 Xiaofen Ding1
Xiaofen Ding1 Jinlong Wu
Jinlong Wu Dong Li
Dong Li Zexi Liu
Zexi Liu
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Psychiatry , 27 September 2024
Sec. Social Psychiatry and Psychiatric Rehabilitation
Volume 15 - 2024 | https://doi.org/10.3389/fpsyt.2024.1436170
This article is part of the Research Topic The Arts Therapies and Neuroscience View all 20 articles
Objective: Individuals with autism spectrum disorder (ASD) exhibit impaired behavior synchronization, which is associated with social deficits. Numerous studies have demonstrated that rhythm-based interventions can effectively mitigate social deficits by promoting behavioral synchronization in individuals with ASD. Therefore, a review of the current literature is warranted in this field. The objectives of this review were to explore the effects of rhythm-based interventions on overall social skills and to study the differences in the effects of rhythm-based interventions on specific social skills.
Method: The databases PubMed, Web of Science, Scopus, and Psycinfo were systematically explored until March 2024. A total of eleven research studies, encompassing 408 participants diagnosed with ASD, were incorporated into the meta-analysis. Effect sizes (Hedges’ g) were computed for each comparison and amalgamated using random-effects models to evaluate the social skills of individuals with ASD. The methodological quality of each study was evaluated using the Physiotherapy Evidence Database scale(PEDro).
Results: Overall, some valuable observations were made. Rhythm-based interventions had a medium effect on the overall social skills for ASD (Hedges’s=0.681; 95%CI[0.075 to 1.286], P < 0.05). Regarding domain-specific social skills, rhythm-based interventions had a large effect on social interaction (g = 1.299,95% CI [0.508 to 2.091]), a small effect on communication (g = 0.383, 95% CI [0.033 to 0.733], P < 0.05), and a large effect on emotion (g = 1.752, 95% CI [0.294 to 3.210], P < 0.05). However, we found a favorable but non-significant effect (g = 0.125, 95% CI [-0.039 to 0.289], P > 0.05) of rhythm-based interventions on empathy. All study qualities were high (score≥6) using the Physiotherapy Evidence Database (PEDro) scale assessment.
Conclusion: This result indicates the importance of rhythm in the clinical rehabilitation of individuals with ASD. We suggest adding appropriate rhythmic elements to clinical interventions, particularly for individuals with ASD who are less socially competent.
Autism spectrum disorder (ASD), a pervasive neurodevelopmental disorder, is distinguished by challenges in social communication and interaction, in addition to repetitive behaviors, interests, and activities that may persist throughout one’s life (1). The prevalence of ASD has increased in recent decades, with 1 in 59 children in the United States and over 600,000 people in the United Kingdom, equivalent to a population prevalence of ∼1% (2). Continuing deficits in social communication and social development can be highly problematic for individuals diagnosed with ASD (3). These difficulties can impact a person’s ability to initiate social interactions, engage in reciprocal conversation, and maintain eye contact and joint attention (4, 5). Such challenges can lead to difficulties in forming and maintaining relationships, ultimately resulting in feelings of social isolation, loneliness, and a diminished quality of life (6).
Researchers has been focused on improving communication and social skills in children with ASD through evidence-based therapeutic interventions (7). Recent studies have been found rhythm-based interventions show several positive effects that enhance communication skills and develop social interactions in individuals with ASD (8–10). These rhythm-based interventions typically encompass a strong, consistent, and recurrent pattern of movement or sound (11–13). Strong rhythmic patterns can may trigger behavioral, neurological, and physiological rhythm changes in individuals with ASD that promote social connections (14). First, some studies found that after the rhythm-based intervention, the synchronization of social movement will be significantly improved for individuals with ASD (15, 16). Second, brain imaging studies have confirmed that rhythmic experiences is closely related to neural synchronization and play a key role in developing basic trust and feelings of connection with others (17, 18). A studies found compared to key-press task alone, rhythmic keystrokes can improve interbrain synchronization between children with ASD and their parents (19). Three, one study showed the act of dancing to music has been proven to trigger physiological synchronization, specifically in terms of heart rate intervals (20). Therefore, incorporating aspects of rhythm cues into interventions for patients with ASD holds great promise mainly because of the increasing emphasis on sensorimotor function in interventions for this population.
Rhythmic-based interventions (such as music and dance therapy) have increasingly emerged as promising compensation methods that can positively affect negative symptoms in individuals with ASD. A meta-analysis (21) showed that dance practice significantly alleviated the overall symptoms of ASD (standardized mean difference (SMD)=−1.48, 95%confidence interval(CI)[−2.55, −0.42], P =0.006, I2 = 75%) and improved social interaction(SMD=0.88, 95%CI [0.46 to1.30], P <0.0001, I2 = 0%), but had no significant effect on empathy (SMD=0.09, 95%CI [−0.25 to 0.42], P =0.61, I2 = 2%). Another recent meta-analysis (22) showed that music therapy was associated with a significant increase in social reactions among children with ASD (SMD=0.24, 95%CI [0.03, 0.46], I2 = 0%, P=0.03). However, music therapy did not elicit a significant increase in symptom severity (SMD=0.17, 95%CI[−0.04 to 0.38], I2 = 0%, P=0.12), social adaptive behavior (SMD=0.02, 95%CI[−0.44, 0.48], I2 = 0%, P=0.93), or speech (SMD=0.04, 95%CI[−0.39 to 0.47], I2 = 0%, P=0.86) in children with ASD.
Nonetheless, we have identified three gaps in the literature. First, previous studies rarely focused on the importance of rhythmic effects on social skills in individuals with ASD. Second, few reviews have distinguished between specific types of social skills (i.e., communication, social interaction, or emotion). It is difficult to identify the effects of rhythmic-based interventions on specific types of social skills among individuals with ASD. Furthermore, past reviews and meta-analyses had limitations including small sample sizes, absence of a control group, and study designs such as case studies or single-subject research lacking outcome measures.
Considering the crucial role of rhythm-based intervention for individuals with ASD in enhancing social skills. To better understand the effects of rhythmic interventions on social skills, a review of the current literature is warranted. The aim of the present meta-analysis, therefore, is to quantitatively evaluate the most recent studies on the effects of rhythm-based interventions on social skills of ASD individuals. It helps clinicians and rehabilitators design better intervention programs with key treatment factors for individuals with ASD. Consequently, the objectives of this review were to explore the effect of rhythm-based interventions on overall social skills and to study the effect of rhythm-based interventions on specific social skills.
The meta-analysis complied with the Preferred Reporting Items for Systematic Reviews and Meta-analyses(PRISMA) reporting checklist (23). Detailed search terms are shown in Supplementary Table 1.
We systematically searched the literature on the effect of rhythm-based interventions on social interaction skills for patients with ASD in PubMed, Web of Science, Scopus, and Psycinfo from the beginning of database construction of each database until March 2024. Our search strategy combined terms related to rhythm-based interventions (such as music, dance, or drums) and ASD. Additionally, we conducted a thorough manual search of the reference lists in all studies that were included, along with a comprehensive review to uncover additional pertinent articles (4, 21, 22, 24–27). Detailed search terms are shown in Supplementary Table 2.
The quantitative synthesis for meta-analysis included only randomized controlled trials (RCTs) published in peer-reviewed English journals and reporting sufficient statistical details. Studies that did not involve comparison groups or did not provide comparison results between groups were not considered. Observational studies and other types of non-RCTs, such as cross-sectional, case-control, and cohort studies, as well as reviews, reports, papers, and policy documents, were excluded from the analysis.
The study focused on individuals diagnosed with ASD based on the criteria in the DSM (The Diagnostic and Statistical Manual of Mental Disorders) or other standardized diagnostic measures. There were no age restrictions. Excluded were studies that included participants with various disabilities that made it difficult to separate data relevant to children and adolescents with ASD. The main inclusion was any form of intervention that included rhythmic experiences, such as singing, playing the piano, drumming, etc., to the exclusion of other types of auditory stimuli that did not include rhythm. The studies that were not considered auditory interventions. Studies have measured social skill outcomes using validated instruments, such as communication questionnaires, emphasizing social skills.
Records that align with the specified search criteria will be imported into Endnote 20 software (Clarivate Inc., Philadelphia, PA, USA) for deduplication purposes. Two reviewers independently undertook the multi-step search process, evaluating studies based on titles, abstracts, and full texts to carry out an initial review. Any discrepancies between the reviewers were deliberated upon until consensus was achieved. If no agreement could be reached, a third reviewer intervened, making a conclusive decision after consultation with the original two reviewers. The agreement between the two reviewers during abstract and full-text screening was quantified using kappa values, in accordance with prior guidelines. The specific reasons for excluding full-text studies are detailed in Supplementary Table 3.
A standardized data extraction form was developed to meticulously collect and document the characteristics of each study. To ensure the accuracy and reliability of the data extraction process, it was performed independently by two reviewers. In instances where discrepancies arose, a third reviewer was involved to independently perform data extraction for resolution. The data collected encompassed a variety of crucial elements, including bibliographic details such as the author and year of publication, country/regions, participant characteristics like diagnostic criteria, sample age, sex, and sample size, as well as detailed descriptions of the intervention components, which covered the design, intensity, frequency, and length of the intervention, along with its setting. Information on the control group, outcome measures, and any relevant data was also meticulously documented. When certain relevant data were not available in the original papers, email inquiries were made to the corresponding authors to obtain the missing information. In cases where there was no response or the data could not be provided, the missing information was marked as “not applicable” (N.A.). Additionally, the ImageJ processing program (Version 1.50i, https://imagej.nih.gov/ij/) was employed to calculate the pixel value statistics for the defined selections and to extract numerical data from the figures.
Two reviewers independently assessed the methodological quality of each study included in the analysis using the PEDro scale, which comprises 11 criteria related to eligibility, randomization, allocation, blinding of subjects and experimenters, intention-to-treat analysis, between-group comparisons, and outcome measures (28). The scores on the PEDro scale range from 0 to 11, with a median score of 6. Studies were categorized as excellent (9–10 points), good (6–8 points), fair (4–5 points), or poor (less than 4 points) quality (29). Any discrepancies in quality ratings between reviewers were resolved through discussion until a consensus was reached, with a third researcher intervening if necessary to make the final decision.
A meta-analysis was carried out to investigate the impact of exercise interventions on EFs. SMDs with 95% CIs were calculated for each study when utilizing different tools to assess outcome variables. The SMDs were determined and weighted based on the inverse variance of the study, taking into account sample sizes, outcomes, and cognitive measures. A random-effects model was applied to calculate potential effect sizes that were distributed heterogeneously, utilizing sampling error and between-study variance for effect size estimation (30).
Hedges’ served as the effect size indicator to address potential overestimation when fewer than 20 studies were included (31). The magnitude of Hedges’ values was categorized as small (Hedges’ g = 0.2–0.5), moderate (Hedges’ g = 0.5–0.8), and large effect (Hedges’ g > 0.8) (32). Statistical heterogeneity was assessed using I2 and the p-value for Q statistics, with I2 values representing low (≤ 25%), moderate (50%), or high (≥ 75%) levels of heterogeneity. Due to the inclusion of fewer than ten studies in each analysis, publication bias was not explored (33). The analysis was conducted utilizing the Comprehensive Meta-analysis version 3 software (Biostat, USA) (34).
Figure 1 shows the detailed article screening process. The initial search identified 4674 records from electronic databases using our literature search strategy (PubMed, n=714; Embase, n=515; PsycInfo, n=800; Scopus, n=2646). After deleting 1394 duplicate records using Endnote software, 3280 were screened. The manual deleted 590 duplicate records by a reviewer, and 2691 records were included. Of which, 2578 did not meet the inclusion criteria of this study based on their titles and abstracts. Finally, the full-text articles of 33 studies were screened; 22 were excluded, and 11 (35–45) were included in the present meta-analysis (Figure 1).
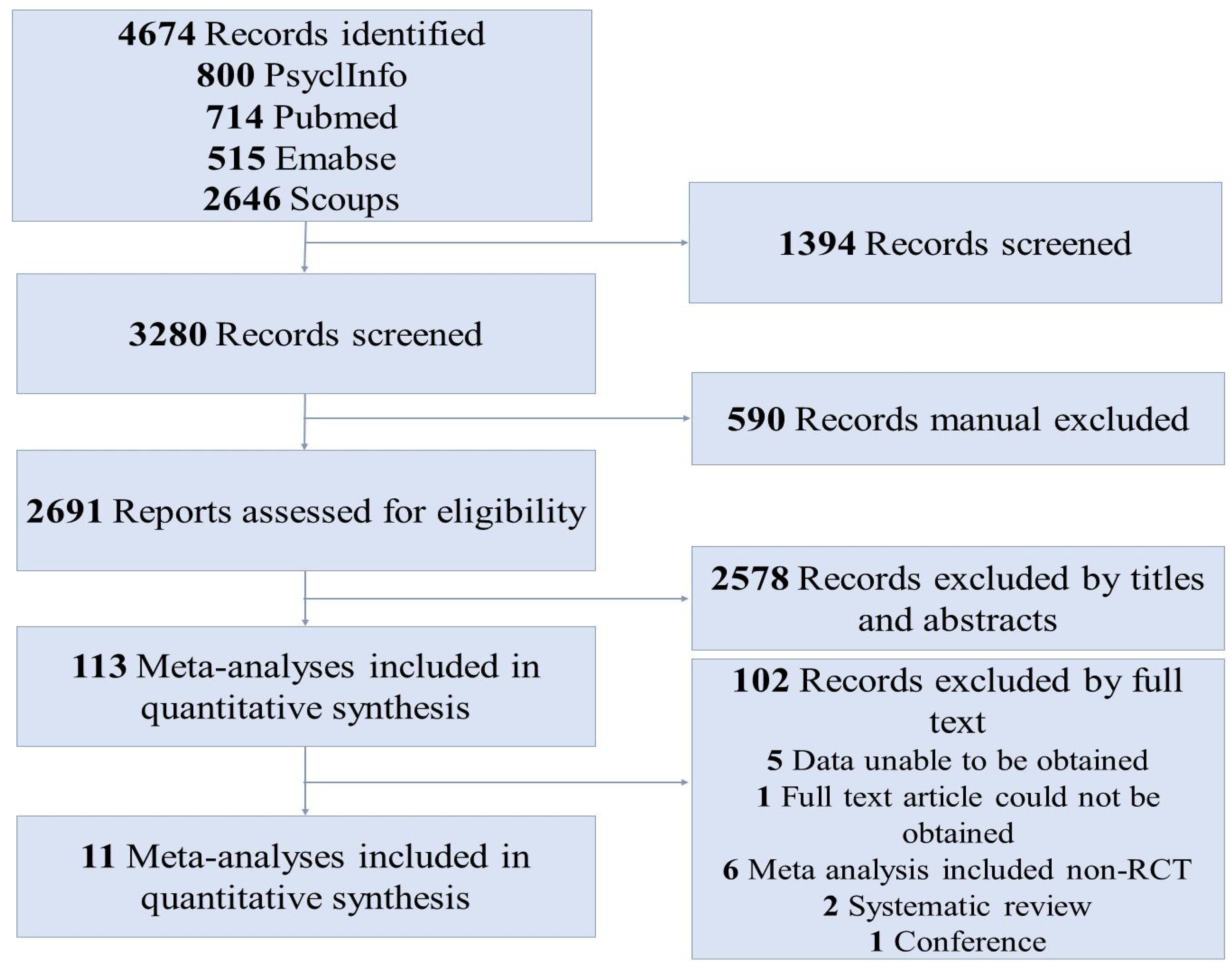
Figure 1. Flow diagram of the article screening process.
The characteristics of each study are summarized in Table 1. 11 (35–45) studies were included in this meta-analysis published from 2014 to 2023, suggesting that rhythm-based interventions for social skills in individuals with ASD have been explored constantly in this field. Of the included interventions, four (35, 39, 40, 42) were conducted in the Germany, two (41, 44) were conducted in USA. The remaining intervention studies were conducted in Iran (38), Canada (43), India (36), Brazil (45), and Romani (37).
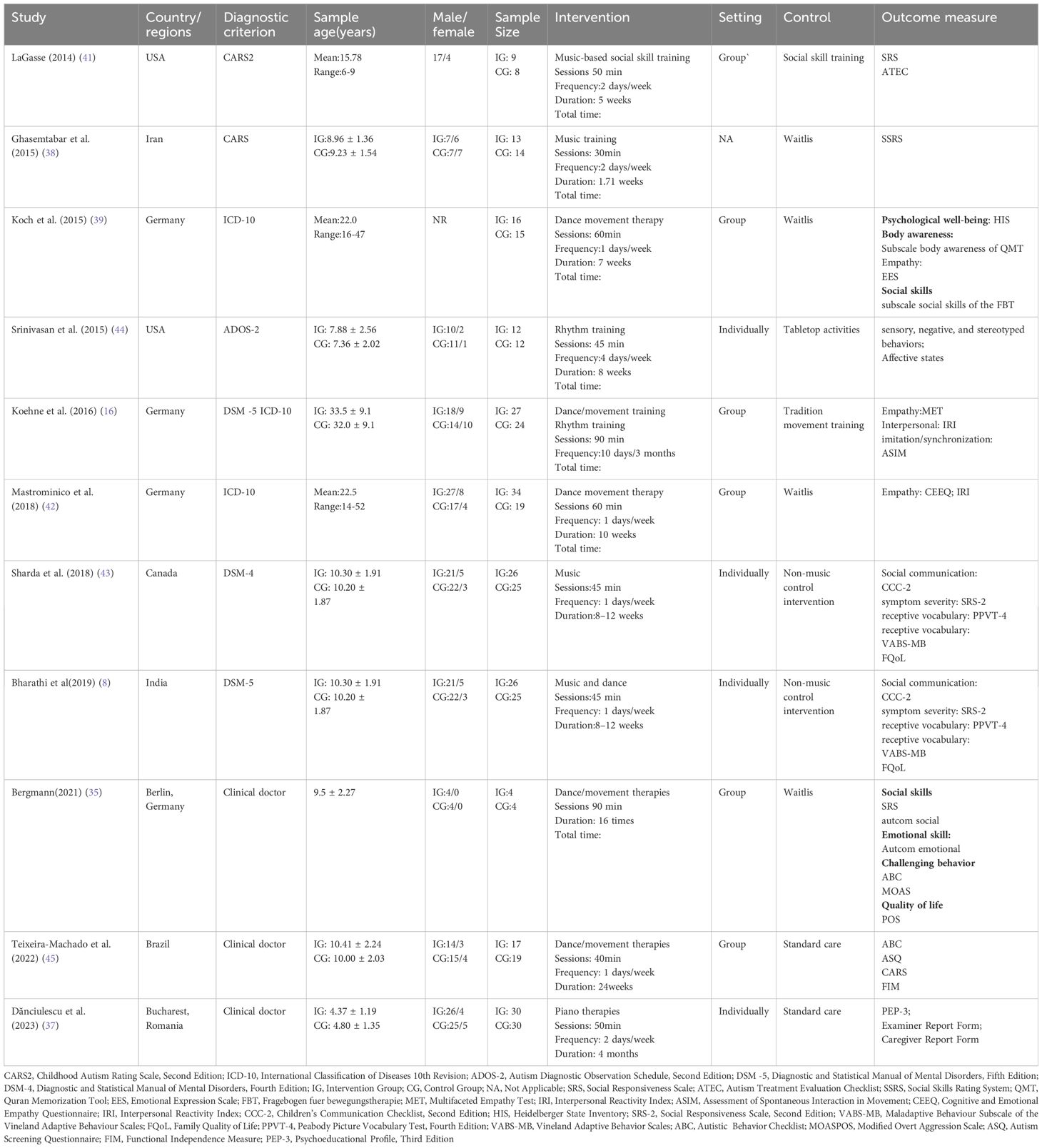
Table 1. Study characteristics meeting inclusion criteria.
The total sample size included in this meta-analysis was 408 participants, including both experimental (n=214) and control (n=195) groups. Eight studies (36, 38–44) focused on participants with official ASD diagnoses based on the established diagnostic criteria, while three studies (35, 37, 45) did not provide specific details regarding the methods used for ASD diagnosis. The participants ranged from preschool children to adults. Music, dance, rhythm, and piano training were used as interventions in the experimental group, and Waitlis, social skill training, tabletop activities, traditional movement training, non-music control intervention, and traditional care were conducted in the experimental group—intervention settings, including the group and individual. The intervention frequency ranged from one to four times per week, each lasting 30–90 min. It is important to note that session time here refers to the total intervention time, not the rhythm-based intervention. The current systematic review conducted an extensive search strategy to investigate the potential significance of rhythm information for individuals diagnosed with ASD. A total of 11 studies were incorporated in the systematic review, offering valuable insights for enhancing rehabilitation programs for individuals with ASD.
The main outcomes of this meta-analysis are described in Table 2 and Figures 2–6. Studies investigating the effects of rhythm-based interventions on social skills in individuals with ASD (n = 248) were identified as suitable for and included in the meta-analysis. Of the five (35, 36, 38, 39, 43) studies with eight outcomes that evaluated rhythm-based interventions on overall social skills, the results presented in Figure 2 indicate a medium effect size for individuals with ASD on overall social skills (g= 0.681; 95%CI[0.075 to 1.286], P < 0.05) with high heterogeneity. Two (36, 45) studies with six outcomes evaluated social interaction, and the results showed that rhythm-based interventions had a large effect on the social interaction of individuals with ASD (g = 1.299; 95%CI[0.508–2.091], P < 0.05) with high heterogeneity. Three (37, 40, 45) studies with five outcomes revealed large effects of rhythm-based interventions on communication (g = 1.522, 95% CI [0.631 to 2.414], P < 0.05) in tandem with high heterogeneity. Three (35, 44, 45) studies with six outcomes concentrated on emotion specified significantly large effects(g = 1.752, 95% CI [0.294–3.210], P < 0.05) with high heterogeneity. In addition, four (36, 39, 40, 42) studies with 11 outcomes showed a favorable but non-significant effect (g=0.125, 95% CI [-0.039 to 0.289], P > 0.05) of rhythm-based interventions on empathy in individuals with ASD with low heterogeneity.
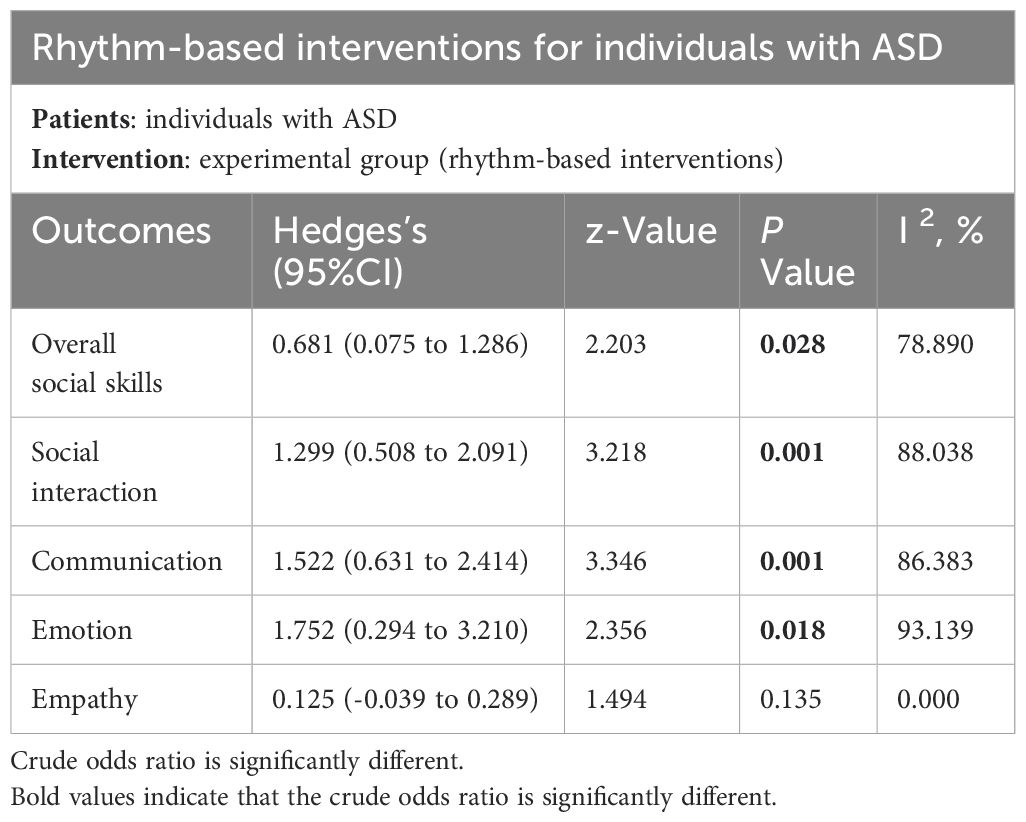
Table 2. Summary of the effect of the rhythm-based interventions for individuals with ASD.
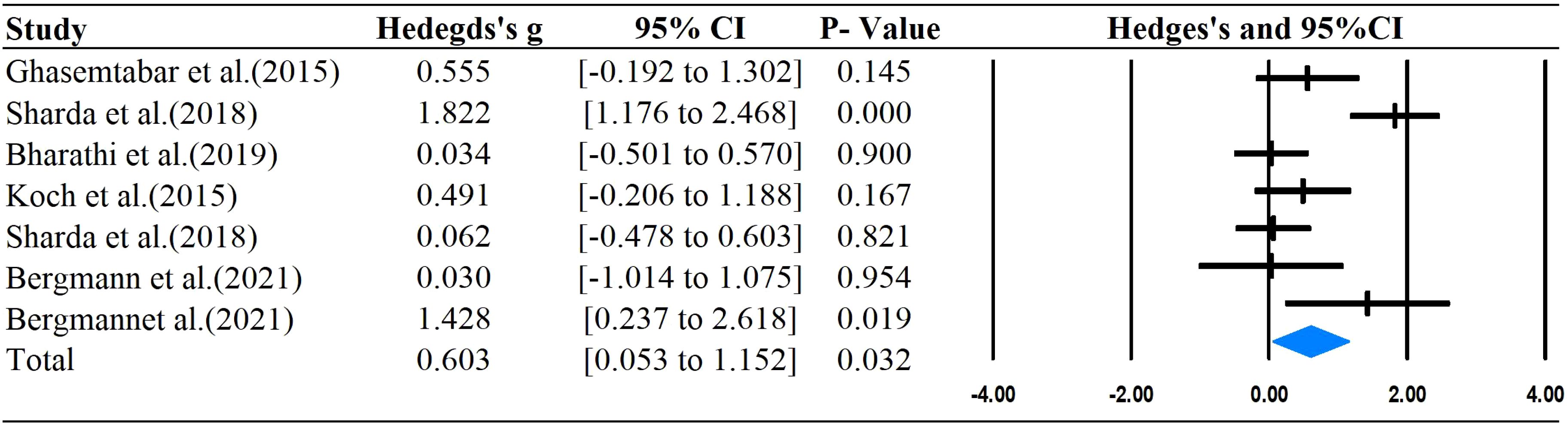
Figure 2. Forest plots for the effect of rhythm-based interventions on overall social skills.
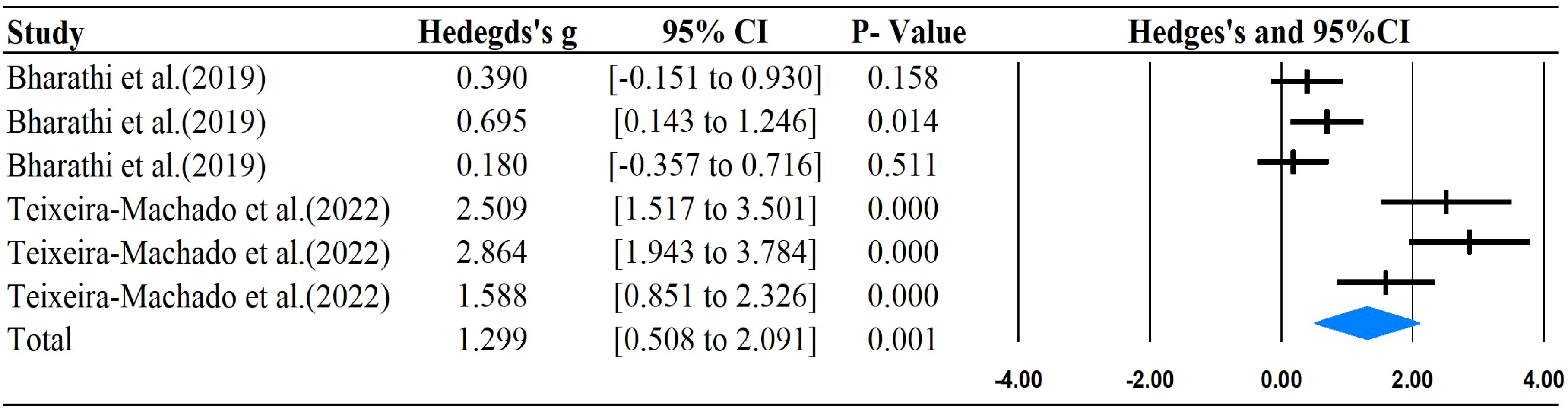
Figure 3. Forest plots for the effect of rhythm-based interventions on social interaction.
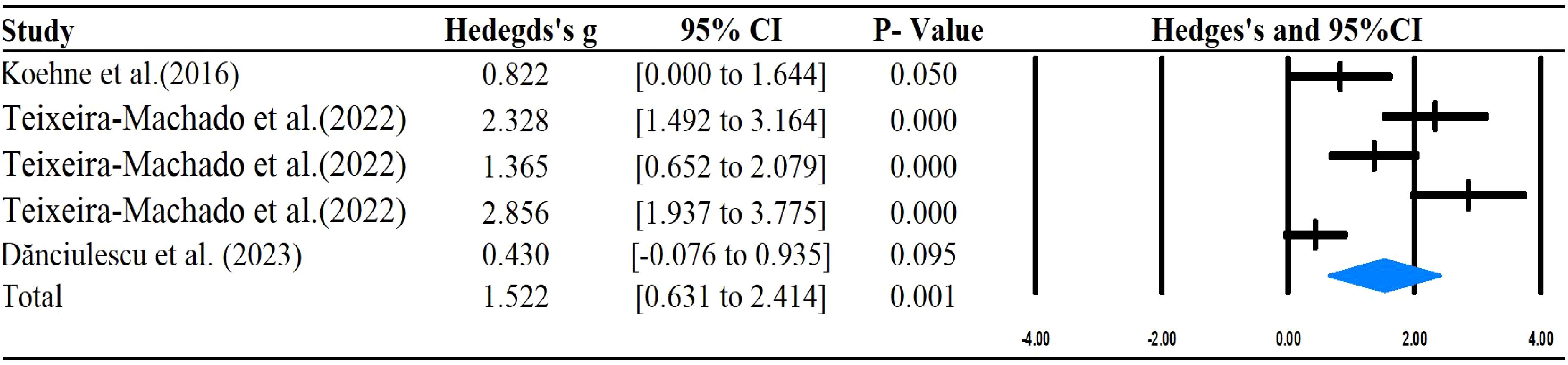
Figure 4. Forest plots for the effect of rhythm-based interventions on communication.
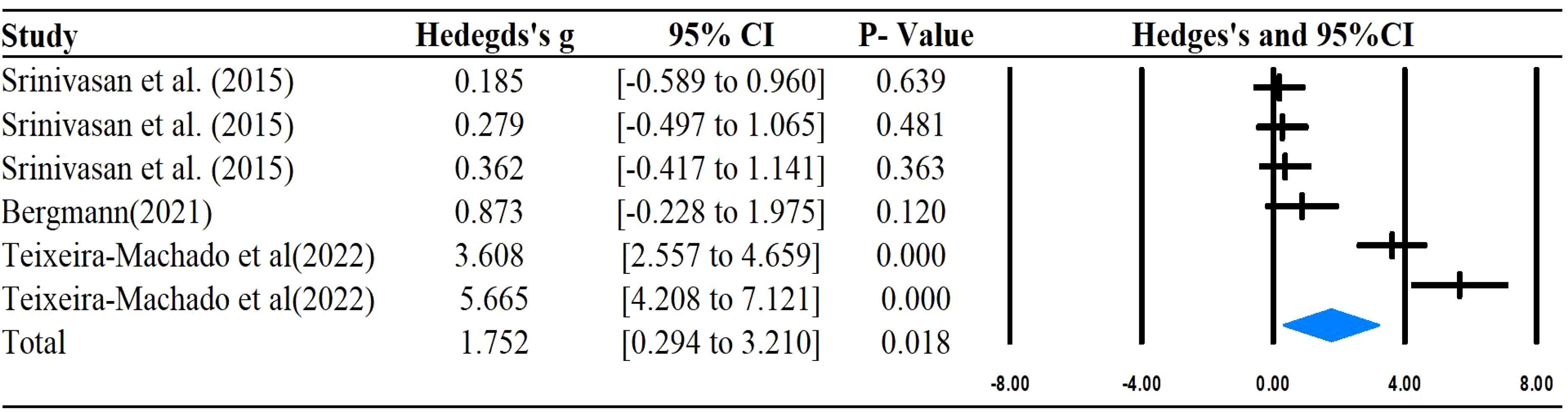
Figure 5. Forest plots for the effect of rhythm-based interventions on emotion.
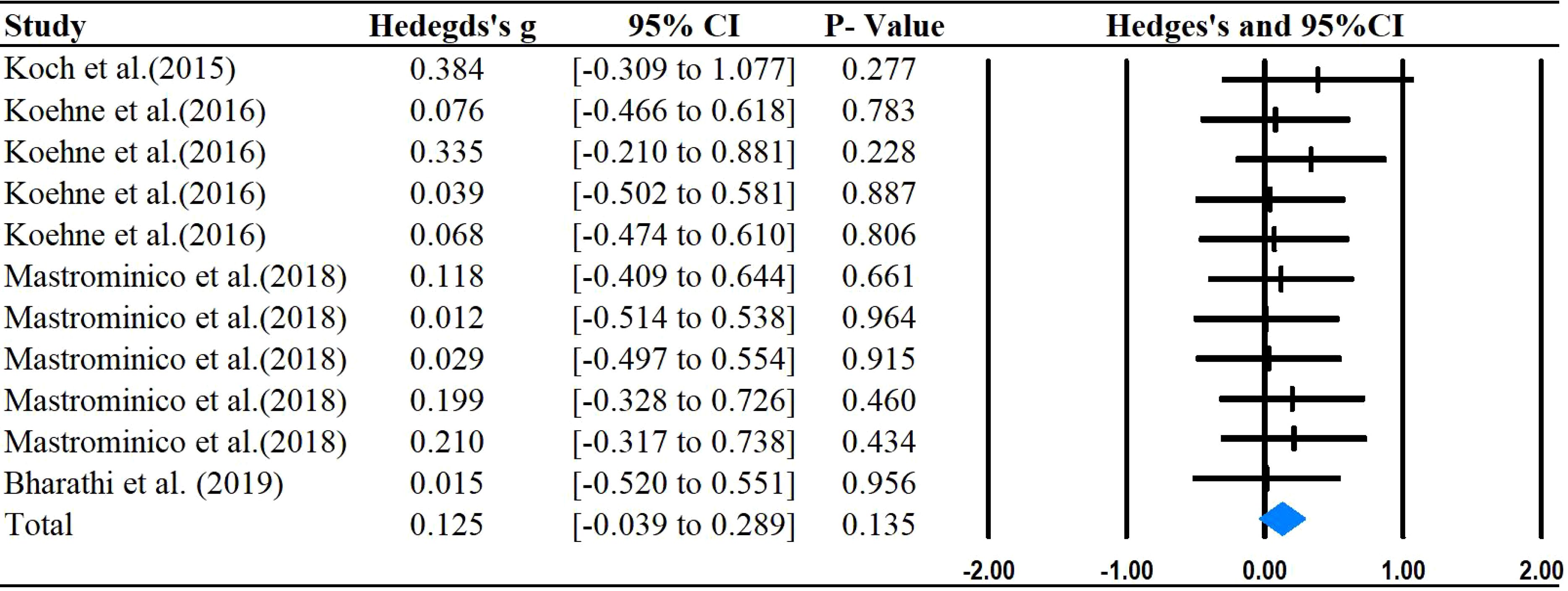
Figure 6. Forest plots for the effect of rhythm-based interventions on empathy.
Table 3 provides an evaluation of the quality of the studies included in the analysis. On average, the studies exhibited a high level of quality, with a mean quality score of 7. Many of the studies received lower marks due to the absence of blinding, which is often unavoidable in exercise intervention trials given the study design. Scoring two points for the blinding of participants and therapists involved in these interventions is particularly difficult.
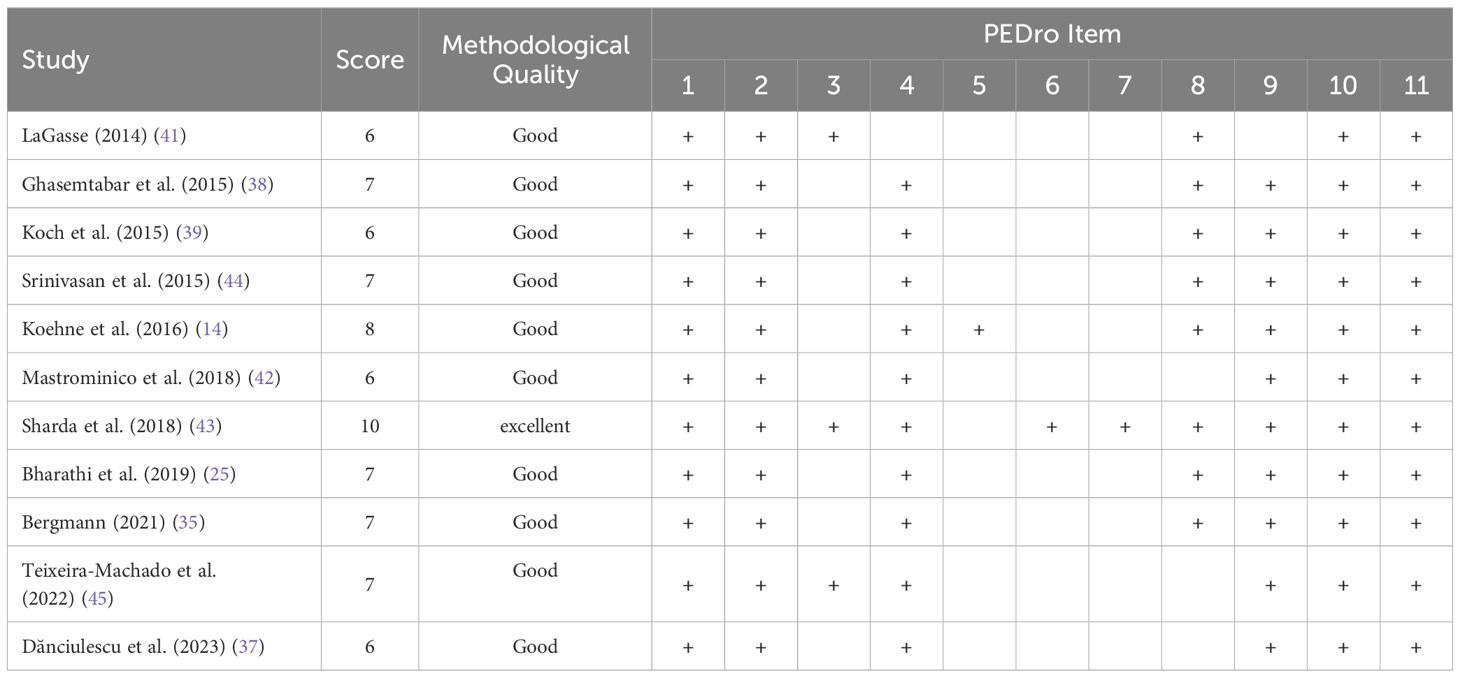
Table 3. Methodological quality assessment of included studies.
This is the first systematic quantitative analysis review focusing on specific rhythm techniques as the primary component of interventions targeting social skills in individuals with ASD. Existing evidence suggests a moderate to large effect of rhythm-based interventions on overall social skills (g = 0.681), social interaction (g = 1.299), communication (g = 1.522), and emotion (g = 1.752) compared with the control group. However, we did not observe a statistically significant effect (g = 0.125) of rhythm-based interventions on empathy among individuals with ASD. This is partially consistent with an earlier meta-analysis supporting rhythm-based interventions for ASD in several social skills (21, 22). For example, Chen et al. found that dance practice can significantly improve social interaction but does not significantly affect empathy for individuals with ASD. Another meta-analysis of music therapy indicated that music therapy only improved social reactions among children with ASD. However, music therapy did not improve social adaptive behavior or speech in children with ASD.
Our findings regarding the positive effects of rhythm-based interventions on overall social skills extend the results of previous systematic reviews (4). In addition, we mentioned previously the results of dance and music therapy. Our review confirmed a moderate to large training effect on overall social skills in individuals with ASD. This provides positive information for the rehabilitation education of children with clinical ASD. The underlying mechanism of rhythm-based interventions that induced social skill improvements may be related to two aspects. First, rhythm-based interventions usually involve a clear beat on the metronome. These clear beats can easily evoke synchronous behaviors (such as emotes, pronunciation, intonation, and body expression) and neural synchronization (18, 46). These synchronous behaviors and neural synchronization have significant social implications, particularly in enhancing social connections (47, 48). Another possible explanation is that these rhythm-based interventions are usually accompanied by music to sing or dance, which increases the production of the neuropeptides oxytocin and vasopressin (49, 50). These two hormones are beneficial for improving social skills in individuals with ASD (51, 52).
A lack of communication and social interaction is regarded as one of the core characteristics of primary social dysfunction in ASD (53). Interventions that utilize rhythm have been shown to markedly enhance social interaction and communication when compared to other forms of physical activity or no intervention at all. Several previous reviews also support these results. Notice that all primal studies interventions can be considered embodied rhythmic interventions. Therapists could incorporate rhythm into interventions for individuals with ASD to improve communication, social interaction, and emotional organization (54). By using rhythm as a tool, therapists can connect with individuals with ASD on a social level, fostering a sense of understanding and recognition (11). This in turn can lead to stronger social bonds and encourage prosocial behavior among pairs of individuals with ASD (55). Additionally, research has shown that activities involving synchronization, entrainment of rhythmic vocalizations, and bimanual motor actions can effectively stimulate speech, motor skills, and language related-brain networks in individuals with ASD (8, 25). These early findings suggest that rhythm- based interventions can promote cortical reorganization and functional changes through neuroplasticity.
Empathy, which is the capacity to comprehend and resonate with the emotions of others, showed varied outcomes with rhythm-based interventions, leading to a meta-analytic effect size that was not significant. The dance intervention also showed no improvement in empathy for ASD in a recent meta-analysis (21). This may have something to do with the complexity of empathy. Empathy is a multi-dimensional phenomenon encompassing both cognitive and affective components. These two components are cognitive empathy and affective empathy (56). Our study does not distinguish between cognitive and affective empathy (56) in calculating the process. Therefore, there may be some bias. Future research should determine the effects of rhythm intervention on different empathies. Conversely, some researchers argue that the neurological systems responsible for empathy may be compromised in individuals with autism spectrum disorders, making it challenging to see improvement through short-term training (57). Thus, Future research should consider rhythm-based interventions administered at higher dosage levels and over extended periods for better efficacy.
The current systematic review conducted an extensive search strategy to investigate the potential significance of rhythm information for individuals diagnosed with ASD. In total, 11 studies were included in the systematic review, providing helpful information for optimizing rehabilitation programs in individuals with ASD. A recent study reported that individuals can use rhythm information to regulate neural oscillatory characteristics and cognitive contributions. This provides a preliminary theoretical basis for our result regarding rhythm intervention to improve social cognition (58). Compared with TMS and tACS, rhythmic visual and sound stimulation has less risk and higher acceptability and has a specific application prospect in clinical rehabilitation. Whether rhythm intervention can be used to regulate brain activity and improve social skills for individuals with ASD still needs more research to explore the neural mechanism behind it.
The present study contains some limitations that may limit the quality of the evidence. First, only studies in English were included; hence some relevant studies in other languages might have been overlooked. Second, this study had significant heterogeneity, and further subgroup analysis of the results was impossible due to the limited number of RCTs. Moreover, it should be mentioned that the current study only analyzed rhythm as a factor of intervention rather than an intervention.
Rhythm-based interventions are an effective way to improve the social ability of individuals with ASD. This result indicates the importance of rhythm in the clinical rehabilitation of children with ASD. We suggest adding appropriate rhythmic elements to clinical interventions, especially for individuals with ASD who are less socially competent. Future research could provide insight into the mechanisms underlying the benefits of rhythm interventions in individuals with ASD.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
XD: Writing – original draft. JW: Writing – review & editing. DL: Writing – review & editing. ZL: Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. The article was supported by the Research Foundation for National educational science planning project [grant numberBLA230102].
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2024.1436170/full#supplementary-material
Supplementary Table 1 | PRISMA checklist
Supplementary Table 2 | Search strategy
Supplementary Table 3 | List of excluded studies with reason for full text
1. Lord C, Elsabbagh M, Baird G, Veenstra-Vanderweele J. Autism spectrum disorder. Lancet. (2018) 392:508–20. doi: 10.1016/S0140-6736(18)31129-2
2. Baio JWL, Christensen DL, et al. Prevalence of autism spectrum disorder among children aged 8 years — Autism and developmental disabilities monitoring network, 11 sites, United States, 2014. MMWR Surveillance Summaries. (2018) 67:1. doi: 10.15585/mmwr.ss6706a1
3. Yoder P, Stone WL, Walden T, Malesa E. Predicting social impairment and ASD diagnosis in younger siblings of children with autism spectrum disorder. J Autism Dev Disord. (2009) 39:1381–91. doi: 10.1007/s10803-009-0753-0
4. Morris P, Hope E, Foulsham T, Mills JP. The effectiveness of mirroring- and rhythm-based interventions for children with autism spectrum disorder: a systematic review. Rev J Autism Dev Disord. (2021) 8:541–61. doi: 10.1007/s40489-021-00236-z
5. Franchini M AVL, Schaer M, Smith IM. Initiation of joint attention and related visual attention processes in infants with autism spectrum disorder: Literature review. Child Neuropsychol. (2019) 25:287–317. doi: 10.1080/09297049.2018.1490706
6. Landa R. Early communication development and intervention for children with autism. Ment Retard Dev Disabil Res Rev. (2007) 13:16–25. doi: 10.1002/mrdd.20134
7. Camargo SPH, Rispoli M, Ganz J, Hong ER, Davis H, Mason R. A review of the quality of behaviorally-based intervention research to improve social interaction skills of children with ASD in inclusive settings. J Autism Dev Disord. (2014) 44:2096–116. doi: 10.1007/s10803-014-2060-7
8. Bharathi G JK, Balasubramanian V, Vellingiri B. The potential role of rhythmic entrainment and music therapy intervention for individuals with autism spectrum disorders. J Exercise Rehabil. (2019) 15:180. doi: 10.12965/jer.1836578.289
9. Manders E, Goodill S, Koch SC, Giarelli E, Polansky M, Fisher K, et al. The mirroring dance: Synchrony and interaction quality of five adolescents and adults on the autism spectrum in dance/movement therapy. Front Psychol. (2021) 12:717389. doi: 10.3389/fpsyg.2021.717389
10. Yoo GE, Kim SJ. Dyadic drum playing and social skills: Implications for rhythm-mediated intervention for children with autism spectrum disorder. J music Ther. (2018) 55:340–75. doi: 10.1093/jmt/thy013
11. Martin M. Moving on the spectrum: Dance/movement therapy as a potential early intervention tool for children with Autism Spectrum Disorders. Arts Psychother. (2014) 41:545–53. doi: 10.1016/j.aip.2014.10.003
12. Willemin T, Litchke LG, Liu T, Ekins C. Social emotional effects of drumtastic (R): A dyadic within-group drumming pilot program for children with autism spectrum disorder. Int J Special Educ. (2018) 33:94–103.
13. Stephens CE. Spontaneous imitation by children with autism during a repetitive musical play routine. Autism. (2008) 12:645–71. doi: 10.1177/1362361308097117
14. Glass D, Yuill N. Social motor synchrony in autism spectrum conditions: A systematic review. Autism. (2024) 28:1638–53. doi: 10.1177/13623613231213295
15. Dvir T, Lotan N, Viderman R, Elefant C. The body communicates: Movement synchrony during music therapy with children diagnosed with ASD. Arts Psychother. (2020) 69:101658. doi: 10.1016/j.aip.2020.101658
16. Koehne S, Behrends A, Fairhurst MT, Dziobek I. Fostering social cognition through an imitation-and synchronization-based dance/movement intervention in adults with autism spectrum disorder: A controlled proof-of-concept study. Psychother psychosomatics. (2016) 85:27–35. doi: 10.1159/000441111
17. Rojiani R, Zhang X, Noah A, Hirsch J. Communication of emotion via drumming: dual-brain imaging with functional near-infrared spectroscopy. Soc Cogn Affect Neurosci. (2018) 13:1047–57. doi: 10.1093/scan/nsy076
18. Cheng S, Wang J, Luo R, Hao N. Brain to brain musical interaction: A systematic review of neural synchrony in musical activities. Neurosci Biobehav Rev. (2024) 105812. doi: 10.1016/j.neubiorev.2024.105812
19. Wang Q, Han Z, Hu X, Feng S, Wang H, Liu T, et al. Autism symptoms modulate interpersonal neural synchronization in children with autism spectrum disorder in cooperative interactions. Brain Topography. (2020) 33:112–22. doi: 10.1007/s10548-019-00731-x
20. Ellamil M, Berson J, Wong J, et al. One in the dance: musical correlates of group synchrony in a real-world club environment. PloS One. (2016) 11:e0164783. doi: 10.1371/journal.pone.0164783
21. Chen T, Wen R, Liu H, Zhong X, Jiang C. Dance intervention for negative symptoms in individuals with autism spectrum disorder: A systematic review and meta-analysis. Complementary Therapies Clin Pract. (2022) 47:10156. doi: 10.1016/j.ctcp.2022.101565
22. Jiang P, Sun S, Zhang J, Li C, Ma G, Wang J, et al. Effectiveness of music therapy in children with autism spectrum disorder: A systematic review and meta-analysis. Front Psychiatry. (2022) 13. doi: 10.3389/fpsyt.2022.905113
23. Page MJ, Mckenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Bmj-British Med J. (2021) 372:n71. doi: 10.1136/bmj.n71
24. Takahashi H, Matsushima K, Kato T. The effectiveness of dance/movement therapy interventions for autism spectrum disorder: A systematic review. Am J Dance Ther. (2019) 41:55–74. doi: 10.1007/s10465-019-09296-5
25. Bharathi G, Jayaramayya K, Balasubramanian V, Vellingiri B. The potential role of rh hmic entrainment and music therapy intervention for individuals with autism spectrum disorders. J Exercise Rehabil. (2019) 15:180–6. doi: 10.12965/jer.1836578.289
26. Koch SC, Riege RFF, Tisborn K, Biondo J, Martin L, Beelmann A. Effects of dance movement therapy and dance on health-related psychological outcomes. A meta-analysis update. Front Psychol. (2019) 10. doi: 10.3389/fpsyg.2019.01806
27. DeJesus BM, Oliveira RC, de Carvalho FO, de Jesus Mari J, Arida RM, Teixeira-Machado L. Dance promotes positive benefits for negative symptoms in autism spectrum disorder (ASD): A systematic review. Complementary Therapies Med. (2020) 49:102299. doi: 10.1016/j.ctim.2020.102299
28. Fang Q, Aiken CA, Fang C, Pan Z. Effects of exergaming on physical and cognitive functions in individuals with autism spectrum disorder: A systematic review. Games Health J. (2019) 8:74–84. doi: 10.1089/g4h.2018.0032
29. Wu J, Loprinzi PD, Ren Z. The rehabilitative effects of virtual reality games on balance performance among children with cerebral palsy: A meta-analysis of randomized controlled trials. Int J Environ Res Public Health. (2019) 16:4161. doi: 10.3390/ijerph16214161
30. Borenstein MHL, Jpt H, Rothstein H. Introduction to meta-analysis. West Sussex: John Wiley & Sons, Ltd (2009).
31. Lakens D. Calculating and reporting effect sizes to facilitate cumulative science: a practical primer for t-tests and ANOVAs. Front Psychol. (2013) 4. doi: 10.3389/fpsyg.2013.00863
33. Hoeben M, Langelaan M, Klevering J, Keunen JE, van Rens GH. Low vision rehabilitation for better quality of life in visually impaired adults. Cochrane Database Systematic Rev. (2020) 1). doi: 10.1002/14651858.CD006543.pub2
34. Zuin M, Trentini A, Marsillach J, D’Amuri A, Bosi C, Roncon L, et al. Paraoxonase-1 (PON-1) arylesterase activity levels in patients with coronary artery disease: A meta-analysis. Dis Markers. (2022) 2022:4264314. doi: 10.1155/2022/4264314
35. Bergmann T, Birkner J, Sappok T, et al. The Autism-Competency-Group (AutCom). A promising approach to promote social skills in adults with autism spectrum disorder and intellectual disability. Int J Dev Disabil. (2021) 67:349–65. doi: 10.1080/20473869.2021.1967697
36. Bharathi G, Venugopal A, Vellingiri B. Music therapy as a therapeutic tool in improving the social skills of autistic children. Egyptian J Neurology Psychiatry Neurosurg. (2019) 55:1–6. doi: 10.1186/s41983-019-0091-x
37. Dănciulescu T, Zaharia A. Piano with a twist: A pilot study exploring the preliminary effects of a piano therapy program for children with autism spectrum disorder. Arts Psychother. (2023) 82:101987. doi: 10.1016/j.aip.2022.101987
38. Ghasemtabar SN, Hosseini M, Fayyaz I, Arab S, Naghashian H, Poudineh Z. Music therapy: An effective approach in improving social skills of children with autism. Adv BioMed Res. (2015) 4:157. doi: 10.4103/2277-9175.161584
39. Koch SC, Mehl L, Sobanski E, Fuchs T. Fixing the mirrors: a feasibility study of the effects of dance movement therapy on young adults with autism spectrum disorder. Autism. (2015) 19:338–50. doi: 10.1177/1362361314522353
40. Koehne S, Behrends A, Fairhurst MT, Dziobek I. Fostering social cognition through an imitation- and synchronization-based dance/movement intervention in adults with autism spectrum disorder: A controlled proof-of-concept study. Psychother Psychosomatics. (2016) 85:27–35. doi: 10.1159/000441111
41. Lagasse AB. Effects of a music therapy group intervention on enhancing social skills in children with autism. J Music Ther. (2014) 51:250–75. doi: 10.1093/jmt/thu012
42. Mastrominico A, Fuchs T, Manders E, Steffinger L, Hirjak D, Sieber M, et al. Effects of dance movement therapy on adult patients with autism spectrum disorder: A randomized controlled trial. Behav Sci (Basel). (2018) 8:61. doi: 10.3390/bs8070061
43. Sharda M, Tuerk C, Chowdhury R, Jamey K, Foster N, Custo-Blanch M, et al. Music improves social communication and auditory–motor connectivity in children with autism. Trans Psychiatry. (2018) 8:231. doi: 10.1038/s41398-018-0287-3
44. Srinivasan SM, Park IK, Neelly LB, Bhat AN. A comparison of the effects of rhythm and robotic interventions on repetitive behaviors and affective states of children with Autism Spectrum Disorder (ASD). Res Autism Spectr Disord. (2015) 18:51–63. doi: 10.1016/j.rasd.2015.07.004
45. Teixeira-MaChado L, Arida RM, Ziebold C, Barboza AB, Ribeiro L, Teles MC, et al. A pilot randomized controlled clinical trial of dance practice for functionality in autistic children and adolescent with all levels of need support. Complement Ther Clin Pract. (2022) 49:101650. doi: 10.1016/j.ctcp.2022.101650
46. Liu T, Duan L, Dai R, Pelowski M, Zhu C. Team-work, team-brain: exploring synchrony and team interdependence in a nine-person drumming task via multiparticipant hyperscanning and inter-brain network topology with fNIRS. NeuroImage. (2021) 237:118147. doi: 10.1016/j.neuroimage.2021.118147
47. Vicaria IM, Dickens L. Meta-analyses of the intra- and interpersonal outcomes of interpersonal coordination. J Nonverbal Behav. (2016) 40:335–61. doi: 10.1007/s10919-016-0238-8
48. Rennung M, Goritz AS. Prosocial consequences of interpersonal synchrony: A meta-analysis. Int J Psychol. (2016) 51:1065–. doi: 10.1027/2151-2604/a000252
49. Chanda ML, Levitin DJ. The neurochemistry of music. Trends Cogn Sci. (2013) 17:179–93. doi: 10.1016/j.tics.2013.02.007
50. Gebauer L, Witek MAG, Hansen NC, Thomas J, Konvalinka I, Vuust P. Oxytocin improves synchronisation in leader-follower interaction. Sci Rep. (2016) 6:38416. doi: 10.1038/srep38416
51. Parker KJ, Oztan O, Libove RA, Mohsin N, Karhson DS, Sumiyoshi RD, et al. A randomized placebo-controlled pilot trial shows that intranasal vasopressin improves social deficits in children with autism. Sci Trans Med. (2019) 11. doi: 10.1126/scitranslmed.aau7356
52. Parker KJ, Oztan O, Libove RA, Sumiyoshi RD, Jackson LP, Karhson DS, et al. Intranasal oxytocin treatment for social deficits and biomarkers of response in children with autism. Proc Natl Acad Sci United States America. (2017) 114:8119–24. doi: 10.1073/pnas.1705521114
53. Damianidou D, Eidels A, Arthur-Kelly M. The use of robots in social communications and interactions for individuals with ASD: a systematic review. Adv Neurodev Disord. (2020) 4:357–88. doi: 10.1007/s41252-020-00184-5
54. Kleinman S. Dance movement therapy - A healing art - levy,Fj. Am J Dance Ther. (1989) 11:61–3. doi: 10.1007/BF00844266
55. Peng W, Lou W, Huang X, Ye Q, Tong RK, Cui F. Suffer together, bond together: Brain-to-brain synchronization and mutual affective empathy when sharing painful experiences. Neuroimage. (2021) 238:118249. doi: 10.1016/j.neuroimage.2021.118249
56. Dvash J, Shamay-Tsoory SG. Theory of mind and empathy as multidimensional constructs neurological foundations. Topics Lang Disord. (2014) 34:282–95. doi: 10.1097/TLD.0000000000000040
57. Shamay-Tsoory SG. The neural bases for empathy. SAGE Journals. (2010) 17:18–24. doi: 10.1177/1073858410379268
Keywords: rhythm, ASD, social skills, communication, emotion, empathy, meta
Citation: Ding X, Wu J, Li D and Liu Z (2024) The benefit of rhythm-based interventions for individuals with autism spectrum disorder: a systematic review and meta-analysis with random controlled trials. Front. Psychiatry 15:1436170. doi: 10.3389/fpsyt.2024.1436170
Received: 21 May 2024; Accepted: 30 August 2024;
Published: 27 September 2024.
Edited by:
Christianne E. Strang, University of Alabama at Birmingham, United StatesReviewed by:
Marco Bilucaglia, Università IULM, ItalyCopyright © 2024 Ding, Wu, Li and Liu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Zexi Liu, ZG91ZG91MjM5NDYzNzZAb3V0bG9vay5jb20=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.