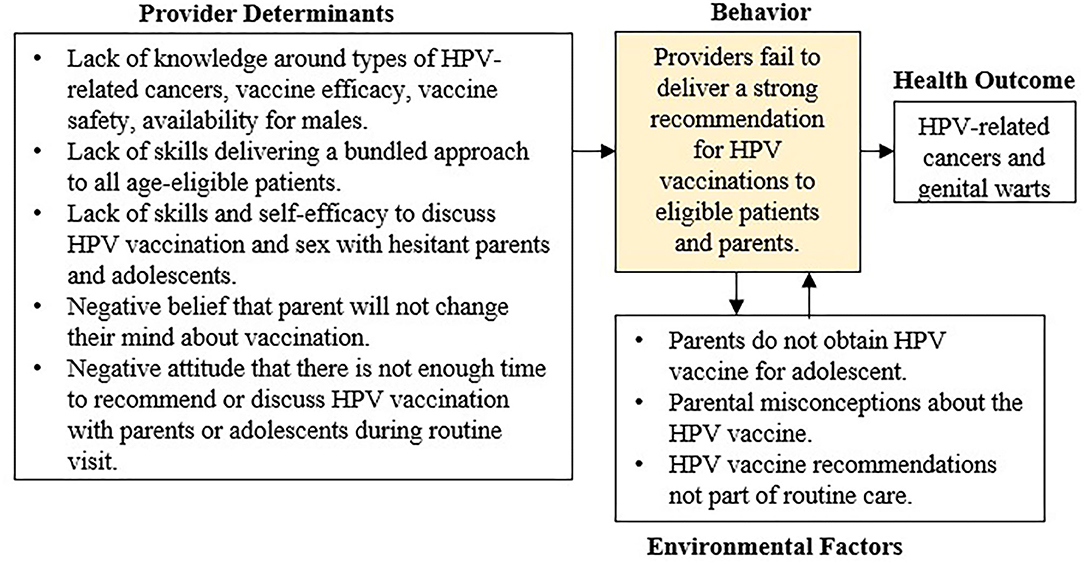
Figure 1. Logic model of the problem.
The behavioral outcome was stated as “FQHC providers deliver a strong recommendation for the HPV vaccine and administering the vaccine.” We identified seven performance objectives for the outcome (Table 1).
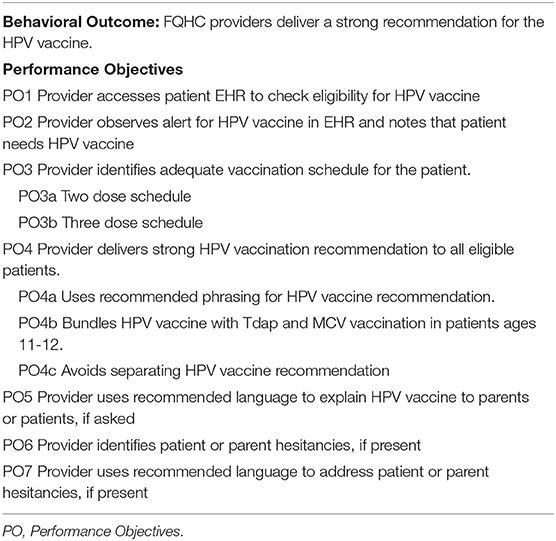
Table 1. Behavioral outcome and performance objectives.
Based on previous research, the process map, and surveys from FQHC providers and staff, we identified the following determinants, or cognitive factors that would need to change to achieve the outcome: (1) knowledge; (2) skills and self-efficacy; (3) outcome expectations; and (4) normative beliefs. For example, behavior change models such as Social Cognitive Theory suggest that self-efficacy is a direct and proximal determinant of behavior change and is most predictive of behavioral outcomes (56–58). To increase an individual's self-efficacy, one must have the knowledge and skills to perform the behavior. Studies have shown that providers often lack knowledge around guidelines and do not have the skills to deliver strong and consistent HPV recommendations to eligible patients (20, 26). Moreover, direct feedback from FQHC staff confirmed the need for more education and training around HPV vaccination guidelines for eligible patients. Next, we crossed the determinants with performance objectives to generate a matrix of change objectives that served as the blueprint for designing the HPV provider intervention (Table 2).
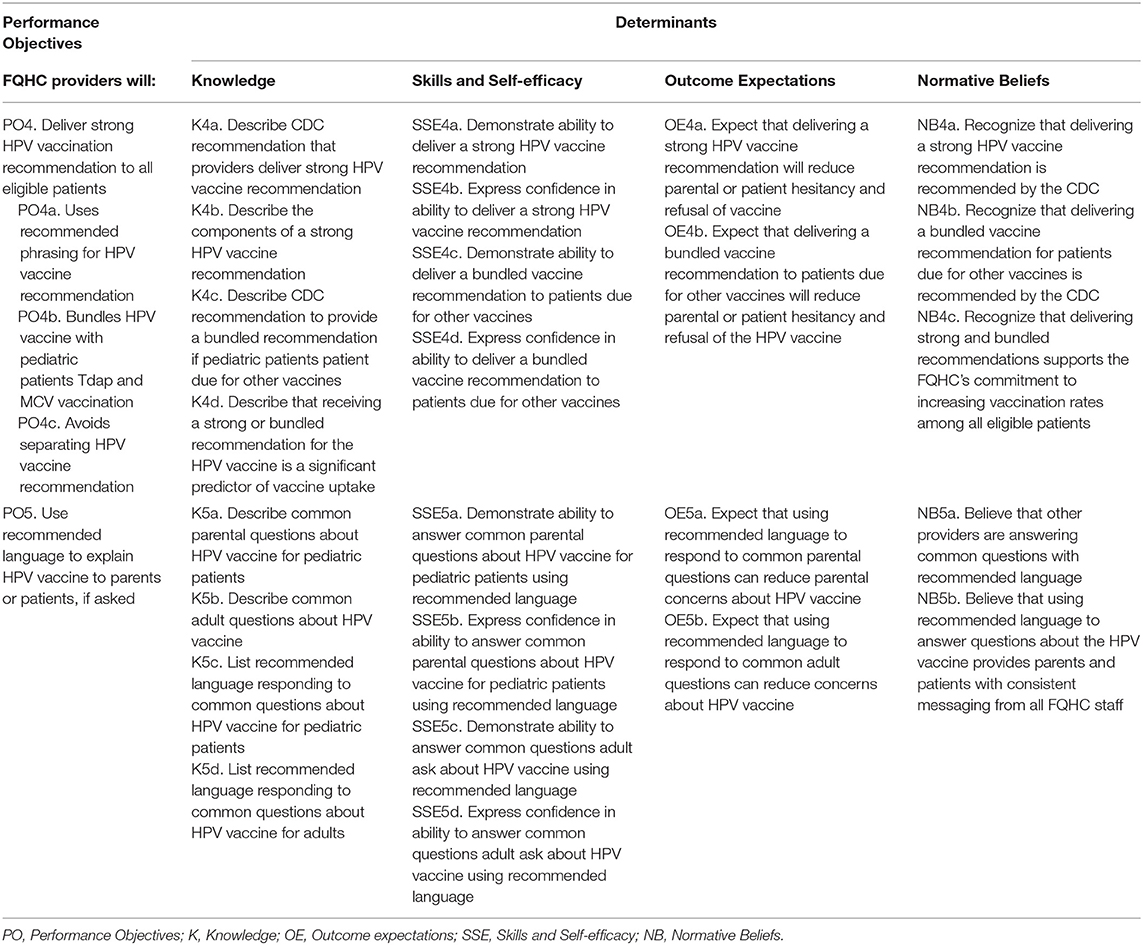
Table 2. Partial matrix of change for behavioral outcome.
Using the matrix of change objectives generated in Step 2, the team developed the program components of the HPV provider training by mapping the change objectives and determinants to change methods, and selected practical applications to deliver the methods (Table 3). The team selected change methods, or theory-based techniques, from prominent health behavior theories known to influence behavioral determinants—persuasive communication (Social Cognitive Theory), giving information (Theories of Information Processing), modeling and skills training (Social Cognitive Theory). These change methods were operationalized into practical applications (strategies) that consider the real-world clinical setting and FQHC culture including healthcare providers using convincing language to describe problems related to the vaccine, understanding the guidelines for all eligible patients, and demonstrating the ability to give a strong recommendations. The team also developed surveys to assess the impact of change methods on determinants, but due to the low response rates, it was not possible to conduct analyses for hypothesis testing. However, analysis of the completed surveys provided valuable insight into HPV vaccination practices at the FQHC.
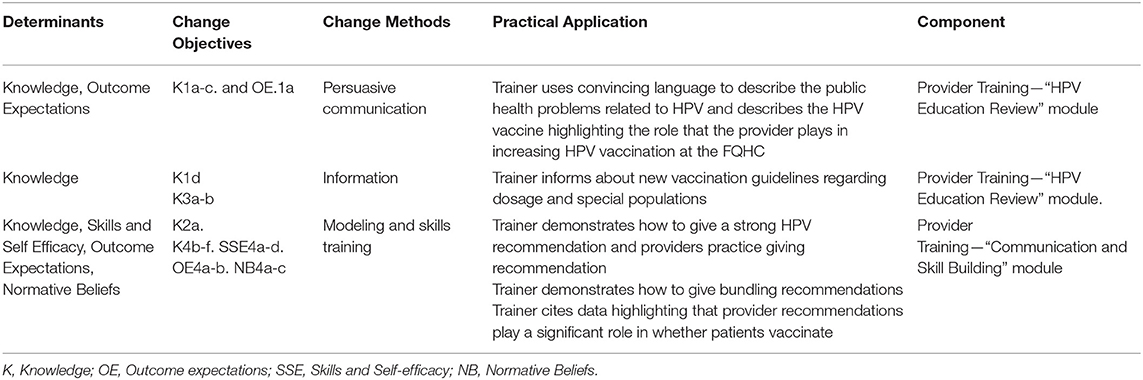
Table 3. Change methods, practical applications, and program components.
In step 4, we designed, produced, and pre-tested the components of the intervention. Program materials included detailed flowcharts, synopses and scripts, and text and image vignettes delivered via PowerPoint. The team enlisted support from cancer prevention researchers with experience designing materials for providers to produce program materials.
A gynecologic oncologist—a member of the planning group with experience conducting HPV vaccine educational sessions—delivered the in-person provider intervention, which included three components: (1) didactic instruction and education, (2) interactive role-play opportunities using tailored messages, and (3) take-home materials. The didactic educational component highlighted up-to-date research on HPV, HPV-related cancers, vaccination rates, and guidelines, and it emphasized the importance of bundled communication. Additionally, the educational component reviewed individual provider and staff roles during adolescent clinic encounters and outlined processes in place to improve HPV vaccine uptake, such as recall reminders and pre-clinic huddles. The role-playing component was designed to strengthen the communication skills required to provide a strong HPV vaccine recommendation to patients aged 11–12, 13–18, and 18–26 years in accordance with vaccination guidelines. We incorporated communication strategies that staff could use when dealing with hesitant parents and patients, as well as responses to frequently asked questions. The one time, in-person program was designed for 1 h to fit into providers work schedule and all providers also received take-home materials including a fact-sheet about HPV vaccination and clinical guidelines.
Based on feedback, the in-person intervention was recorded as a webinar so that providers and staff could view the program at any time. Two versions of the webinar were audio-recorded and delivered based on provider role (physician vs. medical assistant). Figure 2 illustrates how we designed messages that included prompts for responding to eligible patients and parents who are hesitant about the vaccine.
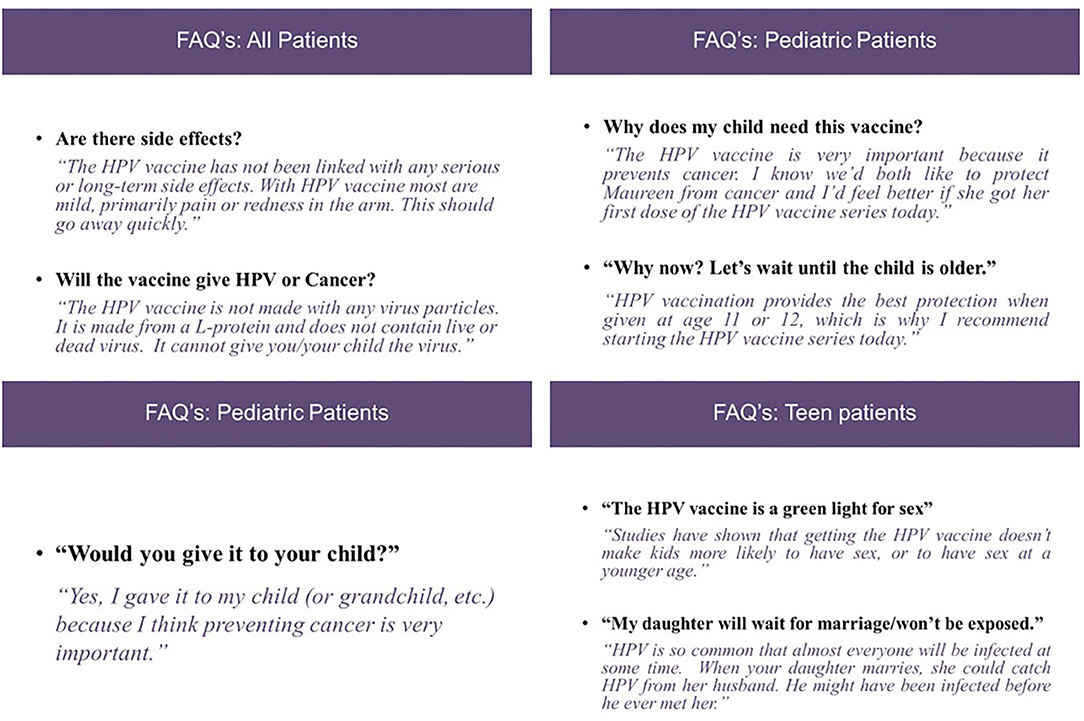
Figure 2. Example of provide responses to parental concerns around HPV vaccination.
First, the planning group identified stakeholders for the implementation of the provider training and developed detailed summaries of the tasks that implementers would need to do to successfully implement the provider training. The planning group identified two primary implementers of the program: a clinic champion, and a gynecological oncologist/HPV vaccine advocate. The gynecological oncologist was a member of the planning group and was involved in the entire planning process. Performance objectives, or sub-behaviors that the gynecological oncologist needed to do for implementation included the following: (1) preparing for the training sessions, (2) coordinating with clinic HPV champion to schedule the in-person provider training, and (3) conducting the in-person provider training. The clinic champion implementation performance objectives included: (1) overseeing implementation efforts, (2) identifying providers who needed the training, (3) providing feedback to planning committee, and (4) interacting with the research team, FQHC providers and staff as necessary to share and address barriers to implementation and provide suggestions for overcoming these barriers. Next, we identified factors (personal determinants) influencing implementation behaviors and crossed these with performance objectives. After completing the matrix of change objectives, we identified change methods to influence the determinants of implementation behaviors and operationalized these into implementation strategies that included coordination meetings with clinic champions, gynecological oncologists training and practice presentations. Between March and August 2016, the gynecological oncologist delivered the intervention to 57 FQHC providers and staff members from four clinics including 10 physicians, 32 medical assistants, 2 nurses, and various administrative staff.
Following initial in-person sessions, we conducted interviews and surveys with staff and providers who completed the in-person training to identify areas for improvement. Providers and staff participating in the surveys and interviews requested revisions to the training in order to improve program delivery by decreasing barriers to participation be creating flexible time options for completing the training and to better tailor the content. For example, results from the interviews recommended that we redesign the presentation to fit a webinar format to minimize disruption to busy clinic schedules. Additionally, the providers requested two separate modules for providers and medical assistant and a reduction in the number of slides to decrease the overall training time in hopes of reaching a larger amount of providers. FQHC providers also requested additional information around special populations including men who have sex with men, transgender, and HIV positive individuals. Through analysis of surveys and interviews, we identified additional barriers and facilitators to HPV vaccination that we used to inform the development of case studies that demonstrate how to make a strong HPV vaccine recommendation and address common parental/adolescent concerns. These case studies were incorporated into the revised webinar training.
Participatory approaches used throughout both the planning and implementation of the intervention, also informed intervention modifications at each stage of delivery. Modifications to the intervention were based on feedback and guided by of the iterative process of IM, resulting in changes to the content (to increase relevance for the specific needs of the patient population) and delivery of the HPV provider training (to increase provider participation). For example, we updated performance objective four and incorporated new information that outlined the vaccination recommendations for all eligible age groups as well as specific populations frequently served by the FQHC including the LGBTQ community, transgender people, and people with HIV. The FQHC team agreed to distribute the webinar using their online learning management system. Between April 2017 and March 2018, 133 FQHC staff competed the webinar training.
Improving healthcare provider communication is one of the most highly prioritized goals in the national movement to increase HPV vaccination rates (59). Yet, healthcare providers continue to face substantial challenges delivering strong recommendations for the HPV vaccine (26). Studies consistently recommend education and support to improve provider knowledge, skills, and comfort related to discussing the HPV vaccination with patients and parents (20, 26, 28). Yet, few published studies describe the processes used to develop interventions or incorporate theory and participatory approaches throughout the development process (60–63). Theory-driven interventions that go beyond providing information to increase knowledge or embedding cues in electronic medical records are needed to support providers in recommending HPV vaccination effectively and efficiently in a highly complex communication environment (20, 64).
In this article, we provided a comprehensive and detailed description of how we used IM to systematically develop a theory-based HPV provider intervention tailored to the needs and preferences of an FQHC. Using IM, we were able to identify and establish sub-behaviors needed to achieve the behavioral outcome and provided a blueprint to map methods and strategies to address multiple determinants derived from theory, including knowledge, skills, self-efficacy, outcome expectations, and normative beliefs. IM encourages participatory approaches to engage stakeholders as part of an iterative process of program planning, development, and implementation (35). By explicitly reporting all decisions and considerations throughout the interventions process, IM makes intervention development and planning transparent. Though beyond the scope of this paper, the FQHC did surpass its overall goal of increasing the percentage of age-eligible FQHC patients who initiate the HPV vaccine within 1 year by 7%.
The iterative and participatory process of IM may facilitate the implementation to real-world setting and support reach a larger provider audience. FQHC staff and leadership, responsible for implementing the intervention, served as members of the planning committee and played a critical role throughout the process by ensuring that the intervention addressed the needs and fit of the organization. Having staff and leadership directly involved in the process played a critical role in modifying the intervention to fit the population and demonstrated the organizations commitment which, in turn, may increase sustainability (65). We acknowledge that participatory approaches can be challenging, especially when engaging clinic leaderships and providers. Providers have many responsibilities and are not always able to take time away from the office in planning meetings, especially unpaid. We addressed this challenge by working in collaboration with clinic managers and conducting interviews and surveys with FQHC clinic staff and providers who completed the training to identify areas for improvement that resulted in revisions to the format and delivery of the intervention. The systematic and iterative process of IM allowed the team to develop and revise matrices that can continue to serve as a tool for studying and understanding the potential causal mechanisms of the intervention and for comparing approaches across interventions.
There are limitations to our development process using IM. While tailoring to the FQHCs data and delivery platforms improved reach and relevance, this may limit broader intervention scale-up to other clinics and organizations. Additionally, the provider training was designed for providers serving low income, minority communities and may not be effective in other settings since materials may not resonate for other race/ethnicity populations. However, IM provides a blueprint that allows for adaptations to different populations and settings by retaining core program components (34). Further, the ability to develop and tailor intervention components to specific context may promote the uptake of the intervention by addressing the unique needs and avoiding implementation errors (66). The iterative and participatory process of IM resulted in changes to the program delivery and the removal of change methods that may be salient to behavior change, potentially reducing effectiveness. While the multi-level intervention was successful in increasing HPV vaccination at the FQHC, we did not perform an evaluation specifically on the HPV provider intervention due to low response rates on provider surveys resulting from lack of time. As a result, it is unclear to what extent the provider intervention contributed to increased HPV vaccination rates. However, analysis of completed surveys did provide data used to identify additional barriers experienced by FQHC staff when vaccinating pediatric and adult populations.
Improving provider communication remains a prioritized goal to increase HPV vaccination coverage. This paper may provide useful insights for researchers, planners, and organizations interested in developing provider communication interventions in highly complex environments by providing a systematic framework that researchers can use to report the processes and rationale behind developing interventions. As a result, the process of IM may help to advance the development of HPV interventions at multiple levels by aiding in the interpretation of intervention findings, helping to identify causal mechanisms driving change, and assisting with adaptation by identifying core components of the intervention.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation, to any qualified researcher.
The studies involving human participants were reviewed and approved by University of Texas Health Science Center at Houston Institutional Review Board. The patients/participants provided their written informed consent to participate in this study.
MF, LS, and LR: study and manuscript conceptualization. JA: background, methods, results, and discussion. SR, LS, LR, and MF: contributed to background, methods, results, and discussion. TM: contributed to methods. All authors: contributed to the article and approved the submitted version.
This research was funded by the Cancer Prevention Research Institute of Texas grants PP140208. JA was supported by a Predoctoral Fellowship from the University of Texas Health Science Center School of Public Health's Cancer Education and Career Development Program (NIH/NCI T32CA057712).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The content is solely the responsibility of the authors and does not necessarily represent the official views of the Cancer Prevention Research Institute of Texas, the National Cancer Institute, or the National Institutes of Health.
1. Satterwhite CL, Torrone E, Meites E, Dunne EF, Mahajan R, Ocfemia MC, et al. Sexually transmitted infections among US women and men: prevalence and incidence estimates, (2008). Sex Transm Dis. (2013) 40:187–93. doi: 10.1097/OLQ.0b013e318286bb53
2. Chesson HW, Dunne EF, Hariri S, Markowitz LE. The estimated lifetime probability of acquiring human papillomavirus in the United States. Sex Transm Dis. (2014) 41:660–4. doi: 10.1097/OLQ.0000000000000193
3. Kash N, Lee MA, Kollipara R, Downing C, Guidry J, Tyring SK. Safety and efficacy data on vaccines and immunization to human papillomavirus. J Clin Med. (2015) 4:614. doi: 10.3390/jcm4040614
4. Reagan-Steiner S, Yankey D, Jeyarajah J, Elam-Evans LD, Robinette Curtis C, Macneil J, et al. National, regional, state, and selected local area vaccination coverage among adolescents aged 13-17 years - United States, (2015). Morbid Mortal Weekly Rep. (2016) 65:850–8. doi: 10.15585/mmwr.mm6533a4
5. Markowitz LE, Hariri S, Lin C, Dunne EF, Steinau M, McQuillan G, et al. Reduction in human papillomavirus (HPV) prevalence among young women following HPV vaccine introduction in the United States, National Health and Nutrition Examination Surveys, 2003-2010. J Infect Dis. (2013) 208:385–93. doi: 10.1093/infdis/jit192
6. Markowitz LE, Dunne EF, Saraiya M, Chesson HW, Curtis CR, Gee J, et al. Human papillomavirus vaccination recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Recommend Rep. (2014) 63:1–30. doi: 10.15585/mmwr.mm6832a3externalicon
7. Petrosky E, Bocchini JA Jr, Hariri S, Chesson H, Curtis RC, Saraiya M, et al. Use of 9-valent human papillomavirus (HPV) vaccine: Updated hpv vaccination recommendations of the advisory committee on immunization practices. Morbid Mortal Weekly Rep. (2015) 64:300–4.
8. Meites E, Szilagyi PG, Chesson HW, Unger ER, Romero JR, LE M. Human papillomavirus vaccination for adults: updated recommendations of the Advisory Committee on Immunization Practices. MMWR Morb Mortal Wkly Rep. (2019) 68:698–702. doi: 10.15585/mmwr.mm6832a3
9. President's Cancer Panel. HPV Vaccination for Cancer Prevention: Progress, Opportunities, and a Renewed Call to Action. A Report to the President of the United States from the Chair of the President's Cancer Panel. Bethesda, MD: President's Cancer Panel (2018).
10. Office of Disease Prevention and Health Promotion. Immunization and Infectious Diseases: Healthy People. (2020). Available online at: https://www.healthypeople.gov/node/3527/objectives#4657 (accessed June 11, 2018).
11. Walker TY, Elam-Evans LD, Yankey D, Markowitz LE, Williams CL, Fredua B, et al. National, regional, state, and selected local area vaccination coverage among adolescents aged 13-17 years - United States, 2018. Morbid Mortal Weekly Rep. (2019) 69:1109–16. doi: 10.15585/mmwr.mm6833a2
12. Dempsey A, Cohn L, Dalton V, Ruffin M. Worsening disparities in HPV vaccine utilization among 19-26 year old women. Vaccine. (2011) 29:528–34. doi: 10.1016/j.vaccine.2010.10.051
13. Gelman A, Miller E, Schwarz EB, Akers AY, Jeong K, Borrero S. Racial disparities in human papillomavirus vaccination: does access matter? J Adolesc Health. (2013) 53:756–62. doi: 10.1016/j.jadohealth.2013.07.002
14. Niccolai LM, Mehta NR, Hadler JL. Racial/ethnic and poverty disparities in human papillomavirus vaccination completion. Am J Prev Med. (2011) 41:428–33. doi: 10.1016/j.amepre.2011.06.032
15. Pruitt SL, Schootman M. Geographic disparity, area poverty, and human papillomavirus vaccination. Am J Prev Med. (2010) 38:525–33. doi: 10.1016/j.amepre.2010.01.018
16. Widdice LE, Bernstein DI, Leonard AC, Marsolo KA, Kahn JA. Adherence to the HPV vaccine dosing intervals and factors associated with completion of 3 doses. Pediatrics. (2011) 127:77–84. doi: 10.1542/peds.2010-0812
17. Ylitalo KR, Lee H, Mehta NK. Health care provider recommendation, human papillomavirus vaccination, and Race/Ethnicity in the US national immunization survey. Am J Public Health. (2013) 103:164–9. doi: 10.2105/AJPH.2011.300600
18. Dempsey AF, Pyrzanowski J, Lockhart S, Campagna E, Barnard J, O'Leary ST. Parents' perceptions of provider communication regarding adolescent vaccines. Hum Vaccines Immunother. (2016) 12:1469–75. doi: 10.1080/21645515.2016.1147636
19. Dorell C, Yankey D, Kennedy A, Stokley S. Factors that influence parental vaccination decisions for adolescents, 13 to 17 years old: National Immunization Survey-Teen, 2010. Clin Pediatr. (2013) 52:162–70. doi: 10.1177/0009922812468208
20. Gilkey MB, McRee A-L. Provider communication about HPV vaccination: a systematic review. Hum Vaccines Immunother. (2016) 12:1454–68. doi: 10.1080/21645515.2015.1129090
21. Gottlieb SL, Brewer NT, Sternberg MR, Smith JS, Ziarnowski K, Liddon N, et al. Human papillomavirus vaccine initiation in an area with elevated rates of cervical cancer. J Adolesc Health. (2009) 45:430–7. doi: 10.1016/j.jadohealth.2009.03.029
22. Guerry SL, De Rosa CJ, Markowitz LE, Walker S, Liddon N, Kerndt PR, et al. Human papillomavirus vaccine initiation among adolescent girls in high-risk communities. Vaccine. (2011) 29:2235–41. doi: 10.1016/j.vaccine.2011.01.052
23. Vadaparampil ST, Malo TL, Kahn JA, Salmon DA, Lee JH, Quinn GP, et al. Physicians' human papillomavirus vaccine recommendations, 2009 and 2011. Am J Prev Med. (2014) 46:80–4. doi: 10.1016/j.amepre.2013.07.009
24. Allison MA, Hurley LP, Markowitz L, Crane LA, Brtnikova M, Beaty BL, et al. Primary care physicians' perspectives about HPV vaccine. Pediatrics. (2016) 137:e20152488. doi: 10.1542/peds.2015-2488
25. Kulczycki A, Qu H, Shewchuk R. Primary care physicians' adherence to guidelines and their likelihood to prescribe the human papillomavirus vaccine for 11- and 12-year-old girls. Women's Health Issues. (2016) 26:34–39. doi: 10.1016/j.whi.2015.07.012
26. Holman DM, Benard V, Roland KB, Watson M, Liddon N, Stokley S. Barriers to human papillomavirus vaccination among US adolescents: a systematic review of the literature. JAMA Pediatr. (2014) 168:76–82. doi: 10.1001/jamapediatrics.2013.2752
27. McRee AL, Gilkey MB, Dempsey AF. HPV vaccine hesitancy: findings from a statewide survey of health care providers. J Pediatr Health Care. (2014) 28:541–9. doi: 10.1016/j.pedhc.2014.05.003
28. Smulian EA, Mitchell KR, Stokley S. Interventions to increase HPV vaccination coverage: a systematic review. Hum Vaccin Immunother. (2016) 12:1566–88. doi: 10.1080/21645515.2015.1125055
29. Niccolai LM, Hansen CE. Practice- and community-based interventions to increase human papillomavirus vaccine coverage: a systematic review. JAMA Pediatr. (2015) 169:686–92. doi: 10.1001/jamapediatrics.2015.0310
30. Fu LY, Bonhomme LA, Cooper SC, Joseph JG, Zimet GD. Educational interventions to increase HPV vaccination acceptance: a systematic review. Vaccine. (2014) 32:1901–20. doi: 10.1016/j.vaccine.2014.01.091
31. Garbutt JM, Dodd S, Walling E, Lee AA, Kulka K, Lobb R. Theory-based development of an implementation intervention to increase HPV vaccination in pediatric primary care practices. Implement Sci. (2018) 13:45. doi: 10.1186/s13012-018-0729-6
32. Glanz K, Bishop DB. The role of behavioral science theory in development and implementation of public health interventions. Annu Rev Public Health. (2010) 31:399–18. doi: 10.1146/annurev.publhealth.012809.103604
33. Davies P, Walker AE, Grimshaw JM. A systematic review of the use of theory in the design of guideline dissemination and implementation strategies and interpretation of the results of rigorous evaluations. Implement Sci. (2010) 5:14. doi: 10.1186/1748-5908-5-14
34. Fernandez ME, Ruiter RAC, Markham CM, Kok G. Intervention mapping: theory- and evidence-based health promotion program planning: perspective and examples. Front Public Health. (2019) 7:209. doi: 10.3389/fpubh.2019.00209
35. Bartholomew LK, Markham CM, Ruiter RAC, Fernandez ME, Kok G, Parcel GS. Planning Health Promotion Programs: An Intervention Mapping Approach. 4 ed. San Francisco, CA: Jossey-Bass (2016).
36. Fernandez ME, Savas LS, Lipizzi E, Roncancio AM, Khan MM, Fernandez-Espada N, et al. Evaluation of two HPV vaccination educational interventions for hispanic parents. Paper Presented at: Poster. Austin, TX (2015).
37. Rodriguez SA, Roncancio AM, Savas LS, Lopez DM, Vernon SW, Fernandez ME. Using intervention mapping to develop and adapt two educational interventions for parents to increase HPV vaccination among hispanic adolescents. Front Public Health. (2018) 6:164. doi: 10.3389/fpubh.2018.00164
38. Fernandez ME, Gonzales A, Tortolero-Luna G, Partida S, Bartholomew LK. Using intervention mapping to develop a breast and cervical cancer screening program for Hispanic farmworkers: Cultivando La Salud. Health Promot Pract. (2005) 6:394–404. doi: 10.1177/1524839905278810
39. Hou SI, Fernandez ME, Parcel GS. Development of a cervical cancer educational program for Chinese women using intervention mapping. Health Promot Pract. (2004) 5:80–7. doi: 10.1177/1524839903257311
40. Vernon SW, del Junco DJ, Tiro JA, Coan SP, Perz CA, Bastian LA, et al. Promoting regular mammography screening II. Results from a randomized controlled trial in US women veterans. J Natl Cancer Inst. (2008) 100:347–58. doi: 10.1093/jnci/djn026
41. Byrd TL, Wilson KM, Smith JL, Heckert A, Orians CE, Vernon SW, et al. Using intervention mapping as a participatory strategy: development of a cervical cancer screening intervention for Hispanic women. Health Educ Behav. (2012) 39:603–11. doi: 10.1177/1090198111426452
42. Scarinci IC, Bandura L, Hidalgo B, Cherrington A. Development of a theory-based (PEN-3 and Health Belief Model), culturally relevant intervention on cervical cancer prevention among Latina immigrants using intervention mapping. Health Promot Pract. (2012) 13:29–40. doi: 10.1177/1524839910366416
43. Fernandez ME, Savas LS, Carmack CC, Chan W, Lairson DR, Byrd TL, et al. A randomized controlled trial of two interventions to increase colorectal cancer screening among Hispanics on the Texas-Mexico border. Cancer Causes Control. (2015) 26:1–10. doi: 10.1007/s10552-014-0472-5
44. Highfield L, Valerio MA, Fernandez ME, Eldridge-Bartholomew LK. Development of an implementation intervention using intervention mapping to increase mammography among low income women. Front Public Health. (2018) 6:300. doi: 10.3389/fpubh.2018.00300
45. Bartholomew LK, Cushman WC, Cutler JA, Davis BR, Dawson G, Einhorn PT, et al. Getting clinical trial results into practice: design, implementation, and process evaluation of the allhat dissemination project. Clintrials. (2009) 6:329–43. doi: 10.1177/1740774509338234
46. Donaldson A, Lloyd DG, Gabbe BJ, Cook J, Finch CF. We have the programme, what next? Planning the implementation of an injury prevention programme. Injury Prev. (2017) 23:273–80. doi: 10.1136/injuryprev-2015-041737
47. Highfield L, Hartman MA, Mullen PD, Rodriguez SA, Fernandez ME, Bartholomew LK. Intervention mapping to adapt evidence-based interventions for use in practice: increasing mammography among African American women. Biomed Res Int. (2015) 2015:160103. doi: 10.1155/2015/160103
48. Peskin MF, Hernandez BF, Gabay EK, Shegog R, Cuccaro P, Li D, et al. Using intervention mapping to develop iCHAMPSS: a web-based decision support system to help school districts adopt, Implement, and Maintain effective sexual health programs. In: Bartholomew LK, Markham C, Ruiter RAC, Fernandez ME, Kok G, Parcel G, editors. Planning Health Promotion Programs. An Intervention Mapping Approach. San Francisco, CA; Hoboken, NJ: Jossey-Bass A John Wiley & Sons Brand (2016). p. 367.
49. Fernandez ME, Allen JD, Mistry R, Kahn JA. Integrating clinical, community, and policy perspectives on human papillomavirus vaccination. Annu Rev Public Health. (2010) 31:235–52. doi: 10.1146/annurev.publhealth.012809.103609
50. Savas LS, Fernandez ME, Jobe D, Carmack CC. Human papillomavirus vaccine: 2-1-1 helplines and minority parent decision-making. Am J Prev Med. (2012) 43(Suppl. 5):S490–6. doi: 10.1016/j.amepre.2012.09.003
51. Morales-Campos DY, Markham CM, Peskin MF, Fernandez ME. Hispanic mothers' and high school girls' perceptions of cervical cancer, human papilloma virus, and the human papilloma virus vaccine. J Adolesc Health. (2013) 52(Suppl. 5):S69–75. doi: 10.1016/j.jadohealth.2012.09.020
52. Glenn BA, Tsui J, Coronado GD, Fernandez ME, Savas LS, Taylor VM, et al. Understanding HPV vaccination among Latino adolescent girls in three U.S. regions. J Immigr Minor Health. (2015) 17:96–103. doi: 10.1007/s10903-014-9996-8
53. Fernandez ME, McCurdy SA, Arvey SR, Tyson SK, Morales-Campos D, Flores B, et al. HPV knowledge, attitudes, and cultural beliefs among Hispanic men and women living on the Texas-Mexico border. Ethn Health. (2009) 14:607–24. doi: 10.1080/13557850903248621
54. Antonacci G, Reed JE, Lennox L, Barlow J. The use of process mapping in healthcare quality improvement projects. Health Serv Manage Res. (2018) 31:74–84. doi: 10.1177/0951484818770411
55. Ward J, Clarkson J, Morris Z, Jun GT. Health care process modelling: which method when? Int J Qual Health Care. (2009) 21:214–24. doi: 10.1093/intqhc/mzp016
56. Bandura A. Human agency in social cognitive theory. Am Psychol. (1989) 44:1175–84. doi: 10.1037/0003-066X.44.9.1175
57. Bandura A. Social cognitive theory: an agentic perspective. Ann Rev Psychol. (2001) 52:1–26. doi: 10.1146/annurev.psych.52.1.1
58. Bandura A. Self-efficacy: toward a unifying theory of behavioral change. Psychol Rev. (1977) 84:191–215. doi: 10.1037/0033-295X.84.2.191
59. Rimer B, Harper H, Witte O. Accelerating HPV Vaccine Uptake: Urgency for Action to Prevent Cancer; A Report to the President of the United States from the President's Cancer Panel. Bethesda, MD: National Cancer Institute (2014).
60. Albrecht L, Archibald M, Arseneau D, Scott SD. Development of a checklist to assess the quality of reporting of knowledge translation interventions using the Workgroup for Intervention Development and Evaluation Research (WIDER) recommendations. Implement Sci. (2013) 8:52. doi: 10.1186/1748-5908-8-52
61. Hoffmann TC, Glasziou PP, Boutron I, Milne R, Perera R, Moher D, et al. Better reporting of interventions: template for intervention description and replication (TIDieR) checklist and guide. BMJ. (2014) 348:g1687. doi: 10.1136/bmj.g1687
62. Garcini LM, Galvan T, Barnack-Tavlaris JL. The study of human papillomavirus (HPV) vaccine uptake from a parental perspective: a systematic review of observational studies in the United States. Vaccine. (2012) 30:4588–95. doi: 10.1016/j.vaccine.2012.04.096
63. Brewer NT, Fazekas KI. Predictors of HPV vaccine acceptability: a theory-informed, systematic review. Prev Med. (2007) 45:107–14. doi: 10.1016/j.ypmed.2007.05.013
64. Hswen Y, Gilkey MB, Rimer BK, Brewer NT. Improving physician recommendations for human papillomavirus vaccination: the role of professional organizations. Sexually Transmitt Dis. (2017) 44:42–7. doi: 10.1097/OLQ.0000000000000543
65. Shelton RC, Cooper BR, Stirman SW. The sustainability of evidence-based interventions and practices in public health and health care. Ann Rev Public Health. (2018) 39:55–76. doi: 10.1146/annurev-publhealth-040617-014731
Keywords: HPV vaccination, provider communication, intervention mapping, intervention development, cancer prevention
Citation: Austin JD, Rodriguez SA, Savas LS, Megdal T, Ramondetta L and Fernandez ME (2020) Using Intervention Mapping to Develop a Provider Intervention to Increase HPV Vaccination in a Federally Qualified Health Center. Front. Public Health 8:530596. doi: 10.3389/fpubh.2020.530596
Received: 29 January 2020; Accepted: 18 November 2020;
Published: 18 December 2020.
Edited by:
Rosemary M. Caron, University of New Hampshire, United StatesReviewed by:
Krista Mincey, Xavier University of Louisiana, United StatesCopyright © 2020 Austin, Rodriguez, Savas, Megdal, Ramondetta and Fernandez. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Maria E. Fernandez, bWFyaWEuZS5mZXJuYW5kZXpAdXRoLnRtYy5lZHU=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.