
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Public Health , 19 March 2019
Sec. Public Health Education and Promotion
Volume 7 - 2019 | https://doi.org/10.3389/fpubh.2019.00055
 Sven Messing1*
Sven Messing1* Alfred Rütten1Karim Abu-Omar1Ulrike Ungerer-Röhrich2Lee Goodwin1Ionuţ Burlacu1Günther Gediga3
Alfred Rütten1Karim Abu-Omar1Ulrike Ungerer-Röhrich2Lee Goodwin1Ionuţ Burlacu1Günther Gediga3Introduction: A vast majority of children and adolescents are physically inactive. As a result, high obesity rates and related diseases have made physical activity promotion a politically relevant topic. In order to form the basis for political decision making, evidence is required regarding the efficacy and effectiveness of interventions for physical activity promotion. In contrast to previous research, this systematic review of reviews targets three key settings (family and home, childcare, school), and is among the largest to have been conducted.
Methods: A systematic review of reviews was conducted as part of a large-scale project to develop national recommendations for physical activity promotion in Germany. Six electronic databases were searched and inclusion criteria were defined. Two independent reviewers screened the titles and abstracts of potentially relevant literature. 213 reviews were identified and categorised by target group. A total of 74 reviews were identified dealing with children and adolescents. Each review underwent a quality assessment.
Results: 39 reviews with the highest quality and relevance were analysed. Three reviews focused on the family and home setting, 4 on the childcare setting, 28 on the school setting and 4 on other settings. Evidence revealed the key role played by parents in promoting physical activity in children within each setting. Furthermore, evidence pointed toward the efficacy of multi-component interventions in the childcare and school setting. Several evidence-based intervention strategies were identified for childcare facilities and schools.
Discussion: The review of reviews identified a number of promising strategies for PA promotion among children and adolescents. Among reviews, multi-component interventions in childcare facilities and schools stand out prominently. At the same time, the review of reviews indicated that there is still a lack of studies on the efficacy of interventions that go beyond the individual level. We recommend that future research should also target community and policy level interventions and interventions other than the school setting. In order to make more specific recommendations regarding the scale-up of promising intervention strategies, further knowledge about the effectiveness, health equity and cost effectiveness of interventions is needed.
With recent studies showing that 124 million children worldwide are obese (1), physical activity (PA)—alongside nutrition—is a key in the fight against childhood obesity. Nevertheless, 75% of boys and 85% of girls in Europe (2) do not fulfil the World Health Organisation (WHO) recommendations of at least 60 min of moderate-to-vigorous-intensity PA per day (3). As the impact of PA on children's physical, psychosocial, and intellectual development is well proven (4), PA promotion is a highly relevant topic.
On the political level, central organisations are calling for action in order to combat childhood obesity. In 2011, the General Assembly of the United Nations declared that non-communicable diseases are one of the largest challenges of the twenty-first century, and that all sectors need to generate effective responses for the prevention and control of non-communicable diseases (5). Additionally, the European Union published an Action Plan on Childhood Obesity 2014–2020 (6), and the WHO formulated specific recommendations in their report “Ending Childhood Obesity” (7). Furthermore, efforts specifically focusing on PA promotion are increasing. For example, the European Union Physical Activity Guidelines recommended a number of policy actions (8), while the WHO developed a European Physical Activity Strategy for 2016–2025 (9).
Due to the high relevance of this topic in politics and public health, a large number of reviews have been conducted to identify effective interventions for PA promotion (10). From the perspective of evidence-based medicine, the preferred method of knowledge summarisation is through the conduction of a systematic review of reviews (11). Such evidence is needed as the basis for decision making and allows research to have an impact on policy and practice (12).
Over the past years, interventions for PA promotion have been investigated in reviews of reviews. Steenbock et al. (13) analysed the efficacy of interventions to promote PA and healthy eating in the childcare setting, while Kriemler et al. (14) dealt with the effects of school-based interventions on PA and fitness in children and adolescents. Moreover, the overarching review of Heath et al. (15), which investigates many different types of PA interventions (not only for children and adolescents), also includes findings on school-based interventions.
In contrast to the above reviews, our systematic review of reviews summarises the best available evidence for the target group of children and adolescents across the settings of family and home, childcare and school. Such information is required for the drafting of policy recommendations on the use of intervention strategies in settings to promote PA among children and adolescents. Another reason for obtaining such information is to identify potential “best buys” for PA promotion. Additionally, our review of reviews across settings was conducted to shed light on potential research gaps. The results were not only utilised to synthesise evidence, but have also formed parts of the German recommendations for PA promotion. To our knowledge, this review of reviews is the largest to be conducted with analysis on the efficacy and effectiveness of PA promoting interventions for children and adolescents.
This systematic review of reviews was part of a large-scale project to develop national recommendations for PA and PA promotion. The overarching aim was to provide recommendations by target group: children and adolescents, adults, older adults, adults with a chronic disease, general population. This article provides an in-depth overview of results for the target group “children and adolescents.”
In order to formulate recommendations that centre on the efficacy and effectiveness of interventions, a systematic review of reviews was conducted. Six electronic databases (PubMed, Scopus, Sport Discus, PsycInfo, ERIC, IBSS) were searched in 2015 for all publication years using the following search terms: “physical activity,” “intervention,” “evidence,” “effect,” “health,” and “review.” Alternative terms (e.g., bike, biking, cycling, walking, active transport, human powered transport, sedentary, exercise, sport) were defined and MESH-terms were formulated. Once the relevant literature had been identified, titles and abstracts were screened by two independent reviewers. The screening process was based on the following criteria: (a) The review contains empirical results from single studies. (b) The review includes interventions centred on the promotion of PA or the reduction of inactivity. (c) The review focuses on the efficacy and/or effectiveness of interventions. (d) Some of the single studies included in the review are of longitudinal design. (e) Reviews were written in English or German. Duplicates were excluded.
The titles and abstracts of the identified records were screened to ensure that the above inclusion criteria were met. Two reviewers independently screened full texts from 223 reviews in a secondary screening process. Additional hand searches were conducted to identify further reviews. The remaining 213 reviews were then categorised by target group (children and adolescents, adults, older people, people with preconditions, general population).
Seventy-four reviews dealt with the target group of children and adolescents (see Figure 1). Out of the 74 reviews, 51 were identified as a part of this systematic review of reviews, and 23 were obtained via hand search. Each of the 74 reviews underwent analysis. During the process of formulating national recommendations for PA, reviews were excluded due to the following reasons: reviews did not fulfil the inclusion criteria (16–21), did not deal with intervention studies (22), did not focus primarily on PA (23–30), were conducted unsystematically (31–39), only included a few studies dealing with PA promotion (40–42), were outdated or reported limited results (43–47), or were of very low quality (48). Once the exclusion process was complete, the total number of remaining reviews consisted of 39.
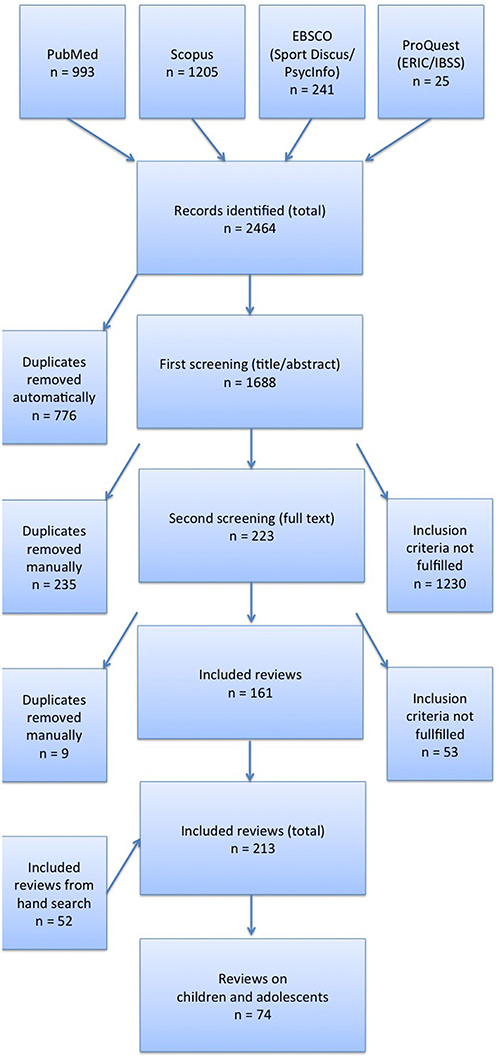
Figure 1. Flow chart.
One independent researcher assessed the quality of reviews using the AGREE instrument (49). This instrument was utilised in the formulation of the Canadian Physical Activity Guidelines (50).
The AGREE instrument comprises of five criteria that deal with the methodological quality of studies. However, as the AGREE criteria are relatively easy to fulfil, methodologically weak reviews also receive high ratings. To counter this issue, an additional instrument was developed to enhance the accurate assessment of methodological quality for the identified reviews and meta-analyses (see Table 1). In order to assess review quality, both instruments were applied by calculating percentage values for each review. These values showed the percentages of fulfilled criteria per review, both on the basis of the AGREE criteria and the criteria from our newly developed instrument. The percentage values recorded for each review were calculated based on applicable criteria (e.g., some criteria were only applicable for meta-analyses).
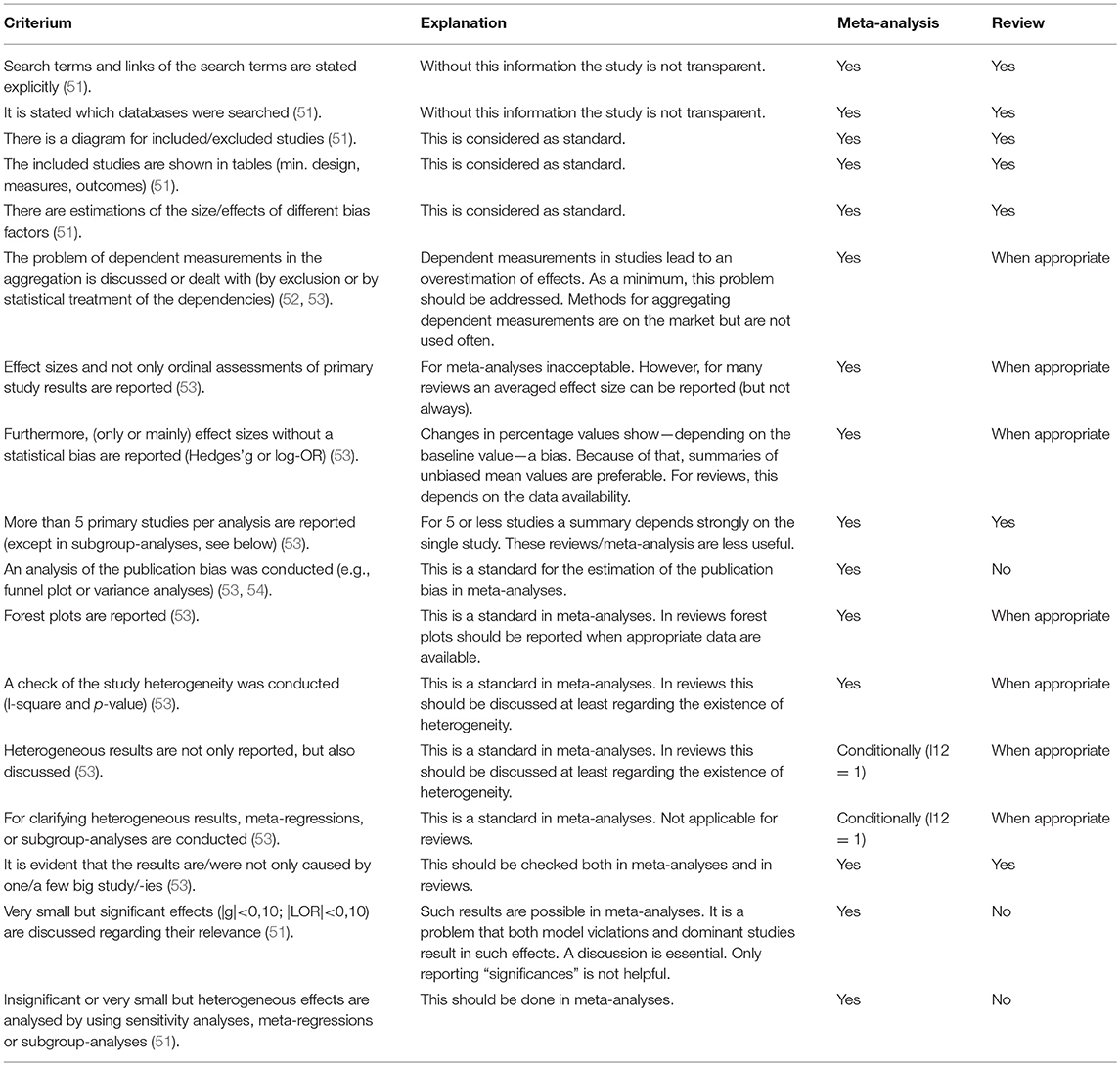
Table 1. Quality checklist.
Combining the results of AGREE and our instrument ensured reliability when differentiating between the quality of reviews (especially for high quality reviews), thus improving the overall quality of assessment. Based on the combined results obtained from both instruments, the quality of each review was defined as high, medium or low.
Following the methodology proposed by Smith et al. (11), reviews were evaluated independently by two researchers. The evaluation focused on summarising evidence pertaining to various intervention types.
A narrative synthesis of these 39 reviews is presented in this manuscript. The synthesis presents the results regarding the efficacy and effectiveness of PA promoting interventions. While efficacy trials test whether an intervention works under optimum conditions, effectiveness trials test an intervention under real-world conditions (55). However, even though the distinction of efficacy and effectiveness is highly relevant in health promotion research (56), both terms are often used interchangeably. When summarizing the main findings of the authors in our tables we overtook their wording, so that it might seem that many reviews analysed the effectiveness of interventions. In reality, and as stated in the discussion, most reviews analysed their efficacy.
Table 2 provides an overview of the quality of reviews analysed in different settings.
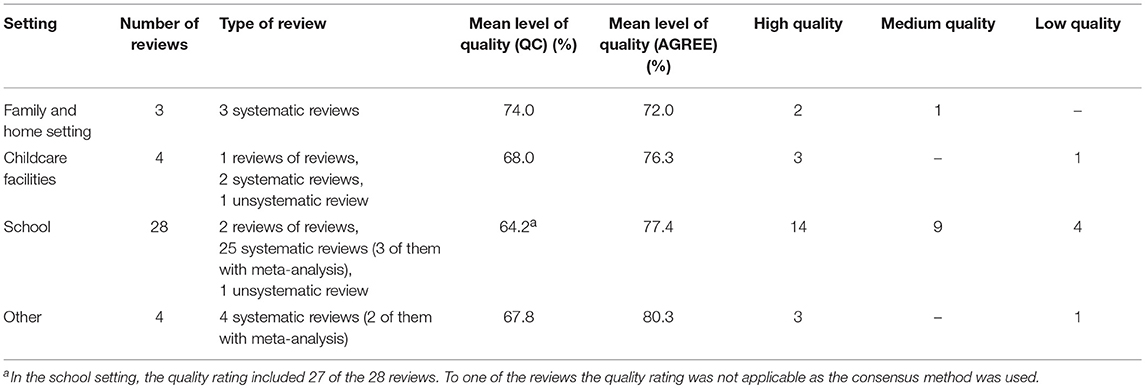
Table 2. Quality rating of the included reviews.
Three systematic reviews were identified that deal specifically with interventions in the family and home setting (Table 3) (57–59).
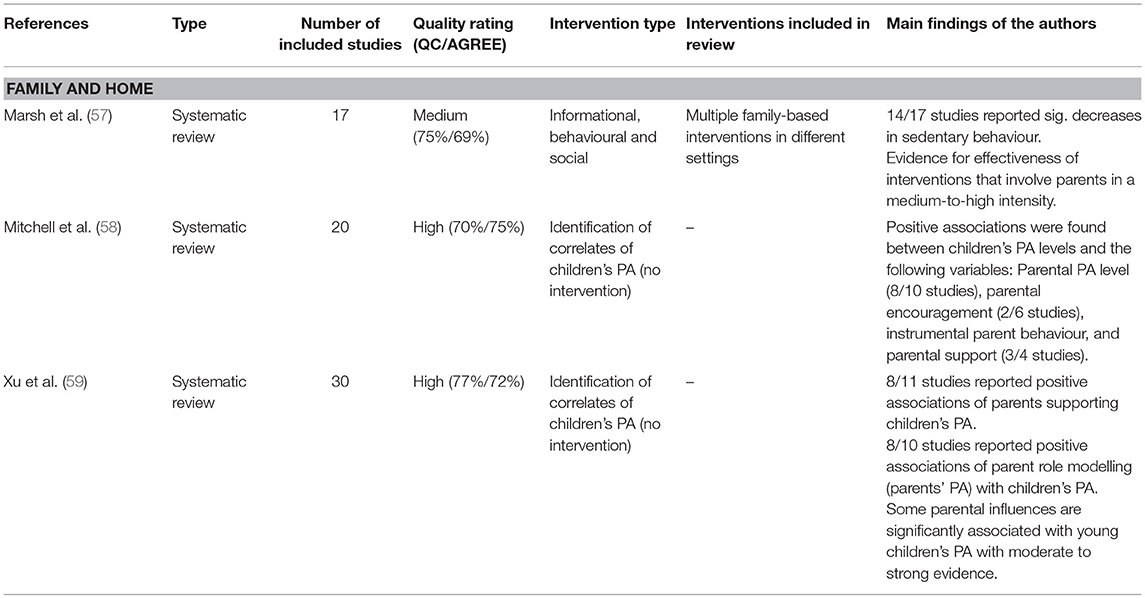
Table 3. Reviews focusing on the family and home setting.
All three reviews stated that parental encouragement and support can increase PA in children (58, 59), as well as reduce sedentary behaviour (57). Two reviews showed that parental behaviour influences the behaviour of their child. While one review identified a positive association between children's PA levels and the PA levels of their parents (58), another review found that a reduction in parental (sedentary) screen time can lead to decreased screen time in children (59). One review concluded that the level of parental involvement is more important than the setting in which the intervention is conducted (57).
The availability of PA equipment seemed to have a positive effect on children's PA levels, whereas busy work schedules and parent fatigue demonstrated negative effects (58).
Inconsistencies were found regarding the influence of parental enjoyment, maternal depressive symptoms, maternal self-efficacy, parental rules limiting sedentary behaviour, parental perceptions on the importance of PA, the level of child safety, and the child's physical competence (58).
Four of the identified reviews dealt with PA promotion in childcare facilities (Table 4). In general, the majority of interventions for pre-schoolers seem to be centre-based and teacher-delivered (60).
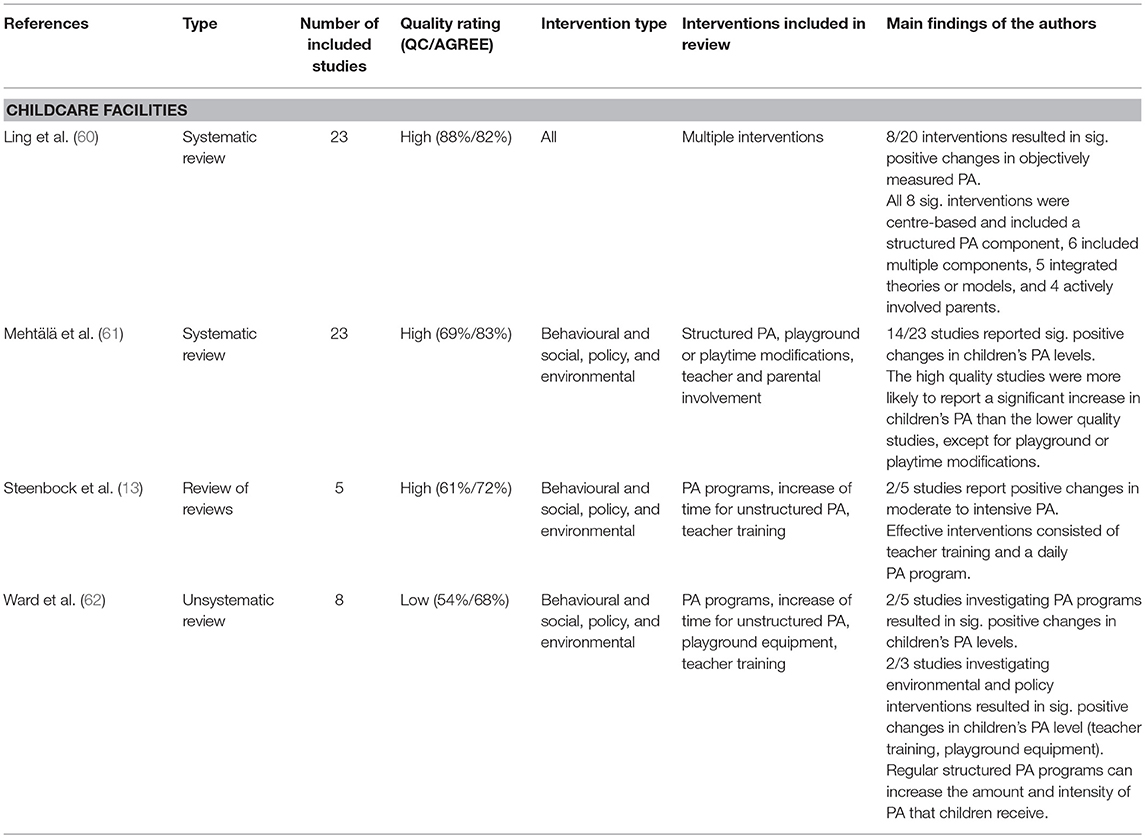
Table 4. Reviews focusing on the childcare setting.
The reviews stated that theory or model-based interventions are more successful. The review by Ling et al. (60) stressed that most theory or model-based interventions show a positive effect. In contrast, only one third of non-theory-based interventions were effective. The authors also indicated that the use of appropriate behavioural change strategies may be more important than theoretical models (60).
Furthermore, based on the available evidence, Ling et al. (60) concluded that multi-component interventions are more successful than single-component interventions. One of these components should be a structured PA programme (60, 62). Interventions that had a positive effect on PA behaviour in children integrated structured PA into the formal curriculum (60, 62). Both reviews stressed that the increase of structured PA should not be implemented at the expense of children's play time (60, 62).
Additionally, as children are most active during the first 10–15 min of being outdoors, experts suggest the provision of more free time (62). Another way to alter the free play environment at preschool is to provide additional play equipment—when play equipment isn't provided, children are more prone to sedentary behaviour and engagement in games that promote inactivity (62).
To conduct interventions for PA promotion, Mehtälä et al. (61) recommended PA-specific in-service teacher training. Both experience and personal characteristics played an important role in the promotion of PA among children in the childcare setting (61). Furthermore, Ward et al. (62) stated that there is a need for teacher training, and that structured PA programs should be implemented by staff who are specialised and well-trained. Having well-qualified staff could also support skill development and competence in children (13).
Two reviews recommended involving parents (13, 60), while one review stated that evidence on parental support “remains unclear” (61). Nevertheless, Mehtälä et al. (61) also stated that family is the most influential setting for young children, and that a partnership between families and childcare is crucial. Regarding specific strategies for parental involvement, providing health promotion information to parents is recommended in one review (13).
28 of the identified reviews focused on the school setting (see Table 5). Strong evidence indicates that multi-component interventions are effective in the promotion of PA (14, 63–69). While multi-component interventions are more effective than single-component interventions (14, 70) they do not seem to produce synergistic results (63, 71).
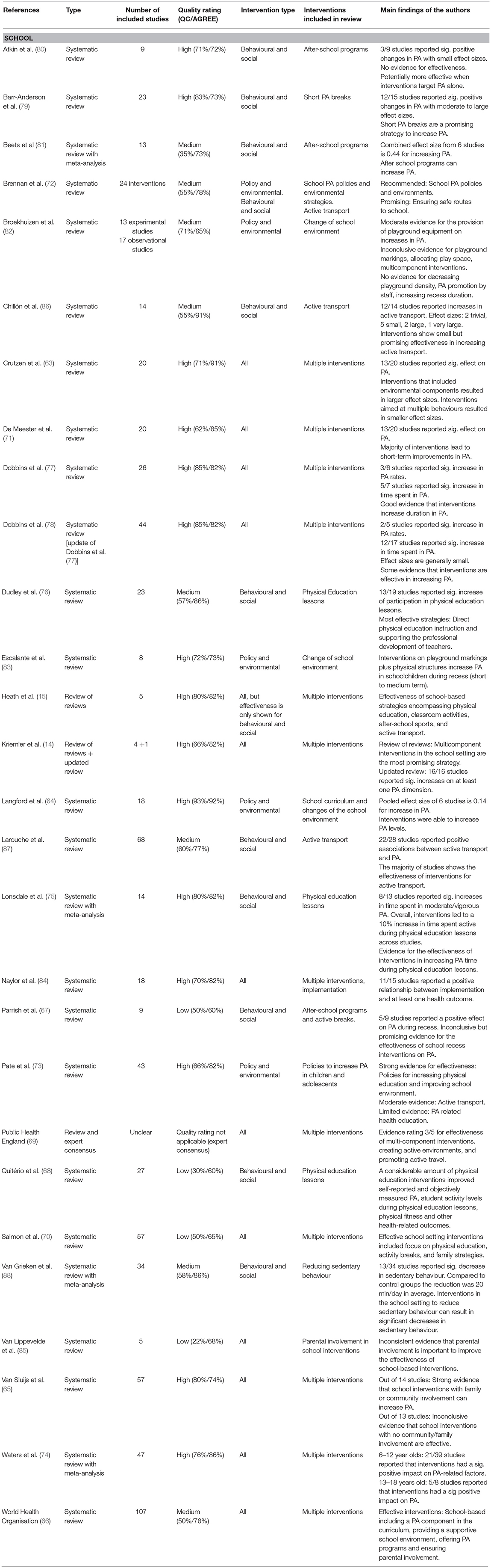
Table 5. Reviews focusing on the school setting.
As one part of a multi-component approach, a range of reviews stated that interventions targeting physical education lessons are effective. Firstly, evidence shows that increasing the number of PE lessons is a key strategy to promote PA in school children (15, 72–74). Secondly, improving the quality of PE lessons can be effective (15, 75). Lonsdale et al. (75) indicated that interventions can increase time spent in moderate-to-vigorous PA by 24% in PE lessons, thus substantially influencing the total amount of PA. Third, and strongly connected to higher quality PE lessons, reviews specified teacher training and capacity building as effective strategies to promote PA in school children (15, 66, 69, 74–76).
Furthermore, several reviews provide evidence for the integration of (more) PA into the curriculum (15, 66, 69, 74, 77, 78). Evidence on integrating (PA-related) health education into the curriculum is inconclusive. While the integration of health education into the curriculum was recommended in one of the reviews (68), another review stated that results were mixed (73).
Activity breaks—the integration of short bouts of PA into organisational routine—is another effective strategy to promote PA in the school setting (15, 70, 79), and has demonstrated “modest but consistent benefits” (79).
After-school programs focused on PA and/or sports are also effective (15, 70, 80, 81). In this context, improving students' attendance rates is highly important as the effectiveness of a program depends strongly on attendance (81).
Changing the school environment also has an influence on PA in school children and is recommended in numerous reviews (63, 66, 69, 71, 73, 74). In particular, the provision of equipment for games and playgrounds (15, 67, 82) has proved effective. One review stated that the use of playground markings can increase PA in children during recess and lunchtime (67), whereas another study found inconclusive evidence (82). In one review, significant associations were found between decreased playground density and PA in children (82). Evidence on the effectiveness of interventions that only focus on environmental changes is limited (65, 83); such interventions should be integrated in multicomponent approaches (65, 83).
Numerous reviews reported positive effects when involving parents (63, 66, 71, 74, 84, 85) and families (14, 65, 70) in school-based interventions. Only one review indicated that evidence for parental involvement was inconclusive due to a lack of studies (85). One review of reviews mentioned that most but not all included records support the effectiveness of family involvement (14).
Community involvement was linked with positive outcomes in two reviews (65, 70). Surprisingly, one review stated that school-based interventions employing a community component were ineffective (70).
The involvement of pupils is another relevant factor (69), as peer support can increase PA levels in school children (63, 71). Adjusting interventions to this specific target population is necessary (15).
Promoting active transport to school is another effective strategy to promote PA among children and adolescents (15, 69, 73, 86, 87). This strategy is related to promising policies such as ensuring safe routes to school and improving urban design (72, 73).
Finally, a number of reviews in the school setting addressed whether an intervention should acknowledge several behavioural components. While Pate et al (73) didn't find any differences between interventions addressing single or multiple behavioural components, five other reviews did. The evidence shows that interventions addressing more than one health behaviour are less effective (63, 71). The integration of other components in addition to PA was considered as a “stumbling block for success” (14). This point is stressed in another review that focuses on after-school programs (80). In general, intervention effectiveness is higher when focus is placed on a specific goal compared to interventions that require broader focus (86).
Four reviews were classified as “other” as their results were not connected with one specific setting (Table 6).
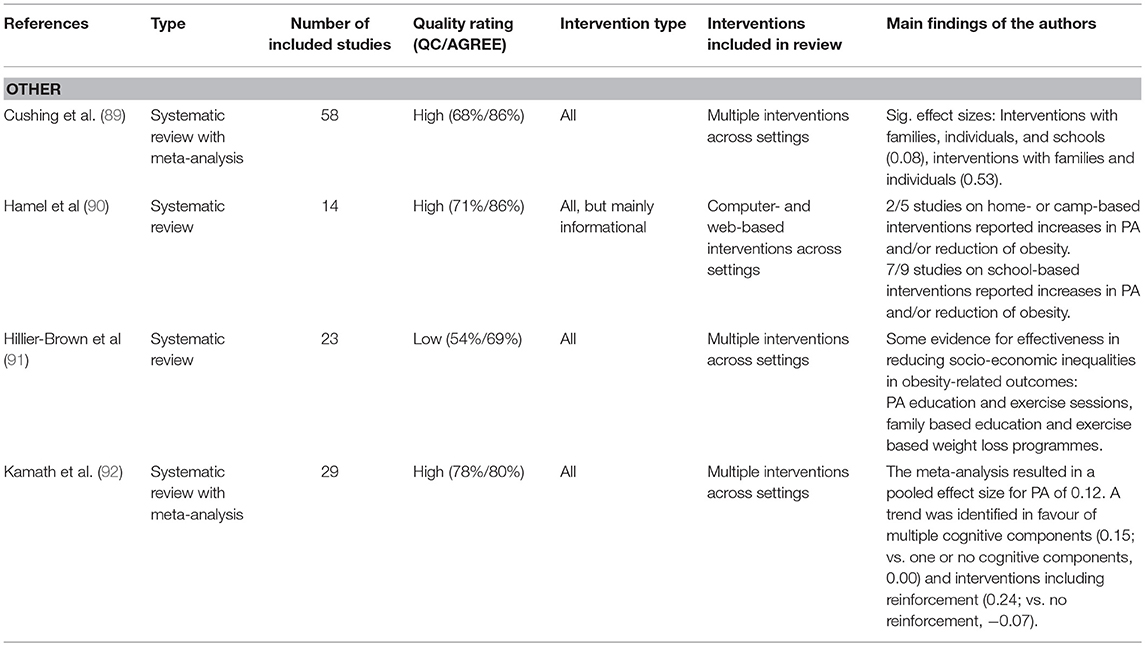
Table 6. Reviews focusing on other settings.
Three of these reviews analysed a broad range of health promoting interventions (89, 91, 92). As the reviews dealt with interventions not only pertaining to PA, results on efficacy are not as specific as other reviews. Overall, the reviews stated that health promotion interventions can be effective in terms of health (89), obesity prevention (92), and the reduction of socioeconomic inequalities in obesity (91). One of the reviews stated that interventions in the healthcare setting can be effective (91).
One of the reviews analysed computer- and web-based interventions in both the home and school setting (90). This intervention type can be effective, especially with regard to schools (90).
This systematic review of reviews provided important findings regarding PA promotion for children and adolescents:
• Parents play a key role in the family and home setting. In settings such as childcare facilities and schools, evidence shows that parental involvement is an important factor for the efficacy of interventions.
• Multi-component interventions proved to be effective in the childcare setting and the school setting.
• For childcare facilities, reviews stated that interventions should be theory or model-based, include a PA programme, provide more free time, and contain teacher training.
• In schools, evidence is available for increasing the number of PE lessons, as well as improving the quality of PE lessons, teacher training and capacity building. Furthermore, findings indicate the efficacy of other intervention strategies: implementation of more PA into the curriculum; activity breaks; after-school programs; changes in the school environment; promotion of active transport; community and peer involvement.
Additionally, several gaps were identified in the evidence base. These gaps partly reflect underlying controversies regarding research paradigms utilised to study effects of PA interventions:
• Research focuses primarily on individual level interventions even though community and policy level interventions are considered to be more effective in terms of public health (61). Such focus on individual level interventions can be explained by the predominance of evidence-based medicine (92) for the evaluation of interventions. Within the paradigm of evidence-based medicine, it is of high importance to generate knowledge through randomised and controlled trials. These study designs, however, have low applicability if one wants to examine policy or environmental interventions. Due to this, a combined use of systematic reviews, meta-analysis and realist synthesis as employed in a recent analysis of family-based PA interventions (93) seems to be beneficial.
• Research is dominated by studies investigating interventions in the school setting. Interventions in the settings of family and childcare were only investigated in a limited number of reviews—even though there is a lack of knowledge regarding interventions outside of the school setting (70). One review couldn't identify a single study including effective interventions for children aged 0–5 years (74). In particular, for nations where children only spend half a day in school (for example, in Germany), school-based interventions might have less relevance for PA promotion. This is because schools have neither the capacities nor the facilities for additional interventions for PA promotion. For such nations, more knowledge is needed on PA promotion outside of the school setting.
• Research on interventions in settings other than family, childcare and school is almost non-existent. As other studies show that computer- and web-based interventions can be effective in promoting PA of children and adolescents (90), this gap in the evidence base could limit public health impact. Moreover, we could not find any evidence regarding the sport club setting. In particular, for nations which have a sport club-based system for PA in leisure-time, such knowledge could prove valuable.
• Most reviews investigated the “efficacy” of interventions with very limited information on “effectiveness” (90). This is problematic as researchers raise the question whether interventions that are successful in efficacy studies are also effective in the real world (56). From a Public Health perspective, study designs that allow for the simultaneous testing of both efficacy and effectiveness—such as pragmatic trials (93)—might be more appropriate to generate this evidence. This could allow accelerating scale-up processes of interventions. Also the RE-AIM framework can be used for analysing both efficacy and effectiveness of interventions, as recent systematic reviews of physical activity interventions for children and youth show (94, 95).
From an international perspective, the key findings and gaps in the evidence base are associated with several challenges for PA promotion. Such challenges are mainly caused due to focus being placed on the school setting:
• Firstly, the concrete implementation of effective interventions depends on the structure of the educational system. In a study comparing the educational governance of the USA and France, the authors stated that “institutional sectors in liberal polities are often organised as complex multi-layered governance systems characterised by fragmented decision-making structures.” In state-centred polity on the other hand, “one can expect more tightly structured institutional sectors” (96). These findings affect the implementation of the results from this systematic review of reviews into practice (e.g., with regard to the number and quality of PE lessons). In Germany, the federal system's fragmented decision-making structure allows federal states to decide on school curricula (97, 98). In Hungary however, regulation on daily PE classes was implemented as a nation-wide policy in 2012/2013 (99).
• Secondly, interventions that are most needed might also be connected with overall school policy. In Germany, school lessons usually finish at 1 p.m. or 2 p.m. However, the percentage of pupils visiting all-day schools has constantly risen over the years (from 9.8% in 2002 up to 39.3% in 2015) (100). With an increasing number of pupils visiting all-day schools, the need for additional sport facilities, and changes in the school environment might be most relevant.
• For school children, the integration of sectors other than education is only investigated as part of a multi-component approach. The necessity of focusing on the family setting is stressed by findings on the importance of parental involvement. For the promotion of active transport to school, the influence of urban planning requires further investigation.
• The question of how to finance interventions in the education sector was not even raised in the reviews, even though the lack of public funding and resources is perceived as a barrier for childhood obesity prevention by two thirds of stakeholders in Europe (101). Intersectoral partnerships might be a promising approach to finance programs with combined resources.
Based on this comprehensive and up-to-date cross-sectoral review, national recommendations for physical activity promotion were developed in Germany. These recommendations aim to have an impact on public health by offering scientific orientation for experts and stakeholders. Alongside the efficacy of interventions, the national recommendations also consider aspects regarding PA promotion in children and adolescents (102):
• Effectiveness: In terms of public health, did the intervention prove to be effective on a large scale?
• Health equity: Is the intervention able to address and reduce health inequalities?
• Cost effectiveness: Does the intervention demonstrate a good relation between costs and the expected benefits?
• Quality criteria: Which criteria need to be considered to ensure the successful implementation of an intervention?
Considering these aspects is highly beneficial for bridging the gap between evidence and practice. For decision makers, effectiveness and health equity are important criteria, as well as cost effectiveness. Furthermore, quality criteria are important for practitioners, and decision makers: For example, evidence shows that the involvement of all relevant stakeholders—children, families, teaching staff and management—in the planning of an intervention increases the likelihood of its success (102–108).
In order to improve the evidence base, future research on PA promotion for children and adolescents should focus on the above-mentioned aspects (109).
AR acquired the funding, administrated the project, developed concept and methodology of this study and analysed the data. SM supported both literature search and data analysis and wrote the original manuscript draft. KA-O oversaw the literature search and data analysis and supported the development of the original draft. UU-R performed data analyses. LG contributed to manuscript preparation through the revision of numerous drafts. IB supported the literature search. GG developed the quality assessment tool and assessed the quality of reviews. All authors critically reviewed and edited the manuscript.
This research was conducted as part of a project funded by the German Federal Ministry of Health (ZMVI 5 2514FSB-200).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
PA, Physical activity; WHO, World Health Organisation.
1. NCD Risk Factor Collaboration (NCD-RisC). Worldwide trends in body-mass index, underweight, overweight, and obesity from 1975 to 2016: a pooled analysis of 2416 population-based measurement studies in 128.9 million children, adolescents, and adults. Lancet. (2017) 90:2627–42. doi: 10.1016/S0140-6736(17)32129-3
2. WHO Regional Office for Europe. Adolescent obesity and related behaviours: trends and inequalities in the WHO European Region, 2002-2014. Copenhagen (2017). Available online at: http://www.euro.who.int/__data/assets/pdf_file/0019/339211/WHO_ObesityReport_2017_v3.pdf (Accessed September 4, 2018).
3. World Health Organization. Global Recommendations on Physical Activity for Health. (2010). Available online at: http://www.who.int/dietphysicalactivity/publications/9789241599979/en/ (Accessed September 4, 2018).
4. Timmons BW, Leblanc AG, Carson V, Connor Gorber S, Dillman C, Janssen I, et al. Systematic review of physical activity and health in the early years (aged 0-4 years). Appl Physiol Nutr Metab. (2012) 37:773–92. doi: 10.1139/h2012-070
5. United Nations. Resolution 66/2. Political Declaration of the High-Level Meeting of the General Assembly on the Prevention and Control of Non-communicable Diseases. New York, NY (2011). Available online at: http://www.who.int/nmh/events/un_ncd_summit2011/political_declaration_en.pdf (Accessed September 4, 2018).
6. European Union. EU Action Plan on Childhood Obesity 2014-2020. Brussels (2014). Available online at: https://ec.europa.eu/health/sites/health/files/nutrition_physical_activity/docs/childhoodobesity_actionplan_2014_2020_en.pdf (Accessed September 4, 2018).
7. World Health Organization. Report of the Commission on Ending Childhood Obesity. Geneva (2016). Available online at: https://www.who.int/end-childhood-obesity/publications/echo-report/en/ (Accessed September 4, 2018).
8. European Commission. EU Physical Activity Guidelines. Recommended Policy Actions in Support of Health-Enhancing Physical Activity. (2008). Available online at: http://ec.europa.eu/assets/eac/sport/library/policy_documents/eu-physical-activity-guidelines-2008_en.pdf (Accessed September 4, 2018).
9. WHO Regional Office for Europe. Physical activity strategy for the WHO European Region 2016-2025. Vilnius 2015. Available online at: http://www.who.int/end-childhood-obesity/publications/echo-report/en/ (Accessed September 4, 2018).
10. Rütten A, Schow D, Breda J, Galea G, Kahlmeier S, Oppert JM, et al. Three types of scientific evidence to inform physical activity policy: results from a comparative scoping review. Int J Public Health. (2016) 61:553–63. doi: 10.1007/s00038-016-0807-y
11. Smith V, Devane D, Begley CM, Clarke M. Methodology in conducting a systematic review of systematic reviews of healthcare interventions. BMC Med Res Methodol. (2011) 11:15. doi: 10.1186/1471-2288-11-15
12. Brownson RC, Jones E. Bridging the gap: translating research into policy and practice. Prev Med. (2009) 49:313–5. doi: 10.1016/j.ypmed.2009.06.008
13. *Steenbock B, Pischke CR, Schonbach J, Pottgen S, Brand T. Wie wirksam sind ernährungs- und bewegungsbezogene primärpräventive Interventionen im Setting Kita? Ein review von reviews. Bundesgesundheitsblatt, Gesundheitsforschung, Gesundheitsschutz. (2015) 58:609–19. doi: 10.1007/s00103-014-2100-7
14. *Kriemler S, Meyer U, Martin E, van Sluijs EM, Andersen LB, Martin BW. Effect of school-based interventions on physical activity and fitness in children and adolescents: a review of reviews and systematic update. Br J Sports Med. (2011) 45:923–30. doi: 10.1136/bjsports-2011-090186
15. *Heath GW, Parra DC, Sarmiento OL, Andersen LB, Owen N, Goenka S, et al. Evidence-based intervention in physical activity: lessons from around the world. Lancet. (2012) 380:272–81. doi: 10.1016/S0140-6736(12)60816-2
16. Williams AJ, Henley WE, Williams CA, Hurst AJ, Logan S, Wyatt KM. Systematic review and meta-analysis of the association between childhood overweight and obesity and primary school diet and physical activity policies. Int J Behav Nutr Phys Act. (2013) 10:101. doi: 10.1186/1479-5868-10-101
17. Yeh MC, Beharie N, Obenchain J. Effectiveness of school-based policies to reduce childhood obesity. In: Black CI, editor. Overweightness and Walking. New York, NY: Nova Science Publishers, Inc. (2010). p. 193–209.
18. Basch CE. Healthier Students Are Better Learners: A Missing Link in School Reforms to Close the Achievement Gap. Equity Matters: Research Review No 6. (2010).
19. Metos J, Murtaugh M. Words or reality: are school district wellness policies implemented? A systematic review of the literature. Child Obes. (2011) 7:90–100. doi: 10.1089/chi.2011.07.02.0514.metos
20. McPherson AC, Keith R, Swift JA. Obesity prevention for children with physical disabilities: a scoping review of physical activity and nutrition interventions. Disabil Rehabil. (2014) 36:1573–87. doi: 10.3109/09638288.2013.863391
21. Sargent GM, Forrest LE, Parker RM. Nurse delivered lifestyle interventions in primary health care to treat chronic disease risk factors associated with obesity: a systematic review. Obes Rev. (2012) 13:1148–71. doi: 10.1111/j.1467-789X.2012.01029.x
22. Lee MC, Orenstein MR, Richardson MJ. Systematic review of active commuting to school and children's physical activity and weight. J Phys Act Health. (2008) 5:930–49. doi: 10.1123/jpah.5.6.930
23. Bond M, Wyatt K, Lloyd J, Welch K, Taylor R. Systematic review of the effectiveness and cost-effectiveness of weight management schemes for the under fives: a short report. Health Technol Assess. (2009) 13:1–75. doi: 10.3310/hta13610
24. Brand T, Pischke CR, Steenbock B, Schoenbach J, Poettgen S, Samkange-Zeeb F, et al. What works in community-based interventions promoting physical activity and healthy eating? A review of reviews. Int J Environ Res Public Health. (2014) 11:5866–88. doi: 10.3390/ijerph110605866
25. Brown T, Summerbell C. Systematic review of school-based interventions that focus on changing dietary intake and physical activity levels to prevent childhood obesity: an update to the obesity guidance produced by the National Institute for Health and Clinical Excellence. Obes Rev. (2009) 10:110–41. doi: 10.1111/j.1467-789X.2008.00515.x
26. Kelly SA, Melnyk BM. Systematic review of multicomponent interventions with overweight middle adolescents: implications for clinical practice and research. Worldviews Evid-Based Nurs. (2008) 5:113–35. doi: 10.1111/j.1741-6787.2008.00131.x
27. Verstraeten R, Roberfroid D, Lachat C, Leroy JL, Holdsworth M, Maes L, et al. Effectiveness of preventive school-based obesity interventions in low- and middle-income countries: a systematic review. Am J Clin Nutr. (2012) 96:415–38. doi: 10.3945/ajcn.112.035378
28. Collins CE, Burrows TL, Bray J, Asher R, Young M, Morgan PJ. Effectiveness of parent-centred interventions for the prevention and treatment of childhood overweight and obesity in community settings: a systematic review. JBI Database Syst Rev Implement Rep. (2013) 11:180–257. doi: 10.11124/jbisrir-2013-709
29. Wang Y, Wu Y, Wilson RF, Bleich S, Cheskin L, Weston C, et al. Childhood obesity prevention programs: comparative effectiveness review and meta-analysis. In: Comparative Effectiveness Reviews, No. 115. Rockville, MD: Agency for Healthcare Research and Quality (US) (2013).
30. Hieftje K, Edelman EJ, Camenga DR, Fiellin LE. Electronic media-based health interventions promoting behavior change in youth: a systematic review. JAMA Pediatr. (2013) 167:574–80. doi: 10.1001/jamapediatrics.2013.1095
31. Bassett DR, Fitzhugh EC, Heath GW, Erwin PC, Frederick GM, Wolff DL, et al. Estimated energy expenditures for school-based policies and active living. Am J Prev Med. (2013) 44:108–13. doi: 10.1016/j.amepre.2012.10.017
32. Cale L, Harris J. Interventions to promote young people's physical activity: issues, implications and recommendations for practice. Health Educ J. (2006) 65:320–37. doi: 10.1177/0017896906069370
33. Floriani V, Kennedy C. Promotion of physical activity in primary care for obesity treatment/prevention in children. Curr Opin Pediatr. (2007) 19:99–103. doi: 10.1097/MOP.0b013e328013c88c
34. He G, Huang WY, Wong SH. Physical activity research in Hong Kong from 1987 to 2012: evidence on children and adolescents. Asia Pac J Public Health. (2014) 26:560–74. doi: 10.1177/1010539513499623
35. Salmon J, Tremblay MS, Marshall SJ, Hume C. Health risks, correlates, and interventions to reduce sedentary behavior in young people. Am J Prev Med. (2011) 41:197–206. doi: 10.1016/j.amepre.2011.05.001
36. Sreevatsava M, Narayan KMV, Cunningham SA. Evidence for interventions to prevent and control obesity among children and adolescents: its applicability to India. Indian J Pediatr. (2012) 80:115–22. doi: 10.1007/s12098-012-0881-y
37. Steinbeck KS. The importance of physical activity in the prevention of overweight and obesity in childhood: a review and an opinion. Obes Rev. (2001) 2:117–30. doi: 10.1046/j.1467-789x.2001.00033.x
38. Kumanyika SK, Swank M, Stachecki J, Whitt-Glover MC, Brennan LK. Examining the evidence for policy and environmental strategies to prevent childhood obesity in black communities: new directions and next steps. Obes Rev. (2014) 15:177–203. doi: 10.1111/obr.12206
39. Sallis JF, Carlson JA, Mignano AM. Promoting youth physical activity through physical education and after-school programs. Adolesc Med State Art Rev. (2012) 23:493–510. doi: 10.1177/1524839914567740
40. Faulkner G, Paul Grootendorst P, Nguyen VH, Ferrence R, Mendelson R, Donnelly P, et al. Economic Policy, Obesity and Health: A Scoping Review. Final report submitted to the Heart and Stroke Foundation of Canada (2010).
41. Kristensen AH, Flottemesch TJ, Maciosek MV, Jenson J, Barclay G, Ashe M, et al. Reducing childhood obesity through U.S. federal policy. A microsimulation analysis. Am J Prev Med. (2014) 47:604–12. doi: 10.1016/j.amepre.2014.07.011
42. Trost SG, Ward DS, Senso M. Effects of child care policy and environment on physical activity. Med Sci Sports Exerc. (2010) 42:520–5. doi: 10.1249/MSS.0b013e3181cea3ef
43. Campbell KJ, Hesketh KD. Strategies which aim to positively impact on weight, physical activity, diet and sedentary behaviours in children from zero to five years. A systematic review of the literature. Obes Rev. (2007) 8:327–38. doi: 10.1111/j.1467-789X.2006.00305.x
44. Kahn EB, Ramsey LT, Brownson RC, Heath GW, Howze EH, Powell KE, et al. The effectiveness of interventions to increase physical activity: a systematic review. Am J Prev Med. (2002) 22:73–107. doi: 10.1016/S0749-3797(02)00434-8
45. Lister-Sharp D, Chapman S, Stewart-Brown S, Sowden A. Health promoting schools and health promotion in schools: two systematic reviews. Health Technol Assess. (1999) 3:1–207.
46. Maher CA, Lewis LK, Ferrar K, Marshall S, De Bourdeaudhuij I, Vandelanotte C. Are health behavior change interventions that use online social networks effective? A systematic review. J Med Internet Res. (2014) 16:e40. doi: 10.2196/jmir.2952
47. Matson-Koffman DM, Brownstein JN, Neiner JA, Greaney ML. A site-specific literature review of policy and environmental interventions that promote physical activity and nutrition for cardiovascular health: what works? Am J Health Promot. (2005) 19:167–93. doi: 10.4278/0890-1171-19.3.167
48. Borras PA. Health promoting schools, interventions and strategies to increase physical activity: review and recommendations. J Phys Educ Health Soc Perspect. (2012) 2:45–51. Available online at: http://cejsh.icm.edu.pl/cejsh/element/bwmeta1.element.desklight-5fd2e3c6-83ec-4212-9d71-fb38a43adcb2
49. Cluzeau F, Burgers J, Brouwers M, Grol R, Mäkelä M, Littlejohns P, et al. Development and validation of an international appraisal instrument for assessing the quality of clinical practice guidelines: the AGREE project. Qual Safety Health Care. (2003) 12:18–23. Available online at: https://qualitysafety.bmj.com/content/12/1/18
50. Tremblay MS, Kho ME, Tricco AC, Duggan M. Process description and evaluation of Canadian Physical Activity Guidelines development. Int J Behav Nutr Phys Act. (2010) 7:42. doi: 10.1186/1479-5868-7-42
51. Higgins JP, Green S. Cochrane Handbook for Systematic Reviews of Interventions. Version 5.1.0 [updated March 2011]. Available online at: http://handbook-5-1.cochrane.org
52. Hedges LV, Tipton E, Johnson MC. Robust variance estimation in meta-regression with dependent effect size estimates. Res Synth Methods. (2010) 1:39–65. doi: 10.1002/jrsm.5
53. Borenstein M, Hedges LV, Higgins JPT, Rothstein HR. Introduction to Meta-Analysis. Hoboken, NJ: Wiley (2009).
54. Sterne JA, Egger M, Smith GD. Systematic reviews in health care: investigating and dealing with publication and other biases in meta-analysis. BMJ. (2001) 323:101–5. doi: 10.1136/bmj.323.7304.101
55. Flay BR. Efficacy and effectiveness trials (and other phases of research) in the development of health promotion programs. Prev Med. (1986) 15:451–74.
56. Glasgow RE, Lichtenstein E, Marcus AC. Why don't we see more translation of health promotion research to practice? rethinking the efficacy-to-effectiveness transition. Am J Public Health. (2003) 93:1261–7.
57. *Marsh S, Foley LS, Wilks DC, Maddison R. Family-based interventions for reducing sedentary time in youth: a systematic review of randomized controlled trials. Obes Rev. (2014) 15:117–33. doi: 10.1111/obr.12105
58. *Mitchell J, Skouteris H, McCabe M, Ricciardelli LA, Milgrom J, Baur LA, et al. Physical activity in young children: a systematic review of parental influences. Early Child Develop Care. (2012) 182:1411–37. doi: 10.1080/03004430.2011.619658
59. *Xu H, Wen LM, Rissel C. Associations of parental influences with physical activity and screen time among young children: a systematic review. J Obes. (2015) 2015:546925. doi: 10.1155/2015/546925
60. *Ling J, Robbins LB, Wen F, Peng W. Interventions to increase physical activity in children aged 2-5 years: a systematic review. Pediatr Exerc Sci. (2015) 27:314–33. doi: 10.1123/pes.2014-0148
61. *Mehtälä MAK, Sääkslahti AK, Inkinen ME, Poskiparta MEH. A socio-ecological approach to physical activity interventions in childcare: a systematic review. Int J Behav Nutr Phys Act. (2014) 11:22. doi: 10.1186/1479-5868-11-22
62. *Ward DS, Vaughn A, McWilliams C, Hales D. Interventions for increasing physical activity at child care. Med Sci Sports Exerc. (2010) 42:526–34. doi: 10.1249/MSS.0b013e3181cea406
63. *Crutzen R. Adding effect sizes to a systematic review on interventions for promoting physical activity among European teenagers. Int J Behav Nutr Phys Act. (2010) 7:29. doi: 10.1186/1479-5868-7-29
64. *Langford R, Bonell CP, Jones HE, Pouliou T, Murphy SM, Waters E, et al. The WHO Health Promoting School framework for improving the health and well-being of students and their academic achievement. Cochrane Lib. (2014) CD00895. doi: 10.1002/14651858.CD008958.pub2
65. *Van Sluijs EMF, McMinn AM, Griffin SJ. Effectiveness of interventions to promote physical activity in children and adolescents: systematic review of controlled trials. BMJ. (2007) 335:703. doi: 10.1136/bmj.39320.843947.BE
66. *World Health Organisation. Interventions on Diet and Physical Activity: What Works: Summary Report. Geneva (2009). Available onlne at: http://www.who.int/dietphysicalactivity/whatworks/en/ (Accessed September 4,2018).
67. *Parrish A-M, Okely A, Stanley R, Ridgers N. The effect of school recess interventions on physical activity. Sports Med. (2013) 43:287–99. doi: 10.1007/s40279-013-0024-2
68. *Quitério ALD. School physical education: the effectiveness of health-related interventions and recommendations for health-promotion practice. Health Educ J. (2013) 72:716–32. doi: 10.1177/0017896912460934
69. *Public Health England. What Works in Schools and Colleges to Increase Physical Activity? A briefing for head teachers, college principals, staff working in education settings, directors of public health and wider partners. London (2015).
70. *Salmon J, Booth ML, Phongsavan P, Murphy N, Timperio A. Promoting physical activity participation among children and adolescents. Epidemiol Rev. (2007) 29:144–59. doi: 10.1093/epirev/mxm010
71. *De Meester F, van Lenthe FJ, Spittaels H, Lien N, De Bourdeaudhuij I. Interventions for promoting physical activity among European teenagers: a systematic review. Int J Behav Nutr Phys Act. (2009) 6:82. doi: 10.1186/1479-5868-6-82
72. *Brennan LK, Brownson RC, Orleans CT. Childhood obesity policy research and practice. Evidence for policy and environmental strategies. Am J Prev Med. (2014) 46:1–16. doi: 10.1016/j.amepre.2013.08.022
73. *Pate RR, Trilk JL, Byun W, Wang J. Policies to increase physical activity in children and youth. J Exerc Sci Fitness. (2011) 9:1–14. doi: 10.1016/S1728-869X(11)60001-4
74. *Waters E, De Silva-Sanigorski A, Burford BJ, Brown T, Campbell KJ, Gao Y, et al. Interventions for preventing obesity in children. Cochrane Database Syst Rev. (2011) CD001871. doi: 10.1002/14651858.CD001871.pub3
75. *Lonsdale C, Rosenkranz RR, Peralta LR, Bennie A, Fahey P, Lubans DR. A systematic review and meta-analysis of interventions designed to increase moderate-to-vigorous physical activity in school physical education lessons. Prev Med. (2013) 56:152–61. doi: 10.1016/j.ypmed.2012.12.004
76. *Dudley D, Okely A, Pearson P, Cotton W. A systematic review of the effectiveness of physical education and school sport interventions targeting physical activity, movement skills and enjoyment of physical activity. Eur Phys Educ Rev. (2011) 17:353–78. doi: 10.1177/1356336X11416734
77. *Dobbins M, De Corby K, Robeson P, Husson H, Tirilis D. School-based physical activity programs for promoting physical activity and fitness in children and adolescents aged 6-18. Cochrane Database Syst Rev. (2009) CD007651. doi: 10.1002/14651858.CD007651
78. *Dobbins M, Husson H, DeCorby K, LaRocca RL. School-based physical activity programs for promoting physical activity and fitness in children and adolescents aged 6 to 18. Cochrane Database Syst Rev. (2013) 2:CD007651. doi: 10.1002/14651858.CD007651.pub2
79. *Barr-Anderson DJ, Auyoung M, Whitt-Glover MC, Glenn BA, Yancey AK. Integration of short bouts of physical activity into organizational routine: a systematic review of the literature. Am J Prev Med. (2011) 40:76–93. doi: 10.1016/j.amepre.2010.09.033
80. *Atkin A, Gorely T, Biddle S, Cavill N, Foster C. Interventions to promote physical activity in young people conducted in the hours immediately after school: a systematic review. Int J Behav Med. (2011) 18:176–87. doi: 10.1007/s12529-010-9111-z
81. *Beets MW, Beighle A, Erwin HE, Huberty JL. After-school program impact on physical activity and fitness. A meta-analysis. Am J Prev Med. (2009) 36:527–37. doi: 10.1016/j.amepre.2009.01.033
82. *Broekhuizen K, Scholten AM, De Vries SI. The value of (pre)school playgrounds for children's physical activity level: a systematic review. Int J Behav Nutr Phys Act. (2014) 11:59. doi: 10.1186/1479-5868-11-59
83. *Escalante Y, García-Hermoso A, Backx K, Saavedra JM. Playground designs to increase physical activity levels during school recess: a systematic review. Health Educ Behavior. (2014) 41:138–44. doi: 10.1177/1090198113490725
84. *Naylor PJ, Nettlefold L, Race D, Hoy C, Ashe MC, Wharf Higgins J, et al. Implementation of school based physical activity interventions: a systematic review. Prev Med. (2015) 72:95–115. doi: 10.1016/j.ypmed.2014.12.034
85. *Van Lippevelde W, Verloigne M, De Bourdeaudhuij I, Brug J, Bjelland M, Lien N, et al. Does parental involvement make a difference in school-based nutrition and physical activity interventions? A systematic review of randomized controlled trials. Int J Public Health. (2012) 57:673–8. doi: 10.1007/s00038-012-0335-3
86. *Chillón P, Evenson KR, Vaughn A, Ward DS. A systematic review of interventions for promoting active transportation to school. Int J Behav Nutr Phys Act. (2011) 8:10. doi: 10.1186/1479-5868-8-10
87. *Larouche R, Saunders TJ, Faulkner G, Colley R, Tremblay M. Associations between active school transport and physical activity, body composition, and cardiovascular fitness: a systematic review of 68 studies. J Phys Activ Health. (2014) 11:206–27. doi: 10.1123/jpah.2011-0345
88. *van Grieken A, Ezendam NPM, Paulis WD, van der Wouden JC, Raat H. Primary prevention of overweight in children and adolescents: a meta-analysis of the effectiveness of interventions aiming to decrease sedentary behaviour. Int J Behav Nutrition Phys Activ. (2012) 9:61. doi: 10.1186/1479-5868-9-61
89. *Cushing CC, Brannon EE, Suorsa KI, Wilson DK. Systematic review and meta-analysis of health promotion interventions for children and adolescents using an ecological framework. J Pediatr Psychol. (2014) 39:949–62. doi: 10.1093/jpepsy/jsu042
90. *Hamel LM, Robbins LB, Wilbur J. Computer- and web-based interventions to increase preadolescent and adolescent physical activity: a systematic review. J Adv Nurs. (2011) 67:251–68. doi: 10.1111/j.1365-2648.2010.05493.x
91. *Hillier-Brown FC, Bambra CL, Cairns JM, Kasim A, Moore HJ, Summerbell CD. A systematic review of the effectiveness of individual, community and societal level interventions at reducing socioeconomic inequalities in obesity amongst children. BMC Public Health. (2014) 14:834. doi: 10.1186/1471-2458-14-834
92. *Kamath CC, Vickers KS, Ehrlich A, McGovern L, Johnson J, Singhal V, et al. Behavioral interventions to prevent childhood obesity: a systematic review and metaanalyses of randomized trials. Endocr Soc. (2008) 93:4606–15. doi: 10.1210/jc.2006-2411
93. Brown HE, Atkin AJ, Panter J, Wong G, Chinapaw MJM, van Sluijs EM. Family-based interventions to increase physical activity in children: a systematic review, meta-analysis and realist synthesis. Obesity Rev. (2016) 17:345–60. doi: 10.1111/obr.12362
94. McGoey T, Root Z, Bruner MW, Law B. Evaluation of physical activity interventions in youth via the reach, efficacy/effectiveness, adoption, implementation, and maintenance (RE-AIM) framework: a systematic review of randomised and nonrandomized trials. Prev Med. (2015) 76:58–67. doi: 10.1016/j.ypmed.2015.04.006
95. McGoey T, Root Z, Bruner MW, Law B. Evaluation of physical activity interventions in children via the reach, efficacy/effectiveness, adoption, implementation, and maintenance (RE-AIM) framework: a systematic review of randomized and non-randomized trials. Prev Med. (2016) 82:8–19. doi: 10.1016/j.ypmed.2015.11.004
96. Rowan B, Miskel B. Institutional theory and the study of educational organisations. In: Murphy J, Louis KS, editors. Handbook of Research in Educational Administration. San Francisco, CA: Jossey-Bass (1999). p. 359–84.
97. Basic Law for the Federal Republic of Germany (Grundgesetz) (1949) Art. 30. Available online at: http://www.gesetze-im-internet.de/gg/art_30.html
98. Conference of Education Ministers Ministers. Sport. (2017). Available online at: https://www.kmk.org/themen/sport.html (Accessed December 7, 2017).
99. Hungarian School Sport Federation HSS. Netfit (2017). Available online at: http://www.mdsz.hu/en/netfit-2/about-netfit/ (Accessed December 7, 2017).
100. Conference of Education Ministers. Neue KMK-Statistik für Ganztagsschulen 2015/2016. Available online at: https://www.ganztagsschulen.org/de/19001.php (Accessed December 7, 2017).
101. Abu-Omar K, Messing S, Sarkadi-Nagy E, Kovács VA, Brukało K, Hassapidou M, et al. Barriers, facilitators and capacities for childhood obesity prevention in 12 European nations: results of a policy-maker survey. Public Health Panorama. (2018) 4:360–7. doi: 10.1186/s12889-018-6368-7
102. Rütten A, Pfeifer K. National Recommendations for Physical Activity and Physical Activity Promotion. Erlangen: FAU University Press (2016).
103. European Project Getting Evidence into Practice. European Quality Instrument for Health Promotion (EQUIHP). (2005). Available online at: http://ec.europa.eu/health/ph_projects/2003/action1/docs/2003_1_15_a10_en.pdf (Accessed September 4, 2018).
104. Horodyska K, Luszczynska A, van den Berg M, Hendriksen M, Roos G, De Bourdeaudhuij I, et al. Good practice characteristics of diet and physical activity interventions and policies: an umbrella review. BMC Public Health. (2015) 15:1–16. doi: 10.1186/s12889-015-1354-9
105. Marques AI, Santos L, Soares P, Santos R, Oliveira-Tavares A, Mota J, et al. A proposed adaptation of the European Foundation for Quality Management Excellence Model to physical activity programmes for the elderly - development of a quality self-assessment tool using a modified Delphi process. Int J Behav Nutr Phys Act. (2011) 8:1–9. doi: 10.1186/1479-5868-8-104
106. Stirman SW, Kimberly J, Cook N, Calloway A, Castro F, Charns M. The sustainability of new programs and innovations: a review of the empirical literature and recommendations for future research. Implement Sci. (2012) 7:17. doi: 10.1186/1748-5908-7-17
107. BZgA. Qualitätskriterien für Maßnahmen der Gesundheitsförderung und Primärprävention von Übergewicht bei Kindern und Jugendlichen. In: Gesundheitsförderung konkret, Band 13. Cologne: Bundeszentrale für gesundheitliche Aufklärung (2010). Available online at: https://www.bzga.de/infomaterialien/fachpublikationen/fachpublikationen/band-13-qualitaetskriterien-fuer-massnahmen-der-gesundheitsfoerderung-und-primaerpraevention-von-uebergewi/
108. Messing S, Rütten A. Qualitätskriterien für die Konzipierung, Implementierung und evaluation von interventionen zur bewegungsförderung: ergebnisse eines state-of-the-art reviews. Das Gesundheitswesen. (2017) 79(Suppl. 1):S60–5. doi: 10.1055/s-0042-123378
*^The 39 reviews on which our systematic reviews of reviews is based are indicated with an asterisk in the reference list.
Keywords: physical activity, children, adolescents, review, family, childcare, family, recommendations
Citation: Messing S, Rütten A, Abu-Omar K, Ungerer-Röhrich U, Goodwin L, Burlacu I and Gediga G (2019) How Can Physical Activity Be Promoted Among Children and Adolescents? A Systematic Review of Reviews Across Settings. Front. Public Health 7:55. doi: 10.3389/fpubh.2019.00055
Received: 20 December 2017; Accepted: 25 February 2019;
Published: 19 March 2019.
Edited by:
Harshad Thakur, Tata Institute of Social Sciences, IndiaReviewed by:
Daniel Martinez Garcia, EveryWhere Schools, SpainCopyright © 2019 Messing, Rütten, Abu-Omar, Ungerer-Röhrich, Goodwin, Burlacu and Gediga. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Sven Messing, c3Zlbi5tZXNzaW5nQGZhdS5kZQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.