 Dalma Tényi
Dalma Tényi Györgyi Csábi
Györgyi Csábi József Janszky1
József Janszky1 Róbert Herold
Róbert Herold Tamás Tényi
Tamás Tényi- 1Department of Neurology, Medical School, Clinical Center, University of Pécs, Pécs, Hungary
- 2Department of Pediatrics, Medical School, Clinical Center, University of Pécs, Pécs, Hungary
- 3Department of Psychiatry and Psychotherapy, Medical School, Clinical Center, University of Pécs, Pécs, Hungary
It has been recognized that subtle, cosmetically insignificant anomalies tend to occur cumulatively in diseases with neurodevelopmental origin. These visible signs of morphogenesis errors are called minor physical anomalies (MPAs), serving as sensitive external markers of abnormal neurodevelopment. After the introduction of the Waldrop Scale, the studies conducted on MPAs in diseases with neurodevelopmental origin gave conflicting results. It has been debated that this discrepancy can be – at least partly – attributed to the use of the Waldrop Scale. Understanding the need of a comprehensive scale of MPAs that also differentiates according to the time of development, Hungarian pediatrician professor of University of Pécs, Károly Méhes developed a scale with 57 items, the only scale differentiating minor malformations from phenogenetic variants. With the use of the Méhes Scale, our research group has been investigating the role of abnormal neurodevelopment in different neuropsychiatric and neurologic disorders since 1997. 25 years into our research, in this review we summarize the results of our 18 research articles on MPAs in different diseases. We have found an increased number of MPAs, especially in the head and mouth region, in patients with schizophrenia, bipolar disorder, Tourette syndrome, autism and many epilepsy syndromes, fortifying the role of abnormal neurodevelopment in these diseases. Moreover, an increased number of MPAs was detected among the first-degree relatives of patients with schizophrenia and bipolar I disorder, supporting the hypothesis about MPAs being endophenotypic trait markers.
1 Introduction
Neurodevelopmental disorders are complex chronic conditions defined by deficits in the domains of motor skills, cognition, behavior and/or communication, appearing on grounds of abnormal central nervous system (CNS) development. The Diagnostic and Statistical Manual of Mental Disorders, 5th Edition, Text Revision: DSM-5-TR categorizes the following conditions under Neurodevelopmental Disorders: autism spectrum disorder, attention deficit hyperactivity disorder (ADHD), intellectual disability, communication disorder, specific learning disorders, motor disorders and tic disorders. The diagnosis of each disorder is based on a constellation of behaviors and symptoms listed in DSM-5-TR (1). Recently it has been debated whether neurodevelopmental disorders are in fact independent entities. It is widely known that different conditions tend to overlap, thus it is rather unusual for a neurodevelopmental disorder to appear on its own (2, 3). Frequent comorbidity can be observed in case of autism spectrum disorder and ADHD (4), moreover, according to DSM-5-TR (1), autism spectrum disorder serves no longer as an exclusion criterion for ADHD as in previous versions. Patients with Fragile X syndrome, a common cause of inherited intellectual disability, are also at risk of autism (5). Children with cerebral palsy may have co-existing ADHD, autism spectrum disorder or intellectual disability (6, 7). Another key defining characteristic is the disease onset, as these disorders generally present in childhood, moreover the cognitive and behavioral dysfunctions do not tend to appear immediately after the insult, but stay latent and become identifiable upon different stages of brain development. For example, in children with mild perinatal asphyxia, cognitive or behavioral abnormalities may become apparent only years after birth and till then, only hardly noticeable, minor neurological signs may be detected. It is also widely known that the symptoms of neurodevelopmental disorders do not always remain constant but may fluctuate, become worse or get better. Additionally, although the symptoms may be significantly improved with either pharmaco- or behavioral therapy long term, neurodevelopmental disorders are incurable disorders to date (2). On grounds of clinical observations in terms of similarities among different neurodevelopmental disorders, it has become questionable whether the strict, behavior based diagnostic approach is valid by all means. Another important aspect is the realization that in addition to the classic, DSM-5-TR defined neurodevelopmental disorders, abnormal CNS maturation plays a role also in other neurologic and psychiatric diseases: for example epilepsy of cortical dysplasia etiology or heterotopic lesions in schizophrenia (8). Growing amounts of scientific evidence suggest the multifactorial nature of neurodevelopmental disorders in terms of etiology, since – among others - chanellopathies, connectopathies, abnormal neurotransmission, genetic defects and epigenetic impact (perinatal asphyxia, vitamin deficiency, infections, toxic effects) may result in abnormal neurodevelopment (9). Many methods are available for the detection of aberrant neurodevelopment, for either clinical or research purposes (10). Careful medical history taking in terms of the pre-, peri- and early postnatal period and the later psychomotor development is highly important, since anomalies in these phases may suggest an underlying maldevelopment. Genetic testing may detect the single, direct cause of the disease (e.g. Fragile X syndrome) or point out genetic variants predisposing to abnormal neurodevelopment. Neuroimaging and postmortem brain studies may also serve as important methods in the detection of the structural background of behavioral and cognitive symptoms. It is evident that examining methods are not scarce, although more of them may not be available in every clinical setting due to technical or financial reasons.
2 Minor physical anomalies as trait markers for abnormal neurodevelopment
Central nervous system development begins around the 3. week of gestation, in the very beginning of the so-called embryonic stage of development (3-8. week), during which organogenesis takes place. At the end of the 2nd gestational week, the primitive streak becomes apparent and quickly starts to differentiate into the endo-, meso- and ectoderm (11). The pluripotent cells of the ectoderm begin to produce neuroepithelial cells, forming the neural plate, which invaginates and closes, creating the neural tube by the end of the 3rd gestational week. Around the 5th gestational week, the cranial end of the neural tube begins to swell, and differentiate into the telencephalon (which at the end forms the cerebral cortex, basal ganglia and hippocampus), diencephalon (developing into thalamus and hypothalamus), mesencephalon, metencephalon (later forming the pons and cerebellum) and myelencephalon (developing into the medulla oblongata) (11). At the 5th gestational week, the two important parts of the telencephalon can already be differentiated: the dorsal and the ventral neurogenic zones. The progenitor cells of the dorsal part migrate radially, developing into the cortical excitatory pyramidal neurons till the 20-23rd gestational week. The progenitor cells of the ventral part, on the other hand, start to migrate tangentially, forming the cortical inhibitory neurons, which process continues to go on even postnatally (11, 12).
Since the surface ectoderm (which later forms the skin) and the neuroectoderm differentiate from the same ectodermal tissue early in gestation, it seems reasonable to assume that an insult affecting this vulnerable stage of development may cause both CNS and skin anomalies. In fact, this connection is well-established in phacomatoses (also known as neurocutaneous syndromes), in which one of the main disease characteristic is the co-occurrence of skin and CNS anomalies: café au lait spots, schwannomas and neurofibromas in neurofibromatosis type I and II; facial angiofibromas and cortical tubers in tuberous sclerosis; leptomeningeal angioma and nevus flammeus in Sturge-Weber syndrome (13).
Analogue to the phenomena observed in neurocutaneous disorders, it has been recognized that subtle, cosmetically insignificant (mostly even only hardly recognizable) anomalies, identifiable even in healthy individuals, tend to occur cumulatively in diseases with neurodevelopmental origin. These visible signs of morphogenesis errors are called minor physical anomalies (MPAs), serving as sensitive external markers of abnormal neurodevelopment and may carry major informational value for diagnostic, prognostic and epidemiological purposes (14, 15). They are considered to be results of maldevelopment between the 3rd and 20-23rd gestational week and since they persist into adult life they can be detected on physical examination at any age from neonates to the elderly.
3 Scales to measure minor physical anomalies – development of the Méhes Scale
The first comprehensive studies on the abundance of MPAs in diseases with disordered behavior dates back to the 1960s. Goldfarb and Brostein (16) discovered that children with schizophrenia present with a higher number of MPAs. In their pioneering work, Mary Waldrop and Goering (17) detected increased number of minor physical anomalies in hyperactive children using the 18 item long Waldrop Scale, developed based on the work by Goldfarb and Brostein (16). After the introduction of the Waldrop Scale, a great amount of studies were conducted studying the connection between MPAs and neurodevelopmental disorders. Studies on the prevalence of MPAs in patients with hyperactivity (17), schizophrenia (18–24), affective disorders (21, 24) gave conflicting results (25–27). Although the development of the first scale to evaluate MPAs was highly innovatory and gave exceptional insight into the neurodevelopmental background of many disorders, it has been debated that the discrepancy between the studies can be – at least partly – attributed to the use of the Waldrop Scale and the shortcomings thereof. The Waldrop Scale contains only 18 MPAs, while in pediatric literature more than 50 have been listed. In the late 90s, only one year apart, three new scales have been developed. Recognizing the shortness of the Waldrop Scale as its weak point, in 1997, Lane and her coworkers (28) introduced a scale with 62 items for the assessment of dysmorphic features in schizophrenia. A year after that, pointing out its lack of extensiveness and the fact that these 18 item long list originated from results of an unpublished study, Ismail and his coworkers (29) conducted another scale with 41 items to investigate MPA profile in patients with schizophrenia. Besides the low number of items, the Waldrop Scale has been also criticized for not distinguishing between MPAs according to their time of development (30). Based on the report of the International Working Group (31), both Opitz (32) and Méhes (25) urged a clear distinction between morphogenetic events developing during organogenesis (i.e. in the embryonic state) and after organogenesis.
Understanding the need of a complex, comprehensive scale of MPAs that also differentiates according to the time of development, Hungarian pediatrician professor of University of Pécs, Károly Méhes developed a scale with 57 items, the only scale that differentiates minor malformations from phenogenetic variants (Table 1). Minor malformations are always abnormal, “all-or-none” type qualitative defects of embryogenesis, arising during organogenesis. On the other hand, developing after organogenesis, phenogenetic variants represent quantitative defects of final morphogenesis, and they can be regarded as exact equivalents of normal anthropometric variants (14, 25, 32). The background of the development of the Méhes Scale, a comprehensive instruction of its use, a detailed description of each anomaly and also, results of early studies on the topological profile of MPAs with the use of the Méhes Scale in childhood malignancies, diabetes, intellectual disability and cerebral palsy has been published in the pioneering work entitled “Informative morphogenetic variants in the newborn” by Méhes in 1988 (14).
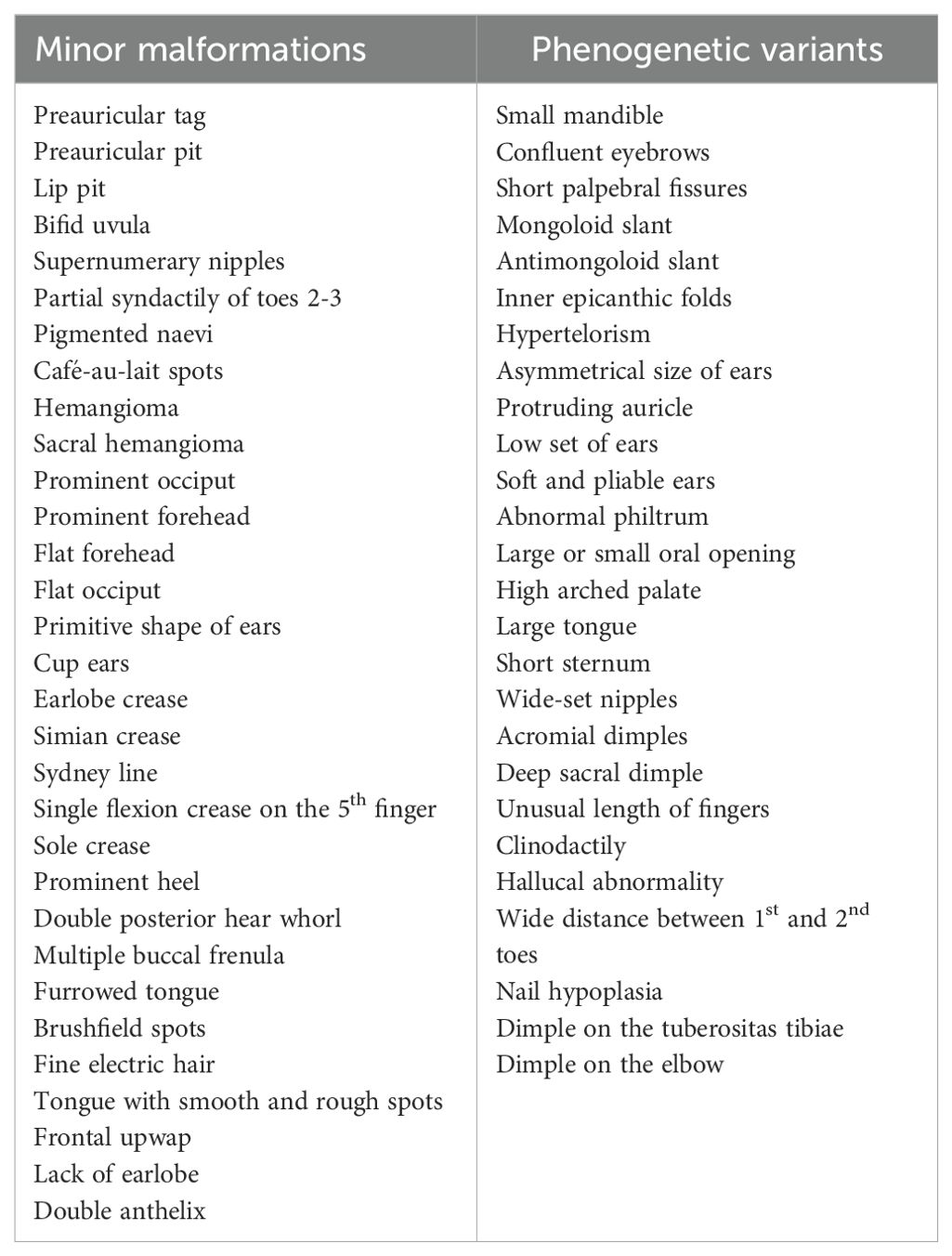
Table 1. The Méhes Scale.
Owing to its complexity and comprehensiveness, training is needed to be able to correctly apply the Méhes Scale in terms of adequately determine MPAs. Another limitation of the Scale is that based on the MPA profile it does not determine the kind of insult afftecting the central nervous system (e.g. genetic, vitamin difciency, trauma etc.), further research is needed in this direction.
4 25 years into the research on neurodevelopment with the use of the Méhes Scale
Conducted by a trained physician, the thorough physical examination according to the Méhes Scale may be carried out in a couple of minutes. As the examination requires no special equipment (in case of certain items only caliper and tape to improve objectivity), it serves as an effective, sensitive, fast and low-cost method for not only research purposes but in everyday clinical practice to identify patients with a possible underlying disorder with neurodevelopmental origin.
With the use of the Méhes Scale, our research group has been investigating the role of abnormal neurodevelopment as a contributing etiological factor in different neuropsychiatric disorders. Starting off with the investigation of patients with schizophrenia, we published our first results in 1997. Later we extended our research field to affective disorders, Tourette syndrome and at last, we turned our attention to the investigation of MPAs in epilepsy, on which we published our results in 2022, on the 25th anniversary of our research work (Table 2).
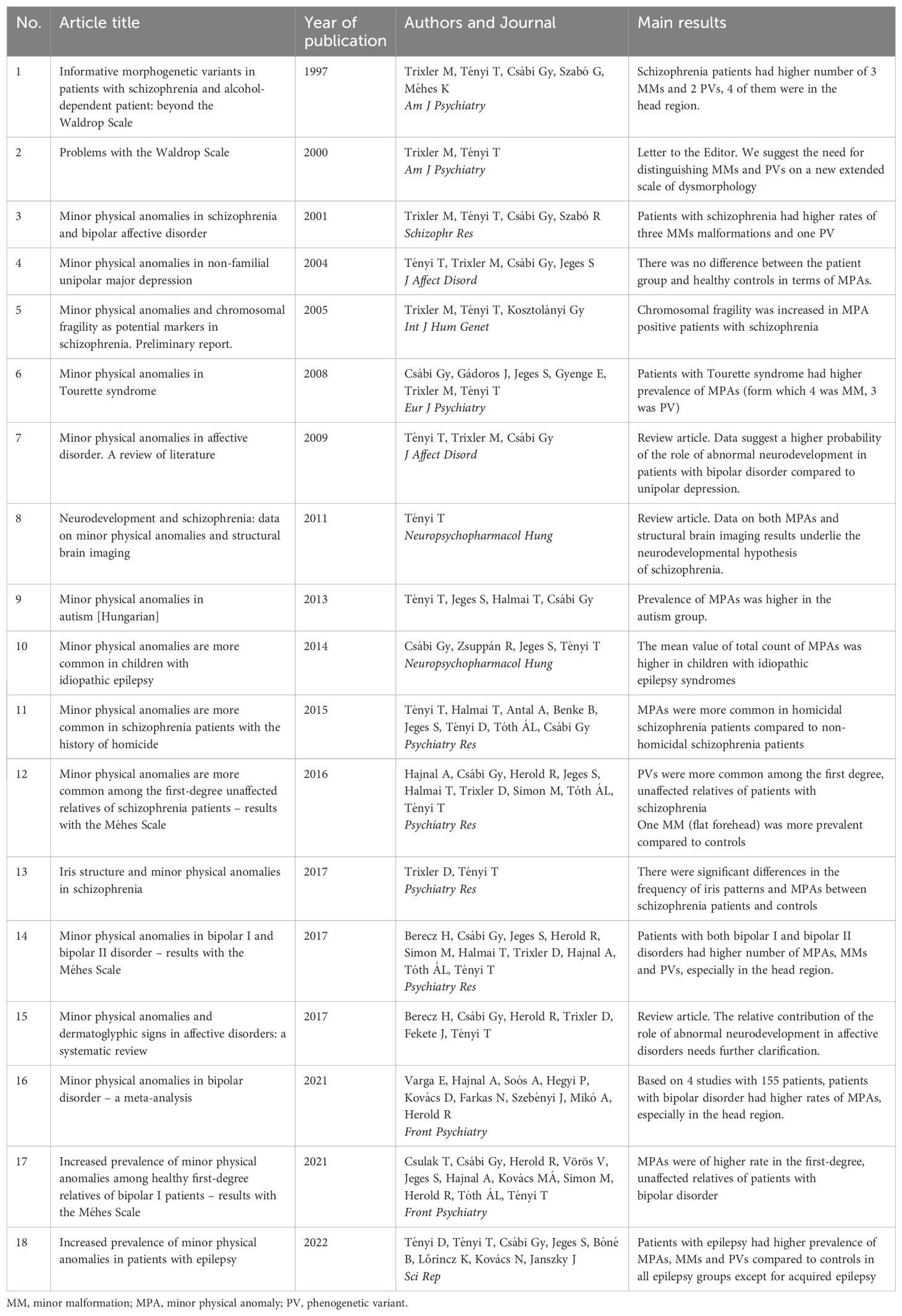
Table 2. List of our working group’s research articles on minor physical anomalies with the use of the Méhes Scale.
4.1 Schizophrenia
It has been argued that the dichotomist approach of the etiology of schizophrenia, that is the differentiation of neurodegenerative and neurodevelopmental mechanisms, is artificial and misguiding as the pathophysiology may show elements of both processes (12, 33–35). Magnetic resonance imaging studies indicated progressive changes in cerebral structures, fortifying the concept of neurodegeneration, however, the neurodevelopmental theory still remains as focal point. This hypothesis suggests that as a result of different insults (stress, obstetric complication, infection, vitamin D deficiency among others) occurring on grounds of a genetically defined susceptible constellation (12), subtle abnormalities in brain development occur in utero, remain latent for years before manifesting as symptoms of schizophrenia (36–39). Moreover, Catts and colleagues argue that neurodevelopment is not final at birth but continue postnatally well into adolescence, considering schizophrenia as a result of defected cortical maturation and retainment of an immature cerebral cortex (12). The neurodevelopmental theory of schizophrenia is fortified by the numerous imaging studies reporting on reduced gray matter volumes in the mesiotemporal structures and frontal lobe, enlarged lateral and third ventricles, abnormal gyrification patterns and heterotopic lesions (34, 40, 41).
Another strengthening factor of the neurodevelopmental theory is the excess of MPAs in patients with schizophrenia, which has been detected in several studies (18, 19, 28, 42–44). In the majority of them the Waldrop Scale or a modification thereof was used to assess MPAs (28, 29, 45, 46). The sometimes conflicting results of these studies may be, at least partly attributed to the scale in question itself, since it’s not comprehensive and unable to provide information on the timing of maldevelopment, which would be crucial in terms of future studies on possible primary/secondary prevention. With the use of the Méhes Scale, we detected five minor physical anomalies to be more common in patients with schizophrenia compared to patients with alcohol dependence serving as control subjects (47). As the Méhes Scale differentiates between minor malformations and phenogenetic variants, we were able to gain further insight regarding the timing of maldevelopment. We found that three of these MPAs were minor malformations (furrowed tongue, multiple buccal frenula, hemangioma), and the other two were phenogenetic variants (protruding auricle, large tongue), thus we can conclude that the insult is not just limited to a single developmental step but rather owns a long-acting effect and induces complex changes in neurodevelopment (47). In another study of ours, we have found that compared to normal controls, patients with schizophrenia showed higher rates of three minor malformations (furrowed tongue, flat occiput, primitive shape of ears) and one phenogenetic variant (wide distance between the toes 1 and 2). Also, as compared to patients with bipolar affective disorder, patients with schizophrenia had a higher number of one minor malformation (primitive shape of ears) (48). Given the comprehensive nature of the scale, we were able to study the topological profile of MPAs. We have found that they are mostly confined to the head and mouth region, fortifying their hypothesized connection to defective neurodevelopment (47, 48). In another study of ours we were the firsts to study iris structural patterns in schizophrenia patients in relation to MPAs. Our results fortified the neurodevelopmental concept by revealing a connection between structural iris patterns and MPAs (49).
It has been debated in what degree are MPAs results of epigenetic or genetic causes. There were studies that suggested a familial-genetic (20) background, on the other hand, the significant contributing role of epigenetic factors is supported by a study that found a higher prevalence of MPAs in patients with schizophrenia with a negative family history (50), however de novo genetic variants could also explain a large proportion of schizophrenia cases and be responsible for MPAs at the same time. In a study of ours we have found increased chromosomal fragility in MPA-positive patients with schizophrenia compared to controls, which provides significant support for the genetic determination of MPAs (51).
One of the most important clinical aspect of schizophrenia is the response rate to treatment, hence the overall severity of the disease. Treatment resistance has been connected to an increased prevalence of MPAs, which implies stronger insults in early neurodevelopment, thus, a more pronounced neurodevelopmental effect in pathogenesis (52). This result is in line with neuroimaging studies: treatment resistance has been connected to more reduced gray matter volume in frontal areas, enlarged white matter volume based on structural MRI studies, and different connectivity in resting state MRI studies (53). Another major clinical feature of schizophrenia is the risk of violence and aggressive behavior of the patients, which could be regarded as a factor of disease severity. The important role of aberrant neurodevelopment in the degree of violence in patients with schizophrenia has been supported by neuroimaging studies, detecting more pronounced frontal and temporal lobe abnormalities (54). Crowner and colleagues were the firsts to investigate the frequency of MPAs in violent psychiatric patients. The study was conducted using the Waldrop Scale and detected no relationship between MPA profile and violent behavior (55). Applying the Méhes Scale on a homologous sample, examining schizophrenia patients with the history homicide, we have found a clear positive correlation between the MPA frequency and violent behavior, implying a more severely affected neurodevelopment in these patients (56). According to the results of an electrophysiology study, having been conducted with the use of a modified version of the Méhes Scale, a possible endophenotype could be the abnormal profile of gamma oscillations, which are detectable with quantitative electroencephalogram (EEG) in schizophrenia patients. This was the first study on gamma activity in relation to MPAs in schizophrenia, however the authors argue that gamma abnormalities are well known phenomena in schizophrenia. Increased gamma power and synchrony are correlated with positive symptoms, consistent with enhanced structural connectivity, on the other hand, negative symptoms have been correlated in both increased and decreased activity (57). We consider these results to be beneficial not only in terms of research in schizophrenia etiology but also for clinical practice, since it may serve as a screening tool for therapy resistance and possible violent behavior.
4.2 Affective disorders
Since the early 1900s bipolar disorder (formerly known as “manic-depressive insanity”) has been carefully distinguished from other psychotic disorders (58). Since then, there is a growing evidence that the clear distinction of these disorders might be misleading, and the new concept of a psychiatric continuum ranging from unipolar depression, bipolar disorder, schizoaffective disorder and schizophrenia has been introduced (58–60). The theory of this continuum, more precisely the connection between bipolar disorder and schizophrenia has been strongly supported by decades-long research as these two disorders share many characteristics. A certain level of genetic overlap has been detected, they have several common risk factors, various structural brain abnormalities, share endophenotypes (neurocognitive, neuropsychological impairment, interpersonal difficulties) and regarding the pathophysiology, neurotransmitter abnormalities are thought to play a central role in both disorders. Based on this great amount of evidence, the theory of aberrant neurodevelopment as a central etiological factor could be extended from schizophrenia to bipolar disorder (58, 59, 61, 62).
Although it has been ongoing since the early 1990s, the strength of evidence from research of MPAs in affective disorders is not high. It can be traced back to the rather small amount of studies with conflicting results, which can be attributable to the – in many cases – heterogenous patient groups (mixed groups of bipolar, unipolar and schizoaffective patients) and the use of the Waldrop Scale or a modified version thereof (63, 64). In those few studies where patients with unipolar and bipolar depression were analyzed separately, results seem to be inconsistent: in some of them an increased frequency of MPAs in patients group could be detected compared to controls, however, these results could not be replicated in other studies, reviewed by Tényi et al. (63).
Acknowledging the rising concept of an existing continuum between unipolar depression and schizophrenia, we decided to extend our research on MPAs from schizophrenia to affective disorders and to try to resolve the conflicting results with the use of the Méhes Scale. In our first study (48), we have found that one minor malformation, namely furrowed tongue was more common in patients with bipolar disorder. In another, more extended investigation, we analyzed patients with bipolar I and bipolar II disorder separately. We detected an increased frequency of the total number of MPAs, minor malformations and phenogenetic variants in both bipolar I and bipolar II patient groups compared to controls. Moreover, analyzing the total number of anomalies in the mouth and ear region, we have found a higher frequency in patients with both bipolar I and bipolar II disorders. There proved to be no difference between the two patient groups in terms of the total number of MPAs, minor malformations and phenogenetic variants. In course of the individual analysis of the 57 MPAs, we have found that furrowed tongue is more common in bipolar I disorder and high arched palate is more common in patients with bipolar I and II disorder (65). On the other hand, in another study of ours, analyzing patients with non-familial unipolar recurrent major depression, we detected no difference between depressive patients and controls neither in the total number of MPAs, nor in the individual analysis of each anomaly (66). Conducted by our research group, in a recent meta-analysis, including four studies with 155 patients, an increased number of MPAs could be detected in patients with bipolar disorder compared to healthy controls (62). Taken together, our studies on the MPA profile of affective disorders underlie the current concept of the disease continuum between affective disorders and schizophrenia and the consequent rise of the theory of abnormal neurodevelopment being an etiological factor in bipolar disorder. Similar to schizophrenia, in terms of the topological profile, a definite head-area dominance of MPAs can be observed, further supporting neurodevelopmental origin. Distinguishing minor malformations from phenogenetic variants we gained further insight into the dynamic of maldevelopment: having detected that both minor malformations and phenogenetic variants are more common is bipolar disorder – similar to schizophrenia –, it implies a longer interval of CNS vulnerability to insults predisposing to bipolar disorder.
4.3 Analysis of MPAs in unaffected relatives of schizophrenia and bipolar patients
Endophenotypes are heritable traits that are indicators for a genetic susceptibility of a psychiatric disorder, they bridge the gap between symptom presentation and genetic variability. According Gottesman and Gould (67) “Endophenotype should be (1) associated with the illness, (2) heritable, (3) state-independent, (4) found in unaffected relatives at a higher rate than in the general population, and (5) shown to co-segregate with the illness within families” (68, pp 225). Since both schizophrenia and bipolar disorder operate with a strong genetic background, the intensive research on endophenotypes are by all means justified. Reviewing the analyses on the MPA profile of healthy relatives of schizophrenia patients, results seem to be conflicting: using the Waldrop Scale or modified Waldrop Scales, certain studies have found an increased number of MPAs in unaffected first-degree relatives, which results could not be replicated in other investigations (68). In our study on first-degree relatives of schizophrenia patients, with the use of the Méhes Scale, an overrepresentation of MPAs could be detected compared to controls, moreover, in line with our previous results, these anomalies had the tendency to appear in the mouth and head regions (68). More recently we turned our attention and extended endophenotype research towards affective disorders. We were the firsts to report on an increased number of MPAs among the first-degree relatives of patients with bipolar I disorder (69). Since in the individual analyses, among the two overrepresented MPAs, one was a minor malformation (sole crease) and the other one was a phenogenetic variant (high arched palate), it seems plausible that aberrant neurodevelopment may appear anytime between 3rd and 20-23rd gestational weeks (69). Increased number of MPAs in the unaffected relatives support the hypothesis about MPAs serving as endophenotypic trait markers in schizophrenia and bipolar I disorder, which, apart from its scientific value in etiology research, may also hold promise in prevention.
4.4 Tourette syndrome
Tourette syndrome is a neuropsychiatric syndrome characterized by multiple chronic tics, that may be either simplex or complex, vocal or motor. Its etiology seems to be multifactorial. Tourette syndrome is considered to lie on genetic grounds, being polygenic, involving several common risk variants mixed with uncommon, inherited or de novo genetic mutations. Besides the genetics, epigenetic factors may also contribute to the pathogenesis, resulting in structural and functional brain anomalies (70). Growing evidence suggests the strong neurodevelopmental nature of the disease. Supplying parallel support for the structural imaging studies, we were the firsts to investigate the MPA profile of children with Tourette syndrome. We detected a higher number of MPAs in the patients group compared to healthy controls and, similarly to our other studies on schizophrenia and bipolar disorder, these anomalies were more pronounced on the head region (high arched palate, posterior hair whorl), further supporting the neurodevelopmental theory (71).
4.5 Autism spectrum disorder
Autism, a disorder with the core symptoms of communication deficit, impaired social interaction and repetitive, stereotypic behaviors and interests, is thought to be caused by a complex interplay between multiple genetic and environmental factors. As opposed to earlier beliefs about autism carrying a strong psychological aspect (e.g. refrigerator mother theory), decades-long research has proven that it is in fact a neurodevelopmental disorder and psychological factors hardly even contribute to the pathogenesis (72, 73). In support of this theory, data from seven studies on the frequency of MPAs in autism (which were conducted by the Waldrop Scale) were analyzed in a meta-analysis, which showed a higher prevalence of MPAs in autism. However, as there were only very few data on the individual analysis of MPAs in autism, we analyzed 20 patients with the use of the comprehensive Méhes Scale (74). Our results corresponded to the previous studies, since we detected an increased frequency of MPAs in patients compared to controls, moreover, in course of the individual sub-analyses, primitive shape of ears, abnormal philtrum, clinodactylia and wide distance between toes 1 and 2 have proven to be the most common (74). After our publication, a Swedish research group published a study - analyzing minor malformations and phenogenetic variants separately in a similar way to ours - in which they reported a significantly higher overall MPA prevalence among adult patients with autism spectrum disorder, moreover they have found a higher prevalence of MPAs in the craniofacial region, namely the ear (75).
4.6 Epilepsy
Epilepsy is a large heterogenic group of neurological disorders, differing in etiology. In many epilepsy syndromes, previously assumed to be caused by one specific anomaly (e.g. channelopathy in juvenile myoclonic epilepsy or hippocampal sclerosis in temporal lobe epilepsy), it has been recognized that abnormal neurodevelopment also contributes to the epileptogenesis, which resulted in the recent rise of the concept of epilepsy as a neurodevelopmental disorder (76).
Early in the 20th century, increased frequency of MPAs in epilepsy patients was reported (77), however, these studies were not carried out with a scale based on modern dysmorphology. In a pilot study, analyzing 24 subjects and 24 controls, we detected an increased frequency of MPAs in patients with idiopathic childhood epilepsy (78).
We aimed to get further insight into the MPA profile of epilepsy patients, and in our subsequent study 235 adult epilepsy patients were included according to the following subgroups: acquired epilepsy (e.g. post-stroke, posttraumatic), temporal lobe epilepsy, epilepsy with cortical dysgenesis etiology, cryptogenic epilepsy and idiopathic generalized epilepsy (79). A higher number of MPAs in all epilepsy subgroups could be detected except for acquired epilepsy. The overrepresentation of these anomalies supports the view that epilepsy is related to factors early in development. However, in case of patients with acquired epilepsy, the insult seems to impact an intact nervous system, without a possible predisposing effect of a neurodevelopmental abnormality (79). In concordance with our studies on patients with schizophrenia, bipolar disorder, autism and Tourette syndrome, the two MPAs that were more common in epilepsy patients (furrowed tongue and high arched palate), both involved the head region (47, 48, 56, 65, 71, 74). Moreover, also similar to patients with schizophrenia, therapy resistance was associated with higher number of MPAs (52). Using the Méhes Scale as a screening tool, early identification of high-risk patients for pharmacoresistance may become possible.
5 Conclusion
Results of a wide range of decades-long research support the etiological role of aberrant neurodevelopment in disorders previously regarded as non-organic diseases. Besides genetic, epigenetic, neuroimaging and histological investigations, this growing evidence is further supported by the studying of MPAs, which serve as external markers for abnormal neurodevelopment. With the use of the Méhes Scale, a comprehensive, modern scale of dysmorphology, conducted by Professor Károly Méhes at the University of Pécs, our research group has been investigating the MPA profile of neurodevelopmental disorders since 1997.
25 years into our work we conducted research on patients with schizophrenia, bipolar disorder, unipolar depression, Tourette syndrome, autism and, on the 25th anniversary of our research we published our results on MPAs in epilepsy patients, extending our research field from neuropsychiatric to neurologic disorders.
Author contributions
DT: Conceptualization, Investigation, Writing – original draft. GC: Writing – review & editing. JJ: Writing – review & editing. RH: Writing – review & editing. TT: Conceptualization, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. DT and JJ were supported by the National Research, Development and Innovation Office Research Fund (NFKI_K_22-142479) and TKP-2021-EGA-13. DT, TT, and JJ were supported by the National Laboratory of Translational Neuroscience. TT was supported by the National Excellence Program (FIKP-IV).
In memoriam
In memoriam Professor Károly Méhes (1936-2007).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. American Psychiatric Association D, Association AP. Diagnostic and statistical manual of mental disorders, Fifth Edition, Text Revision: DSM-5-TR. Am Psychiatr Assoc. (2022). doi: 10.1176/appi.books.9780890425787
2. Thapar A, Cooper M, Rutter M. Neurodevelopmental disorders. Lancet Psychiatry. (2017) 4:339–46. doi: 10.1016/S2215-0366(16)30376-5
3. Ismail FY, Shapiro BK. What are neurodevelopmental disorders? Curr Opin Neurol. (2019) 32:611–16. doi: 10.1097/WCO.0000000000000710
4. da Silva BS, Grevet EH, Silva LCF, Ramos JKN, Rovaris DL, Bau CHD. An overview on neurobiology and therapeutics of attention-deficit/hyperactivity disorder. Discov Ment Health. (2023) 3:2. doi: 10.1007/s44192-022-00030-1
5. Aishworiya R, Protic D, Hagerman R. Autism spectrum disorder in the fragile X premutation state: possible mechanisms and implications. J Neurol. (2022) 269:4676–83. doi: 10.1007/s00415-022-11209-5
6. Reid SM, Meehan EM, Arnup SJ, Reddihough DS. Intellectual disability in cerebral palsy: a population-based retrospective study. Dev Med Child Neurol. (2018) 60:687–94. doi: 10.1111/dmcn.13773
7. Craig F, Savino R, Trabacca A. A systematic review of comorbidity between cerebral palsy, autism spectrum disorders and Attention Deficit Hyperactivity Disorder. Eur J Paediatr Neurol. (2019) 23:31–42. doi: 10.1016/j.ejpn.2018.10.005
8. Fry AE, Kerr MP, Gibbon F, Turnpenny PD, Hamandi K, Stoodley N, et al. Neuropsychiatric disease in patients with periventricular heterotopia. J Neuropsychiatry Clin Neurosci. (2013) 25:1. doi: 10.1176/appi.neuropsych.11110336
9. Parenti I, Rabaneda LG, Schoen H, Novarino G. Neurodevelopmental disorders: from genetics to functional pathways. Trends Neurosci. (2020) 43:608–21. doi: 10.1016/j.tins.2020.05.004
10. Bondi BC, Tassone VK, Bucsea O, Descrocher M, Pepler DJ. A systematic review of neurodevelopmental assessments in infancy and early childhood: developing a conceptual framework, repository of measures, and clinical recommendations. Neuropsychol Rev. (2024). doi: 10.1007/s11065-024-09641-7
11. Elshazzly M, Lopez MJ, Reddy V, Caban O. Embryology, central nervous system. In: StatPearls. StatPearls Publishing, Treasure Island (FL (2024). Available at: https://www.ncbi.nlm.nih.gov/books/NBK526024/.
12. Catts VS, Fung SJ, Long LE, Joshi D, Vercammen A, Allen KM, et al. Rethinking schizophrenia in the context of normal neurodevelopment. Front Cell Neurosci. (2013) 7:60. doi: 10.3389/fncel.2013.00060
13. Ruggieri M, Polizzi A, Marceca GP, Catanzaro S, Pratico AD, Di Rocco C. Introduction to phacomatoses (neurocutaneous disorders) in childhood. Childs Nerv Syst. (2020) 36:2229–68. doi: 10.1007/s00381-020-04758-5
15. Pinsky L. Informative morphogenetic variants. In: Issues and reviews in teratology, (New York, NY: Springer US) vol. 3. (1985). p. 1135–70. Minor congenital anomalies revisited.
16. Goldfarb W, Botstein A. Physical stigmata in schizophrenic children. Brooklyn, New York: Henry Ittleson Center for Child Research (1967).
17. Waldrop M, Goering JD. Hyperactivity and minor physical anomalies in elementary school children. Am J Ortopsychiatry. (1971) 41:602–7. doi: 10.1111/j.1939-0025.1971.tb03219.x
18. Gualtieri CT, Adams A, Shen CD, Loiselle D. Minor physical anomalies in alcoholic and schizophrenic adult and hyperactive and autistic children. Am J Psychiatry. (1982) 139:640–3. doi: 10.1176/ajp.139.5.64
19. Green MF, Satz P, Gaier DJ, Ganzell S, Kharabi F. Minor physical anomalies in schizophrenia. Schizophr Bull. (1989) 15:91–9. doi: 10.1093/schbul/15.1.91
20. O’Callaghan E, Larkin C, Kinsella A, Waddington JL. Familial, obstetric, and other clinical correlates of minor physical anomalies in schizophrenia. Am J Psychiatry. (1991) 148:479–83. doi: 10.1176/ajp.148.4.479
21. Green MF, Satz P, Christenson C. Minor physical anomalies in schizophrenia patients, bipolar patients, and their siblings. Schizophr Bull. (1994) 20:433–40. doi: 10.1093/schbul/20.3.433
22. Alexander RC, Reddy R, Mukherjee S. Minor physical anomalies in schizophrenia. Biol Psychiatry. (1992) 31:209. doi: 10.1016/0006-3223(92)90697-X
23. Alexander RC, Mukherjee S, Richter J, Kaufmann CA. Minor physical anomalies in schizophrenia. J Nerv Ment Dis. (1994) 182:639–44. doi: 10.1097/00005053-199411000-00007
24. Torrey EF, Bowler AE, Taylor EH, Gottesman II. Schizophrenia and manic-depressive disorder: the biological roots of mental illness as revealed by a landmark study of identical twins. New York: Basic Books (1994).
25. Méhes K. Minor malformations in the neonate: utility in screening infants at risk of hidden major defects. Prog Clin Biol Res. (1985) 163:45–9.
26. Feingold M, Bossert WH. Normal values for selected physical parameters: an aid to syndrome delineation. Birth Defects Orig Artic Ser. (1974) 10:1–16.
27. Merlob P. Mild errors of morphogenesis one of the most controversial subjects in dysmorphology. Iss Rev Teratology. (1994) 7:57–102.
28. Lane A, Kinsella A, Murphy P, Byrne M, Keenan J, Colgan K, et al. The anthropometric assessment of dysmorphic features in schizophrenia as an index of its developmental origins. Psychol Med. (1997) 27:1155–64. doi: 10.1017/S0033291797005503
29. Ismail B, Cantor-Graae E, McNeil T. Minor physical anomalies in schizophrenic patients and their siblings. Am J Psychiatry. (1998) 155:1695–702. doi: 10.1176/ajp.155.12.1695
30. Trixler M, Tényi T. Problems with the waldrop scale. Am J Psychiatry. (2000) 157:486. doi: 10.1176/appi.ajp.157.3.486
31. Spranger J, Benirschke K, Hall JG, Lenz W, Lowry RB, Opitz JM. Errors of morphogenesis: Concepts and terms: Recommendations of an International Working Group. J Pediatr. (1982) 100:160–5. doi: 10.1016/S0022-3476(82)80261-8
32. Opitz JM. Invited editorial comment: study of minor anomalies in childhood Malignancy. Eur J Pediatr. (1985) 144:252–4. doi: 10.1007/BF00451953
33. Olabi B, Ellison-Wright I, McIntosh AM, Wood SJ, Bullmore E, Lawrie SM. Are there progressive brain changes in schizophrenia? A meta-analysis of structural magnetic resonance imaging studies. Biol Psychiatry. (2011) 70:88–96. doi: 10.1016/j.biopsych.2011.01.032
34. Tényi T. Neurodevelopment and schizophrenia: data on minor physical anomalies and structural brain imaging. Neuropsychopharmacol Hung. (2011) 13:229–32. doi: 10.5706/nph201112006
35. Woods BT. Is schizophrenia a progressive neurodevelopmental disorder? Toward a unitary pathogenetic mechanism. Am J Psychiatry. (1998) 155:1661–70. doi: 10.1176/ajp.155.12.1661
36. McNeil TF, Cantor-Graae, Ismail B. Obstetric complications and congenital malformation in schizophrenia. Brain Res Rev. (2000) 31:166–78. doi: 10.1016/s0165-0173(99)00034-x
37. Cannon M, Jones PB, Murray RM. Obstetric complications and schizophrenia: historical and meta-analytic review. Am J Psychiatry. (2002) 159:1080–92. doi: 10.1176/appi.ajp.159.7.1080
38. Cui X, McGrath JJ, Burne THJ, Eyles DW. Vitamin D and schizophrenia: 20 years on. Mol Psychiatry. (2021) 26:2708–20. doi: 10.1038/s41380-021-01025-0
39. Brown AS. Exposure to prenatal infection and risk of schizophrenia. Front Psychiatry. (2011) 2:63. doi: 10.3389/fpsyt.2011.00063
40. Lippi G. Neuropsychiatric symptoms and diagnosis of grey matter heterotopia: A case-based reflection. S Afr J Psychiatr. (2017) 23:923. doi: 10.4102/sajpsychiatry.v23i0.923
41. Howes OD, Cummings C, Chapman GE, Shatalina E. Neuroimaging in schizophrenia: an overview of findings and their implications for synaptic changes. Neuropsychopharmacol. (2023) 48:151–67. doi: 10.1038/s41386-022-01426-x
42. Sivkov ST, Akabaliev VH. Minor physical anomalies in schizophrenic patients and normal controls. Psychiatry. (2003) 66:222–33. doi: 10.1521/psyc.66.3.222.25163
43. Weinberg SM, Jenkins EA, Marazita ML, Maher BS. Minor physical anomalies in schizophrenia: a meta-analysis. Schizoph Res. (2007) 89:72–85. doi: 10.1016/j.schres.2006.09.002
44. Xu T, Chan RCK, Compton MT. Minor physical anomalies in patients with schizophrenia, unaffected first-degree relatives, and healthy controls: a meta-analysis. PloS One. (2011) 6:e24129. doi: 10.1371/journal.pone.0024129
45. Gourion D, Goldberger C, Bourdel MC, Bayle FJ, Loo H, Krebs MO. Minor physical anomalies in patients with schizophrenia and their parents: prevalence and pattern of craniofacial abnormalities. Psychiatry Res. (2004) 125:21–8. doi: 10.1016/j.psychres.2003.06.001
46. McGrath JJ, van OSJ, Hoyos C, Jones PB, Harvey I, Murray RM. Minor physical anomalies in psychoses: associations with clinical and putative aetiological variables. Schizophr Res. (1995) 18:9–20. doi: 10.1016/0920-9964(95)00016-x
47. Trixler M, Tényi T, Csábi Gy, Szabó G, Méhes K. Informative morphogenetic variants in patients with schizophrenia and alcohol-dependent patients: beyond the Waldrop Scale. Am J Psychiatry. (1997) 154:5. doi: 10.1176/ajp.154.5.691
48. Trixler M, Tényi T, Csábi Gy, Szabó R. Minor physical anomalies in schizophrenia and bipolar affective disorder. Schizophr Res. (2001) 52:195–201. doi: 10.1016/s0920-9964(00)00182-1
49. Trixler D, Tényi T. Iris structure and minor physical anomalies in schizophrenia. Psychiatry Res. (2017) 256:412–6. doi: 10.1016/j.psychres.2017.07.004
50. Griffiths MT, Sigmundsson T, Takei N, Frangou S, Birkett PB, Sharma T, et al. Minor physical anomalies in familial and sporadic schizophrenia: the Maudsley family study. J Neurol Neurosurg Psychiatry. (1998) 64:56–60. doi: 10.1136/jnnp.64.1.56
51. Trixler M, Tényi T, Kosztolányi Gy. Minor physical anomalies and chromosomal fragility as potential markers in schizophrenia. Preliminary report. Int J Hum Genet. (2005) 5:173–7. doi: 10.1080/09723757.2005.11885921
52. Lin AS, Chang SS, Lin SH, Peng YC, Hwu HG, Chen WJ. Minor physical anomalies and craniofacial measures in patients with treatment-resistant schizophrenia. Psychol Med. (2015) 45:1839–50. doi: 10.1017/S0033291714002931
53. Mouchlianitis E, McCutcheon R, Howes OD. Brain-imaging studies of treatment-resistant schizophrenia: a systematic review. Lancet Psychiatry. (2016) 3:451–63. doi: 10.1016/S2215-0366(15)00540-4
54. Soyka M. Neurobiology of aggression and violence in schizophrenia. Schizophr Bull. (2001) 37:913–20. doi: 10.1093/schbul/sbr103
55. Crowner ML, Jaeger J, Convit A, Britzer D, Volavka J. Minor physical anomalies in violent adult inpatients. Eur J Psychiatry. (2008) 22:1163–6. doi: 10.1016/0006-3223(87)90060-6
56. Tényi T, Halmai T, Antal A, Benke B, Jeges S, Tényi D, et al. Minor physical anomalies are more common in schizophrenia patients with the history of homicide. Psychiatry Res. (2015) 225:702–5. doi: 10.1016/j.psychres.2014.11.012
57. Tikka SK, Nizamie SH, Das B, Katshu MZUH, Goyal N. Increased spontaneous gamma power and synchrony in schizophrenia patients having higher minor physical anomalies. Psychiatry Res. (2013) 207:164–72. doi: 10.1016/j.psychres.2012.09.006
58. Möller HJ. Bipolar disorder and schizophrenia: distinct illnesses or a continuum? J Clin Psychiatry. (2003) 6:23–7.
59. Crow TJ. The continuum of psychosis and its genetic origins. The sixty-fifth Maudsley lecture. Br J Psychiatry. (1990) 156:788–97. doi: 10.1192/bjp.156.6.788
60. Torrey EF. Epidemiological comparison of schizophrenia and bipolar disorder. Schizophr Res. (1999) 39:101–6. doi: 10.1016/s0920-9964(99)00107-3
61. Akabaliev VH, Sivkov ST, Mantarkov MY. Minor physical anomalies in schizophrenia and bipolar I disorder and the neurodevelopmental continuum of psychosis. Bipolar Disord. (2014) 16:633–41. doi: 10.1111/bdi.12211
62. Varga E, Hajnal A, Soós A, Hegyi P, Kovács D, Farkas N, et al. Minor physical anomalies in bipolar disorder - a meta-analysis. Front Psychiatry. (2021) 12:598734. doi: 10.3389/fpsyt.2021.598734
63. Tényi T, Trixler M, Csábi Gy. Minor physical anomalies in affective disorders. A review of the literature. J Affect Disord. (2009) 12:11–8. doi: 10.1016/j.jad.2008.04.025
64. Berecz H, Csábi Gy, Herold R, Trixler D, Fekete J, Tényi T. Minor physical anomalies and dermatoglyphic signs in affective disorders: A systematic review. Psychiatr Hung. (2017) 32:108–27.
65. Berecz H, Csábi Gy, Jeges S, Herold R, Simon M, Halmai T, et al. Minor physical anomalies in bipolar I and bipolar II disorders - Results with the Méhes Scale. Psychiatry Res. (2017) 249:120–4. doi: 10.1016/j.psychres.2017.01.014
66. Tényi T, Trixler M, Csábi Gy, Jeges S. Minor physical anomalies in non-familial unipolar recurrent major depression. J Affect Disord. (2004) 79:259–62. doi: 10.1016/S0165-0327(02)00360-9
67. Gottesman II, Gould TD. The endophenotype concept in psychiatry: etymology and strategic intentions. Am J Psychiatry. (2003) 160:636–45. doi: 10.1176/appi.ajp.160.4.636
68. Hajnal A, Csábi Gy, Herold R, Jeges S, Halmai T, Trixler D, et al. Increased prevalence of minor physical anomalies among the healthy first-degree relatives of bipolar I patients – results with the Méhes Scale. Psychiatry Res. (2016) 237:672241. doi: 10.3389/fpsyt.2021.672241
69. Csulak T, Csábi Gy, Herold R, Vörös V, Jeges S, Hajnal A, et al. Increased prevalence of minor physical anomalies among the healthy first-degree relatives of bipolar I patients - results with the Méhes Scale. Front Psychiatry. (2021) 12:672241. doi: 10.3389/fpsyt.2021.672241
70. Robertson MM, Eapen V, Singer HS, Martino D, Scharf JM, Paschou P, et al. Gilles de la Tourette syndrome. Nat Rev Dis Primers. (2017) 3:16097. doi: 10.1038/nrdp.2016.97
71. Csábi Gy, Gádoros J, Jeges S, Gyenge E, Trixler M, Tényi T. Minor physical anomalies in Tourette syndrome. Eur J Psychiatry. (2008) 22:173–80. doi: 10.4321/S0213-61632008000300006
72. Ozgen HM, Hop JW, Hox JJ, Beemer FA, van Engeland H. Minor physical anomalies in autism: a meta-analysis. Mol Psychiatry. (2010) 15:300–7. doi: 10.1038/mp.2008.75
73. Beopoulos A, Géa M, Fasano A, Iris F. Autism spectrum disorders pathogenesis: toward a comprehensive model based on neuroanatomic and neurodevelopment considerations. Front Neurosci. (2022) 16:988735. doi: 10.3389/fnins.2022.988735
74. Tényi T, Jeges S, Halmai T, Csábi Gy. Minor physical anomalies in autism. Ideggyogy Sz. (2013) 66:269–72.
75. Manouilenko I, Eriksson JM, Humble MB, Bejerot S. Minor physical anomalies with adults with autism spectrum disorder and healthy controls. Autism Res Treat. (2014) 2014:743482. doi: 10.1155/2014/743482
76. Bozzi Y, Casarosa S, Caleo M. Epilepsy as a neurodevelopmental disorder. Front Psychiatry. (2012) 3:19. doi: 10.3389/fpsyt.2012.00019
77. Paskind HA, Brown M. Constitutional differences between deteriorated and nondeteriorated patients with epilepsy. I. Stigmas of degeneracy. Arch Neurol Psychiatry. (1936) 36:1037–44. doi: 10.1001/ARCHNEURPSYC.1936.02260110122009
78. Csábi Gy, Zsuppán R, Jeges S, Tényi T. Minor physical anomalies are more common in children with idiopathic epilepsy. Neuropsychopharmacol Hung. (2014) 16:115–20.
Keywords: minor physical anomalies, Méhes Scale, neurodevelopmental disorders, schizophrenia, epilepsy
Citation: Tényi D, Csábi G, Janszky J, Herold R and Tényi T (2024) 25 years into research with the Méhes Scale, a comprehensive scale of modern dysmorphology. Front. Psychiatry 15:1479156. doi: 10.3389/fpsyt.2024.1479156
Received: 11 August 2024; Accepted: 18 October 2024;
Published: 04 November 2024.
Edited by:
Cecilia Samame, Catholic University of Uruguay, UruguayReviewed by:
Ferihan Ahmed-Popova, Plovdiv Medical University, BulgariaMarcelo Arancibia, Center for Translational Studies in Stress and Mental Health (C-ESTRES) Universidad de Valparaíso, Chile
Copyright © 2024 Tényi, Csábi, Janszky, Herold and Tényi. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Dalma Tényi, dGVueWkuZGFsbWFAcHRlLmh1