
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychiatry , 12 March 2025
Sec. Aging Psychiatry
Volume 16 - 2025 | https://doi.org/10.3389/fpsyt.2025.1486626
 Wen Wang1,2,3†
Wen Wang1,2,3† Junrong Ye1,2,4†
Junrong Ye1,2,4† Yanheng Wei2,4†Jiawei Huang1,2Haoyun Wang5
Yanheng Wei2,4†Jiawei Huang1,2Haoyun Wang5 Fei Liu2,6Shengwei Wu2,7
Fei Liu2,6Shengwei Wu2,7 Jialan Wu2,8
Jialan Wu2,8 Zezhi Li2,9*Jianxiong Guo2,7*
Zezhi Li2,9*Jianxiong Guo2,7* Aixiang Xiao2,4*
Aixiang Xiao2,4*Objective: This study aims to identify the clinical characteristics of schizophrenia, depression, and AD among older adults.
Methods: General information of patients was collected, including diagnosis, age, gender, level of education, marital status, drinking behavior, smoking behavior, course of mental disorder, type of admission, history of modified electroconvulsive therapy (MECT) and hospitalization period. The Brief Psychiatric Rating Scale (BPRS), Geriatric Depression Scale (GDS), Generalized Anxiety Disorder 7-Item Scale (GAD-7), Insight and Treatment Attitudes Questionnaire (ITAQ), and Mini-Mental State Examination (MMSE) were employed to evaluate the participants’ mental status. The Functional Activities Questionnaire (FAQ), Social Support Rating Scale (SSRS), Barthel ADL Index, Standardized Swallowing Assessment (SSA), and Mini-Nutritional Assessment (MNA) were applied to measure social and daily living function. The Nurses’ Global Assessment of Suicide Risk (NGASR) and The Brøset Violence Checklist (BVC) were used to assess the patients’ risk of suicide.
Results: Totally 271 participants were recruited, the numbers of participants with schizophrenia, depression, and Alzheimer’s diseases (AD), were 81 (29.9%), 85 (31.4%), and 105 (38.7%), respectively. One-way ANOVA was used to compare the variance of the crude score results among three groups of subjects. The results showed that patients with depression had the highest GDS total score, followed by patients with AD, and patients with schizophrenia had the lowest score (P < 0.001). The total scores of GAD-7 and ITAQ in patients with depression were higher than those in patients with AD and schizophrenia (P < 0.001). The total score of MMSE in patients with schizophrenia and depression was higher than that in patients with AD (P < 0.001). The incidence of circulatory system diseases in patients with depression and AD was higher than that in patients with schizophrenia (P < 0.05). The incidence of respiratory system diseases in patients with AD was highest, followed by patients with schizophrenia, and patients with depression had the lowest incidence (P < 0.05). The incidence of nervous system diseases in patients with AD was highest, followed by patients with depression, and patients with schizophrenia had the lowest incidence (P < 0.05). The total scores of FAQ and SSA in patients with AD were higher than those in patients with schizophrenia and depression (P < 0.001), while patients with depression had statistically lower SSRS scores than patients with schizophrenia and patients with AD (P < 0.05). Furthermore, patients with AD had lower Barthel ADL Index scores and water-swallowing test (P < 0.001). MNA scores of patients with schizophrenia were higher than those of patients with depression and AD, with statistical significance (P < 0.05). The NGASR scores of patients with depression were higher than those of patients with schizophrenia and AD, which was statistically significant (P < 0.001). Patients with AD had the highest BVC total score, followed by that of patients with schizophrenia and patients with depression had lowest score, and the difference was statistically significant (P < 0.05).
Conclusions: Patients with geriatric psychosis may experience abnormalities in various aspects that influenced daily living, including disorders of thinking, cognition, emotion, and behavior. Patients with schizophrenia have cognitive impairment. Cognitive training and medication are important. Patients with depression were considered to be at a greater risk for suicide compared to those with schizophrenia and AD. Active clinical measures must be adopted to improve patients’ depressive symptoms, change their suicidal attitudes, and enhance their self-confidence. Patients with AD were prone to respiratory and neurological diseases. Treatment of respiratory infections and hypoxia and other respiratory diseases would be necessary, and cognitive function training should be conducted. In addition, regarding to high risk of swallowing disorders and malnutrition, swallowing function training should be carried out to ensure food intake and prevent malnutrition. Driven by psychiatric symptoms, violent behavior was prevalent, thus effective communication and de-escalation techniques are needed. Although the symptoms of these three diseases are different, timely professional intervention and support from family members are urgently needed.
Population aging has become a major challenge worldwide. A significant shift in the global age structure can be ascribed to a decline in the birth rate and increase in the life expectancy in recent years (1). In 2010, the United Nations Population Program predicted that the proportion of people aged above 80 years old will increase fourfold by 2050 (2). Zhang et al. (2021) estimated that the number of people aged over 65 years old would increase to 19.1% of the world’s population (3). Although aging population had become a global threat, empirical findings had revealed that aging population would have greater impacts on low and middle income countries (LMICs) than developed countries in the near future.
By 2050, the global population aged above 60 years is projected to reach 2 billion, and approximately 80% of them would be from LMICs (4). China, one of the largest LMICs with great amount of aged population, is witnessing a rapid growth in the population of older adults. In 2020, residents aged over 65 years old accounted for approximately 13.5% of the national population, indicating that the country had entered the “aging society.” From 1980 to 2020, the elderly population in China had been continuously increasing. During the period, the proportion of adults aged 60 and above increased sharply, from 6.9% to 18.7%. By 2020, the elderly population size was 264.0 million (5). Cho et al. (2020) estimated the number of senior citizens in China, and their results suggested that the percentage of citizens aged above 80 years would annually increase until 2050 (6). As the second most populous country worldwide, major demographic changes had brought great challenges to health care service of the elderly in China (7–9). As a result of aging population, unexpected influential social issues had occurred. The number of older adults facing chronic diseases, disability, and care dependency had increased significantly, and concerns about older adults’ mental health had risen (10). As symptomatic treatments solely focus on physical recovery, the mental illness caused by chronic diseases and disability had been ignored to some extent.
Empirical studies demonstrated that older adults had a huge demand of mental health care (11). Notably, more than one out of five adults aged above 60 years were reported to be diagnosed with at least one mental disorders (12). In addition to impacting the quality of life of elderly individuals, mental disorders are likely to exacerbate physical illnesses, leading to higher morbidity and mortality rates (13). An empirical study found that mental disorders in elderly people were frequently accompanied by cognitive disorders, such as perceptual disorders and memory disorders (14). Furthermore, the patients’ physical functions began to deteriorate, and many patients were surrounded by varying degrees and types of physical illness. Consequently, a number of these mental illnesses were chronic, which would need a lengthy hospital stay with a high recurrence rate, and most patients were hospitalized repeatedly (15). This situation had not only significantly increased the requirement for medical assistance and care for elderly people with mental illness but had also managed to make caregiving complicated and burdensome. Elderly individuals would physically and mentally benefit from appropriate nursing care. A research in 2021 showed that, the proportion of hospitalized elderly patients with mental disorders accounted for 20.2% of total hospitalized psychiatric patients. Among 7086 hospitalized elderly patients with mental disorders, schizophrenia and depression accounted for 14.4% and 16.7%, respectively (16). Previous researches had examined the clinical characteristics of patients with schizophrenia, depression and Alzheimer’s diseases (AD) (17). Hou et al. (2017) reported that schizophrenic patients generally had sleep problems and poor quality of life. A meta-analysis by Xu et al. (2022) indicated that impairments in facial emotion recognition was a common clinical characteristic observed in individuals with schizophrenia, such facial emotion recognition difficulties predicted subsequent declines in work performance, social participation, and independent living skills among older patients with schizophrenia (18). Besides, a multi-center cross-sectional study of patients who were 65 years old or older of 13 primary care clinics in Wuhan showed that certain demographic variables, psychosocial factors, and major medical conditions were significantly associated with the severity of depressive disorders of older patients (19). In addition, Zhong et al. (2020) found that patients with unipolar disorder (UD) depression had less impairment in cognitive function among all domains than those with bipolar disorder (BD) depression, and had shorter P300 latency than BD depression patients (20). Understanding the clinical characteristics of major mental disorders could help in developing effective interventions as well as optimizing the allocation of medical resources. To this end, we analyzed 271 patients consecutively admitted to a public provincial psychiatric hospital and presented the clinical characteristics of mental disorders.
This study aimed to determine the clinical characteristics of admitted aged patients with mental disorders (schizophrenia, depression and AD), and to shed lights on developing targeted effective nursing interventions.
A consecutive sampling method was used to recruit 271 hospitalized patients with schizophrenia, depression and AD in the Affiliated Brain Hospital, Guangzhou Medical University from February 2021 to March 2022. All participants or their family member are willing to sign the written informed consent. Inclusion criteria: (a) in accordance with International Classification of Diseases-10 (ICD-10) diagnostic criteria for schizophrenia, depression and AD; (b) age 60 years and above; (c) no sedatives or other medications that affect blood pressure and heart rate have been taken in the last two weeks; (d) be able to respond naturally and complete scale rating; (e) willingness to sign the written informed consent. Exclusion criteria: (a) poor compliance and inability to cooperate with questionnaire completion; (b) those with severe mental retardation, hearing disability; (c) combined severe physical diseases, such as cardiovascular, hepatic, or renal diseases.
General information questionnaire was designed to collect age, gender, education, marital status, alcohol consumption, smoking, course of mental disorder, type of admission, history of modified electroconvulsive therapy and hospitalization period.
The Brief Psychiatric Rating Scale (BPRS) contains 18 items with five types of factors that are rated on a scale of 1 to 7, including the anxiety–depression factor, lack of vitality factor, thought disorder factor, activation factor, and hostile suspicion factor (21). BPRS is a well-established instrument extensively utilized to assess the severity of positive, negative, general and affective symptoms in individuals with severe mental disorders, particularly those diagnosed with schizophrenia (22). In this study, Cronbach’ s α of the scale was 0.733.
The Geriatric Depression Scale (GDS) was introduced by Brink and Yesavage in 1982. GDS was specifically developed for the evaluation of depressive symptoms in older adults (23). The scale has 30 items, including depressed mood, reduced activity, agitation, and self-reported pain, among others. Each item is followed by a number of items in parenthesis indicating the degree of depression. A score of 1 is given to each question if it is consistent with one of the items, with 1–10 being normal, 11–20 being mild depression, and 20 or more being moderate depression (23, 24). In this study, Cronbach’ s α of GDS was 0.948.
The Generalized Anxiety Disorder 7-Item Scale (GAD) is a screening tool to evaluate the severity of symptoms of generalized anxiety disorder that consists of items that are rated on a score ranging from 0 to 3, from “never” to “almost every day.”. The GAD-7 score of ≥ 10 was used as the cut-off value for screening for generalized anxiety disorder. The cut-off marks for mild, moderate, and severe generalized anxiety disorder were 5, 10, and 15, respectively (25). GAD had been widely adopted in various studies as a screening tool for anxiety symptoms among adults (26). In this study, Cronbach’ s α was 0.860.
The Insight and Treatment Attitude Questionnaire (ITAQ), developed by McEvoy (1989), defines self-awareness as “recognizing that one has a disease and requesting treatment,” and its main purpose is to assess schizophrenic patients’ awareness of their illness and their attitudes toward taking medication. The questionnaire contains 11 questions and is scored on a scale of 0 to 2: 0 for “no self-knowledge,” 1 for “partial self-knowledge,” and 2 for “full self-knowledge.” The questionnaire has the lowest score of 0 and a highest score of 22. The higher the score, the greater the patient’s self-awareness (27). In the study, Cronbach’ s α was 0.941.
The Mini-Mental State Examination (MMSE) was developed by Folstein in 1975. MMSE is one of the most extensively utilized tools for assessing cognitive function in older adults and predicting the onset of AD (28). The MMSE has 19 items. Items 1–5 are time-oriented, while items 6–10 are place-oriented. Item 11 is divided into three sub-items for verbal immediate memory, whereas item 12 is divided into five sub-items that examine attention and computation. Item 13 is divided into three sub-items to check short term memory. Item 14 is broken down into two sub-items for naming objects. The verbal retelling is item 15, and item 16 is concerned with reading comprehension. Item 17 assesses verbal comprehension, and item 18 assesses verbal communication. Finally item 19 is concerned with graphic tracing. The MMSE has a total score range of 0–30 (29). In this study, Cronbach’ s α was 0.799.
The Functional Activities Questionnaire (FAQ) is a commonly used scale for evaluating patients with early AD. FAQ is a screening tool for social dysfunction and adopted in studies of older adults. The scale consists of 10 questions, including: (1) using communication tools; (2) organizing objects; (3) shopping by oneself; (4) skillful activities; (5) using electrical appliances; (6) preparing meals; (7) learning about new things; (8) paying attention and understanding; (9) remembering appointments; and (10) going out alone. The rating index is the sum of the items’ scores on a 4-point scale ranging from 0 to 3. The higher the score, the greater the severity of the impairment (30). In the study, Cronbach’ s α of FAQ was 0.986.
The Social Support Rating Scale (SSRS) developed by Xiao Shuiyuan (1994) is widely used to assess levels of social support and adopted in various studies among different patients in China (31, 32). This scale includes three dimensions: subjective support, objective support, and social support utilization. For items 1–4 and 8–10, only one item was selected for each item, and 1, 2, 3, and 4 points were assigned to items 1, 2, 3, and 4, respectively. Item 5 was divided into four items, A, B, C, and D, and the total score was given for each item ranging from none to full support, and 1–4 points were given for items 6 and 7, respectively. If the respondents answered “the following sources,” they were given several points for each source. The overall score is the sum of 10 items: 1, 3, 4, and 5 are considered subjective support, 2, 6, and 7 are considered objective support, and 8, 9, and 10 are considered utilization of support (33). In the study, Cronbach’ s α of SSRS was 0.766.
The Activities of Daily Living (ADL) scale was developed by Lawton and Brody in 1969 and consists of the Barthel Index, a 10-item scale with four functional levels as per the patient’s need for help and the degree of that need. The higher the score, the more independent and the less dependent the patient is. The assessment was performed by asking the elderly about each item and could also be based on report. ADL was mainly used to assess the ability of the subject in daily life (34). Impairments in activities of daily living are common in older adults with mental disorders, such as AD, depression, and schizophrenia, and can significantly impact their independence and quality of life. The scale is suitable for assessing older adults with mental disorders (35). In this study, Cronbach’ s α was 0.929.
The water-swallowing test, or the Kubota drinking test, was first published in Japan in 1982. In this test, the patient is instructed to drink 30 ml of warm water while sitting up straight, and the amount of time needed as well as any choking symptoms are noted. (First degree: able to swallow 30 ml water without coughing or choking in one sitting; second degree: swallowed 30 ml water in twice or more times without choking or coughing; third degree: swallowed 30 ml water for once, but with choking; fourth degree: able to swallow 30 ml water in small portions but with choking; fifth degree: frequent choking and coughing, unable to swallow 30 ml water). Research had demonstrated a significantly high prevalence of dysphagia among patients with mental disorders, particularly those with cognitive impairment and severe AD (36). This test could accurately assess the patient’s swallowing function and ascertain the degree of swallowing dysfunction (37). In the study, Cronbach’ s α was 0.895.
The Standard Swallowing Assessment (SSA) scale was designed and proposed by Ellul et al. in 1996 as a method applied to assess swallowing function. From easy to difficult, the three components of this scale are: clinical assessment, which rates a person’s level of consciousness, control over their head and body, normal breathing pattern, normal lip closure, abnormal soft palate movement, abnormal laryngeal function, pharyngeal reflex, and spontaneous cough; swallowing five milliliters of water three times and observing whether water flows; and effective laryngeal movement. The third phase can be continued if no abnormalities are detected in the second part (three repetitions, two or more normal). The participants swallow 60 mL of water and observe completeness, the time required to complete swallowing, whether there is coughing during or after swallowing, whether there is wheezing during or after swallowing, and the function of the larynx after swallowing. The scale was scored on a scale of 5–12. The scale scores ranged from 18 to 46, and the higher the score, the worse the swallowing function (38). The high incidence of swallowing difficulties in mental illnesses such as AD has attracted attention. Currently, a research by Ye et al. (2024) has applied SSA to evaluate the swallowing function of patients with AD, demonstrating good reliability and validity (39). In this study, Cronbach’ s α of SSA was 0.914.
The Mini-Nutritional Assessment (MNA) scale was first proposed by Guigoz et al. in the 1990s to evaluate the nutritional status of the elderly. MNA includes 18 items and assesses four aspects: anthropometric measurements (BMI, weight loss, mid-arm and mid-calf circumferences); general assessment (related to lifestyle, medication, and mobility); dietary intake (related to number of meals, food and fluid intake, and autonomy of feeding) and subjective assessment (self-perception of health and nutrition). Scores less than 17 out of 30 are considered malnourished, scores between 17 and 23.5 indicate the risk of malnutrition, and scores of 24 or above are considered normal (40). In this study, Cronbach’ s α was 0.754.
The Nurses’ Global Assessment of Suicide Risk (NGASR) scale is an instrument which widely adopted by psychiatric nurses to assess suicide risk and make accurate, weighted clinical judgments (41). NGASR has been found to be quick and easy to administer, without need for preliminary training. NGASR consists of 15 items including recent negative life events, verbal expression of suicidal intent, feelings of despair, and history of suicide, each of which includes two answer choices of either “yes” or “no.” The five answers to items 1, 4, 7, 9, and 12 were scored as 3 points, the 10 answers to items 2, 3, 5, 6, 8, 10, 11, 13, 14, and 15 received 1 point, and all answers to items “no” were scored as 0 points. The total score was then obtained according to the rules of adding points. The maximum score of the scale is 25, with a total score of 0–5 representing low suicide risk, 6–8 representing medium suicide risk, 9–11 representing high suicide risk, and 12 representing very high suicide risk (42). In the study, Cronbach’ s α of NGASR was 0.760.
The Brøset Violence Checklist (BVC) was developed by Almvik et al. (1997) to assess the risk of violence in patients with inpatient psychiatric disorders. Each entry on the scale is given a score of 0 or 1 (none = 0; yes = 1). The scale measures the presence or absence of six behaviors: confusion, irritation, boisterousness, verbal threat, somatic threat, and destructive activity. The maximum total score was 6, with 0 representing the “lack of a behavior,” 1 being “its presence,” 6 being the “presence of a behavior”. The ratings ranged from 0 for low risk to 1–2 for moderate risk, indicating the need for preventative actions, to 3–6 for high risk, indicating the need for both preventive measures and a strategy to deal with violent aggression (43, 44). In the study, Cronbach’ s α was 0.739.
This study adopted a questionnaire-survey method to collect data. Researchers who had completed consistency training distributed questionnaires in a tertiary psychiatric hospital. The filling time for questionnaire was approximately 25-30 minutes. General information and disease condition were accessed through hospital information system, and other information was collected in by patients with the assistance of researchers.
Statistical analysis was performed using the SPSS 25.0 statistical software. Measurement data was presented with mean ± sd, counting data was expressed using frequency and percentage. The difference between the two categories was performed by independent sample t-test, one-way ANOVA for three or more categories, and non-parametric K independent sample test for rank variable. Qualitative data is represented by composition ratios or rates, while intergroup comparisons are made using χ 2 inspection. And the level of significance was set at 0.05.
The 271 cases included 81 patients with schizophrenia, (26 males [32.1%], 55 females [67.9%]; 85 patients with depression (24 males [28.2%], 61 females [71.8%]), and 105 patients with AD (37 males [35.2%], 68 females [64.8%]). The female patients account for the largest proportion (67.9%), and those aged 60 to 69 are the most numerous (46.1%). The highest proportion of patients are those who are married (72.3%) (Table 1).
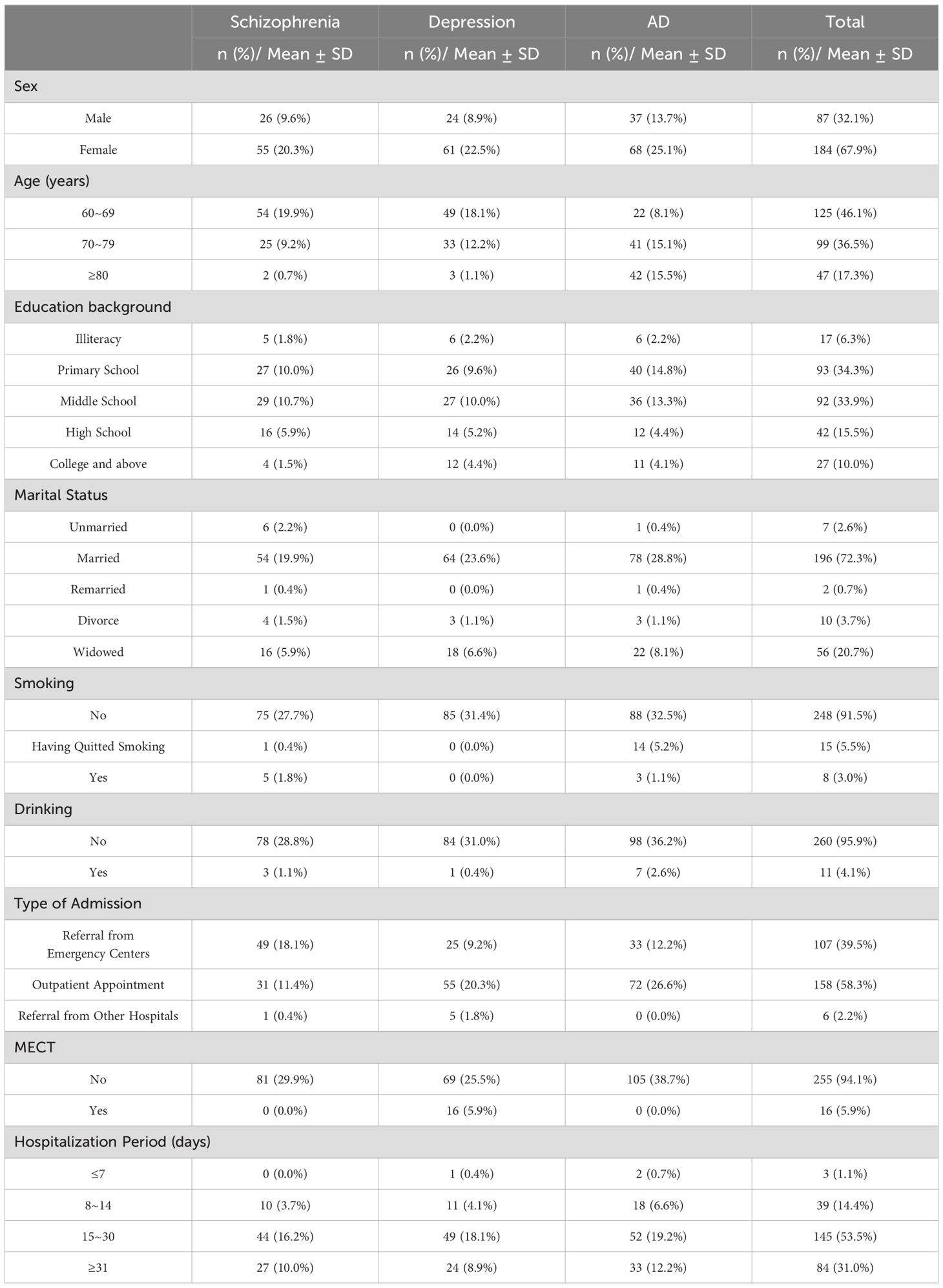
Table 1. General information.
The results showed that patients with depression had the highest GDS total score, followed by patients with AD, and patients with schizophrenia had the lowest score (P < 0.001). The total scores of GAD-7 and ITAQ in patients with depression were higher than those in patients with AD and schizophrenia (P < 0.001). The total score of MMSE in patients with schizophrenia and depression was higher than that in patients with AD (P < 0.001) (Table 2).
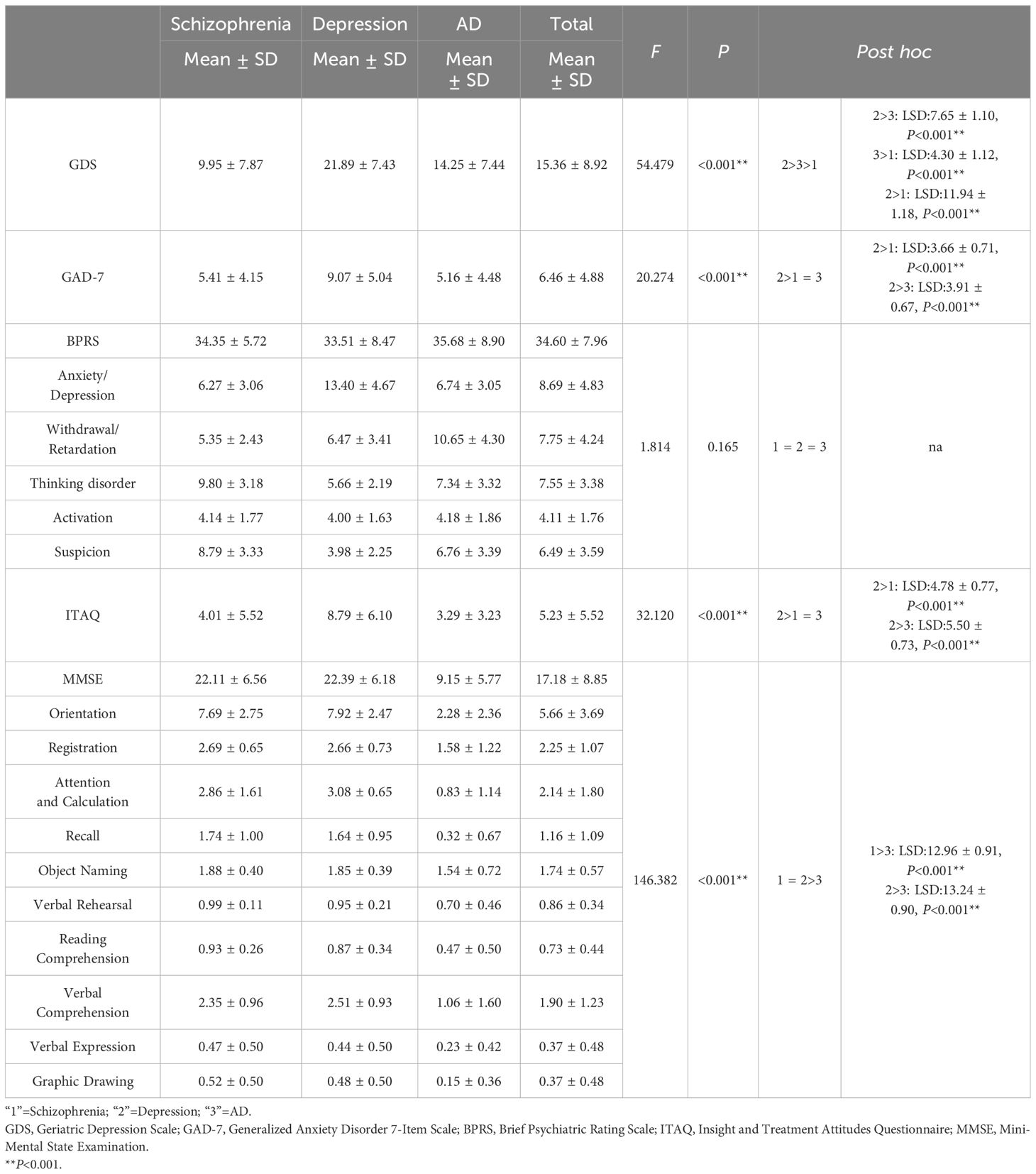
Table 2. Mental status.
The results showed that approximately 60% of respondents had been diagnosed with at least two types of somatic diseases. The three most frequent diseases were from cardiovascular (54.6%), endocrine (36.2%), and nervous (35.1%) systems. The incidence of circulatory system diseases in patients with depression and AD was higher than that in patients with schizophrenia (P < 0.05). The incidence of respiratory system diseases in patients with AD was highest, followed by patients with schizophrenia, and patients with depression had the lowest incidence (P < 0.05). The incidence of nervous system diseases in patients with AD was highest, followed by patients with depression, and patients with schizophrenia had the lowest incidence (P < 0.05) (Table 3).
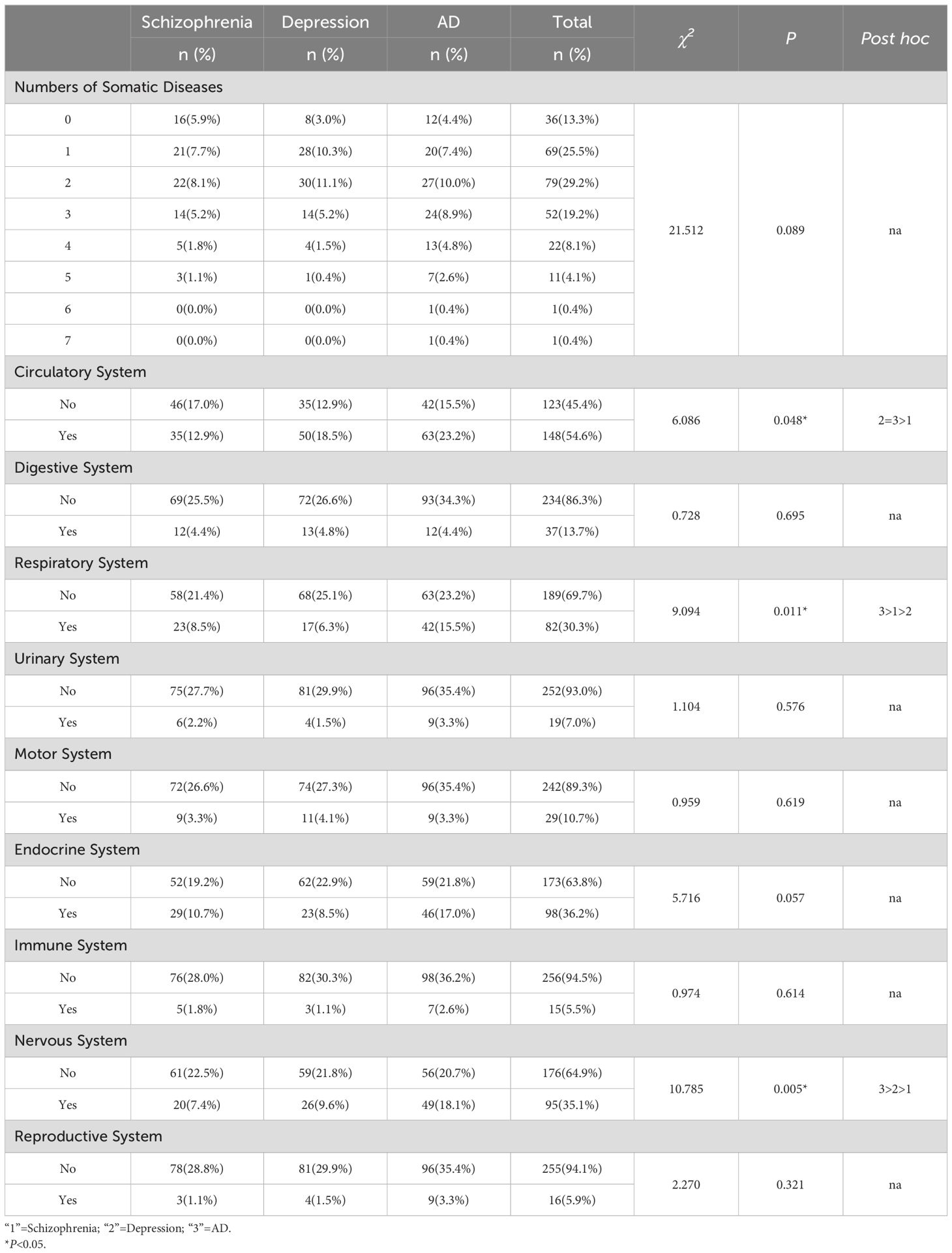
Table 3. Somatic diseases.
The FAQ, SSRS, Barthel ADL Index, water-swallowing test, SSA, and MNA scale were used to evaluate the patients’ social and daily activities. The outcomes demonstrated that the total scores of FAQ and SSA in patients with AD were higher than those in patients with schizophrenia and depression (P < 0.001), while patients with depression had statistically lower SSRS scores than patients with schizophrenia and patients with AD (P < 0.05). Furthermore, patients with AD had lower Barthel ADL Index scores and water-swallowing test (P < 0.001). MNA scores of patients with schizophrenia were higher than those of patients with depression and AD, with statistical significance (P < 0.05) (Table 4).
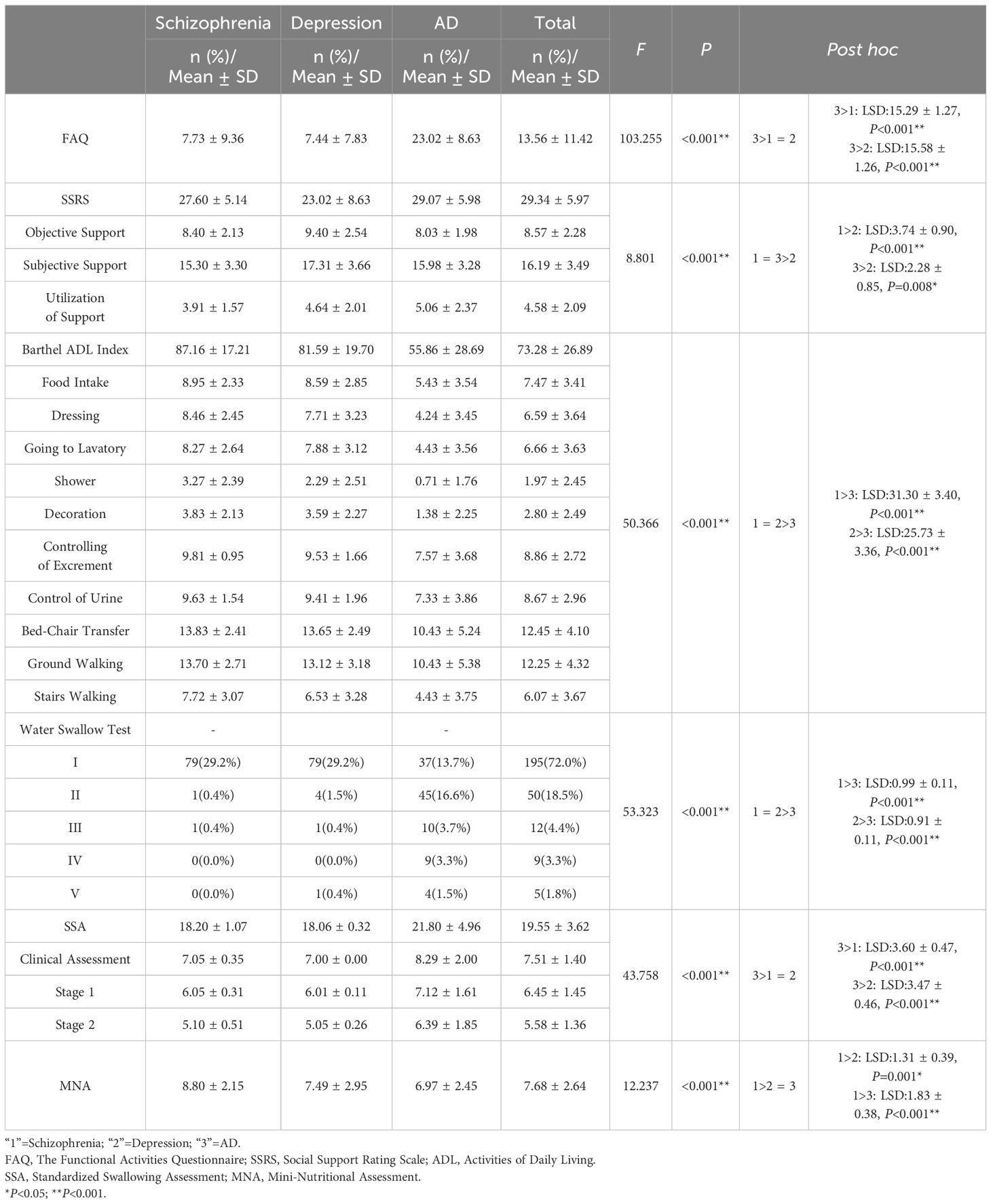
Table 4. Social and daily living function.
The NGASR and BVC were used to assess the patients’ risk of suicide. The results revealed that the NGASR scores of patients with depression were higher than those of patients with schizophrenia and AD, which was statistically significant (P < 0.001). Patients with AD had the highest BVC total score, followed by that of patients with schizophrenia and patients with depression had lowest score, and the difference was statistically significant (P < 0.05) (Table 5).
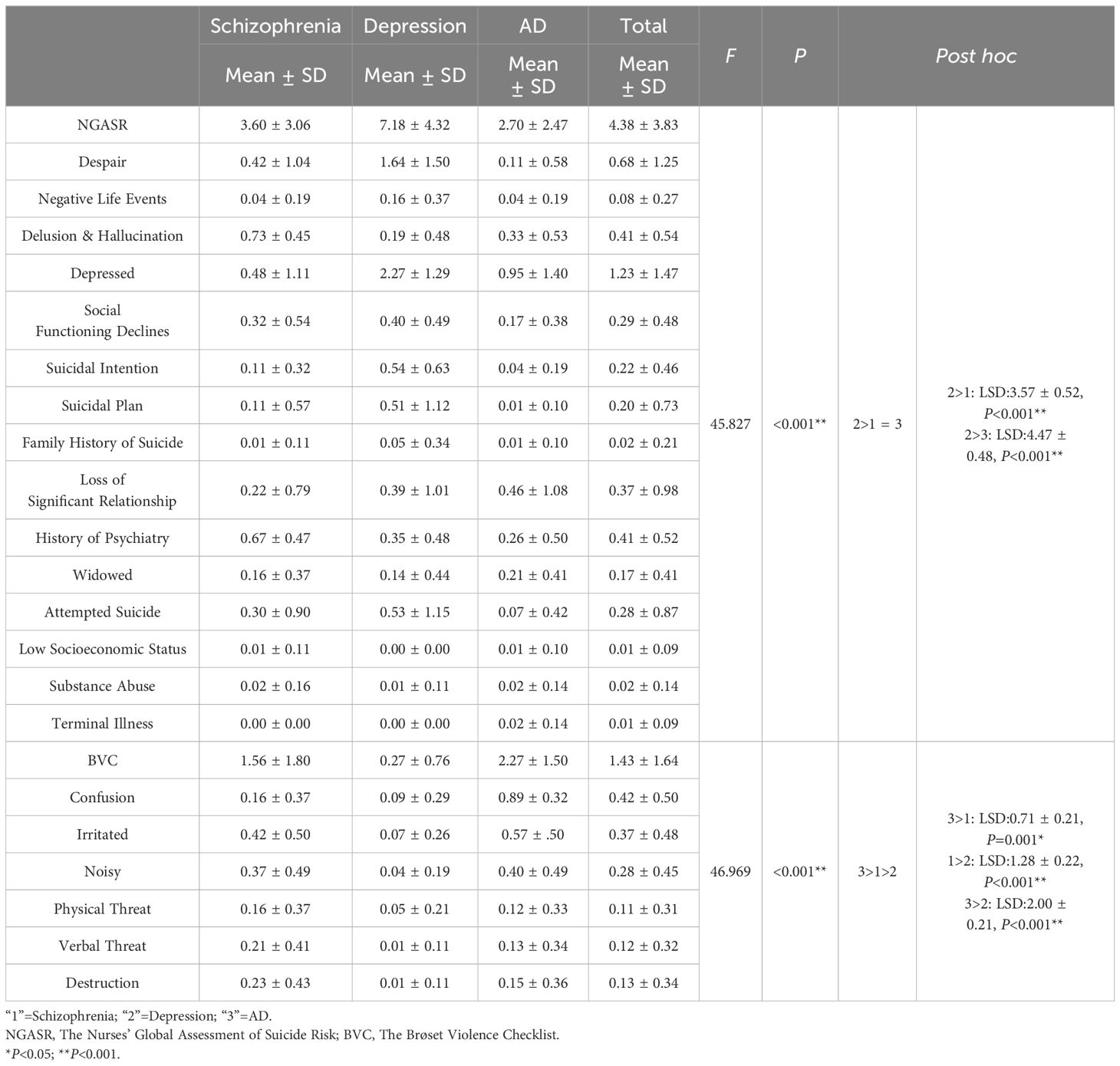
Table 5. Nursing risk.
Understanding the clinical characteristics of mental disorders among older adults can help medical professionals to rationally allocate medical resources as well as to develop nursing care plans. Our finding suggested that depression, schizophrenia, and AD were three most prevalent mental disorders among older adults. Previous studies by Huang et al. (2019) reported that among adults aged above 65 years, the weighted lifetime prevalence of AD was more than 5%, followed by depression and schizophrenia (45). In addition to mental disorders, a number of older adults suffered from somatic discomfort, for instance chronic pain, weakness, and malnutrition (46). Moreover, older people were found to be more prone to experience adverse life events including retirement, widowhood, infirmity, and loss of independence. Such events can result in experiencing psychological emotions like hopelessness and loneliness. Owing to a variety of biological, psychological, and social factors, older adults had a lower capacity for life adaptation, which might have a negative psychological impact and even trigger mental disorders.
Almost half of respondents were diagnosed with at least three somatic diseases, and circulatory diseases were the most threatening. Physical condition should be a vital factor influencing mental health among older adults. The decline of physical health was found to result in poor mental well beings. Therefore, applying interventions to relieving somatic diseases is significant to improve the mental health among older adults. Our findings highlighted that the majority of aged psychiatric patients (55.7%) had been affected by circulatory diseases. Ungvari et al. (2021) noted that the health conditions of older adults diagnosed with hypertension were more likely to be complicated with cognitive impairments (47). Therefore, in regard to mental health care for older adults, despite the chief complaint of mental illnesses, attention should be paid to patients’ physical condition as well, particularly to various circulatory diseases (48). In addition, we found that the proportion of respiratory system diseases and nervous system diseases among patients with AD was higher compared to schizophrenia and depression. A study by Agnieszka et al. (2024) showed that patients with AD experienced respiratory disturbances (49), which was consistent with our results. Respiratory system disorders are a frequent cause of mortality in patients with AD, potentially attributable to diminished respiratory muscle strength. AD is a chronic, progressive neurodegenerative disorder characterized by neurodegenerative changes in the brain. These changes could adversely affect lung function, contributing to respiratory system diseases. Conversely, impaired lung function leads to hypoxia, which might exacerbate neurodegenerative processes and accelerate the progression of dementia. Therefore timely detection and treatment of respiratory infections is important. In addition, nursing staff should regularly assess cognitive function and develop targeted cognitive training plans based to delay the decline of cognitive function, such as memory training, attention training (49).
Adequate care requirements should be offered to individuals who have been diagnosed with varied mental diseases. The results of this study demonstrated that the MMSE score of schizophrenic patients was (22.11 ± 6.56), indicating that they had cognitive impairment. Our result was in consistent with the study by Goonathilake et al. (2022) (50). Patients with schizophrenia were typically distressed by hallucinations and delusions, such psychotic symptoms would impair individuals’ ability to perceive reality objectively and lead to cognitive impairment. In relation to schizophrenia, neurodevelopmental theories proposed, abnormal brain development could impede the acquisition of cognitive abilities throughout the ontogenetic process, thus neurodevelopmental abnormalities might serve as one of critical reasons of the cognitive deficits in individuals with schizophrenia (51, 52). Furthermore, patients with schizophrenia experience worse decline in cognitive abilities in later life, this might due to the adverse effects on cerebrovascular function caused by unhealthy lifestyle, obesity, or hyperglycemia (53, 54). Noticeably, the study by Zhu et al. (2022) reported that amisulpride augmentation therapy improved cognitive performance and psychopathology in clozapine-resistant treatment-refractory schizophrenia, however further research evaluating the effectiveness of amisulpride augmentation therapy in older adults are needed (55). Besides, this study demonstrated that elderly patients with depression, and AD exhibited significant psychiatric symptoms as well. Previous research had identified substantial symptom overlap among various mental disorders. For instance, cognitive impairments in domains such as attention, social cognition, and working memory were common in conditions like schizophrenia and severe depression. This overlap in symptoms might be partially attributed to genetic connections between these mental illnesses (56). Compared with patients with schizophrenia and depression, patients with AD had lower Barthel ADL index scores and worse swallowing function, based on study’s findings. As opposed to the other two sorts of patients, they scored higher on the FAQ and SSA. This was in accordance with earlier studies that have demonstrated a progressive decline in patients with AD’ capacity to perform daily tasks or even live independently. Due to mental disorder, the diminished capacity might be ascribed to impaired cognitive and judgmental abilities among patients with AD. Furthermore, several previous cohort studies had demonstrated a correlation between the intensity of symptoms experienced by patients with AD and the degree of decrease in their capacity to carry out activities of daily living (57). Dysphagia is common in dementia patients. In individuals with dementia, the voluntary phases of swallowing, particularly the oral preparation and oral phases, are impaired due to cognitive deficits that hinder voluntary motor control (58, 59). To realize the autonomy and independence of patients with AD as soon as possible, adequate nursing measures should be adopted at different stages of the disease (60). As a result of the dysfunction brought on by the condition, people with AD have a significant requirement for food intake and personal hygiene since they have a considerably diminished capacity to take care of themselves. The results of this study, which showed that patients with depression had a higher NGASR score than patients with schizophrenia or AD, our finding was consistent with the researches indicating that hospitalized patients with depression were at greater risk of suicide than patients with other mental disorders (61). A study included psychological autopsy found that more than half of suicide victims exhibited characteristics of depression at some point in their lives (62). This could be explained by the fact that individuals with depression frequently displayed negative attitudes, pessimism, and suicidal thoughts and actions. Thus, the main clinical focus of psychiatric caregivers should be prompt assessment of patients with depression who were at high risk of suicide and appropriate care interventions to lower the risk. Hence, extensive nursing care should be provided to elderly patients who are depressed. Nurses should closely monitor patient’s abnormal bahavior and react promptly to an emergency and avoid suicide. In addition, compared to the other two types of disorders, patients with AD had a higher risk of violence. The aggressive and destructive behavior of elderly patients with AD might cause considerable pressure on caregivers. This might be related to the severe decline in cognitive abilities of patients with AD as the disease progresses, which affects their ability to think clearly and communicate effectively, ultimately leading to the occurrence of violence. Effective communication and moderation techniques could help prevent and mitigate aggressive incidents. Besides, providing support and education for nursing staff is crucial. The goal of intervention is to create a safe and supportive environment for patients, and to adopt a compassionate and multi-faceted approach to managing aggressive behavior (63).
Limitations of this study should be noted. This study is a retrospective study of elderly patients admitted to the psychiatric department continuously. Participants were recruited from Brain Hospital Affiliated to Guangzhou Medical University, this might have selection bias and recall bias. In this study, the symptom severity of the same diseases varies greatly from the samples, the sample collection time span was large, and the symptom manifestations may be different in different seasons, which might affect its objectivity. In future studies, sample collection should be done from the same source and in a concentrated time to improve sample homogeneity.
In conclusion, a great proportion of elderly individuals with mental illness might experienced irregularities in their thinking, cognition, emotions, and behavior. The manifestations of various types of mental illness had diverse clinical characteristics, physical sickness frequently coexists with mental illness in elderly individuals. Treatment of various types of mental disorders, such as employing various nursing interventions, is crucial for aged adults with mental illnesses.
The results of this study help nursing staff understand the clinical characteristics of hospitalized elderly patients with mental disorders, provide evidence for the future prevention and treatment of elderly schizophrenia, emotional disorders, and AD, and also provide ideas for the development of effective intervention measures. The adoption of various nursing interventions is crucial for all types of mental illness.
The raw data supporting the conclusions of this article will be made available upon reasonable request to the corresponding author.
This study obtained ethical approval from the IRB of the Affiliated Brain Hospital of Guangzhou Medical University. Informed consent was obtained from all participants before inclusion. The entire study was carried out in accordance with the Declaration of Helsinki. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
WW: Conceptualization, Data curation, Investigation, Methodology, Resources, Software, Validation, Visualization, Writing – original draft, Writing – review & editing. JY: Conceptualization, Data curation, Investigation, Methodology, Resources, Software, Validation, Visualization, Writing – original draft, Writing – review & editing. YW: Conceptualization, Data curation, Investigation, Methodology, Resources, Software, Validation, Visualization, Writing – original draft, Writing – review & editing. JH: Conceptualization, Data curation, Investigation, Methodology, Validation, Visualization, Writing – original draft. HW: Conceptualization, Data curation, Investigation, Methodology, Validation, Visualization, Writing – original draft. FL: Conceptualization, Data curation, Investigation, Methodology, Validation, Visualization, Writing – original draft. SW: Conceptualization, Investigation, Methodology, Software, Validation, Visualization, Writing – original draft. JW: Conceptualization, Investigation, Methodology, Software, Validation, Visualization, Writing – original draft. ZL: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. JG: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. AX: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing.
The author(s) declare that financial support was received for the research and/or publication of this article. This work was supported by Research Project of Guangzhou Municipal Health Commission (2023A031002), Research Project of Guangzhou Municipal Health Commission (SL2022A03J01476), Research Project of Department of Education of Guangdong Province (2021JD119) and Guangzhou Research oriented Hospital.
We would like to thank all the patients who have contributed to this study.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Bloom DE, Canning D, Fink G. Population aging and economic growth. PGDA Work Papers. (2008) 23:61–89.
2. Gwozdz W, Sousa-Poza A. Ageing, health and life satisfaction of the oldest old: an analysis for Germany. Soc Sci Electron Publish. (2010) 97:397–417. doi: 10.1007/s11205-009-9508-8
3. Zhang X, Huang J, Luo Y. The effect of the universal two-child policy on medical insurance funds with a rapidly ageing population: evidence from China’s urban and rural residents’ medical insurance. BMC Public Health. (2021) 21:1444. doi: 10.1186/s12889-021-11367-7
4. Khan HTA. Population ageing in a globalized world: Risks and dilemmas? J Eval Clin Pract. (2019) 25:754–60. doi: 10.1111/jep.13071
5. Zhang HG, Fan F, Zhong BL, Chiu HF. Relationship between left-behind status and cognitive function in older Chinese adults: a prospective 3-year cohort study. Gen Psychiatr. (2023) 36:e101054. doi: 10.1136/gpsych-2023-101054
6. Cho SJ, Stout-Delgado HW. Aging and lung disease. Annu Rev Physiol. (2020) 82:433–59. doi: 10.1146/annurev-physiol-021119-034610
7. Ma Y, Liang L, Zheng F, Shi L, Zhong B, Xie W. Association between sleep duration and cognitive decline. JAMA Netw Open. (2020) 3:e2013573. doi: 10.1001/jamanetworkopen.2020.13573
8. Chen X, Giles J, Yao Y, Yip W, Meng Q, Berkman L, et al. The path to healthy ageing in China: a Peking University-Lancet Commission. Lancet. (2022) 400:1967–2006. doi: 10.1016/S0140-6736(22)01546-X
9. Zhu Y, Li C, Xie W, Zhong B, Wu Y, Blumenthal JA. Trajectories of depressive symptoms and subsequent cognitive decline in older adults: a pooled analysis of two longitudinal cohorts. Age Ageing. (2022) 51:afab191. doi: 10.1093/ageing/afab191
10. Yu J, Li J, Cuijpers P, Wu S, Wu Z. Prevalence and correlates of depressive symptoms in Chinese older adults: a population-based study. Int J Geriatr Psychiatry. (2012) 27:305–12. doi: 10.1002/gps.v27.3
11. Phongsavan P, Grunseit AC, Bauman A, Broom D, Byles J, Clarke J, et al. Age, gender, social contacts, and psychological distress: findings from the 45 and up study. J Aging Health. (2013) 25:921–43. doi: 10.1177/0898264313497510
12. Byers AL, Yaffe K, Covinsky KE, Friedman MB, Bruce ML. High occurrence of mood and anxiety disorders among older adults: The National Comorbidity Survey Replication. Arch Gen Psychiatry. (2010) 67:489–96. doi: 10.1001/archgenpsychiatry.2010.35
13. Richmond-Rakerd LS, D’Souza S, Milne BJ, Caspi A, Moffitt TE. Longitudinal associations of mental disorders with physical diseases and mortality among 2.3 million New Zealand citizens. JAMA Netw Open. (2021) 4:e2033448. doi: 10.1001/jamanetworkopen.2020.33448
14. Donovan NJ, Amariglio RE, Zoller AS, Rudel RK, Gomez-Isla T, Blacker D, et al. Subjective cognitive concerns and neuropsychiatric predictors of progression to the early clinical stages of Alzheimer disease. Am J Geriatr Psychiatry. (2014) 22:1642–51. doi: 10.1016/j.jagp.2014.02.007
15. Weeks SM, Giles K. Length of stay in hospital for people with severe mental illness. Int J Evid Based Healthc. (2015) 13:273–4. doi: 10.1097/XEB.0000000000000032
16. Liu ZW, Sun L, Zhang JJ, Yang RC, Liu Y. Disease composition and clinical characteristics of geriatric mental disorder inpatients in a psychiatric hospital of Fuyang. J Int Psychl. (2024) 51:123–126,142.
17. Hou CL, Zang Y, Ma XR, Cai MY, Li Y, Jia FJ, et al. The relationship between sleep patterns, quality of life, and social and clinical characteristics in Chinese patients with schizophrenia. Perspect Psychiatr Care. (2017) 53:342–9. doi: 10.1111/ppc.2017.53.issue-4
18. Xu YM, Deng F, Zhong BL. Facial emotion identification impairments in Chinese persons living with schizophrenia: A meta-analysis. Front Psychiatry. (2022) 13:1097350. doi: 10.3389/fpsyt.2022.1097350
19. Zhong BL, Ruan YF, Xu YM, Chen WC, Liu LF. Prevalence and recognition of depressive disorders among Chinese older adults receiving primary care: A multi-center cross-sectional study. J Affect Disord. (2020) 260:26–31. doi: 10.1016/j.jad.2019.09.011
20. Zhong BL, Xu YM, Xie WX, Li Y. Can P300 aid in the differential diagnosis of unipolar disorder versus bipolar disorder depression? A meta-analysis of comparative studies. J Affect Disord. (2019) 245:219–27. doi: 10.1016/j.jad.2018.11.010
21. Lukoff D, Liberman RP, Nuechterlein KH. Symptom monitoring in the rehabilitation of schizophrenic patients. Schizophr Bull. (1986) 12:578–602. doi: 10.1093/schbul/12.4.578
22. Overall JE, Gorham DR. The brief psychiatric rating scale. Psychol Rep. (1962) 10:799–812. doi: 10.2466/pr0.1962.10.3.799
23. Zhang HY, Chong MC, Tan MP, Chua YP, Zhang JH. The association between depressive symptoms and sarcopenia among community-dwelling older adults: A cross-sectional study. J Multidiscip Healthc. (2022) 15:837–46. doi: 10.2147/JMDH.S355680
24. Yesavage JA, Brink TL, Rose TL, Lum O, Huang V, Adey M, et al. Development and validation of a geriatric depression screening scale: a preliminary report. J Psychiatr Res. (1982) 17:37–49. doi: 10.1016/0022-3956(82)90033-4
25. Dhira TA, Rahman MA, Sarker AR, Mehareen J. Validity and reliability of the Generalized AnxietyDisorder-7 (GAD-7) among university students of Bangladesh. PloS One. (2021) 16:e0261590. doi: 10.1371/journal.pone.0261590
26. Islam MA, Barna SD, Raihan H, Khan MNA, Hossain MT. Depression and anxiety among university students during the COVID-19 pandemic in Bangladesh: A web-based cross-sectional survey. PloS One. (2020) 15:e0238162. doi: 10.1371/journal.pone.0238162
27. McEvoy JP, Apperson LJ, Appelbaum PS, Ortlip P, Brecosky J, Hammill K, et al. Insight in schizophrenia. Its relationship to acute psychopathol J Nerv Ment Dis. (1989) 177:43–7. doi: 10.1097/00005053-198901000-00007
28. Martins NIM, Caldas PR, Cabral ED, Lins CCDSA, Coriolano MDGWS. Cognitive assessment instruments used in elderly Brazilians in the last five years. Instrumentos de avaliação cognitiva utilizados nos últimos cinco anos em idosos brasileiros. Cien Saude Colet. (2019) 24:2513–30. doi: 10.1590/1413-81232018247.20862017
29. Folstein MF, Folstein SE, McHugh PR. Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res. (1975) 12:189–98. doi: 10.1016/0022-3956(75)90026-6
30. Pfeffer RI, Kurosaki TT, Harrah CH Jr, Chance JM, Filos S. Measurement of functional activities in older adults in the community. J Gerontol. (1982) 37:323–9. doi: 10.1093/geronj/37.3.323
31. Li Y, Fang C, Xiong M, Hou H, Zhang Y, Zhang C. Exploring fear of cancer recurrence and related factors among breast cancer patients: A cross-sectional study. J Adv Nurs. (2024) 80:2403–14. doi: 10.1111/jan.16009
32. Wu Y, Yan Z, Fornah L, Zhao J, Wu S. The mediation effect of social support between stigma and social alienation in patients with stroke. Front Public Health. (2023) 11:1290177. doi: 10.3389/fpubh.2023.1290177
33. Xiao SY. Theoretical basis and research application of Social Support Rating Scale. J Clin Psychiatry. (1994) 4:98–100.
34. Hormozi S, Alizadeh-Khoei M, Sharifi F, Taati F, Aminalroaya R, Fadaee S, et al. Iranian version of barthel index: validity and reliability in outpatients’ Elderly. Int J Prev Med. (2019) 10:130. doi: 10.4103/ijpvm.IJPVM_579_18
35. Ye J, Pan Y, Wei Y, Yuan L, Hu Z, Wu S, et al. Influencing factors of elderly hospitalized psychiatric patients complicated with physical disease: a cross-sectional study of 332 patients in Guangzhou China. BMC Psychiatry. (2024) 24:952. doi: 10.1186/s12888-024-06402-x
36. Ye J, Pan Y, Zhou T, Liu F, Wei Y, Chen J, et al. Evaluating dysphagia in Alzheimer’s disease: the significance of age and medical comorbidities,a cross-sectional study from a tertiary psychiatric hospital in Guangzhou China. Front Psychiatry. (2024) 15:1482951. doi: 10.3389/fpsyt.2024.1482951
37. Osawa A, Maeshima S, Tanahashi N. Water-swallowing test: screening for aspiration in stroke patients. Cerebrovasc Dis. (2013) 35:276–81. doi: 10.1159/000348683
38. Ellul J, Barer D. Interobserver reliability of a standardised swallowing assessment (SSA). Cerebrovascul Dis. (1996) 6:152–3.
39. Ye J, Wu C, Chen J, Wang H, Pan Y, Huang X, et al. Effectiveness of nurse-delivered stepwise swallowing training on dysphagia in patients with Alzheimer’s disease: A multi-center randomized controlled trial. Int J Nurs Stud. (2024) 150:104649. doi: 10.1016/j.ijnurstu.2023.104649
40. Vellas B, Guigoz Y, Garry PJ, Nourhashemi F, Bennahum D, Lauque S, et al. The Mini Nutritional Assessment (MNA) and its use in grading the nutritional state of elderly patients. Nutrition. (1999) 15:116–22. doi: 10.1016/S0899-9007(98)00171-3
41. van Veen M, van Weeghel I, Koekkoek B, Braam AW. Structured assessment of suicide risk in a psychiatric emergency service: Psychometric evaluation of the Nurses’ Global Assessment of Suicide Risk scale (NGASR). Int J Soc Psychiatry. (2015) 61:287–96. doi: 10.1177/0020764014543311
42. Ferrara P, D’Agostino A, Destrebecq A. Predictive validity of the NGASR in suicide attempts and early readmission to a psychiatric inpatient unit. Psychiatr Serv. (2019) 70:1072. doi: 10.1176/appi.ps.201900185
43. Woods P, Almvik R. The Brøset violence checklist (BVC). Acta Psychiatr Scand Suppl. (2002) 106:103–5. doi: 10.1034/j.1600-0447.106.s412.22.x
44. Abderhalden C, Needham I, Dassen T, Halfens R, Haug HJ, Fischer J. Predicting inpatient violence using an extended version of the Brøset-Violence-Checklist: instrument development and clinical application. BMC Psychiatry. (2006) 6:17. doi: 10.1186/1471-244X-6-17
45. Huang Y, Wang Y, Wang H, Liu Z, Yu X, Yan J, et al. Prevalence of mental disorders in China: a cross-sectional epidemiological study. Lancet Psychiatry. (2019) 6:211–24. doi: 10.1016/S2215-0366(18)30511-X
46. Houben N, Janssen EPCJ, Hendriks MRC, van der Kellen D, van Alphen BPJ, van Meijel B. Physical health status of older adults with severe mental illness: The PHiSMI-E cohort study. Int J Ment Health Nurs. (2019) 28:457–67. doi: 10.1111/inm.2019.28.issue-2
47. Ungvari Z, Toth P, Tarantini S, Prodan CI, Sorond F, Merkely B, et al. Hypertension-induced cognitive impairment: from pathophysiology to public health. Nat Rev Nephrol. (2021) 17:639–54. doi: 10.1038/s41581-021-00430-6
48. Cannon JA, Moffitt P, Perez-Moreno AC, Walters MR, Broomfield NM, McMurray JJV, et al. Cognitive impairment and heart failure: systematic review and meta-analysis. J Card Fail. (2017) 23:464–75. doi: 10.1016/j.cardfail.2017.04.007
49. Wrzesień A, Andrzejewski K, Jampolska M, Kaczyńska K. Respiratory dysfunction in Alzheimer’s disease-consequence or underlying cause? Applying animal models to the study of respiratory malfunctions. Int J Mol Sci. (2024) 25:2327. doi: 10.3390/ijms25042327
50. Goonathilake P, Ediriweera D, Ruban R, Isuru A. Prevalence and correlates of cognitive impairment in schizophrenia: a cross-sectional study from a teaching hospital southern Sri Lanka. BMC Psychiatry. (2022) 22:716. doi: 10.1186/s12888-022-04368-2
51. Murray RM, Lewis SW. Is schizophrenia a neurodevelopmental disorder? Br Med J (Clin Res Ed). (1987) 295:681–2.
52. Bora E. Neurodevelopmental origin of cognitive impairment in schizophrenia. Psychol Med. (2015) 45:1–9. doi: 10.1017/S0033291714001263
53. Smith E, Hay P, Campbell L, Trollor JN. A review of the association between obesity and cognitive function across the lifespan: implications for novel approaches to prevention and treatment. Obes Rev. (2011) 12:740–55. doi: 10.1111/j.1467-789X.2011.00920.x
54. Strachan MWJ, Reynolds RM, Marioni RE, Price JF. Cognitive function, AD and type 2 diabetes mellitus in the elderly. Nat Rev Endocrinol. (2011) 7:108–14. doi: 10.1038/nrendo.2010.228
55. Zhu MH, Liu ZJ, Hu QY, Yang JY, Jin Y, Zhu N, et al. Amisulpride augmentation therapy improves cognitive performance and psychopathology in clozapine-resistant treatment-refractory schizophrenia: a 12-week randomized, double-blind, placebo-controlled trial. Mil Med Res. (2022) 9:59. doi: 10.1186/s40779-022-00420-0
56. Liu Y, Xiao X, Yang Y, Yao R, Yang Q, Zhu Y, et al. The risk of Alzheimer’s disease and cognitive impairment characteristics in eight mental disorders: A UK Biobank observational study and Mendelian randomization analysis. Alzheimers Dement. (2024) 20:4841–53. doi: 10.1002/alz.14049
57. Buccione I, Perri R, Carlesimo GA, Fadda L, Serra L, Scalmana S, et al. Cognitive and behavioural predictors of progression rates in AD disease. Eur J Neurol. (2007) 14:440–6. doi: 10.1111/j.1468-1331.2007.01693.x
58. Nawaz S, Tulunay-Ugur OE. Dysphagia in the older patient. Otolaryngol Clin North Am. (2018) 51:769–77. doi: 10.1016/j.otc.2018.03.006
59. Parlak MM, Babademez MA, Alicura Tokgöz S, Bizpınar Ö, Saylam G. Evaluation of swallowing function according to the stage of Alzheimer’s disease. Folia Phoniatr Logop. (2022) 74:186–94. doi: 10.1159/000519263
60. Suwa S, Yumoto A, Ueno M, Yamabe T, Hoshishiba Y, Sato M. Characteristics of care methods for daily life disabilities in Alzheimer’s type AD that respect autonomy and independence. Nurs Open. (2019) 6:930–41. doi: 10.1002/nop2.2019.6.issue-3
61. Forray A, Yonkers KA. The collision of mental health, substance use disorder, and suicide. Obstet Gynecol. (2021) 137:1083–90. doi: 10.1097/AOG.0000000000004391
62. Ribeiro JD, Huang X, Fox KR, Franklin JC. Depression and hopelessness as risk factors for suicide ideation, attempts and death: meta-analysis of longitudinal studies. Br J Psychiatry. (2018) 212:279–86. doi: 10.1192/bjp.2018.27
Keywords: aged, Alzheimer’s diseases, depression, schizophrenia, characteristics
Citation: Wang W, Ye J, Wei Y, Huang J, Wang H, Liu F, Wu S, Wu J, Li Z, Guo J and Xiao A (2025) Clinical characteristics of schizophrenia, depression, and Alzheimer’s diseases among older adults: a retrospective study of 271 consecutive admissions. Front. Psychiatry 16:1486626. doi: 10.3389/fpsyt.2025.1486626
Received: 26 August 2024; Accepted: 17 February 2025;
Published: 12 March 2025.
Edited by:
Vincenzo De Luca, University of Toronto, CanadaReviewed by:
Yan-Min Xu, Wuhan Mental Health Center, ChinaCopyright © 2025 Wang, Ye, Wei, Huang, Wang, Liu, Wu, Wu, Li, Guo and Xiao. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Zezhi Li, YmlvbHBzeWNoaWF0cnlAMTI2LmNvbQ==; Jianxiong Guo, anhndW9uZXQwMUAxMjYuY29t; Aixiang Xiao, NTQzMDYxOTEwQHFxLmNvbQ==
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.