 Katharina Froelich
Katharina Froelich Jan Schürmann
Jan Schürmann Christian G. Huber
Christian G. Huber Manuel Trachsel
Manuel Trachsel- 1Clinical Ethics Unit, University Hospital Basel (USB), University Psychiatric Clinics (UPK) Basel, Geriatric University Hospital FELIX PLATTER Basel (UAFP), and University Children’s Hospital Basel (UKBB), Basel, Switzerland
- 2Medical Faculty, University of Basel, Basel, Switzerland
- 3Clinic for Adult Psychiatry, University Psychiatric Clinics (UPK) Basel, Basel, Switzerland
Introduction: Debriefing is recommended after any coercive measure in psychiatry, but there are no wellestablished standards, and ist effectiveness remains unclear. Incorporating shared decision-making (SDM) into post-coercion debriefing interventions has potentially beneficial effects.
Methods: This scoping review provides an overview of the general characteristics of such interventions and the extent to which SDM elements are already used in such interventions.
Results: A total of 2562 references were identified in the scholarly databases Embase, PubMed, Web of Science, and PsycINFO. In addition, 14 articles were identified through manual searches of reference lists. 42 full-text articles were screened for eligibility, 13 articles met the eligibility criteria and were further analyzed.
Discussion: No intervention tool was found that clearly included all SDM elements. However, three elements of SDM were present at least partially in all interventions: definition and explanation of the health care problem, the clarification of the patient's values and preferences, and a decision or explicit deferral of the decision. Further research is needed to systematically examine the implementation and clinical effectiveness of post-coercion debriefing interventions, particularly regarding the inclusion of shared decision-making elements.
1 Introduction
In Switzerland, 10.4% of all adult patients in acute and primary psychiatric care were affected by a formal coercive measure such as seclusion, restraint, or forced medication in 2022 (1). Coercive measures are defined as any measure “carried out against the patient’s self-determined wishes or in spite of his or her opposition” (2). They can be a significant burden for patients, relatives and health care providers (3–5). Moreover, the use of coercion contradicts the ethical principle of respect for patient autonomy and should therefore only be used when necessary and appropriate to prevent a serious risk to self or others (6). The elimination of unjustified coercion and the reduction of coercion in psychiatry is a goal of several national and transnational guidelines (7, 8).
Debriefing with patients after coercive measures is one intervention among several others to achieve this goal (9). A debriefing should reflect on the situation that led to the use of coercive measures and aim at a retrospective understanding of the different perspectives of all those involved. This should provide emotional relief and transparency and strengthen the therapeutic relationship (10). Medical ethical guidelines in Switzerland and Germany recommend that a debriefing should take place after every coercive measure (2, 8). However, no standards have yet been established for the content, implementation, and conduct of debriefings (10). Only a few projects have systematically implemented post-coercion debriefings, mostly as part of more complex programs such as the Weddinger Model (11) or the Six Core Strategies (12). To date, there is little research on the effectiveness of debriefing as a stand-alone intervention to prevent future coercion (13, 14).
In addition to a retrospective reflection on the coercive event, debriefing can emphasize prevention by allowing strategies to be developed to avoid or reduce the impact of coercive measures in the future (15). Hereby, insights from the retrospective part of the debriefing can be used to inform future care plans (16). Shared decision-making (SDM) can be considered as one approach to shape and conduct this prospective part of the post-coercion debriefing intervention. This involves health care professionals and patients discussing available options together and choosing the option that best fits the patient’s circumstances and preferences (17). Patient-centered care, which emphasizes participation, recovery, and transparency, advocates SDM as the preferred form of medical decision making (18, 19). However, there is currently no established standard approach to SDM in psychiatry (20), and most approaches focus on psychopharmacological decisions and therefore do not address the complex realities of psychiatric patients (21).
There is growing evidence of the beneficial effects of using SDM in psychiatric interventions. SDM interventions have been shown to be effective for reducing involuntary admissions (22, 23). Recently, an SDM intervention for the first week after involuntary admission was developed and found to be feasible and well received by patients and treatment providers (24). Another study found that an SDM intervention for patients admitted to a mental health facility against their will improved patients’ perceived involvement in decision making in a manner similar to that observed for those admitted voluntarily (25). However, the intervention, which did not specifically target decision making in the context of a coercive event, did not reduce aggressive incidents or coercive measures. Most patients want to be involved in decisions about restraint (26). Involvement of involuntary patients is also a strong predictor of their subjective quality of life and treatment satisfaction for these patients (27). Facilitating and confounding factors of SDM in involuntarily admitted patients have also been investigated (28).
Decision aids (DAs) are important tools for translating the principles of SDM into clinical and practical reality (29). Digitalization provides an opportunity to design DAs in an interactive, personalized, and potentially more effective manner (30). Digital DAs have promising practical applications in psychiatry to improve patient motivation and the therapeutic relationship, and to reduce decision-making conflict (31). Therefore, digital DAs may have the potential to facilitate SDM in post-coercion debriefing in psychiatry.
The findings of this scoping review will inform the development of a digital DA to support clinical practitioners in implementing SDM in post-coercion debriefing interventions in psychiatry. Previous research does not explicitly report on SDM interventions that were used in this context. Krieger and colleagues (10) conducted a narrative review of post-coercion debriefing but provided limited information on specific tools and their characteristics. Therefore, a systematic search for literature on SDM elements in debriefing interventions in the described context is considered as necessary. The aim of this scoping review is to identify the range of SDM elements used in post-coercion debriefing interventions in psychiatry. In addition, an analysis of general characteristics will provide further insight into the practical application and the requirements of these interventions. This scoping review addresses the following two research questions:
1. What SDM elements are included in post-coercion debriefing interventions in psychiatry?
2. What general characteristics are found in post-coercion debriefing interventions in psychiatry?
2 Methods
We conducted the present scoping review in accordance with the JBI methodology for scoping reviews (32). The final version of the report follows the Preferred Reporting Items for Systematic review and Meta-analysis extension for Scoping Reviews (PRISMA-ScR) as proposed by Tricco and colleagues (33). The review protocol was not pre-registered.
2.1 Study eligibility
Eligible publications were peer-reviewed articles including original theoretical, qualitative, quantitative, multi-methods, and mixed-methods studies, as well as all evaluation study designs (pre-experimental, experimental, randomized controlled trials (RCTs), quasi-experimental). Unpublished or non-peer-reviewed articles were not included, as the reviewers expected high-quality results to be published in peer-reviewed journals. Articles in English, German and French were included based on the language skills of the research team. Articles published between 01/01/2013 and 13/07/2023 were included as no relevant literature was expected to be published before this date.
Articles were selected if they reported data on intervention tools with SDM elements following coercive measures in psychiatry. The target population was 18 years of age or older with a DSM or ICD psychiatric diagnosis and experience with coercive measures in psychiatry. All psychiatric settings for adult patients were included (inpatient and outpatient) such as acute or long-term adult psychiatric wards, geriatric psychiatric wards, psychiatric outpatient clinics, or forensic psychiatric wards. Somatic hospitals, retirement homes and nursing homes were excluded due to the specific nature of these settings.
Post-coercion debriefing interventions were broadly defined as any structured conversation between patient and health care professionals following a coercive event with the aim of enabling patients and staff to view the event from each other’s perspectives, repairing ruptures in the therapeutic alliance and strengthening working relationships, providing emotional expression and relief in relation to the experienced situation, or preventing the use of further coercive measures.
Studies were selected if they addressed the issue of future coercion and/or its prevention, in addition to reflecting on a past coercive event, and used at least two key elements of SDM in this intervention. The key elements of SDM were operationalized according to the established SDM model of Makoul and Clayman (17) (Table 1).
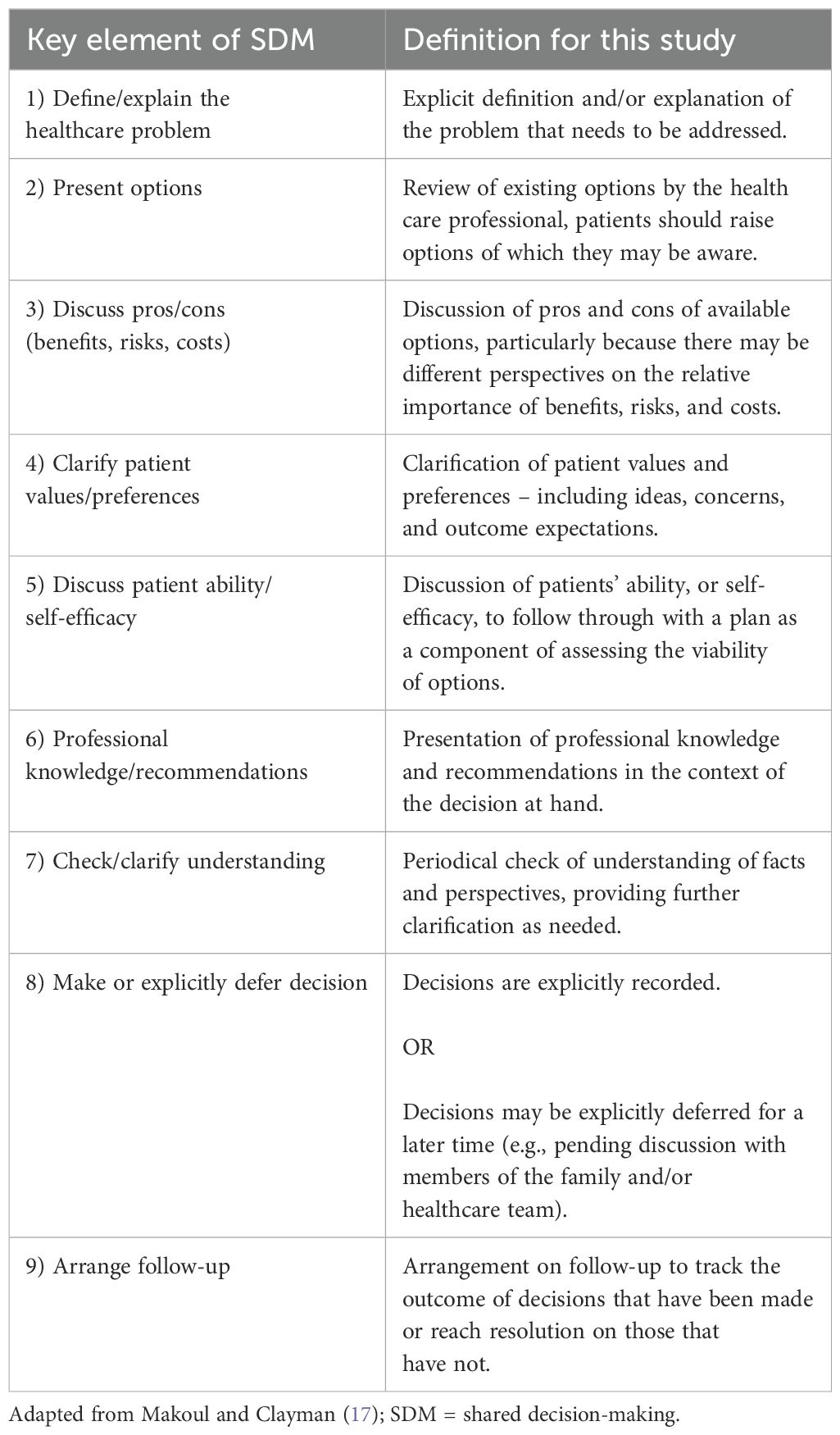
Table 1. Definitions for the key elements of SDM.
2.2 Information sources and search strategy
An initial limited search of PubMed and Cochrane was conducted to identify articles on the topic. In consultation with an academic librarian from the University Library of Basel, the text words contained in the titles and abstracts of relevant articles and the index terms used to describe the articles were used to develop full search strategies. For peer-reviewed literature, the databases Embase, Web of Science, PubMed, and PsycINFO were searched using search terms related to the concepts of psychiatry, coercion, intervention, and SDM. The search strategy, including all identified keywords and index terms, was adapted for each included database (see Supplementary Material). Search terms included Emtree in Embase, free text terms in Web of Science, MeSH in PubMed, and indexed terms from the thesaurus in PsycINFO.
2.3 Study selection
Following the search, all identified references were collated and uploaded into Citavi (version 6.17, Lumivero: Denver, USA) and then imported into the Covidence systemic review software (Veritas Health Innovation: Melbourne, Australia, 2023). After deduplication, two reviewers (JS and KF) independently screened all titles and abstracts against the inclusion criteria. Disagreements were resolved by a third reviewer (MT). In the next stage of the screening process, the full texts of the selected references were screened using the same procedure. Reasons for exclusion of references were recorded.
2.4 Data extraction
Data were extracted from each included article by two independent reviewers (JS and KF). Disagreements were resolved by discussion to reach consensus. An extraction form developed by the reviewers was used, which was modified and revised as necessary during the process. Data were extracted on bibliographic information (authors, title, year of publication, country), general study details (study design, sample size, setting, focus on specific disorders) and general characteristics of the intervention applied (name of intervention tool, participants and their roles, duration of the intervention, timepoint of application, training before use of tool). In addition, an in-depth qualitative analysis of the application of SDM elements in the intervention tools was conducted. We therefore used the definitions in Table 1 to determine which key SDM elements were present. In two cases (13, 34) the authors of the articles were contacted to request additional data for this analysis, which we were unable obtain.
2.5 Data analysis and synthesis of results
Data on general elements of the articles were presented in tabular form. The results of the qualitative analysis of the SDM elements in the intervention tools were used to categorize each of the nine SDM elements as present or absent for each article in an additional table. The elements were marked as “unclear” if the interventions were not clearly described and/or if the reviewers were uncertain whether the relevant element was met in all aspects. All tabulated results are accompanied by a narrative summary describing how they relate to the objectives and questions of the scoping review.
3 Results
3.1 Study selection
An overview of the study selection process is described in the PRISMA flow diagram (Figure 1). A total of 2562 references were identified in the selected scientific databases (Embase n = 1012; Web of Science n = 594; PubMed n = 555; PsycINFO n = 401). An additional 14 articles were identified by hand searching the reference lists of the identified articles.
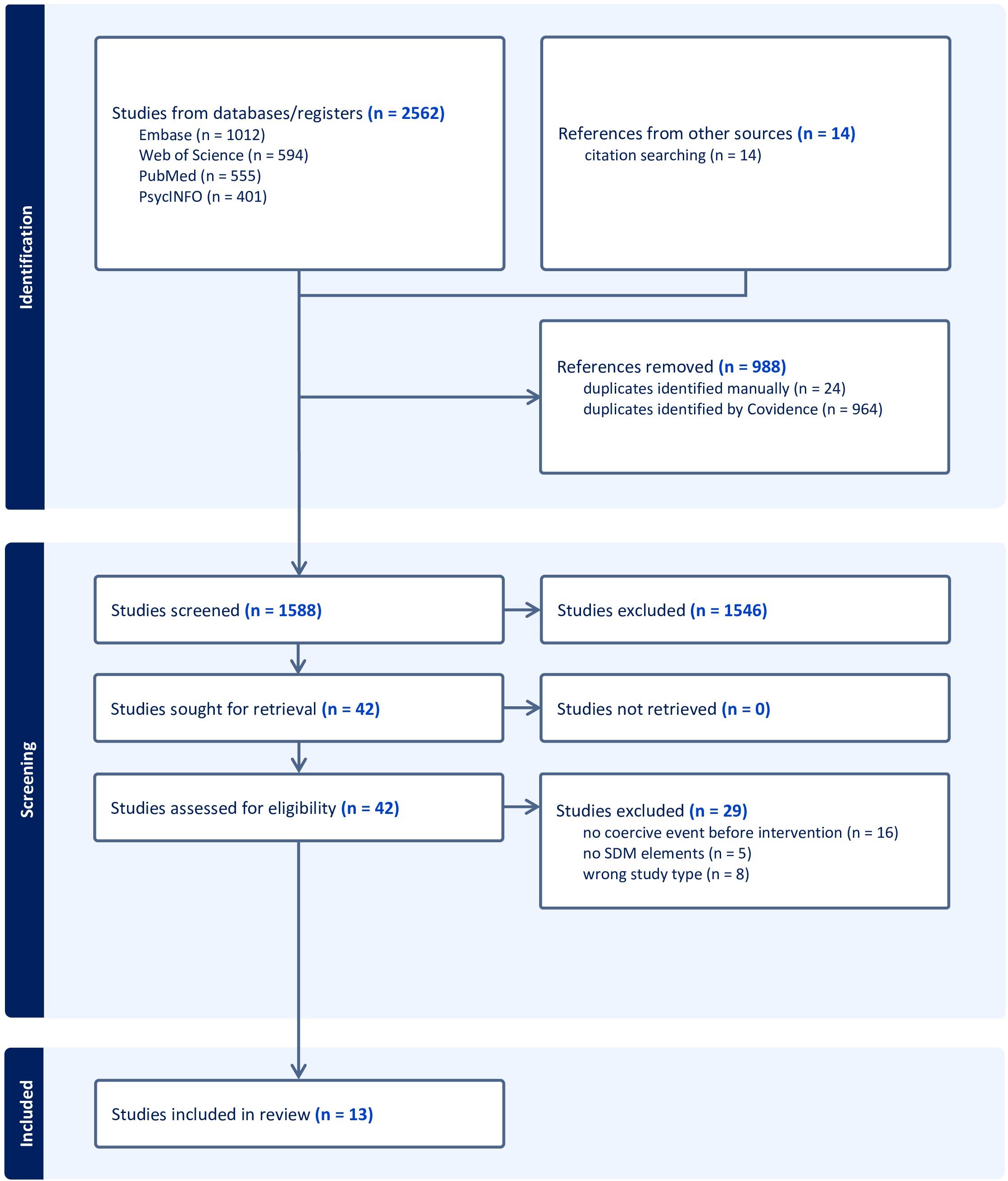
Figure 1. PRISMA flow diagram.
After removing duplicates, 1588 references underwent title/abstract screening. 42 full-text articles were assessed for eligibility. We excluded 29 articles, most often because the intervention did not follow a coercive event (n = 16), did not include SDM elements (n = 5), or because the study design did not meet the inclusion criteria (n = 8). Thirteen articles met the eligibility criteria and were further analyzed.
3.2 Study details
Table 2 shows the bibliographic information and study details of the 13 articles included in this scoping review. More than one third of the articles each used a qualitative study design (n = 5; 38%) or an experimental study design (randomized controlled trial n = 3; 23%; quasi-experimental n = 2; 15%). Two articles (15%) described interventions at a theoretical level. Most researchers or research teams were based in Europe (n = 10; 77%). More than half of the articles (n = 8; 62%) involved research with patients, some articles involved research with care providers (n = 3; 23%). A variety of settings were represented, with the most articles coming from acute inpatient settings (n = 6; 46%). As some settings were not described in detail, but only mentioned that the intervention took place in a hospital, we estimate this number to be higher. In two articles, the intervention also took place in a community mental health setting (n = 2; 15%). The majority of the articles focusing on specific psychiatric disorders included patients with psychotic disorders (n = 8; 62%). Other psychiatric diagnoses mentioned were affective disorders (n = 2; 15%) and substance use disorders (n = 2; 15%).
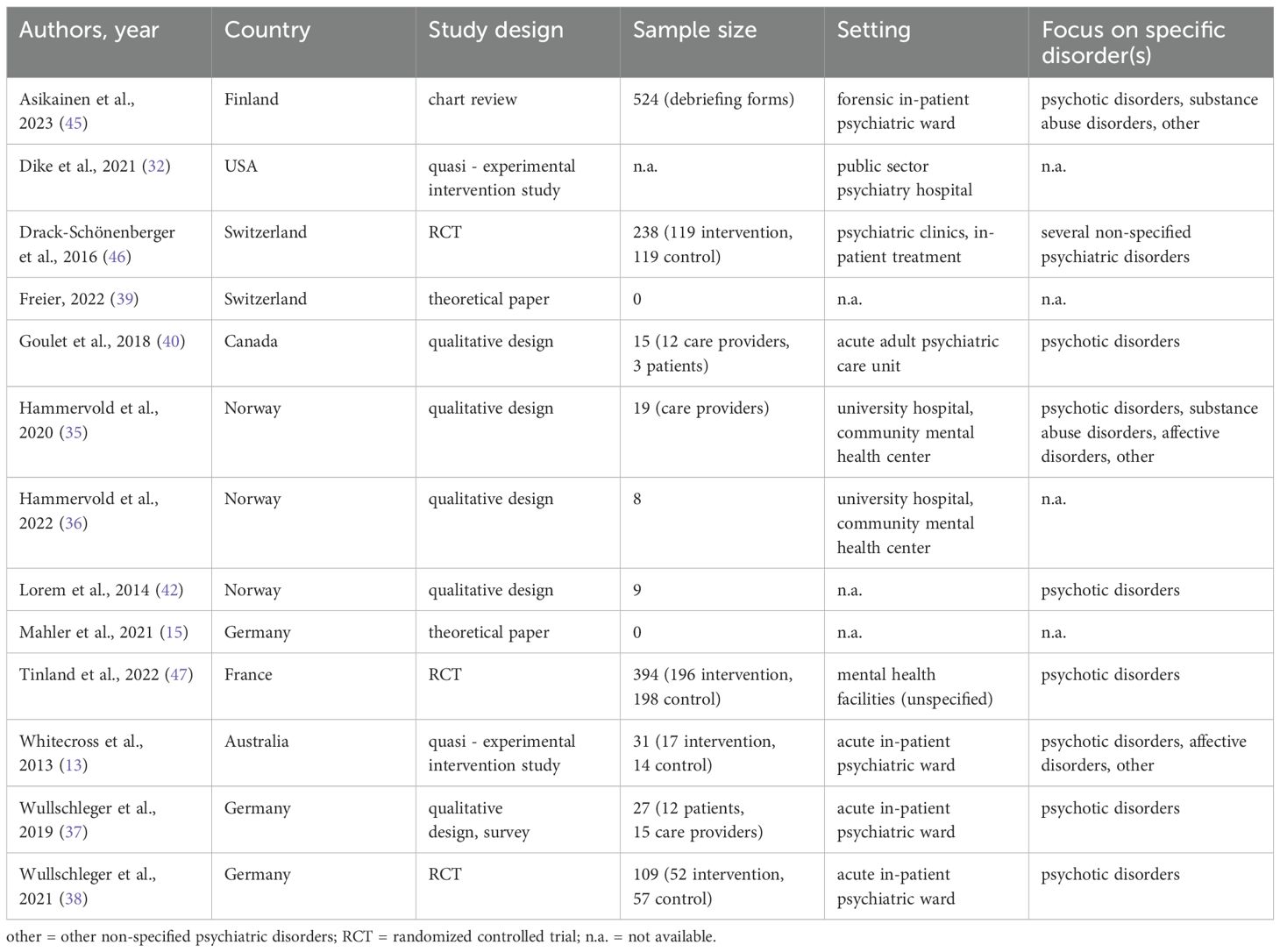
Table 2. Bibliographic information and study details of the included articles.
3.3 General characteristics of the interventions
A selection of relevant general characteristics of the post-coercion interventions is shown in Table 3. Several articles described the same intervention (35, 36): and (15, 37, 38). The two theoretical articles applied the same rationale and general outline with slight adaptations of the research questions used (15, 39). One article additionally described a tool for a debriefing with caregivers involved in the coercive event, but without the presence of the patient (40).
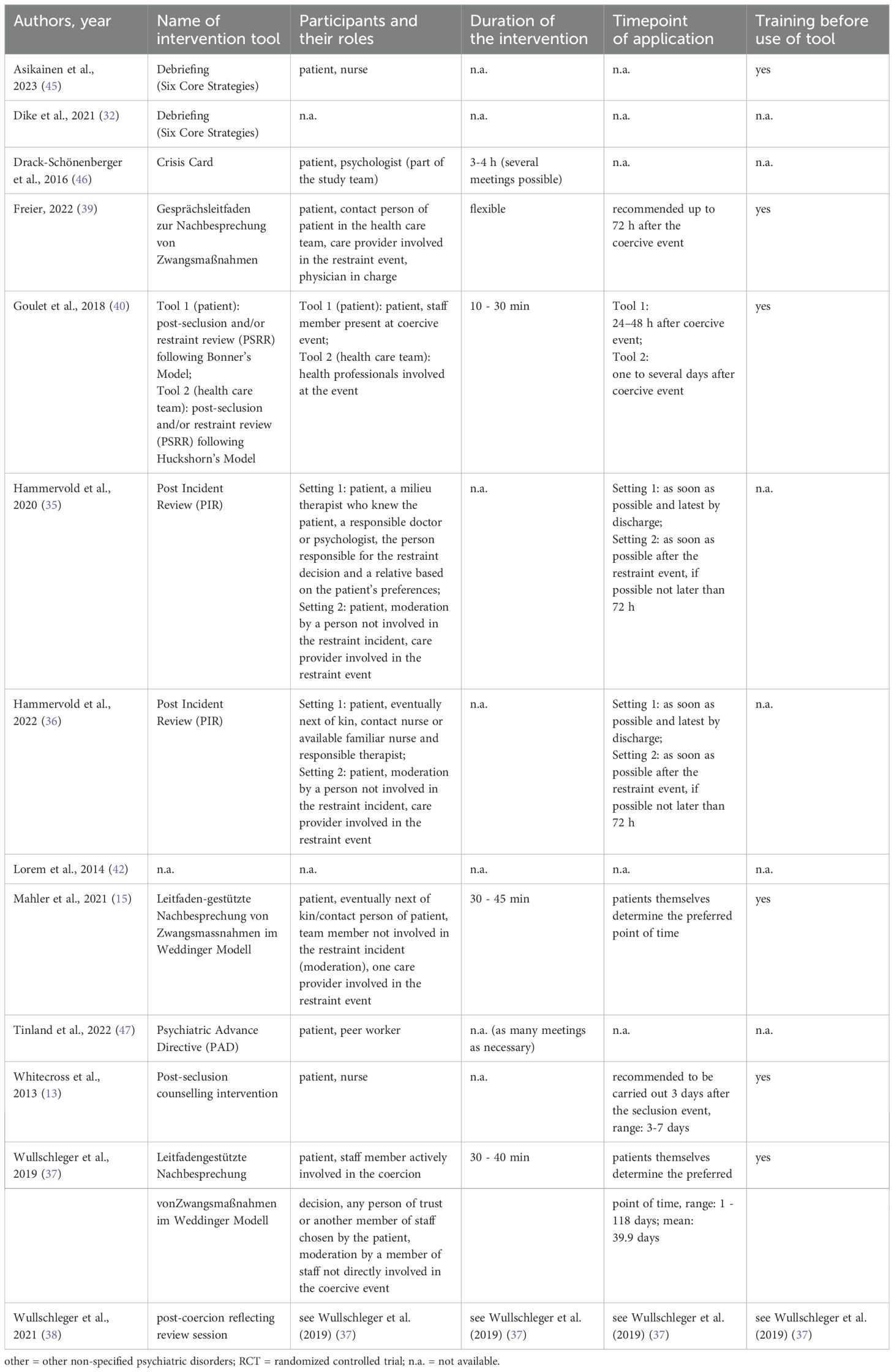
Table 3. General characteristics of the identified post-coercion debriefing interventions.
The number of participants in the intervention ranged from the patient with one member of the study team to several participants with different roles. These included, for example, the patient’s next of kin, the patient’s contact person in the health care team, care providers involved in the coercive event, or other responsible care providers. Almost half of the articles (n = 6; 46%) described the specific role of a moderator, who was to be a person not involved in the coercive event.
The duration of the intervention ranged from 10 to 45 minutes. Some articles emphasized the importance of flexibility and the possibility of conducting multiple sessions if needed. Eight articles (62%) reported a recommended time point for the implementation of the intervention after the coercive event. Recommendations ranged from 48 hours to 3 days but reported data from the experimental studies showed that interventions were delivered up to 118 days later. In some interventions (n = 3; 23%), patients themselves were allowed to choose the preferred point of time. More than half of the articles (n = 7; 54%) mentioned a training of the health care professionals before the tool was used in practice. This included presentations and opportunities to consult with the researchers (40) or prompt cards outlining the principles and process for conducting the debriefing intervention (13).
3.4 SDM elements
Table 4 shows the SDM elements present in each post-coercion intervention. There was no intervention in which all SDM elements were clearly present. Three elements of SDM were present in all interventions, in some cases at least partially: 1.) definition and explanation of the health care problem, 4.) the clarification of patient’s values and preferences, and 8.) a final decision or explicit deferral of the decision. Almost all interventions (n = 12; 92%) included the SDM element of 2.) presenting and reviewing existing options.
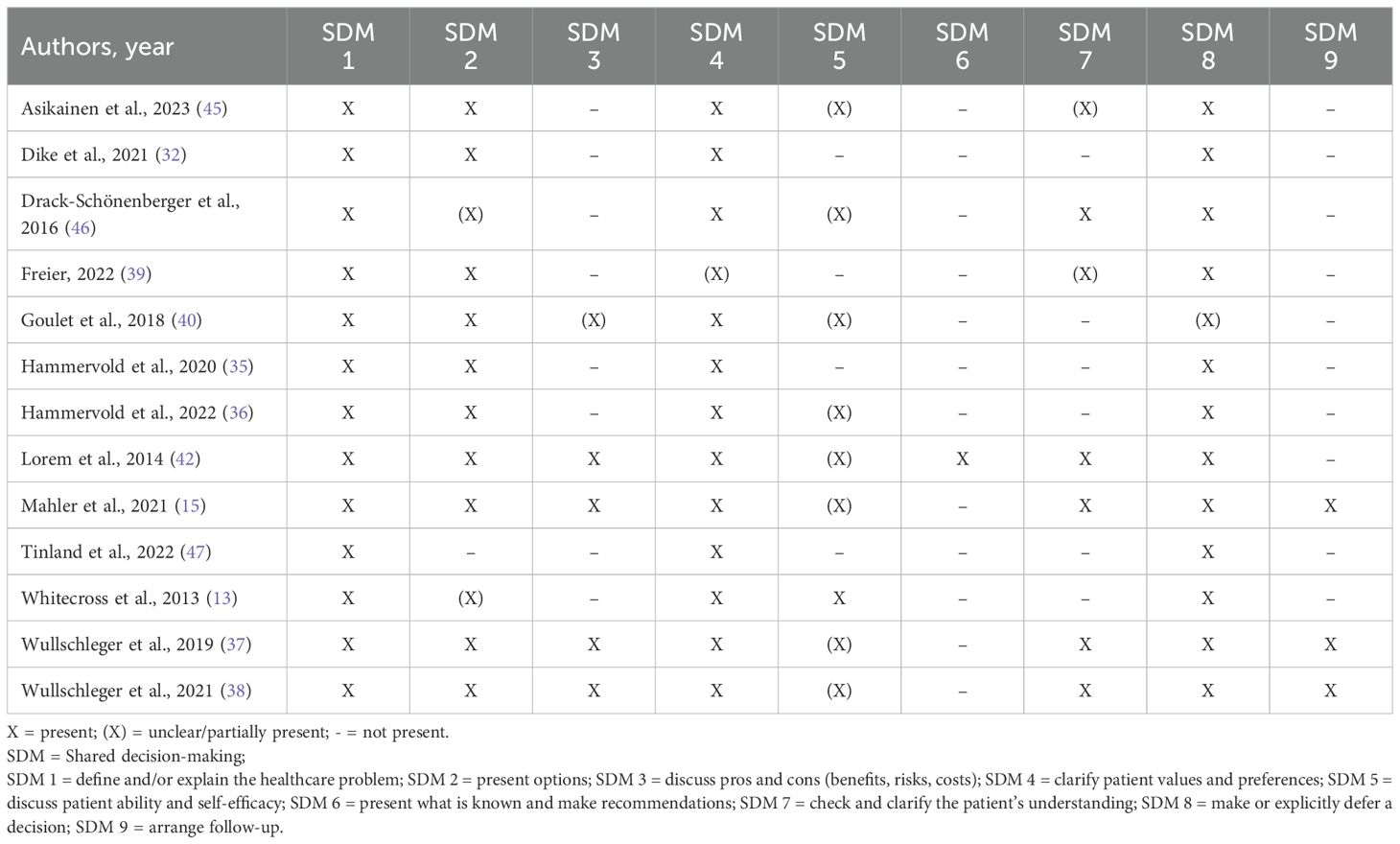
Table 4. SDM elements of the identified post-coercion debriefing interventions.
The other SDM elements were less common, and there was more uncertainty about whether these elements were present, particularly regarding 5.) discussing of patient ability and self-efficacy (n = 9; 69%), 7.) checking and clarifying of the patient’s understanding (n = 7; 54%), and 3.) discussing the pros and cons (n = 5; 38%). The SDM element mentioned in only one article (8%) was 6.) presenting of professional knowledge and recommending of options.
4 Discussion
4.1 Overview of findings
The aim of this scoping review was to examine general characteristics and SDM elements in post-coercion debriefing interventions in psychiatry. Our findings provide additional insights into the extent to which the concept of SDM is already being used in this context.
The main finding from the analysis of the general characteristics was a great variety regarding the participants, the proposed time point of application and the content of the intervention across the articles. As national and international guidelines provide little information on how to conduct debriefings, lack of standards may explain this observation. In addition, the diversity may be well in line with the conclusion of previous research, which also reported on heterogeneity in debriefing intervention elements and the underlying theoretical approaches (10, 15, 41).
Another important finding is the limited extent of SDM elements used in the debriefing interventions. Our review of the literature documents no study that describes a debriefing intervention that fulfills all elements of the analyzed SDM concept. Furthermore, the concept itself is only mentioned by name in one study (42). Interventions may include general qualities of the SDM concept, such as patient participation or the involvement of at least two people, but not necessarily all the essential elements as proposed by Makoul and Clayman’s integrative model of SDM (17).
The heterogeneity in general and in SDM elements makes it more difficult to identify effective elements for the construction of a new tool. However, the interventions described below were particularly interesting because of the extensive description of general intervention characteristics and/or the variety of SDM elements they included. These two debriefing interventions could serve as a useful starting point for what an SDM intervention after coercive measures might look like:
Mahler et al. (15) proposed a debriefing intervention as part of a more complex concept for patient-oriented psychiatry, the ‘Weddinger Modell’ (11). The intervention is attended by the patient, a contact person of the patient (optional) and a care provider involved in the coercive event. A member of the team who was not involved in the coercive event facilitates the 30 to 45-minute guideline-based intervention. The patient determines the preferred time for the debriefing intervention. The debriefing intervention fulfills all SDM elements except for the element 6.) presentation of professional knowledge and recommendation of options. The intervention was also used by other identified literature. A theoretical article by Freier suggested a slightly adapted wording of the intervention (39). Wullschleger et al. investigated the feasibility and effectiveness of the debriefing intervention in a qualitative pilot study (37) and an RCT (38). According to their results, the debriefing intervention was well received and could contribute to reducing the burden of PTSD symptoms in patients with psychotic disorders following a coercive event in an acute setting.
Lorem et al. (42) presented an approach that fulfills all SDM elements except for the element 9.) follow-up, although this was mentioned as a good addition for the future. It is also the only article that clearly included the SDM element 6.) presentation of professional knowledge and the recommendation of options. However, the study focuses on the narrow context of treatment planning for antipsychotic medication without discussing the preceding coercive event in detail and without providing further details on general elements of the intervention.
The findings also support the notion that the debriefing process can include different steps, with partly different goals. Most debriefing interventions focused on a retrospective evaluation of the coercive event, aiming at transparency and emotional relief. In a second step, some interventions moved on to the planning for future care and dealing with possible future coercive events, focusing on preventive goals such as reducing coercive measures in the future. The information and insights from the first step provide the basis for the decision-making process. Both steps may also serve the same goals, such as strengthening the therapeutic relationship. The concept of SDM can be applied mainly in this second step, as this part of the process is aimed at further treatment planning. Therefore, a structured decision aid might be useful to ensure that all elements of SDM are included. This leads to the conclusion that the processual nature of debriefing interventions involving SDM, with different steps and objectives, should be adequately addressed in a new intervention that includes an analysis tool and a structured decision aid.
The review did not identify any digital application of post-coercion debriefing interventions. It remains unclear to what extent elements used in analog applications can be directly adapted.
4.2 Strengths and limitations
A strength of the present review is the systematic literature search with broad search blocks and inclusion criteria that captured a wide range of scientific articles addressing the topic. The overview of general and SDM elements used in the interventions provides a helpful starting point for the development of a new digital DA for debriefing in the context of coercive measures.
However, there may be other studies that addressed the topic of SDM peripherally or through proxies that fell outside the scope of our search, despite the use of many keywords. Most articles discussed issues related to patient participation in decision making at debriefing interventions but did not explicitly aim to adapt the principle of SDM.
The scoping review does not address the quality of evidence by design and therefore provides only a descriptive summary of the available articles on the topic. For the construction of an effective digital decision aid, it will be important to build on elements of evidence-based interventions and to adapt them appropriately. Therefore, it can be recommended to focus mainly on elements of the interventions that have been tested for effectiveness in RCTs.
In addition, we should draw on the expertise of design research in the construction of a digital tool, as no further evidence on this point can be drawn from this review.
5 Conclusions
In general, more research is needed to systematically examine the implementation and clinical effectiveness of post-coercion debriefing interventions. The variety of study designs in this scoping review, ranging from purely theoretical descriptions to RCTs, poses a challenge for the interpretation of the existing evidence, but allows insights into different aspects of interest.
In future studies, it is important to rigorously evaluate different types of debriefing interventions to identify therapeutically effective elements. A more robust understanding of the specific facets of decision making that are most important to patients and health care providers would aid in the development of debriefing interventions. Studies using qualitative methods or mixed-methods approaches may provide better means of elucidating these aspects than quantitative studies.
In addition, it may be essential for further research to include considerations of the impact of psychiatric patients’ decision-making capacities. It has been suggested that most psychiatric patients, including those with severe illnesses such as schizophrenia, may have the capacity to participate in medical decisions related to their illness (43). Nevertheless, patients’ potentially diminished capacity must be addressed. Ensuring a nuanced understanding of SDM in these cases may enhance the development of person-centered decision-making processes (44).
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author.
Author contributions
KF: Data curation, Formal analysis, Investigation, Methodology, Software, Visualization, Writing – review & editing, Writing – original draft. JS: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Software, Supervision, Writing – original draft, Writing – review & editing. CH: Conceptualization, Supervision, Writing – review & editing. MT: Writing – review & editing, Supervision, Project administration, Methodology, Investigation, Conceptualization.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Acknowledgments
The authors would like to thank Christian Appenzeller-Herzog (librarian at the University of Basel) for his expert assistance in developing the search strategy. The authors would also like to thank Fabienne Roth for her helpful comments on the manuscript.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2024.1446619/full#supplementary-material
References
1. Nationaler Verein für Qualitätsentwicklung in Spitälern und Kliniken [ANQ]. Symptombelastung und Freiheitsbeschränkende Massnahmen. Stationäre Psychiatrie Erwachsene: Nationaler Vergleichsbericht 2022. Bern (2023). Available at: https://www.anq.ch/wp-content/uploads/2023/09/ANQpsy_EP_Nationaler-Vergleichsbericht_2022.pdf.
3. Tingleff EB, Bradley SK, Gildberg FA, Munksgaard G, Hounsgaard L. Treat me with respect”. A systematic review and thematic analysis of psychiatric patients’ reported perceptions of the situations associated with the process of coercion. J Psychiatr Ment Health Nurs. (2017) 24:681–98. doi: 10.1111/jpm.12410
4. Chieze M, Hurst S, Kaiser S, Sentissi O. Effects of seclusion and restraint in adult psychiatry: A systematic review. Front Psychiatry. (2019) 10:491. doi: 10.3389/fpsyt.2019.00491
5. Jankovic J, Yeeles K, Katsakou C, Amos T, Morriss R, Rose D, et al. Family caregivers’ experiences of involuntary psychiatric hospital admissions of their relatives - a qualitative study. PloS One. (2011) 6:e25425. doi: 10.1371/journal.pone.0025425
6. Bruns H, Gather J, Henking T, Vollmann J. Überlegungen aus klinisch-ethischer Perspektive. In: Henking T, Vollmann J, editors. Zwangsbehandlung psychisch kranker Menschen. Berlin, Heidelberg: Springer-Verlag Berlin Heidelberg (2015). p. 92–114.
7. Gooding P. Compendium report: Good Practices in the Council of Europe to Promote Voluntary Measures in Mental Health Services. Council of Europe (2021).
8. Steinert T, Hirsch S. S3-Leitlinie Verhinderung von Zwang: Prävention und Therapie aggressiven Verhaltens bei Erwachsenen. Nervenarzt. (2020) 91:611–6. doi: 10.1007/s00115-019-00801-2
9. Hirsch S, Steinert T. Measures to avoid coercion in psychiatry and their efficacy. Dtsch Arztebl Int. (2019) 116:336–43. doi: 10.3238/arztebl.2019.0336
10. Krieger E, Fischer R, Moritz S, Nagel M. Strukturierte Nachbesprechung von Zwangsmaßnahmen mit Patienten – Überblick und aktueller Stand. Nervenarzt. (2021) 92:44–9. doi: 10.1007/s00115-020-00969-y
11. Mahler L, Oster A, Vandamme A. Das Weddinger modell. Nervenheilkunde. (2021) 40:430–5. doi: 10.1055/a-1389-7279
12. National Association of State Mental Health Program Directors. Six Core Strategies to Reduce Seclusion and Restraint Use. Alexandria: National Association of State Mental Health Program Directors (NASMHPD) (2008).
13. Whitecross F, Seeary A, Lee S. Measuring the impacts of seclusion on psychiatry inpatients and the effectiveness of a pilot single-session post-seclusion counselling intervention. Int J Ment Health Nurs. (2013) 22:512–21. doi: 10.1111/inm.12023
14. Wullschleger A, Vandamme A, Mielau J, Stoll L, Heinz A, Bermpohl F, et al. Effect of standardized post-coercion review on subjective coercion: Results of a randomized-controlled trial. Eur Psychiatry. (2021) 64:e78. doi: 10.1192/j.eurpsy.2021.2256
15. Mahler L, Wullschleger A, Oster A. Nachbesprechung von Zwangsmaβnahmen – Ein Praxisleitfaden. Köln: Psychiatr Verlag. (2021).
16. Ling S, Cleverley K, Perivolaris A. Understanding mental health service user experiences of restraint through debriefing: A qualitative analysis. Can J Psychiatry. (2015) 60:386–92. doi: 10.1177/070674371506000903
17. Makoul G, Clayman ML. An integrative model of shared decision making in medical encounters. Patient Educ Couns. (2006) 60:301–12. doi: 10.1016/j.pec.2005.06.010
18. Schmolke M, Amering M, Svettini A. Recovery, empowerment, and person centeredness. In: Mezzich JE, Botbol M, Christodoulou GN, Cloninger CR, Salloum IM, editors. Person Centered Psychiatry. Springer International Publishing, Cham (2016). p. 97–111.
19. Mead N, Bower P. Patient-centredness: a conceptual framework and review of the empirical literature. Soc Sci Med. (2000) 51:1087–110. doi: 10.1016/s0277-9536(00)00098-8
20. Gurtner C, Schols JMGA, Lohrmann C, Halfens RJ, Hahn S. Conceptual understanding and applicability of shared decision-making in psychiatric care: An integrative review. J Psychiatr Ment Health Nurs. (2021) 28:531–48. doi: 10.1111/jpm.12712
21. Chmielowska M, Zisman-Ilani Y, Saunders R, Pilling S. Trends, challenges, and priorities for shared decision making in mental health: The first umbrella review. Int J Soc Psychiatry. (2023) 69:823–40. doi: 10.1177/00207640221140291
22. de Jong MH, Kamperman AM, Oorschot M, Priebe S, Bramer W, van de Sande R, et al. Interventions to reduce compulsory psychiatric admissions: A systematic review and meta-analysis. JAMA Psychiatry. (2016) 73:657–64. doi: 10.1001/jamapsychiatry.2016.0501
23. Barbui C, Purgato M, Abdulmalik J, Caldas-de-Almeida JM, Eaton J, Gureje O, et al. Efficacy of interventions to reduce coercive treatment in mental health services: umbrella review of randomised evidence. Br J Psychiatry. (2021) 218:185–95. doi: 10.1192/bjp.2020.144
24. Burn E, Conneely M, Leverton M, Giacco D. Giving patients choices during involuntary admission: A new intervention. Front Psychiatry. (2019) 10:433. doi: 10.3389/fpsyt.2019.00433
25. Hamann J, John M, Holzhüter F, Siafis S, Brieger P, Heres S. Shared decision making, aggression, and coercion in inpatients with schizophrenia. Eur Psychiatry. (2020) 63:e90. doi: 10.1192/j.eurpsy.2020.88
26. Sugiura K, Pertega E, Holmberg C. Experiences of involuntary psychiatric admission decision-making: a systematic review and meta-synthesis of the perspectives of service users, informal carers, and professionals. Int J Law Psychiatry. (2020) 73:101645. doi: 10.1016/j.ijlp.2020.101645
27. van Kranenburg GD, Diekman WJ, van den Brink RH, Mulder WG, Pijnenborg GH, Mulder CL. Determinants of quality of life and treatment satisfaction during long-term involuntary in-patient treatment of dual-diagnosis patients. Front Psychiatry. (2022) 13:801826. doi: 10.3389/fpsyt.2022.801826
28. Giacco D, Mavromara L, Gamblen J, Conneely M, Priebe S. Shared decision-making with involuntary hospital patients: a qualitative study of barriers and facilitators. BJPsych Open. (2018) 4:113–8. doi: 10.1192/bjo.2018.6
29. Park M, Doan TT-T, Jung J, Giap T-T-T, Kim J. Decision aids for promoting shared decision-making: A review of systematic reviews. Nurs Health Sci. (2024) 26:e13071. doi: 10.1111/nhs.13071
30. Lopez-Olivo MA, Suarez-Almazor ME. Digital patient education and decision aids. Rheum Dis Clin North Am. (2019) 45:245–56. doi: 10.1016/j.rdc.2019.01.001
31. Vitger T, Korsbek L, Austin SF, Petersen L, Nordentoft M, Hjorthøj C. Digital shared decision-making interventions in mental healthcare: A systematic review and meta-analysis. Front Psychiatry. (2021) 12:691251. doi: 10.3389/fpsyt.2021.691251
32. Peters MD, Marnie C, Tricco AC, Pollock D, Munn Z, Alexander L, et al. Updated methodological guidance for the conduct of scoping reviews. JBI Evid Synth. (2020) 18:2119–26. doi: 10.11124/JBIES-20-00167
33. Tricco AC, Lillie E, Zarin W, O’Brien KK, Colquhoun H, Levac D, et al. PRISMA extension for scoping reviews (PRISMA-scR): checklist and explanation. Ann Intern Med. (2018) 169:467–73. doi: 10.7326/M18-0850
34. Dike CC, Lamb-Pagone J, Howe D, Beavers P, Bugella BA, Hillbrand M. Implementing a program to reduce restraint and seclusion utilization in a public-sector hospital: Clinical innovations, preliminary findings, and lessons learned. Psychol Serv. (2021) 18:663–70. doi: 10.1037/ser0000502
35. Hammervold UE, Norvoll R, Vevatne K, Sagvaag H. Post-incident reviews-a gift to the Ward or just another procedure? Care providers’ experiences and considerations regarding post-incident reviews after restraint in mental health services. A qualitative study. BMC Health Serv Res. (2020) 20:499. doi: 10.1186/s12913-020-05370-8
36. Hammervold UE, Norvoll R, Sagvaag H. Post-incident reviews after restraints-Potential and pitfalls. Patients’ experiences and considerations. J Psychiatr Ment Health Nurs. (2022) 29:472–83. doi: 10.1111/jpm.12776
37. Wullschleger A, Vandamme A, Ried J, Pluta M, Montag C, Mahler L. Standardisierte Nachbesprechung von Zwangsmaßnahmen auf psychiatrischen Akutstationen: Ergebnisse einer Pilotstudie. Psychiatr Prax. (2019) 46:128–34. doi: 10.1055/a-0651-6812
38. Wullschleger A, Vandamme A, Mielau J, Renner L, Bermpohl F, Heinz A, et al. Effect of standardized post-coercion review session on symptoms of PTSD: results from a randomized controlled trial. Eur Arch Psychiatry Clin Neurosci. (2021) 271:1077–87. doi: 10.1007/s00406-020-01215-x
40. Goulet M-H, Larue C, Lemieux AJ. A pilot study of “post-seclusion and/or restraint review” intervention with patients and staff in a mental health setting. Perspect Psychiatr Care. (2018) 54:212–20. doi: 10.1111/ppc.12225
41. Goulet M-H, Larue C. Post-seclusion and/or restraint review in psychiatry: A scoping review. Arch Psychiatr Nurs. (2016) 30:120–8. doi: 10.1016/j.apnu.2015.09.001
42. Lorem GF, Frafjord JS, Steffensen M, Wang CE. Medication and participation: A qualitative study of patient experiences with antipsychotic drugs. Nurs Ethics. (2014) 21:347–58. doi: 10.1177/0969733013498528
43. Calcedo-Barba A, Fructuoso A, Martinez-Raga J, Paz S, Sánchez de Carmona M, Vicens E. A meta-review of literature reviews assessing the capacity of patients with severe mental disorders to make decisions about their healthcare. BMC Psychiatry. (2020) 20:339. doi: 10.1186/s12888-020-02756-0
44. El-Alti L. Shared decision making in psychiatry: dissolving the responsibility problem. Health Care Anal. (2023) 31:65–80. doi: 10.1007/s10728-022-00451-7
45. Asikainen J, Vehviläinen-Julkunen K, Repo-Tiihonen E, Louheranta O. Use of debriefing following restrictive practices in forensic psychiatric care. JFP. (2023) 25:46–56. doi: 10.1108/JFP-08-2022-0040
46. Drack-Schönenberger T, Bleiker M, Lengler S, Blank C, Rössler W, Lay B. Krisenkarten zur Prävention von Zwangseinweisungen. Psychiatr Prax. (2016) 43:253–9. doi: 10.1055/s-0034-1387549
47. Tinland A, Loubière S, Mougeot F, Jouet E, Pontier M, Baumstarck K, et al. Effect of psychiatric advance directives facilitated by peer workers on compulsory admission among people with mental illness: A randomized clinical trial. JAMA Psychiatry. (2022) 79:752–9. doi: 10.1001/jamapsychiatry.2022.1627
Keywords: coercion, debriefing, shared decision-making, psychiatry, decision aids, scoping review
Citation: Froelich K, Schürmann J, Huber CG and Trachsel M (2024) Shared decision-making in post-coercion debriefing interventions in psychiatry – a scoping review. Front. Psychiatry 15:1446619. doi: 10.3389/fpsyt.2024.1446619
Received: 10 June 2024; Accepted: 30 August 2024;
Published: 27 September 2024.
Edited by:
Armida Mucci, University of Campania Luigi Vanvitelli, ItalyReviewed by:
Dirk Richter, Universitäre Psychiatrische Dienste Bern, SwitzerlandJack Tomlin, University of Greenwich, United Kingdom
Copyright © 2024 Froelich, Schürmann, Huber and Trachsel. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Manuel Trachsel, bWFudWVsLnRyYWNoc2VsQHVuaWJhcy5jaA==