 Gil Boudet1
Gil Boudet1 Pierre Chausse2
Pierre Chausse2 David Thivel3,4Sylvie Rousset5
David Thivel3,4Sylvie Rousset5 Martial Mermillod4,6
Martial Mermillod4,6 Julien S. Baker7
Julien S. Baker7 Lenise M. Parreira1
Lenise M. Parreira1 Yolande Esquirol8Martine Duclos9
Yolande Esquirol8Martine Duclos9 Frédéric Dutheil10,11*
Frédéric Dutheil10,11*- 1Faculté de Médecine, Institut de Médecine du Travail, Université Clermont-Auvergne, Clermont-Ferrand, France
- 2Cellule d'Accompagnement Technologique–Department of Technological Accompaniment, CNRS, LaPSCo, Université Clermont Auvergne, Clermont-Ferrand, France
- 3Laboratory of the Metabolic Adaptations to Exercise Under Physiological and Pathological Conditions (AME2P EA 3533), Université Clermont Auvergne, Clermont-Ferrand, France
- 4Institut Universitaire de France, Paris, France
- 5Unité de Nutrition Humaine, INRA, Université Clermont Auvergne, Clermont-Ferrand, France
- 6LPNC, CNRS, Université Grenoble Alpes, Université Savoie Mont Blanc, Grenoble, France
- 7School of Science and Sport, Institute of Clinical Exercise and Health Sciences, University of the West of Scotland, Hamilton, United Kingdom
- 8Occupational and Preventive Medicine, INSERM UMR-1027, Université Paul Sabatier Toulouse 3, CHU Toulouse, Toulouse, France
- 9Sport Medicine and Functional Explorations, CRNH, INRA UMR-1019, University Hospital of Clermont-Ferrand, Université Clermont Auvergne, CHU Clermont-Ferrand, Clermont-Ferrand, France
- 10LaPSCo, Physiological and Psychosocial Stress, Preventive and Occupational Medicine, CNRS, University Hospital of Clermont-Ferrand, Université Clermont Auvergne, CHU Clermont-Ferrand, WittyFit, Clermont-Ferrand, France
- 11Faculty of Health, School of Exercise Science, Australian Catholic University, Melbourne, VIC, Australia
Background: Prolonged sedentary behavior (SB) is associated with increased risk for chronic conditions. A growing number of the workforce is employed in office setting with high occupational exposure to SB. There is a new focus in assessing, understanding and reducing SB in the workplace. There are many subjective (questionnaires) and objective methods (monitoring with wearable devices) available to determine SB. Therefore, we aimed to provide a global understanding on methods currently used for SB assessment at work.
Methods: We carried out a systematic review on methods to measure SB at work. Pubmed, Cochrane, Embase, and Web of Science were searched for peer-reviewed English-language articles published between 1st January 2000 and 17th March 2019.
Results: We included 154 articles: 89 were cross-sectional and 65 were longitudinal studies, for a total of 474,091 participants. SB was assessed by self-reported questionnaires in 91 studies, by wearables devices in also 91 studies, and simultaneously by a questionnaire and wearables devices in 30 studies. Among the 91 studies using wearable devices, 73 studies used only one device, 15 studies used several devices, and three studies used complex physiological systems. Studies exploring SB on a large sample used significantly more only questionnaires and/or one wearable device.
Conclusions: Available questionnaires are the most accessible method for studies on large population with a limited budget. For smaller groups, SB at work can be objectively measured with wearable devices (accelerometers, heart-rate monitors, pressure meters, goniometers, electromyography meters, gas-meters) and the results can be associated and compared with a subjective measure (questionnaire). The number of devices worn can increase the accuracy but make the analysis more complex and time consuming.
Introduction
Sedentary behavior (SB), has been defined as sitting or lying with low energy expenditure ≤1.5 METs (1) and is an independent risk factor for numerous adverse health outcomes. In industrialized modern societies, more and more time is spent for SB activities during normal lifestyle behavior, such as working on computers, traveling by car, and watching television during leisure time (2, 3). Further to this, more workers are now employed in low activity jobs such as administrative work. Office workers can have SB for more than 3/4 of their working day (4). Chronic disease and all-cause mortality have been linked with self-reported time spent sitting (5–13). A dose response relationship has been demonstrated between all-cause mortality and daily total sitting, with a 2% increase in all-cause mortality per hour seated per day (14). Even after adjustment on the quantity of moderate or vigorous physical activity (15, 16), the risk of death persists, demonstrating that time spent sitting is a risk factor independent of the level of physical activity. SB can be measured by declarative methods (auto-administrate questionnaires) and objective methods (observation, video, or technical instruments). Descriptive parameters of physical activity and sedentary activity used most often are duration, frequency, intensity, domain or context (leisure, work, domestic, transport), and the type of activity. Indicators combining these parameters can be calculated globally or for each one of the domains individually. The most common are the volume (time × frequency) and the energy expenditure (duration × frequency × intensity), the latter being calculated to account for overall physical activity. Time spent in front of a screen (television, video, video games, computer…) is currently the most used sedentary indicator and in the majority studies, is the time spent watching television measured by survey techniques. Considering the public health impact of SB at work, there is now a growing research interest about sedentariness at work. However, SB is measured through a wide range of methods, but no scientific articles provide a global overview on all methods used to quantify sedentary behavior.
Objective
The aim of this paper was to provide a global understanding on methods currently available for SB assessment at work.
Search Strategy
Published studies with measures of SB at work were retrieved through a systematic search of the Pubmed, Cochrane, Embase, and Web of Science databases. We selected articles published between 1st January 2000 and 27th March 2019 because SB gained momentum in recent years, with more diversity on assessing SB at work, and because only recent articles distinguished between SB and physical inactivity and their specific health effects (6, 17–19). The search strategy and keywords used are detailed in Supplementary Material Appendix 1. We restricted our search to articles in humans and written in English. We did not restrict our search to specific countries or regions, nor on a minimal sample size. Included articles had to describe tools used to measure SB at work. The search strategy is displayed in Figure 1. Three authors (GB, PC, FD) conducted all literature searches and agreed on the final decision for articles inclusion. A fourth author (MD) reviewed articles when no consensus was met. Then, eligible articles were reviewed by all authors.
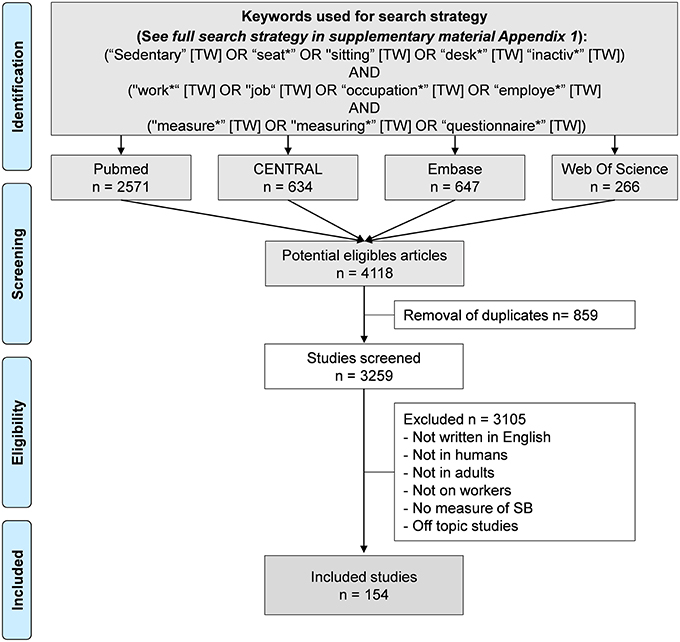
Figure 1. Search strategy.
Data Extraction and Synthesis
We extracted the following information: type of study (longitudinal, cross-sectional), category of material (questionnaire, one common sensor, multiple sensors, complex physiological system), number of subjects and the main measure of sedentariness. Identified devices which assessed sedentary behavior at work where tabulated to highlight the performance and the usability of methods and devices to access sedentary behavior at work (see Table S1 for the complete lists of included articles with those details).
Characteristics of Included Articles
An initial search retrieved a possible 4,118 articles. Removing duplicates and applying the selection criteria decreased the number of articles reporting measures of SB at work to 154 articles (Figure 1). Among the 154 included articles, 89 were cross-sectional studies, and 65 were longitudinal studies, for a total of 474 091 participants. SB was assessed by self-reported questionnaires in 91 studies, and by wearables devices in also 91 studies. Among those studies, 30 studies used simultaneously a questionnaire and wearables devices. Among the 91 studies using wearable devices, 73 studies used only one device, 15 studies used several devices, and three studies used complex physiological systems. Studies exploring SB on a large population used significantly more only questionnaires and/or one wearable device. Complete list of included articles, with details on the type of the study, number of participants, type of measures of SB, and main outcomes are presented in Table S1. Methods of measuring SB retrieved in included articles are detailed below. For practitioners and researchers who want to evaluate SB at the workplace, we propose a strategy for the best options to evaluate SB in the workplace, depending on several factors, including comfort, number of subjects, duration of measures, accuracy, and budget (Figures 2, 3 and Table 1).
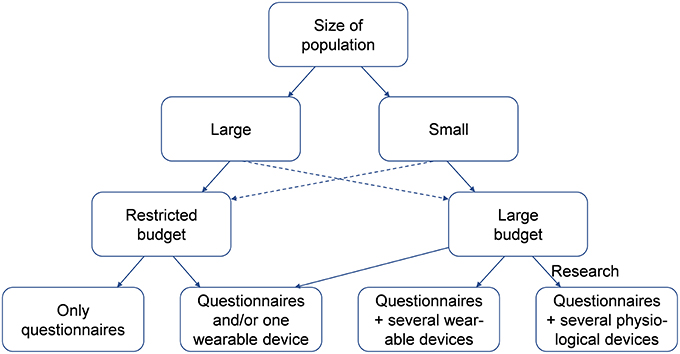
Figure 2. Decision strategy for the best option to measure sedentary behavior at work.
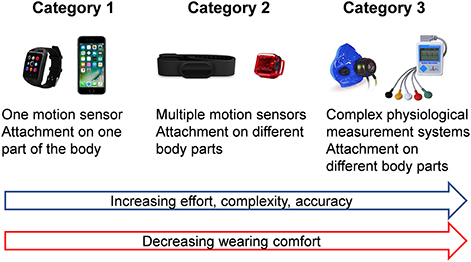
Figure 3. Categorization of wearable devices to measure sedentary behavior depending on accuracy and complexity.
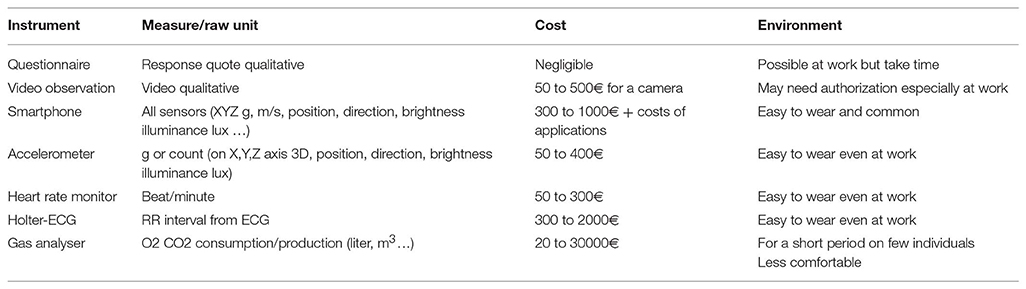
Table 1. Instrument, raw unit, cost, and environment of tools to measure sedentary behavior at work.
Methods of Measuring Sedentary Behavior
Declarative Methods-Self-Reported Questionnaires
These questionnaires are the most common method of measuring SB, relying on recall ability of participants (20). The commonly used self-report questionnaires for SB at work assessment are: The Global Physical Activity Questionnaire (GPAQ), International Physical Activity Questionnaire (IPAQ) (21, 22), Workforce Sitting Questionnaire (WSQ, Adapted from the Marshall Questionnaire), Occupational Sitting and Physical Activity Questionnaire (OSPAQ) (23) and European Physical activity Questionnaire (EPAQ) (24). Questionnaires differed on global characteristics of SB or PA (such as duration, intensity or frequency), precision of data (habitual or recent, leisure, or non-leisure activities), reporting data (such as time, calories, or scores), time of recall (such as last week or over the 12 last months), and method for conducting the survey (such as paper, computer, face-to-face) (25). Questionnaires have the advantages of their low cost and low effort, both for responders and researchers, rendering them accessible for studies in large populations. However, self-reported SB at the workplace has been demonstrated to be imprecise, biased in measurement of light or moderate physical activity, and in the assessment of energy expenditure. Severe others limitations are the dependency on written language and external factors such as age, seasonal variation, complexity of the questionnaire, and social desirability) (26–30). Characteristics and performances of questionnaires for SB assessment at work are presented in Table 2.
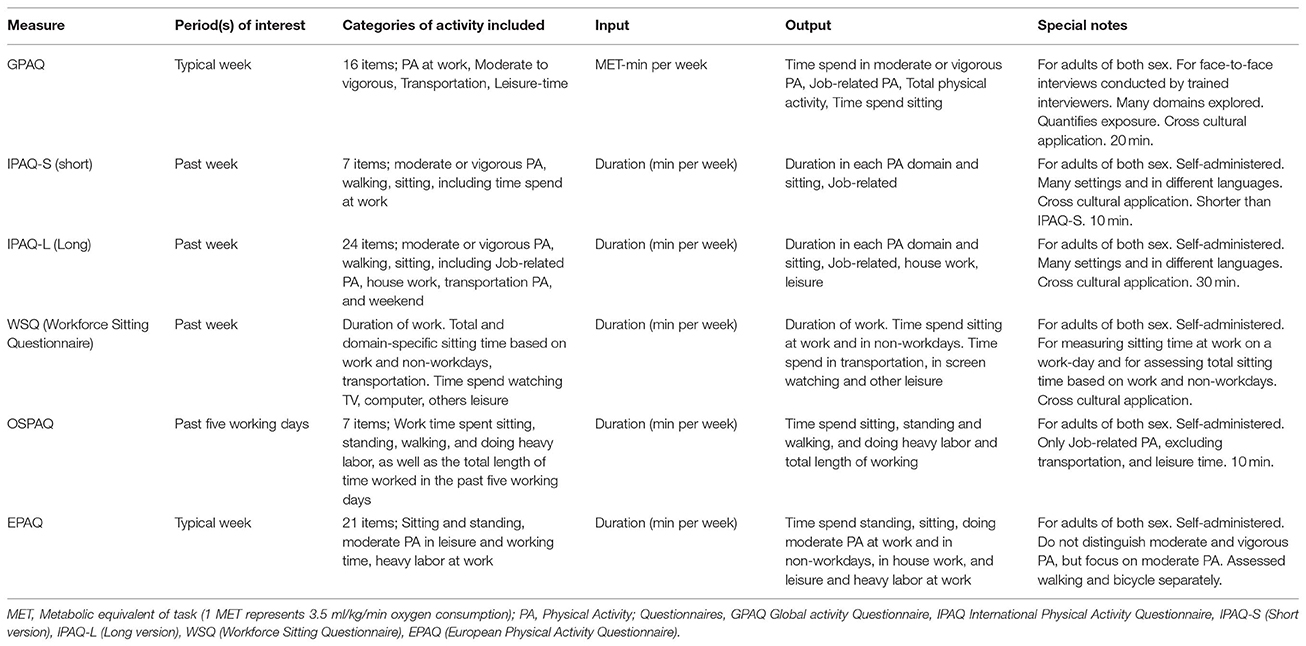
Table 2. Characteristics of self-report questionnaires to measure sedentary behavior at work.
Objective Methods
Visual Observation (Direct or Videotaped)
SB at work can also be assessed by visual observation, either recorded or on-site. Visual observation is still a classical method used by ergonomics, occupational physicians, or researchers (30). This method of assessment is often use for assessing body postures at work in delimited space (e.g., work space). Contextual information (such as location, clothing, or time) and details on SB (such as type or personal activities) could be assessed with this method. However, direct observations are costly and time consuming (31), and are therefore mostly adapted for small populations and on short periods. Visual observations are also dependent on observers who may rate differently the same behavior (32). Observed workers may also modify their behavior (observational bias) because of the logistic burden associated with data collection. Videotaped monitoring at work also needs the authorization of the employers and workers and ethical consideration.
Cardiorespiratory Assessment
Indirect Calorimetry (IC)
With IC, total energy expenditure is calculated from Weir's formula that takes into account oxygen consumption and carbon dioxide production (33). This accurate and non-invasive method can be used in routine but not in large epidemiological studies nor for measures in an ecologic environment (outside of a laboratory or a specific workplace setting). Moreover, materials needed are costly. For data collection, the workers needs to wear a facemask linked with a central unit. For ambulatory measurements, the central unit could be worn in a backpack. Thus by discriminating energy expenditure, SB is defined as seated, reclining, or lying activities requiring low levels of energy expenditure (i.e., ≤1.5 METs), light-intensity physical activity (LPA) as standing is between 1.6 and 2.9 METs and Moderate- to vigorous-intensity physical activity (MVPA) require energy expenditure ≥3.0 METs). IC can evaluate sedentary time. These analyzers are now portable like the Cosmed K5 (34) or Metamax Cortex (35). Their use over a long period can be difficult to support depending on the activity of the worker but are still feasible. Because of the relatively slight differences in energy expenditure between sitting and standing posture (36, 37), assessment of energy expenditure does not provide reliable information about the body posture. So, measurement of body posture is also required for assessment of SB at work. Conversely, most of body positions at work can be assessed by wearable devices. The use of multiple devices may also inform on anatomical location of movements.
Holter-Electrocardiography (Holter-ECG)
A linear relationship between cardiorespiratory response and energy expenditure, and thus with activity intensity has been clearly demonstrated (38). Heart rate (HR) can therefore be used to estimate energy expenditure. Coupling HR monitoring and accelerometers leads to a better accuracy in the assessment of SB and physical activity (30, 39). Historically, electrical HR sensors detect the electric impulses that are linked with the myocardial contraction. The signal allows detection of all heartbeats, and therefore of the HR. In clinical setting, the gold-standard for electrocardiographic assessment is a 12-lead ECG. In an ecologic environment (outside of hospital), a portable 3 or 5-lead Holter-ECG is commonly used for scientific research. It allows abnormal heart rhythms and cardiac symptoms detection and is considered as a medical device. Commercially wearables Holter-ECG are often based on simply a 1- or 2-lead ECG. Despite its accuracy and validity, measures with 1- or 2-lead Holter-ECG are more susceptible to artifacts because of external factors, and therefore are not consider as a medical device. Major causes are motion, physical and muscle activity, or detachment of electrodes (40, 41). To allow better diagnostic accuracy, the worker can place time markers for specific activities or events at the workplace. Data can be stored directly into a specific memory into the device or in a digital storage media (e.g., SD cards). Data are downloaded and analyzed with specific softwares by a cardiologist, a physician, or a researcher.
Heart-Rate Monitors
There are two different types of technology used by HR monitors: the electrical signal (chest belt) and optical sensor (wristwatch or armband) (42). Chest belts detect electrical signals sent through the heart each time it contracts (ECG-based detection of RR interval). Sometimes, chest belts can transmit HR data on a wristwatch providing a feedback (pulse monitoring) to the user. The Optical HR measurement is based on photoplethysmography (PPG). The Optical HR devices use integrated LED and light sensors to detect HR through rhythmic changes in blood flow occurring at each systole (blood volume pulse) (43). These sensors are cheap, discrete, and comfortable. They are mostly placed on wrists and arms, and sometimes ear lobes or fingertips. Main limitations are artifacts because of motion and a decreased sensitivity with some skin texture (44). ECG-based chest belts still offer the most reliable, consistent, and accurate way to monitor HR thanks to higher sampling rates and the position of the electrodes closer to the heart (45). However, many people prefer the comfort and convenience of optical sensors built into watches, such as Applewatch. HR monitors are able to capture energy expenditure during working activities and to categorize levels of physical activity. Moreover, they can estimate the energy expenditure even with no vertical trunk displacement that is not taking into account by most accelerometers and pedometers (46). HR monitors are less accurate to estimate energy expenditure particularly at very high and low intensities (47), because the relationship between HR and energy expenditure is not linear for high intensity of physical activity or at rest and low-intensity (with confounding factors such as body position, stress, or caffeine affecting the HR—energy expenditure relationship) (47). Others factors also affect this linear relationship or reduce its accuracy, such as age, sex, body composition and muscle mass, or fitness level (48).
Accelerometers
Accelerometers are currently used to measure and quantify the physical activity intensity category related to SB and have become the method of choice for measuring SB. Accelerometers are easy to use, accurate, and able to capture large amounts of data, particularly in large studies. These devices detect movement in real time and measure acceleration (counts) in three orthogonal planes (anteroposterior, mediolateral, and vertical) (49). The postulate is that the acceleration detected is proportional to the force produced by the muscles engaged in motion, and therefore related to energy expenditure. Time of SB is assessed by two different ways to detect body posture (standing, sitting, or lying): (1) posture by tri-axial sensors using gravitational components, or (2) spinal curvature by three uni-axial gyroscopes orthogonally aligned. Some accelerometers fail to differentiate walking intensity or body position (such as standing or sitting) (50). New accelerometers have a better validity than older models, compared to energy expenditure measured by doubly labeled water (DLW). However, accelerometers cannot provide contextual information (such as type of activity and setting) and induce a reactivity bias (51). Accuracy to determine SB depends on the threshold chosen for each count (count cut-point) (52). Most of the time, the acceleration counts characterize sedentary (absence of movement) and active behavior. The most commonly used cut-points for adult populations are <100 counts/min for SB, 100–1,951 counts/min for light-intensity physical activity (LPA), and ≥1,952 counts/min for moderate- to vigorous-intensity physical activity (MVPA) for the ActiGraph accelerometer (53, 54). However, these cut-points were developed in specific populations and during strict, laboratory-based protocols. Other studies validating the ActiGraph have found vastly different cut-points for SB (range 50–250 counts/min) and MVPA (191–2,691 counts/min) in adults, depending on the population and type of validation setting (55, 56). The cut-point method has several limitations; it cannot differentiate standing from sitting/lying, but standing is considered LPA because it elicits different physiologic responses and has different long-term health consequences than sitting/lying (57, 58). Thus, the interpretation of what is considered to be active behavior is consequently different and makes the comparison between the studies difficult. Obese people spend more time in SB than normal weight individuals (59, 60). Thus, cut-points have to be more accurate to show difference among and between normal-weight and obese populations. Accelerometers worn on the right thigh achieve high accuracy for classification of three distinct physical activity intensity categories (SB, LPA, and MVPA) as well as breaks in SB in a semi-structured setting. Wrist accelerometers also have high accuracy for assessment of SB but have some misclassifications of LPA and MVPA, with interestingly better accuracy when they are worn on the left wrist compared to the right wrist (or hip). These findings support the use of accelerometers worn at the thigh to assess the time spent in SB and different categories of physical activity intensity. Alternately, for researchers using wrist-worn accelerometers to assess physical activity, wear on the non-dominant wrist is likely to allow for higher measurement accuracy than wear on the dominant wrist (61). Due to limitations of the cut-point approach to measure categories of physical activity intensity, researchers have utilized modelization technics to improve accuracy of physical activity measurement from accelerometers worn on various body locations (62, 63). An accelerometer does not give the position information of the subject. It will be completed by a gyroscope (measuring orientation and angular velocity) (Samsung Gear S3) and a magnetometer (detecting Erath's magnetic three perpendicular axes X, Y, Z) (Actigraph GT9X) (64). The ActivPal is an alternative tri-axial accelerometer thigh-worn. The thigh position allows the determination of step counts, stepping speed, and start-end of each period spent sitting, lying, standing, or stepping, as well as breaks in SB and postural transitions. The ActivPAL is a monobloc system that is discrete, easily used by individuals, without calibration, and reliable for the measurement of SB (65, 66). Therefore, ActivPAL is increasingly used in ecological environment outside laboratories.
Global Positioning System (GPS)
Global Positioning System (GPS) can complete this variety of sensors by giving the geographical position (latitude and longitude) and time of each geographical position, but mainly outside building. Newer GPS can also deliver information such as speed (retrieved from time between different geographical positions), elevation, and indoor/outdoor activities. However, most workers spend a high proportion of their time indoors, and unfortunately GPS are only able to receive indoor signal from small buildings with a wooden roof or high buildings with large windows. GPS are unable to determine room-level of indoor location (67). However, even if GPS is mostly for outdoor activities, newest GPS can also track SB indoors. Moreover, some devices also include useful tools such as a brightness sensor to access sleep quality. These wearable lightweight GPS devices are easily forgotten by users. The researcher should take care to check the sampling frequency, resolution, and the maximum amplitude of the device. In order to make long observations, it is also necessary to check the device battery and storage space. Recent smart-phones or smartwatches are equipped with all the mentioned sensors.
Smartwatches and Smartphones
Smartwatches are wrist-worn computerized devices with extensive communication capabilities. They are linked to one mobile operating system. In perpetual development, manufacturers continue to implement new features, such as GPS, fitness/health tracking, or waterproof frames (16). The gestures of the hands, such as smoking, are now accessible thanks to the addition of reliable and sensitive inertial sensors (17). In a recent meta-analysis (68) the most popular smartwatches (connected devices) on the market were compared: from Apple, Fitbit, Garmin, Lumo, Misfit, Samsung Gear, and TomTom. Generally, smartwatches tend to underestimate energy expenditure compared to laboratory reference measurements (Oxycon Mobile, CosMed K4b2, or MetaMax 3B). Moreover, while smartwatches get better to estimate energy expenditure with an increased intensity, validity becomes poorer with low intensity, and sedentary measures. Because everyone has a smartphone, they are an alternative to smartwatches or other wearable devices. Now, all smartphones combine many sensors, such as GPS or Global Navigation Satellite System (GLONASS), accelerometer, e-compass, gyroscope, proximity sensor, or ambient light sensor. Conveniently, smartphones can be linked with an HR belt, a smartwatch, or even a gas analyzer. However, all wrist and forearm devices have a tendency for underestimating HR, especially for exercises at high intensity and with amplitude of arm movement (such as exercising on a treadmill or an elliptical machine)—and conversely, measures of HR are more accurate at rest or for exercise without movement of arms (such as on a cycle ergometer). While HR is underestimated for high intensity of physical activity, step count on the opposite is underestimated for slower walking speeds and in free-living conditions. Smartphones are also particularly attractive for context awareness and phone-based personal information (69). The recognition of some activities are dependent on position-attachment of the phone on the body (70). For example, to recognize a specific activity, the smartphone should be placed on the major members involved within the activity. Unfortunately, a smartphone placed onto the body can also be non-compatible with some activities in an ecological environment (free-living conditions). Algorithm used for long recording periods can quickly consume the battery power, and may need a power supply. Another point consists of choosing the accurate available application.
Mobile Applications
Smartphone applications experienced a boom in medical science. In 2016, the Play Store displayed 105,000 and the Apple Store 126,000 health or fitness-related apps (71). These applications propose physical exercises and fitness programs with or without connected objects such as wristband, pedometer, scale, HR monitor, smartphone, and smartwatch. When the mobile applications integrate the use of sensors (accelerometer, HR monitor, GPS), they inform the user of steps, distance, energy expenditure, speed, and heart frequency. The three most popular applications are Fitbit, Noom, and AppleHealth (Table 3). These special features are welcomed by the users. Conversely, most of the applications are not scientifically validated.
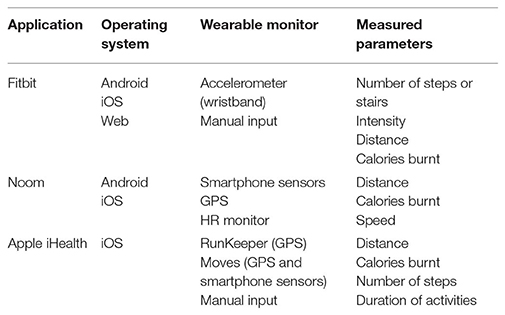
Table 3. Characteristics and physical activity parameters evaluated by the three most downloaded mobile applications.
WellBeNet (eMouve) and IntellilifePro were two applications recently scientifically validated to assess accurately time spent in SB, LPA, MVPA, and the total energy expenditure associated. These two applications were specially developed to discriminate SB from LPA, such as standing or slow walking. Accelerometry data are collected via smartphones [WellBeNet (eMouve)] or via both a smartphone and smartwatch (IntellilifePro).
E-Move
E-move (Android) application detects leg movements as the smartphone is worn in a front pants pocket. Different algorithms were designed for normal and overweight/obese adults. The total energy expenditure and time spent for each category of physical activity given by the E-Mouve algorithms were compared with reference method or device: either Armband or indirect calorimetry (FitmatePro, Cosmed). Absolute error of the total energy expenditure and activity estimates are 5.6 and 5.0%, respectively in normal weight volunteers, and 8.6 and 5.0% in overweight/obese participants (72, 73).
IntellilifePro
IntellifePro is based on the simultaneous use of a smartphone and a smartwatch (Android or Apple) to detect both leg and wrist movements. IntellifePro can discriminate passive from active sitting when in a sitting posture, while the arm, the wrist and/or the hand are engaged in the movement. Absolute error of the total energy expenditure and activity estimates are 3.1, 2.8, 1.5, and 0.04%, for SB, light, moderate, and vigorous intensity, respectively. The absolute error for total energy expenditure was lower than 5% in free living conditions (74).
Pressure Sensors
Another alternative to assess SB is via pressure sensors. Sensors can be placed in a sock, a shoe, or a chair. In a sock or shoe, a high pressure measured by the sensor is related to standing, and a low pressure is related to sitting or lying. On a chair, pressure sensors (sitting pad) are generally binary: active when the user is sitting, and inactive when nobody is sitting on the sensor (75). Current technologies and attachment on the body are presented in Figure 4.
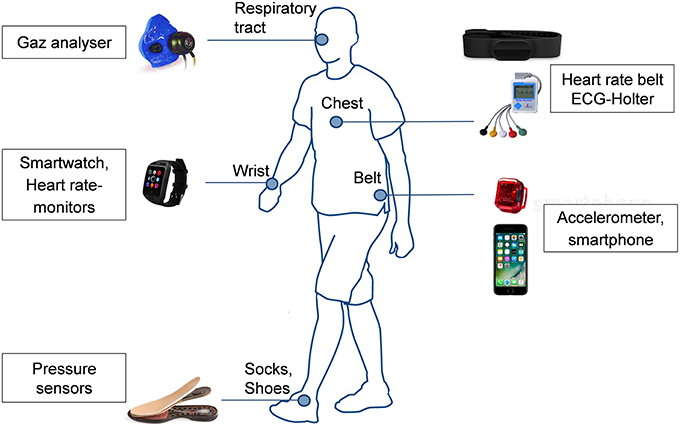
Figure 4. Current technologies to measure sedentary behavior and attachment on the body.
Characteristics of Sedentary Behavior
Total daily duration of SB is commonly used to study the effects on health of SB. However, characteristics of SB are of major importance on health. Particularly, continuous prolonged SB may be more deleterious on health outcomes than shorter bouts of SB but with the same duration (76, 77). The need for a definition of a sedentariness has also been proposed (78). Investigations of SB at work should not only assess total daily duration of SB, but also the patterns and durations of SB and non-SB periods. The context of SB is also important (what, where, why, when, and with whom).
Limitations
Smart clothing (such as shirts with sensors measuring HR, socks or shoes combining pressure and accelerometers, or helmets and caps with a camera and GPS), goniometers (measuring an angle and angular position), electromyography meters (measuring the electrical activities of muscles EMG), and wearable camera have been voluntary excluded of the presented devices because still in development and not yet used to assess SB at work.
Conclusion
We proposed a systematic review on tools available to measure SB at work. SB was mainly assessed by self-reported questionnaires or by only one wearable device. Studies using several devices were less common, and rarely studies used complex physiological systems. The wide range of wearable devices offer a variety of methods to evaluate SB at work. It is not an easy task to select the optimal device and the right measurement strategy for a particular study purpose. The main factors of work (inside or outside, working movements, and postures) and study population (i.e., number, age, gender, body mass index, and comorbidities) may also affect the choice. To assess SB at work, four determinants factors should be considered to choose the appropriate method: (1) quality of measure (e.g., time spent on SB or energy expenditure), (2) objectivity of the data and burden of workers (e.g., time/effort for measures), (3) cost/burden for the researcher, and (4) specific limitations due to environment and working activities. Available questionnaires are the most accessible method for a large population with a limited budget. SB at work (time sitting) is accessible from some specific items. It is also possible to deduct SB in measuring PA at work that is easily measurable. Assessments of SB need both measures of energy expenditure and of body posture (dual or multiple wearable devices with sensors). Accurate measure of SB at work need a sufficient number of subjects affected to the same assigned task and an objective measure coupled to a questionnaire (mixed approach method). For a restrictive group, SB at work can be objectively measured with wearable devices (accelerometers, heart-rate monitors, pressure meters, goniometers, electromyography meters, gas-meters) and can be associated with subjective measures (questionnaires). The number of devices worn increase the accuracy but make the analysis complex and time consuming. Furthers studies are necessary to improve the relative strengths and weakness of subjective or objective methods to assess SB at work.
Author Contributions
FD conceived the article. GB, PC, DT, MD, and FD contributed to drafting the article. All authors performed critical revision of the article.
Conflict of Interest Statement
FD established a public private partnership between the University Hospital of Clermont-Ferrand and WittyFit. However, he is not a member of the company and he is not paid by the company. The public private partnership only involves that he is the scientific leader, he owns all WittyFit data and can use it for research purposes. Therefore, as there is no money involved, the authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
This work was supported by Université Clermont Auvergne, Institute of Occupational Medicine, by the Physiological and Psychosocial Stress team from the Laboratory of Social and Cognitive Psychology (LaPSCo, CNRS), by the laboratory of the Metabolic Adaptations to Exercise under Physiological and Pathological conditions (AME2P EA 3533), and by INRA, UNH, Unité de Nutrition Humaine (UNH, INRA).
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2019.00167/full#supplementary-material
References
1. Sedentary Behaviour Research Network. Letter to the editor: standardized use of the terms “sedentary” and “sedentary behaviours”. Appl Physiol Nutri Metab. (2012) 37:540–2. doi: 10.1139/h2012-024
2. Chau JY, Bonfiglioli C, Zhong A, Pedisic Z, Daley M, McGill B, Bauman A. Sitting ducks face chronic disease: an analysis of newspaper coverage of sedentary behaviour as a health issue in Australia 2000-2012. Health Promot J Aust. (2017) 28:139–43. doi: 10.1071/HE16054
3. Church TS, Thomas DM, Tudor-Locke C, Katzmarzyk PT, Earnest CP, Rodarte RQ, et al. Trends over 5 decades in U.S. occupation-related physical activity and their associations with obesity. PLoS ONE. (2011) 6:e19657. doi: 10.1371/journal.pone.0019657
4. Thorp AA, Healy GN, Winkler E, Clark BK, Gardiner PA, Owen N, et al. Prolonged sedentary time and physical activity in workplace and non-work contexts: a cross-sectional study of office, customer service and call centre employees. Int J Behav Nutr Phys Act. (2012) 9:128. doi: 10.1186/1479-5868-9-128
5. Hu FB, Leitzmann MF, Stampfer MJ, Colditz GA, Willett WC, Rimm EB. Physical activity and television watching in relation to risk for type 2 diabetes mellitus in men. Arch Int Med. (2001) 161:1542–8. doi: 10.1001/archinte.161.12.1542
6. Dunstan DW, Barr EL, Healy GN, Salmon J, Shaw JE, Balkau B, et al. Television viewing time and mortality: the Australian Diabetes, Obesity and Lifestyle Study (AusDiab). Circulation. (2010) 121:384–91. doi: 10.1161/CIRCULATIONAHA.109.894824
7. Ford ES, Li C, Zhao G, Pearson WS, Tsai J, Churilla JR. Sedentary behavior, physical activity, and concentrations of insulin among US adults. Metabolism. (2010) 59:1268–75. doi: 10.1016/j.metabol.2009.11.020
8. Katzmarzyk PT, Church TS, Craig CL, Bouchard C. Sitting time and mortality from all causes, cardiovascular disease, and cancer. Med Sci Sports Exerc. (2009) 41:998–1005. doi: 10.1249/MSS.0b013e3181930355
9. Patel AV, Bernstein L, Deka A, Feigelson HS, Campbell PT, Gapstur SM, et al. Leisure time spent sitting in relation to total mortality in a prospective cohort of US adults. Am J Epidemiol. (2010) 172:419–29. doi: 10.1093/aje/kwq155
10. Schmid D, Ricci C, Leitzmann MF. Associations of objectively assessed physical activity and sedentary time with all-cause mortality in US adults: the NHANES study. PLoS ONE. (2015) 10:e0119591. doi: 10.1371/journal.pone.0119591
11. Stamatakis E, Hamer M, Dunstan DW. Screen-based entertainment time, all-cause mortality, and cardiovascular events: population-based study with ongoing mortality and hospital events follow-up. J Am Coll Cardiol. (2011) 57:292–9. doi: 10.1016/j.jacc.2010.05.065
12. Warren TY, Barry V, Hooker SP, Sui X, Church TS, Blair SN. Sedentary behaviors increase risk of cardiovascular disease mortality in men. Med Sci Sports Exerc. (2010) 42:879–85. doi: 10.1249/MSS.0b013e3181c3aa7e
13. Wijndaele K, Brage S, Besson H, Khaw KT, Sharp SJ, Luben R, et al. Television viewing time independently predicts all-cause and cardiovascular mortality: the EPIC Norfolk study. Int J Epidemiol. (2011) 40:150–9. doi: 10.1093/ije/dyq105
14. Chau JY, Grunseit AC, Chey T, Stamatakis E, Brown WJ, Matthews CE, et al. Daily sitting time and all-cause mortality: a meta-analysis. PLoS ONE. (2013) 8:e80000. doi: 10.1371/journal.pone.0080000
15. Honda T, Chen S, Kishimoto H, Narazaki K, Kumagai S. Identifying associations between sedentary time and cardio-metabolic risk factors in working adults using objective and subjective measures: a cross-sectional analysis. BMC Public Health. (2014) 14:1307. doi: 10.1186/1471-2458-14-1307
16. Thorp AA, Owen N, Neuhaus M, Dunstan DW. Sedentary behaviors and subsequent health outcomes in adults a systematic review of longitudinal studies, 1996-2011. Am J Prevent Med. (2011) 41:207–15. doi: 10.1016/j.amepre.2011.05.004
17. Yates T, Wilmot EG, Davies MJ, Gorely T, Edwardson C, Biddle S, et al. Sedentary behavior: what's in a definition? Am. J. Prev. Med. (2011) 40:e33–4; author reply e34. doi: 10.1016/j.amepre.2011.02.017
18. Hamilton MT, Hamilton DG, Zderic TW. Role of low energy expenditure and sitting in obesity, metabolic syndrome, type 2 diabetes, and cardiovascular disease. Diabetes. (2007) 56:2655–67. doi: 10.2337/db07-0882
19. Bertrais S, Beyeme-Ondoua JP, Czernichow S, Galan P, Hercberg S, Oppert JM. Sedentary behaviors, physical activity, and metabolic syndrome in middle-aged French subjects. Obes Res. (2005) 13:936–44. doi: 10.1038/oby.2005.108
20. Castillo-Retamal M, Hinckson EA. Measuring physical activity and sedentary behaviour at work: a review. Work. (2011) 40:345–57. doi: 10.3233/WOR-2011-1246
21. Hagstromer M, Oja P, Sjostrom M. The International Physical Activity Questionnaire (IPAQ): a study of concurrent and construct validity. Public Health Nutri. (2006) 9:755–62. doi: 10.1079/PHN2005898
22. Craig CL, Marshall AL, Sjostrom M, Bauman AE, Booth ML, Ainsworth BE, et al. International physical activity questionnaire: 12-country reliability and validity. Med Sci Sports Exerc. (2003) 35:1381–95. doi: 10.1249/01.MSS.0000078924.61453.FB
23. Chau JY, Van Der Ploeg HP, Dunn S, Kurko J, Bauman AE. Validity of the occupational sitting and physical activity questionnaire. Med Sci Sports Exerc. (2012) 44:118–25. doi: 10.1249/MSS.0b013e3182251060
24. Prince SA, LeBlanc AG, Colley RC, Saunders TJ. Measurement of sedentary behaviour in population health surveys: a review and recommendations. PeerJ. (2017) 5:e4130. doi: 10.7717/peerj.4130
25. Jacobs DR Jr, Ainsworth BE, Hartman TJ, Leon AS. A simultaneous evaluation of 10 commonly used physical activity questionnaires. Med Sci Sports Exerc. (1993) 25:81–91. doi: 10.1249/00005768-199301000-00012
26. Gupta N, Heiden M, Mathiassen SE, Holtermann A. Prediction of objectively measured physical activity and sedentariness among blue-collar workers using survey questionnaires. Scand J Work Environ Health. (2016) 42:237–45. doi: 10.5271/sjweh.3561
27. Koch M, Lunde LK, Gjulem T, Knardahl S, Veiersted KB. Validity of questionnaire and representativeness of objective methods for measurements of mechanical exposures in construction and health care work. PLoS ONE. (2016) 11:e0162881. doi: 10.1371/journal.pone.0162881
28. Kwak L, Proper KI, Hagstromer M, Sjostrom M. The repeatability and validity of questionnaires assessing occupational physical activity–a systematic review. Scand J Work Environ Health. (2011) 37:6–29. doi: 10.5271/sjweh.3085
29. Lagersted-Olsen J, Korshoj M, Skotte J, Carneiro IG, Sogaard K, Holtermann A. Comparison of objectively measured and self-reported time spent sitting. Int J Sports Med. (2014) 35:534–40. doi: 10.1055/s-0033-1358467
30. Holtermann A, Schellewald V, Mathiassen SE, Gupta N, Pinder A, Punakallio A, et al. A practical guidance for assessments of sedentary behavior at work: a PEROSH initiative. Appl Ergon. (2017) 63:41–52. doi: 10.1016/j.apergo.2017.03.012
31. Trask C, Mathiassen SE, Rostami M, Heiden M. Observer variability in posture assessment from video recordings: the effect of partly visible periods. Appl Ergon. (2017) 60:275–81. doi: 10.1016/j.apergo.2016.12.009
32. Rezagholi M, Mathiassen SE, Liv P. Cost efficiency comparison of four video-based techniques for assessing upper arm postures. Ergonomics. (2012) 55:350–60. doi: 10.1080/00140139.2011.642007
33. Weir JB. New methods for calculating metabolic rate with special reference to protein metabolism. J Physiol. (1949) 109:1–9. doi: 10.1113/jphysiol.1949.sp004363
34. Gao S, Zhai Y, Yang L, Zhang H, Gao Y. Preferred temperature with standing and treadmill workstations. Build Environ. (2018) 138:63–73. doi: 10.1016/j.buildenv.2018.04.027
35. Vogler AJ, Rice AJ, Gore CJ. Validity and reliability of the Cortex MetaMax3B portable metabolic system. J Sports Sci. (2010) 28:733–42. doi: 10.1080/02640410903582776
36. Fountaine CJ, Johann J, Skalko C, Liguori GA. Metabolic and energy cost of sitting, standing, and a novel sitting/stepping protocol in recreationally active college students. Int J Exerc Sci. (2016) 9:223–9.
37. Gibbs BB, Kowalsky RJ, Perdomo SJ, Grier M, Jakicic JM. Energy expenditure of deskwork when sitting, standing or alternating positions. Occup Med. (2017) 67:121–7. doi: 10.1093/occmed/kqw115
38. Strath SJ, Kaminsky LA, Ainsworth BE, Ekelund U, Freedson PS, Gary RA, et al. Guide to the assessment of physical activity: clinical and research applications: a scientific statement from the American Heart Association. Circulation. (2013) 128:2259–79. doi: 10.1161/01.cir.0000435708.67487.da
39. Altini M, Casale P, Penders JF, Amft O. Personalization of energy expenditure estimation in free living using topic models. IEEE J Biomed Health Inform. (2015) 19:1577–86. doi: 10.1109/JBHI.2015.2418256
40. Chase C, Brady WJ. Artifactual electrocardiographic change mimicking clinical abnormality on the ECG. Am J Emerg Med. (2000) 18:312–6. doi: 10.1016/S0735-6757(00)90126-8
41. Boudet G, Chamoux A. Heart rate monitors and abnormal heart rhythm detection. Arch Physiol Biochem. (2000) 108:371–9. doi: 10.1076/apab.108.4.371.4304
42. Shelley KH. Photoplethysmography: beyond the calculation of arterial oxygen saturation and heart rate. Anesthesia Analg. (2007) 105:S31–6. doi: 10.1213/01.ane.0000269512.82836.c9
43. Allen J. Photoplethysmography and its application in clinical physiological measurement. Physiol Meas. (2007) 28:R1–39. doi: 10.1088/0967-3334/28/3/R01
44. Couceiro R, Carvalho P, Paiva RP, Henriques J, Muehlsteff J. Detection of motion artifact patterns in photoplethysmographic signals based on time and period domain analysis. Physiol Meas. (2014) 35:2369–88. doi: 10.1088/0967-3334/35/12/2369
45. Tarniceriu A, Parak J, Renevey P, Nurmi M, Bertschi M, Delgado-Gonzalo R, et al. Towards 24/7 continuous heart rate monitoring. Conf Proc IEEE Eng Med Biol Soc. (2016) 2016:186–9. doi: 10.1109/EMBC.2016.7590671
46. Crouter SE, Albright C, Bassett DR Jr. Accuracy of polar S410 heart rate monitor to estimate energy cost of exercise. Med Sci Sports Exerc. (2004) 36:1433–9. doi: 10.1249/01.MSS.0000135794.01507.48
47. Livingstone MB. Heart-rate monitoring: the answer for assessing energy expenditure and physical activity in population studies? Br J Nutri. (1997) 78:869–71. doi: 10.1079/BJN19970205
48. Keytel LR, Goedecke JH, Noakes TD, Hiiloskorpi H, Laukkanen R, van der Merwe L, et al. Prediction of energy expenditure from heart rate monitoring during submaximal exercise. J Sports Sci. (2005) 23:289–97. doi: 10.1080/02640410470001730089
49. Chen KY, Bassett DR Jr. The technology of accelerometry-based activity monitors: current and future. Med Sci Sports Exerc. (2005) 37:S490–500. doi: 10.1249/01.mss.0000185571.49104.82
50. Hardy LL, Hills AP, Timperio A, Cliff D, Lubans D, Morgan PJ, et al. A hitchhiker's guide to assessing sedentary behaviour among young people: deciding what method to use. J Sci Med Sport. (2013) 16:28–35. doi: 10.1016/j.jsams.2012.05.010
51. Rachele JN, McPhail SM, Washington TL, Cuddihy TF. Practical physical activity measurement in youth: a review of contemporary approaches. World J Pediatr. (2012) 8:207–16. doi: 10.1007/s12519-012-0359-z
52. Loprinzi PD, Lee H, Cardinal BJ, Crespo CJ, Andersen RE, Smit E. The relationship of actigraph accelerometer cut-points for estimating physical activity with selected health outcomes: results from NHANES 2003-06. Res Quart Exerc Sport. (2012) 83:422–30. doi: 10.5641/027013612802573085
53. Treuth MS, Schmitz K, Catellier DJ, McMurray RG, Murray DM, Almeida MJ, et al. Defining accelerometer thresholds for activity intensities in adolescent girls. Med Sci Sports Exerc. (2004) 36:1259–66.
54. Healy GN, Clark BK, Winkler EA, Gardiner PA, Brown WJ, Matthews CE. Measurement of adults' sedentary time in population-based studies. Am J Prevent Med. (2011) 41:216–27. doi: 10.1016/j.amepre.2011.05.005
55. Kozey-Keadle S, Libertine A, Lyden K, Staudenmayer J, Freedson PS. Validation of wearable monitors for assessing sedentary behavior. Med Sci Sports Exerc. (2011) 43:1561–7. doi: 10.1249/MSS.0b013e31820ce174
56. Swartz AM, Strath SJ, Bassett DR Jr, O'Brien WL, King GA, Ainsworth BE. Estimation of energy expenditure using CSA accelerometers at hip and wrist sites. Med Sci Sports Exerc. (2000) 32:S450–6. doi: 10.1097/00005768-200009001-00003
57. Bey L, Hamilton MT. Suppression of skeletal muscle lipoprotein lipase activity during physical inactivity: a molecular reason to maintain daily low-intensity activity. J Physiol. (2003) 551:673–82. doi: 10.1113/jphysiol.2003.045591
58. Katzmarzyk PT. Standing and mortality in a prospective cohort of Canadian adults. Med Sci Sports Exerc. (2014) 46:940–6. doi: 10.1249/MSS.0000000000000198
59. Koolhaas CM, van Rooij FJ, Cepeda M, Tiemeier H, Franco OH, Schoufour JD. Physical activity derived from questionnaires and wrist-worn accelerometers: comparability and the role of demographic, lifestyle, and health factors among a population-based sample of older adults. Clin Epidemiol. (2018) 10:1–16. doi: 10.2147/CLEP.S147613
60. Maillard F, Rousset S, Bruno P, Boirie Y, Duclos M, Boisseau N. High-intensity interval training is more effective than moderate-intensity continuous training in reducing abdominal fat mass in postmenopausal women with type 2 diabetes: a randomized crossover study. Diabetes Metab. (2018) 44:516–7. doi: 10.1016/j.diabet.2018.09.001
61. Montoye HK, Pivarnik JM, Mudd LM, Biswas S, Pfeiffer KA. Validation and comparison of accelerometers worn on the hip, thigh, and wrists for measuring physical activity and sedentary behavior. AIMS Public Health. (2016) 3:298–312. doi: 10.3934/publichealth.2016.2.298
62. Montoye AH, Mudd LM, Biswas S, Pfeiffer KA. Energy expenditure prediction using raw accelerometer data in simulated free living. Med Sci Sports Exerc. (2015) 47:1735–46. doi: 10.1249/MSS.0000000000000597
63. Preece SJ, Goulermas JY, Kenney LP, Howard D, Meijer K, Crompton R. Activity identification using body-mounted sensors–a review of classification techniques. Physiol Meas. (2009) 30:R1–33. doi: 10.1088/0967-3334/30/4/R01
64. Donaldson SC, Montoye AH, Tuttle MS, Kaminsky LA. Variability of objectively measured sedentary behavior. Med Sci Sports Exerc. (2016) 48:755–61. doi: 10.1249/MSS.0000000000000828
65. Grant PM, Ryan CG, Tigbe WW, Granat MH. The validation of a novel activity monitor in the measurement of posture and motion during everyday activities. Br J Sports Med. (2006) 40:992–7. doi: 10.1136/bjsm.2006.030262
66. Godfrey A, Culhane KM, Lyons GM. Comparison of the performance of the activPAL Professional physical activity logger to a discrete accelerometer-based activity monitor. Med Eng Phys. (2007) 29:930–4. doi: 10.1016/j.medengphy.2006.10.001
67. Jankowska MM, Schipperijn J, Kerr J. A framework for using GPS data in physical activity and sedentary behavior studies. Exerc Sport Sci Rev. (2015) 43:48–56. doi: 10.1249/JES.0000000000000035
68. Bunn JA, Navalta JW, Fountaine CJ, Reece JD. Current state of commercial wearable technology in physical activity monitoring 2015-2017. Int J Exerc Sci. (2018) 11:503–15.
69. Galeana-Zapien H, Torres-Huitzil C, Rubio-Loyola J. Mobile phone middleware architecture for energy and context awareness in location-based services. Sensors. (2014) 14:23673–96. doi: 10.3390/s141223673
70. Yurtman A, Barshan B. Activity recognition invariant to sensor orientation with wearable motion sensors. Sensors. (2017) 17:1838. doi: 10.3390/s17081838
71. Dallinga J, Janssen M, van der Werf J, Walravens R, Vos S, Deutekom M. Analysis of the features important for the effectiveness of physical activity-related apps for recreational sports: expert panel approach. JMIR mHealth uHealth. (2018) 6:e143. doi: 10.2196/mhealth.9459
72. Rousset S, Guidoux R, Paris L, Farigon N, Miolanne M, Lahaye C, et al. A novel smartphone accelerometer application for low-intensity activity and energy expenditure estimations in overweight and obese adults. J Med Syst. (2017) 41:117. doi: 10.1007/s10916-017-0763-y
73. Guidoux R, Duclos M, Fleury G, Lacomme P, Lamaudiere N, Manenq PH, et al. A smartphone-driven methodology for estimating physical activities and energy expenditure in free living conditions. J Biomed Inform. (2014) 52:271–8. doi: 10.1016/j.jbi.2014.07.009
74. Duclos M, Fleury G, Lacomme P, Phan R, Ren L, Rousset S. An acceleration vector variance based method for energy expenditure estimation in real-life environment with a smartphone/smartwatch integration. Expert Syst Appl. (2016) 63:435–49. doi: 10.1016/j.eswa.2016.07.021
75. Ma C, Li W, Gravina R, Cao J, Li Q, Fortino G. Activity level assessment using a smart cushion for people with a sedentary lifestyle. Sensors. (2017) 17:E2269. doi: 10.3390/s17102269
76. Carson V, Wong SL, Winkler E, Healy GN, Colley RC, Tremblay MS. Patterns of sedentary time and cardiometabolic risk among Canadian adults. Prev Med. (2014) 65:23–7. doi: 10.1016/j.ypmed.2014.04.005
77. Gupta N, Hallman DM, Mathiassen SE, Aadahl M, Jorgensen MB, Holtermann A. Are temporal patterns of sitting associated with obesity among blue-collar workers? A cross sectional study using accelerometers. BMC Public Health. (2016) 16:148. doi: 10.1186/s12889-016-2803-9
Keywords: occupational health, sedentary lifestyle, workplace, sedentary behavior measurement, work, questionnaires, wearable devices, recommendations
Citation: Boudet G, Chausse P, Thivel D, Rousset S, Mermillod M, Baker JS, Parreira LM, Esquirol Y, Duclos M and Dutheil F (2019) How to Measure Sedentary Behavior at Work? Front. Public Health 7:167. doi: 10.3389/fpubh.2019.00167
Received: 16 October 2018; Accepted: 05 June 2019;
Published: 05 July 2019.
Edited by:
Daniel P. Bailey, University of Bedfordshire Bedford, United KingdomReviewed by:
Anselm Ting Su, Universiti Malaysia Sarawak, MalaysiaJean-Frédéric Brun, Inserm U1046 Physiologie Et Médecine Expérimentale Du Coeur Et Des Muscles, France
Copyright © 2019 Boudet, Chausse, Thivel, Rousset, Mermillod, Baker, Parreira, Esquirol, Duclos and Dutheil. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Frédéric Dutheil, ZnJlZGVyaWMuZHV0aGVpbEB1Y2EuZnI=