
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health, 12 September 2017
Sec. Clinical Diabetes
Volume 5 - 2017 | https://doi.org/10.3389/fpubh.2017.00235
 Shervin Assari1,2*
Shervin Assari1,2* Daniel B. Lee3,4
Daniel B. Lee3,4 Emily Joy Nicklett5
Emily Joy Nicklett5 Maryam Moghani Lankarani1
Maryam Moghani Lankarani1 John D. Piette3,6,7James E. Aikens8
John D. Piette3,6,7James E. Aikens8
Background: A growing body of research suggests that racial discrimination may affect the health of Black men and Black women differently.
Aims: This study examined Black patients with diabetes mellitus (DM) in order to test gender differences in (1) levels of perceived racial discrimination in health care and (2) how perceived discrimination relates to glycemic control.
Methods: A total of 163 Black patients with type 2 DM (78 women and 85 men) provided data on demographics (age and gender), socioeconomic status, perceived racial discrimination in health care, self-rated health, and hemoglobin A1c (HbA1c). Data were analyzed using linear regression.
Results: Black men reported more racial discrimination in health care than Black women. Although racial discrimination in health care was not significantly associated with HbA1c in the pooled sample (b = 0.20, 95% CI = −0.41 −0.80), gender-stratified analysis indicated an association between perceived discrimination and higher HbA1c levels for Black men (b = 0.86, 95% confidence intervals (CI) = 0.01–1.73) but not Black women (b = −0.31, 95% CI = −1.17 to −0.54).
Conclusion: Perceived racial discrimination in diabetes care may be more salient for glycemic control of Black men than Black women. Scholars and clinicians should take gender into account when considering the impacts of race-related discrimination experiences on health outcomes. Policies should reduce racial discrimination in the health care.
Discrimination, defined as differential treatment of members of a group by both individuals and social institutions (1), has adverse effects on physical health (2–5) and mental health (6–12). A particular type of discrimination, racial discrimination, entails targeting racial and ethnic minorities such as Blacks (4, 11, 13–19). In addition, Black men in general (20, 21) report the higher levels of racial discrimination than Black females.
Scientific evidence linking racial discrimination to poor health is overwhelming (13, 22, 23–27). Scholars have attributed this relationship to different mechanisms, including psychological and physiological stress responses (28), unhealthy coping behaviors (4, 29, 30), and lower health care utilization (31, 32). Most of this research has focused on the interpersonal experience of generalized racial discrimination, with less emphasis on perceived discrimination specific to the health care setting (33). At the same time, racial minorities who deny that racism exists are actually at an increased risk for adverse health outcomes (34–36) and lower health care utilization (37).
As patients with diabetes mellitus (DM) have frequent encounters with healthcare facilities, discrimination in the health care setting may be particularly important for racial minority groups with DM (38–40). That is, perceived health care discrimination is associated with worse health outcomes, poorer interpersonal communication with physician, higher hemoglobin A1c (HbA1c) levels, greater number of diabetes symptoms, and poorer physical functioning (39). This effect may be in part due to health behaviors and access to care (41).
Research on discrimination and diabetes is limited (38–40). In one study, DM patients reporting higher levels of healthcare discrimination were less likely to receive HbA1c tests and eye exams (42). In another study, patients with DM who self-reported healthcare discrimination also had lower quality diabetes care (40). Finally, among patients with DM, perceived discrimination was associated with lower quality patient/provider communication and worse glycemic control (39).
Some evidence, mostly derived from community surveys, suggests that gender may modify the effect of perceived discrimination upon health, with a stronger effect for men than women (23, 24, 43–46). Although the mechanisms underlying gender differences in the discrimination and health link is still unknown, masculinity, social hierarchy, and expectation for dominance may have a role (47). Further, even less is known about gender differences in the health effects of perceived racial discrimination in the health care settings. In particular, gender differences in actual and perceived racial discrimination may help explain why discrimination may be more damaging for men than women (47).
The current study had two aims: (1) to investigate gender differences in perceived racial discrimination in health care among Black patients with DM and (2) to compare Black men and women for the relationship between perceived discrimination and patients’ glycemic control. In line with prior documentation that Black men report greater interpersonal discrimination than Black women (48, 47), we expected Black men to experience more perceived discrimination in health care than Black women do. In addition, as considerable evidence suggested that the relation between discrimination and health may be different between men and women (23, 24, 43–45), we expect that perceived health care discrimination would be more strongly associated with glycemic control for Black males than for Black females.
This cross-sectional study was conducted in an outpatient setting in a large Midwestern urban health care system. Data came from the Racial Differences in Diabetes-Depression Comorbidity (RDDDC) study, 2005–2007.
The research protocol followed the tenets of the Declaration of Helsinki. The study protocol was approved by the Institutional Review Board. All participants provided comprehensive written informed consent. Data were kept confidential.
The study used a consecutive sampling strategy. The parent study identified eligible patients from the administrative and clinical databases (23, 49). In order to participate, patients needed to (1) be between 18 and 80 years of age, (2) be ability to complete self-report instruments, (3) have a recorded diagnosis of type 2 DM, and (4) self-identify as either non-Hispanic Caucasian/White or African-American/Black. The current study was limited to the subsample of 163 who identified as Black or African-American. Diagnosis of DM was based on at least one of the following criteria: (1) positive history of hospitalization with a DM-related ICD-9 code (250. x, 357.2, 362.0, or 366.41), (2) two or more outpatient visits with a DM-related ICD-9 code, or (3) prescription for a glucose control medication or monitoring supplies. Use of ICD-9 was the standard practice when the data were collected. The study excluded individuals with type 1 DM through chart review and telephone screening conducted by research staff.
Eligible patients were mailed a study invitation letter followed by a recruitment telephone call from research staff for further screening and enrollment. Data for the present analysis were collected at a single time point.
The study collected data on self-reported age and gender (male vs. female). Socioeconomic status (SES) was assessed using the U.S. Census Bureau Index of SES, adjusted for the regional Consumer Price Index at the time of data collection. Occupation, educational attainment, and income are all related, but none of them by adequately indicates SES. The SES score is based on occupation and educational attainment of the chief income recipient in the family and current family income (50, 51).
Participants rated their own health on a five-point Likert-type scale ranging from “excellent” to “poor.” This single item measure has been widely used in health research, including studies on race, gender, DM, and SRH (43, 44, 52–55). A higher SRH score indicates poorer SRH.
An 8-item modified version of the Chen et al. measure (33) was used to assess patients’ general belief about racism in the health care system, including unfair treatment, poor access to services, low quality of care, and unequal costs. Items are rated using a combination of 3- and 4-point Likert scales, and we calculated the mean score for data analysis. Thus, scores potentially ranged from 1 to 4, with higher scores reflecting greater perceived racial discrimination in health care settings. This measure has been frequently used to measure perceived discrimination in health care and, in our sample, demonstrates good reliability for Black men and women (αOverall = 0.846, αMales = 0.821, αFemales = 0.861).
Table A1 in Appendix shows original items and our modified version. The modification was limited to omitting the only positively worded item “Do you think most African-Americans (Latinos) receive the same quality of health care as whites?” which significantly reduced the reliability of the measure, as all other items measure presence of racism and this item measures lack of racism in the health care.
On the same day that the self-report measures were completed, glycemic control (HbA1c) was evaluated with the DCA 2000 (GMI, Ramsey, MN, USA), which analyzes capillary blood samples through a monoclonal antibody method.
Data were analyzed using Stata 13.0 (Stata Corp., College Station, TX, USA) and Statistical Package for Social Sciences v.20 (SPSS 20). First, we tested normality of distribution of our numerical variables. Descriptive statistics such as means, SDs, and frequencies were used to describe the primary variables. Pearson correlations were examined to assess zero-order correlations. Multivariable linear regression models were used to predict the outcome of HbA1c as a function of perceived racial discrimination. The initial full model included as predictors age, SES, diabetes duration, and insulin. Coefficients were not significant for diabetes duration and insulin (p > 0.05) and were dropped from the final model. The final model included age, gender, and perceived discrimination as predictors of HbA1c. Model 1 only included main effects, and Model 2 included an interaction between gender and perceived discrimination. In secondary analyses, we examined the relationship between discrimination and HbA1c within subsamples of Black men and Black women. Unstandardized beta coefficients, 95% confidence intervals (CI), and p-values were reported. A p-value of 0.05 or less was interpreted as statistically significant.
Table 1 provides descriptive statistics by gender and in the pooled sample. Black men reported significantly higher levels of perceived racial discrimination in health care than Black women did (2.73 ± 0.60 vs. 1.39 ± 0.62, p < 0.05, independent samples t-test). Black men also had higher HbA1c levels on average compared to Black women; however, the difference was not significant (p > 0.05, independent samples t-test). Although Black women had slightly higher education levels than Black men (p > 0.05, independent samples t-test), household income was significantly higher for Black men (82.84 ± 23.80 vs. 67.14 ± 29.86, p < 0.05, independent samples t-test) (Table 1).
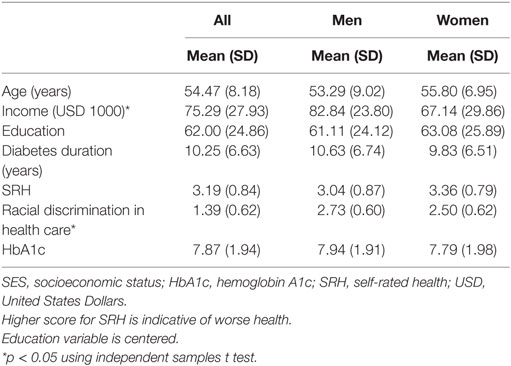
Table 1. Descriptive statistics for pooled and gender-stratified samples.
Table 2 displays zero-order correlations for the pooled and gender-stratified samples. Notably, racial discrimination in health care was associated with HbA1c among Black men but not Black women. Lower age was significantly associated with receiving insulin. Age, education, income, and DM duration were not correlated with HbA1c.
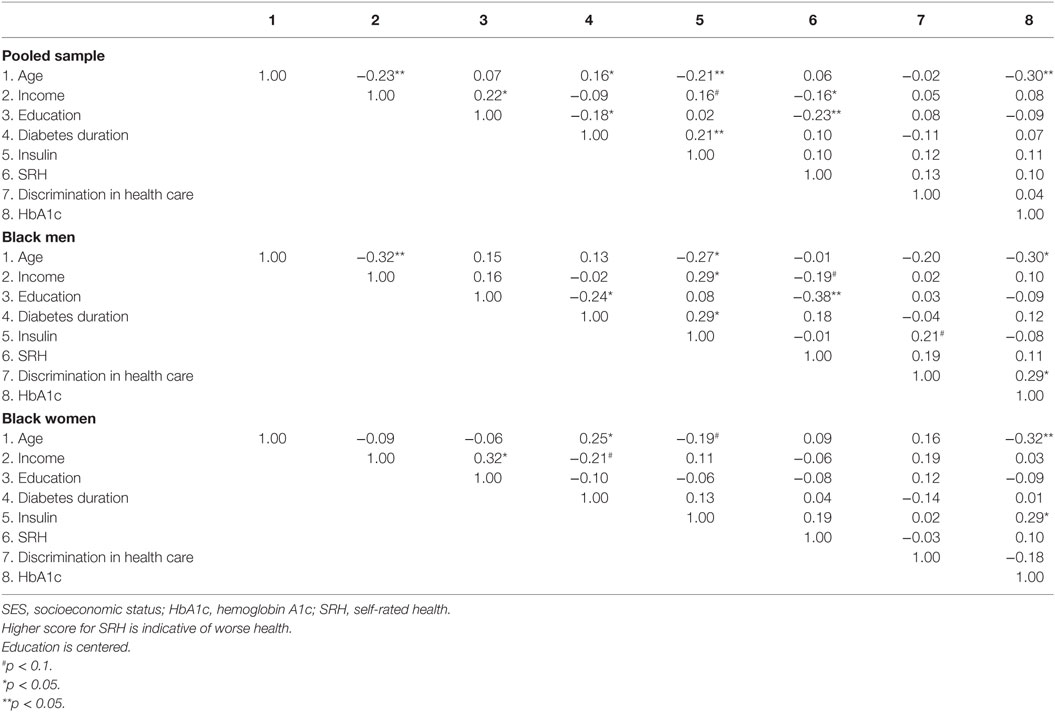
Table 2. Pearson correlations for pooled and gender-stratified samples.
As shown in Table 3, perceived racial discrimination in health care did not have a main effect on HbA1c in the pooled sample (b = 0.20, 95% CI = −0.41 to 0.80). We, however, found a significant interaction between gender and racial discrimination in health care on HbA1c (b = −1.20, 95% CI = −2.40 to 0.00), suggesting a stronger association between racial discrimination in health care and HbA1c for Black men than Black women. Age was significantly and negatively associated with HbA1c in the pooled sample of Blacks (b = −0.08, 95% CI = −0.12 to −0.03).
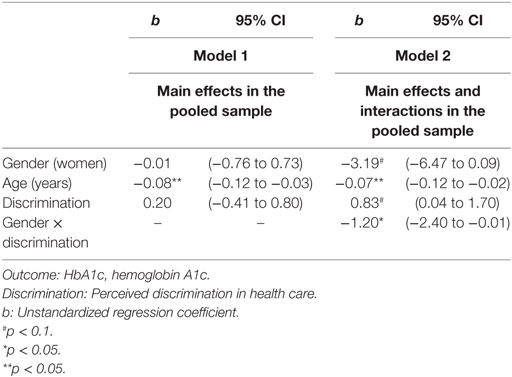
Table 3. Summary of regression analyses in the pooled sample.
Table 4 shows the results of the gender-stratified regression models. Perceived discrimination in health care was positively associated with higher HbA1c for Black men (b = 0.86, 95% CI = 0.00 to 1.73) but not for Black women (b = −0.31, 95% CI = −1.17 to 0.54). Age was significantly and negatively associated with HbA1c in Black women (b = −0.10, 95% CI = −0.18 to −0.01). Although in the same direction, the association between age and HbA1c was marginal in Black men (b = −0.05, 95% CI = −0.11 to 0.01).
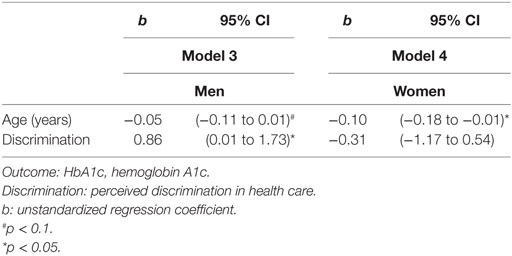
Table 4. Summary of gender-stratified regression models.
We found that among Black DM patients, men reported more racial discrimination in health care settings than women did. Our findings also suggest that perceived health care discrimination is associated with poorer glycemic control among Black men, but not among Black women. These findings collectively indicate the importance of incorporating the interplay between race and gender when considering the health consequences of discrimination.
Our first finding is consistent with prior research that delineates the gendered nature of racial discrimination experience in the lives of Blacks (20, 21). Similar findings have been reported in other contexts such as general population (56–61). Among Blacks, male children and adolescents receive more racial socialization messages that prepare them for these race-related encounters (62–64). Gendered racial socialization, in turn, may result in gender differences in race-related attitudes, identity, and experiences later in life (65, 66). As a result, Black men may be more aware of racism and discrimination across multiple settings (e.g., school, work, health care).
Our second finding, the stronger association between perceived discrimination and glycemic control for Black men than Black women, is also supported by the literature (24, 67, 68). In a study on young Black adults, racial discrimination was associated with depression and anxiety symptoms among males but not females (67). Similarly, a prior study of Arab American adults showed that discrimination was strongly associated with psychological distress among males, but not among females (24).
These findings suggest that Black men and Black women may differently cope with environmental stressors, including discrimination and neighborhood stress. While environmental stressors such as discrimination better predict depression for Black men than for Black women (68–70), neighborhood stress and fear of violence have shown to have stronger effects on obesity for Black women than men (68, 71, 72). This gender-specific health consequences of environmental stressors may be due to Black men’s and women’s tendency to use substances (e.g., alcohol use) and over-eat in response to environmental stress (28, 73). Gender differences in coping (74–76) are also well documented.
There have been two primary explanations offered for the finding that Black men report higher rates of discrimination than Black women (20, 21). The first explanation, called the subordinate male target hypothesis, argues that Black men are subject to more experiences of discrimination (47). The second explanation attributes males’ higher perceived discrimination to measurement bias (47, 77). Ifatunji and Harnois (47) found that subordinate male hypothesis (i.e., that subordination is causing more distress for men than women) explains the gender gap in everyday discrimination.
We tested gender as an effect modifier for the hypothesized effects on glycemic control of perceived discrimination. Prior work suggests that discrimination is more strongly associated with health outcomes for men than for women (24, 45). Moreover, even among men, hejamonic and traditional masculine ideologies may alter how discrimination shapes health (78–80). This suggests that masculine beliefs may explain why Black men report more discrimination in health care setting than women. In addition to gender and masculinity, education (22), social class (81), racial attribution (82), and racial identity (4, 83–85) also probably influence the association between discrimination and health outcomes.
Our findings, which reveal gender differences in the deleterious effect of racial discrimination in health care settings for Blacks with DM, have valuable research and clinical implications. Clinically, racial discrimination in the health care system should be considered as a structural risk factor with health implications for Blacks, particularly Black men. Preventive interventions to address racial discrimination in health care settings should be considered a strategic goal toward elimination of health disparities. Cultural competency training for health care providers is just one of many ways to reduce social inequities in health outcomes (86–91).
Despite the fact that racial disparities in health outcomes and self-care behaviors among adults with type 2 DM is well known (80), little is known regarding the mechanisms behind such racial differences in DM outcomes. The present findings extend this limited understanding by characterizing gender differences within Blacks. Based on our findings, racial discrimination against Blacks particularly Black men may play an important role for DM outcomes.
Current finding that male Black patients with type 2 DM perceive more racial discrimination in health care settings than Black women with the same condition, and perceived racial discrimination in health care settings has an impact in Black men’s overall glycemic control has policy and clinical implications for reducing racial disparities in DM outcomes. The link between the perception of racial discrimination and the poor glycemic control is in line with previous reports on associations between depression and psychological distress and glycemic control (49, 92). Findings are relevant as racial disparities exist in DM outcomes particularly for Blacks (93, 94).
Additional research is needed to understand how racial discrimination in health care settings influences the health care utilization and self-care of Black men. Future research should explore the role of class, masculinity, maladaptive coping, health behaviors, health care use, medication adherence, mental health, racial attribution, and racial identity to explain why Black men are more vulnerable to health consequences of discrimination. Future research should also investigate how exposure to the full spectrum of discrimination influences health of Blacks. Researchers should also direct efforts and resources toward understanding system level determinants of discrimination as experienced by Black patients in health care systems. This study, alongside others (95, 96), suggests that Black men are particularly sensitive to discrimination encounters in health care settings. By cultivating a body of research that reflects racial discrimination in health care settings, scholars and policy makers will be able to design effective policies and interventions to reduce individual- and structural-level discrimination within and beyond the health care setting.
This study is subject to a number of limitations. First, due to a cross-sectional design, we cannot interpret the observed associations as causal in nature. Second, mental health and depression were not measured, which could be confounders or underlying mechanisms for the link between perceived discrimination and glycemic control. Future research should replicate this study using a wider breadth of explanatory factors such as coping, racial identity, health care use, and satisfaction with care. Third, we did not measure frequency of exposure to discrimination and only perceived discrimination and racism in health care. Fourth, although Blacks face similar challenges at least in several other countries in the world, the history of slavery in the United States makes U.S. different from other countries regarding Blacks historical experience of racism and discrimination. U.S. health care system is also different from many other countries. As a result, it is not clear whether the results are generalizable to Blacks living in other countries. Despite these limitations, the study used an innovative conceptual model of discrimination and health that contributes to the growing body of research on racial health disparities.
In summary, we found that among Black patients with DM, men perceived more racial discrimination in health care settings than women and suffered in their glycemic control as a result. The findings from this study highlight the potential deleterious effects of discrimination health care settings as a pathway linking of racial disparities to health outcomes. To identify these methods, however, future research should focus on identifying potential mechanisms (e.g., patient–provider interactions, language, and class) that may further explain the link between racial discrimination and health. Anti-racist societal actions and anti-discrimination policies are needed in order to achieve more social equality.
The University of Michigan Institutional Review Board approved the study protocol for all years of data collection and all participants provided consent for participation in the study.
This analysis was designed and performed by SA, who also contributed to drafts of the manuscript. JP and JA designed the main study, acquired the data, and contributed to all drafts of this manuscript. DL and EN also contributed to the drafts and conducted the revision. All authors confirmed the final version of the manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
This study was funded by the National Institutes of Health (R01DK066016). SA is supported by the Heinz C. Prechter Bipolar Research Fund and the Richard Tam Foundation at the University of Michigan Depression Center. Second author is supported by a grant from the Eunice Kennedy Shriver National Institute of Child Health and Development (NICHD) (T32 HD 79350-2).
1. Williams DR, Mohammed SA. Discrimination and racial disparities in health: evidence and needed research. J Behav Med (2009) 32(1):20–47. doi:10.1007/s10865-008-9185-0
2. Forsyth J, Schoenthaler A, Chaplin WF, Ogedegbe G, Ravenell J. Perceived discrimination and medication adherence in black hypertensive patients: the role of stress and depression. Psychosom Med (2014) 76(3):229–36. doi:10.1097/PSY.0000000000000043
3. Jackson JS, Brown TN, Williams DR, Torres M, Sellers SL, Brown K. Racism and the physical and mental health status of African Americans: a thirteen year national panel study. Ethn Dis (1995) 6(1–2):132–47.
4. Pascoe EA, Smart Richman L. Perceived discrimination and health: a meta-analytic review. Psychol Bull (2009) 135(4):531. doi:10.1037/a0016059
5. Williams DR, Neighbors HW, Jackson JS. Racial/ethnic discrimination and health: findings from community studies. Am J Public Health (2003) 93(2):200–8. doi:10.2105/AJPH.93.2.200
6. Banks KH, Kohn-Wood LP, Spencer M. An examination of the African American experience of everyday discrimination and symptoms of psychological distress. Community Ment Health J (2006) 42(6):555–70. doi:10.1007/s10597-006-9052-9
7. Brondolo E, Ver Halen NB, Pencille M, Beatty D, Contrada RJ. Coping with racism: a selective review of the literature and a theoretical and methodological critique. J Behav Med (2009) 32(1):64–88. doi:10.1007/s10865-008-9193-0
8. Krieger N. Methods for the scientific study of discrimination and health: an ecosocial approach. Am J Public Health (2012) 102(5):936–44. doi:10.2105/AJPH.2011.300544
9. McLaughlin KA, Hatzenbuehler ML, Keyes KM. Responses to discrimination and psychiatric disorders among Black, Hispanic, female, and lesbian, gay, and bisexual individuals. Am J Public Health (2010) 100(8):1477–84. doi:10.2105/AJPH.2009.181586
10. Ong AD, Fuller-Rowell T, Burrow AL. Racial discrimination and the stress process. J Pers Soc Psychol (2009) 96(6):1259. doi:10.1037/a0015335
11. Schulz AJ, Gravlee CC, Williams DR, Israel BA, Mentz G, Rowe Z. Discrimination, symptoms of depression, and self-rated health among African American women in Detroit: results from a longitudinal analysis. Am J Public Health (2006) 96(7):1265–70. doi:10.2105/AJPH.2005.064543
12. Utsey SO, Giesbrecht N, Hook J, Stanard PM. Cultural, sociofamilial, and psychological resources that inhibit psychological distress in African Americans exposed to stressful life events and race-related stress. J Couns Psychol (2008) 55(1):49. doi:10.1037/0022-0167.55.1.49
13. Brown TN, Williams DR, Jackson JS, Neighbors HW, Torres M, Sellers SL, et al. “Being black and feeling blue”: the mental health consequences of racial discrimination. Race Soc (2000) 2(2):117–31. doi:10.1016/S1090-9524(00)00010-3
14. Canady RB, Bullen BL, Holzman C, Broman C, Tian Y. Discrimination and symptoms of depression in pregnancy among African American and White women. Womens Health Issues (2008) 18(4):292–300. doi:10.1016/j.whi.2008.04.003
15. Foynes MM, Shipherd JC, Harrington EF. Race and gender discrimination in the Marines. Cultur Divers Ethnic Minor Psychol (2013) 19(1):111. doi:10.1037/a0030567
16. Odom EC, Vernon-Feagans L. Buffers of racial discrimination: links with depression among rural African American mothers. J Marriage Fam (2010) 72(2):346–59. doi:10.1111/j.1741-3737.2010.00704.x
17. Torres L, Ong AD. A daily diary investigation of latino ethnic identity, discrimination, and depression. Cultur Divers Ethnic Minor Psychol (2010) 16(4):561. doi:10.1037/a0020652
18. Wagner J, Abbott G. Depression and depression care in diabetes relationship to perceived discrimination in African Americans. Diabetes Care (2007) 30(2):364–6. doi:10.2337/dc06-1756
19. Walker RL, Salami TK, Carter SE, Flowers K. Perceived racism and suicide ideation: mediating role of depression but moderating role of religiosity among African American adults. Suicide Life Threat Behav (2014) 44(5):548–59. doi:10.1111/sltb.12089
20. Broman CL, Mavaddat R, Hsu S-Y. The experience and consequences of perceived racial discrimination: a study of African Americans. J Black Psychol (2000) 26(2):165–80. doi:10.1177/0095798400026002003
21. Sellers RM, Shelton JN. The role of racial identity in perceived racial discrimination. J Pers Soc Psychol (2003) 84(5):1079. doi:10.1037/0022-3514.84.5.1079
22. Brondolo E, Brady N, Thompson S, Tobin JN, Cassells A, Sweeney M, et al. Perceived racism and negative affect: analyses of trait and state measures of affect in a community sample. J Soc Clin Psychol (2008) 27(2):150. doi:10.1521/jscp.2008.27.2.150
23. Assari S, Miller RJ, Taylor RJ, Mouzon D, Keith V, Chatters LM. Discrimination fully mediates the effects of incarceration history on psychological distress and depressive symptoms among African American men. J Racial Ethn Health Disparities (2017). doi:10.1007/s40615-017-0364-y
24. Assari S, Lankarani MM. Discrimination and psychological distress: gender differences among Arab Americans. Front Psychiatry (2017) 8:23. doi:10.3389/fpsyt.2017.00023
25. Clark R, Anderson NB, Clark VR, Williams DR. Racism as a stressor for African Americans: a biopsychosocial model. Am Psychol (1999) 54(10):805. doi:10.1037/0003-066X.54.10.805
26. Kessler RC, Mickelson KD, Williams DR. The prevalence, distribution, and mental health correlates of perceived discrimination in the United States. J Health Soc Behav (1999) 40(3):208–30. doi:10.2307/2676349
27. Landrine H, Klonoff EA. The schedule of racist events: a measure of racial discrimination and a study of its negative physical and mental health consequences. J Black Psychol (1996) 22(2):144–68. doi:10.1177/00957984960222002
28. Jackson JS, Knight KM, Rafferty JA. Race and unhealthy behaviors: chronic stress, the HPA axis, and physical and mental health disparities over the life course. Am J Public Health (2010) 100(5):933–9. doi:10.2105/AJPH.2008.143446
29. Himmelstein MS, Young DM, Sanchez DT, Jackson JS. Vigilance in the discrimination-stress model for Black Americans. Psychol Health (2015) 30(3):253–67. doi:10.1080/08870446.2014.966104
30. Sellers RM, Caldwell CH, Schmeelk-Cone KH, Zimmerman MA. Racial identity, racial discrimination, perceived stress, and psychological distress among African American young adults. J Health Soc Behav (2003) 44(3):302–17. doi:10.2307/1519781
31. Haywood C Jr, Lanzkron S, Bediako S, Strouse JJ, Haythornthwaite J, Carroll CP, et al. Perceived discrimination, patient trust, and adherence to medical recommendations among persons with sickle cell disease. J Gen Intern Med (2014) 29(12):1657–62. doi:10.1007/s11606-014-2986-7
32. Haywood C Jr, Diener-West M, Strouse J, Carroll CP, Bediako S, Lanzkron S, et al. Perceived discrimination in health care is associated with a greater burden of pain in sickle cell disease. J Pain Symptom Manage (2014) 48(5):934–43. doi:10.1016/j.jpainsymman.2014.02.002
33. Chen FM, Fryer GE Jr, Phillips RL Jr, Wilson E, Pathman DE. Patients’ beliefs about racism, preferences for physician race, and satisfaction with care. Ann Fam Med (2005) 3(2):138–43. doi:10.1370/afm.282
34. Caughy MOB, O’Campo PJ, Muntaner C. Experiences of racism among African American parents and the mental health of their preschool-aged children. Am J Public Health (2004) 94(12):2118–24. doi:10.2105/AJPH.94.12.2118
35. Krieger N. Racial and gender discrimination: risk factors for high blood pressure? Soc Sci Med (1990) 30(12):1273–81. doi:10.1016/0277-9536(90)90307-E
36. Krieger N, Sidney S. Racial discrimination and blood pressure: the CARDIA Study of young black and white adults. Am J Public Health (1996) 86(10):1370–8. doi:10.2105/AJPH.86.10.1370
37. Slaughter-Acey JC, Caldwell CH, Misra DP. The influence of personal and group racism on entry into prenatal care among African American women. Womens Health Issues (2013) 23(6):e381–7. doi:10.1016/j.whi.2013.08.001
38. Hausmann LR, Kressin NR, Hanusa BH, Ibrahim SA. Perceived racial discrimination in health care and its association with patients’ healthcare experiences: does the measure matter? Ethn Dis (2010) 20:40–7.
39. Piette JD, Bibbins-Domingo K, Schillinger D. Health care discrimination, processes of care, and diabetes patients’ health status. Patient Educ Couns (2006) 60:41–8. doi:10.1016/j.pec.2004.12.001
40. Ryan AM, Gee GC, Griffith D. The effects of perceived discrimination on diabetes management. J Health Care Poor Underserved (2008) 19:149–63. doi:10.1353/hpu.2008.0005
41. Peek ME, Wagner J, Tang H, Baker DC, Chin MH. Self-reported racial discrimination in health care and diabetes outcomes. Med Care (2011) 49(7):618–25. doi:10.1097/MLR.0b013e318215d925
42. Trivedi AN, Ayanian JZ. Perceived discrimination and use of preventive health services. J Gen Intern Med (2006) 21:553–8. doi:10.1111/j.1525-1497.2006.00413.x
43. Assari S. Gender differences in the predictive role of self-rated health on short-term risk of mortality among older adults. SAGE Open Med (2016) 4:2050312116666975. doi:10.1177/2050312116666975
44. Assari S. Psychosocial correlates of body mass index in the united states: intersection of race, gender and age. Iran J Psychiatry Behav Sci (2016) 10(2):e3458. doi:10.17795/ijpbs-3458
45. Brodish AB, Cogburn CD, Fuller-Rowell TE, Peck S, Malanchuk O, Eccles JS. Perceived racial discrimination as a predictor of health behaviors: the moderating role of gender. Race Soc Probl (2011) 3(3):160–9. doi:10.1007/s12552-011-9050-6
46. Neblett EW, Bernard DL, Banks KH. The moderating roles of gender and socioeconomic status in the association between racial discrimination and psychological adjustment. Cogn Behav Pract (2016) 23(3):385–97. doi:10.1016/j.cbpra.2016.05.002
47. Ifatunji MA, Harnois CE. An explanation for the gender gap in perceptions of discrimination among African Americans considering the role of gender bias in measurement. Sociol Race Ethn (2015) 2(3):2332649215613532. doi:10.1177/2332649215613532
48. Browne I, Misra J. The intersection of gender and race in the labor market. Annu Rev Sociol (2003) 29:487–513. doi:10.1146/annurev.soc.29.010202.100016
49. Aikens JE, Perkins DW, Lipton B, Piette JD. Longitudinal analysis of depressive symptoms and glycemic control in type 2 diabetes. Diabetes Care (2009) 32(7):1177–81. doi:10.2337/dc09-0071
50. Bureau of the Census. U.S. Census of Population: Subject Reports, Socioeconomic Status. Final Report PC(2)-5C. Washington, DC: U.S. Government Printing Office (1967). Available from: https://census.gov/library/publications/1964/dec/population-pc-2-5c.html
51. Nam CB, Powers MG. The Socioeconomic Approach to Status Measurement. Houston, TX: Cap and Gown Press (1983).
52. Assari S. Cross-country variation in additive effects of socio-economics, health behaviors, and comorbidities on subjective health of patients with diabetes. J Diabetes Metab Disord (2014) 13(1):36. doi:10.1186/2251-6581-13-36
53. Assari S, Lankarani MM, Burgard S. Black-white difference in long-term predictive power of self-rated health on all-cause mortality in United States. Ann Epidemiol (2016) 26(2):106–14. doi:10.1016/j.annepidem.2015.11.006
54. Schnittker J, Bacak V. The increasing predictive validity of self-rated health. PLoS One (2014) 9(1):e84933. doi:10.1371/journal.pone.0084933
55. Singh-Manoux A, Martikainen P, Ferrie J, Zins M, Marmot M, Goldberg M. What does self rated health measure? Results from the British Whitehall II and French Gazel cohort studies. J Epidemiol Community Health (2006) 60(4):364–72. doi:10.1136/jech.2005.039883
56. Davis JE. Early schooling and academic achievement of African American males. Urban Educ (2003) 38(5):515–37. doi:10.1177/0042085903256220
57. Honora DT. The relationship of gender and achievement to future outlook among African American adolescents. Adolescence (2002) 37(146):301.
58. Noguera PA. The trouble with Black boys: the role and influence of environmental and cultural factors on the academic performance of African American males. Urban Educ (2003) 38(4):431–59. doi:10.1177/0042085903038004005
59. Roderick M. What’s happening to the boys? Early high school experiences and school outcomes among African American male adolescents in Chicago. Urban Educ (2003) 38(5):538–607. doi:10.1177/0042085903256221
60. Swanson DP, Cunningham M, Spencer MB. Black males’ structural conditions, achievement patterns, normative needs, and “opportunities”. Urban Educ (2003) 38(5):608–33. doi:10.1177/0042085903256218
61. Simpson AW, Erickson MT. Teachers’ verbal and nonverbal communication patterns as a function of teacher race, student gender, and student race. Am Educ Res J (1983) 20(2):183–98. doi:10.3102/00028312020002183
62. Howard LC, Rose JC, Barbarin OA. Raising African American boys: an exploration of gender and racial socialization practices. Am J Orthopsychiatry (2013) 83(2 Pt 3):218–30. doi:10.1111/ajop.12031
63. Thomas A, Caldwell CH, Assari S, Jagers RJ, Flay B. You do what you see: how witnessing physical violence is linked to violent behavior among male African American adolescents. J Mens Stud (2016) 24(2):185–207. doi:10.1177/1060826516641104
64. Varner F, Mandara J. Discrimination concerns and expectations as explanations for gendered socialization in African American families. Child Dev (2013) 84(3):875–90. doi:10.1111/cdev.12021
65. Bowman PJ, Howard C. Race-related socialization, motivation, and academic achievement: a study of Black youths in three-generation families. J Am Acad Child Psychiatry (1985) 24(2):134–41. doi:10.1016/S0002-7138(09)60438-6
66. Coard SI, Wallace SA, Stevenson HC Jr, Brotman LM. Towards culturally relevant preventive interventions: the consideration of racial socialization in parent training with African American families. J Child Fam Stud (2004) 13(3):277–93. doi:10.1023/B:JCFS.0000022035.07171.f8
67. Assari S, Moazen-Zadeh E, Caldwell CH, Zimmerman MA. Racial discrimination during adolescence predicts mental health deterioration in adulthood: gender differences among Blacks. Front Public Health (2017) 5:104. doi:10.3389/fpubh.2017.00104
68. Assari S, Smith JR, Caldwell CH, Zimmerman MA. Gender differences in longitudinal links between neighborhood fear, parental support, and depression among African American emerging adults. Societies (2015) 5(1):151–70. doi:10.3390/soc5010151
69. Assari S, Caldwell CH. Neighborhood safety and major depressive disorder in a national sample of Black youth; gender by ethnic differences. Children (Basel) (2017) 4(2):E14. doi:10.3390/children4020014
70. Assari S, Lankarani MM. Association between stressful life events and depression; intersection of race and gender. J Racial Ethn Health Disparities (2016) 3(2):349–56. doi:10.1007/s40615-015-0160-5
71. Assari S, Caldwell CH, Zimmerman MA. Perceived neighborhood safety during adolescence predicts subsequent deterioration of subjective health two decades later; gender differences in a racially-diverse sample. Int J Prev Med (2015) 6:117. doi:10.4103/2008-7802.170431
72. Assari S, Moghani Lankarani M, Caldwell CH, Zimmerman MA. Fear of neighborhood violence during adolescence predicts development of obesity a decade later: gender differences among African Americans. Arch Trauma Res (2016) 5(2):e31475. doi:10.5812/atr.31475
73. Mezuk B, Abdou CM, Hudson D, Kershaw KN, Rafferty JA, Lee H, et al. “White box” epidemiology and the social neuroscience of health behaviors: the environmental affordances model. Soc Ment Health (2013) 3(2). doi:10.1177/2156869313480892
74. Bertakis KD, Azari R, Helms LJ, Callahan EJ, Robbins JA. Gender differences in the utilization of health care services. J Fam Pract (2000) 49(2):147–52.
75. Mayor E. Gender roles and traits in stress and health. Front Psychol (2015) 9(6):779. doi:10.3389/fpsyg.2015.00779
76. Kelly MM, Tyrka AR, Price LH, Carpenter LL. Sex differences in the use of coping strategies: predictors of anxiety and depressive symptoms. Depress Anxiety (2008) 25(10):839–46. doi:10.1002/da.20341
77. Harnois CE, Ifatunji M. Gendered measures, gendered models: toward an intersectional analysis of interpersonal racial discrimination. Ethn Racial Stud (2011) 34(6):1006–28. doi:10.1080/01419870.2010.516836
78. Caldwell CH, Antonakos CL, Tsuchiya K, Assari S, De Loney EH. Masculinity as a moderator of discrimination and parenting on depressive symptoms and drinking behaviors among nonresident African-American fathers. Psychol Men Masc (2013) 14(1):47. doi:10.1037/a0029105
79. Hammond WP. Taking it like a man: masculine role norms as moderators of the racial discrimination–depressive symptoms association among African American men. Am J Public Health (2012) 102(S2):S232–41. doi:10.2105/AJPH.2011.300485
80. Hawkins J, Watkins DC, Kieffer E, Spencer M, Piatt G, Nicklett EJ, et al. An exploratory study of the impact of gender on health behavior among African American and Latino men with type 2 diabetes. Am J Mens Health (2016) 11(2):1557988316681125. doi:10.1177/1557988316681125
81. Hudson DL, Bullard KM, Neighbors HW, Geronimus AT, Yang J, Jackson JS. Are benefits conferred with greater socioeconomic position undermined by racial discrimination among African American men? J Mens Health (2012) 9(2):127–36. doi:10.1016/j.jomh.2012.03.006
82. Assari S, Watkins DC, Caldwell CH. Race attribution modifies the association between daily discrimination and major depressive disorder among Blacks: the role of gender and ethnicity. J Racial Ethn Health Disparities (2015) 2(2):200–10. doi:10.1007/s40615-014-0064-9
83. Seaton EK, Neblett EW, Upton RD, Hammond WP, Sellers RM. The moderating capacity of racial identity between perceived discrimination and psychological well-being over time among African American youth. Child Dev (2011) 82(6):1850–67. doi:10.1111/j.1467-8624.2011.01651.x
84. Sellers RM, Linder NC, Martin PM, Lewis RL. Racial identity matters: the relationship between racial discrimination and psychological functioning in African American adolescents. J Res Adolesc (2006) 16:187–216. doi:10.1111/j.1532-7795.2006.00128.x
85. Smalls C, White R, Chavous T, Sellers R. Racial ideological beliefs and racial discrimination experiences as predictors of academic engagement among African American adolescents. J Black Psychol (2007) 33:299–330. doi:10.1177/0095798407302541
86. Anderson LM, Scrimshaw SC, Fullilove MT, Fielding JE, Normand J; Task Force on Community Preventive Services. Culturally competent healthcare systems. A systematic review. Am J Prev Med (2003) 24(3 Suppl):68–79. doi:10.1016/S0749-3797(02)00657-8
87. Clifford A, McCalman J, Bainbridge R, Tsey K. Interventions to improve cultural competency in health care for Indigenous peoples of Australia, New Zealand, Canada and the USA: a systematic review. Int J Qual Health Care (2015) 27(2):89–98. doi:10.1093/intqhc/mzv010
88. Gallagher RW, Polanin JR. A meta-analysis of educational interventions designed to enhance cultural competence in professional nurses and nursing students. Nurse Educ Today (2015) 35(2):333–40. doi:10.1016/j.nedt.2014.10.021
89. Horvat L, Horey D, Romios P, Kis-Rigo J. Cultural competence education for health professionals. Cochrane Database Syst Rev (2014) 5:CD009405. doi:10.1002/14651858.CD009405.pub2
90. Lie DA, Lee-Rey E, Gomez A, Bereknyei S, Braddock CH III. Does cultural competency training of health professionals improve patient outcomes? A systematic review and proposed algorithm for future research. J Gen Intern Med (2011) 26(3):317–25. doi:10.1007/s11606-010-1529-0
91. Wang J, Kearney JA. The experience of Chinese American parents of children with life-limiting illness: a comprehensive review. Int J Palliat Nurs (2013) 19(7):347–54. doi:10.12968/ijpn.2013.19.7.347
92. Aikens JE. Prospective associations between emotional distress and poor outcomes in type 2 diabetes. Diabetes Care (2012) 35(12):2472–8. doi:10.2337/dc12-0181
93. Carter JS, Pugh JA, Monterrosa A. Non-insulin-dependent diabetes mellitus in minorities in the United States. Ann Intern Med (1996) 125(3):221–32. (AHRQ Grant HS07397). doi:10.7326/0003-4819-125-3-199608010-00011
94. Cook CB, Erdman DM, Ryan GJ, Greenlund KJ, Giles WH, Gallina DL, et al. The pattern of dyslipidemia among urban African-Americans with type 2 diabetes. Diabetes Care (2000) 23(3):319–24. (AHRQ Grant HS09722). doi:10.2337/diacare.23.3.319
95. Hammond WP. Psychosocial correlates of medical mistrust among African American men. Am J Community Psychol (2010) 45(1–2):87–106. doi:10.1007/s10464-009-9280-6
96. Hammond WP, Matthews D, Mohottige D, Agyemang A, Corbie-Smith G. Masculinity, medical mistrust, and preventive health services delays among community-dwelling African-American men. J Gen Intern Med (2010) 25(12):1300–8. doi:10.1007/s11606-010-1481-z
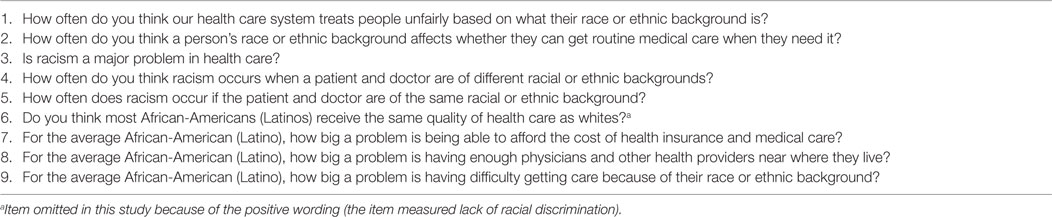
Table A1. Chen measure of perceived racial discrimination in health care.
Keywords: Blacks, African-Americans, gender, racial discrimination, diabetes
Citation: Assari S, Lee DB, Nicklett EJ, Moghani Lankarani M, Piette JD and Aikens JE (2017) Racial Discrimination in Health Care Is Associated with Worse Glycemic Control among Black Men but Not Black Women with Type 2 Diabetes. Front. Public Health 5:235. doi: 10.3389/fpubh.2017.00235
Received: 05 July 2017; Accepted: 21 August 2017;
Published: 12 September 2017
Edited by:
Jeff M. P. Holly, University of Bristol, United KingdomReviewed by:
Denis Richard, Laval University, CanadaCopyright: © 2017 Assari, Lee, Nicklett, Moghani Lankarani, Piette and Aikens. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) or licensor are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Shervin Assari, YXNzYXJpQHVtaWNoLmVkdQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.