 Amy A. Eyler
Amy A. Eyler Cheryl R. Valko
Cheryl R. Valko Katherine A. Curoe
Katherine A. Curoe Ramya Ramadas
Ramya Ramadas Jamie F. Chriqui
Jamie F. Chriqui- 1Prevention Research Center in St. Louis, Brown School, Washington University in St. Louis, St. Louis, MO, United States
- 2Division of Health Policy and Administration and Institute for Health Research and Policy, School of Public Health, University of Illinois at Chicago, Chicago, IL, United States
Background: Preschool years are an important time for shaping healthy eating behaviors. Childcare centers can be a venue for policy change for broad and sustained positive impact on healthy eating environment. The objectives of this study were to assess how self-reported current practices align with updated statewide childcare center licensing regulations in Colorado, US, and to explore correlates of adherence.
Methods: Using a post-test only study design, a survey was sent to all full-day, licensed childcare centers in Colorado (N = 1,398) with a valid street or email address. The survey included questions on allowable food and beverages, mealtime practices, and perceptions of the updated regulations. Frequencies were calculated and logistic regression models computed for a composite score of each of these factors.
Results: Respondents (N = 344) were mostly center directors, with over 8 years of experience, from urban areas. Compliance was high for most food and beverage criteria (over 90%) and all meal practices. One third participated in the federal Child and Adult Care Food Program (CACFP), and were more likely to comply with the state meal regulations than non-CACFP centers.
Conclusion: Although our results show high self-reported compliance, a more thorough study of the policy process would provide comprehensive evidence on effective development, enactment, and implementation of these regulations.
Introduction
Preventing obesity in young children holds promise for reversing the epidemic of childhood obesity (1) Among 2–5 year olds in the United States, the rate of obesity has more than doubled, up from 5% in 1980, to 13.9% in 2015 (2). The increased rate in this group, as well as in older children and adolescents, has made childhood obesity one of the most serious public health challenges of the twenty first century (1, 3).
The preschool years are an important time for promoting healthy eating, as behaviors developed in this period may persist into adulthood (4, 5). An especially relevant setting for nutrition interventions in this age group is the childcare center (6). It is estimated that 80% of preschool age children in the United States spend an average of 40 h a week in out-of-home childcare (7). Because of the number of meals and snacks that children consume during their time in childcare, policies that outline healthy eating and mealtime practice guidelines can be effective and sustainable strategies to increase healthy eating (1, 6). Policies prohibiting serving sugar-sweetened beverages to children, for instance, may help them develop preferences for water or milk during mealtimes (8).
Childcare centers are governed by federal, state, and organizational policies. For example, centers may opt to participate in the Child and Adult Care Food Program (CACFP). CACFP is a federal program that reimburses centers for the cost of eligible meals and snacks served to enrolled children, targeting those children most in need (9). In response to the childhood obesity epidemic and other national child health efforts, recently updated CACFP meal pattern standards require childcare centers to serve more whole grains, a wider variety of fruits and vegetables, and less solid fats and added sugars (9). In addition to national policies, states have the opportunity to set healthy food requirements, as childcare licensing occurs at the state level. Childcare licensing requirements can be outlined in state statutes and/or regulations and the criteria for licensure varies by state.
The state of Colorado recently adopted new criteria for childcare center licensure, including changes in healthy eating requirements. Efforts began in 2015 when the Colorado Department of Human Services Office of Early Childhood and the Colorado Board of Health worked together to develop and approve the new standards. These regulations ensure that all food provided in childcare centers meets CACFP requirements (9, 10), and prohibits sugar-sweetened beverages from being served. Regulations also outline new standards for menu planning and mealtime practices. In addition to nutrition changes, these regulations also specify required amounts of physical activity and limit screen time. Past criteria for licensure did not provide explicit guidance for these nutrition and physical activity requirements. These new standards, in addition to the full list of childcare licensing regulations are the minimum health, safety, and program requirements licensed childcare providers must follow to operate legally. Several agencies offered assistance for centers needing information or other resources in order to comply with the new regulations (10). More than 100,000 children in the state will be impacted by these standards, which took effect February 2016, with full implementation required by September 2016 (11).
The American Heart Association's Voices for Healthy Kids is an advocacy program to improve or create equitable policies that will make the places children live, learn, and play healthier. As part of an evaluation of their policy advocacy efforts, the goals of the current study were to assess self-reported adherence to the updated Colorado childcare regulations related to nutrition, explore perceptions of preparedness for implementation, and identify the use of technical assistance. This study also aimed to identify correlates of reported adherence.
Materials and Methods
Survey Development and Administration
Changes in the state childcare licensing regulations related to nutrition informed the survey questions (see Table 1). Questions included topics such as meal preparation and length of meal times. Other mealtime practices such as use of TV/media and staff member supervision were also included. Because of the requirement changes in allowable beverages, we added questions on the practice of serving water, milk, juice, and soda. In addition to the assessment of the regulatory changes, the survey included characteristics of the respondent and the center for use as independent variables in analyses. These included title/role of respondent, ages served, ownership, staff count, and capacity. We also assessed participation in CACFP and/or the Head Start/Early Head Start Program. Similar to CACFP, Head Start (for children ages 3–4) and Early Head Start (for infants and toddlers) are federally funded program to support quality childcare for low-income families. As a proxy for socioeconomic status of overall clientele, we asked for information on average weekly rate of childcare. These characteristics were important to assess as we hypothesized that centers in urban locations, having larger center capacity size and higher income clientele would correlate with higher adherence to the regulations. The last section of the survey assessed familiarity with the regulation changes, preparation for and implementation of new regulations, additional resources needed, and use of technical assistance. Participants could choose to receive a $20 Amazon gift card for completing the survey to their preferred delivery method, either electronically or via mail. The survey was pilot tested with content experts and aligned with other childcare center food and beverage research (12, 13). One center director, three researchers, and a biostatistician previewed the survey for content and flow. The survey is available in Data Sheet 1: Survey of Child Care Sites in Colorado.
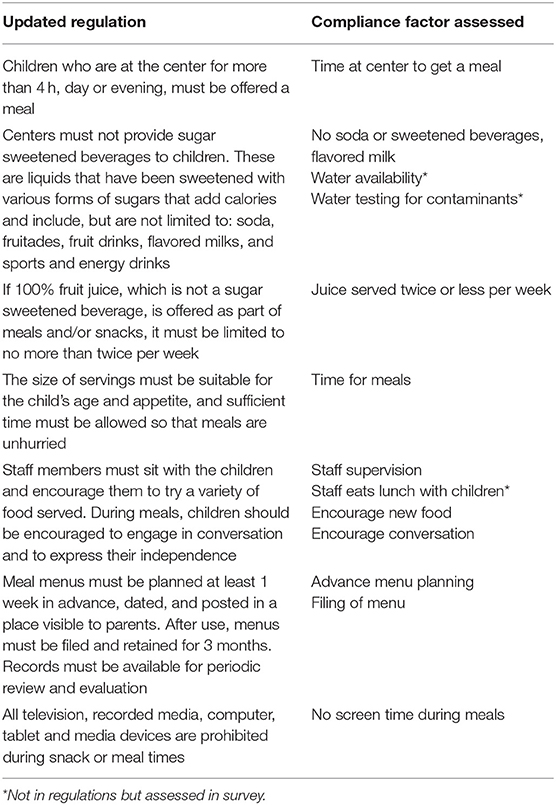
Table 1. Regulation language and related compliance factor assessed in the survey.
Sample
The sample for the survey was all licensed, full-day childcare centers in the state of Colorado that enroll infants and children ages 0–5. We used a 2015 list (N = 1,441) of center names and addresses available from the state's early childhood website (https://data.colorado.gov/Early-childhood/Colorado-Licensed-Child-Care-Facilities-Report/a9rr-k8mu/data). Center contact information was obtained through publicly available data on childcare center webpages. Fourteen centers were no longer open for business at the time of data collection. We found valid email addresses for 963 centers and used street addresses to contact the remaining 435 centers via US Postal Service. Twenty-nine centers had neither valid emails nor street addresses, resulting in a total N = 1,398 for email and postal surveys. An invitation to participate was sent along with a project information page describing the study. The information page stated the survey was voluntary, questions could be skipped, and that the data would only be used in aggregate. Participants were asked to provide an email address if they wished to receive the incentive. The Institutional Review Board at Washington University in St. Louis approved this study.
Data Collection
Data were collected February-April 2018, which was 16 months after the required date of September 2016 for compliance with updated regulations. Email participants received one initial email inviting them to participate in the study and one reminder each week for 4 weeks. Only non-responders received reminder emails. Each email contained a link to the online survey (using the online survey platform Qualtrics.com) and consent information. Centers lacking email addresses received an introductory letter, consent information, the survey, and a self-addressed, postage-paid return envelope. No reminders were sent to those receiving postal surveys.
Analysis
Data from the online survey platform was imported into a Stata Version 15 database (Statacorp LLC, College Station, Texas). The research team manually entered data from the mailed surveys into this database. Frequencies of responses, means, and standard deviations were calculated. Two multiple logistic regression models were computed as part of our analyses. For each model, correlates were center capacity, rural urban commuting area (RUCA) classification (14), CACFP status (yes/no), status as independent center vs. corporate owned/franchise, and average weekly rate for children 2–5. A binomial logistic regression was computed individually against each correlate. Significant correlates (p < 0.05) were put into a larger, adjusted model. Regression diagnostics (Link-tests, correlations, variance inflation projections, and tolerance) were run on the final adjusted models. In the first model, the outcome variable was compliance with the regulations. Since there was little variability in the data set, as most centers reported adherence to the new regulations, aggregate adherence measures were created for meals and drinks, and separated by the age of children served (<2 years and 2+ years). Since none of the centers met all four drink variables, meeting three out of the four regulations was compared to meeting two or less regulations. The second regression model was based on implementation. The outcome variable for this model was readiness to implement updates regulations (i.e., very prepared to implement vs. somewhat/not at all prepared).
Results
We received 256 completed online surveys and 88 completed paper surveys for 344 responses (response rate of 25%). This response rate is comparable to other recent early childcare surveys (12, 13, 15, 16). There was no significant difference in the size of center, CACFP participation, or geographic location between responding and non-responding centers. Table 2 depicts general characteristics of respondents and centers. Most respondents were Center Directors or Assistant Directors (64.1%) with a mean of 8.7 years (SD = 8.5) in their current role. About one-third of centers participated in CACFP (32.7%). Most centers were in urban locations (74.6%) and had an average of 17 staff on site (SD = 17.8). The average weekly rate for children <2 years of age was $309, and $319 for children aged 2–5. The average time (in hours) a child must be at the center to receive a meal was 2.5 (SD = 2.1). Mealtimes were an average of 36 min for children aged 2–5, and 34 min for school age children.
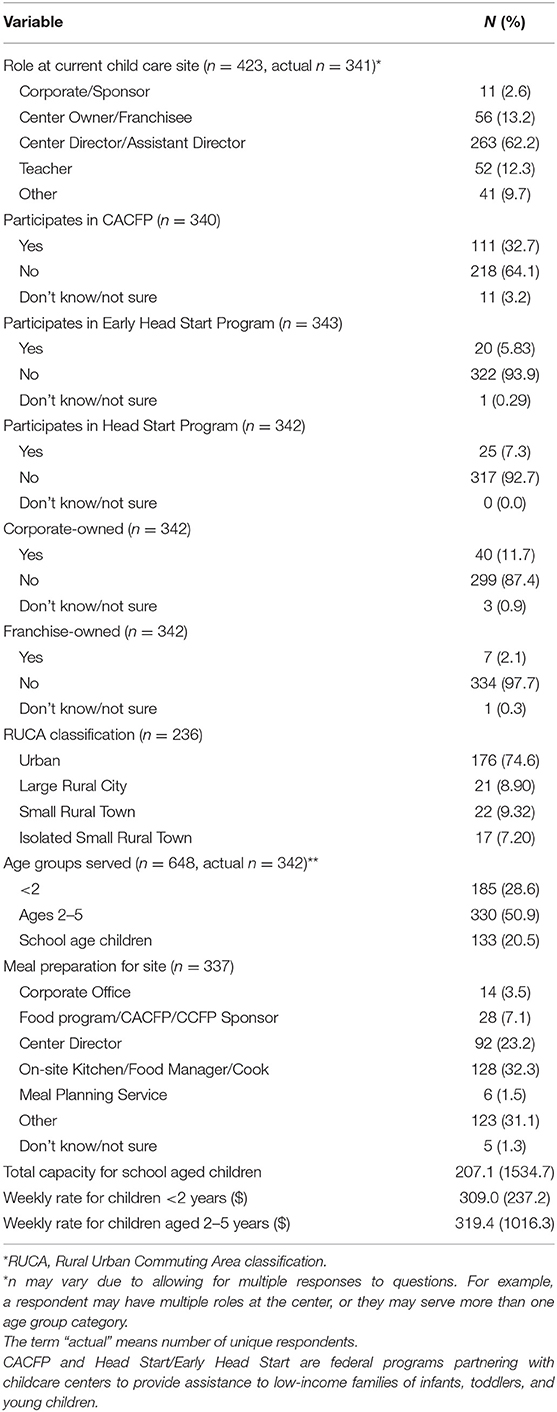
Table 2. General characteristics of Colorado Childcare Regulations Survey participants.
Overall self-reported adherence with the updated regulations was high for respondents of our survey (see Table 3). Most centers reported meeting the requirement of at least 1 week advance meal planning (73.1%) and keeping menus on file for at least 3 months (86.3%). Ninety-five percent of centers had staff sit with children when eating. Although not a requirement, we asked if staff members eat lunch with the children, and less than half reported doing so (41.1%). All respondents encouraged children to engage in conversation during meals, 98.5% indicated that staff encouraged children to try a variety of food during meals, and 97.6% reported prohibiting television or videos during mealtime.
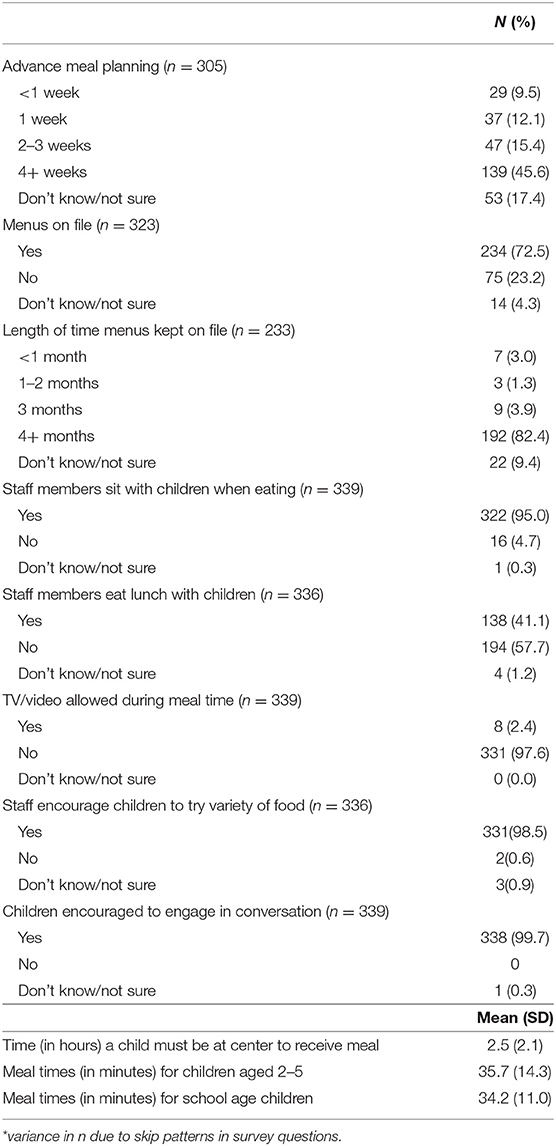
Table 3. Number and percentage of self-reported food environment regulation adherence.
There were several updated regulations relating to allowable drinks served at childcare centers (see Table 4). Almost all of the centers had clean, fresh water available (99.4%), and 71.1% reported regularly testing water for contaminants. No center indicated allowing soda, and most never served fruit drinks (96.6%). The percentage of centers serving flavored milk once or more a day was 11.5% for children ages 2–5 and 13.7% for school aged children.
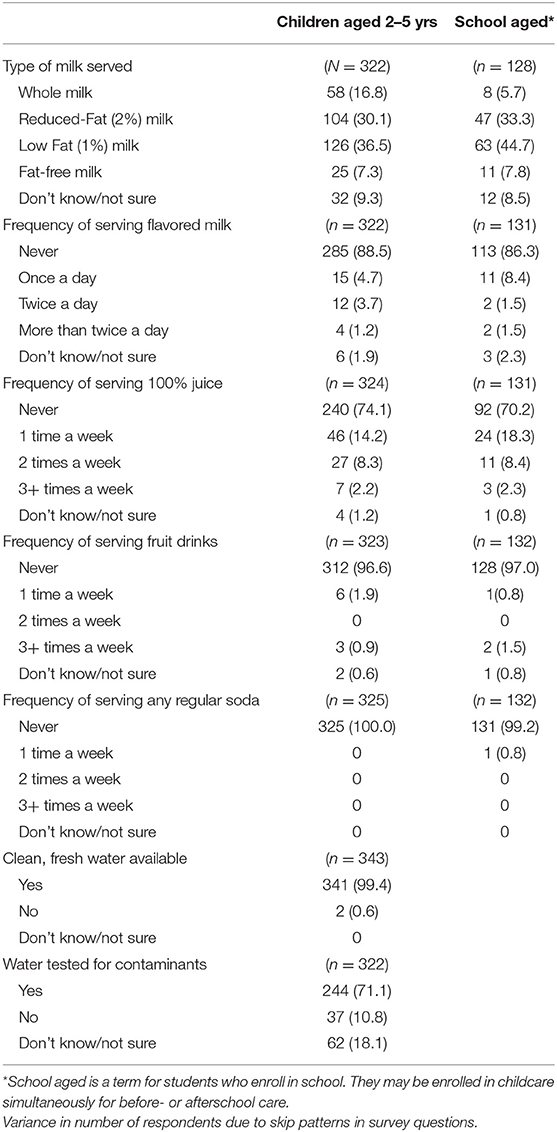
Table 4. Self-reported adherence to regulations related to beverages served in Colorado childcare centers.
Few centers (12.8%) reported not being familiar with the Colorado childcare center regulation updates, and most indicated being somewhat or very much prepared for implementation (96.4%) (see Table 5). About a third (31.5%) indicated that they began implementation of the updated regulations prior to February 2016, and 41.3% reported that no changes were needed because their practices already met the updates. Only 9.2% of respondents indicated that their centers received technical assistance in order to meet the requirements of the updated regulations.
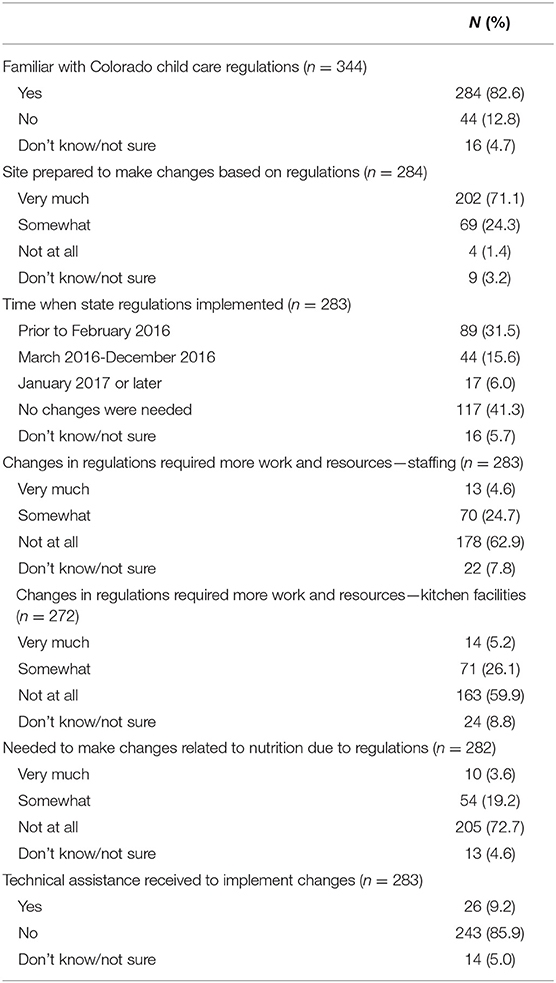
Table 5. Perceptions of regulation preparedness.
There were few significant results from the regression models (see Table 6). The only variables emerging significant in binomial logistic regression were CACFP status and RUCA, which were used in the adjusted regression models. Childcare centers in isolated rural towns had 2.57 higher odds of complying with all meal regulations compared to those in urban areas, but this finding did not remain significant in the adjusted model (AOR 2.23; 95% CI 0.82–6.08). Centers participating in CACFP were almost four times as likely to meet all seven meal regulations than centers not participating in this federal program, and these odds remained statistically significant in the adjusted regression model (AOR 3.87; 95% CI 2.38–6.31). Independent status, total capacity, or weekly rate did not emerge as significant correlates. For compliance with three drink regulations as the outcome vs. meeting less than three drink regulations, odds ratios for total capacity and weekly rate for 2–5 year olds were statistically significant in the adjusted model. For every one unit (one dollar) increase in the weekly rate for 2–5 year olds, the odds of complying will three regulations increased by 1.006 (95% CI: 1.002–1.009). None of the odds ratios for the outcome variables related to readiness to implement were statistically significant; therefore, an aggregate model was not computed.
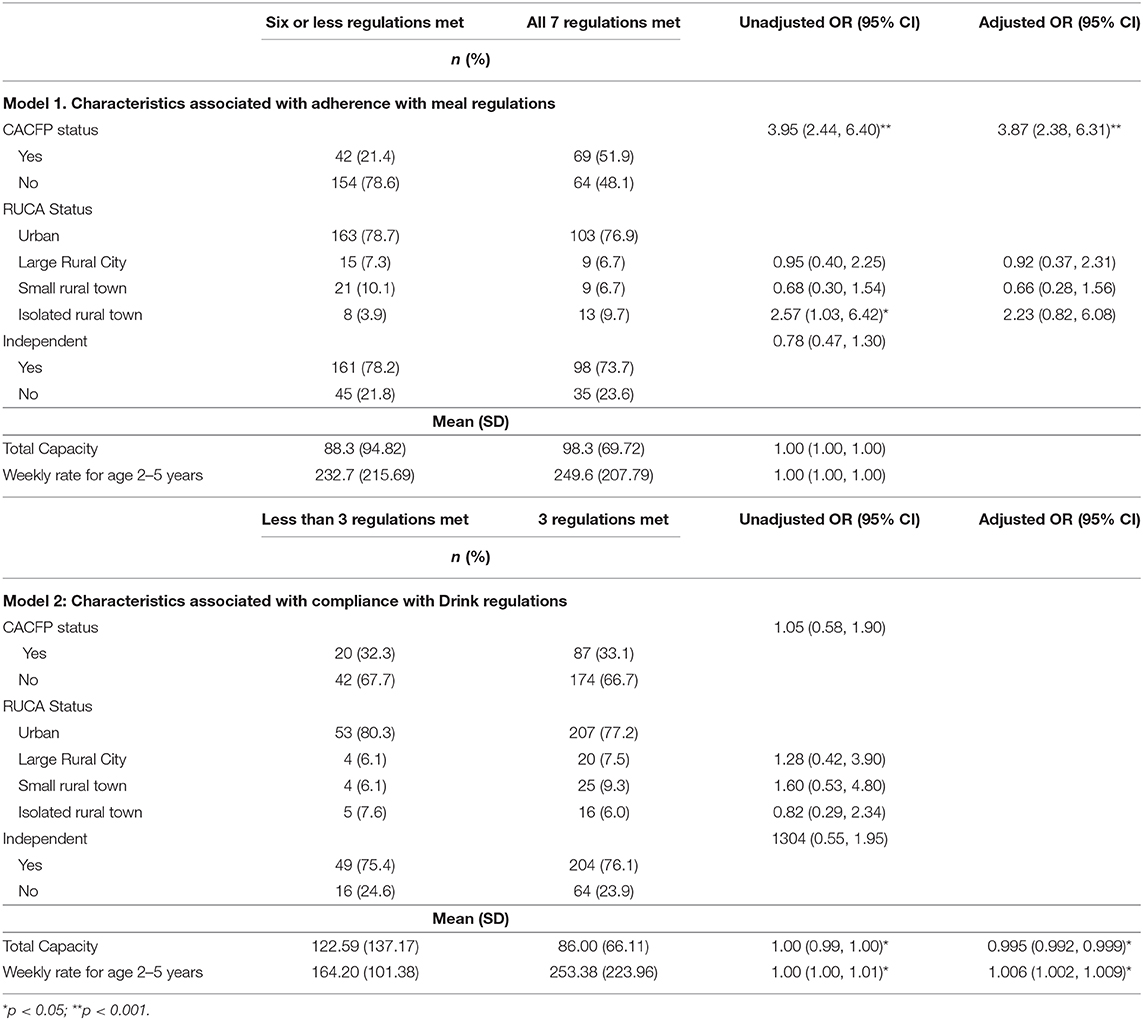
Table 6. Regression models for updated regulation adherence.
Discussion
Policies are an important element in influencing early eating behavior and childhood obesity prevention (1, 3, 17). Policies and regulations for child care are especially relevant due to their broad reach and sustainability (1, 6). However, enactment of the policies must be followed by correct interpretation and timely implementation to achieve the intended outcome (18). There was very high self-reported adherence with all components of the new Colorado childcare regulations, and this may be due to several factors. First, Colorado is one of the healthiest states in the nation. It has the lowest prevalence of adult obesity (19) and ranks second lowest in childhood obesity rates for 2–4 year olds enrolled in the Women, Infants, and Children (WIC) federal nutrition assistance program (20). These rates may be due, in part, to policy priorities for health and thus sets the tone for a culture of adherence within the state. In addition, national publicity and programming to reduce childhood obesity may have helped increase awareness of the changes needed. For example, updated federal requirements for food and snacks served in public schools (20), the presidential priority on childhood obesity prevention (21), and the increasing evidence of detrimental effects of sugar-sweetened beverages may have primed the childcare centers for the regulatory changes in Colorado (20, 22). Many federal requirements for centers receiving CACFP funds align with the Colorado regulations (e.g., prohibiting sugar-sweetened beverages) (8). Centers participating in CACFP would likely already be compliant as indicated by our findings that they were four times more likely to meet all meal regulations than non-CACFP sites. As such, over 40% of participants reported needing no changes because existing policies already met the new requirements. However, this still leaves room for improvement in non-CACFP centers. Second, we assessed aspects of the regulations almost 16 months after required implementation. This gave the centers sufficient time to learn about licensure changes and make use of technical assistance provided by the state and advocacy organizations. Preparation by the centers to adhere to the new regulation may have decreased the need for technical assistance related to implementation. Over 95% of the participants in this study reported being prepared to implement the new regulations, and only 9.2% reported receiving technical assistance. Perhaps a more explicit definition of technical assistance and assessing a timeframe in which it was sought or used would have shown different results. Future studies should include implementation assessment throughout the course of the policy process; from development, enactment, and beyond. This would provide insight on when technical assistance would be most beneficial.
Although our findings showed high self-reported adherence, there is room for improvement. None of respondents allowed regular soda to be served to children, but over 10% indicated serving flavored milk, which contains a significant amount of added sugar. Developing materials for enhanced awareness of specific allowable foods may be helpful to reach 100% compliance.
Positive mealtime experiences in youth can help shape healthy eating behaviors later in life (4, 5, 23). The updated Colorado regulations included several aspects of positive mealtimes including adequate time for eating, no television/video, encouraging conversation, and promoting new foods. Over 95% of participants reported mealtime practices outlined in the regulations were being implemented. Additionally, role modeling behavior is important to developing healthy eating behaviors (16, 24). Even though requiring staff to eat meals with the children was not part of the licensing regulations, we inquired about this practice in the survey. Fewer than half of respondents reported doing so. More research is needed on the impact of childcare staff modeling healthy eating on the development of eating habits in young children.
There is evidence that characteristics of childcare centers such as location and CACFP participation may influence implementation of nutrition policies (25–28). We theorized that larger, urban childcare centers serving higher income populations would have higher adherence to the regulations. However, our logistic regression models resulted in few statistically significant findings. This points to equitable practices in centers across the state and adherence even without CACFP participation.
Policies governing childcare nutrition practices have an important role in child obesity prevention (1, 29). Monitoring for adoption and compliance of these policies is needed to facilitate intended policy impact. While self-reported compliance was high in our Colorado study, results from other US studies vary. For example, a cross-sectional study of Rhode Island childcare center directors also showed comparable compliance with prohibition of sugar-sweetened beverages (30). However, results from a study of adherence in Nebraska childcare centers found sub-optimal reported implementation (80% or less) of several nutrition best practices (25). A Delaware assessment showed compliance ranging from 35.6% for water availability outside to 88% for juice type (31). National studies on federal CACFP regulations also yield mixed self-reported compliance (12, 13). Continuing to strengthen state and national standards, and comprehensively monitoring childcare centers compliance with those standards will enhance the potential for improving childhood obesity prevalence.
Although findings from this study show healthy food environments and practices in Colorado childcare centers, several limitations should be noted. First, Colorado is one of the healthiest states in the United States, particularly related to obesity. Healthy nutrition practices may have been standard prior to the regulation changes. Our post-test only study design did not allow for assessment of change in practices before and after the new regulation. Having baseline data would have strengthened evidence of policy implementation, but we were constrained by timing of the project. We developed the survey to assess variables unique to the Colorado regulations, and thus could not rely on existing validated measures. Best practices for survey research (32, 33) including the use of incentives, follow-up, and the use of email and mail surveys resulted in a response rate of 25%, and the participants may not be representative of all childcare centers in the state, thus generalization is limited. However, when we compared respondent sites to non-respondent sites from the sample list, there were no significant differences in the center characteristics of size of center, CACFP participation, or geographic location. Additionally, social desirability bias may have influenced responses because we were assessing implementation of requirements for licensure. Another limitation was although the survey was sent to the director, it may have been delegated to other staff. We did not collect information on perception of importance by the director, and delegation may have been influenced by low acceptability. These regulations apply to only licensed early childcare centers and do not include licensed home-based day care. There were 1,509 licensed home-based centers in Colorado in 2014, with the capacity to serve almost 9,000 children. Because of the prevalence of home-based day care, this is an important area for future study. In spite of these limitations, our study contributes to knowledge on the potential for policy to influence healthy food practices and environment in childcare centers.
Conclusion
Policies and regulations for childcare centers have the potential to increase exposure to healthy eating environments in early childhood. Although our results show high self-reported preparedness, adherence to the updated regulations and low use of technical assistance, a more thorough study of the policy process would provide comprehensive evidence on effective development, enactment, and implementation of these regulations.
Data Availability Statement
The datasets generated for this study are available on request to the corresponding author.
Ethics Statement
This study was exempt per 45 CFR 46.101(b) (2) of the Federal Policy for the Protection of Human Subjects (Common Rule). The protocol was approved by the Washington University in St. Louis Institutional Review Board.
Author Contributions
Conceptualization: AE and JC. Methodology: AE, CV, and JC. Analysis: RR and KC. Writing-original draft preparation: AE, KC, and RR. Writing-review and editing: AE, CV, RR, KC, and JC. Project administration: CV. Significantly contributed to the development of this manuscript: All authors.
Funding
This project was funded by the Robert Wood Johnson Foundation, through the Policies for Action, Children's Health Weight Hub, Grant #73758.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
This project was conducted within the Prevention Research Center in St. Louis. The authors would like to acknowledge Ms. Linda Dix, for her assistance with administration of the survey. The authors would also like to thank all childcare center personnel who took the time to fill out our survey.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2020.00102/full#supplementary-material
References
1. Institute of Medicine. Early Childhood Obesity Prevention Policies : Health and Medicine Division. (2011). Available online at: http://www.nationalacademies.org/hmd/Reports/2011/Early-Childhood-Obesity-Prevention-Policies.aspx
2. Robert Wood Johnson Foundation. Childhood Obesity Trends – The State of Obesity. (2018). Available online at: https://stateofobesity.org/childhood-obesity-trends/
3. Sahoo K, Sahoo B, Choudhury AK, Sofi NY, Kumar R, Bhadoria AS. Childhood obesity: causes and consequences. J Fam Med Prim Care. (2015) 4:187–92. doi: 10.4103/2249-4863.154628
4. Faienza MF, Wang DQ, Frühbeck G, Garruti G, Portincasa P. The dangerous link between childhood and adulthood predictors of obesity and metabolic syndrome. Int Emerg Med. (2016) 11:175–82. doi: 10.1007/s11739-015-1382-6
5. Savage JS, Fisher JO, Birch LL. Parental influence on eating behavior: conception to adolescence. J Law Med Ethics. (2007) 35:22–34. doi: 10.1111/j.1748-720X.2007.00111.x
6. Ward S, Bélanger M, Donovan D, Carrier N. Systematic review of the relationship between childcare educators' practices and preschoolers' physical activity and eating behaviours. Obes Rev. (2015) 16:1055–70. doi: 10.1111/obr.12315
7. United States Department of Health and Human Services. The NICHD Study of Early Child Care and Youth Development - Findings for Children up to Age 4 1/2 Years (2006). Available online at: https://www.nichd.nih.gov/sites/default/files/publications/pubs/documents/seccyd_06.pdf (accessed February 8, 2019).
8. Briefel RR, Wilson A, Cabili C, Hedley Dodd A. Reducing calories and added sugars by improving children's beverage choices. J Acad Nutr Diet. (2013) 113:269–75. doi: 10.1016/j.jand.2012.10.016
9. United States Department of Agriculture. Child and Adult Care Food Program (CACFP) | Food and Nutrition Service. (2018). Available online at: https://www.fns.usda.gov/cacfp/child-and-adult-care-food-program
10. United States Department of Agriculture. Final Rule: CACFP Meal Pattern Revisions Related to the Healthy, Hunger-Free Kids Act of 2010 | Food and Nutrition Service. (2017). Available online at: https://www.fns.usda.gov/cacfp/fr-042516
11. American Heart Association News. Colorado Sets New Nutrition, Physical Activity Standards for Child-Care Centers - News on Heart.Org. (2015). Available online at: https://newsarchive.heart.org/colorado-sets-new-nutrition-physical-activity-standards-for-child-care-centers/
12. Chriqui JF, Leider J, Schermbeck RM. Early childhood education centers' reported readiness to implement the updated child and adult care food program meal pattern standards in the United States, 2017. Child Obes. (2018) 14:412–20. doi: 10.1089/chi.2018.0075
13. Ritchie LD, Boyle M, Chandran K, Spector P, Whaley SE, James P, et al. Participation in the child and adult care food program is associated with more nutritious foods and beverages in child care. Child Obes. (2012) 8:224–9. doi: 10.1089/chi.2011.0061
14. United States department of Agriculture. USDA ERS - Rural-Urban Continuum Codes. (2016). Available online at: https://www.ers.usda.gov/data-products/rural-urban-continuum-codes/
15. Lee DL, Gurzo K, Yoshida S, Homel Vitale E, Hecht K, Ritchie LD. Compliance with the new 2017 child and adult care food program standards for infants and children before implementation. Child Obes. (2018) 14:393–402. doi: 10.1089/chi.2018.0092
16. Erinosho TO, Hales DP, McWilliams CP, Emunah J, Ward DS. Nutrition policies at child-care centers and impact on role modeling of healthy eating behaviors of caregivers. J Acad Nutr Diet. (2012) 112:119–24. doi: 10.1016/j.jada.2011.08.048
17. Birch LL, Parker L, Burns A. Early Childhood Obesity Prevention Policies. Early Childhood Obesity Prevention Policies. National Academies Press (2011).
18. Purtle J, Dodson E, Brownson RC. Policy dissemination research. In: Brownson RC, Colditz GA., Proctor EK, editors. Dissemination and Implementation Research in Health: Translating Science to Practice, 2nd ed. New York, NY: Oxford University Press (2018). p. 443–8.
19. Centers for Disease Control and Prevention. Adult Obesity Prevalence Maps | Overweight and Obesity. CDC (2018). Available online at: https://www.cdc.gov/obesity/data/prevalence-maps.html
20. Pan L, Freedman DS, Sharma AJ, Castellanos-Brown K, Park S, Smith RB, et al. Trends in obesity among participants aged 2–4 years in the special Supplemental Nutrition Program for women, infants, and children — United States, 2000–2014. MMWR Morbid Mortal Weekly Rep. (2016) 65:1256–60. doi: 10.15585/mmwr.mm6545a2
21. White House Taskforce on Childhood Obesity. Eat Healthy | Let's Move!”. (2015). Available online at: https://letsmove.obamawhitehouse.archives.gov/eat-healthy
22. Wang Y, Claire SN, Gortmaker SL. Increasing caloric contribution from sugar- sweetened beverages and 100% fruit juices among US children and adolescents, 1988-2004. Pediatrics. (2008) 121:e1604–14. doi: 10.1542/peds.2007-2834
23. Birch L, Savage JS, Ventura A. Influences on the development of children's eating behaviours: from infancy to adolescence. Can J Diet Pract Res. (2007) 68:s1–56. doi: 10.3148/68.2.2007.i
24. Higgs S, Thomas J. Social influences on eating. Curr Opin Behav Sci. (2016) 9:1–6. doi: 10.1016/j.cobeha.2015.10.005
25. Dev DA, Garcia AS, Dzewaltowski DA, Sisson S, Franzen-Castle L, Rida Z, et al. Provider reported implementation of nutrition-related practices in childcare centers and family childcare homes in rural and Urban Nebraska. Prev Med Rep. (2020) 17:101021. doi: 10.1016/j.pmedr.2019.101021
26. Frampton AM, Sisson SB, Horm D, Campbell JE, Lora K, Ladner JL. What's for lunch? an analysis of lunch menus in 83 urban and rural Oklahoma child-care centers providing all-day care to preschool children. J Acad Nutr Diet. (2014) 114:1367–74. doi: 10.1016/j.jand.2013.09.025
27. Anderson S, Mikesell M. Child care type, access, and quality in rural areas of the united states: a review. Early Child Dev Care. (2019) 189:1812–26. doi: 10.1080/03004430.2017.1412959
28. Liu ST, Graffagino CL, Leser KA, Trombetta AL, Pirie PL. Obesity prevention practices and policies in child care settings enrolled and not enrolled in the child and adult care food program. Matern Child Health J. (2016) 20:1933–9. doi: 10.1007/s10995-016-2007-z
29. Buscemi J, Kanwischer K, Becker AB, Ward DS, Fitzgibbon ML. Society of behavioral medicine position statement: Early Care and Education (ECE) policies can impact obesity prevention among preschool-aged children. Transl Behav Med. (2015) 5:122–5. doi: 10.1007/s13142-014-0297-5
30. Risica PM, Amin S, Ankoma A, Lawson E. The food and activity environments of childcare centers in Rhode Island: a directors' survey. BMC Nutr. (2016) 2:41. doi: 10.1186/s40795-016-0081-7
31. Lessard L, Williams Leng S, Brennan R. Consistency of compliance with nutrition-related regulations among delaware child care centers. Child Obes. (2013) 9:233–9. doi: 10.1089/chi.2012.0126
32. Fan W, Yan Z. Factors affecting response rates of the web survey: a systematic review. Comput Hum Behav. (2010) 26:132–9. doi: 10.1016/j.chb.2009.10.015
Keywords: policy, childcare, nutrition, regulations, children, obesity
Citation: Eyler AA, Valko CR, Curoe KA, Ramadas R and Chriqui JF (2020) Adherence to Updated Childcare Nutrition Regulations in Colorado, United States. Front. Public Health 8:102. doi: 10.3389/fpubh.2020.00102
Received: 29 April 2019; Accepted: 16 March 2020;
Published: 08 April 2020.
Edited by:
Paul Russell Ward, Flinders University, AustraliaReviewed by:
Georgi Iskrov, Plovdiv Medical University, BulgariaAlice Grady, University of Newcastle, Australia
Copyright © 2020 Eyler, Valko, Curoe, Ramadas and Chriqui. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Amy A. Eyler, YWV5bGVyJiN4MDAwNDA7d3VzdGwuZWR1