 Pierre P. M. Thomas1*
Pierre P. M. Thomas1* Ramesh R. Allam2Elena Ambrosino1Jelena Malogajski3Jonathan A. Lal4
Ramesh R. Allam2Elena Ambrosino1Jelena Malogajski3Jonathan A. Lal4 Servaas A. Morré1,4,5
Servaas A. Morré1,4,5 Remco P. H. Peters6,7
Remco P. H. Peters6,7- 1Department of Genetics and Cell Biology, Faculty of Health, Medicine and Life Sciences, Institute for Public Health Genomics (IPHG), GROW School for Oncology and Developmental Biology, Maastricht University, Maastricht, Netherlands
- 2SHARE India, Hyderabad, India
- 3Department of Public Health, School of Health Professions, Long Island University, Brooklyn, NY, United States
- 4Department of Molecular and Cellular Engineering, Jacob Institute of Biotechnology and Bioengineering, Sam Higginbottom University of Agriculture, Technology and Sciences, Allahabad, India
- 5Laboratory of Immunogenetics, Department of Medical Microbiology and Infection Control, VU University Medical Center, Amsterdam, Netherlands
- 6Clinical Care and Research, Anova Health Institute, Johannesburg, South Africa
- 7Department of Medical Microbiology, CAPHRI School for Public Health and Primary Care, Maastricht University, Maastricht, Netherlands
Chlamydia trachomatis is the world's most prevalent bacterial Sexually Transmitted infection (STI). It is associated with a wide range of health consequences and sequelae in both the short and long term. Enhanced control of urogenital C. trachomatis infection is particularly important in low- and middle-income countries such as India, where most of the burden goes unnoticed and where limited systematic data is available to gauge the current situation. The World Health Organization (WHO) recently issued its latest strategy on STIs, which is aligned with the achievement of the Sustainable Development Goals (SDGs). Taking the WHO framework into account; this paper puts forward an integrated care model to strengthen the management and control of C. trachomatis in India. The model is compiled of five key components of STI management (awareness, prevention diagnosis, treatment and follow-up). The model considers barriers to effective C. trachomatis control into account. The barriers are discussed and compiled into different categories. A roadmap for the implementation of other similar models to enhance C. trachomatis control in the future is provided.
Introduction
The World Health Organization's (WHO) strategy for sexually transmitted infection (STI) control is summarized in the “Global health sector strategy on Sexually Transmitted Infections (STIs) 2016-2021, toward ending STIs” (1). The strategy is aligned with the Sustainable Development Goals (SDGs) which builds upon the Millennium development Goals (MDGs) and offer the layout for better and more sustainable future for all the countries in the world (2). The focus on sexual and reproductive health has become stronger in the SDGs compared with the MDGs (3). The WHO STI strategy addresses several SDGs, including the 3rd goal of good health and wellbeing, the 5th goal of gender equality and the 10th aiming at reducing inequalities (4). The WHO STI strategy is structured around five strategic directions aimed at ending STI epidemics as major public health concerns (Table 1).
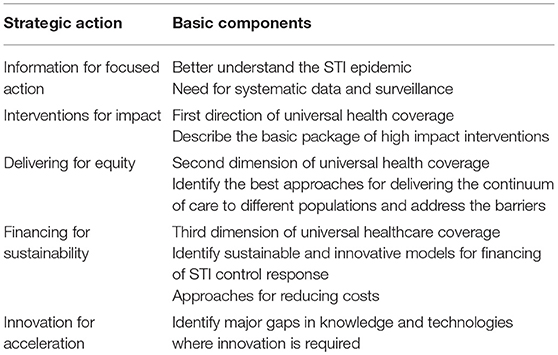
Table 1. Strategic directions of WHO strategy on STIs.
The main focus of the strategy is on Neisseria gonorrhoeae to prevent and stop spread of drug-resistance, Treponema pallidum (prevention of congenital syphilis) and on HPV (reducing cancer-associated mortality). Chlamydia trachomatis infection, with an estimated >130 million incident cases worldwide, is recognized as important, but the WHO strategy suggests that there is a lack of efficient interventions to successfully address the global burden of C. trachomatis (1, 5, 6).
Chlamydia trachomatis infection has a significant impact on sexual, reproductive, maternal and child health. The infection is relatively easily treated with antibiotics (azithromycin and/or doxycycline) that are widely available, even in resource-constrained LMICs (7). Despite the availability of antibiotics many healthcare barriers exist to successful management and control of genital C. trachomatis infections in LMICs such as India. Additionally, the implementation of routine diagnosis and syndromic management has not succeeded in effectively addressing the burden. In this paper we discuss current C. trachomatis control efforts in India and propose an integrated approach aimed at strengthening health service provision to be inclusive of C. trachomatis infections in the Indian setting to include comprehensive care for C. trachomatis.
The Burden of Chlamydia trachomatis Infection in India
India is home to an ethnically diverse population of over one billion inhabitants and to one of the most significant burdens of infectious diseases worldwide. The healthcare system is split between the public healthcare sector, catering to lower-income populations and the private sector mostly utilized by high-income populations (8, 9). It was estimated in 2005–2006 that the private healthcare sector ranks as the first provider of care for 70% of urban and 63% of rural homes respectively (10). There is a large difference in quality of healthcare with the lowest quality of care generally provided in rural public healthcare settings (11). High maternal and child mortality rates emphasizing this large divide (12).
India does not have a surveillance system for STIs other than HIV and there are limited data available with regards to the burden of C. trachomatis infections and its impact on health. A recently published (2017) systematic literature identified a limited number (n = 27) of studies that assessed the prevalence of C. trachomatis in India, with large heterogeneity in terms of prevalence reported and population groups included (13). It should be furthermore stressed that major differences exist within India regarding the genetic makeup of the populations, as well as the functioning of the healthcare system at the state level. All these factors can have in impact of the STI situation. There is no clear overall estimate of C. trachomatis prevalence in the Indian population, but studies did show a high prevalence of C. trachomatis infection among symptomatic women presenting with vaginal discharge at the outpatient department. Much lower prevalence rates were observed in a community-based sample of Indian women (14, 15). High prevalence of infection (up to 15% based on PCR testing) as well as seroprevalence (up to over 60% using ELISA based serology) is reported for women consulting for sub-fertility, confirming the established link between C. trachomatis infection and sub-fertility in the Indian setting (16–21).
India has implemented syndromic case management of STI in the public health sector. This means that individuals with specific symptoms are treated empirically with a combination of antibiotics (22). Currently, vaginal and urethral discharge, the main clinical presentations of C. trachomatis infection, is treated with a combination of azithromycin and cefixime. An important limitation of the syndromic approach, in particular in case of C. trachomatis, is that asymptomatic infections, so over 80% of all infections, remain untreated. This puts a large number of individuals at risk for long-term sequelae associated with this infection. A recent study from India highlights the poor results of syndromic management as well as its link to over-prescription of antimicrobials and to antimicrobial resistance (23). These findings are corroborated by studies from other developing countries, such as South Africa (24).
Untreated C. trachomatis infections, presenting with or without symptoms, may impact on individual's health through in various ways (Figure 1).
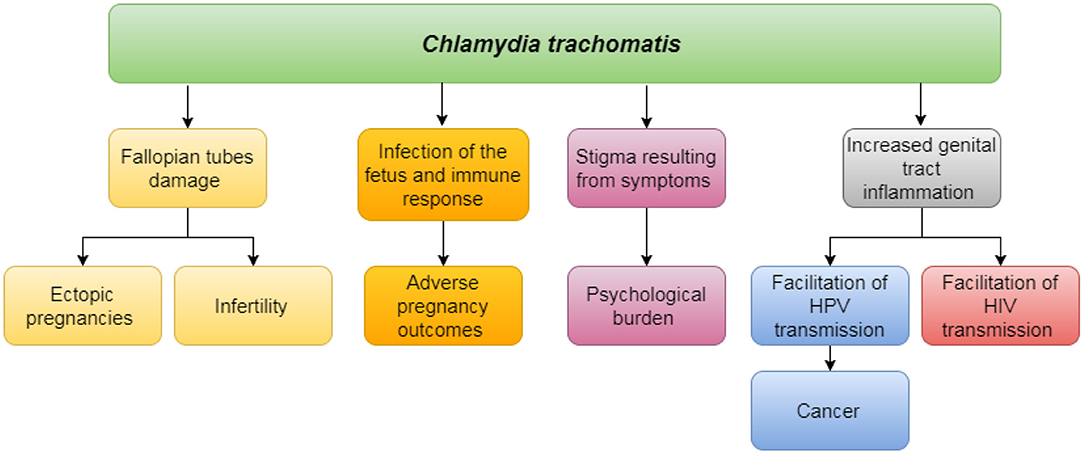
Figure 1. Impact of untreated Chlamydia trachomatis on individual's health.
Untreated chlamydial infections may evolve into Reproductive Tract Infections (RTIs), which may lead to tubal factor infertility and pelvic inflammatory disease and increased risk of ectopic pregnancy in women (and subsequent morbidity and mortality) (25–28). Chlamydia trachomatis may directly impact pregnancy outcomes, through causing spontaneous abortion and stillbirth, may also result in pre-term labor associated with poor outcomes of neonates (29, 30). Genital tract inflammation facilitates transmission and acquisition of HIV and possibly human papilloma virus (HPV) infection. Finally, there is a significant psychological burden associated with STIs in general, including C. trachomatis. Impact on sexual pleasure may negatively affect the individual's sexual health, as well as, relationships. Perceived internal and external stigma and discrimination impact general well-being, especially in conservative societies such as in India (31, 32). The challenge here is that, in the absence of diagnostic texting, these symptoms associated with STI may just as well be caused by any other, not sexually transmitted, infection (33).
Current Initiatives and Barriers to Chlamydia trachomatis Control in India
The current situation of STI care in India is challenging: Patients have to circumnavigate across a wide range of providers, both public and private due to the fragmentation of the healthcare delivery system (34). Out-of-pocket expenditures and informal payments are common and constitute a further barrier to patients accessing care (35, 36). The current system put forward by the Government of India is centered around a referral chain where several actors with different roles are active. The referral chain is featured in the diagram below, along with the key actors at each step (Figure 2).
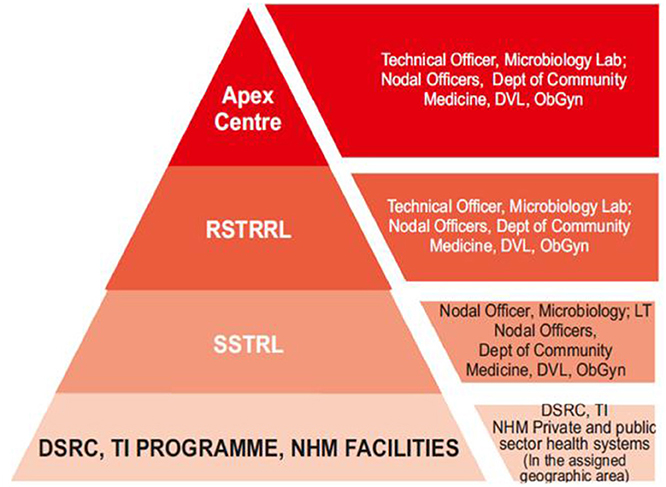
Figure 2. Levels of STI care in India including key actors, adapted from the operational guidelines of the Government of India.
STI clinics and healthcare settings, such as Gynecology and Obstetrics Outpatient departments (OPD) that see patients for these conditions constitute the lowest echelon of the referral chain. The current policy stipulates that syndromic management should be applied to patients presenting with symptoms indicative of STIs, based on pre-defined algorithms. The strategy however encourages laboratory testing whenever it is available. The task of identification and testing of samples gathered at the previously outlined level is the role of the regional and state level laboratories (RSRTL and SSRTl, respectively). These entities should avail the necessary equipment to identify different STIs, including chlamydia and gonorrhea, using PCR or other tests. The regional and state laboratories are also conjointly in charge of monitoring etiological trends and to test for sensitivity to drugs on the samples obtained from public and private STI testing sites. They then ought to report their findings, in order to update syndromic management algorithms when necessary and inform patient treatment (37, 38). The current STI control policy warrants special attentions for core and high-risk groups, as well as, for cases of re-infection and/or treatment failure (22). These activities are overseen at the country level by the national Apex laboratory, located at Safdarjang Hospital in New Delhi which is in charge of overseeing all of the activities related to STI testing and control. There are additional activities undertaken by the government of India aimed at addressing the burden of STIs. A recent project aimed at the eradication of congenital syphilis is also currently in progress and mainly targets pregnant women. In spite of these efforts and endeavors, challenges toward sound management of C. trachomatis and other STIs remain. One of the main hurdles is the lack of awareness on SRH-related topic within Indian communities, particularly among youths (39). Cultural and traditional factors also impact negatively on STI control. The conservative cultural beliefs of Indian communities are not benevolent toward the use of STI services particularly among young women (40). Also, there is limited awareness surrounding issues of STIs, and knowledge about STIs other than HIV is low (41, 42). Gender inequality is similarly a compounding factor for both risk and perceived risk of contracting an STI among married women (43, 44). Lack of knowledge of sexual and reproductive health issues among men has also been put forward (45).
The various barriers to accessing services to address C. trachomatis infection in India are summarized below (Table 2). These are divided in barriers linked to culture and education and barriers inherent to logistics and resources.
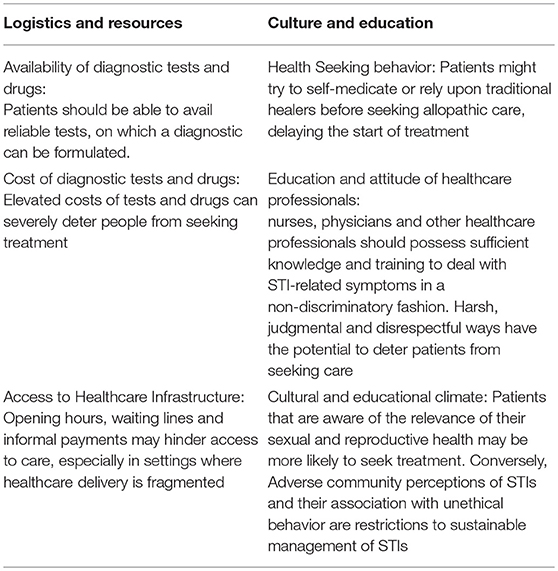
Table 2. Barriers to Chlamydia trachomatis control.
An Integrated Model to Improve Chlamydia trachomatis Care
One of the important aspects highlighted in the WHO strategy is the implementation of a continuum of care, while adopting a holistic approach, aimed at tackling the important driving forces behind the spread of STIs including C. trachomatis. Integrated care is a conceptual framework that conceptualizes the idea of continuum of care theorized in the WHO strategy. It is defined as “The management of health services so that people get the care they need, when they need it in ways that are user-friendly, achieved desired results and provide value for money” (46). Important objectives of integrated care are streamlining the provision of services and to help the patients navigate the delivery of care with simplicity. Such an approach would be appropriate to the Indian setting, where healthcare provision is scattered and informal payments are common (34–36). An integrated approach would facilitate access to care, especially for women and in a context of stigma and discrimination (47). Finally, the integrated approach would promote improvement of clinical practices and prudent use of antibiotics, even in settings where STIs are treated syndromically (48, 49). Furthermore, the previously outlined levels of STI care in India constitutes a valid point of entry for the implementation of an integrated care model aimed at C. trachomatis control and management. This is further supported by the fact that the current strategy aims at bridging the gap between public and private healthcare delivery and management of C. trachomatis treatment. Disease control can in fact be integrated at several levels of the healthcare delivery system. Although there are no accounts of integrated care specifically directed at C. trachomatis, there are many accounts of integration of STI services in primary care (50). In such case, healthcare professionals may raise awareness and provide diagnostic testing for STIs, including C. trachomatis, as part of their routine package of care. The screening program for HIV and syphilis among pregnant women also constitutes a valid opportunity for integration of C. trachomatis diagnosis and management during the same clinic visit, as the chlamydial infections may negatively impact on pregnancy outcomes and neonatal health (51).
Based on the theoretical strengths of an integrated model, in line with the WHO strategy, and the barriers and limitations to C. trachomatis discussed in the previous paragraph, we propose such an integrated model for continuum of care to improve C. trachomatis control in India (Figure 3) (52, 53). The five key components in this model are awareness, prevention, diagnosis, treatment and follow-up. These are linked to factors that influence their delivery and implementation. These components constitute the strategic step in sound C. trachomatis management, as all of these steps allow for each infection to be detected, treated and further spread of the infection. They allow patients to benefit from an evidence-based approach and to be empowered in the face of a set of symptoms which may otherwise lead to discrimination. Additionally, this framework emphasizes the links between the different actors, and well as the factors that contribute to the success of such a model and presents an opportunity for an ongoing feedback loop for quality improvement. The combination of these tasks may however result in additional workload for the care personnel. Performing each of these actions moreover necessitates logistic efforts in order to ensure the functioning of the model. This requires political commitment to the issue of C. trachomatis, and overall support from the community. The implementation process and delivery of integrated care need to be close monitored as specific interventions and contextual adaptation may be required during the process to achieve success. Also, full commitment of relevant stakeholders is imperative and needs to be brought in from the earliest possible stage of implementation. Many lessons can be drawn from the implementation of integrated care frameworks in other LMICs, such as South Africa. This country has seen integration of STI care at different levels of healthcare delivery, and the results stress the importance of quality monitoring and, evaluation of these projects (54, 55).
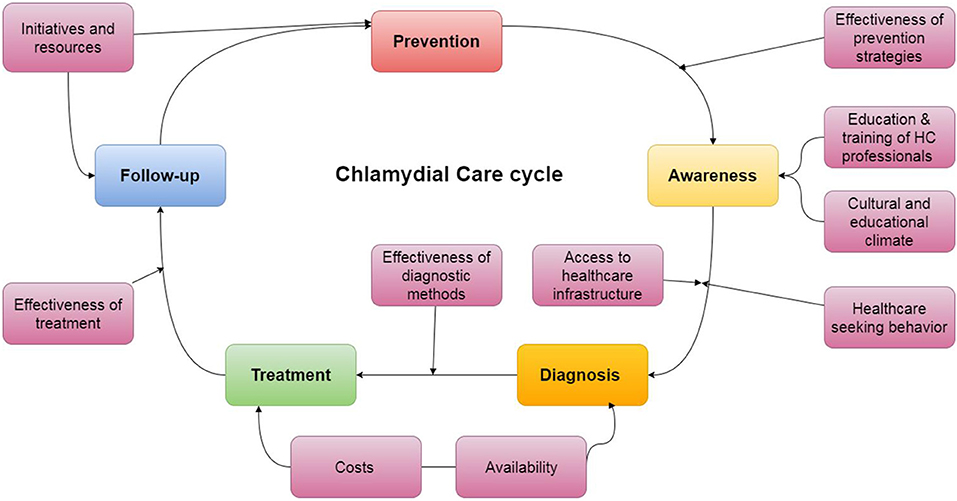
Figure 3. Proposed integrated model to improve Chlamydia trachomatis management and control in India.
Steps for the Future
STIs including C. trachomatis often fail to get much attention and resources from health policy makers to effectively deal with the burdens of infection in developing countries, such as India. To allow for more specific discussions to improve C. trachomatis control, a clear implementation plan with timeframe is required. We propose a tentative set of goals based on current state of research, translation and implementation to improve C. trachomatis control in Indian in the next 20 years (Figure 4).
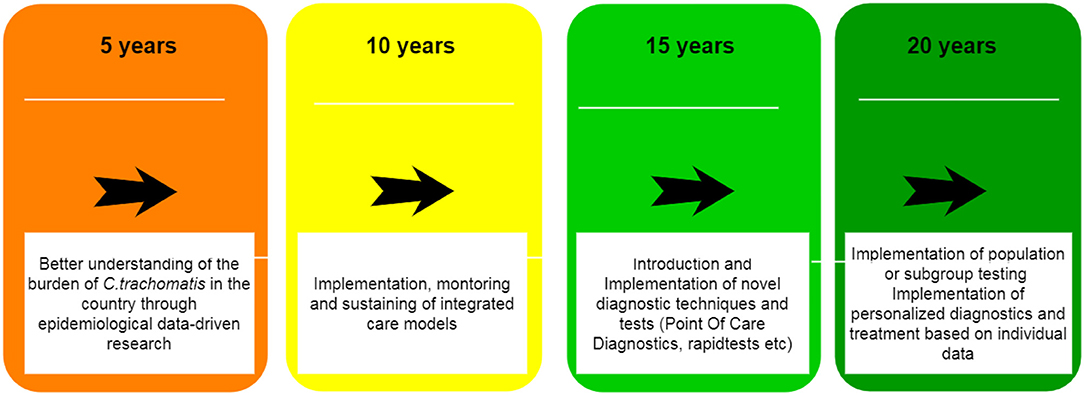
Figure 4. A roadmap to improve Chlamydia trachomatis management and control in India over the next 20 years.
The first important step is to better understand the burden of C. trachomatis infections in India, including specific risk groups in the populations and attributed risk factors. This translates into a need for data at different levels. First a structure for systematic and routine gathering of clinical data should be articulated. This could take the shape of sentinel surveillance of symptoms or clinical cases confirmed in the lab a selection of (a)symptomatic populations. Hospitals and healthcare institutions that are in the possession of databases and biobanks also ought to be encouraged to share their information and potentially open it for research purposes (56). Studies aiming at evaluation incidence and prevalence of the disease in communities and specific population groups (Commercial sex workers, Men who Have sex with Men) should be initiated and supported. The authors have obtained a Dutch grant; acronym “ChlamIndia,” to investigate this and first results will be obtained in the beginning of 2018. Data on the utilization of specialized sexual and reproductive health care also would need to be gathered. In addition, calls for systematic reviews of the literature and meta-analyses of the existing data ought to be performed. These data are imperative to successful design and implementation of control strategies.
The second step would translate into the implementation of an integrated care model, such as proposed in the previous paragraph. This would have to be accompanied by constant monitoring of performance and quality of implementation of these models and a supported managerial and political climate.
The third step caters for the widespread introduction of diagnostic tests to improve clinical care and to start detecting and addressing the burden of asymptomatic C. trachomatis infections in both public and private sector. Availability of a point-of-care (POC) tests that provide quick result and allow for same-day treatment, instead of shipment of specimens to the laboratory and the need for a return visit to discuss the results, would be highly supportive of this process (57, 58). Such tests are already available for some STIs, yet they presently are still underperforming when compared to international NAAT standards as performed in the laboratory especially for C. trachomatis (59). Self-sampling procedures have also been explored in other LMICs and have helped to reduce the barriers toward testing (60). This technique could also help address issues in the Indian setting.
The final step evolves around the principle of precision medicine and constitutes implementation of individually tailored diagnostic and treatment procedures into routine practice such as Point of Care diagnostics and mobile tools. For example, some molecular variations and single nucleotide proteins have been linked to higher likelihood of infection with C. trachomatis or with the development of its long-term sequelae, such as infertility (61). The implementation of genetic and genomic information into routine clinical practice would enable a precision approach to each single case and every single patient, allowing for the full spectrum of information to be taken into account (62). This would contribute to effectiveness and sustainability of services, while providing an empowering environment for the patients to seek care. Although these principles have great promise, a large part of technical development and improved understanding of microbiological, immunological, and host-genetic factors of C. trachomatis infection is required before this will be the new “standard practice.”
Conclusion
Chlamydia trachomatis is the most prevalent bacterial STIs in the world and it is associated with a wide-range of sequelae. Efforts that support management and control of C. trachomatis infection are imperative to improve health outcomes in Low and Middle Income Countries in line with the Sustainable development goals. The challenges surrounding C. trachomatis control in India that we presented are characteristic for many LMICs. Bold efforts are warranted to address the burden of disease and underlying healthcare, cultural and traditional barriers. We have proposed an innovative integrated model alongside an implementation roadmap that would support enhance C. trachomatis management and control in India. This provides a blueprint for debate that ultimately aims to improve health outcomes in resource limited settings across the globe.
Author Contributions
Primary research and models were developed by PT, under close supervision of RP and SM. The manuscript was compiled by PT and steadily improved based on comments from RP and SM. Further comments and advice on the future steps and precision medicine approach were provided by EA and JM. Advice, and insights from the Indian perspective were provided by JL. Information on the current situation and strategies in India, as well an overview of the current policies was provided by RA.
Funding
This work is supported by the Dutch ChlamIndia Grant (NDBE, The Netherlands): The role of ethnicity and environmental factors for Chlamydia trachomatis infections: differences between Dutch and Indian STD and fertility patients.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The reviewer GS and handling editor declared their shared affiliation at time of review.
References
1. World Health Organization. Global Health Sector Strategy on Sexually Transmitted Infections 2016–2021 Towards Ending STIs. Geneva (2016). Available online at: http://apps.who.int/iris/bitstream/10665/246296/1/WHO-RHR-16.09-eng.pdf (Accessed August 8, 2017).
2. United Nations. Millennium Development Goals. Millenium Development Goals Beyond 2015 (2015). Available online at: http://www.un.org/millenniumgoals/
3. World Health Organization (WHO). Health in 2015: from MDGs, Millennium Development Goals to SDGs, Sustainable Development Goals. World Health Organization (2015) p. 204. Available online at: http://who.int/gho/publications/mdgs-sdgs/en/
5. Newman L, Rowley J, Hoorn SV, Wijesooriya NS, Unemo M, Low N, et al. Global estimates of the prevalence and incidence of four curable sexually transmitted infections in 2012 based on systematic review and global reporting. PLoS ONE (2015) 10:e0143304. doi: 10.1371/journal.pone.0143304
6. World Health Organization. Global Incidence and Prevalence of Selected Curable Sexually Transmitted Infections-2008. World Health Organization (2012). Available online at: http://apps.who.int/iris/bitstream/10665/75181/1/9789241503839_eng.pdf
7. Miller KE. Diagnosis and treatment of Chlamydia trachomatis infection. Am Fam Phys. (2006) 73:1411–6.
8. Gadre A. India's private healthcare sector treats patients as revenue generators. BMJ (2015) 350:h826. doi: 10.1136/bmj.h826
9. Sengupta A. Private health sector in India. BMJ (2005) 331: 1157–8. doi: 10.1136/bmj.331.7526.1157
10. Ministry of Health and Family, Welfare,. India National Family Health Survey (NFHS-3). New Delhi (2007) Available online at: http://dhsprogram.com/pubs/pdf/frind3/frind3-vol1andvol2.pdf (Accessed 2017 10, August).
11. Kumar R, Jaiswal V, Tripathi S, Kumar A, Idris MZ. Inequity in health care delivery in India: the problem of rural medical practitioners. Health Care Anal. (2007) 15:223–33. doi: 10.1007/s10728-007-0060-x
12. Ghosh R. Child mortality in India: a complex situation. World J Pediatr. (2012) 8:11–8. doi: 10.1007/s12519-012-0331-y
13. Thomas P, Spaargaren J, Kant R, Lawrence R, Dayal A, Lal JA, et al. Burden of Chlamydia trachomatis in India: a systematic literature review. Pathog Dis. (2017) 75:ftx055. doi: 10.1093/femspd/ftx055
14. Sood S, Mukherjee A, Bala M, Satpathy G, Mahajan N, Sharma A, et al. A pilot study for diagnosis of genital Chlamydia trachomatis infections by polymerase chain reaction among symptomatic Indian women. Indian J Dermatol Venereol Leprol. (2012) 78:443–7. doi: 10.4103/0378-6323.98074
15. Gupta R, Salhan S, Mittal A. Seroprevalence of antibodies against Chlamydia trachomatis inclusion membrane proteins B and C in infected symptomatic women. J Infect Dev Ctries. (2009) 3:191–8. doi: 10.3855/jidc.35
16. Mania-Pramanik J, Kerkar S, Sonawane S, Mehta P, Salvi V. Current Chlamydia trachomatis infection, a major cause of infertility. J Reprod Infertil. (2012) 13:204–10.
17. Malik A, Jain S, Hakim S, Shukla I, Rizvi M. Chlamydia trachomatis infection & female infertility. Indian J Med Res. (2006) 123:770–5.
18. Malik A, Jain S, Rizvi M, Shukla I, Hakim S. Chlamydia trachomatis infection in women with secondary infertility. Fertil Steril. (2009) 91:91–5. doi: 10.1016/j.fertnstert.2007.05.070
19. Sharma K, Aggarwal A, Arora U. Seroprevalence of Chlamydia trachomatis in women with bad obstetric history and infertility. Indian J Med Sci. (2002) 56:216–7.
20. Ghosh M, Choudhuri S, Ray RG, Bhattacharya B, Bhattacharya S. Association of genital Chlamydia trachomatis infection with female infer-tility, study in a Tertiary Care Hospital in Eastern India. Open Microbiol J (2015) 9:110–6. doi: 10.2174/1874285801509010110
21. Vidwan NK, Regi A, Steinhoff M, Huppert JS, Staat MA, Dodd C, et al. Low prevalence of Chlamydia trachomatis infection in non-urban pregnant women in Vellore, S. India. PLoS ONE (2012) 7:e34794. doi: 10.1371/journal.pone.0034794
22. Government of India. Prevention, Management and Control of Reproductive Tract Infections and Sexually Transmitted Infections. New Delhi (2014). Available online at: http://www.naco.gov.in/upload/2014mslns/National RTI STI technical guidelines Sep2014.pdf (Accessed April 6, 2016).
23. Sonkar SC, Wasnik K, Kumar A, Sharma V, Mittal P, Mishra PK, et al. Evaluating the utility of syndromic case management for three sexually transmitted infections in women visiting hospitals in Delhi, India. Sci Rep. (2017) 7:1465. doi: 10.1038/s41598-017-01422-y
24. Kohler PK, Marumo E, Jed SL, Mema G, Galagan S, Tapia K, et al. A national evaluation using standardised patient actors to assess STI services in public sector clinical sentinel surveillance facilities in South Africa. Sex Transm Infect. (2017) 93:247–52. doi: 10.1136/sextrans-2016-052930
25. Manavi K. A review on infection with Chlamydia trachomatis. Best Pract Res Clin Obstet Gynaecol. (2006) 20:941–51. doi: 10.1016/j.bpobgyn.2006.06.003
26. Haggerty CL, Gottlieb SL, Taylor BD, Low N, Xu F, Ness RB. Risk of sequelae after Chlamydia trachomatis genital infection in women. J Infect Dis. (2010) 201(Suppl. 2):S134–55. doi: 10.1086/652395
27. Baud D, Regan L, Greub G. Emerging role of Chlamydia and Chlamydia-like organisms in adverse pregnancy outcomes. Curr Opin Infect Dis. (2008) 21:70–6. doi: 10.1097/QCO.0b013e3282f3e6a5
28. Mårdh PA. Influence of infection with Chlamydia trachomatis on pregnancy outcome, infant health and life-long sequelae in infected offspring. Best Pract Res Clin Obstet Gynaecol. (2002) 16:847–64. doi: 10.1053/beog.2002.0329
29. Ward H, Rönn M. Contribution of sexually transmitted infections to the sexual transmission of HIV. Curr Opin HIV AIDS (2010) 5:305–10. doi: 10.1097/COH.0b013e32833a8844
30. Silva J, Cerqueira F, Medeiros R. Chlamydia trachomatis infection: implications for HPV status and cervical cancer. Arch Gynecol Obstet. (2014) 289:715–23. doi: 10.1007/s00404-013-3122-3
31. Ekstrand ML, Ramakrishna J, Bharat S, Heylen E. Prevalence and drivers of HIV stigma among health providers in urban India: implications for interventions. J Int AIDS Soc. (2013) 16(3 Suppl. 2). 18717. doi: 10.7448/IAS.16.3.18717
32. Bharat S. A systematic review of HIV/AIDS-related stigma and discrimination in India: current understanding and future needs. SAHARA J. (2011) 8:138–49. doi: 10.1080/17290376.2011.9724996
33. Centers for Disease Control Prevention, Bank, W,. Sexually Transmitted Infections in Developing Countries. Current concepts strategies on improving STI prevention, treatment, control (2008). Available online at: http://siteresources.worldbank.org/INTPRH/Resources/STINoteFINAL26Feb08.pdf
34. Gangolli L V, Duggal R, Shukla A. Review of Healthcare In India. San Francisco, CA: Health (2005).
35. Bhojani U, Thriveni B, Devadasan R, Munegowda C, Devadasan N, Kolsteren P, et al. Out-of-pocket healthcare payments on chronic conditions impoverish urban poor in Bangalore, India. BMC (2012) 12:990. doi: 10.1186/1471-2458-12-990
36. Lewis M. Informal payments and the financing of health care in developing and transition countries. Health Aff. (2007) 26:984–97. doi: 10.1377/hlthaff.26.4.984
38. Ministry of Health & Family Welfare Government of India. Operational Guidelines Strategy. New Delhi (2010). Available online at: http://www.who.int/lep/resources/SEAGLP20062.pdf
39. Grover S, Garg N, Rupali R, Kaur B. Awareness about reproductive health, contraceptive methods, STDs including HIV/AIDS, and HPV vaccine, among adolescent girls in district Faridkot in Punjab. Int J Reprod Contrac Obstet Gynecol. (2017) 6:2003. doi: 10.18203/2320-1770.ijrcog20171966
40. Dwibedi B, Pramanik JM, Sahu P, Kar SK, Moharana T. Prevalence of genital Chlamydia infection in females attending an obstetrics and gynecology out patient department in Orissa. Indian J Dermatol Venereol Leprol. (2009) 75:614–6. doi: 10.4103/0378-6323.57730
41. Hemalatha R, Kumar RH, Venkaiah K, Srinivasan K, Brahmam GN V. Prevalence of & knowledge, attitude & practices towards HIV & sexually transmitted infections (STIs) among female sex workers (FSWs) in Andhra Pradesh. Indian J Med Res. (2011) 134:470–5.
42. Subbarao NT, Akhilesh A. Knowledge and attitude about sexually transmitted infections other than HIV among college students. Indian J Sex Transm Dis AIDS (2017) 38:10–4. doi: 10.4103/0253-7184.196888
43. Jones D, Bagga R, Nehra R, Sethi S, Walia K, et al. Reducing sexual risk behavior among high-risk couples in Northern India. Int J Behav Med. (2013) 20:344–54. doi: 10.1007/s12529-012-9235-4
44. Bloom SS, Agrawal A, Singh KK, Suchindran CM. Gender inequality and the risk of HIV among married couples in North India. AIDS Care. (2015) 27:168–75. doi: 10.1080/09540121.2014.940268
45. Beattie TSH, Bhattacharjee P, Suresh M, Isac S, Ramesh BM, Moses S. Personal, interpersonal and structural challenges to accessing HIV testing, treatment and care services among female sex workers, men who have sex with men and transgenders in Karnataka state, South India. J Epidemiol Commun Health (2012) 66(Suppl. 2):ii42–8. doi: 10.1136/jech-2011-200475
46. World Health Organization. Integrated Care Models: An Overview. Copehagen (2016). Available online at: http://www.euro.who.int/__data/assets/pdf_file/0005/322475/Integrated-care-models-overview.pdf (Accessed August 5, 2017).
47. Vasan A, Ellner A, Lawn SD, Gove S, Anatole M, Gupta N, et al. Integrated care as a means to improve primary care delivery for adults and adolescents in the developing world: a critical analysis of Integrated Management of Adolescent and Adult Illness (IMAI). BMC Med. (2014) 12:6. doi: 10.1186/1741-7015-12-6
48. Mayaud P, Mabey D. Approaches to the control of sexually transmitted infections in developing countries: old problems and modern challenges. Sex Transm Infect. (2004) 80:174–82. doi: 10.1136/sti.2002.004101
49. Vuylsteke B. Current status of syndromic management of sexually transmitted infections in developing countries. Sex Transm Infect. (2004) 80:333–4. doi: 10.1136/sti.2004.009407
50. Church K, de Koning K, Hilber AM, Ormel H, Hawkes S. Integrating sexual health services into primary care: an overview of health systems issues and challenges in developing countries. Int J Sex Health (2010) 22:131–43. doi: 10.1080/19317611003672823
51. Tiller CM. Chlamydia during pregnancy: implications and impact on perinatal and neonatal outcomes. J Obstet Gynecol Neonatal Nurs. (2002) 31:93–8. doi: 10.18203/2320-1770.ijrcog20160867
52. World Health Organization. Integrated Health Services -What and Why? Making Health Systems Work. (2008) Available online at: http://www.who.int/healthsystems/technical_brief_final.pdf (Accessed August 5, 2017).
53. Kodner DL, Spreeuwenberg C. Integrated care: meaning, logic, applications, and implications–a discussion paper. Int J Integr Care (2002) 2:e12. doi: 10.5334/ijic.67
54. Kennedy CE, Haberlen SA, Narasimhan M. Integration of sexually transmitted infection (STI) services into HIV care and treatment services for women living with HIV: a systematic review. BMJ Open (2017) 7:e015310. doi: 10.1136/bmjopen-2016-015310
55. Morikawa E, Mudau M, Olivier D, de Vos L, Joseph Davey D, Price C, et al. Acceptability and feasibility of integrating point-of-care diagnostic testing of sexually transmitted infections into a South African Antenatal Care Program for HIV-Infected Pregnant Women. Infect Dis Obstet Gynecol. (2018) 2018:3946862. doi: 10.1155/2018/3946862
56. Anokwa Y, Hartung C, Brunette W. Open source data collection in the developing world. Computer (2009) 4297–9. doi: 10.1109/MC.2009.328
57. Yager P, Domingo GJ, Gerdes J. Point-of-care diagnostics for global health. Annu Rev Biomed Eng. (2008) 10:107–44. doi: 10.1146/annurev.bioeng.10.061807.160524
58. Caliendo AM, Gilbert DN, Ginocchio CC, Hanson KE, May L, Quinn TC, et al. Better tests, better care: improved diagnostics for infectious diseases. Clin Infect Dis. (2013) 57(Suppl. 3):139–70. doi: 10.1093/cid/cit578
59. Pearce DM, Shenton DP, Holden J, Gaydos CA. Evaluation of a novel electrochemical detection method for Chlamydia trachomatis: application for point-of-care diagnostics. IEEE Trans Biomed Eng. (2011) 58(3 Part 2):755–8. doi: 10.1109/TBME.2010.2095851
60. Jones HE, Altini L, de Kock A, Young T, van de Wijgert JHHM. Home-based versus clinic-based self-sampling and testing for sexually transmitted infections in Gugulethu, South Africa: randomised controlled trial. Sex Transm Infect. (2007) 83:552–7. doi: 10.1136/sti.2007.027060
61. den Hartog JE, Morré SA, Land JA. Chlamydia trachomatis-associated tubal factor subfertility: Immunogenetic aspects and serological screening. Hum Reprod Update (2006) 12:719–30. doi: 10.1093/humupd/dml030
Keywords: Chlamydia trachomatis, sexually transmitted diseases, integrated care, sexual and reproductive health, India
Citation: Thomas PPM, Allam RR, Ambrosino E, Malogajski J, Lal JA, Morré SA and Peters RPH (2018) An Integrated Care Model With Implementation Roadmap to Improve Chlamydia trachomatis Management and Control in India. Front. Public Health 6:321. doi: 10.3389/fpubh.2018.00321
Received: 14 March 2018; Accepted: 22 October 2018;
Published: 09 November 2018.
Edited by:
Marc Jean Struelens, European Centre for Disease Prevention and Control, SwedenReviewed by:
Zisis Kozlakidis, International Agency for Research on Cancer (IARC), FranceGianfranco Spiteri, European Centre for Disease Prevention and Control, Sweden
Copyright © 2018 Thomas, Allam, Ambrosino, Malogajski, Lal, Morré and Peters. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Pierre P. M. Thomas, p.thomas@maastrichtuniversity.nl