
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health, 24 April 2019
Sec. Epidemiology
Volume 7 - 2019 | https://doi.org/10.3389/fpubh.2019.00096
 Nina Wawro1,2,3,4*
Nina Wawro1,2,3,4* Ute Amann1,3
Ute Amann1,3 Julia Butt5
Julia Butt5 Christa Meisinger1,3Manas K. Akmatov6,7
Christa Meisinger1,3Manas K. Akmatov6,7 Frank Pessler6,7Annette Peters1,2Wolfgang Rathmann8Stefan Kääb9Tim Waterboer5Jakob Linseisen1,3,4
Frank Pessler6,7Annette Peters1,2Wolfgang Rathmann8Stefan Kääb9Tim Waterboer5Jakob Linseisen1,3,4Introduction: Helicobacter pylori (H. pylori) is a common infection and known risk factor for gastric cancer. We assessed cross-sectional and longitudinal associations to study the impact of H. pylori seropositivity on metabolic diseases.
Methods: Helicobacter pylori seropositivity in serum samples of the KORA study was analyzed by multiplex serology. We calculated sex-specific prevalence of H. pylori seropositivity for the year 2007 based on the first follow-up survey (termed F4) of the KORA study S4. We identified factors associated with H. pylori seropositivity in the F4 survey. Further, we assessed relative risks of incident metabolic diseases/risk factors at the time of the second follow-up survey of S4 (termed FF4) and H. pylori seropositivity at the F4 survey as a determinant. Models were adjusted for age, sex, overweight status, physical activity, smoking status, education level, alcohol intake, and other metabolic diseases.
Results: Based on 3,037 persons aged 32 to 82 years, the H. pylori prevalence for 2007 was 30.2% in men (n = 1,465) and 28.1% in women (n = 1,572). Increasing age, current smoking, low education and no alcohol intake were significantly associated with H. pylori seropositivity in the F4 survey. However, no association between H. pylori seropositivity and BMI, metabolic diseases (type 2 diabetes, hypertension and dyslipidemia, gout or increased uric acid) and gastrointestinal diseases (gastritis, inflammatory bowel disease, and gastric or duodenal ulcer) was observed. No significant associations between H. pylori seropositivity and one of the five investigated incident metabolic diseases/risk factors were detected in the longitudinal analysis.
Conclusion: We identified associations between age, smoking, education and alcohol intake and H. pylori seropositivity but no impact of H. pylori seropositivity on incident metabolic diseases/risk factors.
Helicobacter pylori (H. pylori) infection is one of the world's most common infections. A recent meta-analysis on global prevalence of H. pylori infection reported a wide range from 18.9% in Switzerland up to 87.7% in Nigeria (1). The prevalence in the African region is ~70%, the highest world-wide and is influenced by socio-economic status as well as levels of hygiene (1). As the majority of H. pylori infections are asymptomatic, eradication therapy is not applied to these persons and the infection persists over time, leading to inflammatory changes of the gastric mucosa. A potential risk for severe gastrointestinal diseases including gastric cancer in persons infected with H. pylori is known (2–5). In their recent review, Cellini et al. (6) describe the pathogenic link to be a cross-reactivity mechanism of the H. pylori infection that induces proliferation of CD4+ T lymphocytes. These are the lymphocytes that recognize epitopes of H. pylori, which are structurally similar to those of H+/K+-ATPase (7). In the absence of peripheral tolerance, a Th1-driven autoreactive clone is activated (8) when dendritic cells present these shared epitopes to naïve T cells. Besides gastric cancer, H. pylori infection has been suggested to be causally linked to a variety of extra-gastric diseases and metabolic derangements (3, 9). In particular, the impact of H. pylori seropositivity on newly developed diabetes mellitus has been studied over the last years providing conflicting results. A prospective study over 10 years including Latino elderlies living in California found a positive association between seropositive H. pylori status and incident diabetes (10). However, Yu et al. reported an impact of gastric atrophy but not of H. pylori infection on the incidence of diabetes (11). Further, the influence of H. pylori infection on the incidence of other metabolic disorders, gastrointestinal diseases without gastric cancer and as well extra-gastric diseases, such as neurological or hematological diseases, asthma, allergies, immune disorders or skin diseases, has been studied widely (3, 9, 12). Lastly, there is a large potential burden of impaired drug absorption in the stomach, as persistent H. pylori infections can possibly lead to an altered gastric pH (13). The aim of our study was to calculate the sex-specific prevalence of H. pylori seropositivity for the year 2007 based on the follow-up survey F4 of the KORA S4 study. Secondly, in a cross-sectional approach we aimed to investigate associations between H. pylori seropositivity at F4 and lifestyle factors, metabolic, gastrointestinal, and other diseases. Finally, in a prospective design we investigated the association between seropositive H. pylori status at F4 and incident metabolic diseases/risk factors at FF4 (second follow-up of S4) defined as type 2 diabetes, obesity, relative weight change increase, hypertension, and dyslipidemia.
Our analyses are based on data from the Cooperative Health Research in the Region of Augsburg (KORA) F4 study (2006–2008) and the KORA FF4 study (2013–2014). They are both follow-up examinations of the population-based KORA S4 study (1999–2001), conducted in the city of Augsburg and two surrounding counties. The design and background of the KORA studies have been described in detail elsewhere (14). In brief, medical examinations by trained staff, self-administered questionnaires and the collection of biosamples were applied within the studies. Details on the assessment of the variables of interest are given below. The investigations were carried out in accordance with the Declaration of Helsinki, including written informed consent from all participants. The study was approved by the ethics committee of the Bavarian Chamber of Physicians (Munich, Germany).
The data set included 3,080 participants at F4. Thereof, 3,037 participants had information on their H. pylori status at F4 available, but not necessarily at FF4. A subset of 2,075 persons participated in both surveys (F4 and FF4) and had their H. pylori status at both survey time-points available. Prevalence of H. pylori seropositivity and its association with certain diseases and lifestyle factors was described for participants of the F4 survey. We explored the impact of acute and past H. pylori infection on incident diseases/risk factors in the longitudinal design with F4 as baseline and FF4 as follow-up examination to identify incident diseases.
Antibody responses to H. pylori were determined by multiplex serology as described elsewhere (15). Briefly, 15 H. pylori proteins were recombinantly expressed as GST-X-tag fusion proteins and each antigen affinity-purified on distinct fluorescently labeled glutathione-casein coated bead sets (SeroMap, Luminex Corp., Austin, Tx, USA). A mix of these differently labeled, antigen-coupled bead sets was incubated with serum. A Luminex xMAP analyzer (Luminex Corp., Austin, Tx, USA) identifies the bead set and simultaneously quantifies bound serum IgA, IgM, and IgG by a reporter fluorescent conjugate, Streptavidin-R-Phycoerythrin. The level of antibody response is given as median fluorescence intensity (MFI). Antigen specific cut-offs were applied and seropositivity to H. pylori defined as being positive to at least 4 antigens.
Outcomes of interest for the longitudinal analysis are the following newly developed metabolic diseases/risk factors: type 2 diabetes, obesity, relative weight change increase, hypertension, and dyslipidemia. These variables were assessed at F4 and at FF4 as described subsequently. Prevalent cases at F4 were excluded from the respective longitudinal association analysis of H. pylori seropositivity at F4 and incident disease/risk factor at FF4.
Type 2 diabetes was assessed at F4 and FF4 based on an oral glucose tolerance (OGT) test and the WHO definition and classification of diabetes mellitus (16), and/or diabetes medication reported and further validated by hospital records or by contacting the participants' treating physicians. Therefore, this variable contains known validated diabetic participants (without further OGT test) as well as newly diagnosed type 2 diabetic participants identified by the OGT test. Participants with type 1 diabetes (n = 6 at F4) or unclear diabetes status (n = 38 at F4) were discarded from the analysis.
Obese participants were identified at F4 and FF4 by a body mass index (BMI) ≥30 kg/m2. The BMI was derived from body weight and height and expressed in kg/m2. Additionally, the relative weight change between F4 and FF4 was calculated as the difference of both weights divided by the weight at F4. Relative weight change increase was then defined as a relative weight change greater than zero (yes/no).
Hypertensive participants were identified at F4 and FF4 by their “actual hypertensive” status (yes/no). Actual hypertensive participants were identified according to WHO-ISH guidelines (17) as either normotensive, aware and treated, or hypertensive and aware (treated or not) or hypertensive and unaware.
Dyslipidemia at F4 and FF4 was defined by laboratory data as a ratio of total cholesterol to HDL cholesterol greater or equal to five.
All analyses were adjusted for age, sex, overweight status based on BMI (if not used as outcome variable), smoking status, education level, physical activity and alcohol intake. Age was included as continuous variable. Smoking was categorized into current, former and never smokers. The education level was available as low, medium and high representing “Hauptschule / Volksschule,” “Mittlere Reife / Realschule,” and “Abitur / Fachabitur / Fachhochschulreife,” respectively. Alcohol intake was coded as none, medium (up to 40 g/day) and high (more than 40 g/day) based on an already categorized alcohol intake variable. Participants were classified as physically inactive when they reported to do sport activities irregularly or <1 h per week in both seasons and as physical active otherwise.
The following variables were included in the descriptive analysis and the cross-sectional analysis: continuous BMI, known gout or increased serum uric acid concentration (the corresponding question assessed a physician-based diagnosis during the last 12 months), known gastritis (last 12 months), known inflammatory bowel disease (last 12 months) gastric or duodenal ulcer (last 12 months). In addition, information on the following laboratory data was included: total cholesterol (mmol/L), fasting plasma glucose (mmol/L), and cytotoxin-associated gene-A (CagA) positivity (>1,800 MFI).
A descriptive analysis of all participants who had their HP status available at F4 and FF4 (n = 2,075) was carried out. We report absolute and relative numbers for all adjustment variables and clinical characteristics of interest that had been described above. Further, means and standard deviations (SD) are given for the laboratory data. To compare the groups defined by H. pylori seropositivity the Wilcoxon rank sum test for continuous variables and the chi2-test for categorical variables were applied.
To describe the prevalence of acute and past H. pylori infection, age-standardized proportions were calculated for the KORA F4 population. As a reference group, the age distribution in Germany in the year 2007 was used, split into 10 year intervals (18). All participants with available H. pylori status were included in the analyses at F4, resulting in n = 3,037.
A cross-sectional approach was applied to identify associations of H. pylori seropositivity at F4. In the logistic regression model, all covariates and clinical outcomes described above were included. The odds ratio (OR) and 95% confidence interval (CI) are reported.
In a longitudinal design, we aimed to identify associations of H. pylori seropositivity at the F4 survey and incident metabolic diseases/risk factors at FF4. As mentioned before, prevalent cases at F4 were excluded from the respective analysis. For each outcome we fitted three generalized regression models using the log-link function to estimate relative risks (RR). Model 1 represents a raw model, adjusting only for age and sex. Model 2 additionally included obesity, physical activity, smoking status, education level, and alcohol consumption as covariates. Model 3 is a fully adjusted model, including also information on hypertension, dyslipidemia, type 2 diabetes and gout or increased uric acid. When investigating newly developed obesity, relative weight change increase, hypertension, dyslipidemia and type 2 diabetes, the corresponding adjustment variable was excluded in models 2 and 3. All adjustment information was taken from the F4 survey. Effect modification by age and sex was explored.
As a sensitivity analysis for diabetes, not only were participants suffering from type 2 diabetes at F4 excluded, but also those who were identified as pre-diabetic by the OGT test applied at the F4 examination (16). Generalized regression models 1, 2, and 3 were fitted. Further, analogous linear models with fasting plasma glucose levels as continuous outcome variable were fitted as sensitivity analyses.
All statistical analyses were performed using R3.3.2.
The mean age in the full data set used for calculating the prevalence was 56.2 years (SD 13.3) at F4 (n = 3,037). Mean age was 56.7 years (SD 13.4) in men and 55.6 years (SD 13.1) in women (p < 0.05).
Table 1 shows the baseline characteristics of the 2,075 participants of both surveys stratified by H. pylori seropositivity status at the F4 survey. The 586 (28.2%) persons with acute or past H. pylori infection were significantly (p < 0.05) older, less educated, had higher BMI, suffered more often from prediabetes/diabetes type 2, hypertension, gout or increased uric acid, and showed differences in alcohol intake compared with their counterparts. Conversely, no differences were observed in the prevalence of gastritis, inflammatory bowel disease, gastric or duodenal ulcer and dyslipidemia. In addition, the groups did not differ by sex, physical activity, smoking, total cholesterol, and fasting plasma glucose level. Sixty-three percent of the H. pylori-positive participants were also CagA-positive.
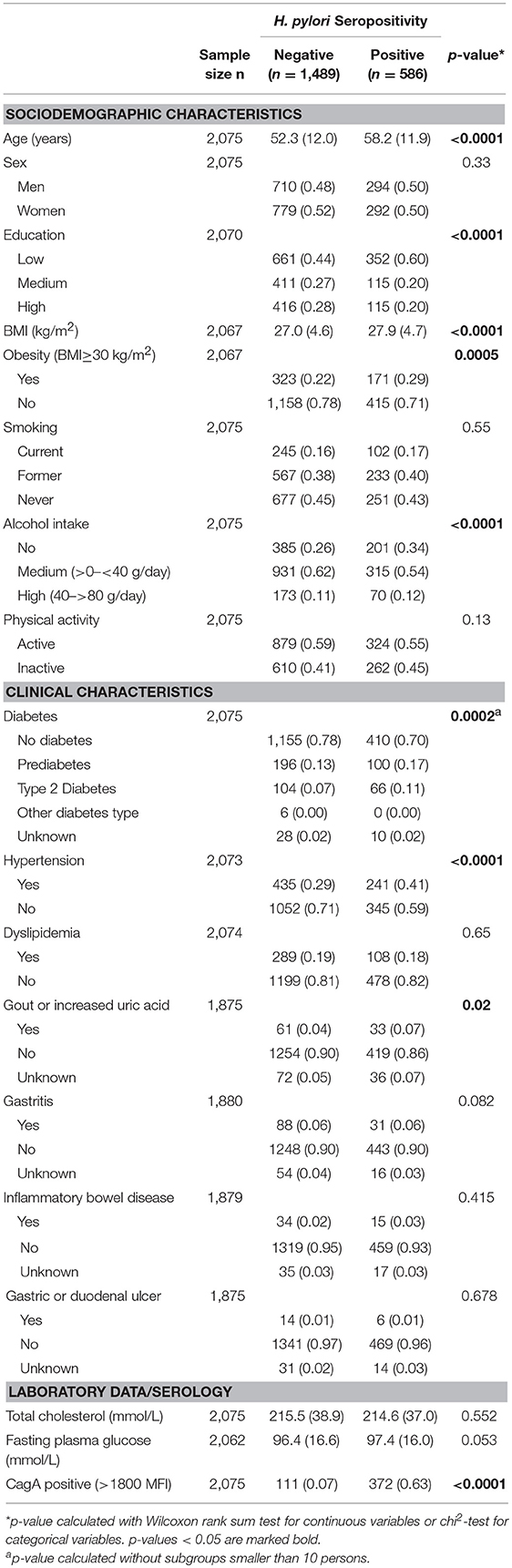
Table 1. Frequency (%) and mean (SD) of characteristic variables by H. pylori seropositivity status at the F4 survey in persons who participated in both surveys (n = 2,075).
Based on the 3,037 persons aged between 32 and 82 years who participated at the F4 survey, the age-standardized H. pylori prevalence for the year 2007 was 30.2% in men (n = 1,465) and 28.1% in women (n = 1,572). When examining the 2,075 participants with information on their H. pylori status available in both surveys, we found 73 participants who were H. pylori seropositive at the F4 survey, but not at the FF4 survey. On the contrary, we observed 72 incident cases of H. pylori infection at the FF4 survey.
In the multivariable logistic regression analysis including 2,458 persons with complete covariate data available at F4, the following factors were significantly associated with a seropositive H. pylori status: increasing age, current smoking, low education level compared to medium education level and no alcohol intake. In this cross-sectional design adjusted for co-variables at the time of the F4 survey, no associations between metabolic diseases/risk factors (BMI, type 2 diabetes, hypertension and dyslipidemia, gout or increased uric acid) and gastrointestinal disease (gastritis, inflammatory bowel disease, gastric, or duodenal ulcer) were observed (Table 2).
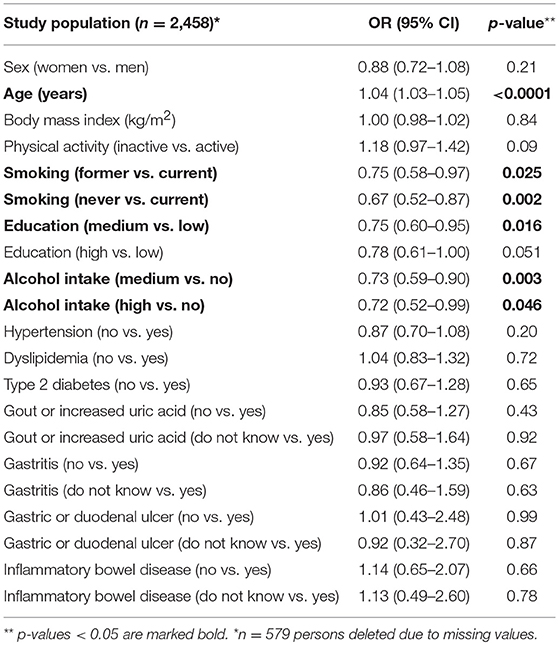
Table 2. Variables associated with H. pylori seropositivity at the F4 survey.
Table 3 provides an overview of the incident metabolic diseases/risk factors used as outcome variables and their frequencies in the 2,075 subjects participating in both surveys. In the generalized regression model analyses, no significant associations between H. pylori seropositivity at the time of the F4 survey and incident metabolic diseases/risk factors at time of the FF4 survey were observed. Sample size, adjusted relative risks (RR) and 95% CI of every statistical analysis are presented in Tables 4, 5. Inclusion of CagA seropositivity in the models did not change the results (data not shown). For the outcome “incident diabetes,” we ran a sensitivity analysis by additionally excluding participants with pre-diabetic status at F4 from the analysis. This revealed a non-significant increased risk of newly developed diabetes (model 3: OR 1.93, p = 0.056) in participants with acute or past H. pylori infection (Table 5). Further sensitivity analysis on fasting plasma glucose levels led to similar results (data not shown). Adding the interaction effects with H. pylori seropositivity to regression model 1 in the longitudinal analyses did not show effect modification by age and sex (data not shown).
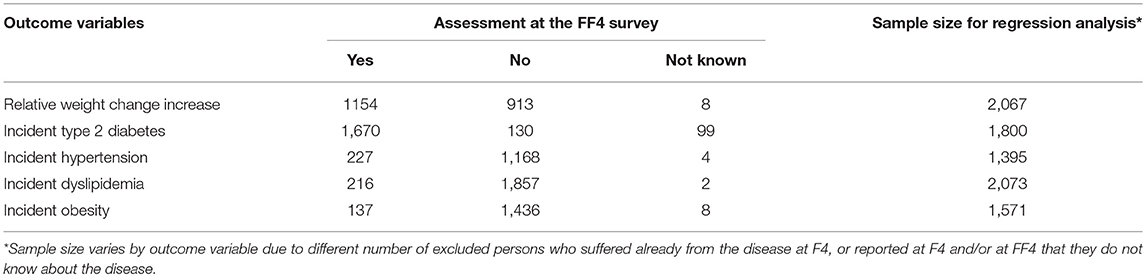
Table 3. Metabolic diseases/risk factors defined as outcome variables and their frequencies in participants assessed at the FF4 survey.
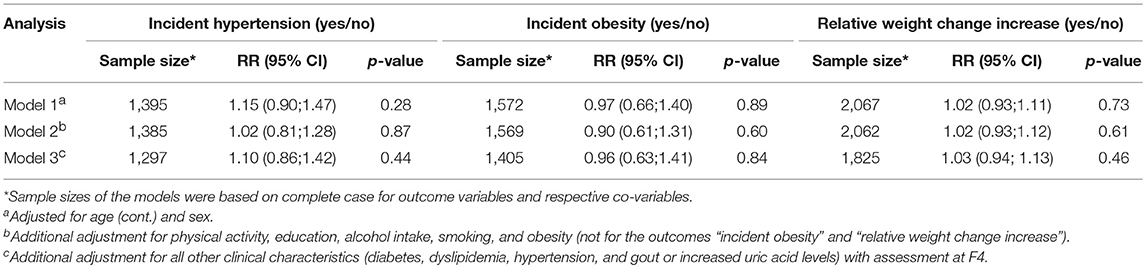
Table 4. Association of H. pylori seropositivity with incident hypertension, obesity, and relative weight change increase.
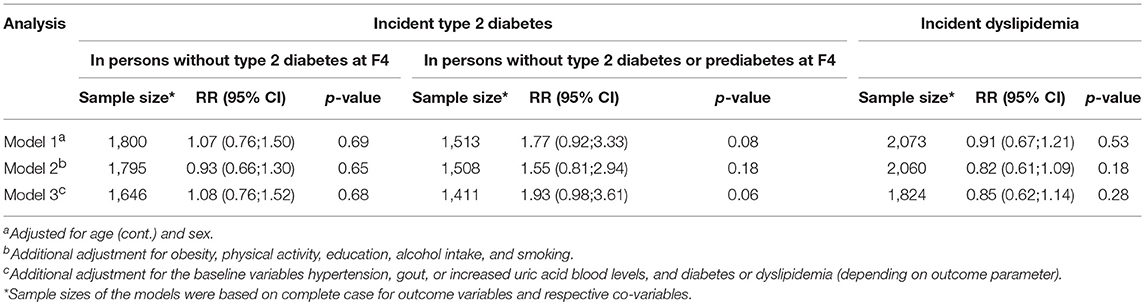
Table 5. Association of H. pylori seropositivity with incident type 2 diabetes and dyslipidemia.
Our results from the population-based KORA study are in line with earlier data on the prevalence of H. pylori seropositivity in West Germany. Further, we confirmed age, education level, smoking and alcohol intake to be associated with H. pylori seropositivity. The longitudinal analysis showed no significant association between H. pylori seropositivity and incident metabolic diseases/risk factors.
Our finding on the age-standardized H. pylori prevalence of 30% in men and 28% in women for the year 2007 is in accordance with an earlier study conducted in West Germany (19) using H. pylori serology. However, using the same assay in a population-based study conducted in the 80s in Germany, Michel, Pawlita (2) reported a H. pylori prevalence of 49% in men and 48% in women. A recent systematic review and meta-analysis on global H. pylori prevalence reported a pooled prevalence estimate for Germany of 35.3% (95% CI 31.2–39.4) based on eight studies which were conducted between 1987 and 2010 (1). Six out of these eight German studies used also serology as method to diagnose H. pylori infection and revealed prevalence estimates from 31.7% (19) up to 44.4% (20), depending on study period and region. It is known from previous studies that H. pylori prevalence depends on the development status of a country, the study region within one country, and socioeconomic status of the participants, see e.g. (21). For Germany, it is known that depending on the selected areas and study period the prevalence varies accordingly (22). Prevalence was significantly higher in all age groups of the eastern part of Germany compared to West Germany (19, 20, 22). In addition, a decrease in H. pylori prevalence over time in many developed countries was described (2, 21).
Our results confirmed that age, education level and alcohol intake are associated with H. pylori seropositivity, but lipid levels are not (23). In contrast to the findings of Rosenstock et al. (23), smoking is significantly associated with H.pylori seropositivity in our analysis whereas BMI is not. In addition, we observed no association for type 2 diabetes, hypertension and dyslipidemia, which is in accordance with the results from earlier cross-sectional studies, see e.g. (23, 24). Age, sex, BMI, and education level have been reported to be related to H. pylori infection earlier (25), as well as an inverse association with alcohol consumption (26) and, among other factors, socioeconomic status (22). Interestingly we did not find an association between gastro-intestinal diseases such as gastritis and gastric or duodenal ulcer and H. pylori seropositivity. One explanation might be that our population includes a high number of symptom-free and/or successfully treated H. pylori infections.
An explanation for the association of alcohol intake and H. pylori seropositivity might be that besides the bactericidal effect, alcoholic beverages stimulate gastric acid secretion. This could result in lowering the pH in the stomach, which could impact the H. pylori load (27, 28). Regarding the association of smoking and H. pylori infection, Endoh and Leung (29) suggested that nicotine reduces gastric mucosal blood flow, epidermal growth factor secretion, and mucus secretion, thus facilitating H. pylori colonization (30). Not every H. pylori infected participant will develop gastric atrophy (11). This aspect could also have influenced our results in the longitudinal analysis, where we did not observe a significant association of H. pylori seropositivity and incident metabolic diseases/risk factors. H. pylori infections can be seen as the most important cause of gastritis and the development of gastric and duodenal ulcer (31). A reason for the non-associations found in our longitudinal analysis could be the relatively short follow-up-time of 6–9 years between the two surveys. Therefore, a seropositive H. pylori status in the participants without significantly higher frequencies of gastrointestinal risk factors such as gastritis or peptic ulcer disease at baseline (F4 survey) might need longer periods and cofactors to evolve non-gastrointestinal diseases due to inflammatory processes suggested in the pathogenesis of those diseases (21). Although the frequency of CagA-positive strains within the H. pylori infected patients in our study was higher (63%) compared with an earlier study in Eastern Germany (32), inclusion of this virulence factor did not change the present results. Earlier prospective cohort studies regarding the impact of H. pylori infection on the incidence of diabetes reported contradictory results (10, 11). In addition, a recent meta-analysis reported increased risks of type 1 and type 2 diabetes mellitus with H. pylori infection for the included 17 case-control studies, but no significance was observed for the 2 included cohort studies (33). As a longitudinal design is mandatory for investigating incident cases without the limitation of potential “reverse causality,” our prospective study adds further non-significant findings about a potential association between H. pylori seropositivity and incident diabetes. To answer the conflicting results on diabetes risk, further prospective studies might be necessary in participants without prevalent diabetes or prediabetes. The diagnosis of an H. pylori infection should also be based on histology obtained by endoscopy to identify all cases. Furthermore, an association between H. pylori infection and newly developed obesity, hypertension, dyslipidemia or relative weight change increase was not observed in our study. As previous studies investigating cardiovascular diseases (9, 34), hypertension (35), lipid profile (3, 35–37), obesity (3), and BMI (35, 36, 38) have been mainly cross-sectional or ecological, rather than prospective in design, little evidence exists so far for meaningful causative associations.
Because our results are based on a representative sample of the German population, plausible estimates of current H. pylori prevalence could be reported. Age, education level, smoking and alcohol intake were associated with H. pylori seropositivity. Based on the findings of missing associations between acute or past H. pylori infection and incident metabolic diseases/risk factors, we conclude that further prospective studies covering a sufficient time span along with histological confirmation of active H. pylori infection are required.
The investigations were carried out in accordance with the Declaration of Helsinki, including written informed consent from all participants. The study was approved by the ethics committee of the Bavarian Chamber of Physicians (Munich, Germany).
NW and UA conceived the study and drafted the manuscript. NW performed the statistical analyses. CM, TW, JB, FP, MA, AP, WR, SK, and JL contributed to data acquisition and to the design of the study, and critically revised the manuscript. All authors have read and approved the final manuscript.
NW and UA were supported by iMed- the Helmholtz Association's Initiative on Personalized Medicine. Serolomics analyses were financially supported by the Helmholtz Association Portfolio Topic Metabolic Dysfunction and Chronic Diseases.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
We thank all the individuals and clinicians for their participation in the KORA F4 and FF4 study. The KORA study was initiated and financed by the Helmholtz Zentrum München—German Research Center for Environmental Health, which is funded by the German Federal Ministry of Education and Research (BMBF) and by the State of Bavaria.
H. pylori, helicobacter pylori; BMI, Body mass index; OGT, oral glucose tolerance; OR, odds ratio; CI, confidence interval; nmol, nanomol; L, liter; MFI, median fluorescence intensity; CagA, cytotoxin-associated gene-A; KORA, Cooperative Health Research in the Region Augsburg); S4, KORA Survey 4; F4, KORA Follow-up of S4; FF4, KORA Second Follow-up of S4.
1. Hooi JKY, Lai WY, Ng WK, Suen MMY, Underwood FE, Tanyingoh D, et al. Global prevalence of Helicobacter pylori infection: systematic review and meta-analysis. Gastroenterology. (2017) 153:420–9. doi: 10.1053/j.gastro.2017.04.022
2. Michel A, Pawlita M, Boeing H, Gissmann L, Waterboer T. Helicobacter pylori antibody patterns in Germany: a cross-sectional population study. Gut Pathog. (2014) 6:10. doi: 10.1186/1757-4749-6-10
3. Graham DY. Helicobacter pylori update: gastric cancer, reliable therapy, and possible benefits. Gastroenterology. (2015) 148:719–31.e3. doi: 10.1053/j.gastro.2015.01.040
4. Sonnenberg A. Review article: historic changes of Helicobacter pylori-associated diseases. Aliment Pharmacol Ther. (2013) 38:329–42. doi: 10.1111/apt.12380
5. Annibale B, Negrini R, Caruana P, Lahner E, Grossi C, Bordi C, et al. Two-thirds of atrophic body gastritis patients have evidence of Helicobacter pylori infection. Helicobacter. (2001) 6:225–33. doi: 10.1046/j.1083-4389.2001.00032.x
6. Cellini M, Santaguida MG, Virili C, Capriello S, Brusca N, Gargano L, et al. Hashimoto's thyroiditis and autoimmune gastritis. Front Endocrinol. (2017) 8:92. doi: 10.3389/fendo.2017.00092
7. D'Elios MM, Bergman MP, Azzurri A, Amedei A, Benagiano M, De Pont JJ, et al. H(+),K(+)-atpase (proton pump) is the target autoantigen of Th1-type cytotoxic T cells in autoimmune gastritis. Gastroenterology. (2001) 120:377–86. doi: 10.1053/gast.2001.21187
8. Varbanova M, Frauenschlager K, Malfertheiner P. Chronic gastritis - an update. Best Pract Res Clin Gastroenterol. (2014) 28:1031–42. doi: 10.1016/j.bpg.2014.10.005
9. Razuka-Ebela D, Giupponi B, Franceschi F. Helicobacter pylori and extragastric diseases. Helicobacter. (2018) 23(Suppl 1):e12520. doi: 10.1111/hel.12520
10. Jeon CY, Haan MN, Cheng C, Clayton ER, Mayeda ER, Miller JW, et al. Helicobacter pylori infection is associated with an increased rate of diabetes. Diabetes Care. (2012) 35:520–5. doi: 10.2337/dc11-1043
11. Yu TY, Wei JN, Kuo CH, Liou JM, Lin MS, Shih SR, et al. The impact of gastric atrophy on the incidence of diabetes. Sci Rep. (2017) 7:39777. doi: 10.1038/srep39777
12. de Korwin JD, Ianiro G, Gibiino G, Gasbarrini A. Helicobacter pylori infection and extragastric diseases in 2017. Helicobacter. (2017) 22(Suppl. 1):e12411. doi: 10.1111/hel.12411
13. Lahner E, Virili C, Santaguida MG, Annibale B, Centanni M. Helicobacter pylori infection and drugs malabsorption. World J Gastroenterol. (2014) 20:10331–7. doi: 10.3748/wjg.v20.i30.10331
14. Holle R, Happich M, Lowel H, Wichmann HE, Group MKS. KORA–a research platform for population based health research. Gesundheitswesen. (2005) 67(Suppl 1):S19–25. doi: 10.1055/s-2005-858235
15. Michel A, Waterboer T, Kist M, Pawlita M. Helicobacter pylori multiplex serology. Helicobacter. (2009) 14:525–35. doi: 10.1111/j.1523-5378.2009.00723.x
16. World Health Organization. Definition, Diagnosis and Classification of Diabetes Mellitus and Its Complications: Report of a WHO Consultation. Geneva. (1999).
17. World Health Organization-International Society of Hypertension. Guidelines for the management of hypertension. guidelines subcommittee. J Hypertens. (1999) 17:151–83.
18. Statistisches Bundesamt (Destatis). Population: Germany,Age in Years,Nationality/Sex/Martial Status. Table 12411-0006 [Bevölkerung: Deutschland, Stichtag, Altersjahre, Nationalität/Geschlecht/Familienstand. Tabelle 12411-0006]. (2017) 23/05/2017.
19. Holtmann G, Goebell H, Holtmann M, Talley NJ. Dyspepsia in healthy blood donors. Pattern of symptoms and association with Helicobacter pylori. Dig Dis Sci. (1994) 39:1090–8.
20. Wex T, Venerito M, Kreutzer J, Gotze T, Kandulski A, Malfertheiner P. Serological prevalence of Helicobacter pylori infection in Saxony-Anhalt, Germany, in 2010. Clin Vaccine Immunol. (2011) 18:2109–12. doi: 10.1128/CVI.05308-11
21. Pilotto A, Franceschi M. Helicobacter pylori infection in older people. World J Gastroenterol. (2014) 20:6364–73. doi: 10.3748/wjg.v20.i21.6364
22. Seher C, Thierfelder W, Dortschy R. [Helicobacter pylori–prevalence in the German population]. Gesundheitswesen. (2000) 62:598–603. doi: 10.1055/s-2000-13047
23. Rosenstock SJ, Jorgensen T, Andersen LP, Bonnevie O. Association of Helicobacter pylori infection with lifestyle, chronic disease, body-indices, and age at menarche in Danish adults. Scand J Public Health. (2000) 28:32–40. doi: 10.1177/140349480002800107
24. Regnstrom J, Jovinge S, Bavenholm P, Ericsson CG, De Faire U, Hamsten A, et al. Helicobacter pylori seropositivity is not associated with inflammatory parameters, lipid concentrations and degree of coronary artery disease. J Intern Med. (1998) 243:109–13. doi: 10.1046/j.1365-2796.1998.00202.x
25. Russo A, Eboli M, Pizzetti P, Di Felice G, Ravagnani F, Spinelli P, et al. Determinants of Helicobacter pylori seroprevalence among Italian blood donors. Eur J Gastroenterol Hepatol. (1999) 11:867–73. doi: 10.1097/00042737-199908000-00010
26. Brenner H, Berg G, Lappus N, Kliebsch U, Bode G, Boeing H. Alcohol consumption and Helicobacter pylori infection: results from the German National Health and Nutrition Survey. Epidemiology. (1999) 10:214–8. doi: 10.1097/00001648-199905000-00004
27. Ogihara A, Kikuchi S, Hasegawa A, Kurosawa M, Miki K, Kaneko E, et al. Relationship between Helicobacter pylori infection and smoking and drinking habits. J Gastroenterol Hepatol. (2000) 15:271–6. doi: 10.1046/j.1440-1746.2000.02077.x
28. Singer MV, Leffmann C, Eysselein VE, Calden H, Goebell H. Action of ethanol and some alcoholic beverages on gastric acid secretion and release of gastrin in humans. Gastroenterology. (1987) 93:1247–54. doi: 10.1016/0016-5085(87)90252-6
29. Endoh K, Leung FW. Effects of smoking and nicotine on the gastric mucosa: a review of clinical and experimental evidence. Gastroenterology. (1994) 107:864–78. doi: 10.1016/0016-5085(94)90138-4
30. Murray LJ, McCrum EE, Evans AE, Bamford KB. Epidemiology of Helicobacter pylori infection among 4742 randomly selected subjects from Northern Ireland. Int J Epidemiol. (1997) 26:880–7. doi: 10.1093/ije/26.4.880
31. Pellicano R, Ribaldone DG, Fagoonee S, Astegiano M, Saracco GM, Megraud F. A 2016 panorama of Helicobacter pylori infection: key messages for clinicians. Panminerva Med. (2016) 58:304–17.
32. Franck C, Hoffmann A, Link A, Schulz C, Wuttig K, Becker E, et al. Prevalence of Helicobacter pylori infection among blood donors in Saxony-Anhalt, Germany - a region at intermediate risk for gastric cancer. Z Gastroenterol. (2017) 55:653–6. doi: 10.1055/s-0043-106311
33. Wang F, Liu J, Lv Z. Association of Helicobacter pylori infection with diabetes mellitus and diabetic nephropathy: a meta-analysis of 39 studies involving more than 20,000 participants. Scand J Infect Dis. (2013) 45:930–8. doi: 10.3109/00365548.2013.844351
34. Yu XJ, Yang X, Feng L, Wang LL, Dong QJ. Association between Helicobacter pylori infection and angiographically demonstrated coronary artery disease: a meta-analysis. Exp Ther Med. (2017) 13:787–93. doi: 10.3892/etm.2017.4028
35. Sotuneh N, Hosseini SR, Shokri-Shirvani J, Bijani A, Ghadimi R. Helicobacter pylori infection and metabolic parameters: is there an association in elderly population? Int J Prev Med. (2014) 5:1537–42.
36. Upala S, Jaruvongvanich V, Riangwiwat T, Jaruvongvanich S, Sanguankeo A. Association between Helicobacter pylori infection and metabolic syndrome: a systematic review and meta-analysis. J Dig Dis. (2016) 17:433–40. doi: 10.1111/1751-2980.12367
37. Laurila A, Bloigu A, Nayha S, Hassi J, Leinonen M, Saikku P. Association of Helicobacter pylori infection with elevated serum lipids. Atherosclerosis. (1999) 142:207–10.
Keywords: Helicobacter pylori, multiplex serology, infection, prevalence, metabolic diseases
Citation: Wawro N, Amann U, Butt J, Meisinger C, Akmatov MK, Pessler F, Peters A, Rathmann W, Kääb S, Waterboer T and Linseisen J (2019) Helicobacter pylori Seropositivity: Prevalence, Associations, and the Impact on Incident Metabolic Diseases/Risk Factors in the Population-Based KORA Study. Front. Public Health 7:96. doi: 10.3389/fpubh.2019.00096
Received: 07 November 2018; Accepted: 04 April 2019;
Published: 24 April 2019.
Edited by:
Jimmy Thomas Efird, University of Newcastle, AustraliaReviewed by:
Marco Centanni, Sapienza University of Rome, ItalyCopyright © 2019 Wawro, Amann, Butt, Meisinger, Akmatov, Pessler, Peters, Rathmann, Kääb, Waterboer and Linseisen. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Nina Wawro, bmluYS53YXdyb0BoZWxtaG9sdHotbXVlbmNoZW4uZGU=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.