
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychiatry , 05 February 2025
Sec. Psychopharmacology
Volume 15 - 2024 | https://doi.org/10.3389/fpsyt.2024.1506142
This article is part of the Research Topic Women in Psychiatry 2024: Psychopharmacology View all 5 articles
 Fernando Mora1,2
Fernando Mora1,2 Carlos Gómez Sánchez-Lafuente3Mariano De Iceta4,5,6Carolina Roset7Antonio Cárdenas8Daniel Pérez8
Carlos Gómez Sánchez-Lafuente3Mariano De Iceta4,5,6Carolina Roset7Antonio Cárdenas8Daniel Pérez8 Elena Álvarez-Barón9
Elena Álvarez-Barón9 Irene Gabarda-Inat9* and Savana Research Group
Irene Gabarda-Inat9* and Savana Research GroupIntroduction: Lurasidone is used for schizophrenia and bipolar depression in many countries, yet there is a lack of existing literature about its use, efficacy, and safety in real life. We aimed to characterize lurasidone-treated patients by analyzing unstructured information in electronic health records (EHRs).
Methods: This was a multicenter, retrospective, observational, and descriptive study that used data extracted from EHRs of patients initiating treatment with lurasidone in four Spanish hospitals from September 2019 to March 2022. Stratification included primary diagnosis, antipsychotic therapy, and lurasidone dose. Natural language processing and machine learning were used to extract and analyze unstructured clinical data using SNOMED CT terminology. Sociodemographic, clinical, and treatment characteristics, as well as symptoms and potential adverse events as efficacy and safety outcomes, were evaluated at inclusion and during follow-up.
Results: Among 2,374,218 patients attending the participating hospitals during the study period with 66,523,391 EHRs, 272 initiated lurasidone and were included. Median (Q1; Q3) age was 46 (37; 56) years, and 60.3% were female. Common comorbidities were hypertension (46.7%), dyslipidemia (44.5%), and diabetes (30.5%), and 87.1% had received a median of three antipsychotics before lurasidone, being olanzapine (52.9%) and quetiapine (45.2%) the most frequently used. During follow-up, 16.9% of the patients discontinued lurasidone, and few patients (<1.2%) reached high doses (111 and 148 mg/day). Lurasidone demonstrated effectiveness in reducing positive and negative symptoms, anxiety, depression, and suicidal ideation, with a marked reduction in most of the adverse events compared to the pre-lurasidone period.
Discussion: Lurasidone reduced positive and negative symptoms frequencies with a favorable safety profile, while low discontinuation rates suggest efficacy-tolerability balance, patient satisfaction, and acceptability. Our data reflect that in Spain lurasidone is used at low doses, limiting its beneficial effects according to clinical trials results.
Antipsychotics are often a first-line treatment for psychiatric disorders such as schizophrenia and bipolar depression (1). The use of second-generation, or atypical, antipsychotics has gained popularity, and their efficacy and safety appear to rival or surpass first-generation antipsychotics (2). Lurasidone is a second-generation oral antipsychotic that was approved by the U.S. Food and Drug Administration (FDA) in 2010 and 2013 for schizophrenia and acute bipolar depression in adults, respectively, either as monotherapy or in combination (3). It was later approved by the European Medicines Agency (EMA) for schizophrenia treatment in adults in 2014 and for adolescents aged 13 to 17 in 2020 (4). Lurasidone has demonstrated safety and efficacy in short- and long-term studies for the treatment of schizophrenia (37-148 mg/day) and bipolar depression (18.5-111 mg/day), with minimal metabolic effects and low weight gain risk (5–7). Systematic reviews have extensively analyzed its efficacy, tolerability, safety, and place in therapy (8, 9). A few meta-analyses suggest that lurasidone has a similar efficacy profile to other antipsychotics, and it offers several advantages, including ease of practical use, early efficacy, and tolerability, particularly cardiometabolic (10, 11). Additionally, lurasidone has been shown to be more effective in treatment-naive patients (12, 13). Despite these studies, there is a lack of existing literature on the real-world use of lurasidone (14, 15).
Describing the patients receiving psychotropic therapies has been crucial as a first step toward understanding this patient population for future comparative studies (16–21), whether focusing on efficacy (22–24), safety (25, 26), or the relevance of monotherapy versus polytherapy (27). While clinical trials are critical for evidence generation, they have limitations in capturing real-world complexities due to controlled settings and participant numbers. Real-world data (RWD) studies, on the other hand, offer a more comprehensive and practical view of the outcomes of medical treatments. Although recent studies have reported RWD on the schizophrenia epidemiology in the Spanish population, they rely on structured data from the Minimum Basic Data Set (MBDS), or coding systems such as the International Classification of Diseases (ICD) or the Anatomical Therapeutic Chemical Classification System (ATC) (28). In this regard, unstructured free text from electronic health records (EHRs) provides richer clinical insights (29, 30). However, since lurasidone’s approval, its use in routine clinical practice has not been extensively documented, and there is a growing interest in how lurasidone might be combined with other antipsychotics in real practice (31). Therefore, it is essential to describe those patients taking lurasidone and the characteristics of its use in our country to enhance our understanding of this clinical population.
This study aimed to portray the clinical characteristics and medical management of patients treated- with lurasidone in Spain either as a stand-alone treatment or in conjunction with other antipsychotics, based on RWD and by analyzing readily available unstructured information recorded by healthcare professionals in patients’ EHRs. To this end, the study relied on using natural language processing (NLP) and machine learning (ML) techniques to extract, organize, and analyze this clinical information to better understand its use, efficacy, and safety in Spanish patients as a step to support clinicians in their decision making when prescribing antipsychotics.
This was a multicenter, observational, and descriptive study in which RWD captured in the EHRs of patients prospectively attended and treated with lurasidone in four Spanish hospitals from September 2019 to March 2022, were retrospectively collected (Figure 1). A cross-sectional analysis of all patients and variables was performed at the time of inclusion with a variable-dependent look-back window as described in the table footnotes. These time windows were intended to establish a reasonable time interval at which the occurrence of variables could be related to a specific time point. Analyses were also performed during the follow-up period (i.e., the time from inclusion to the last EHR available within the study period or from inclusion to the end of treatment with lurasidone). Sample size calculation as well as more details regarding data source, acquisition, integration and quality assessment are shown in the Supplementary Materials.
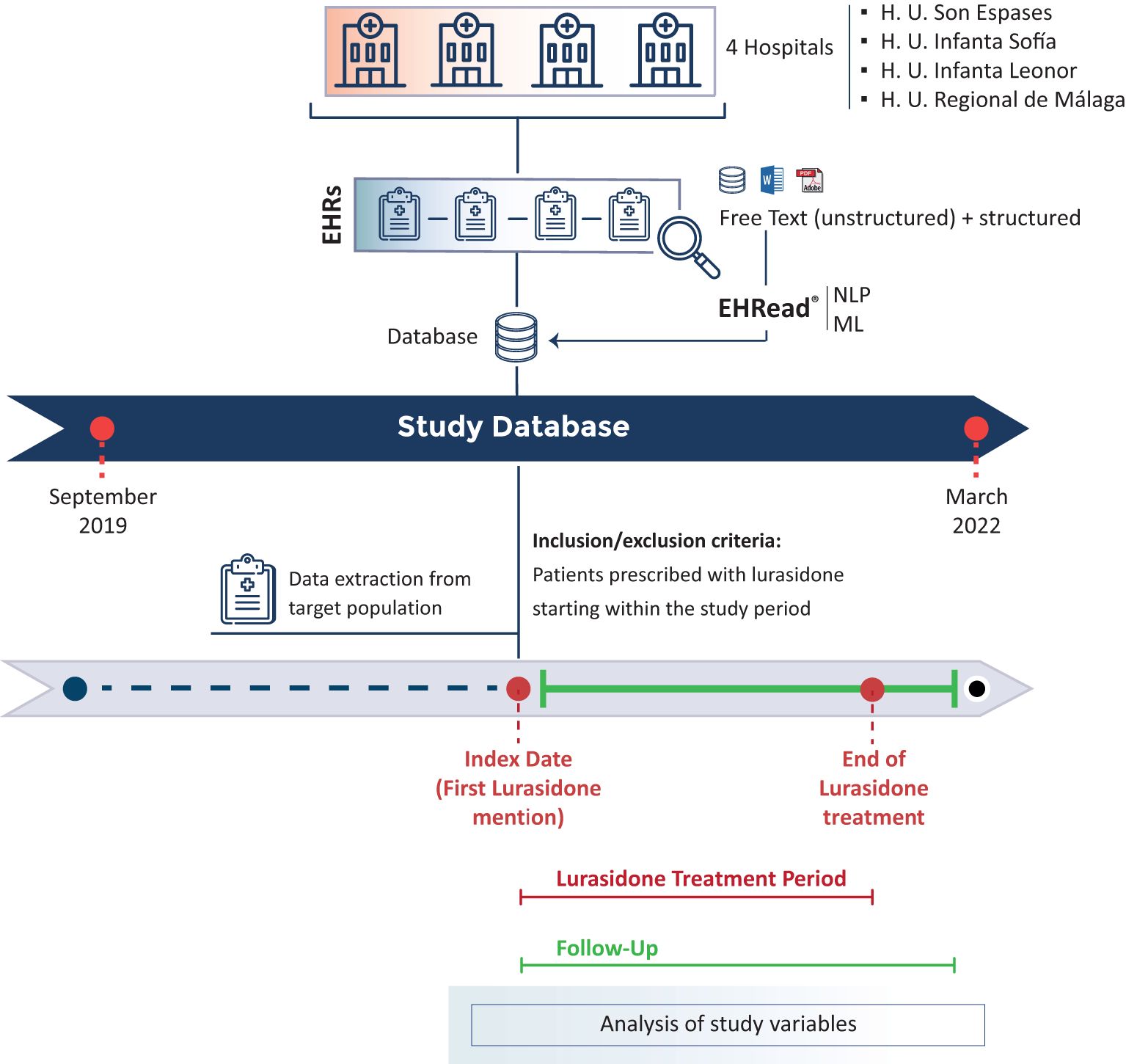
Figure 1. Study design. EHRead® technology by Savana is a system based on Natural Language Processing (NLP) that applies machine learning (ML) to extract, analyze, and interpret the free-text information written in millions of de-identified EHRs. The unstructured and structured free-text information from EHRs from multiple participating sites is organized in study databases. Specific inclusion and exclusion criteria are specified to define the target population. The variables extracted from the database at Index date (baseline), during the follow-up period, and throughout the Lurasidone Treatment Period are organized and analyzed to address multiple clinical questions.
The study population included all patients attending the participating hospitals who initiated lurasidone treatment during the study period according to unstructured (and structured, if available) information in the EHRs. To avoid the inclusion of false positive or non-informative patients, to be considered part of the study population, two independent mentions of lurasidone had to be identified in different EHRs, and at least one of them had to be from the psychiatry department.
There were no exclusion criteria. Included patients were further stratified into different subgroups concerning primary diagnosis (i.e., schizophrenia, schizoaffective disorder, bipolar disorder, psychotic episode, depression, or not specified), maximum dose of lurasidone (18.5 mg, 37 mg, 74 mg, 111 mg, 148 mg or not specified) and type of antipsychotic therapy (lurasidone monotherapy or polytherapy).
Unstructured clinical data were extracted from all available departments (including inpatient, outpatient, and emergency departments) in all included patients at each participating site and analyzed using the EHRead® technology (Medsavana, Madrid, Spain) according to previously described methods (32). Briefly, the free text information from EHRs was extracted and organized using the SNOMED CT terminology. This data-driven methodology relies on NLP and ML to generate a synthetic database containing any detection of medical concepts and associated metadata (33, 34). We evaluated the performance of EHRead® as previously described (35). Details regarding EHRead® data extraction, model development and specific metrics obtained after the external validation are in Supplementary Materials and Supplementary Table 1.
Variable categories included sociodemographic characteristics, toxic habits, comorbidities, clinical characteristics, diagnosis, lurasidone characteristics (timing, dosage, concomitant medication, relapses, etc), other antipsychotics and effectiveness (symptoms), and safety outcomes (potential treatmen-related adverse events). Because this study relied on RWD, the potential number of variables included in the analyses was limited by the free text information contained in the EHRs. See Supplementary Materials for further details.
Frequency tables were used for categorical variables, while continuous variables were described using summary tables which may include the mean, standard deviation (SD), median, and the lower and upper quartiles (Q1; Q3). The number of non-evaluable outcomes and missing data were also reported and not counted in the percentages. The Kaplan-Meier (KM) approach was used for time-to-event analyses. Missing data is detailed in the Supplementary Materials and was handled according to the nature of the data collection process and based on the type of variable (boolean, categorical or numerical) assuming that physicians reflect clinically relevant information in EHRs. Then, missing data imputation was applied to boolean variables, treating the absence of a term for a comorbidity/symptom/adverse event as if the patient did not have it. Data were analyzed and presented using “R” software (version 4.0.2).
This study was classified as a “non-interventional post-authorization study” by the Spanish Agency for Medicines and Health Products (AEMPS) and was reviewed and approved by the Institutional Review Board (IRB) of each participating hospital. It followed a predefined protocol and statistical analysis plan that was designed to ensure the scientific integrity of the research. All methods and analysis followed legal and regulatory requirements and generally accepted research practices as described in the latest edition of the Declaration of Helsinki, Good Pharmacoepidemiology Practices, and applicable local regulations. Informed consent was waived because data were retrospectively analyzed from patient EHRs, anonymized, and aggregated in an irreversibly dissociated manner. Data registry in EHRs was performed as part of routine clinical practice. Data was further included in the study for its secondary use in research and its assessment was blinded.
A total of 66,523,391 EHRs containing clinical data on 2,374,218 patients who attended the participating hospitals during the study period were processed. Of these patients, 272 started treatment with lurasidone and constituted the study population (Figure 2).
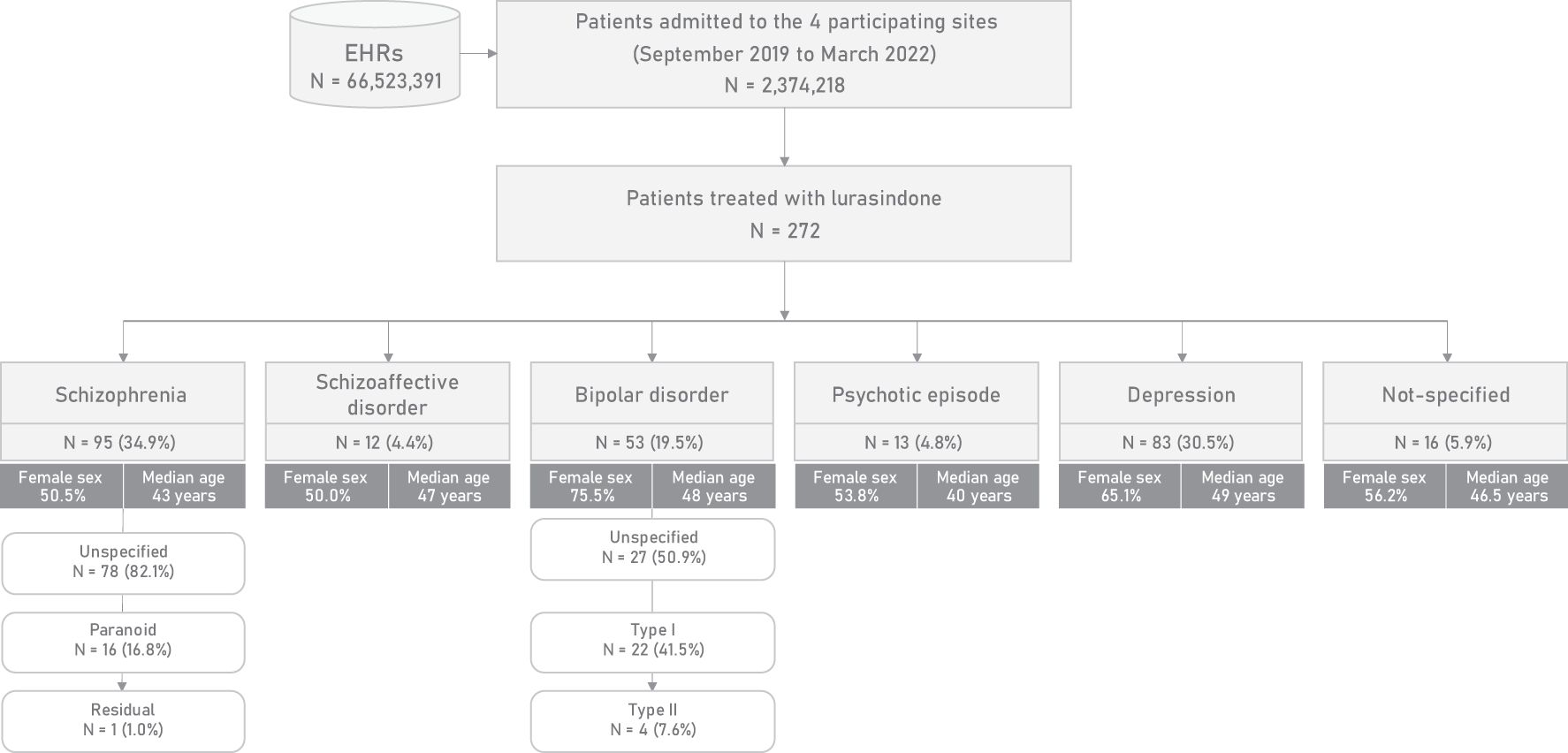
Figure 2. Flowchart of the study population and stratification by primary diagnosis.
Baseline demographic characteristics, toxic habits, comorbidities, and prior treatments of the study population are shown in Table 1. Overall, 60.3% of patients were female, resulting in a male-to-female ratio of 0.7. The median (Q1; Q3) age was 46 years (37, 56), with the majority of patients (87.9%) between the ages of 25 and 65 years. The proportion of patients with a family history of schizophrenia was 9.2%. Up to 48.9% of patients were current smokers and 39.0% were habitual drinkers. Regarding illicit drug use, cannabis, and cocaine were used by 23.2% and 20.2% respectively, while other substances such as ecstasy, methamphetamine, and heroin were much less common. Overall, the proportion of patients with toxic substance abuse was 43.8%. The most common comorbidities at baseline were hypertension (46.7%), dyslipidemia (44.5%), diabetes (30.5%), overweight (21.3%), obesity (23.9%), and stroke (14.3%). Up to 87.1% of patients in the study population had been treated with a median (Q1; Q3) of 3 antipsychotics (2, 4) other than lurasidone prior to the inclusion.
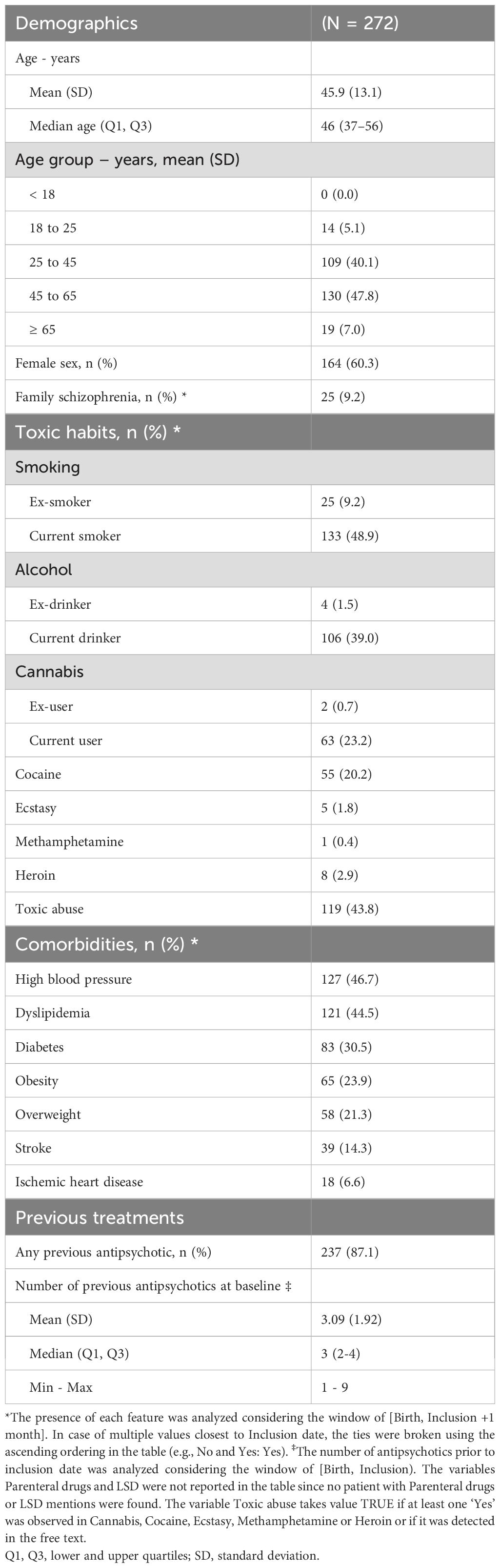
Table 1. Baseline demographics, toxic habits, comorbidities and previous treatments.
The median (Q1; Q3) time from diagnosis of a psychotic disorder to lurasidone treatment was 4.5 years (1.0; 9.7) and patients in our population were treated with the drug for a median (Q1; Q3) of 9.0 months (4.0; 14.0). The baseline and maximum doses of lurasidone achieved during the study period are shown in Figure 3. Before the inclusion, second-generation therapies were used much more frequently than first-generation therapies. The most common was olanzapine (52.9%), followed by quetiapine (45.2%) and aripiprazole (40.8%). Among first-generation antipsychotics, haloperidol was the most commonly prescribed (20.2%). Overall, the percentage of patients receiving antipsychotic combinations during follow-up decreased by about 31% compared with the corresponding percentage before the inclusion (87.1% and 60.3%, respectively). As a concomitant treatment, haloperidol remained the most commonly used first-generation antipsychotic (11.0%), and, among second-generation therapies, olanzapine was again the most commonly used (32.4%), followed by aripiprazole (27.2%) and quetiapine (23.5%) (Supplementary Table 2).
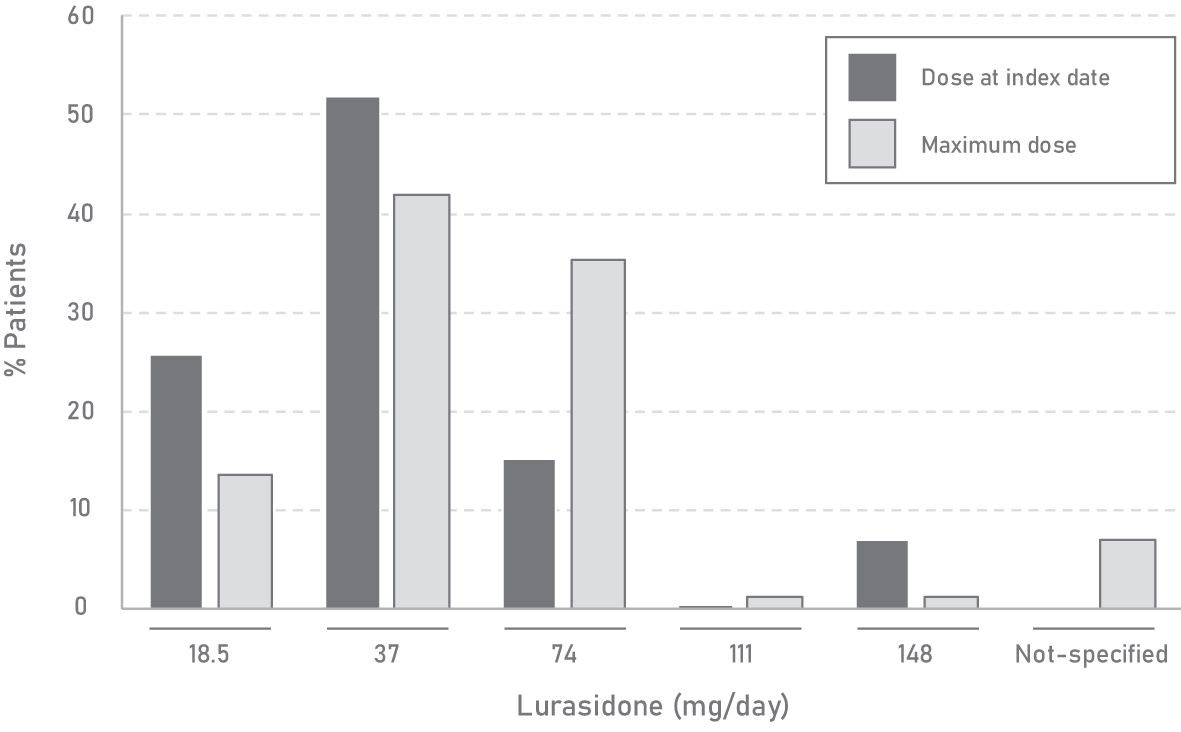
Figure 3. Characteristics of lurasidone doses during lurasidone treatment.
The percentage of patients with at least one relapse in the year before the inclusion was 17.6% in the monotherapy group and 16.5% in the polytherapy group. The corresponding percentages during the lurasidone treatment period were 9.3% and 26.2%, respectively.
Regarding treatment adherence, 16.9% of patients discontinued lurasidone treatment during follow-up. Almost half of the patients (43.5%) who discontinued lurasidone treatment were receiving a dose of 37 mg/day at the time of discontinuation, while 21.7% and 17.4% were receiving 74 mg/day and 18.5 mg/day, respectively, and 17.4% did not have a lurasidone dose specified when discontinuation occurred. In terms of primary diagnosis, 43.5% of patients who discontinued lurasidone had schizophrenia, 28.3% had depression, 19.6% had bipolar disorder, 4.3% had schizoaffective disorder and 4.3% had a not-specified diagnosis. Drug discontinuation rate was lower in patients treated with monotherapy than in those treated with polytherapy (41.3% vs. 58.7%). The median drug retention time for lurasidone was not reached during follow-up. The drug retention rate at 30 months was 65.5% (Supplementary Figure 1).
Lurasidone treatment markedly reduced the frequency of positive symptoms (‒21.8%) and negative symptoms (‒30.1%). However, for catatonia and echolalia, the number of patients at baseline and during follow-up was too small to assess this reduction. Lurasidone treatment also achieved important reductions in anxiety (‒35.1%), depression (‒60.3%), and suicidal ideation (‒25.0%) frequencies. When stratified by primary diagnosis, lurasidone treatment produced a comparable pattern of reductions in signs and symptoms in patients with schizophrenia (Figure 4A; Supplementary Table 3).
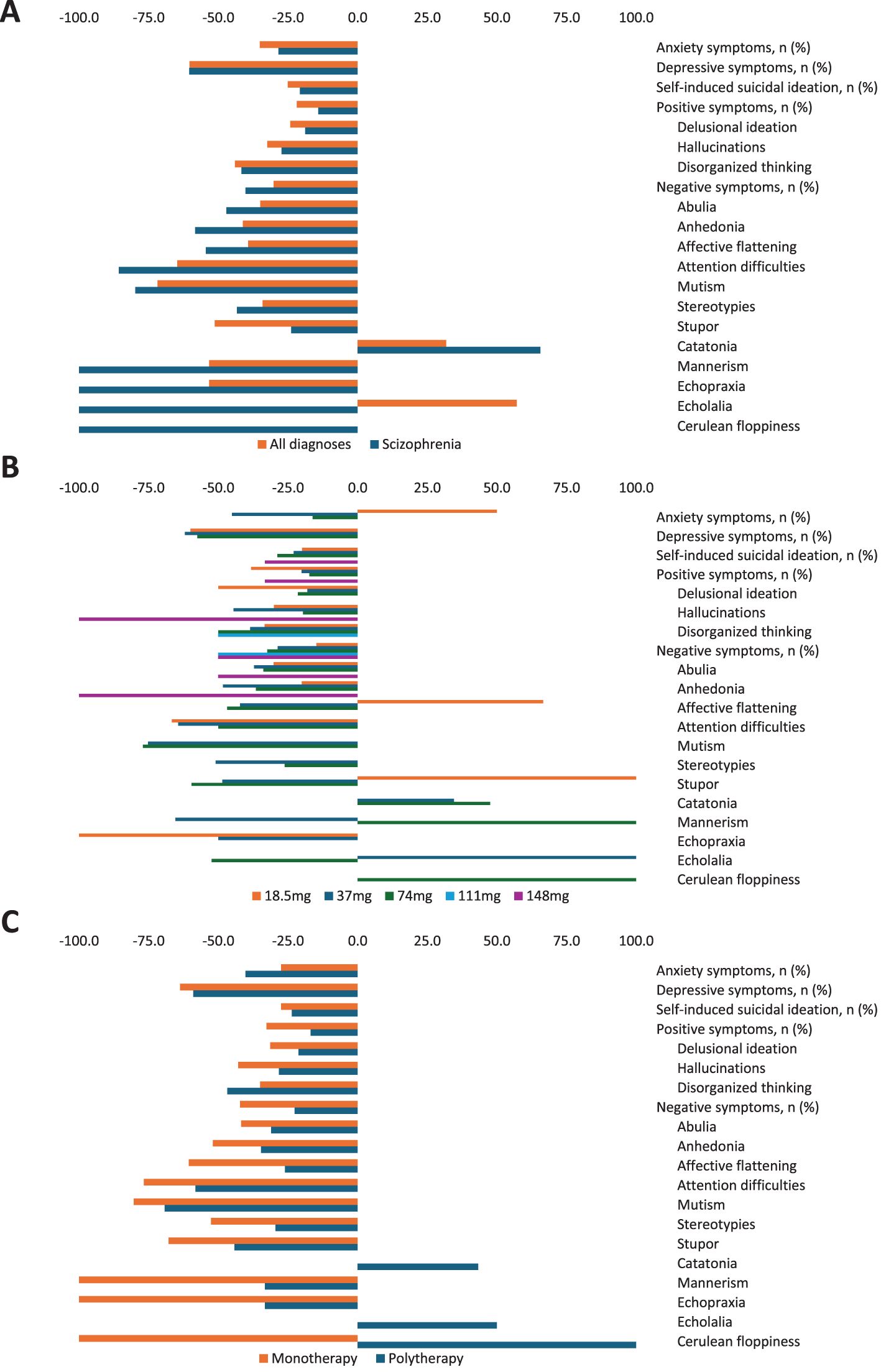
Figure 4. (A) Signs and symptoms variations between baseline and during lurasidone treatment by primary diagnosis, (B) maximum dose, and (C) type of treatment.
Although there was no apparent direct relationship between lurasidone dose and a decrease in the frequency of symptoms given the small sample size in the higher dose groups, it appeared that the greatest improvement in signs and symptoms from baseline was generally achieved with the highest dose used (Figure 4B; Supplementary Table 4). When stratified by treatment type, monotherapy was associated with a greater improvement than polytherapy for most symptoms, including positive symptoms such as delusional ideation or hallucinations, and most negative symptoms, including affective flattening, anhedonia, or abulia. Greater improvements were also achieved with monotherapy for depression and suicidal ideation. On the other hand, polytherapy was better than monotherapy in improving symptoms such as disorganized thinking and anxiety (Figure 4C; Supplementary Table 5).
Potential treatment-emergent adverse events at baseline and during follow-up are shown in Table 2. Among those occurring in ≥10% of patients, the most common were paresthesia (23.5%), obesity (22.8%), and hypercholesterolemia (22.4%). Lurasidone treatment substantially reduced all adverse events, except for rhabdomyolysis, leukopenia, and neuroleptic malignant syndrome, which did not change during follow-up. Overall, lurasidone reduced up to 80% of all recorded potential adverse events by at least ‒50% (Supplementary Table 6). Moreover, a few comorbidities first occurred during lurasidone treatment (Supplementary Table 7).
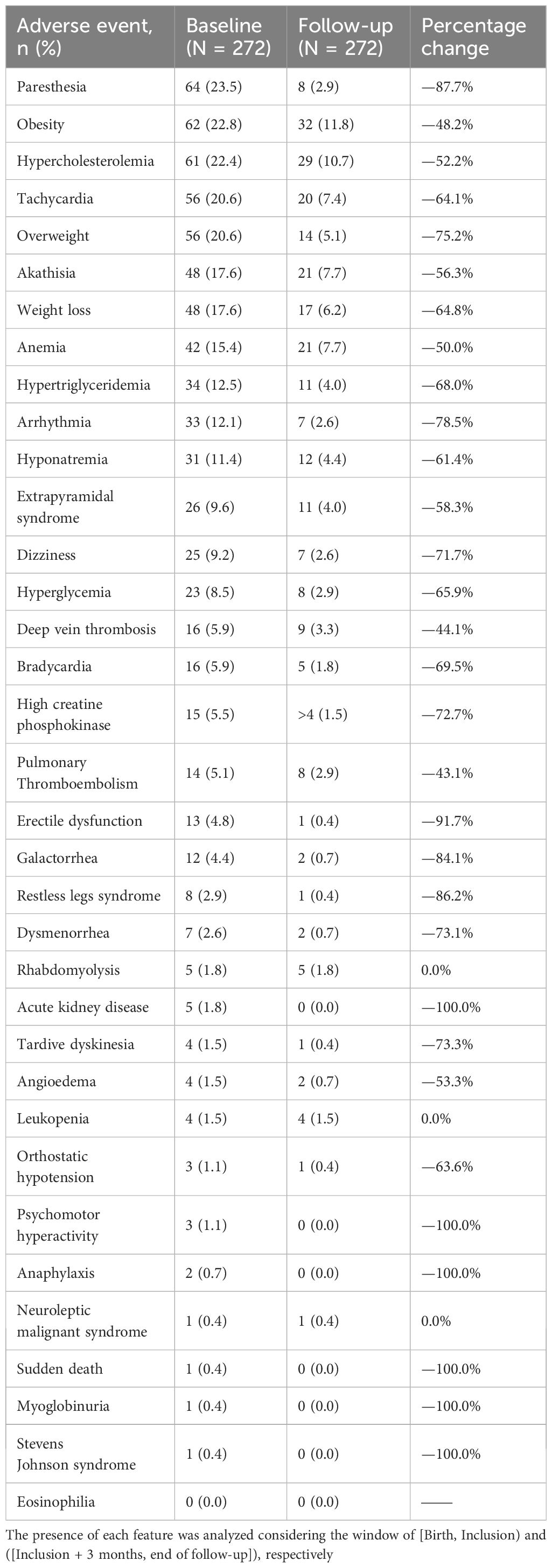
Table 2. Potential treatment-related adverse events at baseline and during follow-up.
In this real-world study using NLP and ML techniques, we established a large cohort of 272 real-life patients with psychiatric disorders who were treated with lurasidone across four Spanish hospitals. The median age of our cohort was 46 years and no patients younger than 18 years were detected, consistent with lurasidone unapproved status in adolescent patients at the start of the study. The most common primary diagnoses were schizophrenia, depression, and bipolar disorder, with differences in age and sex demographics aligned with recent publications (36, 37). For example, we observed a notable predominance of women, which likely reflects the higher prevalence of certain psychiatric disorders among females reported in the literature, such as major depressive disorder (38). Almost half of the patients were using substances, mainly cannabis, which is known to increase the risk of relapse, depressive symptoms, and suicidal behavior after the first episode of psychosis (39, 40). Moreover, substance use, particularly cannabis and synthetic cannabinoids, have been identified as key predictors of readmission in young patients following a psychotic episode, underscoring the need for targeted interventions in this population (41).
In terms of comorbidities, patients with schizophrenia and bipolar disorder are at a higher risk of developing metabolic syndrome and diabetes compared to the general population (42–44). However, the prevalence of cardiometabolic risk in these patients is likely underestimated due to underdiagnosis and undertreatment (45). We observed that a significant percentage of our cohort had conditions like hypertension (46.7%), dyslipidemia (44.5%), diabetes (30.5%), obesity (23.9%), and stroke (14.3%) at inclusion, which supports lurasidone’s preference among patients with such comorbidities due to its favorable metabolic profile (46). This is important because, unlike other antipsychotics such as olanzapine or quetiapine, lurasidone contributes to weight loss in patients with psychiatric disorders and comorbid obesity (47, 48). This was seen in our study with a decreased number of patients reporting obesity during lurasidone treatment.
When looking at lurasidone use, the predominant dosage was 37 mg/day, followed by 74 mg/day, with minimal utilization of 111 mg/day and 148 mg/day (<1.2%). This observation was independent of the primary diagnosis, the occurrence of psychiatric hospitalizations, or the use of lurasidone as monotherapy or polytherapy. The recommended starting dose of lurasidone in schizophrenia patients is 37 mg/day, which may be increased to a maximum of 148 mg/day based on physician judgment and observed clinical response (4). Although the starting dose of lurasidone has demonstrated significant efficacy in reducing the Positive and Negative Syndrome Scale (PANSS) total score, some studies indicate that patients with suboptimal symptom control at lower doses can benefit from higher doses (15, 49). In particular, higher doses (111-148 mg/day) have shown greater efficacy than lower doses (37-74 mg/day) in patients with acute psychotic symptoms of schizophrenia and severe agitation at baseline (50), and this high dose of lurasidone has not been associated with increased weight gain or adverse effects (51). Moreover, specific dose-related anti-hostility effects have been also described (52). This provides evidence that lurasidone is often prescribed at dosages below the recommended levels in Spain, particularly in patients with schizophrenia, which could have limited its effectiveness, especially in patients who failed other antipsychotic therapies. Although the data from this study do not allow us to fully explore the specific reasons behind the administered doses, some potential factors might include the preference for lower doses to minimize side effects, address comorbidities, or comply with institutional barriers such as formulary restrictions and cost. Additionally, lower doses might have been used as adjunctive therapy to manage residual symptoms while reducing the risk of adverse effects associated with other treatments like olanzapine (53). Furthermore, the inclusion of conditions other than schizophrenia in our study where lower doses are typically prescribed may also have contributed to this observation (54).
Long-term effectiveness of antipsychotic drugs is critical considering that more than 80% of patients with schizophrenia experience relapse within the first 5 years of treatment (55). While the benefits of long-acting injectable (LAI) antipsychotics in reducing readmission rates following a first episode of psychosis are well-documented (56, 57), there is other reference highlighting that LAIs and oral antipshychotics did not differ significantly regarding relapse prevention/hospitalization and acceptability (58). Additional evidence supports the efficacy of lurasidone in achieving higher remission rates and reducing the risk of hospitalization compared to quetiapine, which was the second most commonly used antipsychotic in our study prior to lurasidone (41, 59). Furthermore, in bipolar patients, hospitalization risk has been shown to be higher with olanzapine or aripiprazole, underscoring the potential advantages of lurasidone in this population (60). In our whole population, the relapse rate for patients on lurasidone monotherapy was notably lower after the inclusion date (17.6% vs. 9.3%), whereas it increased for those on polytherapy (16.5% vs. 26.2%). While antipsychotic monotherapy is preferred over polytherapy whenever possible [(61) and references therein] and shows better retention rates (62, 63), polytherapy has demonstrated superiority in reducing the likelihood of mortality and hospitalization risk in schizophrenia in patients with second-generation antipsychotics. In our study, patients receiving monotherapy showed lower discontinuation rates than patients receiving polytherapy (41.3% vs. 58.7%). Moreover, when stratified by treatment type, lurasidone monotherapy exhibited superior improvement over polytherapy for most symptoms, including positive and negative, as well as depression and suicidal ideation. In this context, the role of lurasidone in non-core symptoms such as depression and anhedonia has been previously described (64–66). Finally, lurasidone retention after 30 months of follow-up surpassed that reported in other studies, possibly reflecting its favorable efficacy, tolerability, and patient satisfaction, highlighting its acceptability profile (67–71). In this regard, while lurasidone has demonstrated efficacy in both monotherapy and combination therapy, we observed that monotherapy offers several distinct advantages.
On the other hand, our results showed a lack of clear dose-response relationship, possibly due to the complex pharmacodynamics of lurasidone. Variability in patient metabolism, partial adherence, and potential drug-drug interactions may also contribute to this phenomenon (72, 73). However, an independent analysis (51) demonstrated that while the efficacy of lurasidone follows a dose-response pattern in terms of efficacy, this relationship does not extend to its adverse events, underscoring the need for further research into optimized dosing and personalized treatment approaches. Additionally, individualized dosing strategies tailored to patient-specific factors such as comorbidities, treatment history, and tolerability further complicate the dose-response relationship. Lurasidone alleviated both positive and negative symptoms along with depressive and anxiety symptoms; however, we noted a slight increase in the proportion of patients with catatonia during follow-up —a common adverse effect induced by antipsychotics [(74) and references therein]. Comparative efficacy studies suggest no significant differences among available antipsychotics for positive symptoms and disorganization, except for the superior efficacy of clozapine in treating treatment-resistant schizophrenia (75). Interestingly, a retrospective chart review revealed positive outcomes for most patients with treatment-resistant schizophrenia who received a combination of lurasidone and clozapine, showing reductions in positive, depressive, and anxiety symptoms, alongside improvements in psychosocial functioning in a real-world setting (31). Therefore, the combination of lurasidone and clozapine could be an optimal polytherapy strategy for those patients with treatment-resistant schizophrenia.
Despite similar efficacy, antipsychotics exhibit diverse adverse effects. Lurasidone stands out for its favorable tolerability profile, with minimal effects on metabolic parameters and weight gain, although it carries a modest risk of extrapyramidal and other side effects (76). Notably, all major metabolic and CV adverse events were reduced during lurasidone treatment compared to the pre-treatment profile. In general practice, however, lurasidone is combined with other antipsychotics that may worsen the comorbid state of patients.
The main strength of this multicenter study is the use of innovative technology to extract and interpret large-scale RWD, providing useful information of lurasidone usage in Spain. These methods were specifically employed with rigorous validation steps and the inclusion of comprehensive patients’ clinical information across multiple hospital departments, ensuring a more reliable and multidisciplinary perspective of the patient population. This approach is different from prospective studies, where strict inclusion criteria are applied, and patient selection is more controlled. Then, our design aimed to minimize selection bias by capturing a broad, real-world cohort that reflects the diverse patient population receiving lurasidone treatment in routine clinical practice. However, limitations exist, including reliance on structured data and free-text narratives recorded in EHRs which might be constrained by the accuracy of physicians’ descriptions. This limitation could account for patient loss during follow-up and missing data points across variables. While our multicenter approach optimizes an accurate and representative characterization of patients treated with lurasidone in real-world settings, variations in the EHR systems and data collection across sites may introduce data heterogeneity. We also recognize that the inclusion of data exclusively from centers in Spain may limit the generalizability of our findings to other healthcare systems. The Spanish healthcare system, characterized by its publicly funded, universal coverage and standardized use of EHRs, may differ from systems with less uniform access to care or fragmented data infrastructures, potentially affecting the applicability of our results in other contexts. Additionally, we acknowledge that the complex clinical profiles of patients with schizophrenia make it inherently difficult to isolate the impact of any single treatment. However, the objective of this study was purely descriptive, and future research will be needed to compare different patient groups while appropriately balancing confounding factors. Finally, our methodology does not allow us to estimate causal effects.
In conclusion, by applying NLP to the free text in the EHRs of patients treated with lurasidone, we obtained a real-world picture of lurasidone use in Spain which helps fill a large research gap. Lurasidone effectively reduced the frequency of positive and negative symptoms maintaining a good safety profile, even at high doses, in monotherapy or polytherapy. This efficacy and safety spanned all pathologies studied, not just schizophrenia. Despite its positive outcomes and low discontinuation rates, lurasidone dosing in Spanish clinical practice remains conservative, indicating a need for optimized dosing strategies to enhance patient outcomes. Future clinical trials and larger prospective studies are warranted to evaluate the comparative effectiveness of lurasidone in specific subpopulations and to further validate its role in both monotherapy and polytherapy contexts, as well as studies that explore the reasons behind underdosing of the drug in real-world settings.
Data can be shared on reasonable request to the corresponding author after permission has been obtained from the institutions involved.
The studies involving humans were approved by Comité de Ética de la Investigación con medicamentos de las Islas Baleares. CÓDIGO CEIm: IB 4667/21 EOm. The studies were conducted in accordance with the local legislation and institutional requirements. The ethics committee/institutional review board waived the requirement of written informed consent for participation from the participants or the participants’ legal guardians/next of kin because the data were anonymized data and treated as aggregated data.
FM: Investigation, Resources, Writing – review & editing. CG: Investigation, Resources, Writing – review & editing. MD: Investigation, Writing – review & editing. CR: Investigation, Writing – review & editing. AC: Writing – review & editing. DP: Writing – review & editing. EÁ-B: Writing – review & editing. IG-I: Funding acquisition, Investigation, Resources, Supervision, Writing – review & editing, Conceptualization, Project administration, Visualization.
Carlo Sguera, Daniel Salvador, David Casadevall, Eduard Sarró, Eva Castillo, Ignacio Salcedo, Judith Marín-Corral, Miren Taberna, Natalia Polo, Paulo Luz, and Sebastian Menke.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This study was sponsored by Angelini Pharma España SLU.
AC, DP, EÁ-B and IG-I are employees of Angelini Pharma. The study was conducted by Medsavana S.L and Savana Research S.L, of which Savana Research Group members are employees.
The authors declare that this study received funding from Angelini Pharma. The funder had the following involvement in the study: study design, interpretation of data, the writing of this article, and the decision to submit it for publication.
The author(s) declare that no Generative AI was used in the creation of this manuscript.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2024.1506142/full#supplementary-material
1. Arango C, Baeza I, Bernardo M, Canas F, de Dios C, Diaz-Marsa M, et al. Long-acting injectable antipsychotics for the treatment of schizophrenia in Spain. Rev Psiquiatr Salud Ment (Engl Ed). (2019) 12:92–105. doi: 10.1016/j.rpsm.2018.03.006
2. Grunder G, Heinze M, Cordes J, Muhlbauer B, Juckel G, Schulz C, et al. Effects of first-generation antipsychotics versus second-generation antipsychotics on quality of life in schizophrenia: a double-blind, randomized study. Lancet Psychiatry. (2016) 3:717–29. doi: 10.1016/S2215-0366(16)00085-7
3. Drug approval package Latuda (lurasidone hydrochloride). MA, USA: U.S. Food and Drug Administration (2010). Available online at: https://www.accessdata.fda.gov/drugsatfda_docs/nda/2010/200603Orig1s000TOC.cfm.
4. Latuda (Lurasidone). Amsterdam, Netherlands: European Medicines Agency (2014). Available online at: https://www.ema.europa.eu/en/medicines/human/EPAR/latuda.
5. Kroeze WK, Hufeisen SJ, Popadak BA, Renock SM, Steinberg S, Ernsberger P, et al. H1-histamine receptor affinity predicts short-term weight gain for typical and atypical antipsychotic drugs. Neuropsychopharmacology. (2003) 28:519–26. doi: 10.1038/sj.npp.1300027
6. Reynolds GP, Kirk SL. Metabolic side effects of antipsychotic drug treatment–pharmacological mechanisms. Pharmacol Ther. (2010) 125:169–79. doi: 10.1016/j.pharmthera.2009.10.010
7. Lord C, Sekerovic Z, Carrier J. Sleep regulation and sex hormones exposure in men and women across adulthood. Pathol Biol (Paris). (2014) 62:302–10. doi: 10.1016/j.patbio.2014.07.005
8. Citrome L. Lurasidone for schizophrenia: a review of the efficacy and safety profile for this newly approved second-generation antipsychotic. Int J Clin Pract. (2011) 65:189–210. doi: 10.1111/j.1742-1241.2010.02587.x
9. Citrome L. Lurasidone in schizophrenia: new information about dosage and place in therapy. Adv Ther. (2012) 29:815–25. doi: 10.1007/s12325-012-0052-6
10. Leucht S, Corves C, Arbter D, Engel RR, Li C, Davis JM. Second-generation versus first-generation antipsychotic drugs for schizophrenia: a meta-analysis. Lancet. (2009) 373:31–41. doi: 10.1016/S0140-6736(08)61764-X
11. Samalin L, Garnier M, Llorca PM. Clinical potential of lurasidone in the management of schizophrenia. Ther Clin Risk Manage. (2011) 7:239–50. doi: 10.2147/TCRM.S12701
12. Correll CU, Tocco M, Hsu J, Goldman R, Pikalov A. Short-term efficacy and safety of lurasidone versus placebo in antipsychotic-naive vs. Previously treated adolescents with an acute exacerbation of schizophrenia. Eur Psychiatry. (2022) 65:1–35. doi: 10.1192/j.eurpsy.2022.11
13. Correll CU, Tocco M, Pikalov A, Hsu J, Goldman R. Long-term safety and effectiveness of open-label lurasidone in antipsychotic-Naive versus previously treated adolescents with Schizophrenia: A post-hoc analysis. Schizophr Res. (2022) 240:205–13. doi: 10.1016/j.schres.2021.12.046
14. Cruz MP. Lurasidone HCl (Latuda), an oral, once-daily atypical antipsychotic agent for the treatment of patients with schizophrenia. P T. (2011) 36:489–92.
15. Loebel A, Citrome L. Lurasidone: a novel antipsychotic agent for the treatment of schizophrenia and bipolar depression. BJPsych Bull. (2015) 39:237–41. doi: 10.1192/pb.bp.114.048793
16. Pillarella J, Higashi A, Alexander GC, Conti R. Trends in use of second-generation antipsychotics for treatment of bipolar disorder in the United States, 1998-2009. Psychiatr Serv. (2012) 63:83–6. doi: 10.1176/appi.ps.201100092
17. Mills J. More than a half-century with haloperidol: glories, disparities, and use today. Issues Ment Health Nurs. (2023) 44:83–7. doi: 10.1080/01612840.2022.2158683
18. Campos P, Carrió M, Vicedo A, Bioque M. Actitud de los psiquiatras respecto al uso de olanzapina en la práctica clínica: una encuesta nacional. Psiquiatría Biológica. (2020) 27:3–8. doi: 10.1016/j.psiq.2019.11.001
19. Parramon Ponz M, Ovejero S. PMH41 the real world use of oral antipsychotics in Spain-still a need for new treatments? Value Health. (2019) S688. doi: 10.1016/j.jval.2019.09.1515
20. Stroup TS, Gerhard T, Crystal S, Huang C, Olfson M. Geographic and clinical variation in clozapine use in the United States. Psychiatr Serv. (2014) 65:186–92. doi: 10.1176/appi.ps.201300180
21. Raja M. Pharmacotherapy update: risperidone in the treatment of schizophrenia. Clin Med Ther. (2009) 1. doi: 10.4137/CMT.S1123
22. Leucht S, Schneider-Thoma J, Burschinski A, Peter N, Wang D, Dong S, et al. Long-term efficacy of antipsychotic drugs in initially acutely ill adults with schizophrenia: systematic review and network meta-analysis. World Psychiatry. (2023) 22:315–24. doi: 10.1002/wps.21089
23. Phalguni A, McCool R, Wood H, Sanderson A, Rydevik G, Franklin B, et al. Systematic literature review and network meta-analysis of lurasidone, brexpiprazole and cariprazine for schizophrenia. Int Clin Psychopharmacol. (2023) 38:45–56. doi: 10.1097/YIC.0000000000000427
24. Arango C, Ng-Mak D, Finn E, Byrne A, Loebel A. Lurasidone compared to other atypical antipsychotic monotherapies for adolescent schizophrenia: a systematic literature review and network meta-analysis. Eur Child Adolesc Psychiatry. (2020) 29:1195–205. doi: 10.1007/s00787-019-01425-2
25. Sabe M, Pallis K, Solmi M, Crippa A, Sentissi O, Kaiser S. Comparative effects of 11 antipsychotics on weight gain and metabolic function in patients with acute schizophrenia: A dose-response meta-analysis. J Clin Psychiatry. (2023) 84: 22r14490. doi: 10.4088/JCP.22r14490
26. Sabe M, Zhao N, Crippa A, Kaiser S. Antipsychotics for negative and positive symptoms of schizophrenia: dose-response meta-analysis of randomized controlled acute phase trials. NPJ Schizophr. (2021) 7:43. doi: 10.1038/s41537-021-00171-2
27. Hojlund M, Kohler-Forsberg O, Gregersen AT, Rohde C, Mellentin AI, Anhoj SJ, et al. Prevalence, correlates, tolerability-related outcomes, and efficacy-related outcomes of antipsychotic polypharmacy: a systematic review and meta-analysis. Lancet Psychiatry. (2024) 11:975–89. doi: 10.1016/S2215-0366(24)00314-6
28. Orrico-Sanchez A, Lopez-Lacort M, Munoz-Quiles C, Sanfelix-Gimeno G, Diez-Domingo J. Epidemiology of schizophrenia and its management over 8-years period using real-world data in Spain. BMC Psychiatry. (2020) 20:149. doi: 10.1186/s12888-020-02538-8
29. Lee S, Xu Y, Das AG, Martin EA, Doktorchik C, Zhang Z, et al. Unlocking the potential of electronic health records for health research. Int J Popul Data Sci. (2020) 5:1123. doi: 10.23889/ijpds.v5i1.1123
30. Khosla S, Tepie MF, Nagy MJ, Kafatos G, Seewald M, Marchese S, et al. The alignment of real-world evidence and digital health: realizing the opportunity. Ther Innov Regul Sci. (2021) 55:889–98. doi: 10.1007/s43441-021-00288-7
31. Siwek M, Chrobak AA, Gorostowicz A, Krol P, Dudek D. Lurasidone augmentation of clozapine in schizophrenia-retrospective chart review. Brain Sci. (2023) 13:445. doi: 10.3390/brainsci13030445
32. Izquierdo JL, Morena D, Gonzalez Y, Paredero JM, Perez B, Graziani D, et al. Clinical management of COPD in a real-world setting. A Big Data Analysis. Arch Bronconeumol (Engl Ed). (2021) 57:94–100. doi: 10.1016/j.arbr.2019.12.023
33. Benson T. Principles of health interoperability HL7 and SNOMED. 2nd. London, UK: Springer (2012).
34. Espinosa L, Tello J, Pardo A, Medrano I, Ureña A, Salcedo I, et al. Savana: A global information extraction and terminology expansion framework in the medical domain. Procesamiento del Lenguaje Natural. (2016) 57:23–30.
35. Canales L, Menke S, Marchesseau S, D'Agostino A, Del Rio-Bermudez C, Taberna M, et al. Assessing the performance of clinical natural language processing systems: development of an evaluation methodology. JMIR Med Inform. (2021) 9:e20492. doi: 10.2196/20492
36. Solmi M, Radua J, Olivola M, Croce E, Soardo L, Salazar de Pablo G, et al. Age at onset of mental disorders worldwide: large-scale meta-analysis of 192 epidemiological studies. Mol Psychiatry. (2022) 27:281–95. doi: 10.1038/s41380-021-01161-7
37. Green T, Flash S, Reiss AL. Sex differences in psychiatric disorders: what we can learn from sex chromosome aneuploidies. Neuropsychopharmacology. (2019) 44:9–21. doi: 10.1038/s41386-018-0153-2
38. Albert PR. Why is depression more prevalent in women? J Psychiatry Neurosci. (2015) 40:219–21. doi: 10.1503/jpn.150205
39. Schoeler T, Petros N, Di Forti M, Klamerus E, Foglia E, Murray R, et al. Poor medication adherence and risk of relapse associated with continued cannabis use in patients with first-episode psychosis: a prospective analysis. Lancet Psychiatry. (2017) 4:627–33. doi: 10.1016/S2215-0366(17)30233-X
40. Coentre R, Talina MC, Gois C, Figueira ML. Depressive symptoms and suicidal behavior after first-episode psychosis: A comprehensive systematic review. Psychiatry Res. (2017) 253:240–8. doi: 10.1016/j.psychres.2017.04.010
41. Besana F, Civardi SC, Mazzoni F, Carnevale Miacca G, Arienti V, Rocchetti M, et al. Predictors of readmission in young adults with first-episode psychosis: A multicentric retrospective study with a 12-month follow-up. Clin Pract. (2024) 14:1234–44. doi: 10.3390/clinpract14040099
42. Vancampfort D, Wampers M, Mitchell AJ, Correll CU, De Herdt A, Probst M, et al. A meta-analysis of cardio-metabolic abnormalities in drug naive, first-episode and multi-episode patients with schizophrenia versus general population controls. World Psychiatry. (2013) 12:240–50. doi: 10.1002/wps.20069
43. Vancampfort D, Vansteelandt K, Correll CU, Mitchell AJ, De Herdt A, Sienaert P, et al. Metabolic syndrome and metabolic abnormalities in bipolar disorder: a meta-analysis of prevalence rates and moderators. Am J Psychiatry. (2013) 170:265–74. doi: 10.1176/appi.ajp.2012.12050620
44. Crump C, Sundquist K, Winkleby MA, Sundquist J. Comorbidities and mortality in bipolar disorder: a Swedish national cohort study. JAMA Psychiatry. (2013) 70:931–9. doi: 10.1001/jamapsychiatry.2013.1394
45. Correll CU, Ng-Mak DS, Stafkey-Mailey D, Farrelly E, Rajagopalan K, Loebel A. Cardiometabolic comorbidities, readmission, and costs in schizophrenia and bipolar disorder: a real-world analysis. Ann Gen Psychiatry. (2017) 16:9. doi: 10.1186/s12991-017-0133-7
46. Riva MA, Albert U, de Filippis S, Vita A, De Berardis D. Identification of clinical phenotypes in schizophrenia: the role of lurasidone. Ther Adv Psychopharmacol. (2021) 11:20451253211012250. doi: 10.1177/20451253211012250
47. Meyer JM, Mao Y, Pikalov A, Cucchiaro J, Loebel A. Weight change during long-term treatment with lurasidone: pooled analysis of studies in patients with schizophrenia. Int Clin Psychopharmacol. (2015) 30:342–50. doi: 10.1097/YIC.0000000000000091
48. Meyer JM, Ng-Mak DS, Chuang CC, Rajagopalan K, Loebel A. Weight changes before and after lurasidone treatment: a real-world analysis using electronic health records. Ann Gen Psychiatry. (2017) 16:36. doi: 10.1186/s12991-017-0159-x
49. Citrome L. Lurasidone for the acute treatment of adults with schizophrenia: what is the number needed to treat, number needed to harm, and likelihood to be helped or harmed? Clin Schizophr Relat Psychoses. (2012) 6:76–85. doi: 10.3371/CSRP.6.2.5
50. Allen MH, Citrome L, Pikalov A, Hsu J, Loebel A. Efficacy of lurasidone in the treatment of agitation: A post hoc analysis of five short-term studies in acutely ill patients with schizophrenia. Gen Hosp Psychiatry. (2017) 47:75–82. doi: 10.1016/j.genhosppsych.2017.05.002
51. Srisurapanont M, Suttajit S, Likhitsathian S, Maneeton B, Maneeton N. A network meta-analysis of the dose-response effects of lurasidone on acute schizophrenia. Sci Rep. (2021) 11:5571. doi: 10.1038/s41598-021-84836-z
52. Citrome L, Alvarez-Baron E, Gabarda-Inat I, Thangavelu K, Tocco M. The specific anti-hostility effect of lurasidone in patients with an acute exacerbation of schizophrenia: results of pooled post hoc analyses in adolescents and adults. Int Clin Psychopharmacol. (2024). doi: 10.1097/YIC.0000000000000563
53. Guarro Carreras MT, Jimenez Suarez L, Lago Garcia L, Montes Reula L, Neyra Del Rosario A, Rodriguez Batista FA, et al. Towards full recovery with lurasidone: effective doses in the treatment of agitation, affective, positive, and cognitive symptoms in schizophrenia and of dual psychosis. Drugs Context. (2024) 13: 2024–4–4. doi: 10.7573/dic.2024-4-4
54. Lin YW, Chen YB, Hung KC, Liang CS, Tseng PT, Carvalho AF, et al. Efficacy and acceptability of lurasidone for bipolar depression: a systematic review and dose-response meta-analysis. BMJ Ment Health. (2024) 27:e301165. doi: 10.1136/bmjment-2024-301165
55. Robinson D, Woerner MG, Alvir JM, Bilder R, Goldman R, Geisler S, et al. Predictors of relapse following response from a first episode of schizophrenia or schizoaffective disorder. Arch Gen Psychiatry. (1999) 56:241–7. doi: 10.1001/archpsyc.56.3.241
56. Tiihonen J, Mittendorfer-Rutz E, Majak M, Mehtala J, Hoti F, Jedenius E, et al. Real-world effectiveness of antipsychotic treatments in a nationwide cohort of 29 823 patients with schizophrenia. JAMA Psychiatry. (2017) 74:686–93. doi: 10.1001/jamapsychiatry.2017.1322
57. Ostuzzi G, Bertolini F, Del Giovane C, Tedeschi F, Bovo C, Gastaldon C, et al. Maintenance treatment with long-acting injectable antipsychotics for people with nonaffective psychoses: A network meta-analysis. Am J Psychiatry. (2021) 178:424–36. doi: 10.1176/appi.ajp.2020.20071120
58. Vita G, Tavella A, Ostuzzi G, Tedeschi F, De Prisco M, Segarra R, et al. Efficacy and safety of long-acting injectable versus oral antipsychotics in the treatment of patients with early-phase schizophrenia-spectrum disorders: a systematic review and meta-analysis. Ther Adv Psychopharmacol. (2024) 14:20451253241257062. doi: 10.1177/20451253241257062
59. Loebel A, Cucchiaro J, Xu J, Sarma K, Pikalov A, Kane JM. Effectiveness of lurasidone vs. quetiapine XR for relapse prevention in schizophrenia: a 12-month, double-blind, noninferiority study. Schizophr Res. (2013) 147:95–102. doi: 10.1016/j.schres.2013.03.013
60. Kadakia A, Dembek C, Liu Y, Dieyi C, Williams GR. Hospitalization risk in pediatric patients with bipolar disorder treated with lurasidone vs. other oral atypical antipsychotics: a real-world retrospective claims database study. J Med Econ. (2021) 24:1212–20. doi: 10.1080/13696998.2021.1993862
61. Faries D, Ascher-Svanum H, Zhu B, Correll C, Kane J. Antipsychotic monotherapy and polypharmacy in the naturalistic treatment of schizophrenia with atypical antipsychotics. BMC Psychiatry. (2005) 5:26. doi: 10.1186/1471-244X-5-26
62. Fisher MD, Reilly K, Isenberg K, Villa KF. Antipsychotic patterns of use in patients with schizophrenia: polypharmacy versus monotherapy. BMC Psychiatry. (2014) 14:341. doi: 10.1186/s12888-014-0341-5
63. Katona L, Bitter I, Czobor P. A meta-analysis of effectiveness of real-world studies of antipsychotics in schizophrenia: Are the results consistent with the findings of randomized controlled trials? Transl Psychiatry. (2021) 11:510. doi: 10.1038/s41398-021-01636-9
64. De Berardis D, Vellante F, Olivieri L, Rapini G, De Lauretis I, Orsolini L, et al. The effect of paliperidone palmitate long-acting injectable (PP-LAI) on "non-core" symptoms of schizophrenia: a retrospective, collaborative, multicenter study in the "real world" everyday clinical practice. Riv Psichiatr. (2021) 56:143–8. doi: 10.1708/3635.36155
65. Fiorillo A, Sampogna G, Albert U, Bondi E, De Giorgi S, Fagiolini A, et al. The role of lurasidone in managing depressive symptoms in people with schizophrenia: A review. Brain Sci. (2024) 14:225. doi: 10.3390/brainsci14030225
66. Guinart D, Fagiolini A, Fusar-Poli P, Giordano GM, Leucht S, Moreno C, et al. On the road to individualizing pharmacotherapy for adolescents and adults with schizophrenia - results from an expert consensus following the delphi method. Neuropsychiatr Dis Treat. (2024) 20:1139–52. doi: 10.2147/NDT.S456163
67. Lieberman JA, Stroup TS, McEvoy JP, Swartz MS, Rosenheck RA, Perkins DO, et al. Effectiveness of antipsychotic drugs in patients with chronic schizophrenia. N Engl J Med. (2005) 353:1209–23. doi: 10.1056/NEJMoa051688
68. Fagiolini A, Olivola M, Lavatelli L, Bellomo A, Lobaccaro C, Falsetto N, et al. Treatment persistence in patients with schizophrenia treated with lurasidone in Italian clinical practice. Ann Gen Psychiatry. (2022) 21:49. doi: 10.1186/s12991-022-00425-y
69. Sampogna G, Di Vincenzo M, Giuliani L, Menculini G, Mancuso E, Arsenio E, et al. A systematic review on the effectiveness of antipsychotic drugs on the quality of life of patients with schizophrenia. Brain Sci. (2023) 13:1577. doi: 10.3390/brainsci13111577
70. De Filippis S, Vita A, Cuomo A, Amici E, Giovanetti V, Lombardozzi G, et al. Treatment satisfaction and effectiveness of Lurasidone on quality of life and functioning in adult patients with schizophrenia in the real-world Italian clinical practice: a prospective 3-month observational study. Ann Gen Psychiatry. (2024) 23:43. doi: 10.1186/s12991-024-00531-z
71. Awad G, Ng-Mak D, Rajagopalan K, Hsu J, Pikalov A, Loebel A. Long-term health-related quality of life improvements among patients treated with lurasidone: results from the open-label extension of a switch trial in schizophrenia. BMC Psychiatry. (2016) 16:176. doi: 10.1186/s12888-016-0879-5
72. Davis JM, Chen N. Dose response and dose equivalence of antipsychotics. J Clin Psychopharmacol. (2004) 24:192–208. doi: 10.1097/01.jcp.0000117422.05703.ae
73. Potkin SG, Keator DB, Kesler-West ML, Nguyen DD, van Erp TG, Mukherjee J, et al. D2 receptor occupancy following lurasidone treatment in patients with schizophrenia or schizoaffective disorder. CNS Spectr. (2014) 19:176–81. doi: 10.1017/S109285291300059X
74. Sienaert P, Dhossche DM, Vancampfort D, De Hert M, Gazdag G. A clinical review of the treatment of catatonia. Front Psychiatry. (2014) 5:181. doi: 10.3389/fpsyt.2014.00181
75. Huhn M, Nikolakopoulou A, Schneider-Thoma J, Krause M, Samara M, Peter N, et al. Comparative efficacy and tolerability of 32 oral antipsychotics for the acute treatment of adults with multi-episode schizophrenia: a systematic review and network meta-analysis. Lancet. (2019) 394:939–51. doi: 10.1016/S0140-6736(19)31135-3
Keywords: lurasidone, schizophrenia, bipolar depression, Spain, electronic health records
Citation: Mora F, Gómez Sánchez-Lafuente C, De Iceta M, Roset C, Cárdenas A, Pérez D, Álvarez-Barón E, Gabarda-Inat I and Savana Research Group (2025) Lurasidone uses and dosages in Spain: RETROLUR, a real-world retrospective analysis using artificial intelligence. Front. Psychiatry 15:1506142. doi: 10.3389/fpsyt.2024.1506142
Received: 04 October 2024; Accepted: 27 December 2024;
Published: 05 February 2025.
Edited by:
Hiroyoshi Takeuchi, Keio University, JapanReviewed by:
Francesco Monaco, Azienda Sanitaria Locale Salerno, ItalyCopyright © 2025 Mora, Gómez Sánchez-Lafuente, De Iceta, Roset, Cárdenas, Pérez, Álvarez-Barón, Gabarda-Inat and Savana Research Group. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Irene Gabarda-Inat, aXJlbmUuZ2FiYXJkYUBhbmdlbGluaXBoYXJtYS5jb20=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.