 YinHu Tan
YinHu Tan Xue Liang2
Xue Liang2 Yang Wang
Yang Wang
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Psychiatry , 23 January 2025
Sec. Digital Mental Health
Volume 16 - 2025 | https://doi.org/10.3389/fpsyt.2025.1434376
Objective: The purpose of this systematic review and meta-analysis is to examine the impact of telemedicine interventions on the quality of life (QoL) and depression in individuals with spinal cord injury (SCI).
Methods: A literature search was conducted in four electronic databases (PubMed, Web of Science, EMBASE, and the Cochrane Library) from their inception to February 1, 2024. Two authors independently screened the studies and extracted the data. Cochrane’s bias risk tool for randomized controlled trials was used to examine the methodological quality of the included studies. A meta-analysis was conducted using Review Manager (version 5.4) to synthesize the results of the included studies.
Results: A total of 10 trials with 728 participants were included in the review. The results of the meta-analysis showed that telemedicine interventions significantly improved QoL [Standardized Mean Difference (SMD)=0.72, 95% Confidence Interval (CI) (0.11, 1.32), P=0.02] and reduced depression scores [SMD=-0.18, 95% CI (-0.31, -0.05), P=0.006].
Conclusions: Telemedicine interventions are a feasible method to support people with SCI, and can mitigate depression and enhance quality of life. In the future, studies should involve larger sample sizes and extended follow-up periods to validate these findings and to identify the most effective telemedicine interventions for improving the overall health outcomes of individuals with SCI.
Systematic Review Registration: https://www.crd.york.ac.uk/prospero/, identifier CRD42024508702.
SCI is recognized as one of the major clinical challenges of the 21st century, with approximately 500,000 new cases reported worldwide each year (1–3) and a significant increase in incidence among the elderly population (4). Specifically, SCI refers to the structural and functional damage of the spinal cord caused by trauma, disease, or other factors, leading to impairments in motor, sensory, urinary, bowel, and autonomic functions below the level of injury (5), often resulting in permanent paralysis to varying degrees (6). Consequently, post-surgery, people with SCI frequently experience increased pessimism and depression, which diminishes their QoL (7, 8) and imposes a significant economic burden on families and society (9, 10). A study by Van Loo et al. found that 72% of individuals with SCI reported a need for additional care in general, indicating a broad demand for extended support services beyond standard care, which may include but is not limited to telemedicine interventions (11). Telemedicine presents several advantages, including cost savings, enhanced rehabilitation efficiency, and reduced disparities in resource allocation (12). These benefits have led to its widespread adoption for home rehabilitation in people with SCI, particularly following the COVID-19 pandemic (13).
Telemedicine refers to the provision of healthcare services through information and communication technologies, including telephone consultations, video conferencing, web-based platforms, and mobile applications (14). These modalities enable remote monitoring of individuals, consultations, and follow-up care, offering a flexible and accessible alternative to traditional in-person healthcare services. While the effectiveness of telemedicine applications has shown varied results, multiple studies have reported significant positive outcomes for individuals with SCI, particularly in areas such as QoL, functional independence, and care satisfaction. For example, Dallolio et al. (12) found that telemedicine support significantly improved QoL and functional independence for individuals with SCI. In the realm of postoperative pain management, Kolcun et al. (15) observed positive effects from telemedicine, though results for psychological support were mixed. Additionally, Niknamian’s (16) systematic review indicated that telemedicine effectively reduced care costs and enhanced care quality, though results for individuals self-management were variable. Sechrist et al. (17) showed that individuals with SCI experienced significant improvements in satisfaction and rehabilitation outcomes with iPad-based telemedicine, though the effects on long-term psychological support were limited. Similarly, Yuen et al. (18) reported that telemedicine significantly reduced follow-up needs, though psychological support outcomes varied based on individual differences. Additionally, while systematic reviews specifically addressing telemedicine for individuals with SCI are relatively limited compared to other chronic conditions, recent literature has progressively examined its efficacy across diverse health-related concerns within this population. For instance, a systematic review and meta-analysis conducted by Chen et al. (19) demonstrated that telemedicine interventions significantly contribute to the prevention of pressure injuries, which indirectly enhances QoL in individuals with SCI. Rekand et al. (20) investigated the application of remote psychological support for individuals with individuals with SCI, finding that it positively influences the mitigation of depressive symptoms and promotes mental well-being, particularly benefiting those with limited access to in-person psychological services. Furthermore, Mirbaha et al. (21) reviewed various telemedicine service models, underscoring that personalized telemedicine in home care settings markedly improves both QoL and depression management outcomes for individuals with SCI. While these studies elucidate the potential advantages of telemedicine, there remains an absence of systematic reviews and meta-analyses that directly and comprehensively evaluate the effects of telemedicine on overall QoL and depressive symptoms in SCI populations.
Therefore, the objective of this study was to conduct a systematic review and meta-analysis to specifically assess the efficacy of telemedicine interventions in improving quality of life and reducing depression among individuals with SCI, thereby providing further supplementation and evidence to the existing literature.
This systematic review and meta-analysis are reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 statement (22). A protocol for this review was registered on the PROSPERO International Prospective Register of Systematic Reviews (Registration No. PROSPERO CRD42024508702). We searched the following databases for randomized controlled trials from their inception to February 1, 2024: Web of Science, PubMed, Embase, and the Cochrane Library. Different databases were searched using a combination of MeSH terms, subject terms, and free terms. The following terms were used: telemedicine, telerehabilitation, spinal cord injury, and randomized controlled trial. The specific search strategy is detailed in the appendix.
The inclusion criteria for the study were as follows: (1) Study Design: Randomized controlled trials. (2) Participants: Individuals with spinal cord injury. (3) Interventions: The intervention group received telemedicine interventions, including telephone, application-based, web-based, or other remote technologies, while the control group received routine care for SCI. (4) Outcomes: Reported outcomes including at least one of the following: QoL, depression, anxiety, stress.
The exclusion criteria for the study were as follows: (1) Individuals with psychiatric disorders and children with SCI. (2) Secondary studies, such as reviews and systematic evaluations. (3) Studies where the full text was not available or original data was missing. (4) Duplicate publications. (5) Conference papers, dissertations, and theses. (6) Non-English papers.
Endnote X9 software was used to import all references and remove duplicates. The remaining references were independently screened by two researchers according to pre-established inclusion and exclusion criteria. Key information was extracted and cross-checked by both researchers, with any disagreements resolved through discussion or by involving a third researcher. The extracted data included author’s name, year of publication, country, sample size, mean age, research focus, injury duration, injury level, injury etiology, interventions in the experimental and control groups, follow-up duration, and outcome measures.
The risk of bias in the included studies was assessed by two researchers independently using the Cochrane Handbook for Systematic Reviews of Interventions (23). Studies with evident design biases were excluded. The assessment tool covered the following seven domains: random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessors, incomplete outcome data, selective reporting, and other sources of bias. Each domain was rated as “low risk of bias,” “high risk of bias,” or “unclear.” Any disagreements in the assessment were resolved through discussion or by involving a third researcher, resulting in a consensus.
This study employed Review Manager 5.4 software for conducting meta-analyses. When outcome measures were consistent across studies, the effect size was calculated as the mean difference (MD) with corresponding 95% confidence intervals (CIs). For outcome measures with variability, such as differences in assessment tools or measurement scales, standardized mean differences (SMD) were used to facilitate comparability. Heterogeneity among the included studies was assessed using the I² statistic, which measures the proportion of variability across studies attributable to heterogeneity rather than chance. An I² value exceeding 50% indicated substantial heterogeneity, warranting the use of a random-effects model with the DerSimonian and Laird method as implemented in RevMan. For I² values below 50%, a fixed-effects model with the Mantel-Haenszel method was used. Subgroup analyses were performed to investigate sources of heterogeneity based on key study characteristics, including intervention type and duration. A funnel plot was created to visually assess publication bias. Symmetry in the funnel plot indicated a low risk of publication bias, whereas asymmetry suggested potential publication bias or small-study effects. An asymmetrical funnel plot, with missing studies on one side, could suggest selective reporting of significant results. Given the small number of included studies (fewer than 10), the statistical power to detect asymmetry was low, necessitating cautious interpretation of the results.
The PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flow diagram for this study is presented in Figure 1. The search strategy yielded 457 articles from four databases. After removing duplicates and screening titles and abstracts, 48 articles were retained for full-text evaluation. Based on the inclusion and exclusion criteria, only 10 studies (6, 24–32) were included in this meta-analysis. All of these studies were randomized controlled trials published between 2012 and 2023.
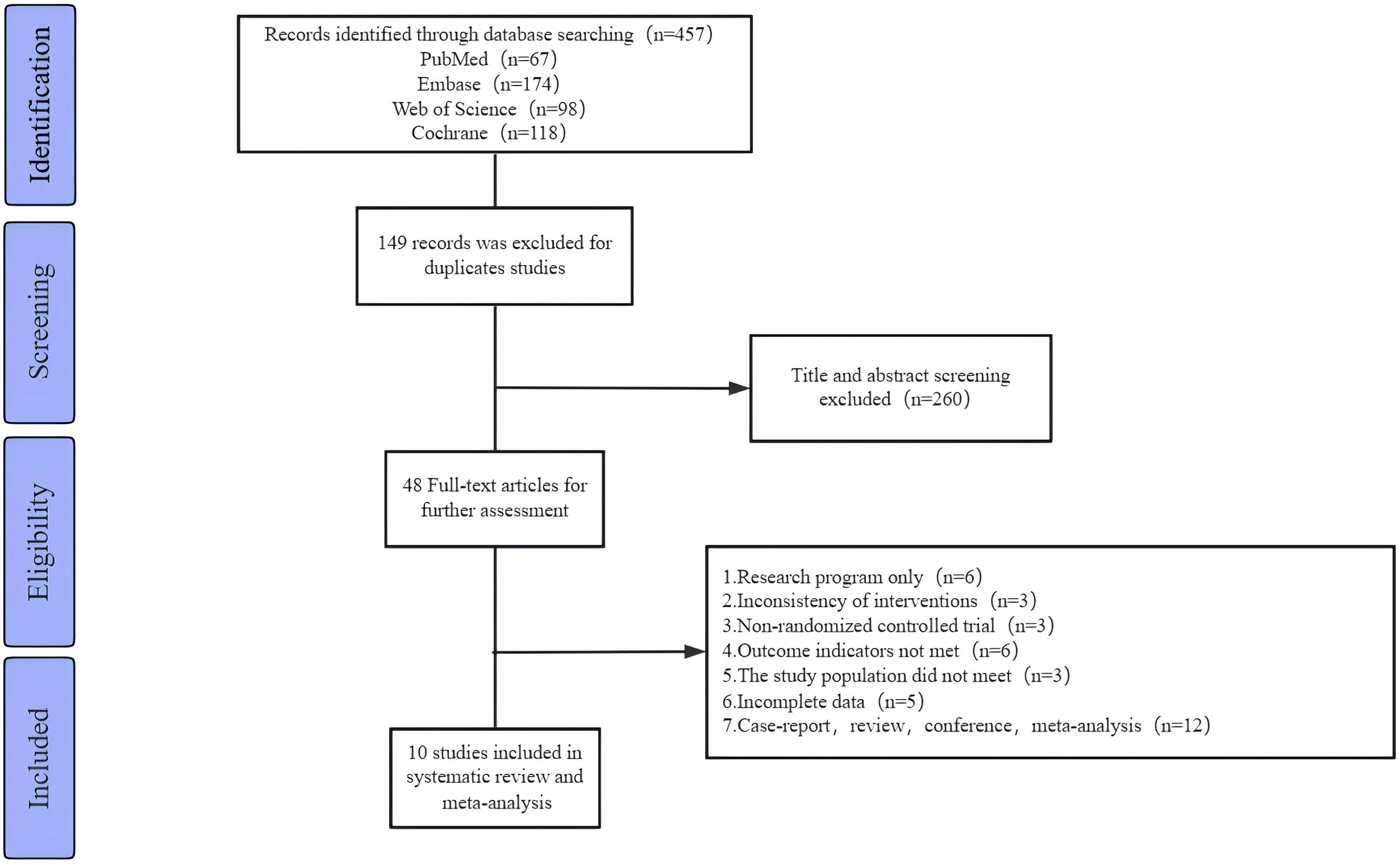
Figure 1. Flowchart of study selection.
According to the Cochrane Handbook’s assessment of bias risk in the included studies, the results indicate that a high risk of bias was present in only a few areas, while most criteria were met satisfactorily, suggesting that the overall quality of the included studies was moderate (33). Seven studies (24, 26–29, 31, 32) described the methods of random sequence generation, while three studies (6, 25, 30) mentioned randomization without providing specific details. Additionally, four studies (24–26, 29) implemented allocation concealment, indicating a lower risk of bias. Regarding detection bias, one study (25) employed double-blinding for both participants and assessors. In eight studies (6, 24, 26, 27, 29–32), it was unclear whether blinding was applied to participants, and in three studies (6, 26, 32), it was unclear whether assessors were blinded. One study (28) exhibited a high risk of bias concerning the blinding of participants or assessors. The risk of bias for incomplete outcome data, selective reporting, or other biases was generally low across the 10 included studies (6, 24–32).Detailed risk of bias assessments and summaries are presented in Figures 2 and 3.
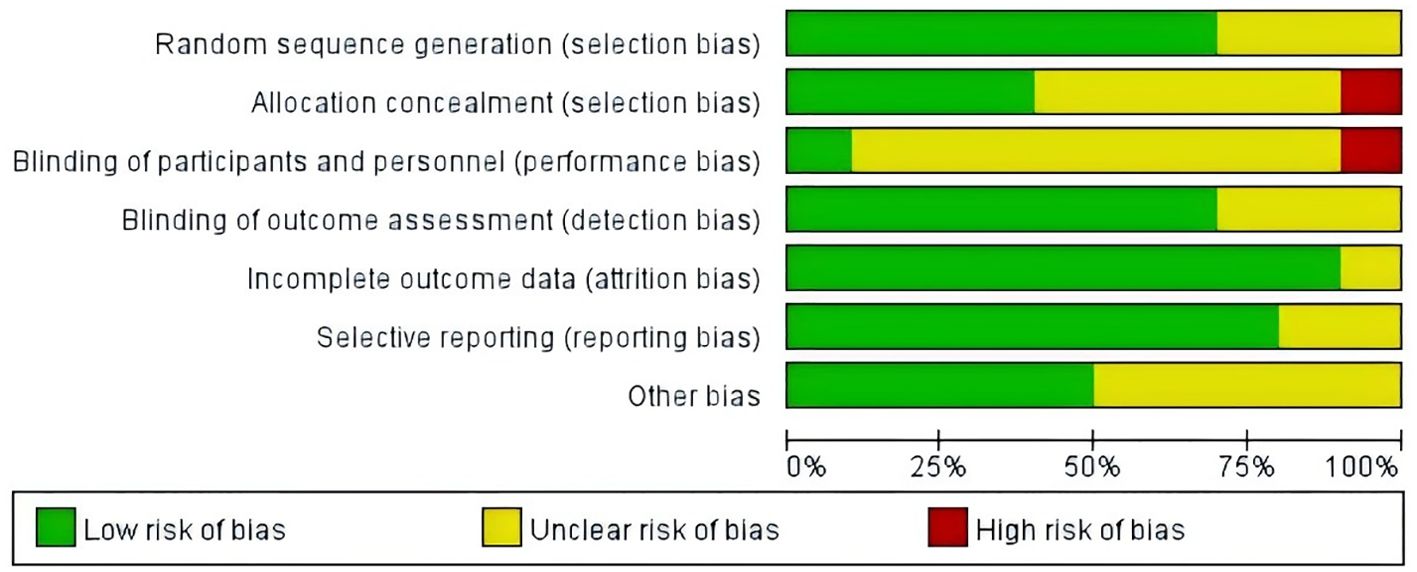
Figure 2. Risk of bias graph.

Figure 3. Risk of bias summary.
Among the 10 included studies (6, 24–32), there were a total of 728 participants, with an average age ranging from 40 to 60 years. These studies were published between 2012 and 2023 and were conducted in seven countries, including the United States (n=3) (28, 30, 31), the United Kingdom (n=1) (26), Australia (n=2) (27, 32), Canada (n=1) (25), China (n=2) (6, 29), India and Bangladesh (n=1) (24). Five studies (24, 27, 28, 30, 31) utilized telephone-based remote interventions, Five studies (25, 26, 29, 32) employed web-based or app-based online learning. In the study by Hearn et al., the remote intervention was delivered via a webpage, enabling participants to engage in mindfulness training through audio sessions provided on the site. However, the article did not specify the website address or the name of the webpage. Chemtob et al. (25) utilized the REACTS® video software for interventions, which provided counseling sessions aimed at enhancing motivation for recovery and participation in physical exercise through behavior change techniques and self-regulation strategies. Coulter et al. (26) employed a self-developed website (www.webbasedphysio.com) for remote personalized physical therapy, enabling individuals to complete rehabilitation exercises tailored to their specific exercise plans, thereby better meeting each individual’s needs. One study utilized SurveyMonkey© software, which provided online learning packages for remote education, helping individuals with SCI find employment, facilitate reintegration into society, and reduce anxiety. Liu et al. (29) utilized an app called ‘Together,’ which included post-discharge health education and follow-up services. Individuals could use the app to interact with researchers via video, phone calls, and text messages to address any issues. The team led by Migliorini et al. (32) developed the Electronic Personal Administration of Cognitive Therapy (ePACT) program, which included a 10-module skills and psychological education plan aimed at improving negative emotions through structured learning. One study (6) utilized an online home care intervention that included video education and an internet platform built using WeChat, a mobile app, telephone, Microblog, and QQ groups. This platform provided multi-channel access to consultation services for care, medical treatment, prevention, and health maintenance. Additionally, researchers could publish disease-related information on the platform for individuals to access and learn from, and they could also engage in one-on-one conversations with the researchers. The follow-up duration in the included studies ranged from 4 weeks to 12 months.
The degree of depression was assessed using various scales, including the Depression Anxiety Stress Scale-21 (DASS-21), Patient Health Questionnaire-9 (PHQ-9), the Hospital Anxiety and Depression Scale (HADS), and Beck Depression Inventory-II (BDI-II), with lower scores indicating less severe depression. The QoL was evaluated using the Delighted-Terrible Scale (DTS), The World Health Organization Quality of Life Brief Scale (WHO-QOL BREF), Euro Quality of Life 5-Dimensional 5-Level (EQ-5D-5L), The Life Satisfaction Questionnaire-11 (LSQ-11), and The MOS 36-Item Short Form Health Survey (SF-36), with higher scores indicating better QoL. Additionally, anxiety was assessed using the HADS and DASS-21 subscales, while stress was evaluated using the DASS-21 subscale. Detailed characteristics of the included studies are presented in Tables 1–3.
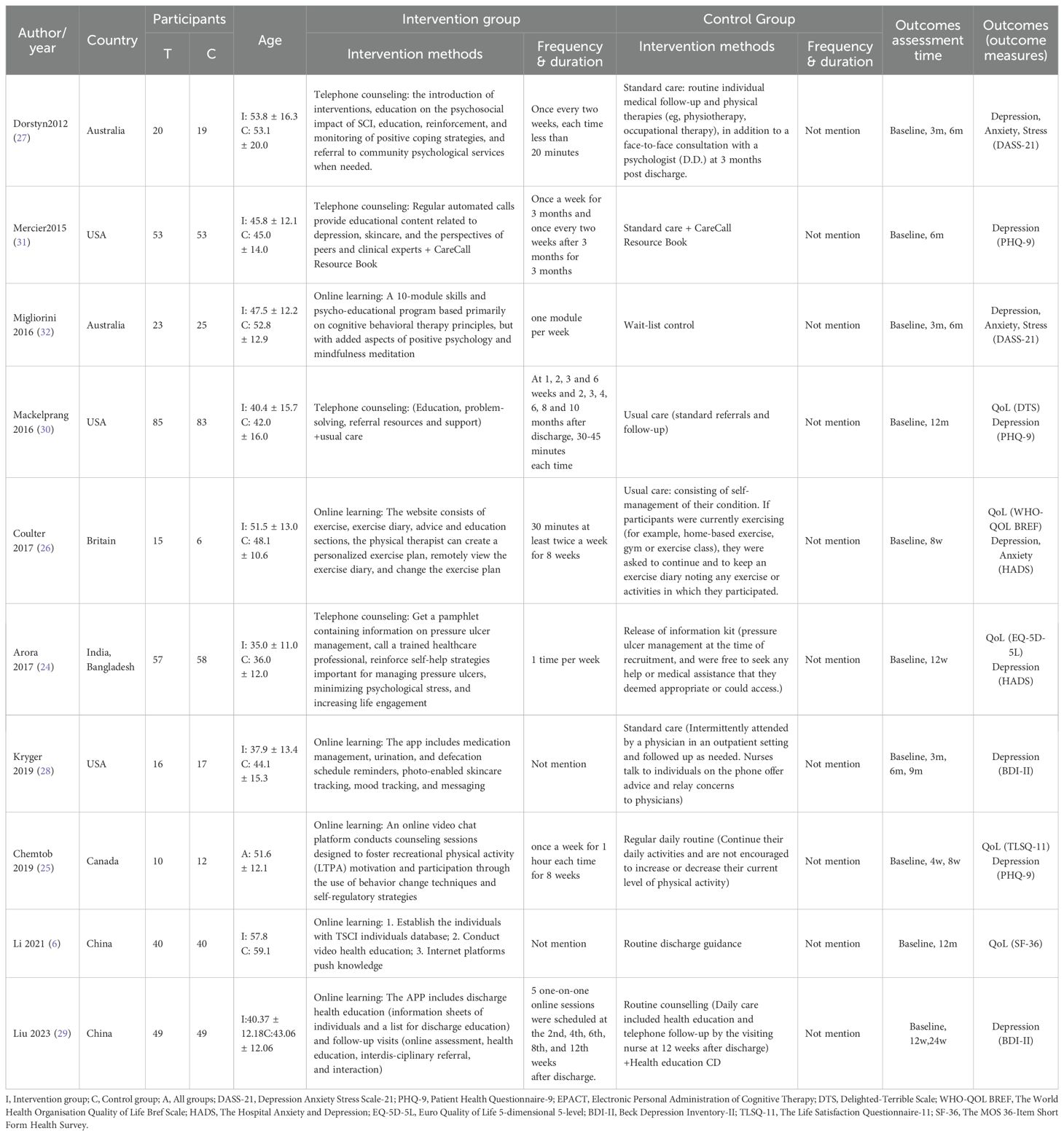
Table 1. Basic characteristics of the study.
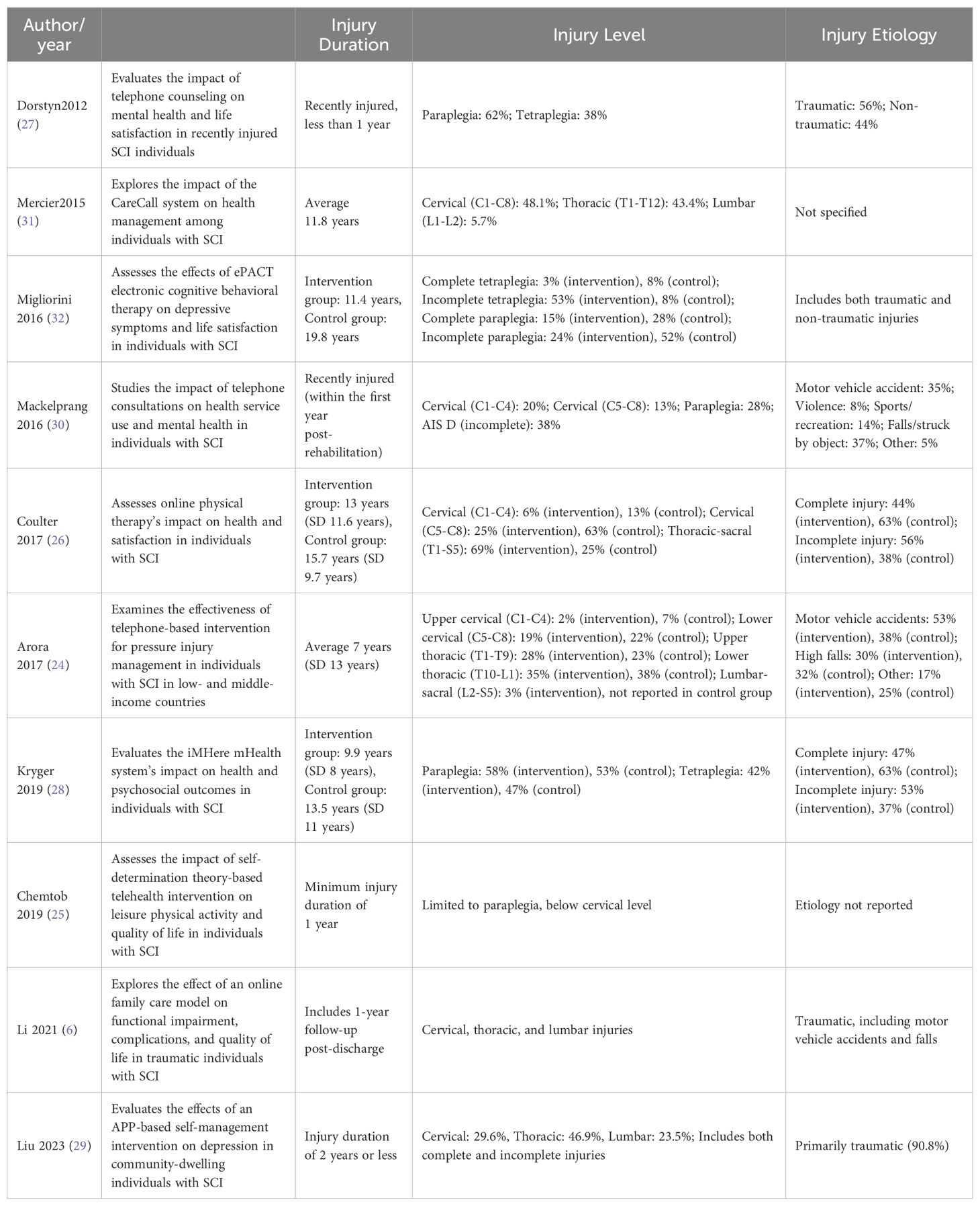
Table 2. Participant Characteristics and Study Focus in Telemedicine Interventions for SCI.
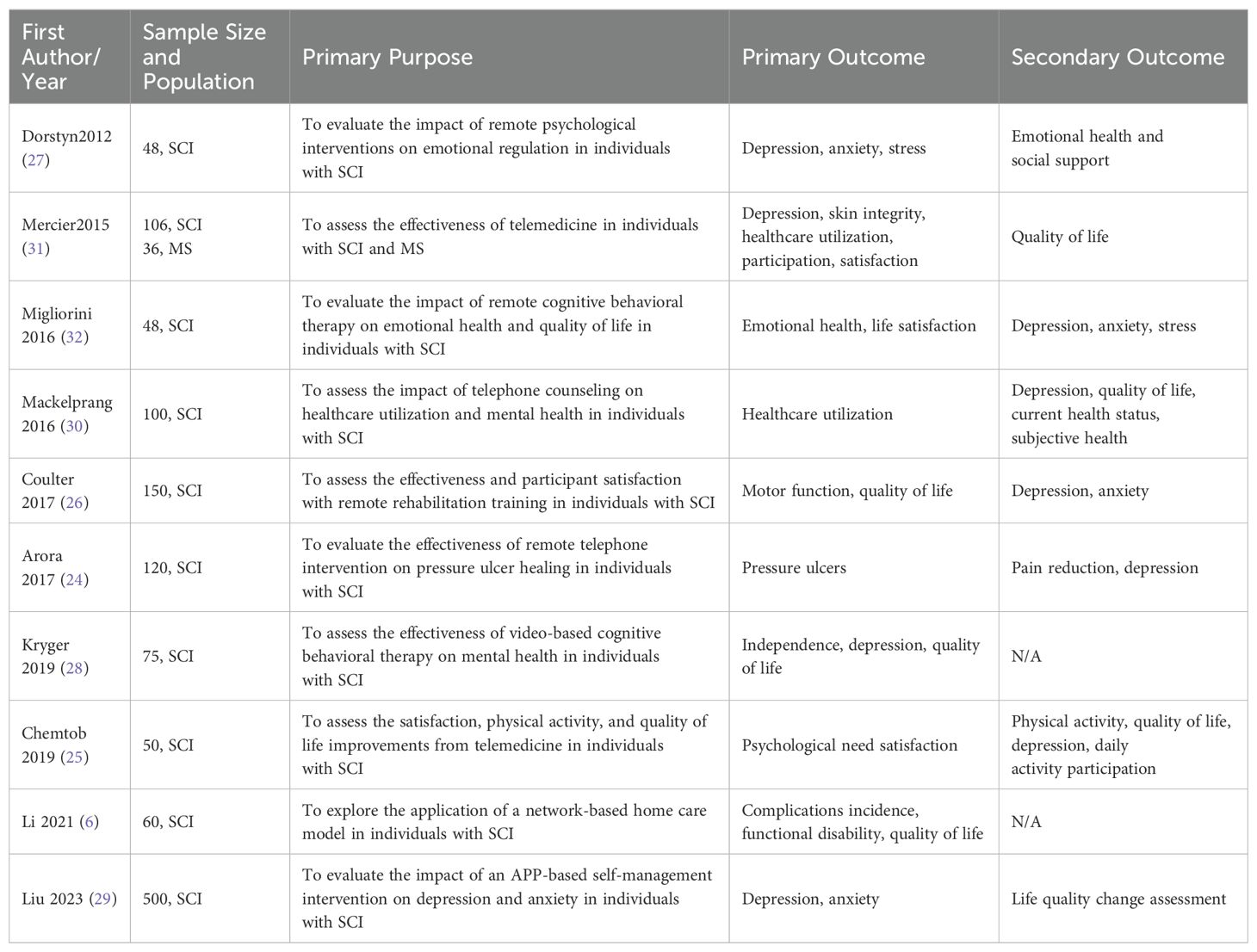
Table 3. Summary of Included Studies: Primary and Secondary Outcome Measures.
Five studies (6, 24–26, 30) reported on the impact of telemedicine on the quality of life (QoL) of individuals with SCI, with high heterogeneity observed among the studies (P<0.0001, I²=86%), likely due to the use of different scales to assess QoL in each study. Therefore, a random-effects model was applied for the analysis. The results indicated that telemedicine significantly improved the QoL for individuals with SCI compared to the control group [SMD=0.72, 95% CI (0.11, 1.32), P=0.02]. Subgroup analyses based on follow-up time and intervention method revealed that within 3 months, telemedicine interventions significantly improved the QoL for individuals with SCI compared to the control group [SMD=0.58, 95% CI (0.28, 0.89), P=0.0002], while no significant difference was observed at 12 months [SMD=0.88, 95% CI (-0.87, 2.64), P=0.32] (Figure 4). Telephone-based telemedicine showed no significant difference compared to the control group [SMD=0.28, 95% CI (-0.29, 0.84), P=0.34], whereas online learning-based telemedicine showed a significant improvement in QoL compared to the control group [SMD=0.72, 95% CI (0.11, 1.32), P=0.01] (Figure 5).
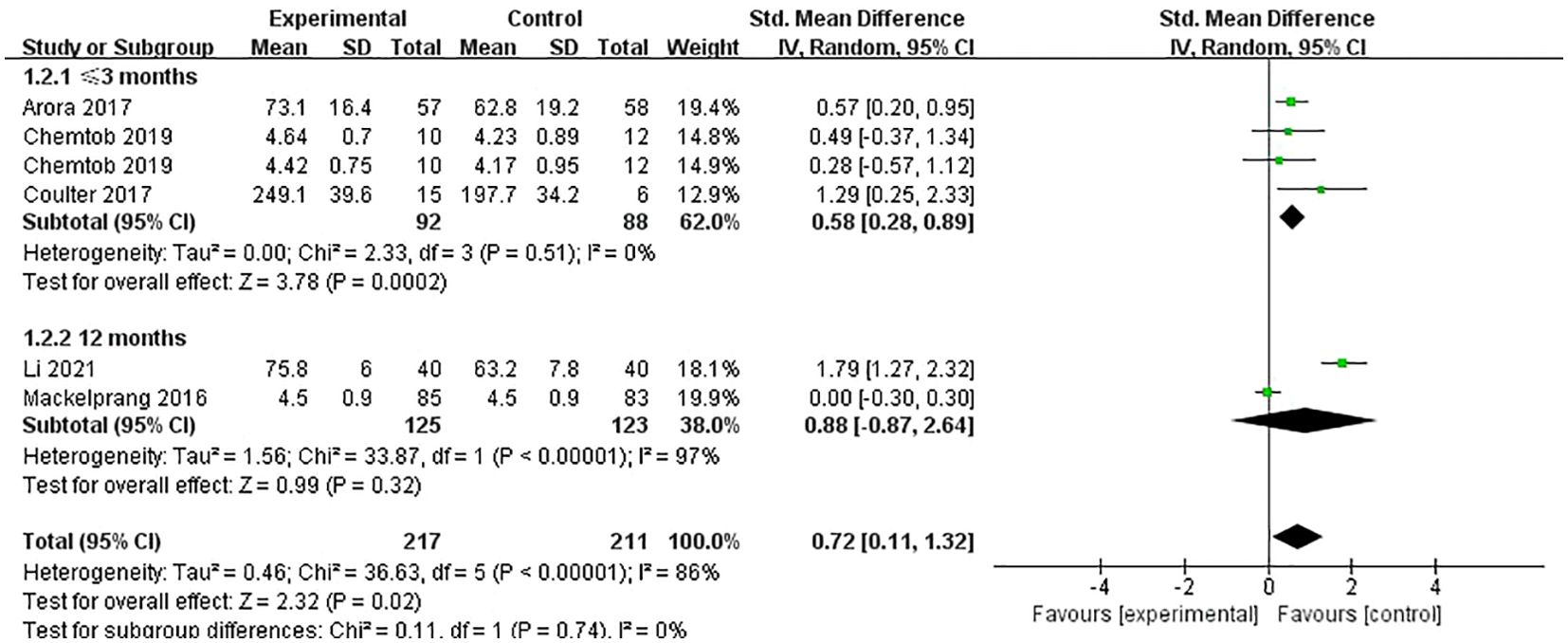
Figure 4. Forest plot: effect of different follow-up times on QoL.
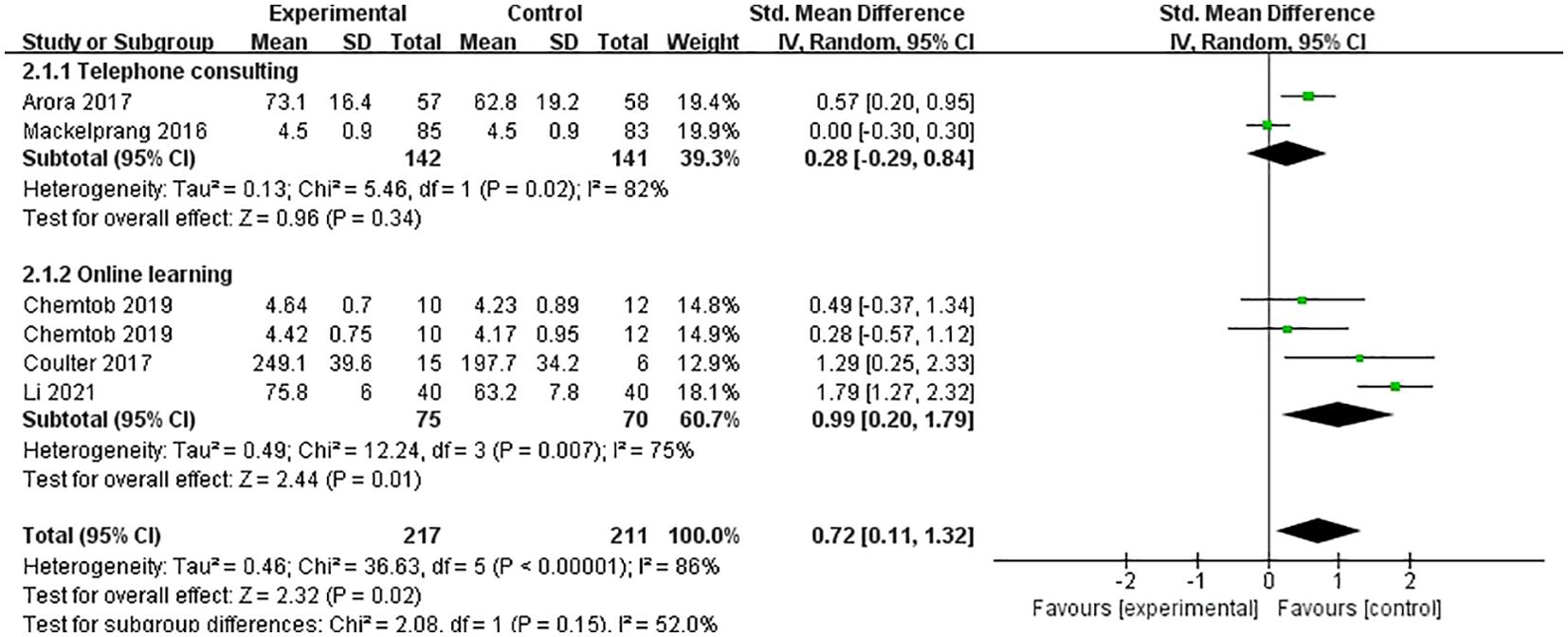
Figure 5. Forest plot: effect of different interventions on QoL.
Nine studies (24–32) reported on the impact of telemedicine on depression in individuals with SCI. The heterogeneity among these studies was low (P=0.08, I²=36%), so a fixed-effects model was used for the analysis. The results indicated that telemedicine significantly improved depression in individuals with SCI compared to the control group [SMD=-0.18, 95% CI (-0.31, -0.05), P=0.006]. Subgroup analyses based on follow-up time and intervention method showed that within 3 months, there was no significant difference in the improvement of depression between the telemedicine group and the control group [SMD=-0.36, 95% CI (-0.88, 0.15), P=0.17], and between 3-6 months, there was also no significant difference [SMD=-0.13, 95% CI (-0.35, 0.09), P=0.24]. However, at 6 months and beyond, there was a significant difference in the improvement of depression between the telemedicine group and the control group [SMD=-0.20, 95% CI (-0.37, -0.03), P=0.02] (Figure 6). For intervention methods, telephone-based telemedicine showed no significant difference compared to the control group [SMD=-0.15, 95% CI (-0.33, 0.04), P=0.12], whereas online learning-based telemedicine showed a significant improvement in depression compared to the control group [SMD=-0.22, 95% CI (-0.41, -0.04), P=0.02] (Figure 7).
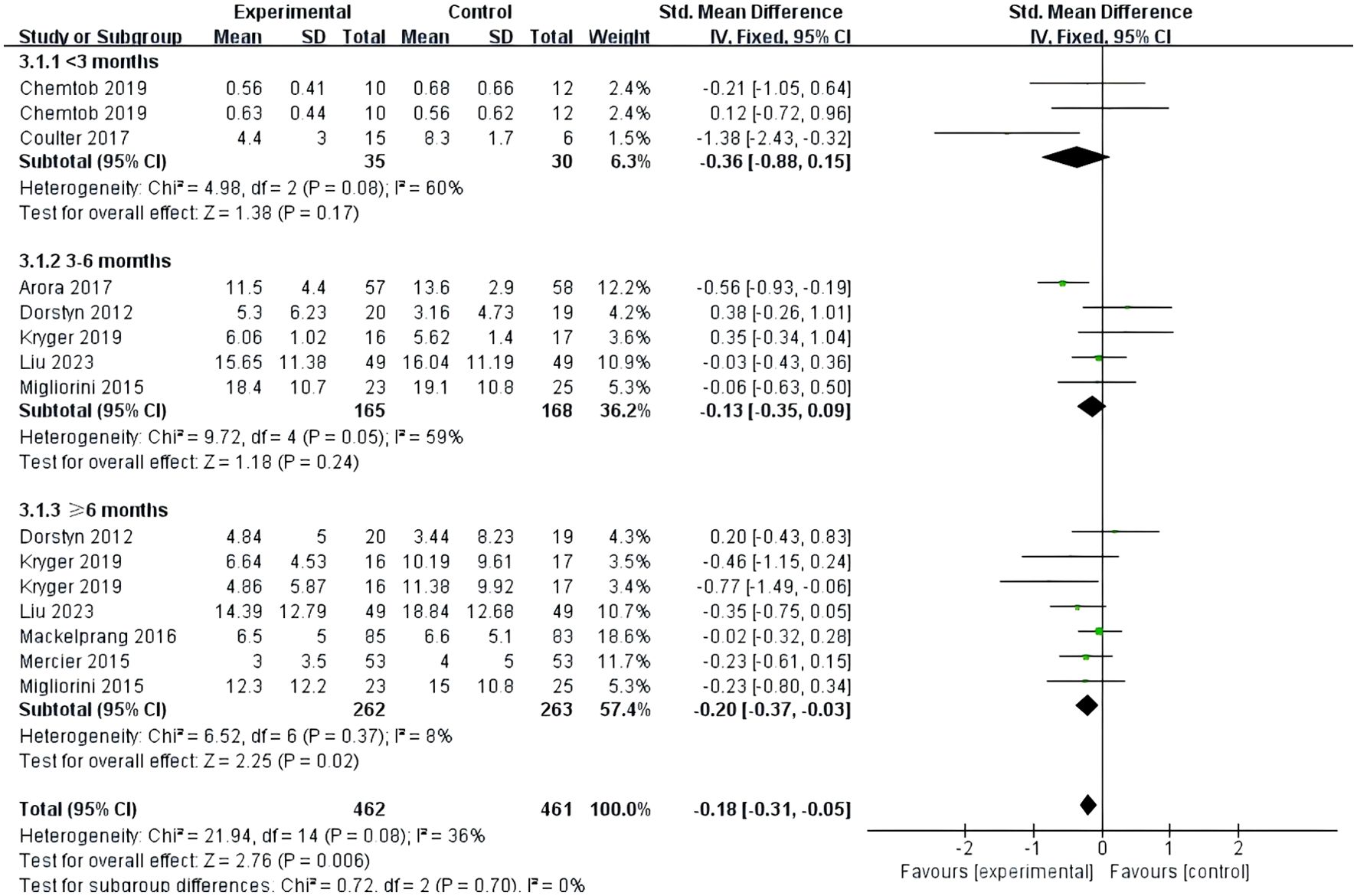
Figure 6. Forest plot: effect of different follow-up times on depression.
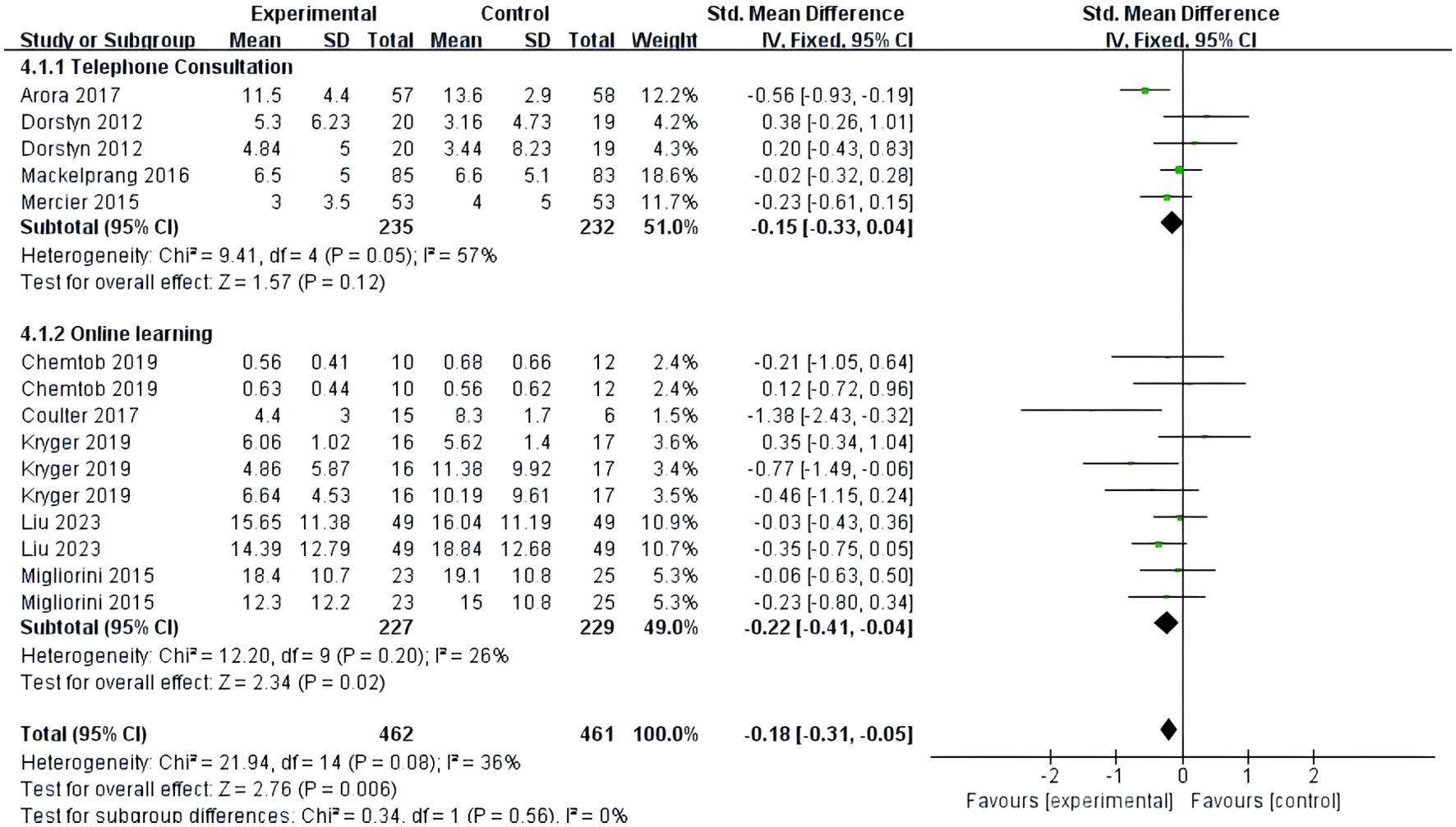
Figure 7. Forest map: effect of different interventions on depression.
Three studies (26, 27, 32) reported on the impact of telemedicine on anxiety in individuals with SCI. Among them, one study (26) used the HADS-A subscale of the HADS to assess anxiety, while the other two (27, 32) used the anxiety subscale of the DASS-21. The heterogeneity among these studies was high (P=0.04, I²=59%), so a random-effects model was used for the analysis. The results indicated that there was no significant difference in the improvement of anxiety between the telemedicine group and the control group [SMD=0.19, 95% CI (-0.27, 0.65), P=0.42]. Subgroup analysis based on follow-up time showed that within 3 months [SMD=0.04, 95% CI (-0.73, 0.82), P=0.91] and at 6 months [SMD=0.32, 95% CI (-0.39, 1.03), P=0.38], there were no significant differences in the improvement of anxiety between the telemedicine group and the control group (Figure 8).
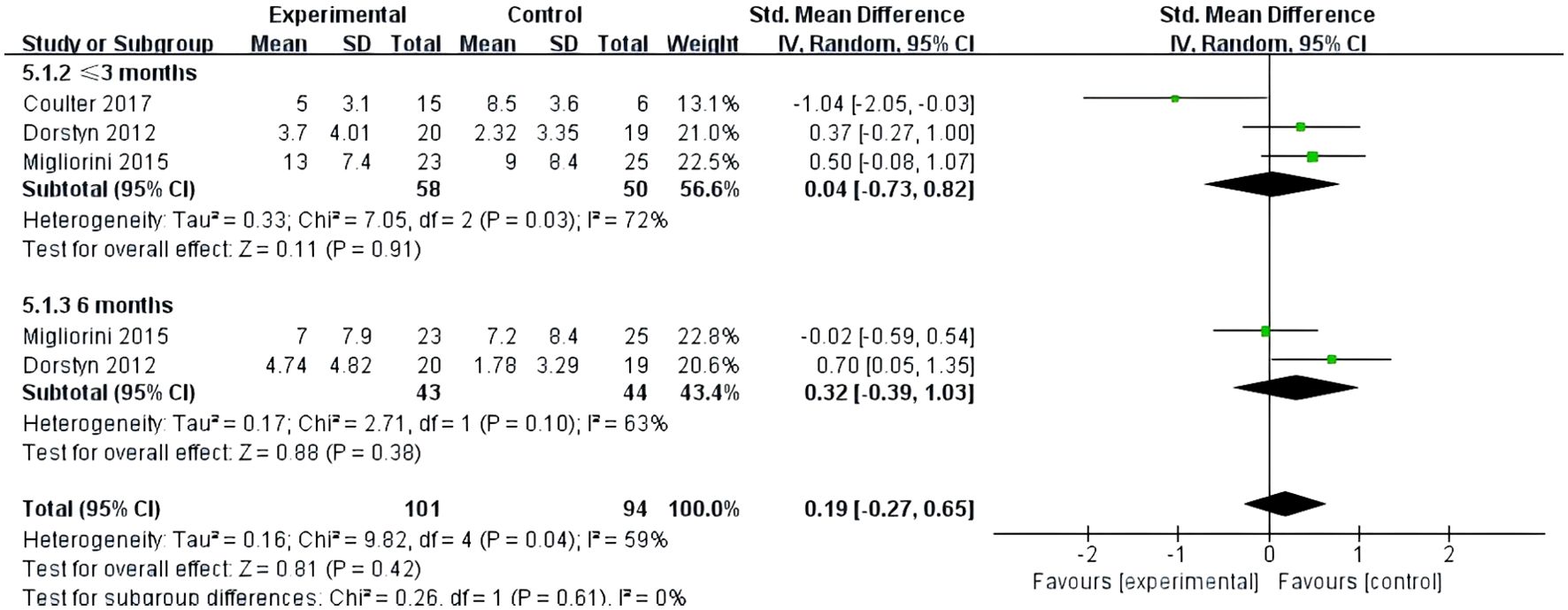
Figure 8. Forest plot: effect of different follow-up times on anxiety.
Two studies (27, 32) reported on the impact of telemedicine on stress in individuals with SCI. Both studies used the stress subscale of the DASS-21 for assessment. The heterogeneity among these studies was low (P=0.68, I²=0%), so a fixed-effects model was used for the analysis. The results indicated that there was no significant difference in the improvement of stress between the telemedicine group and the control group [SMD=0.17, 95% CI (-0.13, 0.47), P=0.27]. Subgroup analysis based on follow-up time showed that at 3 months [SMD=0.34, 95% CI (-0.08, 0.76), P=0.12] and at 6 months [SMD=0.00, 95% CI (-0.42, 0.42), P=0.99], there were no significant differences in the improvement of stress between the telemedicine group and the control group (Figure 9).
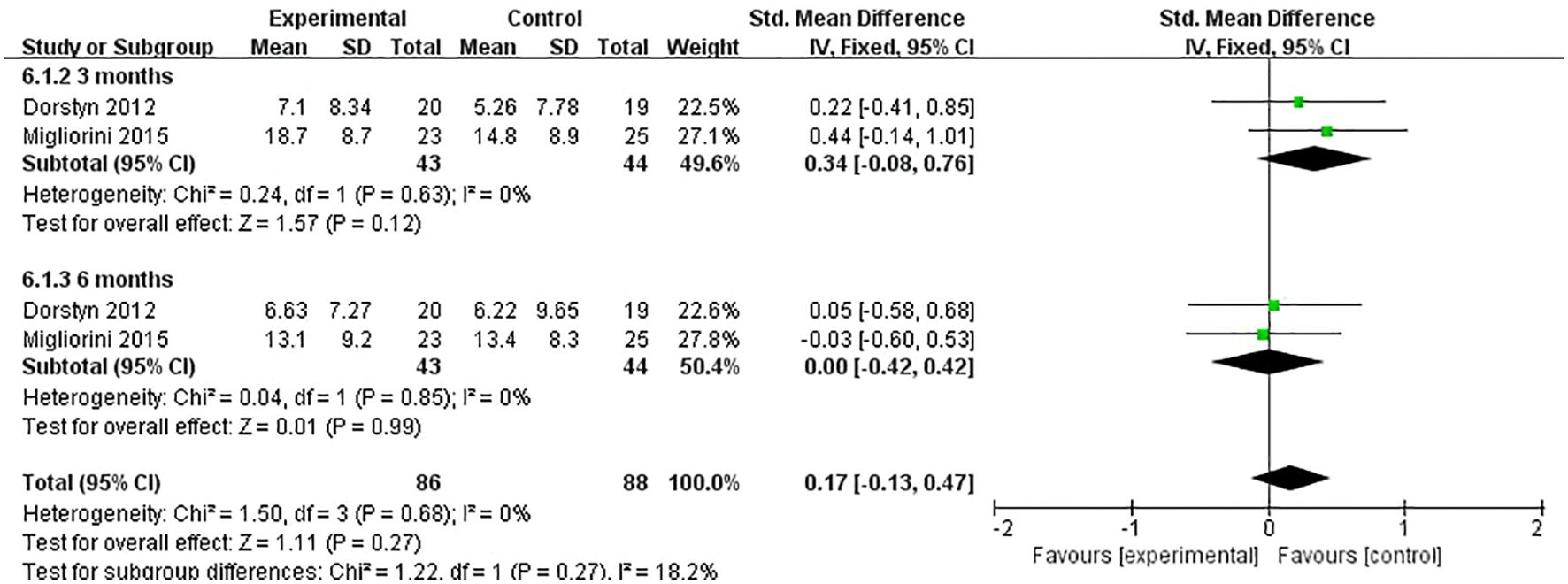
Figure 9. Forest plot: effect of different follow-up times on stress.
A sensitivity analysis was conducted by sequentially removing each of the 10 included studies (6, 24–32), and the results showed no significant changes, indicating that the findings of this study are relatively stable. Funnel plots were generated for the primary outcomes, QoL and depression in individuals with SCI. The results showed that the funnel plots were approximately symmetrically distributed, suggesting a low likelihood of publication bias among the included studies (Figures 10, 11).
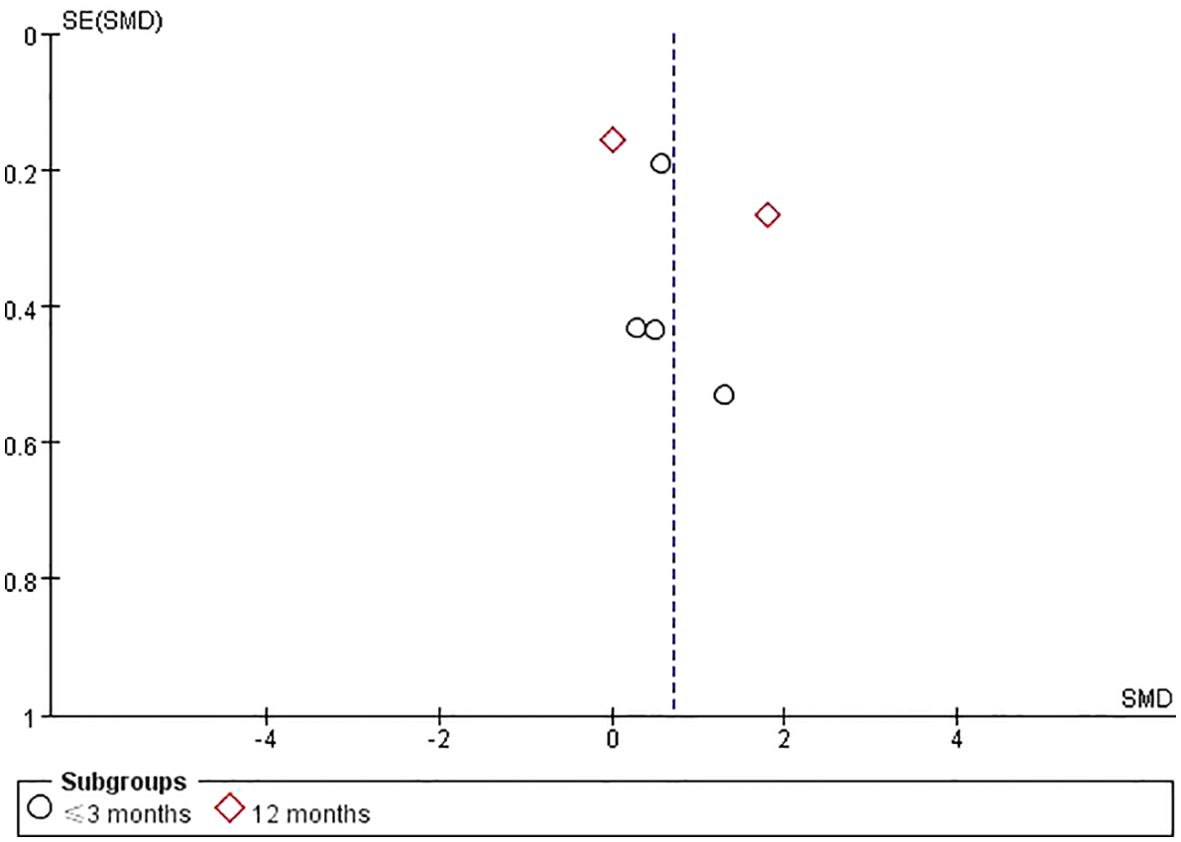
Figure 10. QoL funnel plot.
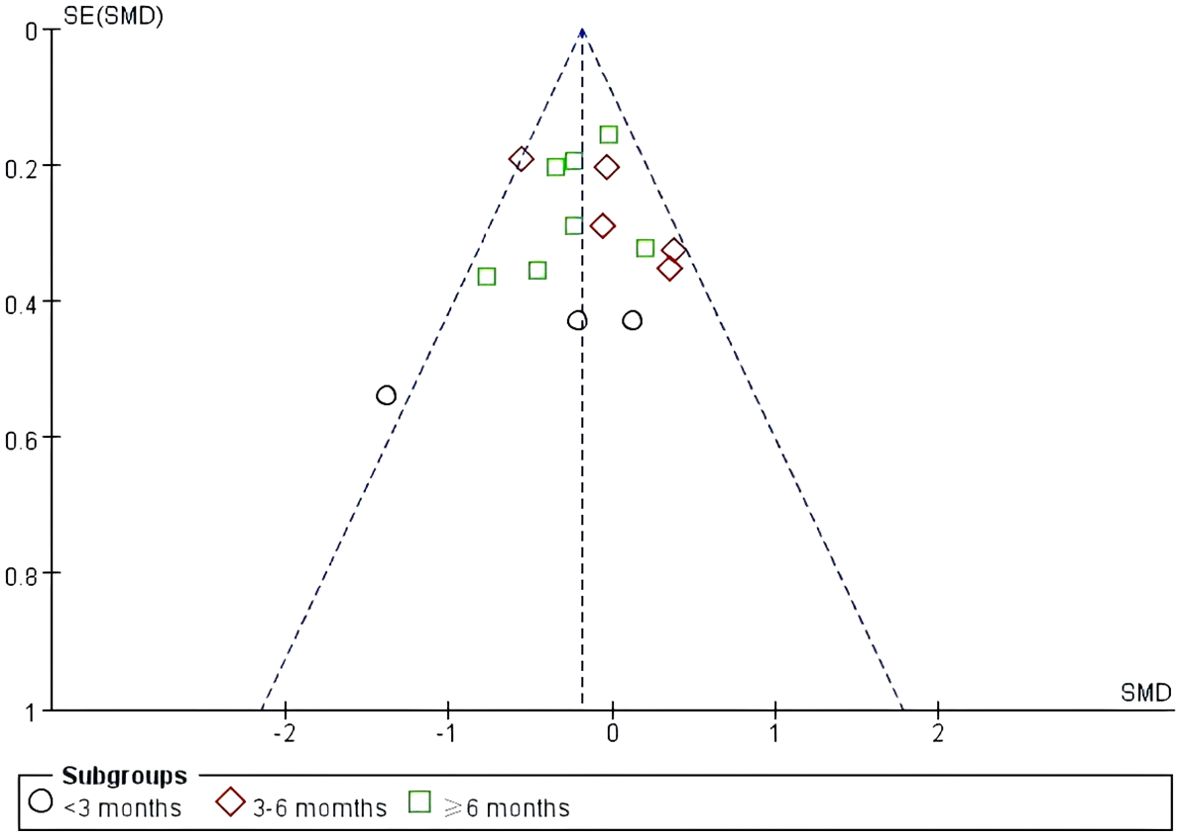
Figure 11. Depression funnel plot.
The results of this study indicate that telemedicine can significantly improve the QoL of individuals with SCI, with a statistically significant difference (P<0.05). Although healthcare institutions are the preferred sites for SCI treatment and rehabilitation, they require individuals to visit in person. Research has shown that the distance between healthcare facilities and individuals’ homes significantly affects the utilization of medical services (34). Telemedicine allows individuals to receive healthcare services at home, alleviating the inconveniences caused by transportation and time constraints, and providing real-time monitoring and rehabilitation services, which facilitate timely adjustments to treatment plans and improve rehabilitation outcomes (35). Additionally, in this systematic review, half of the studies (25, 26, 29, 32) involved individuals with SCI using web-based or app-based online learning. Telemedicine platforms typically offer health education and self-management resources, enabling individuals to learn how to better manage their condition under the guidance of their physicians, thereby enhancing their initiative and enthusiasm for rehabilitation (36). Individuals can also more easily access psychological support services (37), which is crucial for those with SCI who may face psychological stress and social barriers in addition to physical challenges. Overall, telemedicine provides more convenient, comprehensive, and personalized healthcare services for individuals with SCI, helping to improve their QoL and rehabilitation outcomes.
Subgroup analysis showed that within 3 months, telemedicine significantly improved the QoL of individuals with SCI compared to the control group. However, at 12 months, there was no significant difference in QoL between the groups. A possible reason for this discrepancy is that the novelty and convenience of telemedicine might initially motivate individuals with SCI who have not previously received such services to actively participate in the intervention, leading to better outcomes. Over time, however, psychological fatigue may set in, reducing adherence to the rehabilitation plan and diminishing the improvement in QoL. Furthermore, the included studies had a wide range of evaluation periods, lacking consistent data between 3 to 12 months, and only two studies provided data on QoL at 12 months. The small sample size and limited representativeness may affect the study’s results. Future research should include long-term follow-up studies to determine the long-term effects of telemedicine on the QoL of individuals with SCI.
According to a World Health Organization study (38), 2 to 3 out of every 10 individuals with SCI exhibit significant signs of depression. However, since depression and other psychological emotions are often considered common symptoms following SCI, they do not receive sufficient attention from medical personnel and family members (39). The results of this study showed that telemedicine has a significantly better effect on improving depression in individuals with SCI compared to standard care. However, subgroup analysis indicated that the improvement in depression scores was minimal for intervention durations of less than 6 months, with significant improvements observed only after 6 months of telemedicine intervention. People with SCI often face numerous life challenges, including physical limitations and social changes, which foster negative emotions. The development of depression can be influenced by various factors, including individual differences, social support, and the severity of the condition (40).While telemedicine provides convenience, the rehabilitation process for individuals with SCI is slow and challenging. Under these circumstances, the improvement of depressive symptoms may require long-term, continuous intervention. After receiving telemedicine services for six months, individuals with SCI showed significantly better improvement in depression compared to standard care. These findings align with a meta-analysis indicating that telemedicine interventions showed no significant improvement in depression symptoms in the early stages, but significant alleviation of symptoms was observed after 6 months of intervention (41). Additionally, A review (42) indicated that the effectiveness of telemedicine in improving depressive symptoms is nearly equivalent to that of traditional face-to-face therapy, making telemedicine a high-quality alternative for individuals with SCI. Considering these factors, the application of telemedicine in the treatment of depression among individuals with SCI holds substantial value and has significant potential for broader adoption. Over time, understanding the sustainability of treatment effects and potential intervention mechanisms will help provide a more comprehensive evaluation of telemedicine’s role in mental health.
Various telehealth interventions exhibit differing levels of effectiveness in improving QoL and reducing depression among individuals with SCI. Telephone counseling demonstrated limited effectiveness in enhancing QoL or alleviating depression, likely due to its lack of interactivity and real-time feedback. Mackelprang et al. (30) reported that, although telephone counseling offered psychological support and health advice, its lack of visual stimulation and personalized guidance diminished participant engagement and constrained its efficacy. In contrast, online learning and application-based personalized interventions yielded significantly greater benefits. Chemtob et al. (25) demonstrated that video-based learning on the REACTS platform significantly enhanced participants’ life satisfaction (Hedges’ g = 0.51) and engagement in health behaviors (Hedges’ g = 0.97). Similarly, Li et al. (6) developed an integrated internet platform combining video education, online consultations, and follow-ups, which significantly improved QoL and reduced depressive symptoms. The multimedia features of online platforms, including video education and interactive animations, facilitated intuitive and engaging knowledge transmission, thereby enhancing participants’ interest in learning and motivation for rehabilitation. Additionally, these platforms often incorporate real-time data tracking and feedback, enabling healthcare teams to dynamically tailor intervention strategies to participants’ rehabilitation progress. For instance, Coulter (26) and Liu (29) found that online platforms enabled participants to log exercise data, facilitating personalized guidance that significantly improved QoL and alleviated depressive symptoms. Compared to online platforms, telephone counseling exhibited limited effectiveness, although it provided some value in psychological support. Future research should investigate the integration of various telehealth modalities, including online learning, application-based support, and video monitoring, to effectively address the diverse needs of individuals with SCI and optimize rehabilitation outcomes.
The results of this study indicate that telemedicine did not significantly improve anxiety and stress in individuals with SCI. Depression, stress, and anxiety have distinct psychological mechanisms and characteristics. Depression is often associated with low mood, lack of interest, and negative emotions (43), whereas stress and anxiety are more related to stress responses and hyperarousal (44). Telemedicine interventions may be more suited to addressing symptoms of depression but may have limited effectiveness for the complex responses of stress and anxiety. Many telemedicine programs primarily focus on individuals education and psychological counseling, helping them adjust their mindset and resolve practical issues. This approach may more effectively address the core issues of depression but might lack sufficient, targeted strategies to cope with the physiological responses and emotional fluctuations associated with anxiety and stress. Moreover, the anxiety and stress experienced by individuals with SCI often stem from ongoing challenges in their daily lives, including loss of physical function, social isolation, and economic difficulties. Telemedicine alone may not effectively mitigate the impact of these triggers on individuals. Additionally, the limited number of studies included in the analysis that focused on anxiety and stress may have affected the ability to detect significant effects, contributing to the lack of observed improvements. Further research is needed to develop and evaluate more comprehensive and targeted interventions for managing anxiety and stress in individuals with SCI, potentially integrating telemedicine with other support systems to address the multifaceted nature of these emotional responses.
This meta-analysis has several limitations that should be considered. Although the 10 included studies assessed depression and QoL related outcomes, only 5 explicitly designated them as primary outcomes, with the remaining studies focusing on other indicators, such as functional improvement, physical health, or participant satisfaction. As a result, the findings may not fully reflect the potential impact of telemedicine on depression and QoL in individuals with SCI. Additionally, sample heterogeneity—including differences in participants’ demographic characteristics, injury severity, baseline health conditions, and control group care protocols—complicates the interpretation of pooled results and reduces the comparability of findings across studies. Furthermore, the geographical concentration of studies in North America, Europe, and Australia, combined with significant variations in follow-up durations, limits both the generalizability of findings and the understanding of telemedicine’s long-term effects. Some studies conducted only short-term assessments, potentially overlooking the sustained impact of interventions, especially in resource-limited regions.
To address these biases and improve the generalizability of findings, future research should focus on refining study designs. Efforts to recruit larger and more diverse samples, including individuals from a variety of demographic backgrounds, cultural contexts, and injury severities, would improve the representativeness of findings. Standardizing care protocols for control groups across studies would minimize variability and enhance the comparability of results. Additionally, extending follow-up durations, collecting interim data at regular intervals, and employing advanced analytical techniques, such as stratified analysis or meta-regression, would enable a more systematic exploration of the relationships between intervention effects and subgroup characteristics, thereby mitigating biases arising from heterogeneity. Finally, future studies should preregister protocols and ensure transparency in reporting all outcomes, including nonsignificant findings, to minimize the risk of selective reporting bias. Additionally, researchers could consider adopting the Registered Report format, which involves peer review of the study protocol before data collection begins. This extra layer of scrutiny can further reduce biases such as selective reporting and improve the overall quality of research (45). Both preregistration and Registered Reports contribute to enhancing the reliability of scientific findings, though they do so in different ways (46).
These improvements would enable future research to more comprehensively evaluate the therapeutic potential of telemedicine for individuals with SCI and provide stronger evidence of its impact on psychological health and overall QoL.
This study offers several significant strengths. Firstly, this meta-analysis focuses on individuals with SCI, a group that has been underexplored in telemedicine research. By systematically evaluating the impact of telemedicine on the quality of life and depression in people with SCI, this study addresses a critical gap in the literature. Secondly, the study adheres strictly to the Cochrane Handbook guidelines for assessing the quality of the included studies. Although the overall quality of the included studies was moderate, the rigorous methodological approach ensures the reliability and transparency of the findings. Thirdly, through subgroup analyses, this study provides key insights into the differential effects of telemedicine interventions across various time points and delivery methods, offering valuable guidance for optimizing strategies in future research and clinical practice.
Current evidence suggests that implementing telemedicine can improve the QoL and reduce depression in individuals with SCI to some extent. Future research should focus on long-term follow-up studies to evaluate the effectiveness of telemedicine interventions for spinal cord injury management at home. Additionally, combining various telemedicine approaches and designing more rigorous, large-scale randomized controlled trials will be crucial in providing stronger evidence to guide clinical practice.
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
YT: Conceptualization, Data curation, Formal Analysis, Methodology, Resources, Software, Validation, Writing – original draft. XL: Conceptualization, Writing – review & editing. WM: Methodology, Supervision, Writing – review & editing. HX: Formal Analysis, Software, Validation, Writing – original draft. YL: Resources, Supervision, Writing – review & editing. YW: Data curation, Resources, Writing – review & editing. EO: Data curation, Software, Writing – review & editing.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2025.1434376/full#supplementary-material
1. Lim S-W, Shiue Y-L, Ho C-H, Yu S-C, Kao P-H, Wang J-J, et al. Anxiety and depression in patients with traumatic spinal cord injury: a nationwide population-based cohort study. PloS One. (2017) 12:e0169623. doi: 10.1371/journal.pone.0169623
2. Montoto-Marqués A, Ferreiro-Velasco M, Salvador-De La Barrera S, Balboa-Barreiro V, Rodriguez-Sotillo A, Meijide-Faílde R. Epidemiology of traumatic spinal cord injury in Galicia, Spain: trends over a 20-year period. Spinal Cord. (2017) 55:588–94. doi: 10.1038/sc.2017.13
3. Niemi-Nikkola V, Koskinen E, Väärälä E, Kauppila A-M, Kallinen M, Vainionpää A. Incidence of acquired nontraumatic spinal cord injury in Finland: a 4-year prospective multicenter study. Arch Phys Med Rehabil. (2021) 102:44–9. doi: 10.1016/j.apmr.2020.08.015
4. Ko H-Y. Spinal Cord Injury in the Elderly and Aging of Spinal Cord Injuries. In: A Practical Guide to Care of Spinal Cord Injuries: Clinical Questions and Answers. Singapore: Springer (2023). p. 761–73.
5. Kim Y-H, Ha K-Y, Kim S-I. Spinal cord injury and related clinical trials. Clinics orthop surge. (2017) 9:1–9. doi: 10.4055/cios.2017.9.1.1
6. Li Q-P, Li J, Pan H-Y. Effects of online home nursing care model application on patients with traumatic spinal cord injury. Risk Manage Healthc Policy. (2021) 14: 1703–9. doi: 10.2147/RMHP.S301874
7. Dorstyn D, Mathias J, Denson L. Applications of telecounselling in spinal cord injury rehabilitation: a systematic review with effect sizes. Clin rehabil. (2013) 27:1072–83. doi: 10.1177/0269215513488001
8. Liu T, Xie S, Wang Y, Tang J, He X, Yan T, et al. Effects of app-based transitional care on the self-efficacy and quality of life of patients with spinal cord injury in China: randomized controlled trial. JMIR mHealth uHealth. (2021) 9:e22960. doi: 10.2196/22960
9. Chen J, Shen Y, Shao X, Wu W. An emerging role of inflammasomes in spinal cord injury and spinal cord tumor. Front Immunol. (2023) 14:1119591. doi: 10.3389/fimmu.2023.1119591
10. Yang C, Yang X. Early versus late surgical intervention for cervical spinal cord injury: A protocol for systematic review and meta-analysis. Medicine. (2023) 102:e33322. doi: 10.1097/MD.0000000000033322
11. Van Loo M, Post M, Bloemen J, Van Asbeck F. Care needs of persons with long-term spinal cord injury living at home in the Netherlands. Spinal Cord. (2010) 48:423–8. doi: 10.1038/sc.2009.142
12. Dallolio L, Menarini M, China S, Ventura M, Stainthorpe A, Soopramanien A, et al. Functional and clinical outcomes of telemedicine in patients with spinal cord injury. Arch Phys Med Rehabil. (2008) 89:2332–41. doi: 10.1002/central/CN-00667061/full
13. Russell TG. Telerehabilitation: a coming of age. Aust J Physiother. (2009) 55:5–6. doi: 10.1016/S0004-9514(09)70054-6
14. Sood S, Mbarika V, Jugoo S, Dookhy R, Doarn CR, Prakash N, et al. What is telemedicine? A collection of 104 peer-reviewed perspectives and theoretical underpinnings. Telemed e-Health. (2007) 13:573–90. doi: 10.1089/tmj.2006.0073
15. Kolcun JPG, Ryu WHA, Traynelis VC. Systematic review of telemedicine in spine surgery. J Neurosurg Spine. (2021) 34:161–70. doi: 10.3171/2020.6.SPINE20863
16. Niknamian S. Systematic review on tele-wound-care in spinal cord injury (SCI) patients and the impact of telemedicine in decreasing the cost. Phys Med Rehabil Res. (2019) 4:1–6. doi: 10.15761/PMRR.1000199
17. Sechrist S, Lavoie S, Khong CM, Dirlikov B, Shem K. Telemedicine using an iPad in the spinal cord injury population: a utility and patient satisfaction study. Spinal Cord Ser Cases. (2018) 4:71. doi: 10.1038/s41394-018-0105-4
18. Yuen J, Thiyagarajan CA, Belci M. Patient experience survey in telemedicine for spinal cord injury patients. Spinal Cord. (2015) 53:320–3. doi: 10.1038/sc.2014.247
19. Chen G, Wang T, Zhong L, He X, Huang C, Wang Y, et al. Telemedicine for preventing and treating pressure injury after spinal cord injury: systematic review and meta-analysis. J Med Internet Res. (2022) 24:e37618. doi: 10.2196/37618
20. Irgens I, Rekand T, Arora M, Liu N, Marshall R, Biering-Sørensen F, et al. Telehealth for people with spinal cord injury: a narrative review. Spinal Cord. (2018) 56:643–55. doi: 10.1038/s41393-017-0033-3
21. Mirbaha S, Morgan A, Tang A, Smith-Turchyn J, Richardson J. Models of telehealth service delivery in adults with spinal cord injuries: Scoping review. JMIR Rehabil Assist Technol. (2023) 10:e41186. doi: 10.2196/41186
22. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Bmj. (2021) 372:n71. doi: 10.1136/bmj.n71
23. Cumpston M, Li T, Page MJ, Chandler J, Welch VA, Higgins JP, et al. Updated guidance for trusted systematic reviews: a new edition of the Cochrane Handbook for Systematic Reviews of Interventions. Cochrane Database system Rev. (2019) 2019: ED000142. doi: 10.1002/14651858.ED000142
24. Arora M, Harvey L, Glinsky J, Chhabra H, Hossain S, Arumugam N, et al. Telephone-based management of pressure ulcers in people with spinal cord injury in low-and middle-income countries: a randomised controlled trial. Spinal Cord. (2017) 55:141–7. doi: 10.1038/sc.2016.163
25. Chemtob K, Rocchi M, Arbour-Nicitopoulos K, Kairy D, Fillion B, Sweet S. Using tele-health to enhance motivation, leisure time physical activity, and quality of life in adults with spinal cord injury: A self-determination theory-based pilot randomized control trial. Psychol Sport Exercise. (2019) 43:243–52. doi: 10.1016/j.psychsport.2019.03.008
26. Coulter EH, McLean AN, Hasler JP, Allan DB, McFadyen A, Paul L. The effectiveness and satisfaction of web-based physiotherapy in people with spinal cord injury: a pilot randomised controlled trial. Spinal Cord. (2017) 55:383–9. doi: 10.1038/sc.2016.125
27. Dorstyn D, Mathias J, Denson L, Robertson M. Effectiveness of telephone counseling in managing psychological outcomes after spinal cord injury: A preliminary study. Arch Phys Med Rehabil. (2012) 93:2100–8. doi: 10.1016/j.apmr.2012.06.002
28. Kryger MA, Crytzer TM, Fairman A, Quinby EJ, Karavolis M, Pramana G, et al. The effect of the interactive mobile health and rehabilitation system on health and psychosocial outcomes in spinal cord injury: randomized controlled trial. J Med Internet Res. (2019) 21:e14305. doi: 10.2196/14305
29. Liu Y, Hasimu M, Jia M, Tang J, Wang Y, He X, et al. The effects of app-based intervention for depression among community-dwelling individuals with spinal cord injury: a randomized controlled trial. Arch Phys Med Rehabil. (2023) 104:195–202. doi: 10.1016/j.apmr.2022.10.005
30. Mackelprang JL, Hoffman JM, Garbaccio C, Bombardier CH. Outcomes and lessons learned from a randomized controlled trial to reduce health care utilization during the first year after spinal cord injury rehabilitation: telephone counseling versus usual care. Arch Phys Med rehabil. (2016) 97:1793–6. e1. doi: 10.1016/j.apmr.2016.03.002
31. Mercier HW, Ni P, Houlihan BV, Jette AM. Differential impact and use of a telehealth intervention by persons with MS or SCI. Am J Phys Med rehabil. (2015) 94:987–99. doi: 10.1097/PHM.0000000000000291
32. Migliorini C, Sinclair A, Brown D, Tonge B, New P. A randomised control trial of an Internet-based cognitive behaviour treatment for mood disorder in adults with chronic spinal cord injury. Spinal Cord. (2016) 54:695–701. doi: 10.1038/sc.2015.221
33. Higgins JP, Altman DG, Gøtzsche PC, Jüni P, Moher D, Oxman AD, et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. Bmj. (2011) 343:d5928. doi: 10.1136/bmj.d5928
34. LaVela SL, Smith B, Weaver FM, Miskevics SA. Geographical proximity and health care utilization in veterans with SCI&D in the USA. Soc Sci Med. (2004) 59:2387–99. doi: 10.1016/j.socscimed.2004.06.033
35. Syed ST, Gerber BS, Sharp LK. Traveling towards disease: transportation barriers to health care access. J Community Health. (2013) 38:976–93. doi: 10.1007/s10900-013-9681-1
36. Deckwart O, Koehler K, Lezius S, Prescher S, Koehler F, Winkler S. Effects of remote patient management on self-care behaviour in heart failure patients: results from the randomized TIM-HF2 trial. Eur J Cardiovasc Nursing. (2023) 22:786–94. doi: 10.1093/eurjcn/zvad019
37. Klotz KA, Borlot F, Scantlebury MH, Payne ET, Appendino JP, Schönberger J, et al. Telehealth for children with epilepsy is effective and reduces anxiety independent of healthcare setting. Front pedia. (2021) 9:642381. doi: 10.3389/fped.2021.642381
38. Organization WH, Society ISC. International perspectives on spinal cord injury. Geneva, Switzerland: World Health Organization (2013).
39. Craig A, Nicholson Perry K, Guest R, Tran Y, Middleton J. Adjustment following chronic spinal cord injury: Determining factors that contribute to social participation. Br J Health Psychol. (2015) 20:807–23. doi: 10.1111/bjhp.2015.20.issue-4
40. Lee S-J, Kim M-G, Jh K, Min Y-S, Kim C-H, Kim K-T, et al. Factor analysis affecting degree of depression in family caregivers of patients with spinal cord injury: A cross-sectional pilot study. Int J Environ Res Public Health. (2022) 19:10878. doi: 10.3390/ijerph191710878
41. Wu M, Li C, Hu T, Zhao X, Qiao G, Gao X, et al. Effectiveness of telecare interventions on depression symptoms among older adults: systematic review and meta-analysis. JMIR Mhealth Uhealth. (2024) 12:e50787. doi: 10.2196/50787
42. Krzyzaniak N, Greenwood H, Scott AM, Peiris R, Cardona M, Clark J, et al. The effectiveness of telehealth versus face-to face interventions for anxiety disorders: A systematic review and meta-analysis. J Telemed Telecare. (2024) 30:250–61. doi: 10.1177/1357633X211053738
43. Chi L, Hung CL, Lin CY, Song TF, Chu CH, Chang YK, et al. The combined effects of obesity and cardiorespiratory fitness are associated with response inhibition: an ERP study. Int J Environ Res Public Health. (2021) 18:3429. doi: 10.3390/ijerph18073429
44. Sperduti M, Martinelli P, Piolino P. A neurocognitive model of meditation based on activation likelihood estimation (ALE) meta-analysis. Conscious cogn. (2012) 21:269–76. doi: 10.1016/j.concog.2011.09.019
45. Allen C, Mehler DMA. Open science challenges, benefits and tips in early career and beyond. PloS Biol. (2019) 17:e3000246. doi: 10.1371/journal.pbio.3000246
Keywords: telemedicine, telerehabilitation, spinal cord injuries, quality of life, depression, meta-analysis
Citation: Tan Y, Liang X, Ming W, Xing H, Liang Y, Wang Y and Onodu EO (2025) The efficacy of telemedicine interventions on quality of life and depression in individuals with spinal cord injury: a systematic review and meta-analysis. Front. Psychiatry 16:1434376. doi: 10.3389/fpsyt.2025.1434376
Received: 17 May 2024; Accepted: 07 January 2025;
Published: 23 January 2025.
Edited by:
David Ma Mehler, University Hospital RWTH Aachen, GermanyReviewed by:
Kazuko Shem, Santa Clara Valley Medical Center, United StatesCopyright © 2025 Tan, Liang, Ming, Xing, Liang, Wang and Onodu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yang Wang, d2FuZ3lhbmdsbWxAMTYzLmNvbQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.