 Xubin He
Xubin He Si Chen1
Si Chen1
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Psychiatry, 11 November 2024
Sec. Adolescent and Young Adult Psychiatry
Volume 15 - 2024 | https://doi.org/10.3389/fpsyt.2024.1484809
This article is part of the Research TopicChildren's Health and Screen TimeView all 8 articles
Background: Problematic Internet Use (PIU) has been increasingly linked to suicidal behavior among adolescents, raising significant public health concerns, particularly in Chinese youth. This study aimed to systematically review and meta-analyze the correlation between PIU and suicidal behavior in Chinese adolescents to provide a clearer understanding of this association.
Methods: A comprehensive search was conducted across seven databases up to July 1, 2024. Studies investigating the relationship between PIU and suicidal behavior among Chinese adolescents were included. A random-effects meta-analysis was employed to assess pooled effect sizes, with subgroup analyses conducted to explore potential moderators, such as geographic region, age, gender, assessment tools for PIU and suicidal ideation, and the presence of depression. Data analysis was performed using STATA software (version 16).
Results: This meta-analysis, comprising 23 studies with 353,904 participants, identified significant associations between PIU and suicidal behavior among Chinese adolescents. PIU was associated with increased risks of suicidal ideation (OR = 1.72, 95% CI: 1.45, 2.03), suicidal plans (OR = 1.50, 95% CI: 1.02, 2.20), and suicidal attempts (OR = 1.48, 95% CI: 1.16, 1.89). Subgroup analyses indicated higher risks in specific groups: adolescents from Central China (OR = 1.84, 95% CI: 1.46, 2.32), college students (OR = 2.09, 95% CI: 1.66, 2.62). The risk of suicidal ideation was particularly elevated when depression was not controlled (OR = 1.86, 95% CI: 1.53, 2.25). These findings underscore the need for targeted interventions in vulnerable populations.
Conclusion: This meta-analysis demonstrated significant associations between PIU and suicidal behaviors among Chinese adolescents. The findings emphasize the need for targeted interventions, particularly for adolescents from Central and Western China, college students, and those with untreated depression. Focused strategies are required to mitigate the risks associated with PIU and to effectively address suicidal behaviors in these high-risk populations.
Systematic review registration: https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42024577593, identifier CRD42024577593.
Globally, about 703,000 people commit suicide each year, accounting for 1.3% of total deaths. 77% of these occur in low-and middle-income countries, making it the second leading cause of death for 15-29-year-olds (1). By 2040, global suicide deaths are predicted to reach 1.03 million (2). Around 67,000 teenagers worldwide die by suicide each year, with over 88% in low- and middle-income countries (3, 4). In China, suicide is a main cause for teenagers (5), and is rising (6). Furthermore, adolescent suicides often occur in clusters, primarily within schools, making educational institutions critical settings for such incidents (7). Adolescent suicide not only has a profound impact on families but also exerts a negative influence on society. It is estimated that each suicide death affects at least 60 individuals, including family members, friends, and colleagues, increasing their risk of suicidal behavior, mental illness, and physical disorders, and impairing their social functioning (8, 9). Consequently, adolescent suicide has become a significant global public health concern.
The World Health Organization defines suicidal behavior as including suicidal ideation (SI), suicide planning (SP), and suicide attempt (SA) (10). SI refers to the repeated or persistent contemplation of ending one’s life, which may involve identifying a method, formulating a plan, or having an intent to act. SP involves the detailed formulation and design of specific steps toward a suicide attempt. SA refer to the actual execution of behaviors intended to end one’s life (11). Suicidal behavior has been identified as a critical and irreversible stage leading to suicide death, serving as one of the most significant warning indicators of potential suicide risk (12, 13). A survey conducted among 229,129 adolescents in 59 low- and middle-income countries revealed prevalence rates of 16.9% for SI, 17% for SP, and 17% for SA (14). Similarly, a survey of 1,103,309 adolescents in China reported that the rates for SI, SP, and SA were 15.4%, 6.4%, and 3.5%, respectively (15). Studies indicated that an individual’s sensitivity to pain, injury, fear, and death was reduced by repeated suicidal behavior, thereby ultimately increasing the risk of suicide (13). Thus, assessing the factors influencing suicidal behavior is crucial for the prevention of suicide deaths.
As of April 2024, the global internet user base has reached 5.44 billion. Of these, approximately 2.93 billion users are located in Asia, accounting for 53.9% of the worldwide total (16). Notably, China, home to the world’s largest internet user base, had 1.092 billion users by December 2023, as reported by the China Internet Network Information Center (CINIC) in its 53rd statistical report on internet development. Among these, 161 million were adolescents, comprising 14.7% of the total (17). Despite the advantages offered by online access for adolescents in education and daily routines, unchecked and excessive engagement was associated with the development of “Problematic Internet Use (PIU)” (18–20). PIU refers to a pattern of excessive or inappropriate internet use that manifests as frequent and prolonged usage, leading to significant negative impacts on an individual’s daily life, social relationships, academic or occupational performance (21). Although PIU can occur at any age, adolescence is considered the most vulnerable period. Adolescents are not only quick to adopt and become engrossed in the latest technologies and social media tools (22), but they are also more susceptible to the potential negative effects of internet use compared to other groups (23). Research indicates that PIU can lead to a range of serious issues among adolescents, including sleep disturbances, musculoskeletal and neurological problems, academic decline, procrastination, impulsivity, reduced self-esteem, diminished social interaction, feelings of loneliness, and suicidal behavior (24).
The prevalence of PIU and suicidal behavior was found to be high among Chinese adolescents, making it essential to explore their association to better understand the mental health status of this population. Studies indicated that cultural differences might have played a significant role in the relationship between mental health issues and behavioral problems (25). The relationship between PIU and suicidal behavior was particularly complex across different cultural contexts, potentially influencing both the manifestation and severity of suicide risk (26–28). According to the Interpersonal-Psychological Theory of Suicide proposed by Thomas Joiner, suicidal behavior primarily stems from three psychological factors: perceived burdensomeness, lack of belongingness, and acquired capability for suicide (29). Chinese adolescents, due to academic pressure and familial expectations, often experienced a sense of being a burden to others. When they were unable to obtain a sense of belonging in real life, they tended to rely on online social interactions as a form of substitute support. However, excessive dependence on the internet may have worsened feelings of loneliness and emotional distress. Furthermore, exposure to suicide-related information online was likely to reduce their fear of death, thereby further increasing the risk of suicidal behavior (30, 31). Although PIU had been identified as a potential risk factor for suicidal behavior, the relationship was not always clear (32). For instance, a study by Yang et al. found that after controlling for depressive symptoms, the association between PIU and suicidal behavior among adolescents was no longer significant, suggesting the complexity of this relationship (33). Therefore, investigating how PIU influences suicidal behavior among Chinese adolescents is crucial for developing effective prevention strategies.
To date, seven systematic reviews have extensively examined this association, four of which are narrative reviews (34–37). While these reviews supported the existence of a connection, the specifics and intensity of this relationship were still uncertain, largely due to the methodological limitations in the reviews. In a meta-analysis spanning diverse regions across Europe and Asia, it was found that PIU remained linked to suicidal behavior even after accounting for confounding variables like depression (38). However, this analysis did not thoroughly explore the relevant influencing factors specific to the adolescent population. Additionally, two recent systematic reviews (39, 40) highlighted the association between adolescent PIU and suicidal behavior, which was particularly pronounced. The reviews were limited by their small scope, each relying on only 3 or 4 studies, and potential influencing factors were not thoroughly examined. Therefore, this study aimed to synthesize previous research on the relationship between PIU and suicidal behavior among Chinese adolescents, with a particular focus on key variables that had not been thoroughly examined in prior studies. These variables included sociodemographic factors (such as age, gender, and region), differences in measurement tools used in research methods, and the control of confounding factors like depression (38). This approach was intended to address the gaps in existing research and lay the foundation for developing more specific intervention strategies in the future. Thus, the present study further explored the relationship between PIU and suicidal behavior among Chinese adolescents through the following research questions (1): What is the strength of the association between PIU and suicidal behavior among Chinese adolescents? (2) Do the control of variables in research methods (including demographic characteristics and factors such as depression) moderate the association between PIU and suicidal behavior?
The PRISMA guidelines for systematic reviews and meta-analyses were adhered to in the conduct of this study (41). The research protocol was officially registered in PROSPERO under the registration number CRD42024577593. It was noted that the PRISMA guidelines, recognized internationally as a standard, were provided as a comprehensive and rigorous framework for systematic reviews and meta-analyses. Meanwhile, the PROSPERO registration platform was utilized to ensure the transparency, reproducibility, and scientific integrity of the research protocol. This platform was used to help reduce research bias and to enable other researchers to track and evaluate the progress and quality of the study more effectively. Through PROSPERO registration, the design and methods of this study were clearly documented and made publicly accessible, thereby laying a solid foundation for subsequent research communication and application.
To explore the relationship between PIU and suicidal behavior, we searched seven databases (PubMed, Web of Science, EMBASE, CNKI, Wanfang Data, VIP Database, and CBM) from their establishment to July 1, 2024. In the search, we used detailed methods. In titles, abstracts, and subject terms, we carefully selected keywords divided into three groups: (“Suicide”, “Problematic Internet Use”, and “Adolescents”). For “Suicide”, we included common and specific terms like “suicide”, “self-harm”, “attempted suicide”, “suicidal behav*”, “suicidal ideation”, etc. For “Problematic Internet Use”, we covered expressions like “excessive internet use”, “internet addiction”, “problematic online behavior”, “compulsive internet use”, “maladaptive internet usage”, etc. For “Adolescents”, we included common and specific terms like “adolescents”, “teenagers”, “young people”, “youth”, “middle school students”, “college students”, etc. To ensure thoroughness, reference lists of the included studies were manually reviewed to identify any additional relevant articles. Additionally, manual cross-referencing of citations was performed to ensure thoroughness. The entire search strategy was meticulously documented to guarantee reproducibility. Further details regarding the search methodology can be found in Supplementary Material.
Inclusion criteria for the meta-analysis were as follows (1): Population: Studies that focused on Chinese adolescents aged 10 to 24 years (42) (2). Exposure: Research that specifically examined the association between PIU and suicidal behavior (3). Outcomes: Studies that reported relevant outcomes, including SI, SP, SA, with corresponding statistical measures such as Odds Ratio (OR) (4). Study Design: Peer-reviewed articles employing cross-sectional, case-control, or cohort study designs (5). Language: Articles published in either Chinese or English (6). Methodological Rigor: Studies that provided sufficient detail on their methodology, allowing for assessment of bias and overall study quality.
Exclusion criteria were defined as (1): Population: Studies that involved non-Chinese adolescents or included participants outside the age range of 10 to 24 years (2). Exposure: Research that focused on general internet use, other behavioral addictions, or any exposure not directly related to PIU and its association with suicidal behavior (3). Outcomes: Articles that did not report extractable data on suicidal behaviors or provided insufficient statistical information to calculate effect sizes (4). Study Design: Research formats such as reviews, systematic reviews, meta-analyses, conference abstracts, editorials, letters, comments, or case reports were excluded. Studies with a high risk of bias or those lacking peer review were also excluded.
Data extraction was conducted systematically to ensure consistency and accuracy across all included studies. A standardized data extraction form was developed and utilized by two independent reviewers (XBH, CS) to collect essential information, including study characteristics (author(s), year of publication, and study location), population details (sample size, age range, gender distribution, and specific demographic characteristics), exposure variables (definitions and measures of PIU, including criteria, scales, or questionnaires used), and outcome variables related to suicidal behavior (SI, SP, and SA), with corresponding OR and 95% CI where available. Adjustments for potential confounding factors, such as depression, were also noted, and the key findings of each study, particularly those related to the association between PIU and suicidal behavior, were summarized. The initial collection of literature, as well as the identification and removal of duplicate records, was performed using NoteExpress software. To ensure accuracy, all extracted data were cross-checked by a third reviewer (PY), with any discrepancies between the two primary reviewers resolved through discussion and consensus. In cases where consensus could not be reached, a senior researcher (BY) was consulted. The extracted data were then compiled into a comprehensive database for subsequent analysis.
The quality of the included studies was evaluated using two established tools: the Agency for Healthcare Research and Quality (AHRQ) methodology checklist and the Newcastle-Ottawa Scale (NOS). For cross-sectional studies, the AHRQ tool assessed 11 items, including population definition, sampling method, response rate, variable measurement, and data analysis. Each item was scored as “yes” (1 point), “no” (0 points), or “unclear” (0 points), with a maximum score of 11. Studies scoring 8 or above were rated as high quality, 4 to 7 as moderate quality, and below 4 as low quality. For this meta-analysis, only studies with a score of 4 or higher were included (43). For cohort and case-control studies, the NOS was used, which evaluated studies on three criteria: selection (up to 4 stars), comparability (up to 2 stars), and outcome/exposure ascertainment (up to 3 stars). The NOS scores ranged from 0 to 9 stars, with 7 to 9 stars indicating high quality, 4 to 6 stars moderate quality, and below 4 stars low quality. This analysis included only studies with at least 4 stars to ensure methodological robustness (44). Two reviewers, XBH and SC, independently assessed each study, with any discrepancies resolved through discussion or consultation with a third reviewer, PY. The quality assessment ensured that only reliable, high-quality studies contributed to the meta-analysis.
To examine the relationship between PIU and suicidal behavior, including SI, SP, and SA, pooled OR with 95% CI were estimated using random-effects models. STATA software (version 16.0) was employed to conduct all statistical analyses. Heterogeneity across the included studies was assessed through the I² statistic and Cochran’s Q test. Significant heterogeneity was considered present when the I² statistic exceeded 50% or when Cochran’s Q test yielded a p-value of less than 0.05, warranting the application of a random-effects model (45). To assess the robustness of the overall results, sensitivity analyses were conducted. Specifically, the meta-analysis was re-evaluated by excluding studies with a high risk of bias and by using alternative statistical models (46). Furthermore, Publication bias was initially assessed through funnel plot analysis (47) and Egger’s test (48). If publication bias was detected, the trim-and-fill method was subsequently applied to adjust for it (49). A p-value of less than 0.05 was considered statistically significant. Subgroup analyses were conducted to explore the association between PIU and SI. These analyses were stratified by age groups, measurement tools, geographical regions, control variables including depression, and gender distribution to investigate potential sources of heterogeneity and identify variations in the strength of association across different subgroups. The fixed-effects model was employed to assess differences between these subgroups. All findings were reported in compliance with PRISMA guidelines, ensuring that the analysis was both transparent and reproducible.
According to the predefined search strategy, we initially identified 1,474 relevant articles. After initial screening with NoteExpress, 522 papers remained. Then, after reviewing titles and abstracts, the number reduced to 55. A comprehensive full-text analysis was done, and eventually 23 articles meeting the predefined inclusion criteria (33, 50–71) were selected. All studies were conducted as cross-sectional research. Longitudinal studies were excluded because they were either unavailable within the scope of the search results or did not meet the specific inclusion criteria. These selected studies covered 353,904 participants. Regarding assessment tools for SI, 16 studies (50–57, 59, 61, 63, 65, 68–71) used specialized and validated instruments for measuring SI. For example, they might include professional scales for measuring the frequency, intensity, and duration of suicidal thoughts. Meanwhile, 7 studies (33, 58, 60, 62, 64, 66, 67) used self-designed tools. These might be custom-developed based on specific research questions and populations. In terms of the assessment of PIU, 7 studies (33, 51, 55–57, 59, 64) adopted the Young Internet Addiction Test by Young et al. (72), which might cover multiple dimensions like internet usage time, frequency, behavior patterns, and dependence degree. Additionally, 5 studies (50, 60, 62, 69, 71) chose the Chen Internet Addiction Scale by Chen et al. (73), which might focus on aspects such as loss of control, interference with daily life, and withdrawal reactions. Furthermore, 3 studies (66, 68, 70) used the Mobile Phone Addiction Index translated into Chinese by Liu et al. (74), concentrating on evaluating addiction degree, impact on social and daily life, etc. The remaining 8 studies (52–54, 58, 61, 63, 65, 67) adopted other assessment tools based on specific scenarios and requirements. The sample sizes of the included studies varied significantly. The smallest had 439 participants, while the largest covered 136,266. As detailed in the Supplementary Materials, we conducted a very detailed quality assessment. 18 studies were classified as high-quality for excellent performance in research design, methods, data quality, and result reliability. Another 5 met certain standards in various aspects and were categorized as medium-quality. Table 1 summarizes the main characteristics of these literatures, and Figure 1 outlines each inclusion stage.
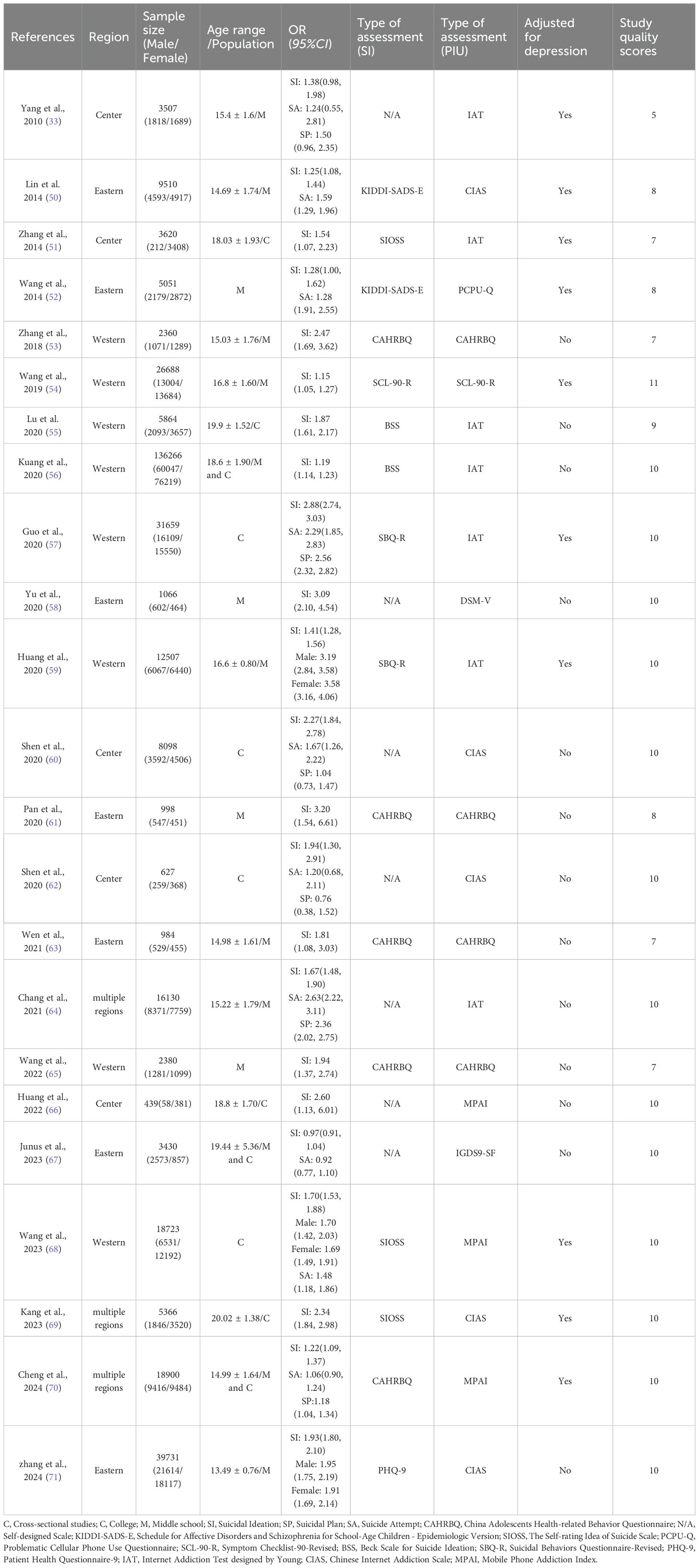
Table 1. Characteristics of the included article.
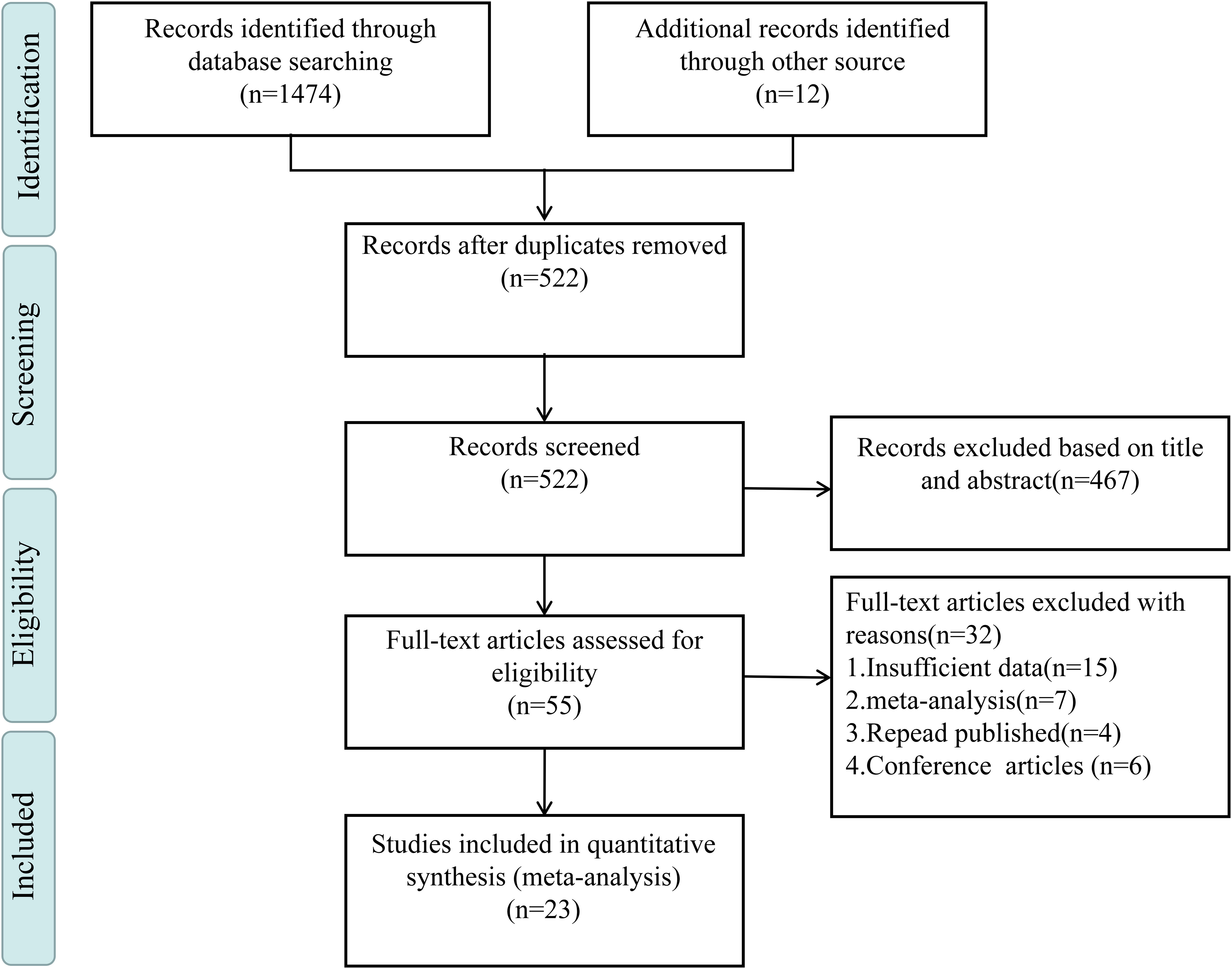
Figure 1. Literature selection process.
A homogeneity test conducted on the 23 studies included in this analysis indicated substantial heterogeneity (I² = 97.8%, P < 0.001). Given this considerable level of heterogeneity, a random-effects model was utilized to estimate the overall effect. The model produced a pooled effect size of (OR = 1.72, 95% CI: 1.45, 2.03), suggesting that individuals with PIU were 1.72 times more likely to experience SI compared to those without PIU. This association was found to be statistically significant (Z = 6.33, P < 0.001), as shown in Figure 2.
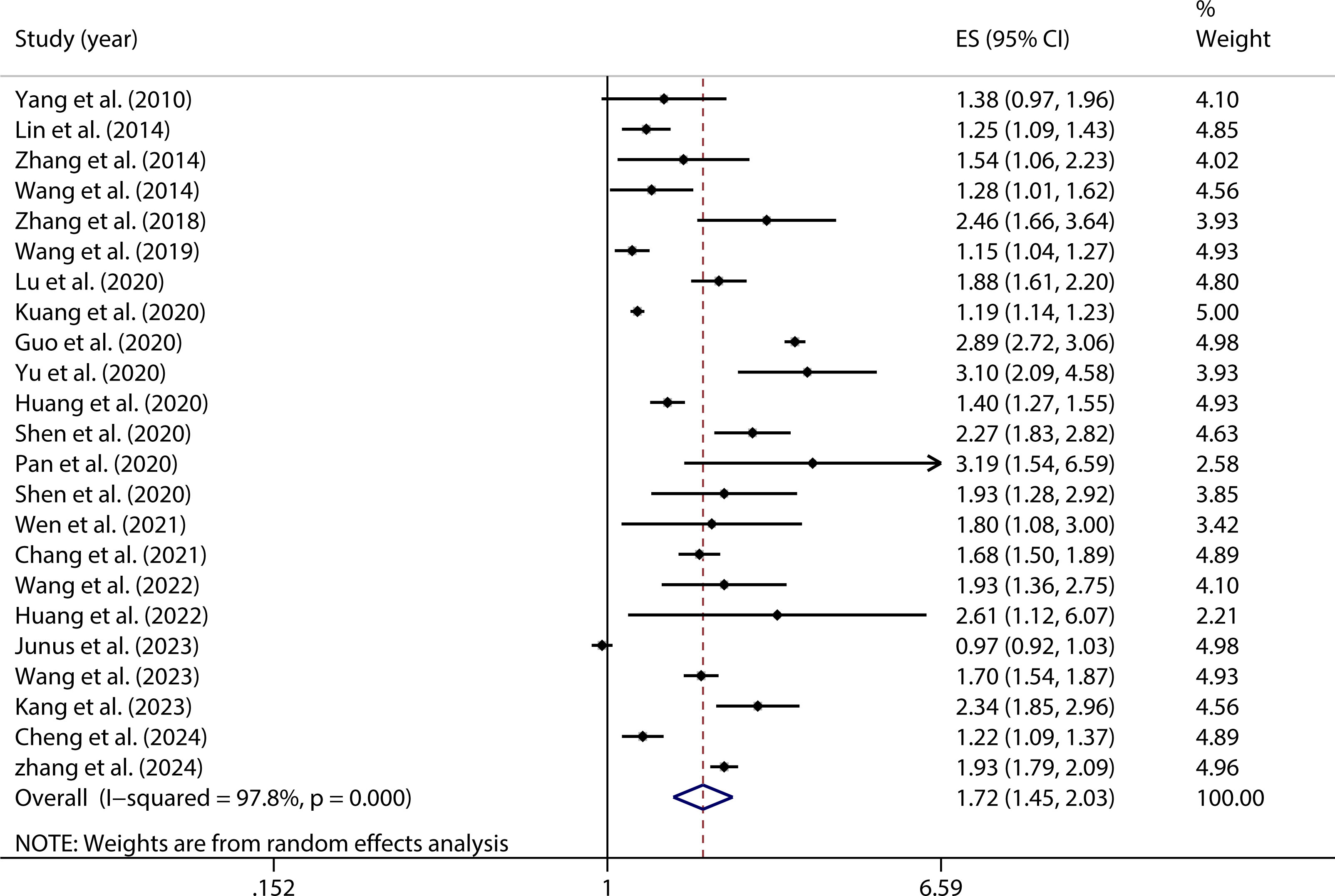
Figure 2. Forest plot of the relationship between PIU and SI.
During the analysis, significant heterogeneity was uncovered through the application of the random-effects model among the studies included in the Meta-analysis. This heterogeneity, which indicated substantial variability in the results across different studies, was recognized as a challenge to the consistency and interpretability of the overall findings. Given the potential impact of this variability on the accuracy of the Meta-analysis, it was deemed essential that additional analyses be undertaken to better understand and address the sources of this heterogeneity. In response, a subgroup analysis was performed, wherein the studies were divided into distinct categories based on specific predefined characteristics, such as population demographics. By isolating and evaluating the factors contributing to the observed heterogeneity, this approach allowed for a more nuanced interpretation of the data. The results of the subgroup analysis provided deeper insights into the variability among studies, thereby enhancing the robustness and validity of the overall conclusions drawn from the Meta-analysis.
A subgroup analysis was undertaken to explore various elements linked to both PIU and SI. These elements included geographical region, age, gender, the specific instruments utilized to assess PIU and SI, as well as the consideration of depression adjustments, as presented in Table 2.
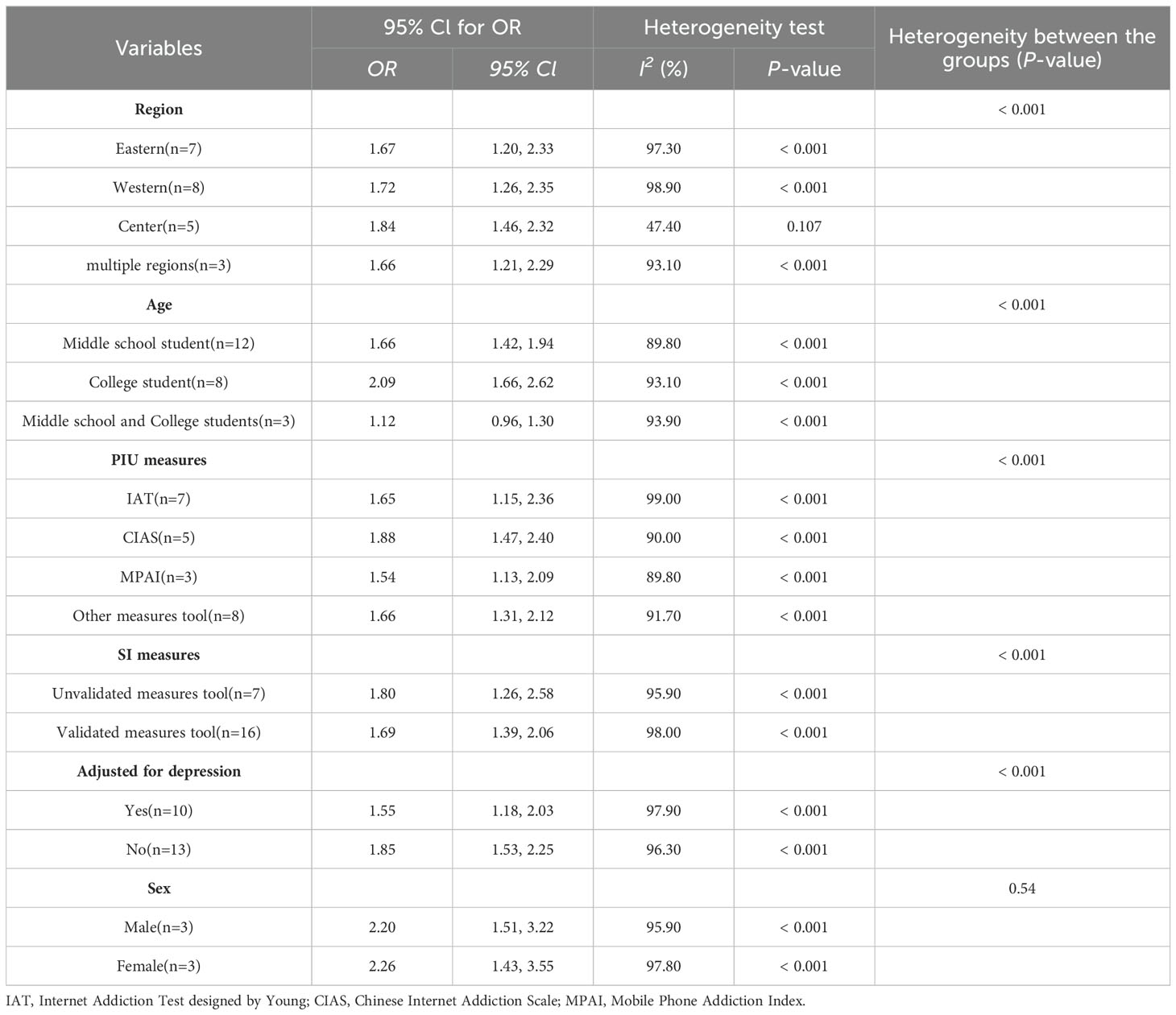
Table 2. Subgroup analysis showing OR of SI for PIU.
As shown in Figure 3, substantial regional differences were identified as moderators in the association between PIU and SI, as outlined in Table 2. Adolescents from the Central region exhibited the highest vulnerability to PIU in the context of SI (OR = 1.84, 95% CI: 1.46, 2.32). On the other hand, those from the Eastern region displayed a significantly lower risk of SI (OR = 1.67, 95% CI: 1.20, 2.33).
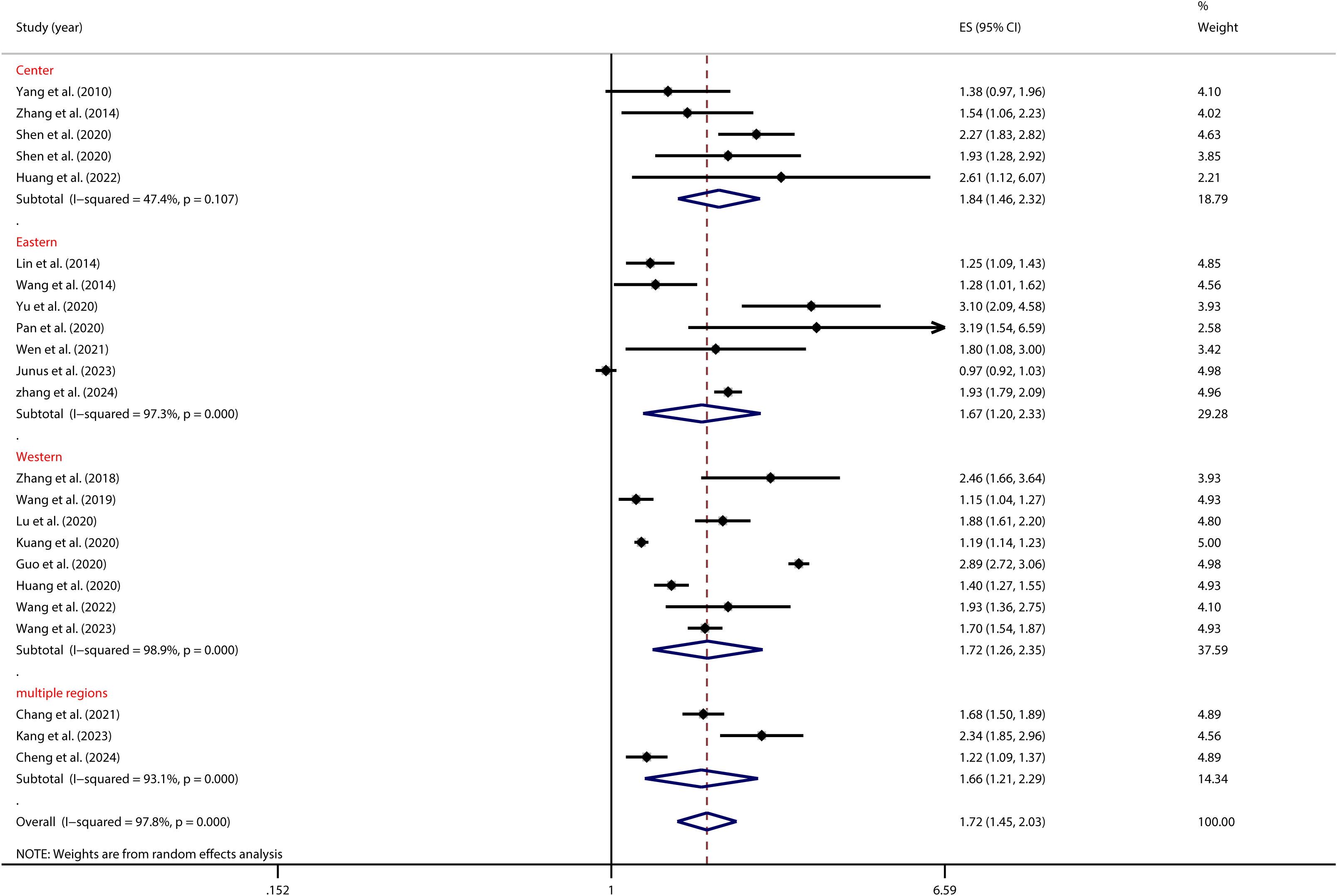
Figure 3. Moderation effect of regional differences on PIU and SI.
As depicted in Figure 4, age significantly influenced the relationship between PIU and SI, as shown in Table 2. Specifically, Chinese college students with PIU had a higher risk of SI (OR = 2.09, 95% CI: 1.66, 2.62) than middle school students (OR = 1.66, 95% CI: 1.42, 1.94).
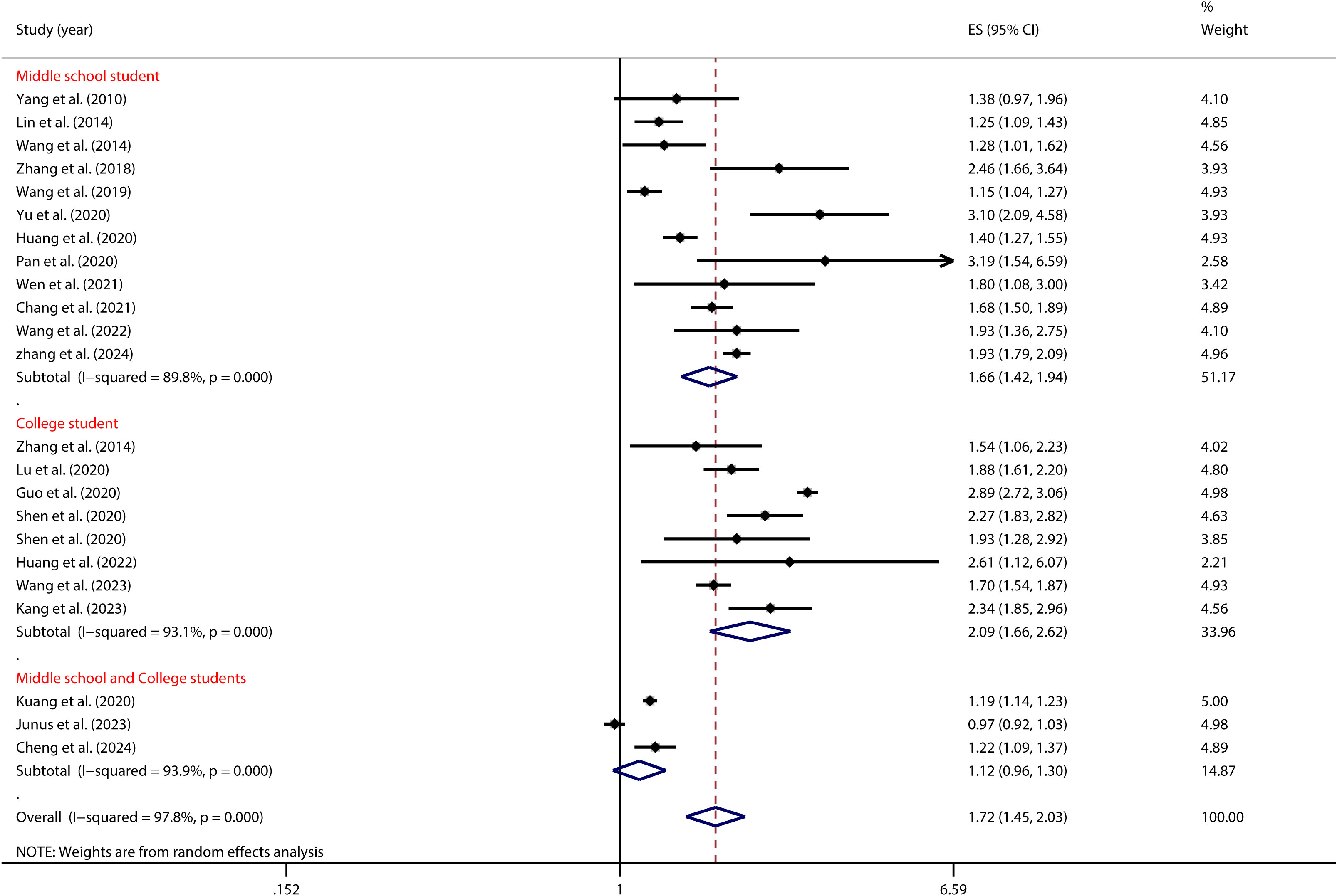
Figure 4. Moderation effect of age on PIU and SI.
As illustrated in Figure 5, the tool used to measure PIU significantly moderated the relationship between adolescent PIU and SI (see Table 2). Specifically, adolescents with mobile phone addiction exhibited a lower risk of SI when assessed using the MPAS (OR = 1.54, 95% CI: 1.13, 2.09) compared to those evaluated with the CIAS (OR = 1.88, 95% CI: 1.47, 2.40). Likewise, Figure 6 illustrates that the tool used to measure SI significantly moderated the relationship between adolescent PIU and SI (see Table 2). The results indicated that among adolescents with PIU, the use of a validated SI measurement tool (OR = 1.69, 95% CI: 1.39, 2.06) yielded a lower risk compared to an unvalidated tool (OR = 1.80, 95% CI: 1.26, 2.58).
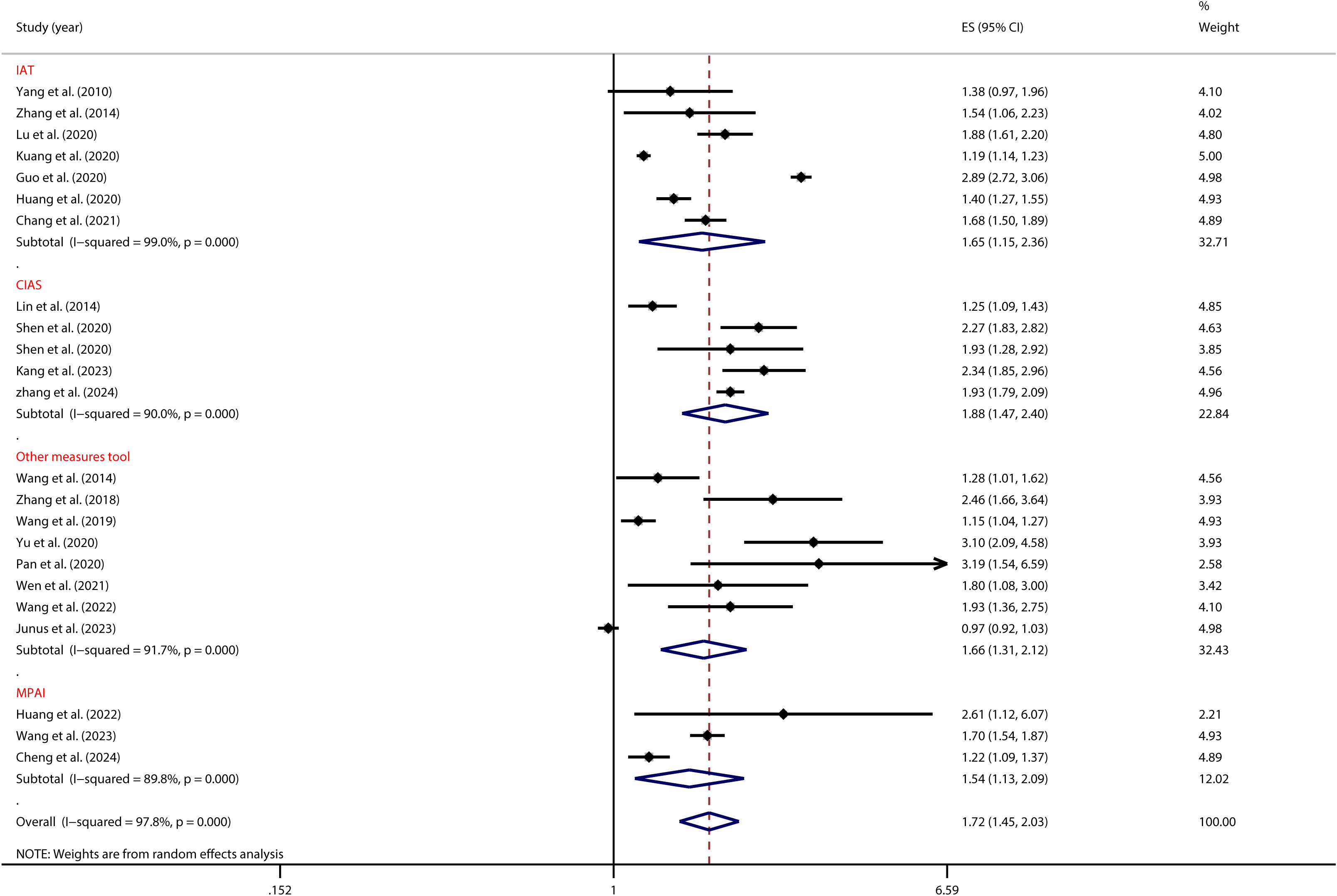
Figure 5. Moderation effect of PIU measures on PIU and SI.
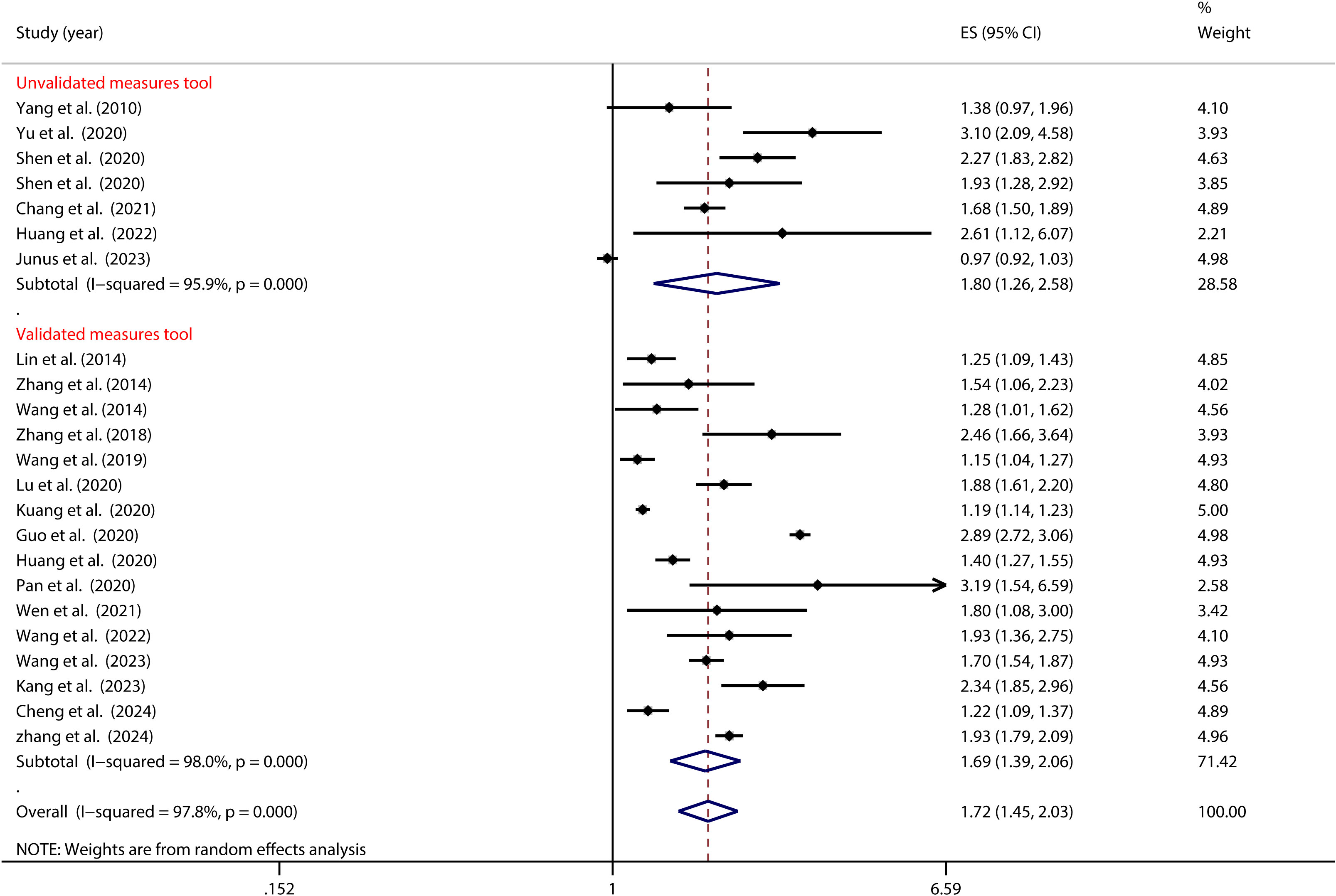
Figure 6. Moderation effect of SI measures on PIU and SI.
Furthermore, as illustrated in Figure 7, the control of depression significantly moderated the association between PIU and SI (as detailed in Table 2). Notably, among Chinese adolescents, the risk of SI was highest when depression was not managed (OR = 1.85, 95% CI: 1.53, 2.25). In contrast, when depression was effectively managed, the risk substantially decreased (OR = 1.55, 95% CI: 1.18, 2.03).
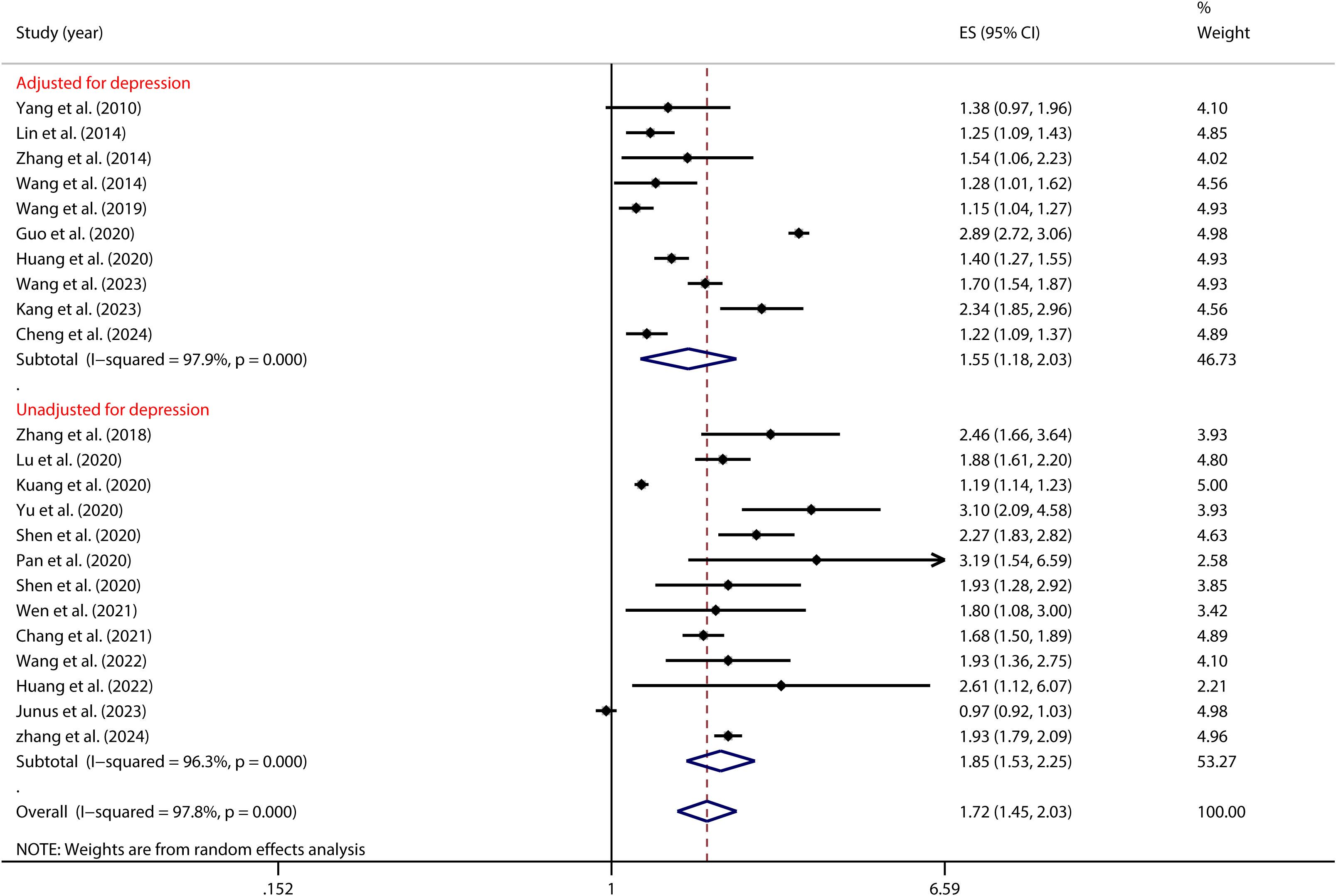
Figure 7. Moderation effect of depression control on PIU and SI.
A homogeneity test conducted on 6 independent samples examining the link between PIU and SP revealed significant heterogeneity across the studies (I² = 96.0%, p < 0.001). Given this high level of variability, a random-effects model was employed to estimate the overall effect. The model produced a pooled effect size of OR = (1.50, 95% CI: 1.02, 2.20), indicating that individuals with PIU were 1.50 times more likely to engage in suicidal planning compared to those without PIU. This association was statistically significant (Z = 2.08, P = 0.037) (see Figure 8).
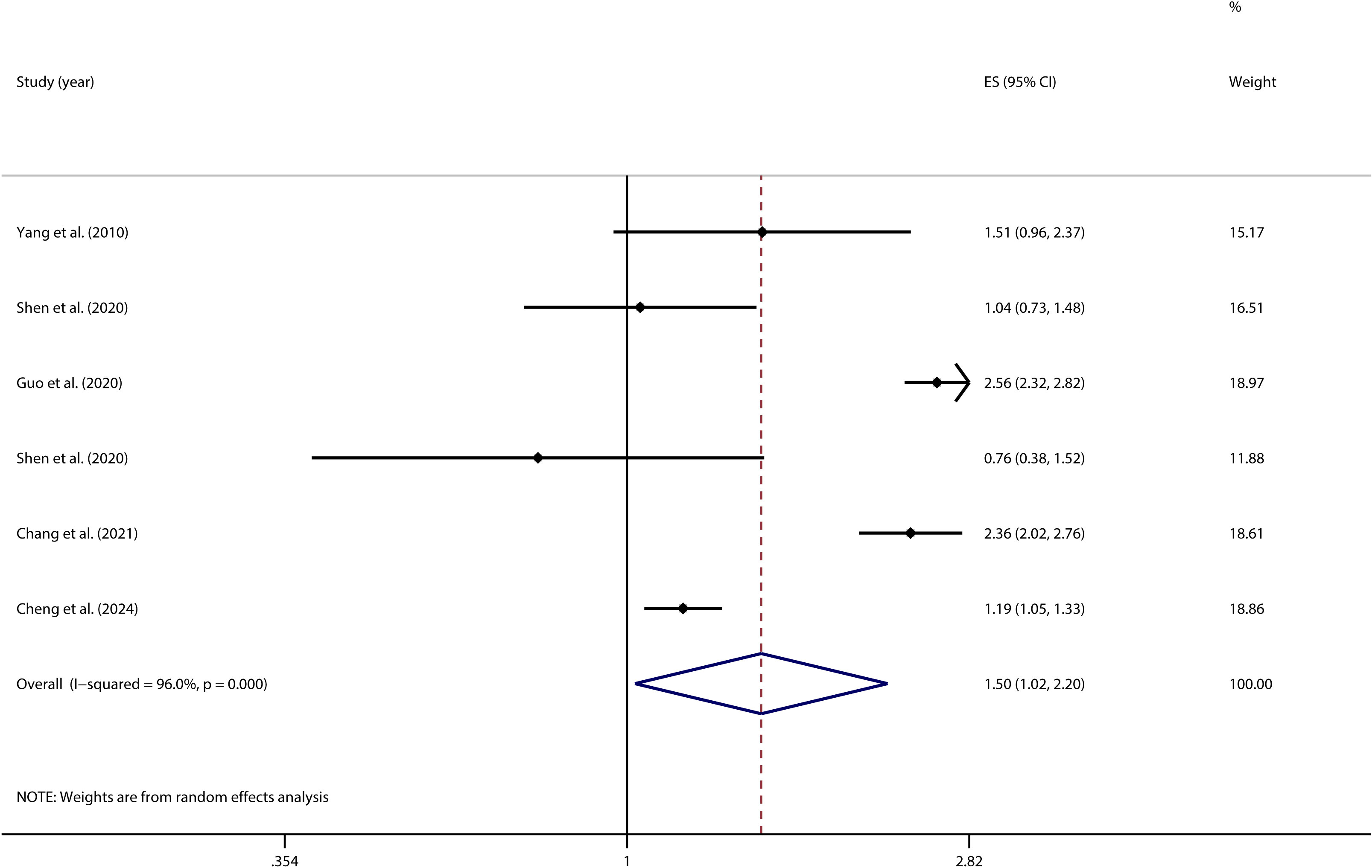
Figure 8. Forest plot of the relationship between PIU and SP.
A homogeneity test conducted on 10 independent samples examining the link between PIU and SA indicated substantial heterogeneity across the studies (I² = 91.6%; p < 0.001). Given this considerable level of heterogeneity, a random-effects model was utilized to provide a more accurate estimation of the overall effect. The model produced a pooled effect size of OR = 1.48 (95% CI: 1.16, 1.89), indicating that individuals with PIU were 1.48 times more likely to attempt suicide compared to those without PIU. This association was statistically significant (Z = 3.20, P = 0.001) (see Figure 9).
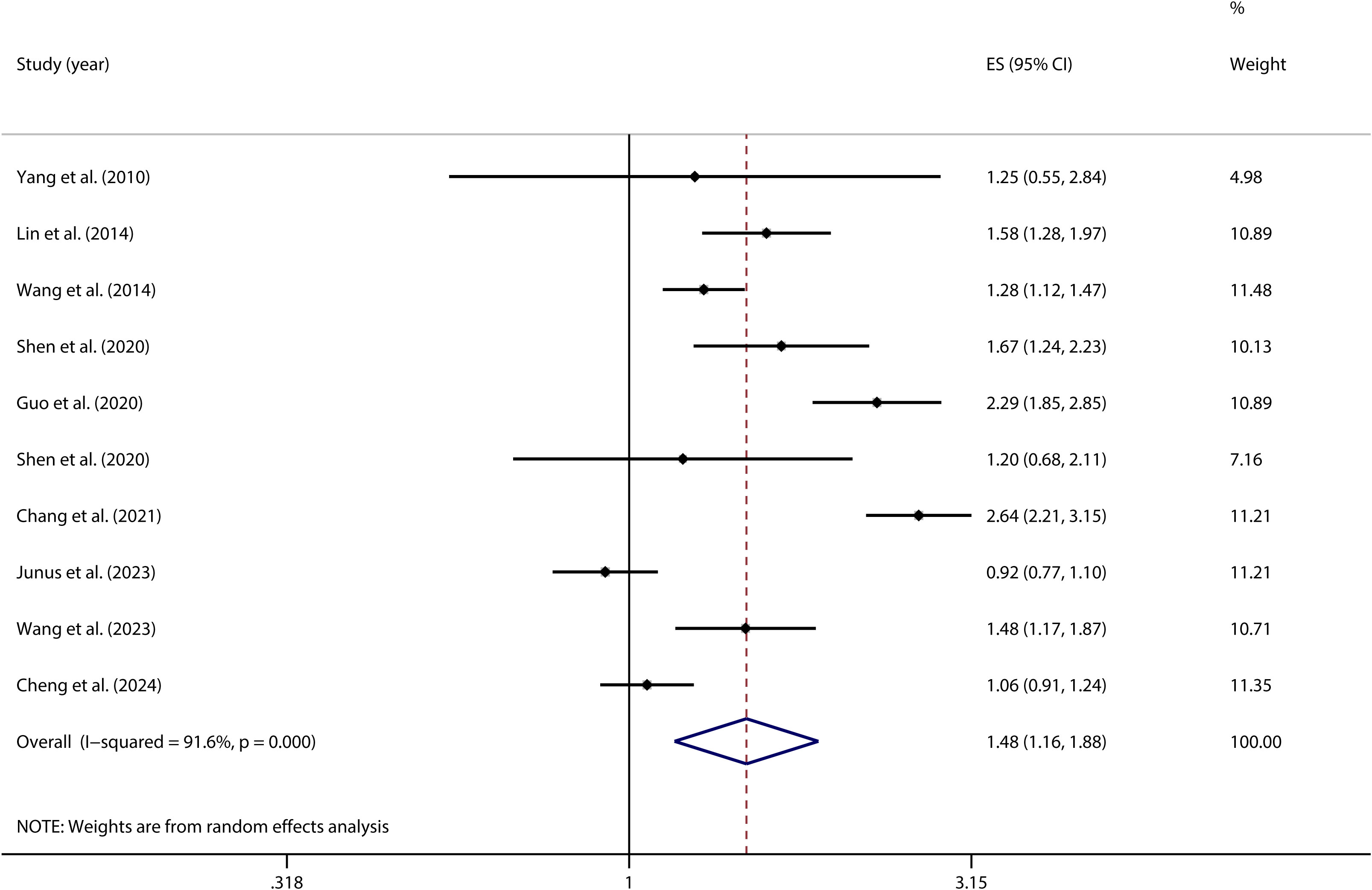
Figure 9. Forest plot of the relationship between PIU and SA.
To evaluate the robustness of the research findings, sensitivity analyses were conducted on the correlations between PIU and SI (see Figure 10), SP (see Supplementary Materials), and SA (see Supplementary Materials). The results indicated that the overall correlation coefficients exhibited only minor variations, thereby highlighting the stability and reliability of these findings.
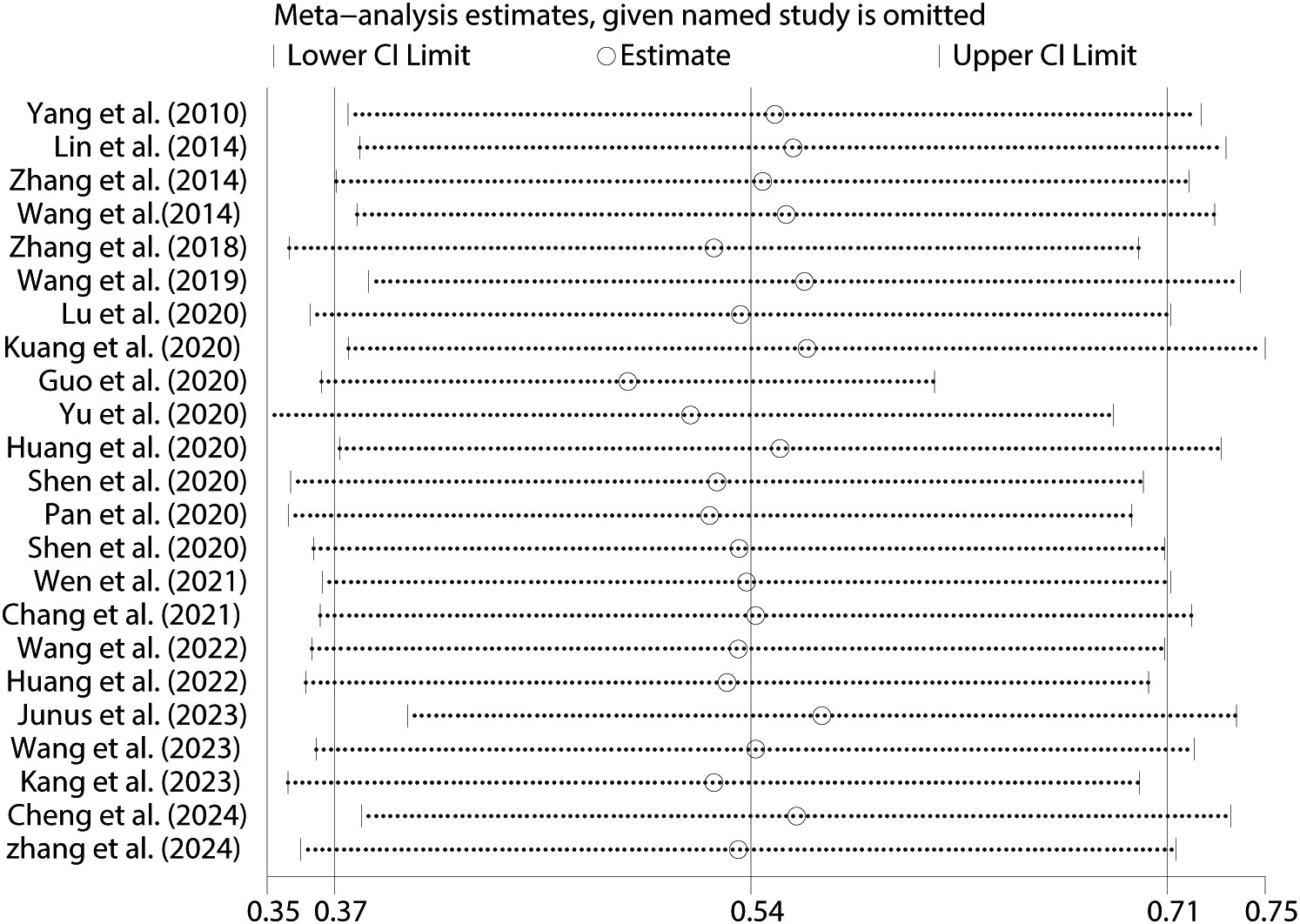
Figure 10. Sensitivity analysis between PIU and SI.
The correlations between PIU and SI (Figure 11), SP (see Supplementary Materials), and SA (see Supplementary Materials) were evaluated using funnel plots. The plots demonstrated a balanced distribution on both sides. Additionally, Egger’s regression tests were conducted for PIU and SI (t = 1.12, p = 0.95) (Figure 12), SP (t = 0.37, p = 0.72) (see Supplementary Materials), and SA (t = 0.83, p = 0.45) (see Supplementary Materials). None of these tests revealed statistically significant differences, further indicating that no substantial publication bias was present.
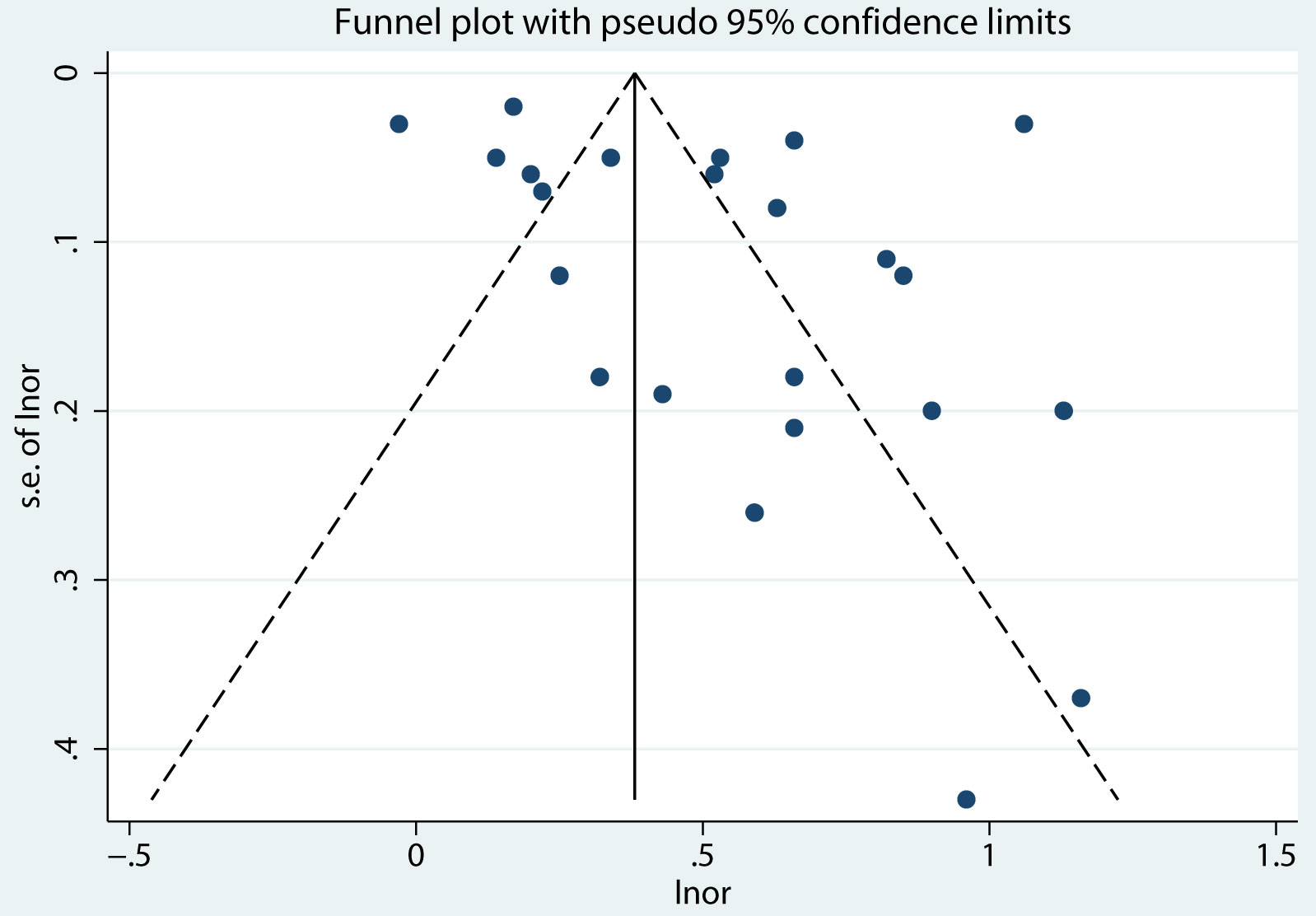
Figure 11. Funnel plot between PIU and SI.
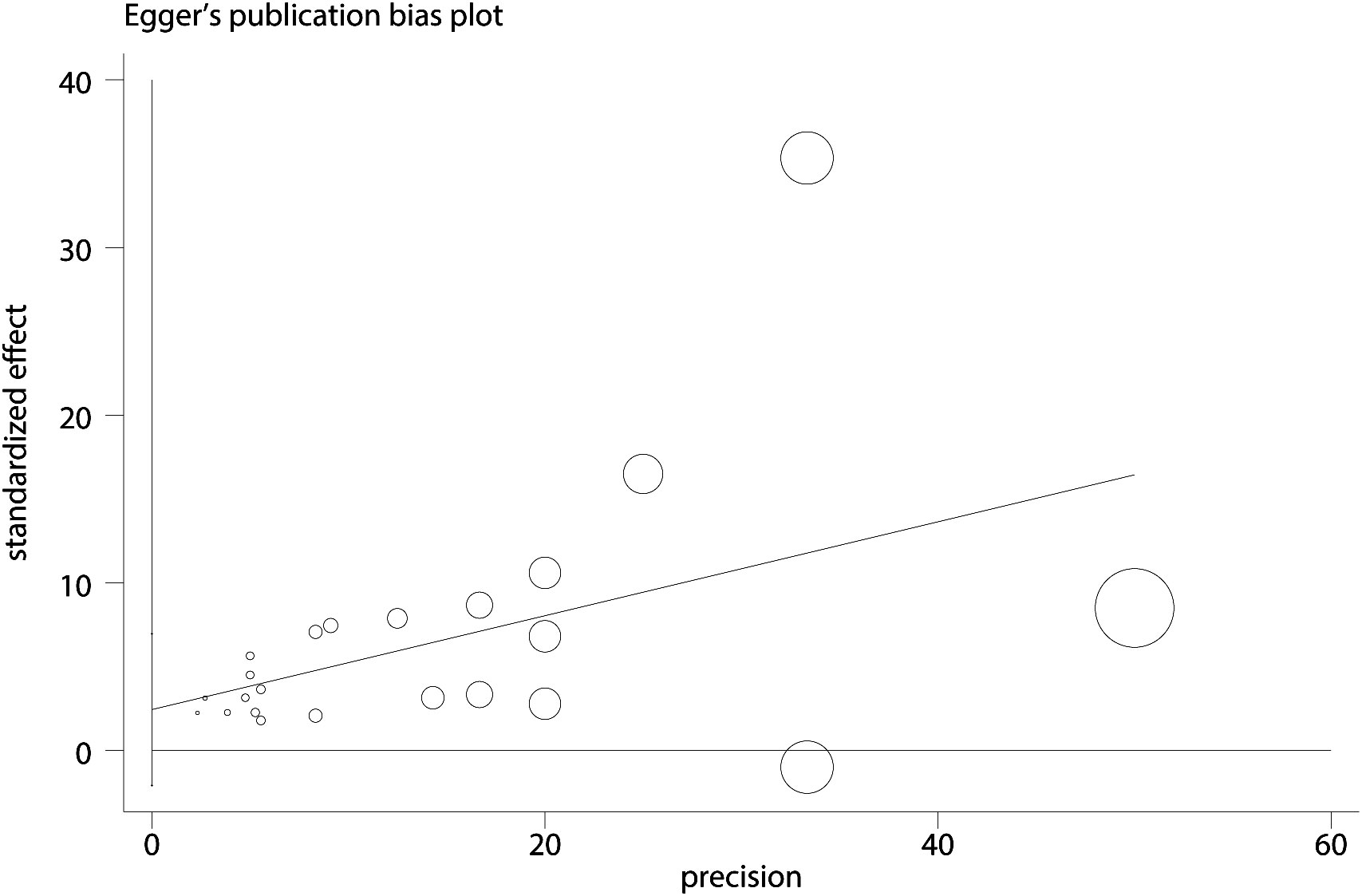
Figure 12. Egger plot between PIU and SI.
In recent years, adolescent suicidal behavior has become a global public health challenge (75). Meanwhile, PIU has drawn more attention as a factor for adolescent problem behaviors (76). Despite research, a clear consensus on the relationship between PIU and suicidal behavior has remained elusive (77). This meta-analysis suggested that Chinese adolescents with PIU had 1.72 times higher odds of having SI, 1.50 times higher odds of experiencing SP, and 1.48 times higher odds of engaging in SA. In contrast, another meta-analysis covering multiple countries in Europe and Asia found that the risks of SI, SP, and SA increased by 2.95 times, 3.17 times, and 2.81 times, respectively (38). This suggested that the risk of suicidal behavior due to PIU among Chinese adolescents might have been relatively lower. The difference could be attributed to the influence of different cultures, environments, and mechanisms. Nevertheless, the association between PIU and suicidal behavior among Chinese adolescents was found to be consistent with Wang et al.’s conclusion (39). This phenomenon could be attributed to: Firstly, a complex interaction was likely to exist between PIU and suicidal behavior, in which the internet served as a platform exposing adolescents to suicide-related information and peers, thereby increasing the risk of imitation and participation in suicidal behaviors (78). This risk was further amplified in the anonymous online environment, where adolescents could explore suicidal thoughts without fear of judgment and obtain related information through pro-suicide websites (79). Anonymity not only potentially led to deindividuation, reducing self-awareness, but also heightened sensitivity to self-harm (50, 80). Furthermore, adolescence was a critical period for identity formation, during which adolescents might have found online groups with similar mindsets. These groups might have sought validation by encouraging suicidal behaviors, further alienating individuals from mainstream culture (50, 81). Particularly for those vulnerable to social rejection and harm, PIU might have become an unhealthy coping mechanism, exposing them to additional online risks, such as the dissemination of pornographic content and cyberbullying, thereby exacerbating feelings of isolation and psychological stress (35, 82, 83). This process was further intensified by social reinforcement mechanisms, significantly increasing the risk of suicidal behavior. Secondly, PIU was identified as addictive. According to the I-PACE model, addictive behaviors were understood to result from complex interactions among vulnerability factors, emotional and cognitive responses, and executive functions (84–86). Prolonged PIU might have caused changes in the brain structure and function of adolescents, especially in regions related to executive control and decision-making. For instance, excessive use was observed to lead to a decline in prefrontal cortex function, affecting judgment and decision-making, thereby increasing suicide risk (87–89). Moreover, PIU might have led to neuroadaptive changes, distorting the perception of rewards and punishments, and increasing the propensity for suicidal behavior (90, 91). This interacted with the social isolation caused by PIU, weakening the ability to cope with emotions, and prompting the transformation of internal distress into external experiences, ultimately triggering suicidal behavior (92, 93). Additionally, PIU was noted to cause depersonalization, damage social functions, and lead to impulse control disorders, thereby increasing the incidence of suicidal behavior (94). Finally, a strong correlation was observed between PIU and mental health issues such as anxiety and depression, both of which have been identified as significant predictors of suicide. While PIU may have initially served as a coping strategy, its prolonged use could have worsened these mental health problems, ultimately elevating the risk of suicide (95). In summary, PIU was determined to have a direct impact on adolescent mental health, contributing to an increased suicide risk through intricate interaction processes.
The findings of this study revealed a significant moderating effect of regional differences on the relationship between PIU and SI among adolescents. Specifically, adolescents in the central and western regions of China with PIU faced a significantly higher risk of SI, whereas those in the eastern regions were at a lower risk. Several potential factors might have contributed to these regional differences. Firstly, economic development in China was uneven, with the eastern regions being more developed compared to the central and western regions. This economic disparity influenced various aspects of life, including access to resources that could have mitigated the impact of PIU. As a result, adolescents in economically disadvantaged areas might have experienced higher levels of stress due to poverty and limited opportunities, which could have exacerbated the effects of PIU on SI (96). Moreover, the level of urbanization in the eastern regions provided more social and recreational opportunities, potentially reducing the negative impact of PIU. Additionally, social support systems varied across regions, with the eastern regions potentially offering stronger and more diverse networks that could have helped adolescents cope with the challenges associated with PIU. In contrast, weaker social support structures in the central and western regions might have led to greater isolation and increased vulnerability to SI among adolescents with PIU (97, 98). Furthermore, cultural attitudes towards mental health might have differed, with more traditional views in the less-developed regions possibly leading to stigmatization and reduced help-seeking behavior (99). Educational disparities also played a significant role. It is likely that the eastern regions had better mental health education and awareness programs, which could have helped adolescents and their families recognize and address PIU early on. Conversely, lower levels of mental health education in the central and western regions might have contributed to a lack of awareness about the dangers of PIU, thereby increasing the risk of severe outcomes like SI (100, 101). Lastly, higher digital literacy in the eastern regions may have equipped adolescents with better coping strategies for managing internet use, thereby reducing the likelihood of PIU.
Moreover, the analysis demonstrated a notable moderating effect of age on the PIU-SI association, revealing that university students were more vulnerable to SI than middle school students when afflicted by PIU. Several key factors may explain the significant age moderation in the PIU-SI relationship. Firstly, developmental differences between university students and middle school students were considered pivotal. University students, being at a more advanced stage of psychological development, faced heightened levels of academic pressure, career uncertainty, and the challenges associated with independent living (102, 103). These factors were likely to exacerbate the effects of PIU, thereby increasing the risk of SI. In contrast, middle school students were generally in more protected environments, characterized by lower social pressures and less psychological maturity, which may have buffered them against the severe consequences of PIU. Secondly, there was a distinct difference in how these age groups engaged with social networks and experienced loneliness. University students were more inclined to rely on virtual social interactions, which could have intensified feelings of loneliness and isolation—both strongly correlated with SI. Conversely, middle school students typically maintained more in-person social interactions, which may have mitigated the psychological impact of PIU (83). Lastly, the availability and accessibility of mental health services differed significantly between these age groups. University students, often residing away from home, might have experienced limited access to support systems, thereby worsening the mental health issues associated with PIU. On the other hand, middle school students generally had more immediate access to parental and school-based support, which could have mitigated the risk of SI (104). These findings underscored the importance of developing age-specific intervention strategies. Educational institutions played a crucial role in implementing programs tailored to the distinct challenges faced by different age groups. Specifically, school-based interventions for middle school students and college wellness initiatives might have proven particularly effective in addressing the unique challenges these populations encountered in managing internet use and mitigating its potential harms.
Furthermore, this study revealed that controlling for depression significantly moderated the relationship between PIU and SI. This finding suggested that the elevated risk of SI among adolescents experiencing PIU could be partially attributed to underlying depressive symptoms, although other variables also played critical roles. This result was consistent with the findings of Wang et al. (52), who noted that depressive symptoms intensified the negative effects associated with PIU. A plausible explanation for this phenomenon was the close association between depressive disorders and PIU. Adolescents suffering from depression might have resorted to excessive internet use as a means of escaping psychological distress. However, such reliance on the internet often escalated into PIU, which, in turn, could have exacerbated depressive symptoms, creating a self-perpetuating cycle that amplified the risk of SI (28, 105). Moreover, adolescents with depression frequently experienced severe social isolation and a lack of effective coping strategies, which further increased their susceptibility to excessive internet use. While engaging with the online environment might have provided temporary relief, it often led to deeper psychological issues, thereby raising the likelihood of SI (106, 107). Given the complexities involved, it was deemed essential that the risk of SI in adolescents with PIU be assessed, irrespective of the presence of depression. Thus, a multifaceted approach—including comprehensive mental health evaluations, early identification of risk factors, and tailored interventions—was considered crucial for reducing the risk of SI in this vulnerable population.
In addition, the type of measurement tool used to assess SI was found to moderate the relationship between PIU and SI. Specifically, the correlation between PIU and SI was observed to be lower when SI was measured using validated tools compared to unvalidated ones. This finding can be plausibly explained by differences in the validity of the measurement instruments. Validated tools have undergone rigorous validation processes, ensuring higher reliability and validity, which allows for a more accurate assessment of SI. In contrast, unvalidated tools may have introduced measurement errors or biases, potentially inflating the observed correlations between PIU and SI (108). Consequently, when validated tools were employed, the positive correlation between PIU and SI was more likely to reflect the true relationship, rather than being exaggerated by the limitations of the measurement tool. Additionally, validated measures were often better designed to reduce social desirability bias in participants’ responses to SI-related questions. For instance, validated tools may have assessed SI more discreetly, thereby reducing the likelihood of participants concealing their true thoughts, which could have contributed to the observed weaker correlation when these tools were used (109).
Similarly, the type of measurement tool used to assess PIU was found to significantly moderate the relationship between PIU and SI. When tools designed to measure mobile phone addiction were employed, the correlation between PIU and SI was comparatively weaker, suggesting that the risk of SI among Chinese adolescents addicted to mobile phones may have been lower than that associated with other forms of internet addiction. Several plausible explanations can account for this observation: To begin with, the nature of mobile phone addiction, which typically involves excessive engagement in social media, instant messaging, and recreational activities, might have provided adolescents with social support and emotional regulation, potentially mitigating the onset of SI (110). In contrast, other forms of internet addiction, such as online gambling or pornography, were likely to result in greater psychological distress and isolation, thereby heightening the risk of SI. Moreover, cultural factors were considered to play a significant role; within the Chinese context, mobile phone use for social interaction and entertainment was widely accepted as a normal aspect of adolescent life. This acceptance might have reduced the negative psychological consequences of excessive use, thereby lowering the risk of SI (111). Lastly, mobile phone addiction may have served as a functional coping strategy for adolescents to escape real-life problems, such as academic pressure or family conflicts. While not a healthy coping mechanism, it might have temporarily diminished the likelihood of developing SI (112–114). Additionally, the specificity of mobile phone addiction measurement tools, which tended to focus on the frequency and duration of use rather than on deeper psychological distress, could have led to an underestimation of the correlation between PIU and SI (115). These considerations suggest that mobile phone addiction among Chinese adolescents may have been associated with a lower risk of SI compared to other types of internet addiction.
Nevertheless, the study results indicated that the relationship between PIU and SI was not significantly moderated by gender. This finding suggested that the impact of PIU on SI remained generally consistent across both males and females. This phenomenon could be attributed to two primary factors: On the one hand, it is plausible that PIU exerted broad and consistent negative effects on mental health that transcended gender differences. Irrespective of gender, excessive or unhealthy internet use could have led to social isolation, sleep disturbances, and emotional instability, all of which might have increased the risk of SI (103, 116, 117). On the other hand, it should be acknowledged that the subgroup analysis in this study included only three articles, which might have limited the generalizability of the findings and the ability to detect a gender moderation effect.
By systematically reviewing studies, this analysis investigated the PIU-suicidal behavior connection in Chinese adolescents. The use of large, varied samples strengthened the conclusions’ reliability. The findings may inform new prevention and management strategies, establishing a solid basis for future interventions.
Nevertheless, certain limitations should be recognized. First, the inclusion of only cross-sectional observational studies meant that the results reflected a correlation between PIU and suicidal behavior, without establishing causality. At the same time, the ongoing debate in the literature regarding the directionality (or bidirectionality) of the relationship between PIU and suicidal behavior was acknowledged, and the incorporation of longitudinal designs in future studies was identified as essential for better understanding these temporal dynamics and causal pathways. Secondly, the significant effects were observed in only a limited number of moderating variables, leaving much of the heterogeneity unaddressed. This limitation indicated that other potential moderating factors influencing the relationship between PIU and suicidal behavior were likely overlooked in the current analysis. Consequently, the full complexity of this relationship may not have been fully captured. It was recommended that future meta-analyses expand their scope to include a wider range of moderating variables, which could lead to a more comprehensive understanding of the factors contributing to variability in outcomes and clarify under which conditions PIU is most strongly associated with suicidal behavior. Thirdly, our analysis was constrained to studies published in Chinese and English, thereby excluding unpublished works, which may have introduced publication bias. Furthermore, by focusing exclusively on Chinese adolescents, the research scope is inherently limited, which restricts the applicability of the findings to broader populations. The exclusion of other age groups, such as children, adults, or elderly individuals, means that the results may not be generalizable beyond the specific demographic studied. Consequently, the insights gained from this research may not fully capture the complexities of PIU and suicidal behavior in different age groups, potentially overlooking important age-related differences that could influence the relationship between these variables. In addition, the reliance on self-report questionnaires across all studies, as opposed to clinical assessments, could have influenced the robustness of the findings. Lastly, a limitation of this study is that subgroup analysis was conducted solely on the relationship between adolescent PIU and SI. This leaves the connections between PIU and SP, as well as SA, underexplored. Future research should conduct subgroup analyses on the relationships between adolescent PIU and SP, as well as SA, to provide a more comprehensive understanding of PIU’s impact on different types of suicidal behavior. Such refined analyses would enable researchers to more accurately identify the underlying mechanisms of various suicidal behaviors, thereby offering stronger evidence for prevention and intervention strategies.
This study systematically reviewed the relationship between PIU and suicidal behavior among Chinese adolescents. A significant positive correlation between PIU and suicidal behavior was revealed, suggesting that PIU might have been a critical risk factor contributing to suicidal behavior in this population. The findings underscored the substantial impact of internet use on adolescent mental health, with a particular emphasis on the increased risk of SI among adolescents in China’s central and western regions, university students, and those suffering from depressive disorders. These groups were found to face more complex psychological and social pressures, which may have intensified the association between PIU and suicidal behavior. By focusing on these vulnerable groups and their distinct challenges, this study offers valuable insights into tailoring preventive strategies to different contexts and regions, thereby enhancing the effectiveness of interventions. Therefore, it was deemed imperative to implement targeted preventive interventions for these high-risk groups.
Based on these findings, it was recommended that mental health education and interventions for adolescents be strengthened. This should have included the widespread dissemination of mental health knowledge at the secondary and tertiary education levels, focusing on enhancing adolescents’ ability to manage stress and regulate emotions, as well as the establishment of early identification and intervention mechanisms to provide timely psychological support. Secondly, it was suggested that regulations and management of internet use be improved to promote healthy internet habits, particularly among adolescents in the central and western regions and university students, to mitigate the negative psychological impacts of problematic internet use. For high-risk groups, such as those with depressive disorders, specific psychological support and interventions, including behavioral correction, psychotherapy, and family support, were recommended. The relevance of these findings lies in their potential to guide policy-makers and practitioners in designing targeted interventions for populations at higher risk of PIU and suicide, contributing to long-term improvements in adolescent mental health. At the same time, it was recommended that the government introduce relevant policies to support the promotion of mental health education and internet use regulations, especially in resource-constrained areas like central and western China. Furthermore, it was suggested that cooperation among families, schools, and society be enhanced to support healthy internet use and mental health among adolescents. Finally, the establishment of a long-term monitoring mechanism was recommended to continuously track the relationship between PIU and adolescent mental health, providing scientific evidence for policy-making and intervention strategies. The relevance of this study lies in its contribution to addressing a critical public health issue by identifying high-risk groups and proposing specific, evidence-based intervention strategies that can inform mental health policy and practice in China.
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author.
XH: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Software, Supervision, Validation, Writing – original draft, Writing – review & editing. SC: Data curation, Methodology, Writing – original draft. QY: Conceptualization, Writing – original draft. PY: Formal analysis, Methodology, Supervision, Writing – review & editing. BY: Funding acquisition, Project administration, Resources, Supervision, Writing – review & editing.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
We extend our sincere thanks to all the individuals and researchers who contributed to this project.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2024.1484809/full#supplementary-material
1. World Health Organization. Suicide worldwide in 2019. (2021). Available online at: https://www.who.int/publications/i/item/9789240026643 (Accessed June 16, 2021).
2. Foreman KJ, Marquez N, Dolgert A, Fukutaki K, Fullman N, McGaughey M, et al. Forecasting life expectancy, years of life lost, and all-cause and cause-specific mortality for 250 causes of death: reference and alternative scenarios for 2016–40 for 195 countries and territories. Lancet. (2018) 392:2052–90. doi: 10.1016/S0140-6736(18)31694-5
3. World Health Organization. World health statistics 2021: monitoring health for the SDGs, sustainable development goals (2021). Available online at: https://www.who.int/publications/i/item/9789240027053 (Accessed December 17, 2021).
4. World Health Organization. More than 1.2 million adolescents die every year, nearly all preventable (2017). Available online at: https://www.who.int/news/item/16-05-2017-more-than-1-2-million-adolescents-die-every-year-nearly-all-preventable (Accessed May 16, 2017).
5. National Health Commission of the People’s Republic of China. China health care statistics yearbook in 2021. Beijing: Peking Union Medical College Press (2021). p. 245.
6. Qu G, Shu L, Zhang J, Wu Y, Ma S, Han T, et al. Suicide ideation, suicide plan, and suicide attempt among left-behind children and adolescents: a systematic review and meta-analysis. Suicide Life-Threat. (2021) 51:515–27. doi: 10.1111/sltb.12731
7. Hawton K, Hill N, Gould M, John A, Lascelles K, Robinson J. Clustering of suicides in children and adolescents. Lancet Child Adolesc. (2020) 4:58–67. doi: 10.1016/S2352-4642(19)30335-9
8. Berman AL. Estimating the population of survivors of suicide: seeking an evidence base. Suicide Life-Threat. (2011) 41:110–6. doi: 10.1111/j.1943-278X.2010.00009.x
9. Pitman A, Osborn D, King M, Erlangsen A. Effects of suicide bereavement on mental health and suicide risk. Lancet Psychiat. (2014) 1:86–94. doi: 10.1016/S2215-0366(14)70224-X
10. World Health Organization. Preventing suicide: a global imperative (2014). Available online at: https://www.who.int/publications/i/item/9789241564779 (Accessed August 17, 2014).
11. Turecki G, Brent DA. Suicide and suicidal behaviour. Lancet. (2016) 387:1227–39. doi: 10.1016/S0140-6736(15)00234-2
12. Large M, Corderoy A, McHugh C. Is suicidal behaviour a stronger predictor of later suicide than suicidal ideation? A systematic review and meta-analysis. Aust Nz J Psychiat. (2021) 55:254–67. doi: 10.1177/0004867420931161
13. Castellví P, Lucas-Romero E, Miranda-Mendizábal A, Parés-Badell O, Almenara J, Alonso I, et al. Longitudinal association between self-injurious thoughts and behaviors and suicidal behavior in adolescents and young adults: a systematic review with meta-analysis. J Affect Disord. (2017) 215:37–48. doi: 10.1016/j.jad.2017.03.035
14. Uddin R, Burton NW, Maple M, Khan SR, Khan A. Suicidal ideation, suicide planning, and suicide attempts among adolescents in 59 low-income and middle-income countries: a population-based study. Lancet Child Adolesc. (2019) 3:223–33. doi: 10.1016/S2352-4642(18)30403-6
15. Chang Q, Shi Y, Yao S, Ban X, Cai Z. Prevalence of suicidal ideation, suicide plans, and suicide attempts among children and adolescents under 18 years of age in mainland China: a systematic review and meta-analysis. Trauma Violence Abus. (2024) 25:2090–102. doi: 10.1177/15248380231205828
16. Statista. Number of internet users worldwide 2024 (2024). Available at: https://www.statista.com/statistics/617136/digital-population-worldwide/ (Accessed May 22, 2024).
17. China Internet Network Information Center. The 53rd statistical report on China internet development (2024). Available online at: https://www.cnnic.net.cn/n4/2024/0322/c88-10964.html (Accessed March 22, 2024).
18. Reyna VF, Farley F. Risk and rationality in adolescent decision making: implications for theory, practice, and public policy. Psychol Sci Publ Int. (2006) 7:1–44. doi: 10.1111/j.1529-1006.2006.00026.x
19. Derevensky JL, Hayman V, Lynette G. Behavioral addictions: excessive gambling, gaming, internet, and smartphone use among children and adolescents. Pediatr Clin N Am. (2019) 66:1163–82. doi: 10.1016/j.pcl.2019.08.008
20. Chao CM, Kao KY, Yu TK. Reactions to problematic internet use among adolescents: inappropriate physical and mental health perspectives. Front Psychol. (2020) 11:1782. doi: 10.3389/fpsyg.2020.01782
21. Spada MM. An overview of problematic internet use. Addict Behav. (2014) 39:3–6. doi: 10.1016/j.addbeh.2013.09.007
22. Jaworska N, MacQueen G. Adolescence as a unique developmental period. J Psychiatr Neurosci. (2015) 40:291–3. doi: 10.1503/jpn.150268
23. Arrivillaga C, Rey L, Extremera N. Adolescents’ problematic internet and smartphone use is related to suicide ideation: does emotional intelligence make a difference? Comput Hum Behav. (2020) 110:106375. doi: 10.1016/j.chb.2020.106375
24. Achangwa C, Ryu HS, Lee JK, Jang JD. Adverse effects of smartphone addiction among university students in South Korea: a systematic review. Healthcare-Basel. (2022) 11:14. doi: 10.3390/healthcare11010014
25. Ferguson GM, Causadias JM, Simenec TS. Acculturation and psychopathology. Annu Rev Clin Psycho. (2023) 19:381–411. doi: 10.1146/annurev-clinpsy-080921-080622
26. Xiong A, Liao S, Luo B, Luo S, Tong Y, Li Z. Associations between problematic internet use, life satisfaction, and deliberate self-harm among chinese adolescents: a multi-centered longitudinal study. Addict Behav. (2023) 147:107808. doi: 10.1016/j.addbeh.2023.107808
27. Herruzo C, Sánchez-Guarnido AJ, Pino MJ, Lucena V, Raya AF, Herruzo FJ. Suicidal behavior and problematic internet use in college students. Psicothema. (2023) 35:77–86. doi: 10.7334/psicothema2022.153
28. Park S, Hong KE, Park EJ, Ha KS, Yoo HJ. The association between problematic internet use and depression, suicidal ideation and bipolar disorder symptoms in korean adolescents. Aust Nz J Psychiat. (2013) 47:153–9. doi: 10.1177/0004867412463613
29. Chu C, Buchman-Schmitt JM, Stanley IH, Hom MA, Tucker RP, Hagan CR, et al. The interpersonal theory of suicide: a systematic review and meta-analysis of a decade of cross-national research. Psychol Bull. (2017) 143:1313–45. doi: 10.1037/bul0000123
30. Lai W, Wang W, Li X, Wang H, Lu C, Guo L. Longitudinal associations between problematic internet use, self-esteem, and depressive symptoms among chinese adolescents. Eur Child Adoles Psy. (2023) 32:1273–83. doi: 10.1007/s00787-022-01944-5
31. Cai Z, Mao P, Wang Z, Wang D, He J, Fan X. Associations between problematic internet use and mental health outcomes of students: a meta-analytic review. Adolesc Res Rev. (2023) 8:45–62. doi: 10.1007/s40894-022-00201-9
32. Li G, Conti AA, Qiu C, Tang W. Adolescent mobile phone addiction during the covid-19 pandemic predicts subsequent suicide risk: a two-wave longitudinal study. BMC Public Health. (2022) 22:1537. doi: 10.1186/s12889-022-13931-1
33. Yang LS, Zhang ZH, Hao JH, Sun YH. Association between adolescent Internet addiction and suicidal behaviours. Chin J Epidemiol. (2010) 31:1115–9. doi: 10.3760/cma.j.issn.0254-6450.2010.10.010
34. Erevik EK, Landrø H, Mattson ÅL, Kristensen JH, Kaur P, Pallesen S. Problem gaming and suicidality: a systematic literature review. Addict Behav Rep. (2022) 15:100419. doi: 10.1016/j.abrep.2022.100419
35. Mok K, Jorm AF, Pirkis J. Suicide-related internet use: a review. Aust Nz J Psychiat. (2015) 49:697–705. doi: 10.1177/0004867415569797
36. Daine K, Hawton K, Singaravelu V, Stewart A, Simkin S, Montgomery P. The power of the web: a systematic review of studies of the influence of the internet on self-harm and suicide in young people. PloS One. (2013) 8:e77555. doi: 10.1371/journal.pone.0077555
37. Jolin E, Weller R. Problematic internet use and suicidal behavior in adolescents: a review. Ann Clin Psychiatry. (2023) 35:272–9. doi: 10.12788/acp.0119
38. Cheng YS, Tseng PT, Lin PY, Chen TY, Stubbs B, Carvalho AF, et al. Internet addiction and its relationship with suicidal behaviors: a meta-analysis of multinational observational studies. J Clin Psychiat. (2018) 79:9291. doi: 10.4088/JCP.17r11761
39. Wang J, Hao QH, Tu Y, Peng W, Wang Y, Li H, et al. Assessing the association between internet addiction disorder and health risk behaviors among adolescents and young adults: a systematic review and meta-analysis. Front Public Health. (2022) 10:809232. doi: 10.3389/fpubh.2022.809232
40. Tang S, Chen R, Ma Z, Li X, Chen J, Zhao J. Associations of problematic smartphone use with depressive symptoms and suicidal ideation in university students before and after the covid-19 outbreak: a meta-analysis. Addict Behav. (2024) 152:107969. doi: 10.1016/j.addbeh.2024.107969
41. Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the prisma statement. Bmj-Brit Med J. (2009) 339:b2535. doi: 10.1136/bmj.b2535
42. Sawyer SM, Azzopardi PS, Wickremarathne D, Patton GC. The age of adolescence. Lancet Child Adolesc Health. (2018) 2:223–8. doi: 10.1016/S2352-4642(18)30022-1
43. Carlson EA. Agency for healthcare research and quality (ahrq) web site. Orthop Nurs. (2008) 27:258–9. doi: 10.1097/01.NOR.0000330315.06351.13
44. Lo C, Mertz D, Loeb M. Newcastle-ottawa scale: comparing reviewers' to authors' assessments. BMC Med Res Methodol. (2014) 14:1–5. doi: 10.1186/1471-2288-14-45
45. Melsen WG, Bootsma MC, Rovers MM, Bonten MJ. The effects of clinical and statistical heterogeneity on the predictive values of results from meta-analyses. Clin Microbiol Infect. (2014) 20:123–9. doi: 10.1111/1469-0691.12494
46. Copas J, Shi JQ. Meta-analysis, funnel plots and sensitivity analysis. Biostatistics. (2000) 1:247–62. doi: 10.1093/biostatistics/1.3.247
47. Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. Bmj-Brit Med J. (2003) 327:557–60. doi: 10.1136/bmj.327.7414.557
48. Egger M, Davey SG, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. Bmj-Brit Med J. (1997) 315:629–34. doi: 10.1136/bmj.315.7109.629
49. Duval S, Tweedie R. A nonparametric “trim and fill” method of accounting for publication bias in meta-analysis. J Am Stat Assoc. (2000) 95:89–98. doi: 10.1080/01621459.2000.10473905
50. Lin IH, Ko CH, Chang YP, Liu TL, Wang PW, Lin HC, et al. The association between suicidality and internet addiction and activities in Taiwanese adolescents. Compr Psychiat. (2014) 55:504–10. doi: 10.1016/j.comppsych.2013.11.012
51. Zhang DD, Feng SQ, Chen L, Miao JP, Yang LS, Sun YH. The relationship between suicidal ideation and internet addiction among female nursing students. Chin J Sch Health. (2014) 35:396–9. doi: 10.16835/j.cnki.1000-9817.2014.03.031
52. Wang PW, Liu TL, Ko CH, Lin HC, Huang MF, Yeh YC, et al. Association between problematic cellular phone use and suicide: the moderating effect of family function and depression. Compr Psychiat. (2014) 55:342–8. doi: 10.1016/j.comppsych.2013.09.006
53. Zhang TC, Zhang FL, Xiong JM, Lu SH, Wen LZ. Health risk behaviors and associated factors among middle school students in Wuling ethnic area. Chin J Sch. Health. (2018) 39:45–9. doi: 10.16835/j.cnki.1000-9817.2018.01.014
54. Wang W, Zhou DD, Ai M, Chen XR, Lv Z, Huang Y, et al. Internet addiction and poor quality of life are significantly associated with suicidal ideation of senior high school students in chongqing, China. Peerj. (2019) 7:e7357. doi: 10.7717/peerj.7357
55. Lu L, Jian S, Dong M, Gao J, Zhang T, Chen X, et al. Childhood trauma and suicidal ideation among chinese university students: the mediating effect of internet addiction and school bullying victimisation. Epidemiol Psych Sci. (2020) 29:e152. doi: 10.1017/S2045796020000682
56. Kuang L, Wang W, Huang Y, Chen X, Lv Z, Cao J, et al. Relationship between internet addiction, susceptible personality traits, and suicidal and self-harm ideation in chinese adolescent students. J Behav Addict. (2020) 9:676–85. doi: 10.1556/2006.2020.00032
57. Guo W, Tao Y, Li X, Lin X, Meng Y, Yang X, et al. Associations of internet addiction severity with psychopathology, serious mental illness, and suicidality: large-sample cross-sectional study. J Med Internet Res. (2020) 22:e17560. doi: 10.2196/17560
58. Yu Y, Yang X, Wang S, Wang H, Chang R, Tsamlag L, et al. Serial multiple mediation of the association between internet gaming disorder and suicidal ideation by insomnia and depression in adolescents in shanghai, China. BMC Psychiatry. (2020) 20:460. doi: 10.1186/s12888-020-02870-z
59. Huang Y, Xu L, Mei Y, Wei Z, Wen H, Liu D. Problematic internet use and the risk of suicide ideation in chinese adolescents: a cross-sectional analysis. Psychiat Res. (2020) 290:112963. doi: 10.1016/j.psychres.2020.112963
60. Shen Y, Meng F, Xu H, Li X, Zhang Y, Huang C, et al. Internet addiction among college students in a chinese population: prevalence, correlates, and its relationship with suicide attempts. Depress Anxiety. (2020) 37:812–21. doi: 10.1002/da.23036
61. Pan GL, Zeng FF, Huang GT. Analysis of health risk behaviors and influencing factors among adolescents in Zhenhai District. Chin J Public Health Manage. (2020) 36:663–6. doi: 10.19568/j.cnki.23-1318.2020.05.016
62. Shen Y, Jin X, Zhang Y, Huang C, Lu J, Luo X, et al. Insomnia in chinese college students with internet addiction: prevalence and associated clinical correlates. Front Psychiatry. (2020) 11:596683. doi: 10.3389/fpsyt.2020.596683
63. Wen LF, Gong JH, Maimaitijiang A, Ma YN, Lü J, Huang XM, et al. Study on the status and influencing factors of negative events among adolescents in Luohu District, Shenzhen. Pract Prev Med. (2021) 28:1479–83. doi: 10.3969/j.issn.1006-3110.2021.12.017
64. Peng C, Wang M, Cheng J, Tan Y, Huang Y, Rong F, et al. Mediation of internet addiction on association between childhood maltreatment and suicidal behaviours among chinese adolescents. Epidemiol Psych Sci. (2021) 30:e64. doi: 10.1017/S2045796021000524
65. Wang W, Zhang QX, Li XL, Wang JH, Zhang JP. Analysis of the status and influencing factors of Internet addiction among junior high school students in Guizhou Province. J Guizhou Med Univ. (2022) 47:661–5. doi: 10.19367/j.cnki.2096-8388.2022.06.007
66. Huang Q, Lin S, Li Y, Huang S, Liao Z, Chen X, et al. Suicidal ideation is associated with excessive smartphone use among chinese college students. Front Public Health. (2022) 9:809463. doi: 10.3389/fpubh.2021.809463
67. Junus A, Hsu YC, Wong C, Yip P. Is internet gaming disorder associated with suicidal behaviors among the younger generation? Multiple logistic regressions on a large-scale purposive sampling survey. J Psychiatr Res. (2023) 161:2–9. doi: 10.1016/j.jpsychires.2023.02.038
68. Wang W, Wu M, Zhu Z, Ma L, Zhang L, Li H. Associations of mobile phone addiction with suicide ideation and suicide attempt: findings from six universities in China. Front Public Health. (2023) 11:1338045. doi: 10.3389/fpubh.2023.1338045
69. Kang M, Xu B, Chen C, Wang D. Internet addiction and suicidal ideation among chinese college students: the mediating role of psychotic-like experiences. Front Public Health. (2023) 11:1276496. doi: 10.3389/fpubh.2023.1276496
70. Cheng J, Peng C, Rong F, Wang Y, Tan Y, Yu Y. Mobile phone addiction and suicide behaviors among chinese adolescents: the mediation of poor sleep quality. J Behav Addict. (2024) 13:88–101. doi: 10.1556/2006.2023.00078
71. Zhang Y, Wang D, Ma Z, Liu W, Su Y, Wang W, et al. Problematic internet use and suicide ideation among chinese adolescents: the indirect effects of insomnia, nightmares, and social jetlag. J Affect Disord. (2024) 344:347–55. doi: 10.1016/j.jad.2023.10.081
72. Young KS. Caught in the net: how to recognize the signs of internet addiction–and a winning strategy for recovery. John Wiley & Sons (1998) p. 1–12.
73. Chen S, Weng L, Su Y, Wu H, Yang P. Development of a chinese internet addiction scale and its psychometric study. Chin J Psychol. (2003) 45:279–94.
74. Liu QQ, Xu XP, Yang XJ, Xiong J, Hu YT. Distinguishing different types of mobile phone addiction: development and validation of the Mobile Phone Addiction Type Scale (MPATS) in adolescents and young adults. Int J Env Res Pub He. (2022) 19:2593. doi: 10.3390/ijerph19052593
75. Hughes JL, Horowitz LM, Ackerman JP, Adrian MC, Campo JV, Bridge JA. Suicide in young people: screening, risk assessment, and intervention. Bmj-Brit Med J. (2023) 381:e070630. doi: 10.1136/bmj-2022-070630
76. Meng SQ, Cheng JL, Li YY, Yang XQ, Zheng JW, Chang XW, et al. Global prevalence of digital addiction in general population: a systematic review and meta-analysis. Clin Psychol Rev. (2022) 92:102128. doi: 10.1016/j.cpr.2022.102128
77. Marchant A, Hawton K, Stewart A, Montgomery P, Singaravelu V, Lloyd K, et al. A systematic review of the relationship between internet use, self-harm and suicidal behaviour in young people: the good, the bad and the unknown. PloS One. (2017) 12:e0181722. doi: 10.1371/journal.pone.0181722
78. Susi K, Glover-Ford F, Stewart A, Knowles BR, Hawton K. Research review: viewing self-harm images on the internet and social media platforms: systematic review of the impact and associated psychological mechanisms. J Child Psychol Psyc. (2023) 64:1115–39. doi: 10.1111/jcpp.13754
79. Durkee T, Hadlaczky G, Westerlund M, Carli V. Internet pathways in suicidality: a review of the evidence. Int J Env Res Pub He. (2011) 8:3938–52. doi: 10.3390/ijerph8103938
80. Kelsall NC, Gimbrone C, Olfson M, Gould MS, Shaman J, Keyes K. Association between prosuicide website searches through google and suicide death in the United States from 2010 to 2021: lagged time-series analysis. J Med Internet Res. (2024) 26:e53404. doi: 10.2196/53404
81. Kim K, Ryu E, Chon MY, Yeun EJ, Choi SY, Seo JS, et al. Internet addiction in korean adolescents and its relation to depression and suicidal ideation: a questionnaire survey. Int J Nurs Stud. (2006) 43:185–92. doi: 10.1016/j.ijnurstu.2005.02.005
82. Gansner M, Belfort E, Cook B, Leahy C, Colon-Perez A, Mirda D, et al. Problematic internet use and associated high-risk behavior in an adolescent clinical sample: results from a survey of psychiatrically hospitalized youth. Cyberpsych Beh Soc N. (2019) 22:349–54. doi: 10.1089/cyber.2018.0329
83. Herrero J, Urueña A, Torres A, Hidalgo A. Socially connected but still isolated: smartphone addiction decreases social support over time. Soc Sci Comput Rev. (2019) 37:73–88. doi: 10.1177/089443931774261
84. Saunders JB, Hao W, Long J, King DL, Mann K, Fauth-Bühler M, et al. Gaming disorder: its delineation as an important condition for diagnosis, management, and prevention. J Behav Addict. (2017) 6:271–9. doi: 10.1556/2006.6.2017.039
85. Elman I, Borsook D, Volkow ND. Pain and suicidality: insights from reward and addiction neuroscience. Prog Neurobiol. (2013) 109:1–27. doi: 10.1016/j.pneurobio.2013.06.003
86. Brand M, Wegmann E, Stark R, Müller A, Wölfling K, Robbins TW, et al. The Interaction of Person-Affect-Cognition-Execution (I-PACE) model for addictive behaviors: update, generalization to addictive behaviors beyond internet-use disorders, and specification of the process character of addictive behaviors. Neurosci Biobehav R. (2019) 104:1–10. doi: 10.1016/j.neubiorev.2019.06.032
87. Barzilay R, Calkins ME, Moore TM, Boyd RC, Jones JD, Benton TD, et al. Neurocognitive functioning in community youth with suicidal ideation: gender and pubertal effects. Brit J Psychiat. (2019) 215:552–8. doi: 10.1192/bjp.2019.55
88. Sun JT, Hu B, Chen TQ, Chen ZH, Shang YX, Li YT, et al. Internet addiction-induced brain structure and function alterations: a systematic review and meta-analysis of voxel-based morphometry and resting-state functional connectivity studies. Brain Imaging Behav. (2023) 17:329–42. doi: 10.1007/s11682-023-00762-w
89. Ioannidis K, Redden SA, Valle S, Chamberlain SR, Grant JE. Problematic internet use: an exploration of associations between cognition and comt rs4818, rs4680 haplotypes. CNS Spectrums. (2020) 25:409–18. doi: 10.1017/S1092852919001019
90. Brand M, Young KS, Laier C, Wölfling K, Potenza MN. Integrating psychological and neurobiological considerations regarding the development and maintenance of specific internet-use disorders: an Interaction of Person-Affect-Cognition-Execution (I-PACE) model. Neurosci Biobehav R. (2016) 71:252–66. doi: 10.1016/j.neubiorev.2016.08.033
91. Miller AB, Prinstein MJ. Adolescent suicide as a failure of acute stress-response systems. Annu Rev Clin Psycho. (2019) 15:425–50. doi: 10.1146/annurev-clinpsy-050718-095625
92. Horwood S, Anglim J. Emotion regulation difficulties, personality, and problematic smartphone use. Cyberpsych Beh Soc N. (2021) 24:275–81. doi: 10.1089/cyber.2020.0328
93. Khatcherian E, Zullino D, De Leo D, Achab S. Feelings of loneliness: understanding the risk of suicidal ideation in adolescents with internet addiction. A theoretical model to answer to a systematic literature review, without results. Int J Env Res Pub He. (2022) 19:2012. doi: 10.3390/ijerph19042012
94. McMahon K, Hoertel N, Olfson M, Wall M, Wang S, Blanco C. Childhood maltreatment and impulsivity as predictors of interpersonal violence, self-injury and suicide attempts: a national study. Psychiat Res. (2018) 269:386–93. doi: 10.1016/j.psychres.2018.08.059
95. Tang C, Wu A, Yan E, Ko J, Kwon JH, Yogo M, et al. Relative risks of internet-related addictions and mood disturbances among college students: a 7-country/region comparison. Public Health. (2018) 165:16–25. doi: 10.1016/j.puhe.2018.09.010
96. Li S, Wang X, Wu Z, Zhang Y. The more internet access, the more mental symptoms students got, the more problematic internet use they suffered: a meta-analysis of mainland chinese adolescents and young adults. Int J Ment Health Ad. (2022) 21:4199–219. doi: 10.1007/s11469-022-00850-w
97. Mei K, Zhang F, Zhang J, Ming H, Jiang Y, Huang S. Perceived social support mitigates the associations among household chaos and health and well-being in rural early adolescents. J Adolescence. (2024) 96:112–23. doi: 10.1002/jad.12260
98. Gong F, Gong Z, Liu H, Yi P, Jia Y, Zhuang J, et al. The impact of problematic internet use on adolescent loneliness-chain mediation effects of social support and family communication. Psychol Res Behav Ma. (2024) 17:1903–16. doi: 10.2147/prbm.s443349
99. Chen SS, Lam TP, Lam KF, Lo TL, Chao D, Mak KY, et al. Youths' attitudes toward open discussion of suicide, preferred contexts, and the impact of internet use: an exploratory sequential mixed-methods study in hong kong. Int J Soc Psychiatr. (2023) 69:575–86. doi: 10.1177/00207640221123394
100. Wang Q, Mati K, Cai Y. The link between problematic internet use, problematic gaming, and psychological distress: does sleep quality matter? BMC Psychiatry. (2021) 21:103. doi: 10.1186/s12888-021-03105-5
101. Xiuqin H, Huimin Z, Mengchen L, Jinan W, Ying Z, Ran T. Mental health, personality, and parental rearing styles of adolescents with internet addiction disorder. Cyberpsych Beh Soc N. (2010) 13:401–6. doi: 10.1089/cyber.2009.0222
102. Poorolajal J, Ahmadpoor J, Mohammadi Y, Soltanian AR, Asghari SZ, Mazloumi E. Prevalence of problematic internet use disorder and associated risk factors and complications among Iranian university students: a national survey. Health Promot Perspe. (2019) 9:207–13. doi: 10.15171/hpp.2019.29
103. Chamarro A, Díaz-Moreno A, Bonilla I, Cladellas R, Griffiths MD, Gómez-Romero MJ, et al. Stress and suicide risk among adolescents: the role of problematic internet use, gaming disorder and emotional regulation. BMC Public Health. (2024) 24:326. doi: 10.1186/s12889-024-17860-z
104. Liu M, Xiao J, Kamper-DeMarco KE, Fu Z. Problematic internet use and suicidality and self-injurious behaviors in adolescents: effects of negative affectivity and social support. J Affect Disord. (2023) 325:289–96. doi: 10.1016/j.jad.2023.01.019
105. Chi X, Liu X, Guo T, Wu M, Chen X. Internet addiction and depression in chinese adolescents: a moderated mediation model. Front Psychiatry. (2019) 10:816. doi: 10.3389/fpsyt.2019.00816
106. Villanueva-Silvestre V, Vázquez-Martínez A, Isorna-Folgar M, Villanueva-Blasco VJ. Problematic internet use, depressive symptomatology and suicidal ideation in university students during covid-19 confinement. Psicothema. (2022) 34:518–27. doi: 10.7334/psicothema2022.40
107. Wang S, Xia L, Wang J, Yuan X, Shi Y, Wang X, et al. Prevalence and clinical correlates of internet addiction symptoms and their association with quality of life in adolescents with major depressive disorder: a multicenter cross-sectional study. Front Psychiatry. (2022) 13:819704. doi: 10.3389/fpsyt.2022.819704
108. Riblet NB, Matsunaga S, Shiner B, Schnurr PP, Watts BV. Are suicide risk scales sensitive to change? A scoping review. J Psychiatr Res. (2023) 161:170–8. doi: 10.1016/j.jpsychires.2023.03.007
109. Levy AG, Scherer AM, Zikmund-Fisher BJ, Larkin K, Barnes GD, Fagerlin A. Assessment of patient nondisclosures to clinicians of experiencing imminent threats. JAMA Netw Open. (2019) 2:e199277. doi: 10.1001/jamanetworkopen.2019.9277
110. Lee J, Ahn JS, Min S, Kim MH. Psychological characteristics and addiction propensity according to content type of smartphone use. Int J Env Res Pub He. (2020) 17:2292. doi: 10.3390/ijerph17072292
111. Li J, Wu Y, Hesketh T. Internet use and cyberbullying: impacts on psychosocial and psychosomatic wellbeing among chinese adolescents. Comput Hum Behav. (2023) 138:107461. doi: 10.1016/j.chb.2022.107461
112. Alan R, Senay Guzel H. The investigation of the relationship between smartphone addiction, and problem-solving skills and ways of coping with stress. Dusunen Adam J Psychiatry Neurol Sci. (2020) 33:244–53. doi: 10.14744/dajpns.2020.00088
113. Zhang X, Gao F, Kang Z, Zhou H, Zhang J, Li J, et al. Perceived academic stress and depression: the mediation role of mobile phone addiction and sleep quality. Front Public Health. (2022) 10:760387. doi: 10.3389/fpubh.2022.760387
114. Liu Q, Yang X, Hu Y, Zhang C, Nie Y. How and when is family dysfunction associated with adolescent mobile phone addiction? Testing a moderated mediation model. Child Youth Serv Rev. (2020) 111:104827. doi: 10.1016/j.childyouth.2020.104827
115. Harris B, Regan T, Schueler J, Fields SA. Problematic mobile phone and smartphone use scales: a systematic review. Front Psychol. (2020) 11:672. doi: 10.3389/fpsyg.2020.00672
116. Guo L, Luo M, Wang W, Huang G, Xu Y, Gao X, et al. Association between problematic internet use, sleep disturbance, and suicidal behavior in chinese adolescents. J Behav Addict. (2018) 7:965–75. doi: 10.1556/2006.7.2018.115
Keywords: problematic internet use, suicidal Behavior, adolescents, China, meta-analysis
Citation: He X, Chen S, Yu Q, Yang P and Yang B (2024) Correlations between problematic internet use and suicidal behavior among Chinese adolescents: a systematic review and meta-analysis. Front. Psychiatry 15:1484809. doi: 10.3389/fpsyt.2024.1484809
Received: 22 August 2024; Accepted: 21 October 2024;
Published: 11 November 2024.
Edited by:
Georgios D. Floros, Aristotle University of Thessaloniki, GreeceReviewed by:
Víctor José Villanueva-Blasco, Valencian International University, SpainCopyright © 2024 He, Chen, Yu, Yang and Yang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ping Yang, NDE1MTcwOTM1QHFxLmNvbQ==; Bo Yang, MTM3NjI1NTM5MUBxcS5jb20=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.