 Adane Misganaw1Mignot Hailu2
Adane Misganaw1Mignot Hailu2 Gashachew Bayleyegn3
Gashachew Bayleyegn3 Mekidem Aderaw4
Mekidem Aderaw4 Zeamanuel Anteneh Yigzaw5
Zeamanuel Anteneh Yigzaw5 Tihtna Alemu6
Tihtna Alemu6 Lakew Asmare7*
Lakew Asmare7*- 1Department of Nursing, Debre Tabor Health Science College, Debre Tabor, Ethiopia
- 2School of Nursing, College of Medicine and Health Science, University of Gondar, Gondar, Ethiopia
- 3Department of Emergency and Critical Care Nursing, School of Nursing, College of Medicine and Health Science, University of Gondar, Gondar, Ethiopia
- 4Comprehensive Specialized Hospital, College of Medicine and Health Science, University of Gondar, Gondar, Ethiopia
- 5Department of Health Promotion and Behavioral Science, School of Public Health, College of Medicine and Health Sciences, Bahir Dar University, Bahir Dar, Ethiopia
- 6Department of Surgical Nursing, School of Nursing, College of Medicine and Health Science, University of Gondar, Gondar, Ethiopia
- 7Department of Epidemiology and Biostatistics, Institute of Public Health, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia
Introduction: Anxiety is a commonly reported mental health disorder that significantly contributes to the global burden of disease. However, proper counseling, problem-solving strategies, and promotion of healthy lifestyle practices have a positive effect on reducing nurse anxiety, but there is limited evidence in Ethiopia, particularly in this study area. Therefore, this study aimed to assess the prevalence and identify factors affecting nurse anxiety in Northwest Ethiopia’s comprehensive specialized hospitals.
Methods: An institution-based cross-sectional study was conducted among 746 study participants from April 14 to May 20, 2023. A simple random sampling technique was used. An interviewer-administered questionnaire was used. Data were entered into EpiData version 4.6.0 and exported to STATA version 17 for analysis. In binary logistic regression, variables with a p-value of less than 0.25 were considered candidates for multivariable logistic regression. An association was declared at a p-value of less than 0.05 with a 95% confidence interval.
Result: In this study, the prevalence of anxiety was 33.9%. Thus, being female [adjusted odds ratios (AOR) = 1.53, 95% CI = 1.08, 2.22], working in an emergency department (AOR = 3.65, 95% CI = 1.83, 7.28), working night duty shifts (AOR = 3.12, 95% CI = 2.19, 4.46), having conflict with coworkers (AOR = 1.7, 95% CI = 1.14, 2.51), and having poor social support (AOR = 2.13, 95% CI = 1.23, 3.69) were variables significantly associated with anxiety.
Conclusion: This study revealed that one-third of nurses experienced anxiety, which is a critical indicator of mental health within this population. Important factors that were found to be significantly associated with anxiety include being female, working in the emergency department, having a conflict with coworkers, having poor social support, and working night duty shifts. These findings show the need for the implementation of counseling services and the adaptation of effective coping strategies for nurses working at comprehensive specialized hospitals. Understanding the impact of anxiety on nurses is important to design interventions aimed at improving their mental health and job satisfaction.
Introduction
Anxiety is a psychological and physiological state characterized by cognitive, physical, emotional, and behavioral factors that can cause unpleasant feelings, anxious thoughts, and tension (1). Anxiety significantly contributes to the global burden of disease (2). According to a World Health Organization (WHO) report, 3.6% of the world population suffers from anxiety, and the total estimated number of people living with anxiety in the world is 264 million (3). Approximately 3.3% of people in Ethiopia are estimated to suffer from anxiety (4). The anxiety prevalence among healthcare professionals in Ethiopia was 26.8% (5). This prevalence is particularly relevant given the demanding nature of nursing work, which often includes high-stress environments and emotional labor (6). Nurses perform many responsibilities in hospitals such as caring for individuals and recovering optimal health and quality of life for their clients (7). Because of these activities and responsibilities, they often face enormous emotional pressure (8). Therefore, nurses frequently deal with unhappiness and become anxious in clinical settings (9, 10).
There are different causes of anxiety among nurses: challenging work environments, lack of human resources, and ongoing changes in the treatment and delivery of patient care (11). These factors affect professionals’ ability to perform their job by impairing their cognitive function, memory, and concentration, in addition to lack of physical exercise, smoking cigarettes, working in emergency departments, depression, night shift work, conflict with colleagues, and khat chewing (12, 13).
However, in recent years, several efforts have been made for nurses to reduce mental disorders, particularly anxiety through proper counseling regarding effective coping mechanisms and problem-solving strategies and the promotion of healthy lifestyle practices (6). Therefore, this study aimed to assess the prevalence and explore factors affecting nurse anxiety in Northwest Ethiopia’s comprehensive specialized hospitals. The findings of this study will provide important information for improving the quality of healthcare and the wellbeing of nursing professionals and treatment outcomes for patients.
Methods
Study design and setting
An institutional-based multicenter cross-sectional study was conducted from April 14 to May 20, 2023, in five comprehensive specialized hospitals found in Northwest Amhara: the University of Gondar Comprehensive Specialized Hospitals (UoGCSH), Debre Tabor Comprehensive Specialized Hospitals (DTCSH), Tibebe Ghion Comprehensive Specialized Hospitals (TGCSH), Felege Hiwot Comprehensive Specialized Hospitals (FHCSH), and Debre Markos Comprehensive Specialized Hospitals (DMCSH). These hospitals serve more than 20 million people. During the study period, a total of 1,610 nurses worked in these five hospitals.
Population
The source population was all professional nurses who were working in Northwest Amhara comprehensive specialized hospitals. Permanently employed nurses working at least 6 months of relevant work experience in these hospitals during the data collection period were the study population. Nurses with known mental problems (based on their employment records) were excluded from the study.
Sample size and sampling procedure
The sample size was determined using a single population proportion formula with a 95% confidence level, margin of error of 3% (0.03), 19.8% proportion of nurses experiencing anxiety from a previous study (6), and 10% non-response rate. Therefore, the final sample size was 746.
The total calculated sample size (746 nurses) was proportionally allocated to each hospital based on the lists of nurses from the hospital’s human resource management registration book: UoGCSH, 290; DTCSH, 102; FHCSH, 107; TGCSH, 146; DMCSH, 101. Finally, a simple random sampling (lottery method) technique was used (Figure 1).
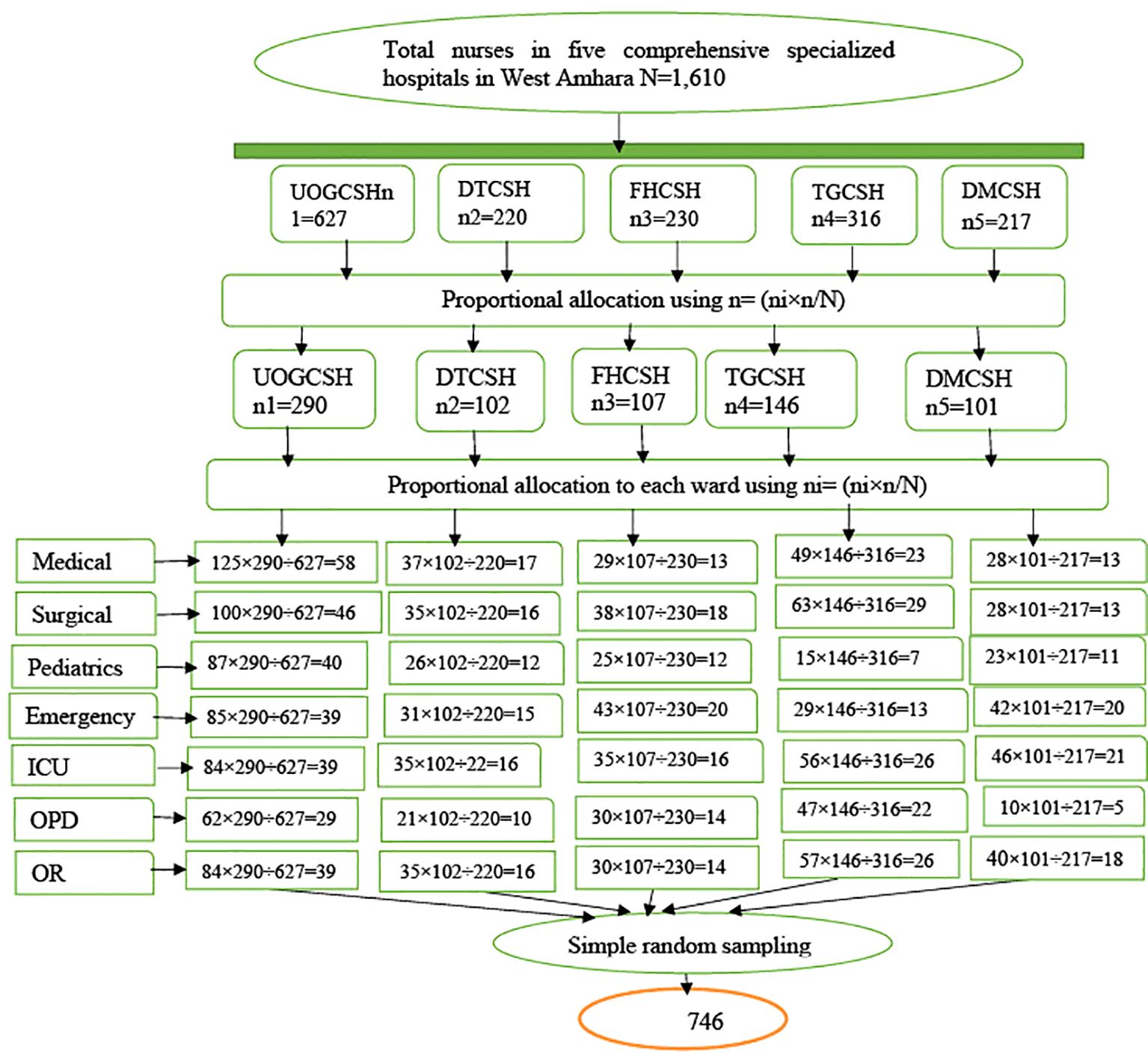
Figure 1. Schematic presentation of the sampling procedure used to select nurses working in Northwest Amhara comprehensive specialized hospitals, Ethiopia, 2023.
Operational definition of variables
Anxiety
Participants who scored below 10 on the Generalized Anxiety Disorder-7 (GAD-7) scale were considered to have no anxiety, and those who scored 10 and above were considered to have anxiety (14).
Depression
Participants who scored below 10 on the Patient Health Questionnaire-9 (PHQ-9) scale were considered to have no depression, and those who scored 10 and above were considered to have depression (15).
Stress
Study participants who scored ≥26 on the Workplace Stress Scale (WRSS) were considered to have work-related stress, and those who scored less than 26 had no work-related stress (16).
Social support
According to the social support scale, which is a brief three-item questionnaire (Oslo-3) that ranges from 3 to 14, those respondents who scored 3–8 were considered to have poor social support, those who scored 9–11 have moderate social support, and two who scored 12–14 have strong social support (17).
Current substance use
These were respondents who used substances (alcohol, khat, and cigarettes) in the last 3 months (18).
Ever substance use
These were respondents who used substances (alcohol, khat, and cigarettes) in their lifetime (18).
Physical exercise
A nurse was considered physically active if he/she exercised or performed any kind of sports activity including walking at least 150 min per week in a planned, structured, and repetitive manner (19).
Data collection procedure and tools
Data were collected using a structured interviewer-administered questionnaire adapted from different literature settings (9, 10, 20, 21). First, the questionnaires were prepared in English, then translated into the local language Amharic, and translated back to English to check consistency by an independent translator. The questionnaires consisted of sociodemographic characteristics (sex, age, marital status, educational status, and monthly income), work-related and clinical factors (work experience, family history of mental illness, working department, job satisfaction, nurse–patient relationship, shift work, work overload, known chronic disease, position, lack of professional autonomy, and conflict with colleagues/coworkers), substance and behavioral-related factors, psychosocial factors (alcohol use, cigarette smoking, khat chewing, physical exercise, and leisure time activities), and psychosocial factors (depression, social support, and work-related stress). The questionnaire was pretested among 37 nurses at Woldia Comprehensive Specialized Hospital before the actual data collection period. Based on the findings of the pretest, minor modification was made to the questionnaires, and some statements were rephrased to make them easily understandable by study participants.
Anxiety was measured using the GAD-7 scale. The GAD-7 scale was reliable with Cronbach’s alpha of 0.92 and test–retest reliability (intra-class correlation = 0.83) with good validity (14). GAD-7 is a seven-item scale that measures anxiety. It was calculated by assigning scores “0” for not at all, “1” for several days, “2” for more than half of days, and “3” for nearly everyday responses for “how often have you been bothered by the seven listed symptoms of anxiety over the last 2 weeks?” Adding the scores, the GAD-7 scale ranged from 0 to 21. The total scores of measurements were interpreted as normal (0–4), mild (5–9), moderate (10–14), and severe (15–21). The cut-off score for detecting anxiety was ≥10. This scale was reliable and valid (14). In Ethiopia, it was validated with Cronbach’s alpha of 0.77 (22). It was widely used in Ethiopia among healthcare workers to measure anxiety (23, 24). Cronbach’s alpha reliability coefficient for GAD-7 in the current study was 0.89, demonstrating good internal consistency.
Depression was measured using the PHQ-9 scale, which comprises nine items that can be scored from 0 (not at all) to 3 (nearly every day). Scores of 0–4, 5–9, 10–15, and 20 represent cut points for normal, mild, moderate, and severe depression (15). The cut-off score for detecting depression was ≥10. It was validated in Ethiopia, and its Cronbach’s alpha was 0.78, indicating acceptable internal consistency (25). Cronbach’s alpha reliability coefficient for PHQ-9 in the current study was 0.81, indicating good internal consistency. Work-related stress was assessed using the WRSS composed of eight statements (16, 26). In terms of scoring, item numbers 6, 7, and 8 were reverse-scored with a 5-point Likert response format, ranging from never (scored 1) to very often (scored 5). Nurses who scored ≥26 on WRSS were considered to have work-related stress. The reliability of the tool was assessed on nurses, and its Cronbach’s alpha reliability coefficient was 0.79 (27). Cronbach’s alpha reliability coefficient for WRSS in the current study was 0.80, indicating good internal consistency. Also, social support was measured using the Oslo 3-item social support scale, and individuals who scored 3–8, 9–11, and 12–14 were considered to have poor, moderate, and strong social support, respectively (17). Cronbach’s alpha reliability coefficient for social support in the current study was 0.61.
Data were collected by five Bachelor of Science (BSc) psychiatric nurses and three Master of Science (MSc) supervisors after 2 days of training were provided. The training covered the goal, the purpose, the patient approach, confidentiality, and consent-taking technique. The collected data were reviewed for completeness and consistency by data collection supervisors and the principal investigator on a daily basis. Data cleaning and coding were performed before the analysis.
Data processing and analysis
The data were coded and entered into EpiData version 4.6 for cleaning and exported to STATA version 17 for analysis. Descriptive statistics were computed and presented in the text, tables, and figure. Variables with p-values of less than 0.2 in the bivariate analysis were entered into the multivariable logistic regression model to determine the effect of each independent variable on the outcome variable. The variance inflation factor was equal to 1.48, which was less than 10, indicating that there was no multi-collinearity. The strength of the association was presented as the odds ratios and 95% confidence interval. A p-value of <0.05 in the multivariate analysis was considered significant. The result of model fitness using the Hosmer and Lemeshow test (p-value = 0.79) indicated that the model was fit.
Results
Sociodemographic characteristics
Among a total of 746 selected respondents, 732 (98.10%) participated in this study. The mean age of the respondents was 31.1 years with 3.97 (mean ± SD). More than half (54.10%) of the respondents were male. Concerning duty shifts, nearly two-thirds of respondents (62.16%) worked during the day shift. The majority (92.76%) of the participants did not have a family history of mental illness (Table 1).
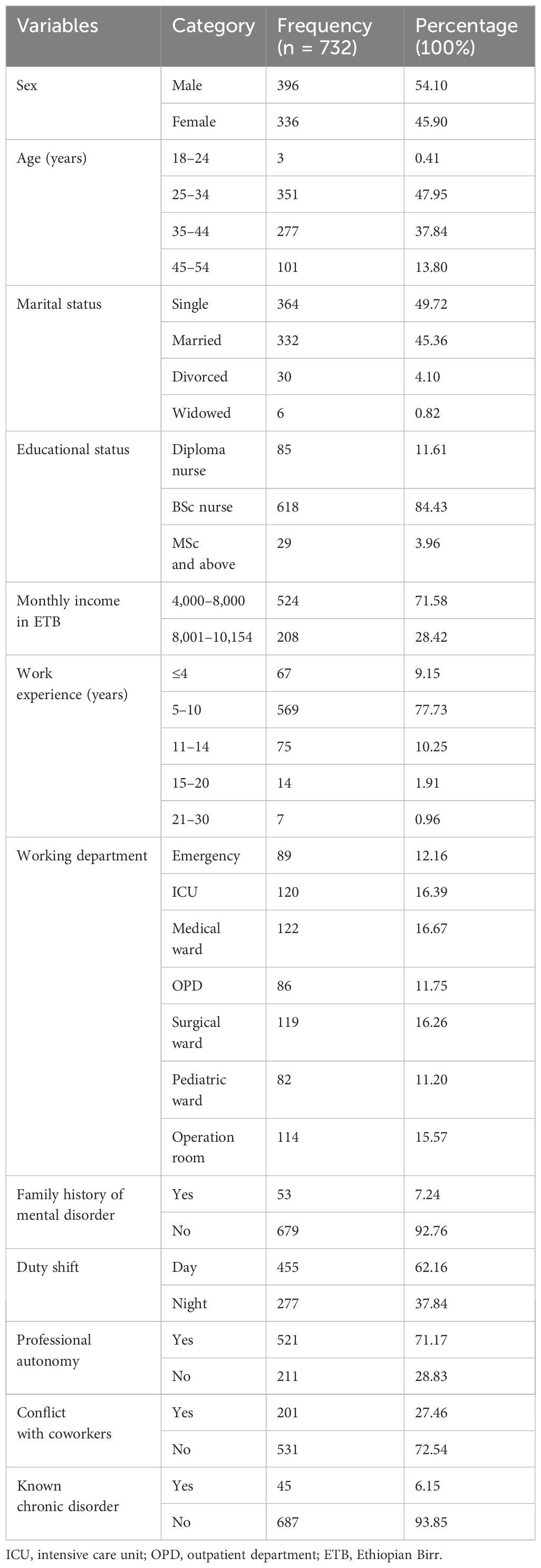
Table 1. Sociodemographic, work-related, and clinical characteristics of nurses working in Northwest Ethiopia Comprehensive Specialized Hospitals, 2023 (n = 732).
Psychosocial, substance use, and behavioral characteristics
In this study, nearly half (49.18%) of participants reported using alcohol at least once during their lifetime. Currently, 93.03% of participants had never consumed alcohol. Regarding leisure time activities, most (82.92%) participants did not have leisure time activities, and 5.33% had them once or twice. A total of 34.02%, 13.39%, and 14.89% of respondents had poor social support, depression, and stress, respectively. Regarding the psychosocial characteristics of nurses, 34.02%, 13.39%, and 14.89% of respondents had poor social support, depression, and stress, respectively (Table 2).
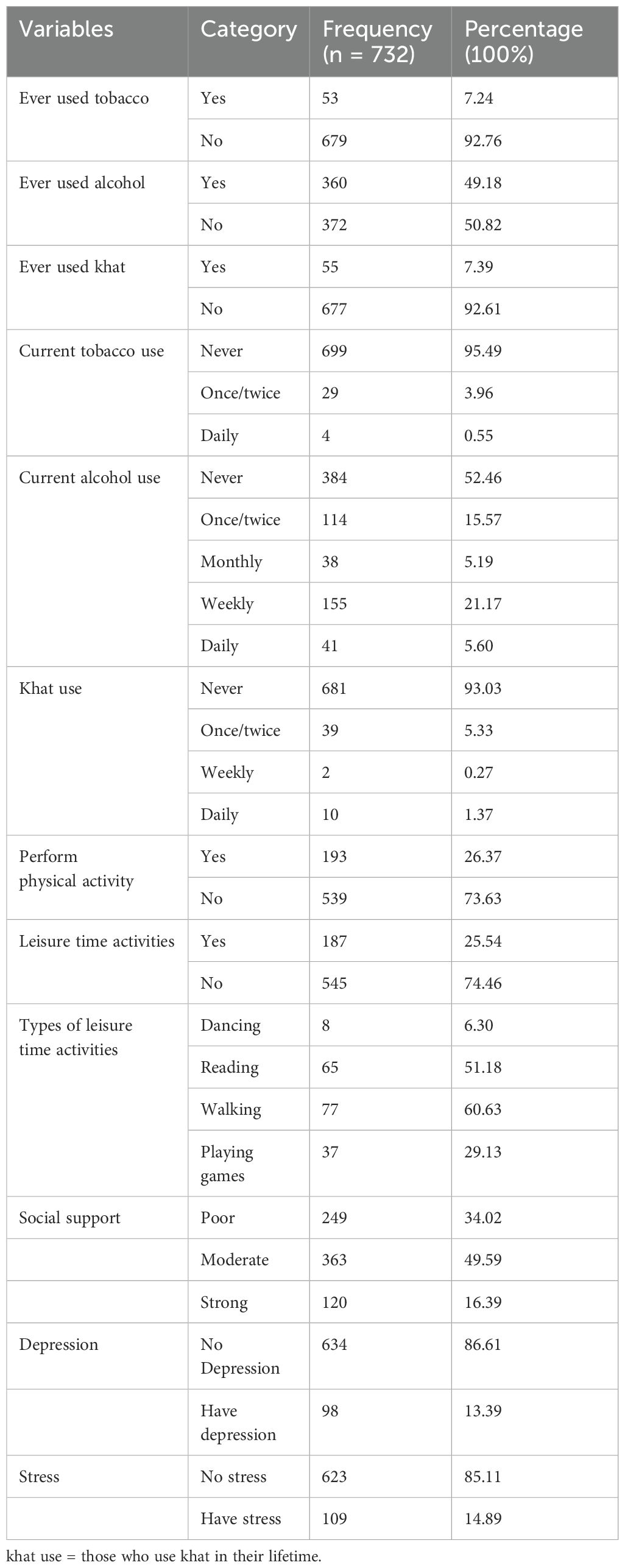
Table 2. Psychosocial, substance use, and behavioral characteristics of nurses, 2023 (n = 732).
Magnitude of anxiety
The magnitude of anxiety among nurses was 33.90% with a 95% CI (30.5%, 37.4%) (Table 3).
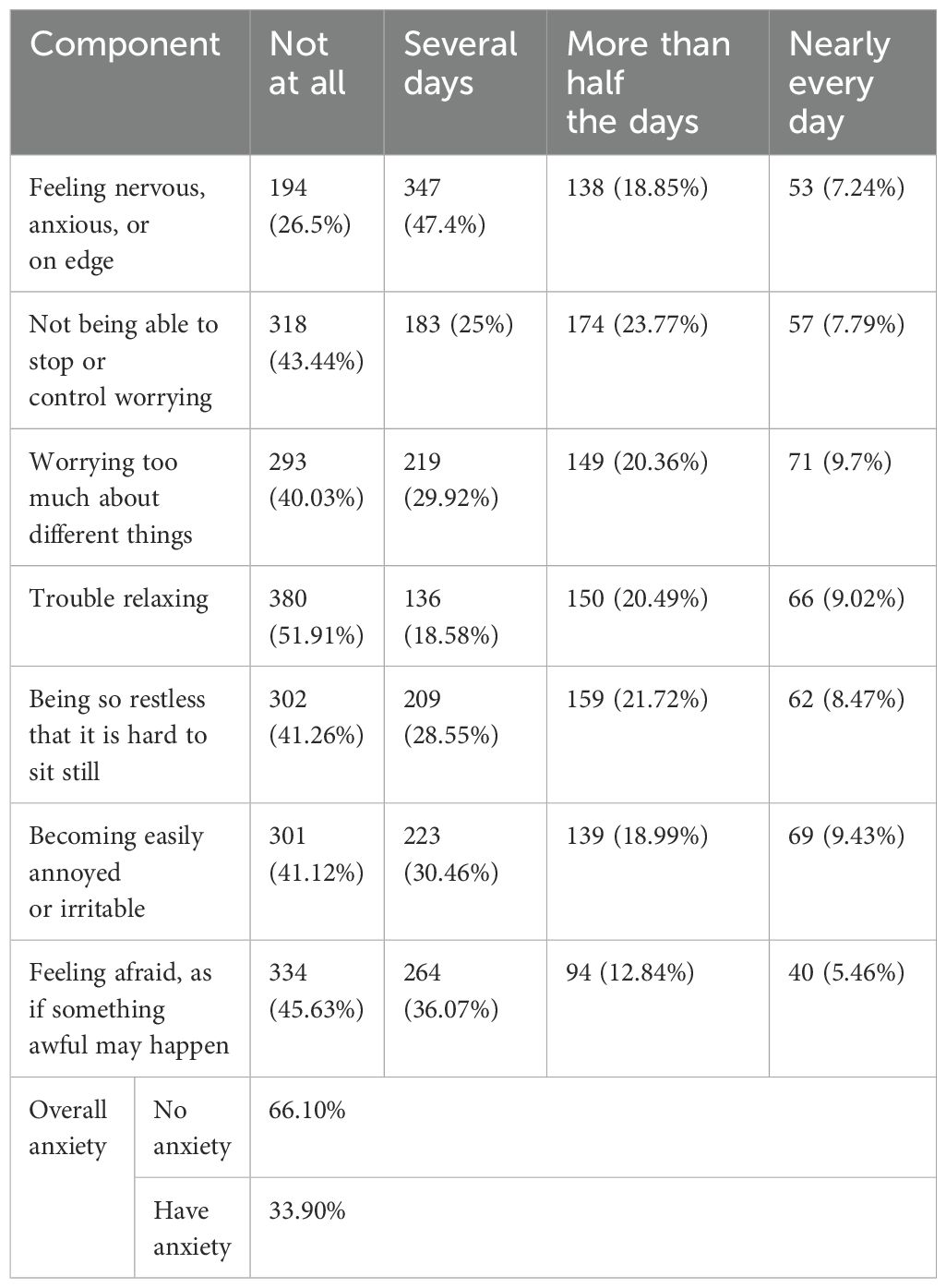
Table 3. Indicators of anxiety measurement tool among nurses, 2023 (N = 732).
Factors associated with anxiety
In this model, the following variables were included in the multivariable analysis because their overall p-value in the bi-variable analysis was <0.25 (Table 4). Thus, the odds of anxiety were 1.53 times greater among female nurses than male nurses (AOR = 1.53, 95% CI = 1.07, 2.20). The number of nurses working in the emergency department was 3.65 times higher than that working in the outpatient department (AOR = 3.65, 95% CI = 1.83, 7.28). Additionally, nurses who were working night duty shifts were 3.12 times more likely to have anxiety than nurses who were working daytime shifts (AOR = 3.12, 95% CI = 2.19, 4.46). Respondents who experienced conflict with coworkers were 1.7 times more likely to develop anxiety than those who did not (AOR = 1.70, 95% CI = 1.14, 2.51), and those who had poor social support were 2.13 times more likely to develop anxiety than nurses who had strong social support (AOR = 2.13, 95% CI = 1.23, 3.69).
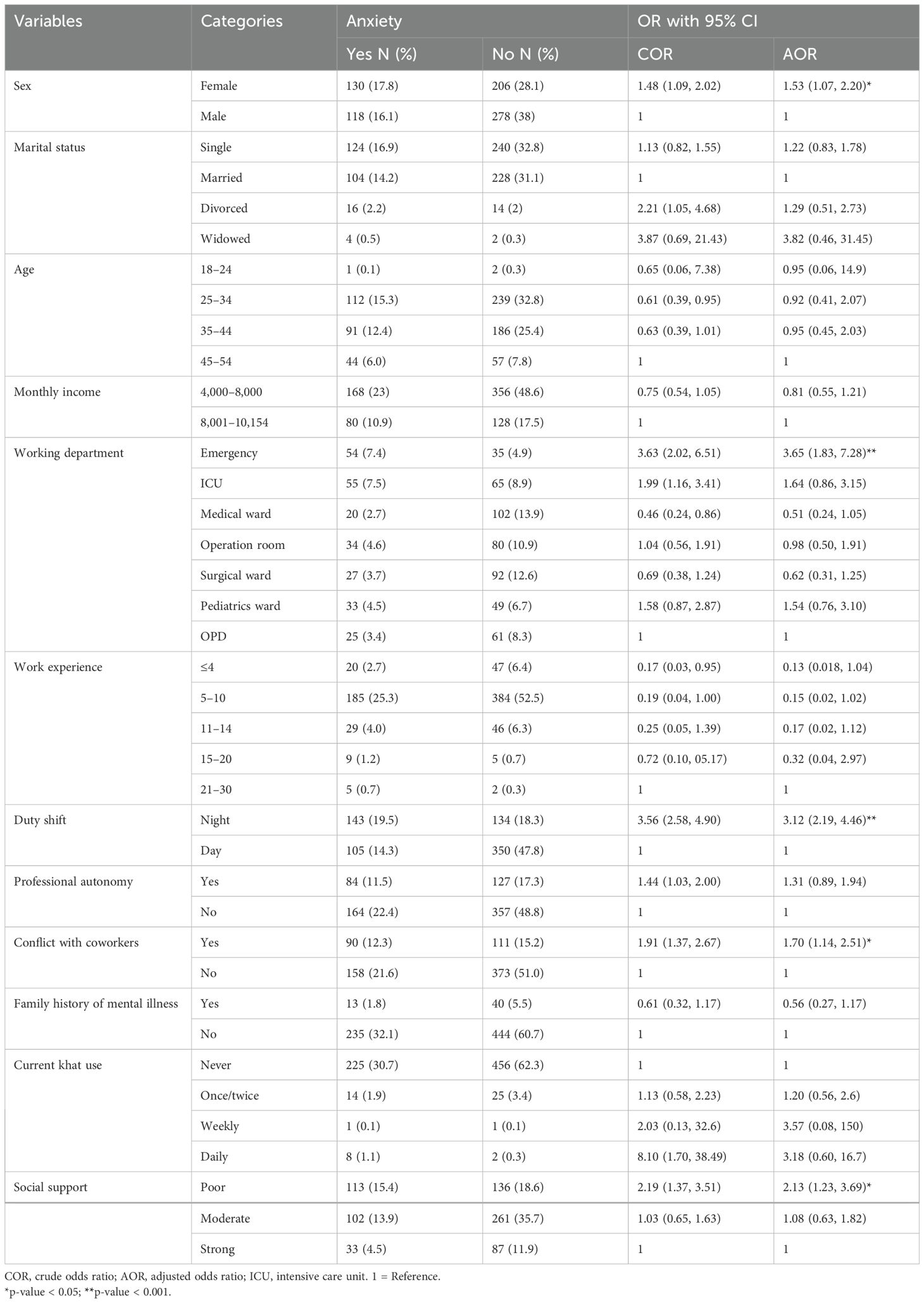
Table 4. Bivariable and multivariable analyses of factors associated with anxiety among nurses working in Northwest Ethiopia Comprehensive Specialized Hospitals, 2023 (n = 732).
Discussion
The study findings showed that 33.90% of nurses experienced anxiety, which is a critical indicator of mental health within this population. This prevalence aligns closely with findings from similar studies conducted in Kenya (35.6%) (28), South Tunisia (32.5%) (29), Italy (33.2%) (30), Iran (31.2%) (31), and China (37.3%) (32). The higher prevalence of anxiety in this study compared to that in previous studies in Addis Ababa (19.8%) (6) and Jimma (19.2%) (13) may be attributed to several factors, including differences in data collection methods and the ongoing socio-political challenges in northern Ethiopia, such as the impact of conflict and the COVID-19 pandemic (20, 21).
The result showed lower anxiety rates found in this study compared to studies conducted in Egypt (64.6%) (33) and South Africa (49.6%) (12) due to differences in inclusion and specific challenges faced by practitioners in different settings. For example, the Egyptian study included nurses with more than 1 year of experience, which may have affected the results. A significant proportion of participants reported poor social support (34.02%), depression (13.39%), and stress (14.89%). These factors are closely related, as poor social support can contribute to mental health issues, and mental illness in turn can lead to social isolation (34). The high prevalence of these problems underscores the need for interventions to improve social support and mental health in this population.
Important factors associated with anxiety include gender, working in emergency departments, working night shifts, and conflicts with coworkers. The finding is that female nurses are 1.53 times more likely to experience anxiety than their male counterparts. This finding is supported by studies conducted in Kenya (28) and Saudi Arabia (35). The possible reason may be biological factors such as differences in the brain structures involved in emotional regulation, which may explain the differences in the processing of negative information, the fluctuations of sex hormones that affect the anxious state of women, and genetic factors (36). Nurses working in the emergency department were nearly four times (3.65) more likely to develop anxiety than nurses working in the outpatient department. The finding of this study is supported by those of studies conducted in Iraq (37). This may be due to the need to deal with too many patients with inadequate numbers of nurses; an increase in the number of patients in emergency departments; and complex and complicated/severe cases, death of patients, and workload schedules in emergency departments. Nurses who were working night duty shifts were 3.12 times more likely to have anxiety than nurses who were working during daytime shifts. This finding is supported by a study conducted in Addis Ababa (6). This may be due to frequent and repeated night shift work, daytime sleepiness, lack of adequate sleep at night, fear of family separation, and difficulties in emotionally adapting to work at night. In this study, nurses who experienced conflict with coworkers were 1.70 times more likely to develop anxiety than nurses who did not have conflict with coworkers. This finding agrees with those of studies conducted among Chinese nurses (13, 32). The possible reason may be that conflict with colleagues increases the risk of experiencing anxiety episodes, which results from the secretion of increased cortisol and leads to damage of neurons in the hippocampus and amygdala, which are important structures of the brain that regulate mood and pleasure, resulting in anxiety (38), and nurses who had poor social support were 2.13 times more likely to develop anxiety than nurses who had strong social support. This finding is supported by studies conducted in South Africa (12) and Ethiopia (6). This may be due to loneliness, low socioeconomic status, death, separation from a loved one, and lack of family support. This may also be due to a lack of social relationships in health facilities, discrimination and stigma in the workplace, social disadvantage, physical violence, and poverty (39).
Furthermore, understanding the impact of anxiety on nurses may inform interventions aimed at improving their mental health and job satisfaction (40). Research in this area is critical for support programs and targeted interventions that can reduce anxiety and improve the overall work environment for clinical nurses.
Strengths and limitations of the study
This is the first study of its kind in the study area, which provides updated information. Also, it may serve as the basis for future studies. However, the study was based on self-reported data; self-reports can lead to information bias, such as social desirability bias even though we tried to minimize it by reminding participants about confidentiality and anonymity during data collection.
Conclusion
This study revealed that one-third of nurses experienced anxiety, which is a critical indicator of mental health within this population. Important factors that were found to be significantly associated with anxiety include being female, working in the emergency department, having a conflict with coworkers, having poor social support, and working night duty shifts. These findings show the need for the implementation of counseling services and the adaptation of effective coping strategies for nurses working at comprehensive specialized hospitals. Understanding the impact of anxiety on nurses is important to design interventions aimed at improving their mental health and job satisfaction. Research in this area is critical for support programs and targeted interventions that can reduce anxiety and improve the overall work environment for clinical nurses.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
Ethics statement
The study was reviewed and approved by the Institutional Review Board of School of Nursing at University of Gondar with Ref. number (S/N/180/2015). Written informed consent from the participants was not required to participate in this study in accordance with the national legislation and the institutional requirements.
Author contributions
LA: Methodology, Writing – review & editing. AM: Conceptualization, Formal analysis, Methodology, Writing – original draft. MH: Methodology, Validation, Writing – review & editing. GB: Data curation, Writing – review & editing. MA: Data curation, Writing – review & editing. ZAY: Writing – review & editing, Methodology. TA: Methodology, Validation, Visualization, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Acknowledgments
The authors acknowledge the Amhara Health Bureau, the University of Gondar Institutional Review Board of the School of Nursing, data collectors, and supervisors for providing valuable time and necessary information for this research.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbreviations
ASSIS, Alcohol, Smoking, and Substance Involvement Screening Test; BSc, Bachelor of Science; GAD, Generalized Anxiety Disorder; PHQ, Patient Health Questionnaire; SD, standard deviation; WRSS, Workplace Stress Scale.
References
1. Adults MDA. National Institute of Mental Health. Available online at: https://www.NIMH.NIH.gov/health/statistics/prevalence/major-depression-among-adults.shtml (Accessed August. 2017;15).
2. Crippa AA, de Lima JLB, de Andrade RAM, de Lima MAM, de Almeida PACL, Nunes ARPD, et al. Global, regional, and national burden of 12 mental disorders in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet Psychiatry. (2022) 9:137–50. doi: 10.1016/S2215-0366(21)00395-3
3. World Health Organization. Depression and other common mental disorders: global health estimates. Geneva, Switzerland: World Health Organization (2017).
4. Abdeta T, Birhanu A, Kibret H, Alemu A, Bayu K, Bogale K, et al. Prevalence of common mental disorders and associated factors among adults living in Harari regional state, eastern Ethiopia: a community-based cross-sectional study. Front Psychiatry. (2023) 14:1183797. doi: 10.3389/fpsyt.2023.1183797
5. Dagne H, Atnafu A, Alemu K, Azale T, Yitayih S, Dagnew B, et al. Anxiety and associated factors among Ethiopian health professionals at an early stage of the COVID-19 pandemic in Ethiopia. PloS One. (2021) 16:e0252664. doi: 10.1371/journal.pone.0252664
6. Belayneh Z, Zegeye A, Tadesse E, Asrat B, Ayano G, Mekuriaw B. Level of anxiety symptoms and its associated factors among nurses working in emergency and intensive care unit at public hospitals in Addis Ababa, Ethiopia. BMC Nursing. (2021) 20:1–7. doi: 10.1186/s12912-021-00701-4
7. Dunphy LM, Winland-Brown J, Porter B, Thomas D. Primary care: Art and science of advanced practice nursing. Philadelphia, Pennsylvania, USA: FA Davis (2015).
8. Mekonen E, Shetie B, Muluneh N. The psychological impact of the COVID-19 outbreak on nurses working in the Northwest of Amhara Regional State Referral Hospitals, Northwest Ethiopia. Psychol Res Behav Manage. (2021) 14:1353–64. doi: 10.2147/PRBM.S291446
9. Butler. Estimating time physicians and other health care workers spend with patients in an intensive care unit using a sensor network. Am J Med. (2018) 131:972 e9– e15. doi: 10.1016/j.amjmed.2018.03.015
10. Legesse H, Degefie T, Hiluf M, Sime K, Tesfaye C, Abebe H, et al. National scale-up of integrated community case management in rural Ethiopia: implementation and early lessons learned. Ethiop Med J. (2014) 52:15–26. doi: 10.4314/emj.v52i1.3.ce10
11. Labrague LJ, McEnroe-Petitte DM, Leocadio MC, Van Bogaert P, Cummings GG. Stress and ways of coping among nurse managers: An integrative review. J Clin Nurs. (2018) 27:1346–59. doi: 10.1111/jocn.2018.27.issue-7pt8
12. Assis B, Azevedo C, Moura C, Mendes PG, Rocha LL, Roncalli AA, et al. Factors associated with stress, anxiety and depression in nursing professionals in the hospital context. Rev Bras Enfermagem. (2022) 75:1–10. doi: 10.1590/0034-7167-2021-0263
13. Yeshaw Y, Mossie A. Depression, anxiety, stress, and their associated factors among Jimma University staff, Jimma, Southwest Ethiopia, 2016: a cross-sectional study. Neuropsychiatr Dis Treat. (2017) 13:2803–12. doi: 10.2147/NDT.S150444
14. Spitzer RL, Kroenke K, Williams JBW, Löwe B. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Internal Med. (2006) 166:1092–7. doi: 10.1001/archinte.166.10.1092
15. Kroenke K, Spitzer RL, Williams JBW. The PHQ-9: validity of a brief depression severity measure. J Gen Internal Med. (2001) 16:606–13. doi: 10.1046/j.1525-1497.2001.016009606.x
16. Scale TWPS. The Marlin Company, North Haven, Connecticut and The American Institute of Stress. Yonkers, New York (2001).
17. Duko B, Toma A, Abraham Y. Prevalence and correlates of common mental disorder among HIV patients attending antiretroviral therapy clinics in Hawassa City, Ethiopia. Ann Gen Psychiatry. (2019) 18:1–6. doi: 10.1186/s12991-019-0241-7
18. Group WHOAW. The alcohol, smoking and substance involvement screening test (ASSIST): development, reliability and feasibility. Addiction. (2002) 97:1183–94. doi: 10.1046/j.1360-0443.2002.00185.x
19. Who. Global Recommendations on Physical Activity for Health: 18–64 Years Old. Switzerland: WHO Geneva (2011).
20. Van Bortel T, Basnayake A, Wurie F, Jambai M, Koroma AS, Muana AT, et al. Psychosocial effects of an Ebola outbreak at individual, community, and international levels. Bull World Health Organization. (2016) 94:210. doi: 10.2471/BLT.15.158543
21. Tedla MG, Kahsay MM. Mental health rehabilitation and support for victims of the Tigray war. Lancet Psychiatry. (2023) 10:e14. doi: 10.1016/S2215-0366(23)00150-5
22. Manzar MD, Salahuddin M, Alghadir A, Anwer S, Peter S, Bahammam AS, et al. Psychometric properties of the Generalized Anxiety Disorder-7 Scale in Ethiopian university students. Bull Menninger Clinic. (2021) 85:405–27. doi: 10.1521/bumc.2021.85.4.405
23. Kibret S, Teshome D, Fenta E, Hunie M, Tamire T. Prevalence of anxiety towards COVID-19 and its associated factors among healthcare workers in a Hospital of Ethiopia. PloS One. (2020) 15:e0243022. doi: 10.1371/journal.pone.0243022
24. Teshome A, Glagn M, Shegaze M, Tekabe B, Getie A, Assefa G, et al. Generalized anxiety disorder and its associated factors among health care workers fighting COVID-19 in Southern Ethiopia. Psychol Res Behav Manage. (2020), 907–17. doi: 10.2147/PRBM.S282822
25. Degefa M, Dubale B, Bayouh F, Ayele B, Zewde Y. Validation of the PHQ-9 depression scale in Ethiopian cancer patients attending the oncology clinic at Tikur Anbessa specialized hospital. BMC Psychiatry. (2020) 20:1–7. doi: 10.1186/s12888-020-02850-3
26. Zewudie BT, Temere BC, Eniyew MA, Mesfin Y, Tenaw SG. Low back pain and associated factors among obstetrics care providers in public hospitals of Amhara Regional State, Ethiopia: a cross-sectional study. BMJ Open. (2022) 12:e055749. doi: 10.1136/bmjopen-2021-055749
27. Mekonen EG, Gebrie MH, Jemberie SM. Work-related stress among nurses working in northwest Amhara Referral Hospitals; a burden for hospitals. Int J Afr Nurs Sci. (2022) 17:100486. doi: 10.1016/j.ijans.2022.100486
28. Kariuki SW. Prevalence of depression and anxiety, their associated risk factors and coping strategies among health care providers of critically ill patients at the Kenyatta national hospital. Psychol Res Behav Manage. (2022) 15:1–10. doi: 10.2147/PRBM.S280978
29. Tfifha M, Abbes W, Sellami I, El Falah W, Hajjaji M, Ghanmi L. Factors associated with anxiety among health care workers practicing in the emergency department in the south of Tunisia. Eur Psychiatry. (2021) 64:S187–S. doi: 10.1192/j.eurpsy.2021.494
30. Simonetti V, Durante A, Ambrosca R, Arcadi P, Graziano G, Pucciarelli G, et al. Anxiety, sleep disorders and self-efficacy among nurses during COVID-19 pandemic: A large cross-sectional study. J Clin Nurs. (2021) 30:1360–71. doi: 10.1111/jocn.v30.9-10
31. Poursadeghiyan M, Abbasi M, Mehri A, Hami M, Raei M, Ebrahimi MH. Relationship between job stress and anxiety, depression and job satisfaction in nurses in Iran. Soc Sci. (2016) 11:2349–55. doi: 10.1016/j.socscimed.2016.05.031
32. Cheung T, Yip PSF. Depression, anxiety, and symptoms of stress among Hong Kong nurses: a cross-sectional study. Int J Environ Res Public Health. (2015) 12:11072–100. doi: 10.3390/ijerph120911072
33. Hamed RA, Abd Elaziz SY, Ahmed AS. Prevalence and predictors of burnout syndrome, post-traumatic stress disorder, depression, and anxiety in nursing staff in various departments. Middle East Curr Psychiatry. (2020) 27:1–8. doi: 10.1186/s43045-020-00044-x
34. Brandt L, Liu S, Heim C, Heinz A. The effects of social isolation stress and discrimination on mental health. Trans Psychiatry. (2022) 12:398. doi: 10.1038/s41398-022-02178-4
35. Alharthy N, Alrajeh OA, Almutairi M, Alhajri A. Assessment of anxiety level of emergency health-care workers by generalized anxiety disorder-7 tool. Int J Appl Basic Med Res. (2017) 7:150. doi: 10.4103/2229-516X.212963
36. Farhane-Medina NZ, Luque B, Tabernero C, Castillo-Mayén R. Factors associated with gender and sex differences in anxiety prevalence and comorbidity: A systematic review. Sci Progress. (2022) 105:1–10. doi: 10.1177/00368504221135469
37. Hussein JR, Yaseen YA. Depression, anxiety, and stress among nurses in Duhok City hospitals. AMJ (Advanced Med Journal) is Sci J Kurdistan Higher Council Med Specialties. (2022) 6:60–9. doi: 10.56056/amj.2022.137
38. Stephens MAC, Wand G. Stress and the HPA axis: role of glucocorticoids in alcohol dependence. Alcohol Research: Curr Rev. (2012) 34:468. doi: 10.1016/j.alcohol.2012.05.002
39. Chang HE, Cho S-H. The influence of social support on the relationship between emotional demands and health of hospital nurses: A cross-sectional study. Healthcare. 9:115. doi: 10.3390/healthcare9010013
Keywords: anxiety, nurses, mental health, occupational stress, Ethiopia
Citation: Misganaw A, Hailu M, Bayleyegn G, Aderaw M, Yigzaw ZA, Alemu T and Asmare L (2024) Exploring factors affecting nurse anxiety in Northwest Ethiopia: a multicenter study. Front. Psychiatry 15:1434701. doi: 10.3389/fpsyt.2024.1434701
Received: 18 May 2024; Accepted: 03 September 2024;
Published: 02 October 2024.
Edited by:
Masoud Rezaei, Iran University of Medical Sciences, IranReviewed by:
Sahar Keyvanloo Shahrestanaki, Iran University of Medical Sciences, IranMasoumeh Neishabouri, Iran University of Medical Sciences, Iran
Behzad Momeni, Iran University of Medical Sciences, Iran
Copyright © 2024 Misganaw, Hailu, Bayleyegn, Aderaw, Yigzaw, Alemu and Asmare. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Lakew Asmare, bGFrZXd0MDcxOTgxQGdtYWlsLmNvbQ==