 Weisi Zeng
Weisi Zeng Jialan Xu1
Jialan Xu1
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Psychiatry , 27 February 2025
Sec. Anxiety and Stress Disorders
Volume 16 - 2025 | https://doi.org/10.3389/fpsyt.2025.1553290
Background: To evaluate the effect of virtual reality therapy on anxiety disorders in adolescents and adults by Meta-analysis
Methods: A comprehensive literature search was conducted by PubMed, Web of Science, Embase, CINAHL, Scopus, Cochrane (from inception to November 2024). Two researchers independently performed literature screening, quality evaluation and data extraction, and Stata16.0 and Review Man 5.4 software were used for Meta-analysis.
Results: A total of 33 studies involving 3182 adolescents and adults with anxiety disorders were included. The results of Meta-analysis showed that compared with conventional interventions, virtual reality therapy significantly improved the symptoms and level of anxiety in patients with anxiety disorder [SMD = -0.95, 95%CI (-1.22,-0.69), Z = 7.05, P < 0.00001].
Conclusion: The current findings suggest that VR therapy interventions have a positive effect on improving the anxiety state of patients with anxiety disorders. The aforementioned research findings must be confirmed by more high-caliber studies due to the number and quality limitations of the contained literature.
Systematic review registration: https://www.crd.york.ac.uk/prospero/display, identifier CRD42024574772.
Anxiety disorders can be classified as either substance/drug-induced or non-substance/drug-induced. Panic disorder, agoraphobia, separation anxiety disorder, social anxiety disorder, specific phobia, obsessive-compulsive disorder, generalized anxiety disorder, acute stress disorder, post-traumatic stress disorder, illness anxiety disorder, adjustment disorder with anxiety, and anxiety disorder resulting from physical diseases are among the categories of anxiety disorders that are not caused by substances (1). The two most prevalent forms of anxiety disorders are panic disorder and generalized anxiety disorder (2). Generalized anxiety disorder, another name for chronic anxiety disorder, is typified by persistent, excessive, and uncontrollable worrying. It can also be accompanied by a number of physical and psychological symptoms. Anxiety disorders are associated with high comorbidity rates, with 68% of GAD patients report having at least one other mental condition (2, 3). Recurrent, unplanned panic attacks are a hallmark of panic disorder, sometimes referred to as acute anxiety attacks (4, 5). Patients with panic disorder and generalized anxiety disorder continue to worry excessively and be overly vigilant, which is accompanied by considerable functional impairment. In extreme situations, it may cause severe autonomic symptoms, which lowers the quality of life for anxiety disorder sufferers (6). The intricate interaction of biological factors, environmental effects, and psychological mechanisms leads to anxiety (7). According to certain studies, state anxiety and trait anxiety are closely associated with patients who suffer from generalized anxiety disorder (8). The prevalence of anxiety disorders is currently estimated to be between 0.9% and 28.3% (9).
During this critical time in their physical and mental development, adolescents are particularly vulnerable to anxiety, sadness, and other negative feelings brought on by the demands of their studies, families, interpersonal relationship, and other aspects. Teenagers in a fast-paced world face stress from family dynamics, lifestyle changes, and academic demands, all of which have a negative impact on their mental health development (10). The prevalence of psychological issues among teenagers today is rising, including social phobia, depression, and anxiety. According to a 2015 meta-analysis of 41 research conducted in 27 different countries, between 11% and 16% of children and adolescents globally experience at least one mental health problem (11). Adolescents and adults with anxiety disorders have more serious social and educational impairments, and people with anxiety are at higher risk of smoking, substance abuse, obesity, and suicide. It is evident that anxiety and its associated problems significantly affect adults’ and teenagers’ lives and careers.
A variety of therapies, including as pharmaceutical, physical, and psychological ones, can considerably lessen the symptoms of anxiety. It has been demonstrated that mindfulness-based stress therapy (MBSR) and mindfulness-based cognitive therapy (MBCT), two therapies that have been adapted from mindfulness interventions, are successful in lowering anxiety (12–15). There is proof that fitness training and music therapy both have steadily improving impacts on anxiety (16, 17). Preclinical trials and investigations involving human subjects have also demonstrated the efficacy of repetitive transcranial magnetic stimulation’s anxiolytic effects (18). In addition, a meta-analysis showed (19) that pharmacotherapy, cognitive behavioral therapy, and a combination of the two treatment modalities all resulted in significant improvements before and after treatment, and that pharmacotherapy was equally effective as psychotherapy. Only a minority percentage of people receive Cognitive Behavior Therapy (CBT), despite the fact that it is the best first line of treatment for anxiety symptoms (20), and that numerous studies have shown its efficacy in treating anxiety-related diseases (21–24). Alternative methods of treating anxiety disorders are required in light of the acceptance of behavioral cognitive therapy (25).
Virtual reality (VR) is a brand-new technology developed since the 20th century. This computer technology synthetically simulates the environment and stimulates various senses through an immersive experience, allowing users to experience realistic, immersive feelings in a three-dimensional simulation (26) and helps people better regulate their emotions by diverting their attention from pain and anxiety (27). Immersion, interactivity, and imagination are the fundamental features of virtual reality technology. The most popular type of virtual reality is immersive virtual reality, which creates a multi-dimensional and multi-sensory virtual world. Through the use of virtual reality headset display devices and headphones, patients are separated from the outside world and sound, allowing their entire body and mind to be submerged in the dynamic visual virtual environment (28). Researches have demonstrated that the use of immersive head-mounted display displays can successfully divert patients’ focus by placing them in realistic scene settings and have a favorable intervention effect on the control of anxiety during surgery (29–33). Researchers in the field of psychology have also proposed virtual reality therapy (VRT). North et al. (34) defined VRT as “an effective treatment method by exposing clients to stimuli similar to those experienced in the real world through computer-generated virtual reality”. The use of virtual reality therapy has expanded beyond exposure therapy (35), to include behavioral cognitive therapy (36), art therapy (37), and sandplay therapy (38) due to the ongoing advancements in virtual reality technology. Simultaneously, VR technology is more widely accepted, has greater image quality, and is less expensive than standard treatment (39). According to one study, virtual reality exposure therapy (VRET) was favored by 76% of participants over conventional exposure therapy (40).
Virtual reality technology is currently being used progressively in the field of mental health, primarily for the clinical assessment and management of mental illnesses (41). It involves evaluating social functioning, behavioral ability, cognitive function, and symptoms (42–44). Patients can also receive mindfulness therapy, virtual reality exposure therapy, and cognitive rehabilitation (45, 46). Virtual reality therapy has emerged as a significant adjunctive treatment modality in the healthcare industry, with applications in pain management (47, 48) and the treatment of post-traumatic stress disorder (49). However, there is a dearth of scientifically supported data regarding the impact of virtual reality therapy interventions on patients suffering from anxiety disorders. This study uses meta-analysis to systematically evaluate the effect of virtual reality therapy in the treatment of patients with anxiety disorder, so as to provide evidence-based basis for researchers and clinicians.
This meta-analysis was completed in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement (50) and was registered with PROSPERO (Registration NO: CRD42024574772).
The researches on the application of artificial intelligence in adolescent mental illness were searched using medical specialty databases of PubMed, Web of Science, Embase, CINAHL, Scopus, Cochrane. The retrieval time was from the establishment of the database to September 2024. In addition, the references of the included literature were traced back to supplement the acquisition of relevant literature. Retrieve take subject and words combination of freedom. Search terms include: anxiety, angst, nervousness, anxiousness, anxiety disorder, adolescent, youth, VR, virtual reality immersion therapy, virtual reality therapy, virtual reality, etc. (The detailed search terms are provided in Supplementary Table S1).
Included studies were randomized controlled trials (RCTs) of adolescents and adults with a diagnosis of anxiety disorder, with no restrictions on population gender, course of illness, or ethnicity. The outcome measures included any clinically validated rating scale assessing change in symptoms or scores of anxiety disorders at post-treatment and follow-up, with a well-defined assessment methodology and measurements, such as the Hamilton Anxiety Scale(HAMA), the Self—Rating the Anxiety Scale(SAS), the Beck Anxiety Inventory(BAI), and others. The experimental group received a virtual reality-based intervention, while the control group received at least one non-virtual reality-based intervention, including cognitive behavior therapy(CBT), mindfulness therapy(MT), treatment as usual (TAU) or other interventions. Only articles in English were included.
All retrieved literature was imported into Endnote 20 software, duplicates were removed, and initial screening was performed by 2 researchers reading the titles and abstracts of the remaining literature according to the inclusion and exclusion criteria. After the initial screening the full text was read again to determine the final inclusion of literature. All relevant data were independently screened, extracted and cross-checked by two researchers (ZWS XJL), and each study included basic information about the study, participant characteristics, intervention, control group and data on outcome indicators.
All data were reviewed by a third researcher(YJY), and uncertainties or inconsistencies were resolved by discussion. For the literature lacking information, try to contact the original authors to supplement it.
The Cochrane Risk of Bias Assessment Tool was utilized to evaluate the risk and quality of the methodology. A total of six aspects of the included literature were used to evaluate the methodological quality and risk of bias: selection bias, implementation bias, measurement bias, follow-up bias, reporting bias and other biases. According to the evaluation criteria, a judgment was made for each study: “High” indicated that the methodology of the included study was incorrect and its quality was high. “Low” indicates that the methodology of the study was correct and the quality of the study was at low risk, while “Unclear” indicates that the current data are not sufficient to judge the correctness and quality of the methodology. The evaluation grade was A when the included literature fully satisfied the low risk of bias, indicating excellent literature quality; B when it partially satisfied the low risk of bias, indicating fair literature quality; and C when it fully failed to meet the low risk of bias, indicating poor literature quality.
Two researchers independently reviewed the screening procedure and quality evaluation to limit the subjectivity of the researchers and to ensure the credibility of the screening process. If there was a disagreement, it was settled through discussion, and a third party had to be involved in the decision-making process.
Review Man 5.4 software was used for data analysis. The 95% Confidence Interval (CI) for continuous variables was presented as either the Weighted Mean Difference (WMD) or the Standardized Mean Difference (SMD). For outcome data, the standardized mean difference (SMD) and 95% confidence interval (CI) were employed due to the nonuniformity of the scales utilized.
The Cochrane Q test was employed to gauge the degree of heterogeneity among the results of each study. The outcome data were homogeneous when P>0.1 and I2 ≤ 50%, and the fixed effect model was chosen to determine the combined effect size. When P ≤ 0.1 and I2>50%, the heterogeneity was considerable, and the reasons for heterogeneity could be found through baseline data, intervention measures, intervention time and other aspects. Descriptive analysis or subgroup analysis of effect sizes can be used to incorporate the heterogeneity caused by the aforementioned factors. The random-effects model was selected for investigation in the event that the source of heterogeneity could not be identified.
Stata16.0 software was used for sensitivity analysis. Egger’s test and funnel plot were used to assess publication bias.
A total of 4451 relevant studies were retrieved. The software Endnote 20 was used to import all of the recovered literature. After deleting the duplicate research, a total of 2903 relevant studies were found. After reviewing the study titles and abstracts, 2556 articles were rejected based on the inclusion and exclusion criteria of this investigation. After re-reading the full text of the literature that might meet the inclusion criteria, 314 studies were excluded, and 33 studies were finally included. Included in the study. Figure 1 depicts the precise procedure and outcomes of the literature screening
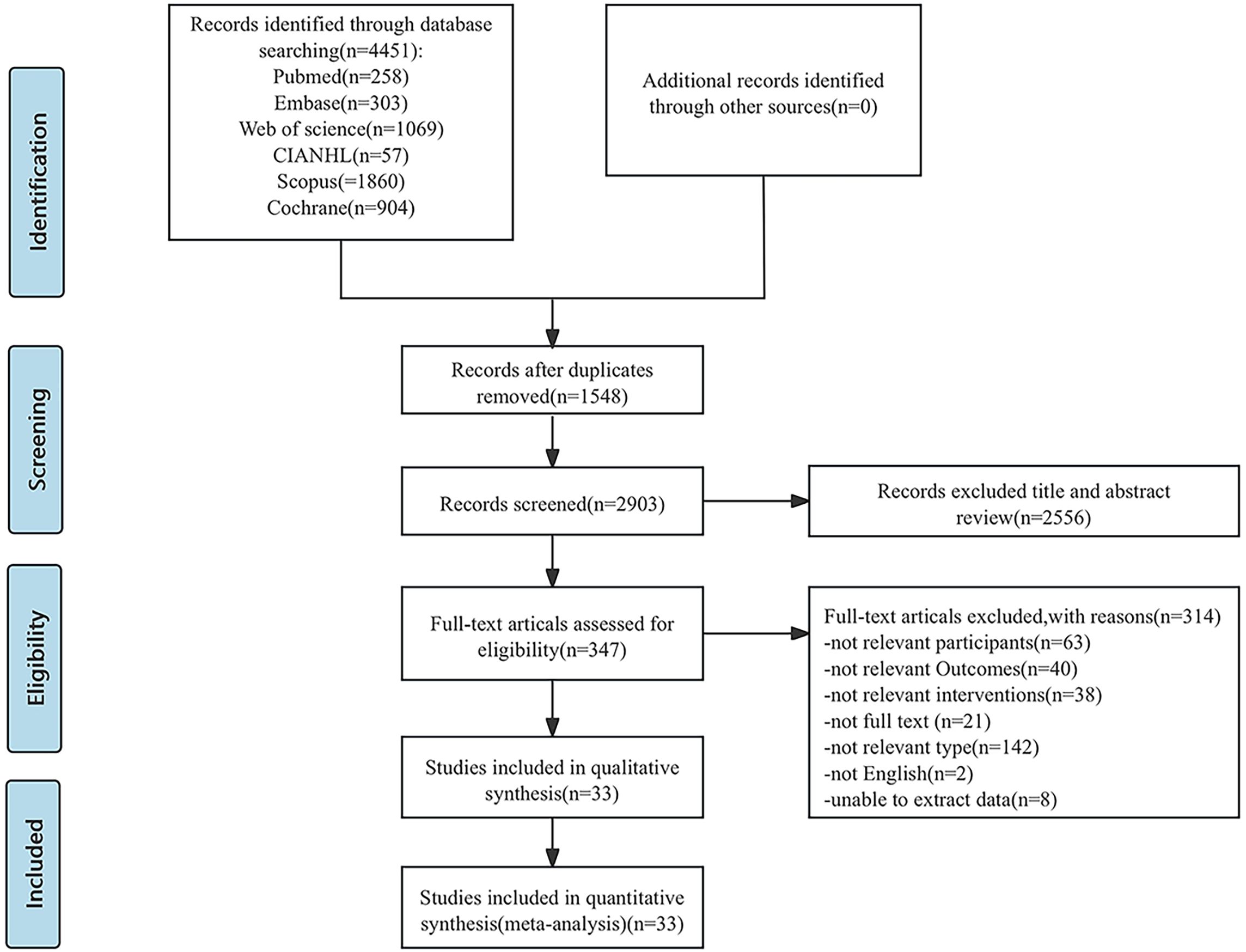
Figure 1. PRISMA flowchart: overview of in- and exclusion process. n, number.
A total of 33 articles (51–83) were included, published from 2019 to 2024, involving 3182 subjects from 18 countries, including the United States, China, and Iran etc. Out of the 33 included papers, 6 employ three-arm controlled studies (56, 57, 62, 71, 78, 80) and 27 employ two-arm controlled studies. Only two intervention groups were chosen for comparison since unit risk bias did not need to be taken into account with the three-arm controlled trial since each group was independent. One study had a low risk of bias, sixteen had an unclear risk of bias, and sixteen had a high risk of bias out of the 33 included studies. There is a significant risk of implementation bias and measurement bias because most studies cannot be completely double-blind due to the requirement for virtual reality equipment in VR therapy. At the same time, the risk of bias in the selection of the included literature is also high, which could be brought on by inconsistent investigation methods and a lack of representative samples. The basic characteristics of the included literature are shown in Table 1. The results of the risk of bias evaluation of the included studies are shown in Figure 2 (The risk of bias summary is provided in Supplementary Figure S2).
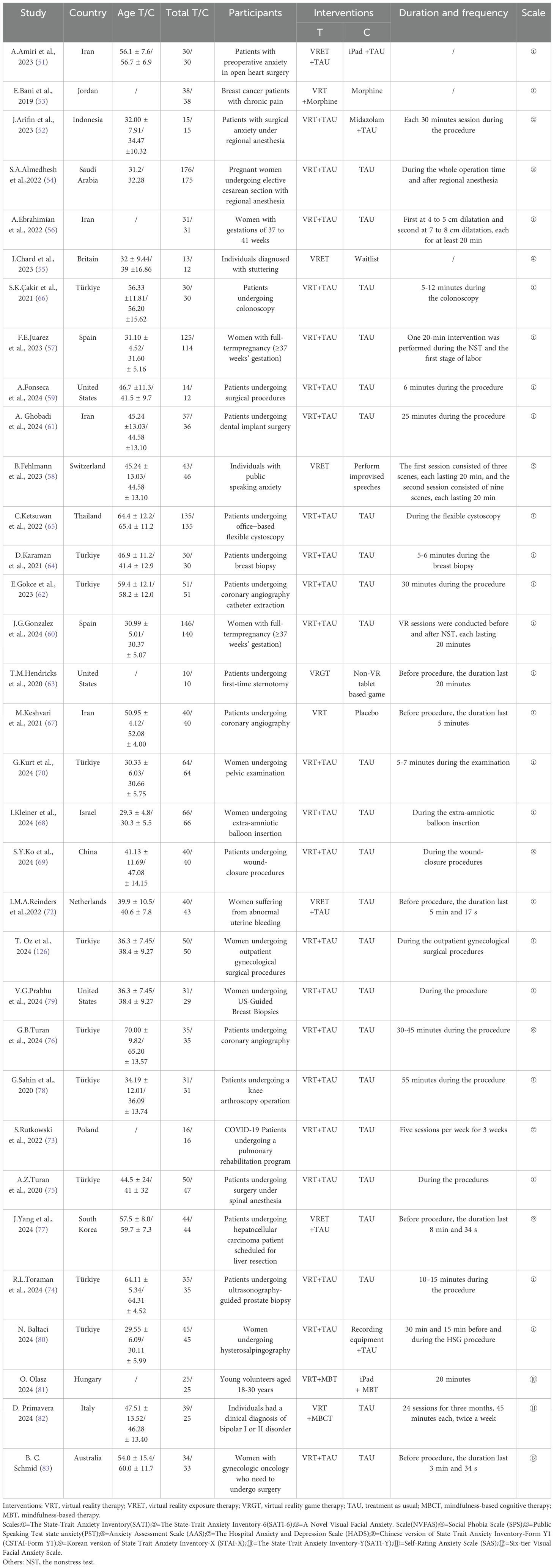
Table 1. Characteristics of 33 studies included in the meta-analysis.
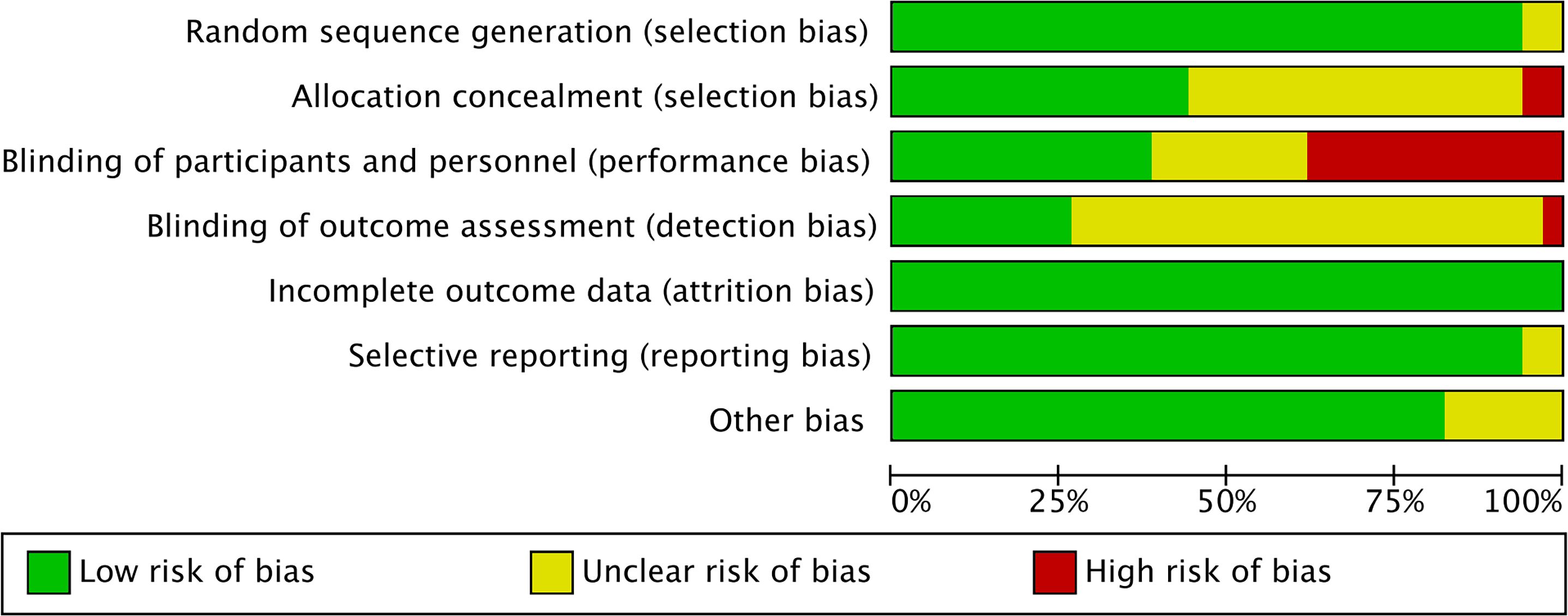
Figure 2. Risk of bias graph.
Among The 33 studies, 26 assessed anxiety levels using the State-Trait Anxiety Inventory (SATI); 4 of these studies (52, 69, 77, 81) used different versions of the SATI, which were combined for analysis because the scoring methodology was the same; and 7 studies assessed anxiety levels using other instruments. Because evaluation tools varied widely, the standardized mean difference (SMD) was selected for effect size pooling. The results demonstrated that the analysis were statistically significant[SMD = -0.95, 95%CI (-1.22, -0.69), Z = 7.05, P < 0.00001], but there was significant heterogeneity among the studies (I2 = 91%, P < 0.00001) as shown in Figure 3. As illustrated in Figure 4, the results of the sensitivity analysis revealed that 11 studies (53, 54, 68, 71, 72, 74–77, 80, 83) significantly influenced the outcomes, while the remaining studies had minimal effects. Because of variations in sample numbers, virtual reality tools and techniques, assessment timing, intervention durations, and anxiety measures utilized in each study, we discovered an additional source of heterogeneity after taking into account all of the aforementioned variations. The heterogeneity was much decreased after these 2 studies(56 (69), were eliminated(I2 = 44%, P=0.02).According to the analysis’s findings, the difference was statistically significant [SMD = -0.76, 95%CI (-0.86,-0.67), Z = 15.59, P < 0.00001], suggesting that VRT could lower anxiety levels in patients with anxiety disorders when compared to the control group (As shown in Supplementary Figure S3).
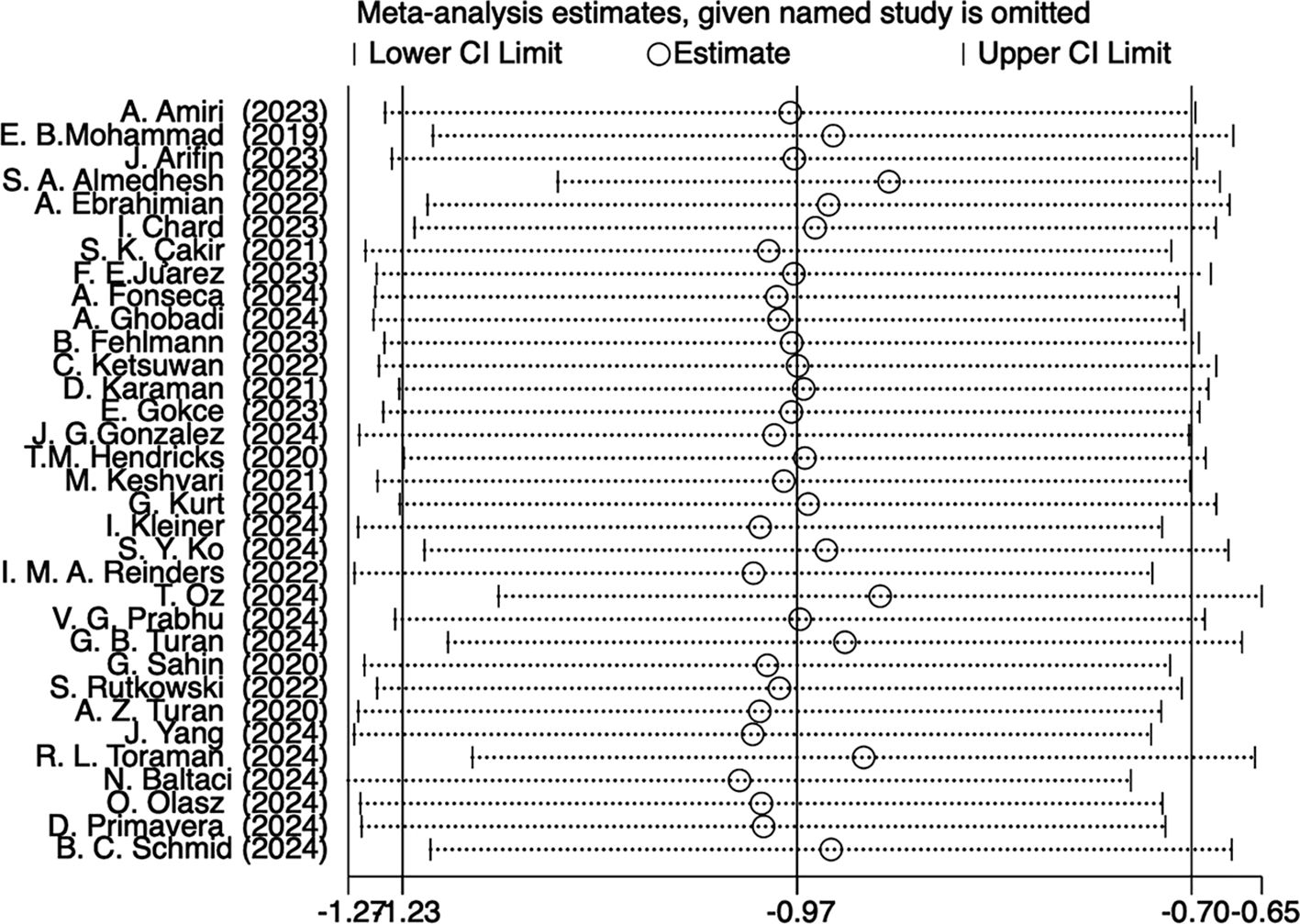
Figure 3. Forest plot.
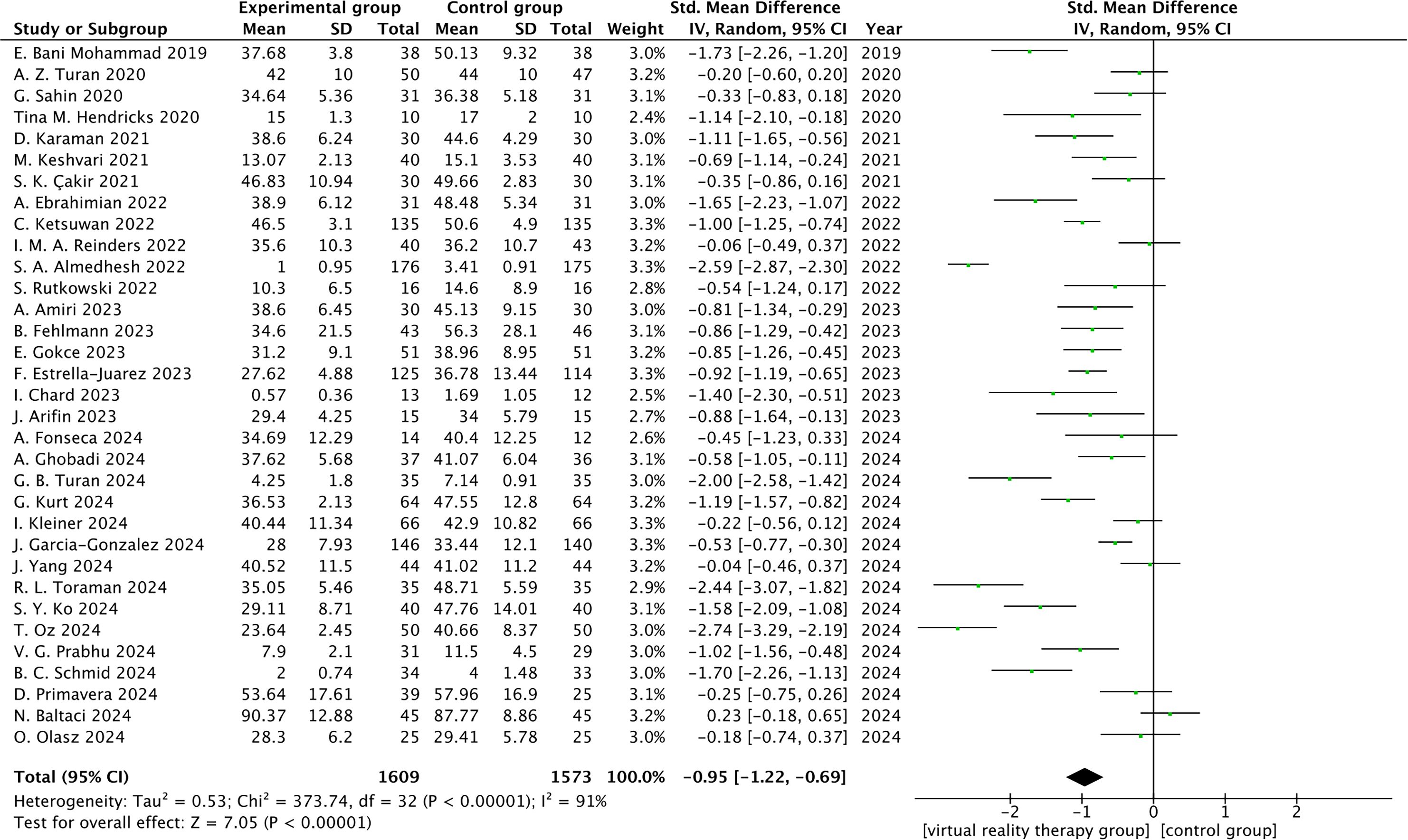
Figure 4. Sensitivity analysis plot.
Subgroup analysis was carried out based on the patients’ age, gender, anxiety type, and scale, their place of origin, as well as intervention type for the Experimental group and control group. All of these factors affected the virtual reality treatment intervention effect, and the South American intervention effect was the most significant, according to the results of the subgroup analysis. The source of heterogeneity, however, is unclear and could be related to the various virtual reality devices used in the intervention, the duration of the intervention, the videos viewed by the devices, the sample sizes, and whether or not other therapies were combined. The comprehensive findings are displayed in Table 2.

Table 2. Effects of virtual reality therapy on anxiety disorders subgroup analysis.
The findings of the publication bias test, which was applied to the 33 publications in this study, indicated that there might be publication bias because the funnel plot was somewhat asymmetrical, as shown in Figure 5. Nevertheless, there was no discernible publication bias according to Egger’s test (P = 0.731).
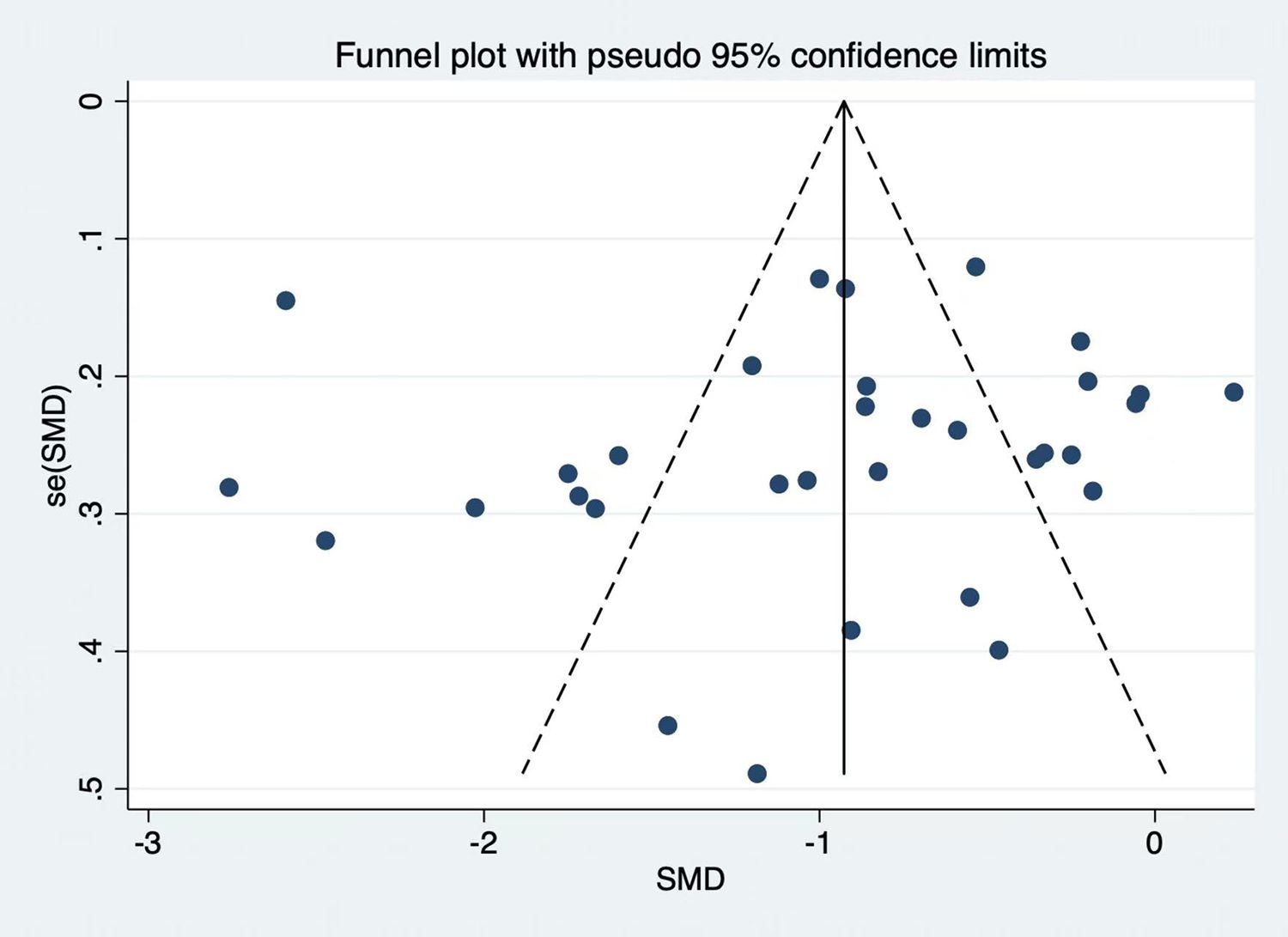
Figure 5. Funnel plot of publication bias.
This meta-analysis evaluated virtual reality therapy’s (VRT) effectiveness in treating anxiety disorders. The criteria for inclusion were met by 33 studies, all of which were randomized controlled trials. Of these, 27 studies included an inactive control group that received usual treatment (i.e., participants received usual medication, health education, and usual care), waitlist, or placebo. Six studies’ control group included active intervention, which included presenting the experimenter with a public speech, utilizing an iPad for preoperative health education, using a tablet device to perform mindfulness exercises, listening to nature sounds using a recording device, and using a non-VR video game. This study examined the impact of virtual reality treatment on individuals with anxiety disorders and came to the conclusion that virtual reality-based interventions can lessen anxiety and help patients with anxiety disorders feel better[SMD = -0.95, 95%CI (-1.22,-0.69), Z = 7.05, P < 0.00001]. Simultaneously, the meta-analysis expanded the VR-based interventions, limited the participants’ condition kinds, and became more focused. Of the 33 included studies, participants’ anxiety types included perioperative anxiety in 21 studies, perinatal anxiety in 3 studies, anxiety during a medical examination in 3 studies, anxiety related to their own illness in 2 studies, public speaking anxiety in 1 study, bipolar disorder related anxiety in 1 study and social anxiety in 2 study. In addition, all 33 eligible studies were published within the last 5 years, which may reflect the development of virtual reality technology and its application in the field of mental health as a research hotspot in recent years. Notably, there is conflicting evidence about VR’s ability to reduce perioperative anxiety. Some studies have shown that VR therapy does not reduce perioperative anxiety (84–86), while others have shown some positive effects (87–91). Three previous studies have shown that virtual reality therapy has been used in patients before surgery with significant results, especially in children (90–92). The inconsistency in the results of these studies may be due to the use of different anxiety scales. The most widely used measure for assessing perioperative anxiety is the Spielberger State and Trait Anxiety Inventory (STAI). Some more focused measures are the Yale Preoperative Anxiety Scale (93), the Amsterdam Perioperative Anxiety and Information Scale (94), the State-Trait Operation Anxiety (95), and others. These scales differ in terms of item content, questionnaire length, and scoring standards, all of which will affect the study’s findings. Therefore, when assessing the effectiveness of VR intervention on perioperative anxiety, it is necessary to take into account the usage of various scales.
Because mental health issues are inextricably linked to their surroundings, individuals can use an interactive virtual reality environment to see whether treatment is feasible. The treatment of mental illnesses has made extensive use of virtual reality in recent years. Distraction therapy and exposure therapy are among the therapeutic modalities. Virtual reality technology plays a major role in treating anxiety disorders by creating an exposure environment. By exposing anxious individuals to frightening stimuli or scenes, virtual reality exposure treatment might help them become desensitized to and eventually eradicate their fear. It has been demonstrated that this method works well for treating some phobias, including panic disorder (PD), social anxiety disorder (SAD), post-traumatic stress disorder (PTSD), and generalized anxiety disorder (GAD) (96).Conventional exposure therapy requires the presentation of real-world stimuli; however, certain stimuli, like driving, flying, altitude, etc., are extremely risky and unlikely to occur in the actual world. Furthermore, it is not practical to use typical exposure therapy for postwar trauma. As a result, virtual reality exposure therapy can effectively compensate for the limited circumstances and incomplete treatment of traditional exposure therapy. In contrast to traditional imagined exposure therapy, virtual reality exposure therapy, according to Emmelkamp et al. (97), can help patients visualize stimuli and environments that they are unable to accept by simulating real experiences and offering personalized and unique scenes for exposure therapy. Park et al. (98) think that virtual reality technology can give psychotherapists a safe, controlled, and controllable environment, increasing the viability and efficacy of exposure treatment. In order to help patients who are afraid of heights learn to overcome their phobia, Hong et al. (99) employed virtual reality to imitate high altitude. Zainal (100), Premkumar (101), Rubin (102) and others used VRET to help people with social anxiety overcome speech anxiety, and the treatment effect was relatively stable after 4 to 6 years of follow-up. The majority of research on VRET’s application in treating PTSD has been on war, auto accidents, and terrorist incidents (103–105). Lehoux et al. (106) used virtual reality to treat substance use disorders (SUD). Additionally, virtual reality was employed by Riva et al. and Corno et al. (107, 108) to treat people with eating disorders. The treatment of obsessive-compulsive disorder has also benefited from advancements in virtual reality technology. Javaherirenani et al. (109) verified that treating patients with clean pollution-induced obsessive-compulsive disorder with virtual exposure therapy is feasible.
According to Stanney et al. (110), over 80% of VR users encounter some related negative effects, despite the fact that the advantages of VR have been extensively documented in the literature. Potential negative health impacts of VR exposure have also been noted in a number of earlier research (111, 112). Health issues include adverse symptoms include nausea and vertigo, confusion, and exhaustion of the muscles (113). Meanwhile, extended usage of VR devices can raise the risk of nearsightedness or hyperopia and cause eye strain, dryness, and impaired vision (114). Macular degeneration is more likely to occur if blue light from VR device screens damages retinal cells over time (115). Long-term VR immersion can also result in psychological issues including addiction, social anxiety, depression, and phobias, as well as physical issues like brain fatigue, neurasthenopia, poor focus, and memory loss (116). Aside from potential health risks, VR-related side effects may also detract from the user experience.
In distraction intervention therapy, virtual reality takes advantage of the features of its 3D reality environment to draw patients’ attention away from the things that make them anxious or in pain in order to alleviate such symptoms. Using VR virtual reality equipment, the intervention content of distraction therapy is different. For example, children’s puncture process can be used to divert their attention, lower their anxiety and fear, and significantly increase the puncture success rate by using VR equipment to enjoy music, movies, animations, games, or exposure to the beach and other natural environments (117–119). Apart from its use in children, virtual reality-based distraction therapy has also been applied to adult cancer patients in hospitals to manage anxiety (120–122). In Bani et al.’s study (121), for instance, hospitalized patients with breast cancer during chemotherapy were assisted using VR virtual reality equipment. Current anxiety can be reduced by diverting the patient’s focus from the stressor’s acute stimulus. It has not been proven whether distraction therapy’s ability to reduce anxiety has a long-lasting effect, and the patient’s anxiety may return once they are back in the real world without the interactive environmental stimulation that VR technology offers. Thus, In order to continually alleviate patients’ anxiety symptoms, enhance their degree of adaptability, and encourage them to adjust as quickly as possible to subsequent stresses, it is necessary to improve the intervention content of VR equipment. Since VR virtual reality equipment can create a simulated three-dimensional environment, patients can be temporarily removed from stressful situations. The 3D scene that the equipment provides can also serve as a setting for mindfulness meditation, allowing patients to focus on mindfulness meditation exercises and improving their cognitive abilities to deal with illnesses or negative emotions. Adapt to stressors as quickly as possible. The effectiveness of mindfulness meditation interventions has been demonstrated to be improved by VR technology. For example, in a study by Lee et al. (123), critically ill patients’ sleep quality was enhanced by using VR virtual reality technology in conjunction with mindfulness meditation, increased the mindfulness meditation intervention’s impact significantly. Nevertheless, VR-based mindfulness research in non-clinical populations is still in its early stages, and future advancements in experimental research design, psychometric tools and indicators, and technical equipment operation are required (124).
In conclusion, the use of virtual reality technology in treatment is growing in popularity and affordability as a result of technological advancements (125). Virtual reality technology, on the other hand, has demonstrated great potential in the assessment and management of anxiety disorders and compensates for many of the drawbacks of conventional approaches. Nonetheless, there are a few things that the current study has to take into account. First and foremost is the patient’s sense of presence. The sense of presence is not only an important metric for analyzing virtual reality technology, but it also plays a significant role in generating dread and panic and finally achieving the intended therapeutic effect. However, few studies have considered the impact of context on the outcome of assessment and treatment. Second, the research should take into account any potential negative effects that virtual reality technology may have on some patients, such as nausea and vertigo.
The majority of current research is still in the preliminary stages of investigation, and more research is required to determine whether virtual reality may be used effectively in the future to diagnose and treat anxiety disorders. In terms of evaluation, the first step is to standardize the VR evaluation procedure in order to establish a comparatively fixed process or model and to elucidate its validity and reliability. Second, more physiological indicators, like heart rate, blood pressure and brain nerve activity, can be combined in the future to examine the relationship between cognitive, behavioral, and physiological indicators because VR can be compatible with other technologies, such as eye movement, electroencephalography (EEG), and brain imaging technologies. Regarding treatment, in order to further validate the effectiveness of VRT on anxiety disorders, a bigger sample size, the inclusion of various patient subtypes, a more rigorous experimental design conducted under controlled conditions, and the combination of pertinent physiological indicators are required; Second, additional research is required to examine the viability and efficacy of VRT in clinical settings. Third, long-term follow-up data are required to observe the effect of VRT on patient treatment. Fourth, in order to properly direct the design of virtual reality, additional research is required to understand the causal relationship between the sense of presence and anxiety, as this is a significant factor influencing patients’ worry and terror. Fifth, VRT still requires the participation of therapists, which means limited treatment duration and high significant treatment expenses. In the future, the participation of therapists and the threshold of treatment can be reduced (such as app and recorded instructions), so that more people can receive evidence-based psychotherapy. Furthermore, considering the possible negative effects of virtual reality, the duration of use can be appropriately controlled, and the device can be removed in time to rest after dizziness and other discomfort symptoms occur. From the perspective of VR designers, future products can be equipped with chips with stronger computing power to reduce delay and reduce the sense of vertigo when using VR equipment as much as possible. It can also make VR equipment lighter and more ergonomic to further improve user wearing comfort. In addition, user health systems can be developed to monitor user experience in real time. Finally, to further investigate the therapeutic effects of VRT, future studies could concentrate on analyzing and measuring the impact of VR devices alone on mental health as opposed to in conjunction with other psychotherapy techniques.
According to available data, VRT is a successful treatment for anxiety disorders. It also lessens the symptoms of anxiety disorders, albeit it is not a complete improvement over traditional treatment. The number and caliber of the included studies place restrictions on the aforementioned research findings. More focused, large-sample, high-quality research on many kinds of anxiety disorders is required in the future for verification.
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author.
WZ: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Writing – original draft, Writing – review & editing. JX: Data curation, Formal analysis, Methodology, Writing – review & editing. JY: Data curation, Writing – review & editing. XC: Project administration, Supervision, Writing – review & editing.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declare that no Generative AI was used in the creation of this manuscript.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2025.1553290/full#supplementary-material
Supplementary Figure 2 | Risk of bias summary.
Supplementary Figure 3 | Forest plot after sensitivity analysis.
1. APA Presidential Task Force on Evidence-Based Practice. Evidence-based practice in psychology. Am Psychol. (2006) 61:271–85. doi: 10.1037/0003-066X.61.4.271
2. Katzman MA, Bleau P, Blier P, Chokka P, Kjernisted K, Van Ameringen M, et al. Canadian clinical practice guidelines for the management of anxiety, posttraumatic stress and obsessive-compulsive disorders. BMC Psychiatry. (2014) 14 Suppl 1:S1. doi: 10.1186/1471-244X-14-S1-S1
3. Showraki M, Showraki T, Brown K. Generalized anxiety disorder: revisited. Psychiatr Q. (2020) 91:905–14. doi: 10.1007/s11126-020-09747-0
4. Chen MH, Tsai SJ. Treatment-resistant panic disorder: clinical significance, concept and management. Prog Neuropsychopharmacol Biol Psychiatry. (2016) 70:219–26. doi: 10.1016/j.pnpbp.2016.02.001
5. Lo YC, Chen HH, Huang SS. Panic disorder correlates with the risk for sexual dysfunction. J Psychiatr Pract. (2020) 26:185–200. doi: 10.1097/PRA.0000000000000460
6. Schiele MA, Domschke K. Epigenetics at the crossroads between genes, environment and resilience in anxiety disorders. Genes Brain Behav. (2018) 17:e12423. doi: 10.1111/gbb.2018.17.issue-3
7. Taylor DJ, Lichstein KL, Durrence HH. Insomnia as a health risk factor. Behav Sleep Med. (2003) 1:227–47. doi: 10.1207/S15402010BSM0104_5
8. Huang Y, Wang Y, Wang H, Liu Z, Yu X, Yan J, et al. Prevalence of mental disorders in China: a cross-sectional epidemiological study. Lancet Psychiatry. (2019) 6:211–24. doi: 10.1016/S2215-0366(18)30511-X
9. Baxter AJ, Scott KM, Vos T, Whiteford HA. Global prevalence of anxiety disorders: a systematic review and meta-regression. Psychol Med. (2013) 43:897–910. doi: 10.1017/S003329171200147X
10. Cheng H, Hayes D, Edbrooke-Childs J, Martin K, Chapman L, Wolpert M. What approaches for promoting shared decision-making are used in child mental health? A scoping review. Clin Psychol Psychother. (2017) 24:O1495–o511. doi: 10.1002/cpp.v24.6
11. Charlson FJ, Baxter AJ, Cheng HG, Shidhaye R, Whiteford HA. The burden of mental, neurological, and substance use disorders in China and India: a systematic analysis of community representative epidemiological studies. Lancet. (2016) 388:376–89. doi: 10.1016/S0140-6736(16)30590-6
12. Newland P, Bettencourt BA. Effectiveness of mindfulness-based art therapy for symptoms of anxiety, depression, and fatigue: A systematic review and meta-analysis. Complement Ther Clin Pract. (2020) 41:101246. doi: 10.1016/j.ctcp.2020.101246
13. Janssen M, Heerkens Y, Kuijer W, van der Heijden B, Engels J. Effects of Mindfulness-Based Stress Reduction on employees' mental health: A systematic review. PLoS One. (2018) 13:e0191332. doi: 10.1371/journal.pone.0191332
14. Goldberg SB, Tucker RP, Greene PA, Davidson RJ, Wampold BE, Kearney DJ, et al. Mindfulness-based interventions for psychiatric disorders: A systematic review and meta-analysis. Clin Psychol Rev. (2018) 59:52–60. doi: 10.1016/j.cpr.2017.10.011
15. Yıldırım D, Çiriş Yıldız C. The effect of mindfulness-based breathing and music therapy practice on nurses' Stress, work-related strain, and psychological well-being during the COVID-19 pandemic: A randomized controlled trial. Holist Nurs Pract. (2022) 36:156–65. doi: 10.1097/HNP.0000000000000511
16. Bradt J, Dileo C, Myers-Coffman K, Biondo J. Music interventions for improving psychological and physical outcomes in people with cancer. Cochrane Database Syst Rev. (2021) 10:Cd006911. doi: 10.1002/14651858.CD006911.pub4
17. Philippot A, Dubois V, Lambrechts K, Grogna D, Robert A, Jonckheer U, et al. Impact of physical exercise on depression and anxiety in adolescent inpatients: A randomized controlled trial. J Affect Disord. (2022) 301:145–53. doi: 10.1016/j.jad.2022.01.011
18. Hutton TM, Aaronson ST, Carpenter LL, Pages K, West WS, Kraemer C, et al. The anxiolytic and antidepressant effects of transcranial magnetic stimulation in patients with anxious depression. J Clin Psychiatry. (2023) 84(1):22m14571. doi: 10.4088/JCP.22m14571
19. Bandelow B, Seidler-Brandler U, Becker A, Wedekind D, Rüther E. Meta-analysis of randomized controlled comparisons of psychopharmacological and psychological treatments for anxiety disorders. World J Biol Psychiatry. (2007) 8:175–87. doi: 10.1080/15622970601110273
20. Coventry PA, Meader N, Melton H, Temple M, Dale H, Wright K, et al. Psychological and pharmacological interventions for posttraumatic stress disorder and comorbid mental health problems following complex traumatic events: Systematic review and component network meta-analysis. PLoS Med. (2020) 17:e1003262. doi: 10.1371/journal.pmed.1003262
21. Hertenstein E, Trinca E, Wunderlin M, Schneider CL, Züst MA, Fehér KD, et al. Cognitive behavioral therapy for insomnia in patients with mental disorders and comorbid insomnia: A systematic review and meta-analysis. Sleep Med Rev. (2022) 62:101597. doi: 10.1016/j.smrv.2022.101597
22. Carpenter JK, Andrews LA, Witcraft SM, Powers MB, Smits JAJ, Hofmann SG. Cognitive behavioral therapy for anxiety and related disorders: A meta-analysis of randomized placebo-controlled trials. Depress Anxiety. (2018) 35:502–14. doi: 10.1002/da.2018.35.issue-6
23. Bhattacharya S, Goicoechea C, Heshmati S, Carpenter JK, Hofmann SG. Efficacy of cognitive behavioral therapy for anxiety-related disorders: A meta-analysis of recent literature. Curr Psychiatry Rep. (2023) 25:19–30. doi: 10.1007/s11920-022-01402-8
24. Lundin J, Lundström A, Gulliksen J, Blendulf J, Ejeby K, Nyman H, et al. Using 360-degree videos for virtual reality exposure in CBT for panic disorder with agoraphobia: a feasibility study. Behav Cognit Psychother. (2022) 50:158–70. doi: 10.1017/S1352465821000473
25. Carl E, Stein AT, Levihn-Coon A, Pogue JR, Rothbaum B, Emmelkamp P, et al. Virtual reality exposure therapy for anxiety and related disorders: A meta-analysis of randomized controlled trials. J Anxiety Disord. (2019) 61:27–36. doi: 10.1016/j.janxdis.2018.08.003
26. Rash I, Helgason M, Jansons D, Mitchell L, Sakakibara BM. The influence of a virtual reality entertainment program on depressive symptoms and sedentary behavior in inpatient stroke survivors: a research protocol for a pilot randomized controlled trial. Pilot Feasibility Stud. (2022) 8:230. doi: 10.1186/s40814-022-01189-8
27. Lepilkina T, Beniashvili AG, Cheremin RA, Malyukova NG, Morozova MA, Bogdanov MA, et al. Efficacy of a relaxation scenario in virtual reality for the comorbid symptoms of anxiety and asthenia in a general hospital setting: A pilot comparative randomized open-label study. Consort Psychiatr. (2023) 4:38–51. doi: 10.17816/CP.202341
28. Guan H, Xu Y, Zhao D. Application of virtual reality technology in clinical practice, teaching, and research in complementary and alternative medicine. Evid Based Complement Alternat Med. (2022) 2022:1373170. doi: 10.1155/2022/1373170
29. Hermans ANL, Betz K, Verhaert DVM, den Uijl DW, Clerx K, Debie L, et al. 360° Virtual reality to improve patient education and reduce anxiety towards atrial fibrillation ablation. Europace. (2023) 25:855–62. doi: 10.1093/europace/euac246
30. Kim Y, Yoo SH, Chun J, Kim JH, Youn YH, Park H. Relieving anxiety through virtual reality prior to endoscopic procedures. Yonsei Med J. (2023) 64:117–22. doi: 10.3349/ymj.2022.0319
31. Matthie NS. The management of chronic pain in sickle cell disease: an interview with Nadine Matthie. Pain Manage. (2023) 13:71–5. doi: 10.2217/pmt-2022-0097
32. Breed HJ, Jones E, Cubitt J. Use of immersive virtual reality to reduce anxiety during complex pediatric dressing changes. BMJ Case Rep. (2023) 16(2):e252998. doi:10.1136/bcr-2022-252998
33. Lacy BE, Cangemi DJ, Spiegel BR. Virtual reality: A new treatment paradigm for disorders of gut-brain interaction? Gastroenterol Hepatol (N Y). (2023) 19:86–94.
34. North MM, North SM, Coble JR. Virtual reality therapy: an effective treatment for psychological disorders. Stud Health Technol Inform. (1997) 44:59–70.
35. Kothgassner OD, Reichmann A, Bock MM. Virtual reality interventions for mental health. Curr Top Behav Neurosci. (2023) 65:371–87. doi: 10.1007/7854_2023_419
36. Yang C, Sander F, Helmert JR, Weiss C, Weitz J, Reissfelder C, et al. Cognitive and motor skill competence are different: Results from a prospective randomized trial using virtual reality simulator and educational video in laparoscopic cholecystectomy. Surgeon. (2023) 21:78–84. doi: 10.1016/j.surge.2022.03.001
37. Tieri G, Iosa M, Fortini A, Aghilarre F, Gentili F, Rubeca C, et al. Efficacy of a virtual reality rehabilitation protocol based on art therapy in patients with stroke: A single-blind randomized controlled trial. Brain Sci. (2024) 14(9):863. doi: 10.3390/brainsci14090863
38. Hirose M, Kijima R, Shirakawa K, Nihei K. Development of a virtual sand box: an application of virtual environment for psychological treatment. Stud Health Technol Inform. (1997) 44:113–20.
39. Miloff A, Lindner P, Hamilton W, Reuterskiöld L, Andersson G, Carlbring P. Single-session gamified virtual reality exposure therapy for spider phobia vs. traditional exposure therapy: study protocol for a randomized controlled non-inferiority trial. Trials. (2016) 17:60. doi: 10.1186/s13063-016-1171-1
40. Lau CKY, Saad A, Camara B, Rahman D, Bolea-Alamanac B. Acceptability of digital mental health interventions for depression and anxiety: systematic review. J Med Internet Res. (2024) 26:e52609. doi: 10.2196/52609
41. Riva G, Serino S. Virtual reality in the assessment, understanding and treatment of mental health disorders. J Clin Med. (2020) 9(11):3434. doi: 10.3390/jcm9113434
42. Pieri L, Tosi G, Romano D. Virtual reality technology in neuropsychological testing: A systematic review. J Neuropsychol. (2023) 17:382–99. doi: 10.1111/jnp.12304
43. Chan KC, Hui CL, Suen YN, Lee EH, Chang WC, Chan SK, et al. Application of immersive virtual reality for assessment and intervention in psychosis: A systematic review. Brain Sci. (2023) 13(3):471. doi: 10.3390/brainsci13030471
44. Wiebe A, Kannen K, Selaskowski B, Mehren A, Thöne AK, Pramme L, et al. Virtual reality in the diagnostic and therapy for mental disorders: A systematic review. Clin Psychol Rev. (2022) 98:102213. doi: 10.1016/j.cpr.2022.102213
45. Zhai K, Dilawar A, Yousef MS, Holroyd S, El-Hammali H, Abdelmonem M. Virtual reality therapy for depression and mood in long-term care facilities. Geriatrics (Basel). (2021) 6(2):58. doi: 10.20944/preprints202104.0280.v1
46. Benchimol-Elkaim B, Khoury B, Tsimicalis A. Nature-based mindfulness programs using virtual reality to reduce pediatric perioperative anxiety: a narrative review. Front Pediatr. (2024) 12:1334221. doi: 10.3389/fped.2024.1334221
47. Tas FQ, van Eijk CAM, Staals LM, Legerstee JS, Dierckx B. Virtual reality in pediatrics, effects on pain and anxiety: A systematic review and meta-analysis update. Pediatr Anesth. (2022) 32:1292–304. doi: 10.1111/pan.v32.12
48. Dreesmann NJ, Su H, Thompson HJ. A systematic review of virtual reality therapeutics for acute pain management. Pain Manag Nurs. (2022) 23:672–81. doi: 10.1016/j.pmn.2022.05.004
49. Schröder D, Wrona KJ, Müller F, Heinemann S, Fischer F, Dockweiler C. Impact of virtual reality applications in the treatment of anxiety disorders: A systematic review and meta-analysis of randomized-controlled trials. J Behav Ther Exp Psychiatry. (2023) 81:101893. doi: 10.1016/j.jbtep.2023.101893
50. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Bmj. (2021) 372:n71. doi: 10.1136/bmj.n71
51. Amiri A, Jalali R, Salari N. The effect of using virtual reality technology on anxiety and vital signs before surgery in patients undergoing open heart surgery. Perioper Med (Lond). (2023) 12:62. doi: 10.1186/s13741-023-00354-8
52. Arifin J, Mochamat M, Pramadika T, Paramita D, Nurcahyo WI. Effects of immersive virtual reality on patient anxiety during surgery under regional anesthesia: A randomized clinical trial. Anesth Pain Med. (2023) 13:e130790. doi: 10.5812/aapm-130790
53. Bani Mohammad E, Ahmad M. Virtual reality as a distraction technique for pain and anxiety among patients with breast cancer: A randomized control trial. Palliat Support Care. (2019) 17:29–34. doi: 10.1017/S1478951518000639
54. Almedhesh SA, Elgzar WT, Ibrahim HA, Osman HA. The effect of virtual reality on anxiety, stress, and hemodynamic parameters during cesarean section. Saudi Med J. (2022) 43:360–9. doi: 10.15537/smj.2022.43.4.20210921
55. Chard I, Van Zalk N, Picinali L. Virtual reality exposure therapy for reducing social anxiety in stuttering: A randomized controlled pilot trial. Front Digit Health. (2023) 5:1061323. doi: 10.3389/fdgth.2023.1061323
56. Ebrahimian A, Bilandi RR, Bilandī MRR, Sabzeh Z. Comparison of the effectiveness of virtual reality and chewing mint gum on labor pain and anxiety: a randomized controlled trial. BMC Pregnancy Childbirth. (2022) 22:49. doi: 10.1186/s12884-021-04359-3
57. Estrella-Juarez F, Requena-Mullor M, Garcia-Gonzalez J, Lopez-Villen A, Alarcon-Rodriguez R. Effect of virtual reality and music therapy on the physiologic parameters of pregnant women and fetuses and on anxiety levels: A randomized controlled trial. J Midwifery Womens Health. (2023) 68:35–43. doi: 10.1111/jmwh.13413
58. Fehlmann B, Mueller FD, Wang N, Ibach MK, Schlitt T, Bentz D, et al. Virtual reality gaze exposure treatment reduces state anxiety during public speaking in individuals with public speaking anxiety: a randomized controlled trial. J Affect Disord Rep. (2023) 14:100627. doi: 10.1016/j.jadr.2023.100627
59. Fonseca A, Qian D, Forbes T, Li BS, Lee C, Burdsall K, et al. Reducing preoperative caregiver anxiety with virtual reality: A pragmatic, randomized controlled study. J Patient Exp. (2024) 11:23743735231220190. doi: 10.1177/23743735231220190
60. García-González J, Martínez-Navarro A, Romero-Del-Rey R, Requena-Mullor M, Zheng R, Lopez-Villen A, et al. State-trait anxiety levels and vital signs of pregnant women following intervention with virtual reality during the nonstress test: A randomized controlled trial. J Affect Disord. (2024) 355:308–14. doi: 10.1016/j.jad.2024.03.148
61. Ghobadi A, Moradpoor H, Sharini H, Khazaie H, Moradpoor P. The effect of virtual reality on reducing patients' anxiety and pain during dental implant surgery. BMC Oral Health. (2024) 24:186. doi: 10.1186/s12903-024-03904-8
62. Gökçe E, Arslan S. Effects of virtual reality and acupressure interventions on pain, anxiety, vital signs and comfort in catheter extraction processes for patients undergoing coronary angiography: A randomized controlled trial. Int J Nurs Pract. (2023) 29:e13176. doi: 10.1111/ijn.13176
63. Hendricks TM, Gutierrez CN, Stulak JM, Dearani JA, Miller JD. The use of virtual reality to reduce preoperative anxiety in first-time sternotomy patients: A randomized controlled pilot trial. Mayo Clin Proc. (2020) 95:1148–57. doi: 10.1016/j.mayocp.2020.02.032
64. Karaman D, Taşdemir N. The effect of using virtual reality during breast biopsy on pain and anxiety: A randomized controlled trial. J Perianesth Nurs. (2021) 36:702–5. doi: 10.1016/j.jopan.2021.04.007
65. Ketsuwan C, Matang W, Ratanapornsompong W, Sangkum P, Phengsalae Y, Kongchareonsombat W, et al. Prospective randomized controlled trial to evaluate effectiveness of virtual reality to decrease anxiety in office-based flexible cystoscopy patients. World J Urol. (2022) 40:2575–81. doi: 10.1007/s00345-022-04142-9
66. Karaveli Çakır S, Evirgen S. The effect of virtual reality on pain and anxiety during colonoscopy: A randomized controlled trial. Turk J Gastroenterol. (2021) 32:451–7. doi: 10.5152/tjg.2021.191081
67. Keshvari M, Yeganeh MR, Paryad E, Roushan ZA, Pouralizadeh M. The effect of virtual reality distraction on reducing patients' anxiety before coronary angiography: a randomized clinical trial study. Egypt Heart J. (2021) 73:98. doi: 10.1186/s43044-021-00224-y
68. Kleiner I, Mor L, Friedman M, Abeid AA, Shoshan NB, Toledano E, et al. The use of virtual reality during extra-amniotic balloon insertion for pain and anxiety relief-a randomized controlled trial. Am J Obstet Gynecol MFM. (2024) 6:101222. doi: 10.1016/j.ajogmf.2023.101222
69. Ko SY, Wong EM, Ngan TL, Leung HK, Kwok KT, Tam HF, et al. Effects of virtual reality on anxiety and pain in adult patients undergoing wound-closure procedures: A pilot randomized controlled trial. Digit Health. (2024) 10:20552076241250157. doi: 10.1177/20552076241250157
70. Kurt G, Ozcan NK. The effect of virtual reality on pain and anxiety management during pelvic examination: A randomized controlled trial. J Midwifery Womens Health. (2024) 69(4):543–9. doi: 10.1111/jmwh.13587
71. Öz T, Demirci N. The effect of virtual reality, music therapy, and stress ball application on pain and anxiety during outpatient gynecological procedures: A randomized controlled trial. J Perianesth Nurs. (2024). doi: 10.1016/j.jopan.2024.01.022
72. Reinders IMA, Cremers GR, van Rooijen SJ, Leemans JC, Perquin CW, Geomini P, et al. The effect of an informative 360-degree virtual reality video on anxiety for women visiting the one-stop clinic for abnormal uterine bleeding: A randomized controlled trial (VISION-trial). Eur J Obstet Gynecol Reprod Biol. (2022) 272:96–103. doi: 10.1016/j.ejogrb.2022.02.179
73. Rutkowski S, Bogacz K, Czech O, Rutkowska A, Szczegielniak J. Effectiveness of an inpatient virtual reality-based pulmonary rehabilitation program among COVID-19 patients on symptoms of anxiety, depression and quality of life: preliminary results from a randomized controlled trial. Int J Environ Res Public Health. (2022) 19(24):16980. doi: 10.3390/ijerph192416980
74. Toraman RL, Eskici Ilgin V. Effect of virtual reality glasses application on pain, anxiety, and patient satisfaction during a transrectal prostate biopsy: A randomized controlled trial. Biol Res Nurs. (2024) 26:485–97. doi: 10.1177/10998004241236154
75. Turan AZ, Yilmaz M, Saracoglu T. The effect of virtual reality glasses on anxiety during surgery under spinal anesthesia: a randomized controlled study. Anesth Pain Intensive Care. (2021) 25:170–5. doi: 10.35975/apic.v25i2.1469
76. Turan GB, Gür F, Özer Z, Tarkan Ç. Effects of virtual reality on pain, anxiety, patient satisfaction in coronary angiography: A randomized trial. Pain Manag Nurs. (2024) 25:e177–e85. doi: 10.1016/j.pmn.2023.11.009
77. Yang J, Rhu J, Lim S, Kang D, Lee H, Choi GS, et al. Impact of virtual reality education on disease-specific knowledge and anxiety for hepatocellular carcinoma patient scheduled for liver resection: a randomized controlled study. Int J Surg. (2024) 110:2810–7. doi: 10.1097/JS9.0000000000001197
78. Sahin G, Basak T. The effects of intraoperative progressive muscle relaxation and virtual reality application on anxiety, vital signs, and satisfaction: A randomized controlled trial. J Perianesth Nurs. (2020) 35:269–76. doi: 10.1016/j.jopan.2019.11.002
79. Prabhu VG, Sprouse HA, Brignull CG, Snider R, Tanner S, Adams KJ, et al. The impact of virtual reality on anxiety and pain during US-guided breast biopsies: A randomized controlled clinical trial. J Breast Imaging. (2024) 6:45–52. doi: 10.1093/jbi/wbad088
80. Baltaci N, Bal S, Koç E, Edis EK. Effects of virtual reality and nature sounds on pain and anxiety during hysterosalpingography: a randomized controlled trial. (2024) 70(7):e20231599. doi: 10.1590/1806-9282.20231599
81. Olasz O, Erdős S, Horváth K. The effects of virtual reality-based mindfulness exercises on the perception of time, psychological and physiological states of young people: A randomized crossover trial. Mindfulness. (2024) 15:2347–54. doi: 10.1007/s12671-024-02438-y
82. Primavera D, Urban A, Cantone E, Nonnis M, Aviles Gonzalez CI, Perra A, et al. The impact on anxiety symptoms of an immersive virtual reality remediation program in bipolar disorders: A randomized clinical trial. J Clin Med. (2024) 13(14):4203. doi: 10.3390/jcm13144203
83. Schmid BC, Marsland D, Jacobs E, Rezniczek GA. A preparatory virtual reality experience reduces anxiety before surgery in gynecologic oncology patients: A randomized controlled trial. (2024) 16(10):1913. doi: 10.3390/cancers16101913
84. Salzwedel C, Petersen C, Blanc I, Koch U, Goetz AE, Schuster M. The effect of detailed, video-assisted anesthesia risk education on patient anxiety and the duration of the preanesthetic interview: a randomized controlled trial. Anesth Analg. (2008) 106:202–9. doi: 10.1213/01.ane.0000287665.96156.72
85. Habibzadeh H, Milan ZD, Radfar M, Alilu L, Cund A. Effects of Peer-Facilitated, Video-Based and Combined Peer-and-Video Education on Anxiety Among Patients Undergoing Coronary Angiography: Randomized controlled trial. Sultan Qaboos Univ Med J. (2018) 18:e61–e7. doi: 10.18295/squmj.2018.18.01.010
86. Li Z, Geng W, Yin J, Zhang J. Effect of one comprehensive education course to lower anxiety and depression among Chinese breast cancer patients during the postoperative radiotherapy period - one randomized clinical trial. Radiat Oncol. (2018) 13:111. doi: 10.1186/s13014-018-1054-6
87. Garcia S. The effects of education on anxiety levels in patients receiving chemotherapy for the first time: an integrative review. Clin J Oncol Nurs. (2014) 18:516–21. doi: 10.1188/14.CJON.18-05AP
88. Singh N, Kanaujia SK, Singh MK, Shukla N, Siddiqui AK, Kohli M. Effect of virtual reality glasses and melody on cortisol and adrenocorticotropic hormone levels in patients with knee replacement surgery under combined spinal epidural anesthesia. Cureus. (2024) 16:e63017. doi: 10.7759/cureus.63017
89. Che YJ, Gao YL, Jing J, Kuang Y, Zhang M. Effects of an informational video about anesthesia on pre- and post-elective cesarean section anxiety and recovery: A randomized controlled trial. Med Sci Monit. (2020) 26:e920428. doi: 10.12659/MSM.920428
90. Samnakay S, von-Ungern-Sternberg BS, Evans D, Sommerfield AC, Hauser ND, Bell E, et al. 3-dimensional virtual reality versus 2-dimensional video for distraction during the induction of anesthesia in children to reduce anxiety: A randomized controlled trial. Anesth Analg. (2024). doi: 10.1213/ANE.0000000000007119
91. Turgut A, Özcan İlçe A, Öztürk H. The effect of immersive virtual reality application on anxiety, pain, and parental satisfaction in the perioperative process of children: A randomized controlled trial. Pain Manag Nurs. (2024) 25(6):584–90. doi: 10.1016/j.pmn.2024.06.002
92. Ryu JH, Park SJ, Park JW, Kim JW, Yoo HJ, Kim TW, et al. Randomized clinical trial of immersive virtual reality tour of the operating theatre in children before anesthesia. Br J Surg. (2017) 104:1628–33. doi: 10.1002/bjs.10684
93. Topalel S, Orekici Temel G, Azizoğlu M. Evaluation of preoperative anxiety in turkish pediatric patients and validity and reliability of the turkish modified yale preoperative anxiety scale. Turk J Anaesthesiol Reanim. (2020) 48:484–90. doi: 10.5152/TJAR.2020.116
94. Moerman N, van Dam FS, Muller MJ, Oosting H. The amsterdam preoperative anxiety and information scale (APAIS). Anesth Analg. (1996) 82:445–51. doi: 10.1097/00000539-199603000-00002
95. Krohne HW, Schmukle SC, de Bruin J. The Inventory "State-Trait Operation Anxiety" (STOA): construction and empirical findings. Psychother Psychosom Med Psychol. (2005) 55:209–20. doi: 10.1055/s-2004-834604
96. van Loenen I, Scholten W, Muntingh A, Smit J, Batelaan N. The effectiveness of virtual reality exposure-based cognitive behavioral therapy for severe anxiety disorders, obsessive-compulsive disorder, and posttraumatic stress disorder: meta-analysis. J Med Internet Res. (2022) 24:e26736. doi: 10.2196/26736
97. Emmelkamp PMG, Meyerbröker K. Virtual reality therapy in mental health. Annu Rev Clin Psychol. (2021) 17:495–519. doi: 10.1146/annurev-clinpsy-081219-115923
98. Park MJ, Kim DJ, Lee U, Na EJ, Jeon HJ. A literature overview of virtual reality (VR) in treatment of psychiatric disorders: recent advances and limitations. Front Psychiatry. (2019) 10:505. doi: 10.3389/fpsyt.2019.00505
99. Hong YJ, Kim HE, Jung YH, Kyeong S, Kim JJ. Usefulness of the mobile virtual reality self-training for overcoming a fear of heights. Cyberpsychol Behav Soc Netw. (2017) 20:753–61. doi: 10.1089/cyber.2017.0085
100. Zainal NH, Chan WW, Saxena AP, Taylor CB, Newman MG. Pilot randomized trial of self-guided virtual reality exposure therapy for social anxiety disorder. Behav Res Ther. (2021) 147:103984. doi: 10.1016/j.brat.2021.103984
101. Premkumar P, Heym N, Brown DJ, Battersby S, Sumich A, Huntington B, et al. The effectiveness of self-guided virtual-reality exposure therapy for public-speaking anxiety. Front Psychiatry. (2021) 12:694610. doi: 10.3389/fpsyt.2021.694610
102. Rubin M, Muller K, Hayhoe MM, Telch MJ. Attention guidance augmentation of virtual reality exposure therapy for social anxiety disorder: a pilot randomized controlled trial. Cognit Behav Ther. (2022) 51:371–87. doi: 10.1080/16506073.2022.2053882
103. Hannigan B, van Deursen R, Barawi K, Kitchiner N, Bisson JI. Factors associated with the outcomes of a novel virtual reality therapy for military veterans with PTSD: Theory development using a mixed methods analysis. PLoS One. (2023) 18:e0285763. doi: 10.1371/journal.pone.0285763
104. Beidel DC, Frueh BC, Neer SM, Bowers CA, Trachik B, Uhde TW, et al. Trauma management therapy with virtual-reality augmented exposure therapy for combat-related PTSD: A randomized controlled trial. J Anxiety Disord. (2019) 61:64–74. doi: 10.1016/j.janxdis.2017.08.005
105. Difede J, Hoffman HG. Virtual reality exposure therapy for World Trade Center Post-traumatic Stress Disorder: a case report. Cyberpsychol Behav. (2002) 5:529–35. doi: 10.1089/109493102321018169
106. Lehoux T, Capobianco A, Lacoste J, Rollier S, Mopsus Y, Melgire M, et al. Virtual reality cue-exposure therapy in reducing cocaine craving: the Promoting Innovative COgnitive behavioral therapy for Cocaine use disorder (PICOC) study protocol for a randomized controlled trial. Trials. (2024) 25:421. doi: 10.1186/s13063-024-08275-7
107. Corno G, Serino S, Cipresso P, Baños RM, Riva G. Assessing the relationship between attitudinal and perceptual component of body image disturbance using virtual reality. Cyberpsychol Behav Soc Netw. (2018) 21:679–86. doi: 10.1089/cyber.2018.0340
108. Riva G, Alcañiz M, Anolli L, Bacchetta M, Baños R, Beltrame F, et al. The VEPSY updated project: virtual reality in clinical psychology. Cyberpsychol Behav. (2001) 4:449–55. doi: 10.1089/109493101750527006
109. Javaherirenani R, Mortazavi SS, Shalbafan M, Ashouri A, Farani AR. Virtual reality exposure and response prevention in the treatment of obsessive-compulsive disorder in patients with contamination subtype in comparison with in vivo exposure therapy: a randomized clinical controlled trial. BMC Psychiatry. (2022) 22:740. doi: 10.1186/s12888-022-04402-3
110. Stanney K, Fidopiastis C, Foster L. Virtual reality is sexist: but it does not have to be. Front Robot AI. (2020) 7:4. doi: 10.3389/frobt.2020.00004
111. Grassini S, Laumann K. Are modern head-mounted displays sexist? A systematic review on gender differences in HMD-mediated virtual reality. Front Psychol. (2020) 11:1604. doi: 10.3389/fpsyg.2020.01604
112. Kim J, Oh H, Kim W, Choi S, Son W, Lee S. A deep motion sickness predictor induced by visual stimuli in virtual reality. IEEE Trans Neural Netw Learn Syst. (2022) 33:554–66. doi: 10.1109/TNNLS.2020.3028080
113. Ramazan K, Devran AY, Muhammed ON. An old approach to a novel problem: effect of combined balance therapy on virtual reality induced motion sickness: a randomized, placebo controlled, double-blinded study. BMC Med Educ. (2024) 24:156. doi: 10.1186/s12909-024-05152-4
114. Somrak A, Pogačnik M, Guna J. Suitability and comparison of questionnaires assessing virtual reality-induced symptoms and effects and user experience in virtual environments. Sensors (Basel). (2021) 21(4):1185. doi: 10.3390/s21041185
115. Souchet AD, Lourdeaux D, Burkhardt JM, Hancock PA. Design guidelines for limiting and eliminating virtual reality-induced symptoms and effects at work: a comprehensive, factor-oriented review. Front Psychol. (2023) 14:1161932. doi: 10.3389/fpsyg.2023.1161932
116. Taveira MC, de Sá J, da Rosa MG. Virtual reality-induced dissociative symptoms: A retrospective study. Games Health J. (2022) 11:262–7. doi: 10.1089/g4h.2022.0009
117. Wong CL, Li CK, Chan CWH, Choi KC, Chen J, Yeung MT, et al. Virtual reality intervention targeting pain and anxiety among pediatric cancer patients undergoing peripheral intravenous cannulation: A randomized controlled trial. Cancer Nurs. (2021) 44:435–42. doi: 10.1097/NCC.0000000000000844
118. Wong CL, Choi KC. Effects of an immersive virtual reality intervention on pain and anxiety among pediatric patients undergoing venipuncture: A randomized clinical trial. JAMA Netw Open. (2023) 6:e230001. doi: 10.1001/jamanetworkopen.2023.0001
119. Yin J, Yuan J, Arfaei N, Catalano PJ, Allen JG, Spengler JD. Effects of biophilic indoor environment on stress and anxiety recovery: A between-subjects experiment in virtual reality. Environ Int. (2020) 136:105427. doi: 10.1016/j.envint.2019.105427
120. Uslu A, Arslan S. The effect of using virtual reality glasses on anxiety and fatigue in women with breast cancer receiving adjuvant chemotherapy: A pretest-posttest randomized controlled study. Semin Oncol Nurs. (2023) 39:151503. doi: 10.1016/j.soncn.2023.151503
121. Ahmad M, Bani Mohammad E, Tayyem E, Al Gamal E, Atout M. Pain and anxiety in patients with breast cancer treated with morphine versus tramal with virtual reality. Health Care Women Int. (2024) 45:782–95. doi: 10.1080/07399332.2023.2257627
122. Chirico A, Maiorano P, Indovina P, Milanese C, Giordano GG, Alivernini F, et al. Virtual reality and music therapy as distraction interventions to alleviate anxiety and improve mood states in breast cancer patients during chemotherapy. J Cell Physiol. (2020) 235:5353–62. doi: 10.1002/jcp.v235.6
123. Lee SY, Kang J. Effect of virtual reality meditation on sleep quality of intensive care unit patients: A randomized controlled trial. Intensive Crit Care Nurs. (2020) 59:102849. doi: 10.1016/j.iccn.2020.102849
124. Failla C, Marino F, Bernardelli L, Gaggioli A, Doria G, Chilà P, et al. Mediating mindfulness-based interventions with virtual reality in non-clinical populations: the state-of-the-art. Healthcare (Basel). (2022) 10(7):1220. doi: 10.3390/healthcare10071220
125. Reger GM, Smolenski D, Norr A, Katz A, Buck B, Rothbaum BO. Does virtual reality increase emotional engagement during exposure for PTSD? Subjective distress during prolonged and virtual reality exposure therapy. J Anxiety Disord. (2019) 61:75–81. doi: 10.1016/j.janxdis.2018.06.001
Keywords: virtual reality therapy, virtual reality exposure therapy, adolescent, adult, anxiety, anxiety disorder
Citation: Zeng W, Xu J, Yu J and Chu X (2025) Effectiveness of virtual reality therapy in the treatment of anxiety disorders in adolescents and adults: a systematic review and meta-analysis of randomized controlled trials. Front. Psychiatry 16:1553290. doi: 10.3389/fpsyt.2025.1553290
Received: 30 December 2024; Accepted: 28 January 2025;
Published: 27 February 2025.
Edited by:
Fabrizio Stasolla, Giustino Fortunato University, ItalyReviewed by:
Slawomir Murawiec, Harmonia Luxmed Medical Center, PolandCopyright © 2025 Zeng, Xu, Yu and Chu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Xin Chu, Y2h1eGluQGNkenl5ZHhmc3l5MTUud2Vjb20ud29yaw==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.