 Setareh Forouzan1,2*
Setareh Forouzan1,2* Mojgan Padyab3,4Hassan Rafiey5Mehdi Ghazinour4
Mojgan Padyab3,4Hassan Rafiey5Mehdi Ghazinour4 Masoumeh Dejman2,6Miguel San Sebastian1
Masoumeh Dejman2,6Miguel San Sebastian1
- 1Department of Public Health and Clinical Medicine, Umea University, Umea, Sweden
- 2Social Determinants of Health Research Centre, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran
- 3Ageing and Living Conditions Programme, Centre for Population Studies, Umea University, Umea, Sweden
- 4Department of Social Work, Umea University, Umea, Sweden
- 5Social Welfare Management Research Center, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran
- 6Department of Mental Health, Bloomberg School of Public Health, Johns Hopkins University, Baltimore, MD, USA
As explained by the World Health Organization (WHO) in 2000, the concept of health system responsiveness is one of the core goals of health systems. Since 2000, further efforts have been made to measure health system responsiveness and the factors affecting responsiveness, yet few studies have applied responsiveness concepts to the evaluation of mental health systems. The present study aims to measure responsiveness and its related domains in the mental health-care system of Tehran. Utilizing the same method used by the WHO for its responsiveness survey, responsiveness for outpatient mental health care was evaluated using a validated Farsi questionnaire. A sample of 500 public mental health service users in Tehran participated and subsequently completed the questionnaire. On average, 47% of participants reported experiencing poor responsiveness. Among responsiveness domains, confidentiality and dignity were the best performing factors while autonomy, access to care, and quality of basic amenities were the worst performing. Respondents who reported their social status as low were more likely to experience poor responsiveness overall. Attention and access to care were responsiveness dimensions that performed poorly but were considered to be highly important by study participants. In summary, the study suggests that measuring responsiveness could provide guidance for further development of mental health-care systems to become more patient orientated and provide patients with more respect.
Introduction
The Universal Declaration of Human Rights and its related conventions and guidelines, which have been ratified by governments globally, contain a wide range of health-related rights. These include the right to health and health care, and particularly the right of individuals with physical and mental disabilities to the highest quality health services (1). When governments proceed to promote and protect public health, their actions must adhere to certain criteria to ensure that people are treated in ways that respect their rights and respond to their legitimate expectations (2). With the intention to assess the extent to which the health-care systems perform close to user expectations (based on their experiences with the health system), in 2000, the concept of responsiveness was developed and operationalized by the World Health Organization (WHO) (3). Responsiveness is defined as a measure of how individuals are treated and the environment in which they are treated and includes eight domains (4). Certain aspects of human rights, such as respecting patients’ autonomy, dignity, confidentiality, and choice of health care as well as client orientation aspects, such as the quality of basic amenities, prompt attention, and access to social support are covered in the concept of responsiveness.
Responsiveness becomes particularly relevant when considering the mental health-care system (5). Compared to other health service users, mentally ill patients are at the greatest risk for having their rights violated because of the characteristics of the mental disorders and the stigma attached to them (6). At the same time, research shows the importance of an active interaction between the mental health system and the service users to achieve better mental health-care outcomes and reduce delays in service referral (7, 8).
Beginning in the late 1980s, in order to achieve the highest attainable level of mental health care, the Islamic Republic of Iran began integrating mental health services into primary health care. At the village or neighborhood level in urban areas, community health workers are in charge of mental health-care responsibilities, including active case finding and referral. At primary care centers, trained general practitioners provide mental health care as part of their general health-care responsibilities. In case of complex mental health problems, general practitioners refer patients to district or provincial health centers, which are supported by university mental health hospitals (9). The strong existing ties between medical education and health sectors facilitate the integration process around the country.
The way in which mental health services were organized after their integration into public health care positively affected the coverage of treatment for people with diverse mental disorders (10). However, despite the increase in coverage shown by national and regional surveys (11, 12), information about the quality of mental health care is lacking.
The application of the WHO responsiveness concept could contribute to assessing some of the quality aspects of the mental health-care system in Iran. This study aims to assess how the domains of responsiveness are performing in the mental health-care system of Tehran. In addition, two interrelated objectives will be explored: (i) Are the perceptions of responsiveness different by sociodemographic characteristics? and (ii) Which responsiveness domains are most important to service users? Is it those with good or poor performance?
Materials and Methods
Setting
In some ways, the health system structure and organization in the Islamic Republic of Iran is unique. At the national level, the Ministry of Health and Medical Education (MoHME) is responsible for health service delivery through planning, designing, and implementing health policies as well as monitoring and supervising health-related activities for the public and private sectors (8). Yet, the MoHME implements health policies and plans via medical universities across the country. There is at least one medical university in every province. The president of a medical university is the highest health authority in the province and is assigned by and reports to the MoHME. The medical universities are in charge of public health activities, health-care provision in public facilities, and medical education. Health-care and public health services are provided through a nation-wide network including a referral system that starts at the household/health post level in the periphery, goes through secondary-level health centers in districts and at provincial and capital level, ends at university hospitals.
As in many large cities, the provision of mental health care in Tehran is complex. A combination of public, private, and special services such as military hospitals and clinics as well as services related to semi-private schools of medicine (e.g., Azad medical university) are involved in mental health-care provision. Most people, especially those from poor neighborhoods, depend on public mental health services because of the high costs of private care.
Study Population
The survey was conducted in Tehran, the capital of Iran, between January and April 2013. In Tehran, mental health services are organized in terms of catchment areas. Each of the four public medical universities provides inpatient and outpatient mental health services for a defined catchment area. These services are provided through mental hospitals and nine affiliated outpatient clinics. However, service users can freely choose to be referred to any of the mental health services.
A non-random sample of 500 mentally ill patients referring to 27 mental health service providers in nine public outpatient clinics distributed in different city regions (north, south, east, west, and central) was selected. Private psychiatric clinics were excluded. The number of participants assigned to each clinic was proportional to the total number of patients attending the clinics during the previous 3 months.
Service users diagnosed as mentally ill based on a psychiatric evaluation record (the psychiatrists were blinded to the study). The study participants were recruited after being initially approached by the interviewers with regard to their willingness to participate. Inclusion criteria were (1) being an adult (18–65 years old), (2) receiving outpatient care during the past 12 months, and (3) being mentally capable of following the interview according to their clinical record. Type of mental disorder was not considered an inclusion criterion since experiences that mental health patients have with services relate more to the services functioning than to the patient’s current diagnosis (13, 14). Service users older than 65 years were not included in our study because previous studies showed that at least about 10% of them have different level of age-associated memory impairment (15).
Trained external interviewers with a bachelor degree in psychology conducted face-to-face interviews. Interviewers explained the procedure of the interview to the participants and obtained their written consent. Participants were asked about the outpatient mental health-care services that they had experienced during the last 12 months; interviews lasted between 45 and 50 min and were strictly anonymous. To ensure subjects were not interviewed twice, each record was labeled with a code. The Ethical Committee and Research Council of the University of Social Welfare and Rehabilitation Sciences in Iran approved the study. In addition, administrative permission was obtained from the Medical Universities in the study area. All study participants were evaluated by a psychiatrist prior to the interview. Based on the psychiatrist-written clinical reports, participants were in the remission phase of their mental disorder and capable of making a decision. The nature and purpose of the study was explained to each participant; then, individual informed consent was confirmed by participants with a signature or a left thumbprint. Before the interview, participants were informed that the completion of the questionnaire was voluntary and their identification would be protected, as the data files were anonymous. Participants were informed of their right to withdraw from the study at any time. Participants gave permission to audiotape the interview session.
The Instrument
The responsiveness concept developed by the WHO was applied in this study (16). In a previous qualitative study, we evaluated the applicability of this concept to mental health care in Iran. With some modifications, the concept was proved to suit Iranian mental health service users’ expectations (17). A new domain of effective care was added; the domain of prompt attention was divided into two new domains (attention and access to care), and the domains choice of health-care providers and autonomy were combined into one domain (Table 1) (18).
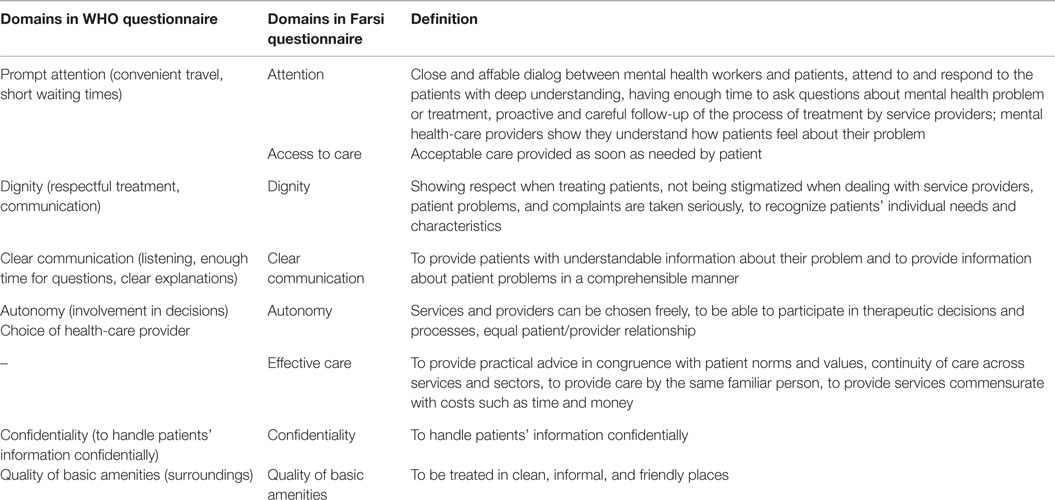
Table 1. Domains covered in the WHO and Farsi responsiveness questionnaires.
In accordance with the WHO health system responsiveness questionnaire (19) and the findings of our previous qualitative study (17), a Farsi version of the mental health system responsiveness questionnaire was adapted to suit the mental health-care system in Iran (18). Classic psychometric criteria of the Farsi version of the questionnaire have been measured and its feasibility, reliability, and validity tested previously (18). The questionnaire consisted of 40 questions representing eight domains. The domain “access to social support” was excluded from the questionnaire since inpatient cases were not included in this study. In addition, to measure the importance of the domains, participants were asked to identify the domain they felt was the most and the least important in mental health care.
Data Analysis
In accordance with WHO’s approach in the Multicountry Survey Study on Health and Responsiveness (MCSS), we scored responsiveness in each domain based on the “rating” question, which was asked only after participants had answered a series of detailed “report” questions related to the relevant domain. For the rating questions, the responses were categorized as 5 (very bad), 4 (bad), 3 (moderate), 2 (good), and 1 (very good). A further summary score for “overall responsiveness” was obtained by calculating the average scores across all the eight domains. The responsiveness outcomes were then dichotomized into good responsiveness (combining the very good and good responses) and poor responsiveness (combining the moderate, bad, and very bad responses) (20). Multivariable logistic regression was used to assess the odds ratios of poor performance of overall responsiveness and its related domains in relation to sociodemographic characteristics of the participants. These characteristics included age, sex, education level (primary or <5 years of education, intermediate level 5–12 years, and higher education >12 years), employment, and subjective social status (SSS). SSS was recorded based on how people perceived their relative position in the social hierarchy (i.e., low, middle, and high). Because the distribution of SSS was asymmetric among study participants, the middle social position (52.7%) was chosen as the reference group. We applied chi-square test to check the bivariate association between overall poor responsiveness and sociodemographic characteristics. All analyses were performed using STATA version 12.0 and p-values <0.05 were considered significant (21).
Results
Study Group
A total of 500 participants aged 18–65 years (mean = 36.4, SD = 12 years) were enrolled in the study. Among them, 38% were females and 62% males. Approximately 24% had 5 years or less of formal education and 28.7% were unemployed. All participants revealed that they used the services more than once during the past 6 months, and 96% had used services more than twice in the last 6 months. The majority of participants (52.7%) indicated that they belonged to the middle social status, and 92.8% of participants had access to medical insurance. Details of the sociodemographic characteristics of the study participants are presented in Table 2.
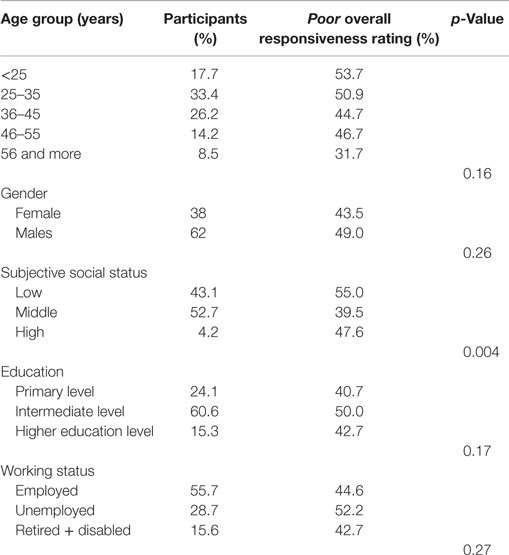
Table 2. Sociodemographic characteristics of the study group and poor overall responsiveness rating.
Responsiveness Performance
On average, 47% of participants reported experiencing poor responsiveness. Table 2 shows the distribution of participants reporting poor responsiveness among the different sociodemographic groups. Youngest participants (53.7%) reported worst responsiveness than did older participants (31.7%). In addition, more participants with low SSS scored responsiveness as poor compared to those with high and middle SSS. Approximately half of the participants with intermediate educations or who were unemployed reported poor responsiveness for services.
Figure 1 shows the proportion of participants who reported responsiveness as very bad, bad, moderate, good, and very good in all domains. The best-performing domains (very good and good) were confidentiality (92.4%) and dignity (81.8%). The worst performing (moderate, bad, and very bad) domains were autonomy (42.7%), access to care (31.9%), and quality of basic amenities (31.3%).
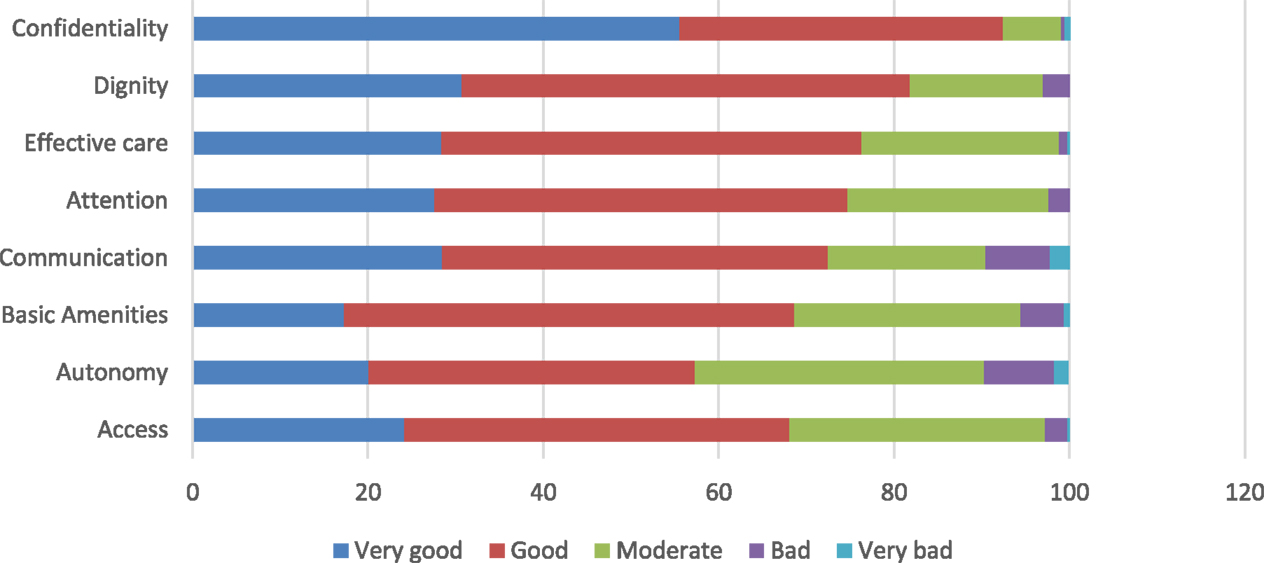
Figure 1. Percentage of participants rating responsiveness domains.
In order to examine the relationship between the poor responsiveness rating and the sociodemographic characteristics of participants, a multivariable logistic regression analysis was performed. Overall, as well per domain, SSS was the only characteristic that showed differences in rating responsiveness (Table 3). Respondents who reported themselves as belonging to a lower social status were more likely to experience overall poor responsiveness (OR = 2.2; 95% CI = 1.5–3.3). Regarding the different responsiveness domains, participants who reported themselves as belonging to a lower social status were about three times more likely to experience poor access to care (OR = 3.2; 95% CI = 2.1–4.9), poor effective care (OR = 2.9; 95% CI = 1.8–4.8), and poor dignity (OR = 2.8; 95% CI = 1.6–4.8). Lower social status was also statistically associated with experiences of poor communication (OR = 2.5; 95% CI = 1.6–3.9), poor attention (OR = 2.2; 95% CI = 1.4–3.5), and poor autonomy (OR = 1.8; 95% CI = 1.2–2.8).

Table 3. Percentage and odds ratios of poor responsiveness (overall and per domain) in respect to subjective social status (SSS).a
Importance of Domains and Performance
The importance of the responsiveness domains in relation to domain performance is presented in Figure 2. The majority of respondents named attention, dignity, access, and confidentiality as the most important domains. However, the access dimension score was among the lowest in terms of performance and the score for attention performance was not good. Only the dignity and confidentiality dimensions scored high both in importance and in performance. Autonomy, quality of basic amenities and clear communication performed poorly but were considered as highly important.
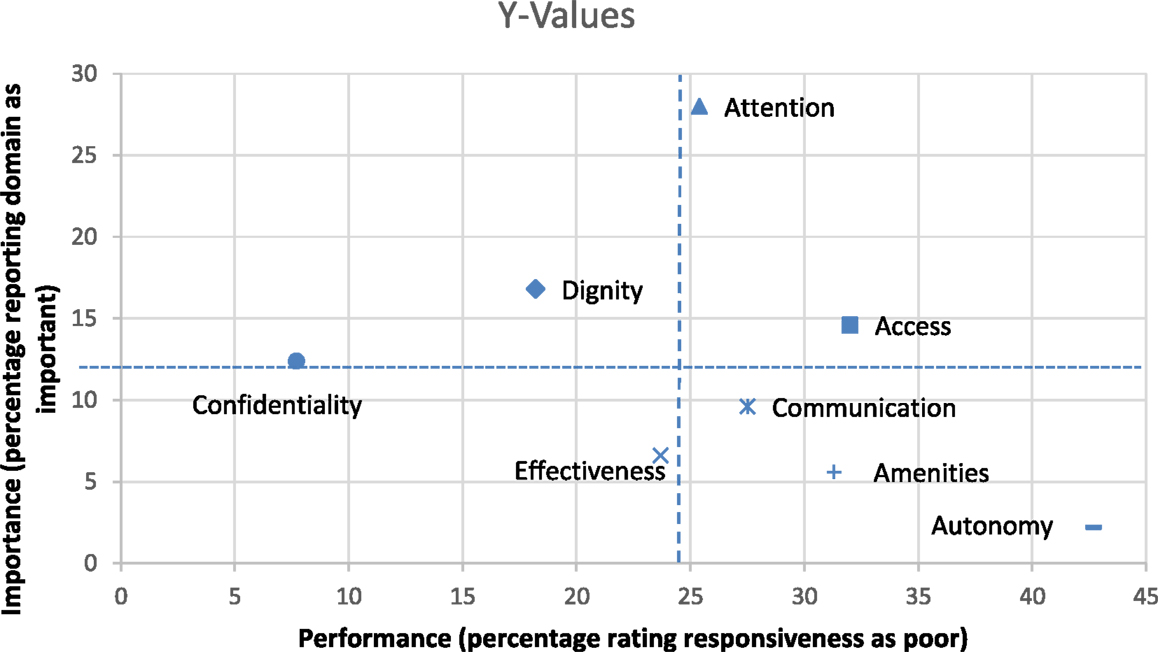
Figure 2. Responsiveness by domains in relation to domain importance.
Discussion
To our knowledge, this is the first study exploring the responsiveness of the mental health-care system in Iran. Previously, only one study from Germany focused on the responsiveness of the mental health-care system (13). However, using the original form of the WHO measure, three previous studies nationally assessed general health-care responsiveness among specific groups of service users (22–24). One of those studies was conducted in Mashhad City, located in North East Iran and investigated the responsiveness of general public and private hospitals (22); the other two were performed in Tehran (23, 24). One of these studies assessed health system responsiveness in a relatively low socioeconomic district of the city (23), while the other measured responsiveness in children’s health care (24).
Our study showed that confidentiality was the best-performing domain in outpatient mental health care. This result is in line with the German study on mental health responsiveness as well as the studies from Tehran (13, 23). This finding indicates that the mental health system in Tehran has been able to build an atmosphere of trust for patients. On the other hand, this finding may be due to the fact that it is sometimes difficult for patients to be aware of the extent to which their personal information is handled confidentially. In addition, our previous qualitative study on mental health responsiveness showed that the service users have uncertainty about the limits of secrecy (17).
Dignity was the second best-performing domain in our study. This finding is also supported in previous responsiveness studies (13, 23, 25). In addition, our previous qualitative study indicated that a significant number of participants had a positive experience of being treated respectfully and not being stigmatized when referring to mental health services (17). This finding indicates that service users are treated with respect regarding their dignity when interacting with the health system in Iran, and in this case, there is no graphic difference between the health system in general and the mental health subsystem.
Autonomy, access to care, and quality of basic amenities were poor-performing domains. It is noteworthy that in our study, autonomy combines the domains of choice and autonomy used in the WHO questionnaire. In this respect, our findings are very similar to the German study on mental health responsiveness. In mental health care, there are indeed fewer opportunities for free choice and service user autonomy. This may be due to the fact that some mentally ill patients may have poor insight into their disorder and also suffer from some degree of impairments in their rational thinking. Therefore, for these patients, active participation in the process of decision making is difficult and complex. On the other hand, there is a specific desire among mental health service users to participate in mental health-care decisions, and the more they recover, the more they want to participate (26, 27). Furthermore, our qualitative study showed that even some information about the medication are provided by the doctors, but there is no consenting for medication and patients’ opinions about the medication and their side effects were not taken seriously (17). In addition, lack of sufficient health facilities as well as unfamiliarity of service providers with methods to increase participation of mental health service users, including shared decision making and transparency of mental health reports, can lead to poor autonomy.
Access to care was the second poor-performing domain. The definition of this domain in our study was very similar to the domain of prompt attention used in the WHO questionnaire. In this regard, our results are different from the German study (13) but very similar to the ones from Tehran (23). The very centralized organization of mental health facilities, as well as a lack of sufficient mental health funding and staff, might negatively influence access to care (28, 29). Improvement of the access scores appears to be resource-dependent; however, a reengineering of the patient referral process especially in big cities, such as Tehran, could undoubtedly be effective in increasing access to services.
Regarding perceptions of responsiveness among different sociodemographic groups, the German study reported that outpatient care was perceived differently depending on respondents’ income and education (13). However, in our study, the only sociodemographic variable associated with poor responsiveness was lower SSS. This could be due to the fact that SSS represents a combination of various markers of socioeconomic status and thus might reflect an individual’s social position more accurately (30). To explain possible reasons for the SSS disparities in health system responsiveness, two groups of reasons can be considered (31): (i) factors related to differential access to quality health services, particularly among poor districts of the city and (ii) service user providers-related factors. The unfair distribution of mental health facilities and human resources in Tehran, especially among suburban poor regions of the city, might partially explain the poor experience of users from low social status. Equity in access to the public health services is therefore needed. In relation to service user provider factors, a systematic review of studies exploring patients’ social position and the doctor–patient communication showed that patients from lower social status were less involved in the decision-making process and had more difficulties in understanding the medical information provided by the physician (32). At the same time, health service providers tend to perceive patients of lower social status more negatively compared with those of higher status (33). Others have also shown that regardless of patient communication behavior, physicians are more skeptical about apprehension of medical information by low-income people (34). These findings are highly relevant to our study results where lower social status participants reported more experiencing poor effective care, attention, dignity, and communication.
There is no statistically significant difference in responsiveness between males and females and between different age groups. This finding is consistent with the result of studies in health system responsiveness in Iran and the German study on mental health system responsiveness (23–25). This finding can be explained by the fact that outpatient mental health care in public facilities in Tehran is uniform.
In terms of the importance of the responsiveness domains, attention, dignity, and access to care received higher scores. This finding is also similar to a study among mentally handicapped children in Tehran (24) and a study of patient expectations in Iran that showed how the quality of interpersonal relationships is an important aspect of health service users’ expectations (35).
Performance of responsiveness domains in relation to the importance given to them in our study showed that attention and access to care do not perform well despite their importance for service users. Access to care seems to be a core expectation in general health care as well as mental health care (13, 23). The previous qualitative study of responsiveness among mental health service users also indicates that the majority of participants’ statements were related to this domain and almost all of them expected a warm and sincere approach from service providers. The complaints about poor performance of these domains may be related to shortage of human resources and facilities as well as unbalanced distribution of services (36).
Conclusion
This is the first time that mental health system responsiveness has been measured in Iran. It represents the actual experiences of the service users when they come in contact with the mental health system. In conclusion, this study showed that dignity and confidentiality were well-performing domains, while autonomy, quality of basic amenities, and access were poor-performing domains. Improvement of all these poor-performing domains is dependent on resources. In addition, attention and access to care, which were rated high in importance and poor in performance, could be priority areas for intervention and reengineering of referral systems and admission processes. The role of the SSS in responsiveness should be further studied.
The need to assess responsiveness and its domains in the delivery of mental health services is not only important for good health practice but also for the provision of health and health-care rights (1). The findings of this study point out the strengths and weaknesses of the mental health system in Iran regarding responsiveness and establish the baseline for a future monitoring system.
Study Limitations
Our study had a few limitations. The cross-sectional study design did not permit investigation of the cause and effect relationship between our independent variables and responsiveness. In addition, this study did not include inpatient service users. Access to social support could not be measured either. Finally, although a different dichotomization of the responsiveness outcome might have resulted in other associations, we decided to follow the guidelines provided by WHO.
Author Contributions
SF: contributions to the conception or design of the work, analysis and interpretation of data, drafting the work, revising it critically, final approval of the version to be published, agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. MP: analysis and interpretation of data, revising it critically, final approval of the version to be published, agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. HR, MG, and MD: contributions to the conception or design of the work, revising it critically, final approval of the version to be published, agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. MS: contributions to the conception or design of the work, interpretation of data, drafting the work, revising it critically, final approval of the version to be published, agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Funding
This work was partly supported by the Global Health Research Scholarship and the Umeå Center for Global Health Research, funded by FAS, the Swedish Council for Working Life and Social Research (Grant no. 2006-1512).
References
1. Gostin L, Hodge JG, Valentine N, Nygren-Krug H. The Domains of Health Responsiveness – A Human Rights Analysis. Geneva: World Health Organization (2003).
2. Jones AM, Rice N, Robone S, Dias PR. Inequality and polarisation in health systems’ responsiveness: a cross-country analysis. J Health Econ (2011) 30(4):616–25. doi: 10.1016/j.jhealeco.2011.05.003
3. Murray CJ, Frenk J. A framework for assessing the performance of health systems. Bull World Health Organ (2000) 78(6):717–31.
4. Darby C, Valentine N, Murray CJ, De Silva A. World Health Organization (WHO): Strategy on Measuring Responsiveness. World Health Organization (2000).
5. Bramesfeld A, Klippel U, Seidel G, Schwartz FW, Dierks ML. How do patients expect the mental health service system to act? Testing the WHO responsiveness concept for its appropriateness in mental health care. Soc Sci Med (2007) 65(5):880–9. doi:10.1016/j.socscimed.2007.03.056
6. Loh A, Leonhart R, Wills CE, Simon D, Harter M. The impact of patient participation on adherence and clinical outcome in primary care of depression. Patient Educ Couns (2007) 65(1):69–78. doi:10.1016/j.pec.2006.05.007
7. Clever SL, Ford DE, Rubenstein LV, Rost KM, Meredith LS, Sherbourne CD, et al. Primary care patients’ involvement in decision-making is associated with improvement in depression. Med Care (2006) 44(5):398–405. doi:10.1097/01.mlr.0000208117.15531.da
9. Mohit A. A brief overview of the development of mental health in Iran, present challenges and the road ahead. Iran J Psychiatry Behav Sci (2009) 3(2):1–3.
10. Yasamy MT, Shahmohammadi D, Bagheri Yazdi SA, Layeghi H, Bolhari J, Razzaghi EM, et al. Mental health in the Islamic republic of Iran: achievements and areas of need. East Mediterr Health J (2001) 7(3):381–91.
11. Noorbala AA, Bagheri Yazdi SA, Yasamy MT, Mohammad K. Mental health survey of the adult population in Iran. Br J Psychiatry (2004) 184:70–3. doi:10.1192/bjp.184.1.70
12. Mohammadi MR, Davidian H, Noorbala AA, Malekafzali H, Naghavi HR, Pouretemad HR, et al. An epidemiological survey of psychiatric disorders in Iran. Clin Pract Epidemiol Ment Health (2005) 1:16. doi:10.1186/1745-0179-1-16
13. Bramesfeld A, Wedegartner F, Elgeti H, Bisson S. How does mental health care perform in respect to service users’ expectations? Evaluating inpatient and outpatient care in Germany with the WHO responsiveness concept. BMC Health Serv Res (2007) 7:99. doi:10.1186/1472-6963-7-99
14. Mattsson M, Lawoko S, Cullberg J, Olsson U, Hansson L, Forsell Y. Background factors as determinants of satisfaction with care among first-episode psychosis patients. Soc Psychiatry Psychiatr Epidemiol (2005) 40(9):749–54. doi:10.1007/s00127-005-0945-7
15. Crook T, Bartus RT, Ferris SH, Whitehouse P, Cohen GD, Gershon S. Age-associated memory impairment: proposed diagnostic criteria and measures of clinical change – report of a national institute of mental health work group. Dev Neuropsychol (1986) 2:261–76. doi:10.1080/87565648609540348
16. De Silva A, Valentine N. A framework for measuring responsiveness. Global Programme on Evidence for Health Policy Discussion Paper series: No. 32. Geneva: World Health Organization (2000).
17. Forouzan AS, Ghazinour M, Dejman M, Rafeiey H, San Sebastian M. Testing the WHO responsiveness concept in the Iranian mental healthcare system: a qualitative study of service users. BMC Health Serv Res (2011) 11:325. doi:10.1186/1472-6963-11-325
18. Forouzan AS, Rafiey H, Padyab M, Ghazinour M, Dejman M, Sebastian MS. Reliability and validity of a mental health system responsiveness questionnaire in Iran. Glob Health Action (2013) 42(10):1106–16.
19. Valentine N, De Silva A, Murray C. Estimating Responsiveness Level and Distribution for 191 Countries: Methods and Results. Geneva: World Health Organization (2000).
20. Valentine NB, Bonsel GJ, Murray CJ. Measuring quality of health care from the user’s perspective in 41 countries: psychometric properties of WHO’s questions on health systems responsiveness. Qual Life Res (2007) 16(7):1107–25. doi:10.1007/s11136-007-9189-1
21. StataCorp L. Stata: Data Analysis and Statistical Software. Special Edition Release. College Station, TX: StataCorp L (2007).
22. Ebrahimipour H, Vafaei Najjar A, Khani Jahani A, Pourtaleb A, Javadi M, Rezazadeh A, et al. Health system responsiveness: a case study of general hospitals in Iran. Int J Health Policy Manag (2013) 1(1):85–90. doi:10.15171/ijhpm.2013.13
23. Rashidian A, Kavosi Z, Majdzadeh R, Pourreza A, Pourmalek F, Arab M, et al. Assessing health system responsiveness: a household survey in 17th district of Tehran. Iran Red Crescent Med J (2011) 13(5):302–8.
24. Asghari SMH, Holakoei K, Majdzadeh R, Soleimani F, Amirsalari S. Health service utilization by mentally handicapped children and factors affecting it. Sci J Public Health Res (2007) 5(31–32):29–37.
25. Valentine NB, Ortiz JP, Tandon A, Kawabata K, Evans DB, Murray JL. Patient experiences with health services: population surveys from 16 OECD countries. Health Systems Performance Assessment: Debates, Methods and Empiricism. Geneva: World Health Organization (2003). p. 643–53.
26. Bergeson SC, Dean JD. A systems approach to patient-centered care. JAMA (2006) 296(23):2848–51. doi:10.1001/jama.296.23.2848
27. Hamann J, Cohen R, Leucht S, Busch R, Kissling W. Do patients with schizophrenia wish to be involved in decisions about their medical treatment? Am J Psychiatry (2005) 162(12):2382–4. doi:10.1176/appi.ajp.162.12.2382
28. Sharifi V. Urban mental health in Iran: challenges and future directions. Iran J Psychiatry Behav Sci (2009) 3(1):9–14.
29. Yasamy MT. Mental health challenges and possible solutions. East Mediterr Health J (2008) 14(Suppl):S114–22.
30. Singh-Manoux A, Adler NE, Marmot MG. Subjective social status: its determinants and its association with measures of ill-health in the Whitehall II study. Soc Sci Med (2003) 56(6):1321–33. doi:10.1016/S0277-9536(02)00131-4
31. Malhotra C, Do YK. Socio-economic disparities in health system responsiveness in India. Health Policy Plann (2012) 1:9. doi:10.1093/heapol/czs051
32. Willems S, De Maesschalck S, Deveugele M, Derese A, De Maeseneer J. Socio-economic status of the patient and doctor–patient communication: does it make a difference? Patient Educ Couns (2005) 56(2):139–46. doi:10.1016/j.pec.2004.02.011
33. Van Ryn M, Burke J. The effect of patient race and socio-economic status on physicians’ perceptions of patients. Soc Sci Med (2000) 50(6):813–28. doi:10.1016/S0277-9536(99)00338-X
34. Ergler CR, Sakdapolrak P, Bohle H-G, Kearns RA. Entitlements to health care: why is there a preference for private facilities among poorer residents of Chennai, India? Soc Sci Med (2011) 72(3):327–37. doi:10.1016/j.socscimed.2010.09.042
35. Dormohammadi T, Asghari F, Rashidian A. What do patients expect from their physicians? Iran J Public Health (2010) 39:70–7.
Keywords: responsiveness, mental health care, outpatient, social status, Iran
Citation: Forouzan S, Padyab M, Rafiey H, Ghazinour M, Dejman M and San Sebastian M (2016) Measuring the Mental Health-Care System Responsiveness: Results of an Outpatient Survey in Tehran. Front. Public Health 3:285. doi: 10.3389/fpubh.2015.00285
Received: 21 September 2015; Accepted: 21 December 2015;
Published: 27 January 2016
Edited by:
Samantha Battams, Torrens University Australia, AustraliaReviewed by:
Arash Javanbakht, University of Michigan, USAJulie Henderson, Flinders University, Australia
Copyright: © 2016 Forouzan, Padyab, Rafiey, Ghazinour, Dejman and San Sebastian. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) or licensor are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Setareh Forouzan, YXNmb3JvdXphbiYjeDAwMDQwO2dtYWlsLmNvbQ==