 Petra Schmid
Petra Schmid Carmen Nauss1
Carmen Nauss1 Carmen Uhlmann
Carmen Uhlmann- 1Klinik für Psychiatrie und Psychotherapie I, Universität Ulm, Ulm, Germany
- 2Zentrum fuer Psychiatry Suedwuerttemberg, Versorgungsforschung, Ravensburg, Germany
- 3Prinzenhof, Leutkirch, Germany
Introduction: Substance use disorders (SUDs) are common, and there is evidence of clinically significant benefit of cognitive behavioral therapy (CBT). The efficacy of CBT in SUDs has been confirmed, although relapse rates of 40%–60% have been reported. An enhancement of CBT-based therapy through an animal-assisted intervention (AAI) with sheep to normalize the occurrence of negative emotions and improve positive emotions as well as mindfulness and self-efficacy expectancy was investigated.
Methods: A single-session AAI with sheep in a group setting was investigated against treatment as usual over time. N = 36 psychiatric inpatients with SUDs were examined by questionnaires before and 1 week after the intervention and additionally immediately after the intervention.
Results: Positive emotions improved significantly in the AAI group 1 week after the intervention with a medium effect size, but not in the control group. Similarly, mindfulness and self-efficacy expectancy improved over time in the AAI group. When exploratory results were evaluated immediately after the intervention while still on the farm, the effects in favor of AAI were even larger.
Conclusions: AAI can thus be considered effective in improving positive emotions, mindfulness, and self-efficacy expectancy. The impressive effect sizes immediately after the intervention encourage us to consider what can be done to maintain these even greater effect sizes over time.
Clinical Trial Registration: https://drks.de/search/de/trial/DRKS00027539, identifier DRKS 00027539.
Introduction
Substance use disorders (SUDs) have a high prevalence worldwide (1). Men are 1.5 to 2.3 times more likely to be affected than women (2). Biological (genetics and developmental stages of the brain) and social (adverse childhood experiences, high stress levels, easy access to drugs, and low social support) factors are recognized as contributing to vulnerability or resilience against the development of SUDs. With regard to the treatment of SUDs, there is evidence of clinically significant benefit of behavioral therapies (1). Cognitive behavioral therapy (CBT) is based on the assumption that behaviors, including substance use, are learned. Through reinforcement processes, the neurobiologically determined rewarding properties of substances (mediated in particular by dopamine) are associated with previously unconditioned stimuli so that a consumption behavior arises and is later maintained (for a detailed overview, see 1). CBT aims to interrupt these learned associations to reduce the likelihood of substance use, manage its consequences, and intervene quickly in the event of relapse (1, 3, 4). This may be achieved by promoting awareness of behavioral patterns and providing the patient with a set of coping skills to functionally regulate negative, as well as positive emotions (1, 3). Self-efficacy, defined as confidence in one’s ability to resolve situations by applying one’s skills (5), increases the likelihood of applying acquired skills and thus also reduces the likelihood of substance use. The efficacy of CBT in SUDs has been confirmed (6), although relapse rates of 40%–60% have been reported (7). Some shortcomings of CBT in SUDs are described. First, CBT focuses heavily on avoidance goals (e.g., risk situations) rather than developing approach-based goals with patients (8). Second, CBT usually works on affect regulation with the goal of cessation of negative emotional states instead of normalizing the occurrence of negative emotions (8) and fostering positive emotions. These may be the key issues for therapeutic success, as SUDs are associated with high levels of negative emotionality and dysfunction in emotion regulation (9), possibly due to traumatic experiences prior to SUDs. For this reason, a non-judgmental mindful perception and acceptance of negative emotions and at the same time an activation of positive emotions is needed to improve treatment of SUD. This could be achieved with an approach based on mindfulness. Mindfulness is defined as an intentional, conscious focus on the immediate, present perception (not on the past or future), which is non-judgmental with regard to thoughts and feelings and is characterized by openness and curiosity (10, 11). In particular, the ability to adopt a non-judgmental and non-reactive attitude toward experiences proved to be a decisive factor for a positive correlation between mindfulness and functional emotion regulation (12). Also, increasing self-efficacy expectations is an important factor in SUD treatment (13). The processes described above could be achieved, for example, through animal-assisted interventions (AAIs) (14). AAI includes interventions that involve animals to positively impact human health and wellbeing (15). AAIs comprise both animal-assisted therapy (AAT) and animal-assisted activity (AAA) (16). AAAs are defined as informal human–animal interactions and interventions conducted by human–animal teams that are goal oriented for motivational, educational, and recreational purposes. AATs, in contrast, are also goal oriented but comprise structured and individualized therapeutic interventions. They are often delivered or directed by licensed healthcare professionals as part of a treatment process (16).
Several reviews on the efficacy of AAI are already available (17–21). They report improvements in positive emotions, social behavior, and level of functioning, while agitated behavior, negative emotions such as anxiety, or clinical symptoms such as depression can be reduced (17, 19, 20). In contrast, reviews criticize both the heterogeneity of the included studies and methodological shortcomings, such as small samples, lack of randomized controlled trials (RCTs), lack of standardization or manualization of interventions, and use of non-specific outcome measures (17, 18, 20). Thus, although there is currently a consensus on the efficacy of AAIs in healthcare, it is not possible to speak of existing evidence (22), and also specific and non-specific factors of AAI have not yet been identified (23).
Therefore, regardless of the reviews, it is worth taking a closer look at single empirical studies with high research standards. In one study, an RCT of n = 61 depressed patients with comorbid child trauma and the effects of a mindfulness-based AAI with sheep was conducted (14). The treatment-as-usual (TAU) group underwent guideline-oriented treatment, and the AAI group received additionally a total of eight manualized animal-assisted sessions in a group setting over an 8-week period. AAI proved to be feasible, highly acceptable, and more effective than treatment as usual in preventing relapse after 1 year; however, statistical significance was scarce. A second AAI study explored the effect of the presence or absence of a therapy dog in the daily routine of inpatients with SUDs and comorbid mental disorders on social interaction as well as on positive and negative emotionality in a control group design. Significant differences in favor of the AAI were found in both the variables improvement of social interaction and emotionality (3). Critically, it is worth noting that there was no standardized procedure for the AAI intervention. Finally, in a series of studies with a pre–post crossover design, the effect of a single-session AAI intervention with a dog was examined. A significant reduction of negative emotions (anxiety) in severely mentally ill inpatients was demonstrated (24–26). Taken together, a group design with a single-session AAI intervention may be useful in improving emotionality in severely mentally ill patients. Due to their genetics, social structure, and sensitivity, sheep have excellent abilities to be used in the field of AAI. They are herd animals and therefore have social behavior skills. Humans can be integrated into their social structure if the sheep are given the opportunity to approach slowly. They provide security and relaxation, as they are very gentle and calm. Due to their sensitivity, mindfulness is necessary in dealing with sheep (27).
The aim of the present pilot study was to examine whether a single session of AAI in a group setting with sheep can reduce negative emotions and improve positive emotions as well as mindfulness and self-efficacy expectancy. For this purpose, psychiatric inpatients with SUDs and comorbid mental disorders were studied directly before and 1 week after the intervention.
Materials and methods
Study design
A controlled, repeated-measures trial was conducted between January 2022 and March 2023 comparing TAU with a single-session animal-assisted intervention in addition to TAU (AAI) in inpatients with SUDs. Allocation to the control group (TAU) or AAI group was determined by the timing of inpatient treatment, as AAI sessions were scheduled in advance. To minimize selection bias due to the lack of an RCT design, exactly the same inclusion and exclusion criteria were applied to the AAI and TAU groups.
Ethical approval was obtained from the ethics committee of the University of Ulm (no. 13/22), including approval of the General Data Protection Regulation EU (GDPR) 2016/679. In accordance with the Declaration of Helsinki, participants were informed and provided written informed consent. The study was registered with the German Registry for Clinical Studies (DRKS00027539, date of first registration March 3, 2022).
Participants
Participants consisted of inpatients in a specialized ward for patients with SUDs and comorbid disorders in a hospital for psychiatry and psychotherapy in Germany. The patients in this ward had already completed the first phase of withdrawal treatment and received further CBT-based psychotherapy. Comorbid diagnoses cover the entire spectrum of mental illnesses. However, patients with comorbid personality disorders, trauma disorders, or attention-deficit/hyperactivity disorder (ADHD) were mainly represented, followed by patients with depression, anxiety, eating disorders, and even schizophrenia.
Inclusion criteria were age between 18 and 65 years, main diagnosis of SUDs, inpatient treatment for at least seven more days, capability for providing consent, and physical requirements such as standing and walking securely. Exclusion criteria were the presence of animal phobia, allergies, and aversion to specific animals (26). Patients in an acute mental crisis were also unable to participate, as were patients with insufficient language comprehension or mental retardation.
One Health Framework
The One Health Framework is an approach addressing human, animal, and environmental health (28). Quality standards for the use of animals in AAI are available (29–33) and also a risk assessment tool for (canine) assisted interventions (34). These standards were adopted.
The AAI took place at the Prinzenhof and was carried out by two certified professionals. PP is a specialist in animal-assisted education and support [certified International Society for animal assisted Therapy (ISAAT)] and the owner of the sheep; CN is a specialist in animal-assisted interventions (ISAAT) and a nurse and knows the participants from the clinical setting. The breed of the sheep was mountain sheep mix or Coburg fox sheep mix. They were partly bottle-fed and were therefore very people-oriented and trusting. The sheep live together as a flock at the Prinzenhof and were looked after and trained by PP. Sheep are animals that normally flee from predators and therefore also often from humans. The animals in this study were well accustomed to humans and did not show pronounced retreat behavior.
Before starting the intervention, the participants were supervised about the rules for handling sheep and the individual characteristics of the sheep to be taken into account. Participants were also informed that the intervention would be stopped immediately if there was a risk of the sheep’s welfare being compromised. In addition, a so-called “protected” area was available to the sheep when working in either the open stable or the paddock. The sheep were conditioned to go to this area whenever they no longer wanted to participate in the intervention. Study participants were instructed not to enter this area and to respect any retreat behavior of the sheep. During the intervention, PP was primarily responsible for the care and supervision of the sheep and CN for the study participants.
AAI procedure
The AAI procedure lasted approximately 5 hours including travel time and took place at the farm “Prinzenhof” in Leutkirch, Germany (see also (35)). The additional costs per intervention group include a fee of 200 € for the “Prinzenhof”, the costs for two professionals for 5 hours, and fuel costs. In case of good weather, the intervention was carried out in the sheep paddock, and in case of bad weather, in the open stable. Each AAI group consisted of four participants and four sheep. The AAI procedure was manualized and divided into seven sections.
1. Observation of the farm owner’s interaction with the sheep: The farm owner (PP) was observed interacting with the sheep in the separated sheep paddock or the open stable. Her interaction with the animals served as a model of mindfulness and respect for the basic needs of the sheep.
2. Introducing the sheep: Still separated by a fence, the sheep were presented individually with names and specific characteristics. This made it easier for the participants to establish a connection with the sheep.
3. Approach via feeding: The sheep were fed by the participants over the fence, and the first physical contact took place.
4. Approach via presence: The participants sat down on prepared logs/chairs in the paddock/open stable. Contact was established exclusively starting from the sheep moving freely. If a sheep joined a participant, it was allowed to make physical contact by petting, although the decision about the duration of the physical contact was up to the sheep. The persistence of contact was closely associated with the participants’ mindfulness of the sheep’s needs. In most cases, the partnerships between sheep and humans were established for the entire session at this stage on the initiative of the sheep.
5. Experiencing competence and attachment: The sheep were leashed by the respective participant, which represented a challenge, even if these sheep were used to it. The sheep then were led out of the paddock/out of the stable and a distance of approximately 200 m was walked together.
6. Free walk-in mindful interaction: Afterward, the leash was removed, and the sheep walked the rest of the course together with the participants. Sheep and participants formed a common flock, which allowed them to experience the connection between sheep and humans. The participants were given the opportunity to interact with the sheep and experience the trust that was built up between them.
7. Farewell: The sheep were returned to the paddock/stable, given water, and were farewelled by the participants. Over snacks and drinks, the participants conducted their feedback session.
Materials
As a primary outcome, the State-Trait Anxiety Inventory—state version (STAI-S (36)) was used. The test quality criteria, such as internal consistency, validity, and test–retest reliability, were satisfactory (Cronbach’s alpha = .90). The questionnaire consists of 20 four-point Likert-scaled items (not at all, somewhat, moderately, and very much so). All items related to the absence or presence of anxiety, with 10 items representing positive emotions, e.g., “I feel secure”, and 10 items representing negative emotions, e.g., “I am worried”. To differentiate between these two expressions, a sum score for positive and one for negative emotions were calculated for the primary outcome.
For secondary outcomes, the Freiburg Mindfulness Inventory short version [FMI (37, 38)] was used. It comprises 14 items, which are assessed on a 4-point Likert scale (almost never, rarely, relatively often, and almost always). The items are worded positively and negatively. The measure has satisfactory test quality criteria. For measuring self-efficacy expectations, the General Self-Efficacy Expectancy Scale, German version [SWE (39)] was applied. The questionnaire consisted of 10 items with agreement from 1 to 4, resulting in a sum score from 10 to 40 (40). Good psychometric proprieties were reported (e.g., Cronbach’s alpha = .92).
The SCL-K-9 (41) as the short version of the Symptom-Checklist [SCL-90-R (42)] was applied to assess the subjectively perceived symptom burden. The nine items were rated on a 5-point Likert scale according to symptoms in the last days. The SCL-K-9 is suitable as a screening instrument for the assessment of a wide range of psychopathological symptoms.
The Objective Social Outcome Index [SIX (43)] was used to assess social integration. The SIX consisted of four items: employment, accommodation, partnership/family, and friendship. The resulting score ranged from 0 to 6. Age, sex, diagnoses, and duration of inpatient stay data were extracted from the medical records after discharge.
Data on sociodemographic variables, degree of social integration, and clinical symptoms were collected to describe and compare the two study groups.
As a qualitative method, the participants were asked to freely write down ideas on the following question: What did the animal-assisted intervention accomplish?
The data were collected before the intervention (PRE) and 1 week after the intervention (POST). At PRE, the STAI-S, FMI, SWE, SCL-K-9, SIX, and sociodemographic data were collected. At POST, the STAI-S and FMI were SWE were measured again. Additionally, some questionnaires were given directly after the intervention while still on the farm (INT). Every participant first wrote down his/her ideas on the following question: What did the animal-assisted intervention accomplish? Afterward, the STAI-S, FMI, and SWE were presented.
Power calculation
For AAIs in psychiatric samples, effect sizes of d = .457 (26) and d = .869 (25) were reported for STAI-S over time. According to the case number calculation with G*Power 3.1 and based on the averaged effect size of both reported studies (d = .66), α = 0.05, β = 0.80, one-sided testing and calculating t-test for dependent samples, n = 16 participants per group with full dataset were targeted. To compensate for possible drop-outs, n = 38 participants were to be recruited.
Statistical analysis
The analysis was performed using IBM SPSS 27®. Dichotomous variables were evaluated with the Chi2 test. Normal distribution was tested using the Kolmogorov–Smirnov test. Group differences were analyzed for normally distributed data with t-tests for independent groups. Variance homogeneity was analyzed using Levene’s test. For non-normally distributed data and ordinal scaled variables, group differences were tested using the Mann-Whitney U test.
To examine improvements in the two primary outcome sum scores of the STAI-S (negative and positive emotion) over time (PRE and POST), Wilcoxon tests were calculated separately for the AAI and TAU groups. In case of significant improvements observed in Wilcoxon tests, r resp. Cohen’s d was calculated for effect size, with r = .1 resp. d = .2 representing a small effect, r = .3 resp. d = .5 representing a medium effect, and r = .5 resp. d = .8 representing a large effect (44). To examine the between-groups effects, Mann–Whitney U tests were calculated. Due to the significant improvements in AAI in contrast to the TAU group between PRE and POST, the results directly after the intervention (INT) were included in the analysis. Here, the Wilcoxon test (PRE vs. INT) and Mann–Whitney U test (AAI vs. TAU) were calculated. In order to consider all three times (PRE, INT, and POST) in one analysis, a repeated-measures ANOVA was calculated. As Field (45) points out, even if the normal distribution assumption is violated (at INT in this case) or if the assumption of homogeneity of variance is violated (at PRE and POST in this case), ANOVA is considered to be a robust procedure and can therefore be used. The assumption of sphericity was checked using Mauchly’s test of sphericity and was not violated.
For secondary outcomes, the assumption of homogeneity of variance was violated at SWE POST, FMI PRE, and POST; hence, corrections were applied. t-Tests for independent resp. dependent samples were calculated, as well as repeated-measures ANOVAs.
For qualitative analysis of participants’ statements to the question “What did the animal-assisted intervention accomplish?” at INT, they were then analyzed in content using an alternating inductive and deductive procedure. The principle of openness prevailed. The statements relevant to the research purpose were paraphrased and then coded. The codes were then summarized into main and subcategories by consensus. The main categories and the identified subcategories as well as corresponding examples were presented.
Results
Comparability of groups
Of the n = 38 recruited patients, n = 20 were assigned to the AAI group and n = 18 to the TAU group. After excluding participants due to missing data, n = 19 participants in the AAI group and n = 17 participants in the TAU group were included in the analyses (see Figure 1). The groups did not differ significantly in age [t (34) = −0.871; p >.05], gender [Chi2(1,36) = 0.000; p >.05], main diagnosis [Chi2(3,36) = 1.730; p >.05], number of secondary diagnoses (U = 160.50; p >.05), and length of stay (U = 143.50; p >.05) in social integration, measured by the SIX (U = 127.00; p >.05), or in subjectively perceived symptom burden, measured by SCL-9-K [t(27.739) = 0.236; p >.05] (see Table 1).
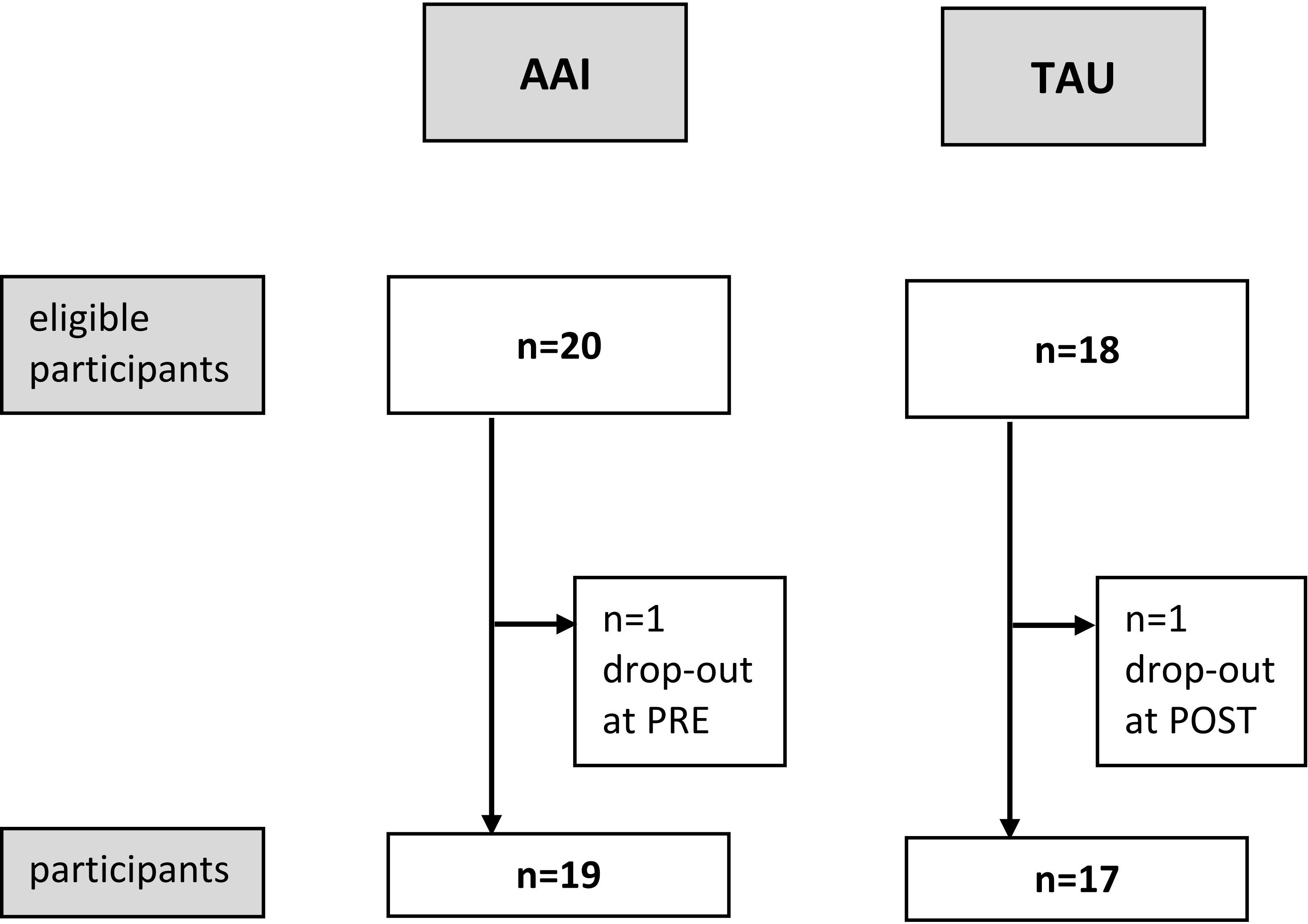
Figure 1. CONSORT for recruitment of both groups, animal-assisted intervention (AAI) and treatment as usual (TAU).
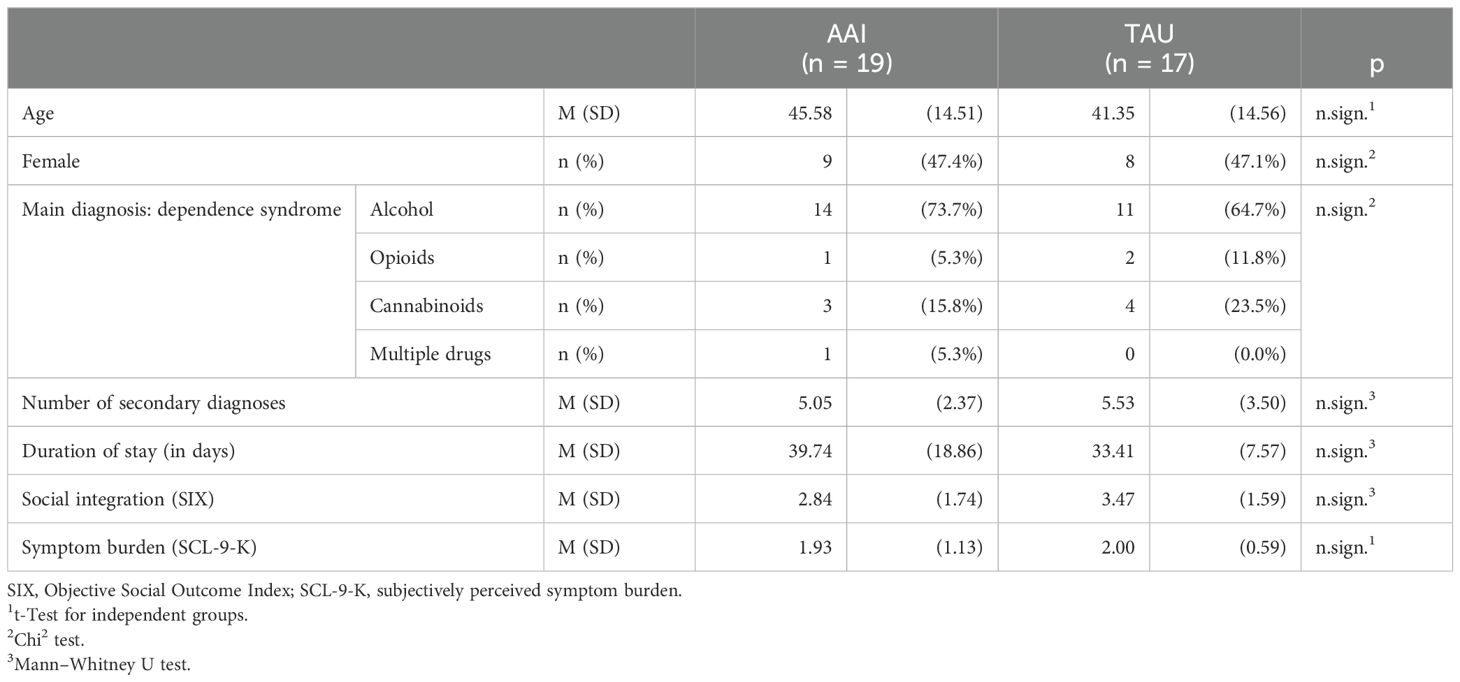
Table 1. Group comparison of animal-assisted intervention (AAI) and treatment as usual (TAU).
Primary outcome
The STAI-S positive emotion sum score displayed a significant improvement over time (PRE and POST) for the AAI group (z = −2.447; p <.05) with a medium effect size (r = .397). However, there was no significant reduction over time in the STAI-S negative emotion sum score (z = −1.724; p = .085). There were no significant differences between the two groups (AAI vs. TAU), neither for PRE (negative emotions: U = 132.500; p >.05, positive emotions: U = 155.500; p >.05) nor for POST (negative emotions: U = 140.000; p >.05, positive emotions: U = 123.500; p >.05). When analyzing the difference between the time before and immediately after the intervention (INT) in the AAI group, the STAI-S negative emotion sum score was significantly reduced (z = −3.336; p <.05) with a large effect size (r = .548), and the STAI-S positive emotion sum score was significantly improved (z = −3.623; p <.001), also with a large effect size (r = .596). At INT, the two groups (AAI and TAU) differed significantly in both sum scores again with large effect sizes (negative emotions: U = 58.000; p <.001; r = .531; positive emotions: U = 39.500; p <.001; r = .634). In repeated-measures ANOVA, a significant time × group interaction was observed for the STAI-S negative emotion sum score [F(2,64) = 6.802; p <.01] and the STAI-S positive emotion sum score [F(2,66) = 11.968; p <.001] (see Figures 2, 3).
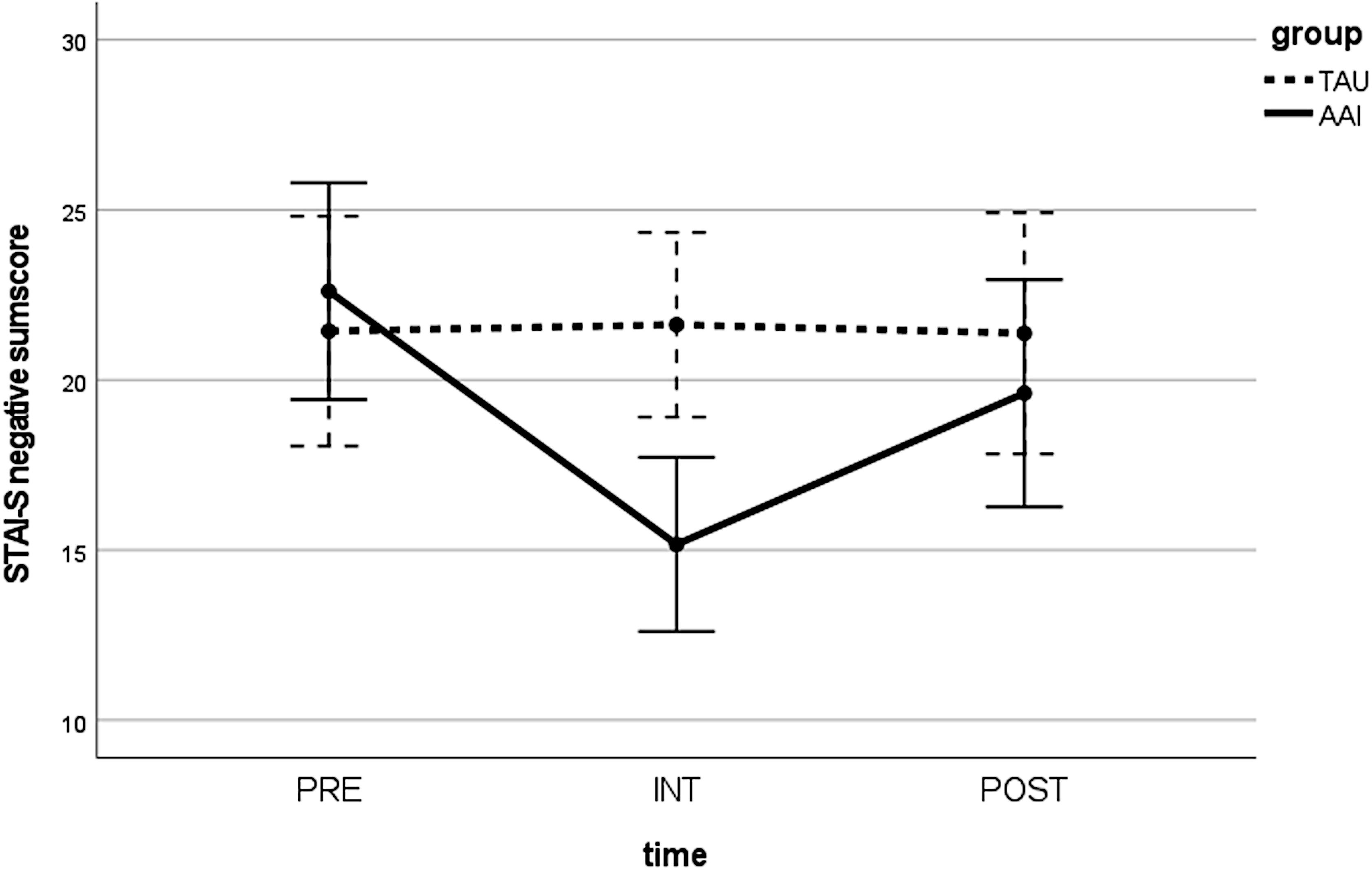
Figure 2. Values in the STAI-S positive emotion sum score over time (PRE, INT, and POST) for both groups (AAI vs. TAU). STAI-S, State-Trait Anxiety Inventory—state version; PRE, pre-measurement before intervention; INT, measurement directly after intervention; POST, post-measurement 1 week after intervention; AAI, animal-assisted intervention; TAU, treatment as usual.
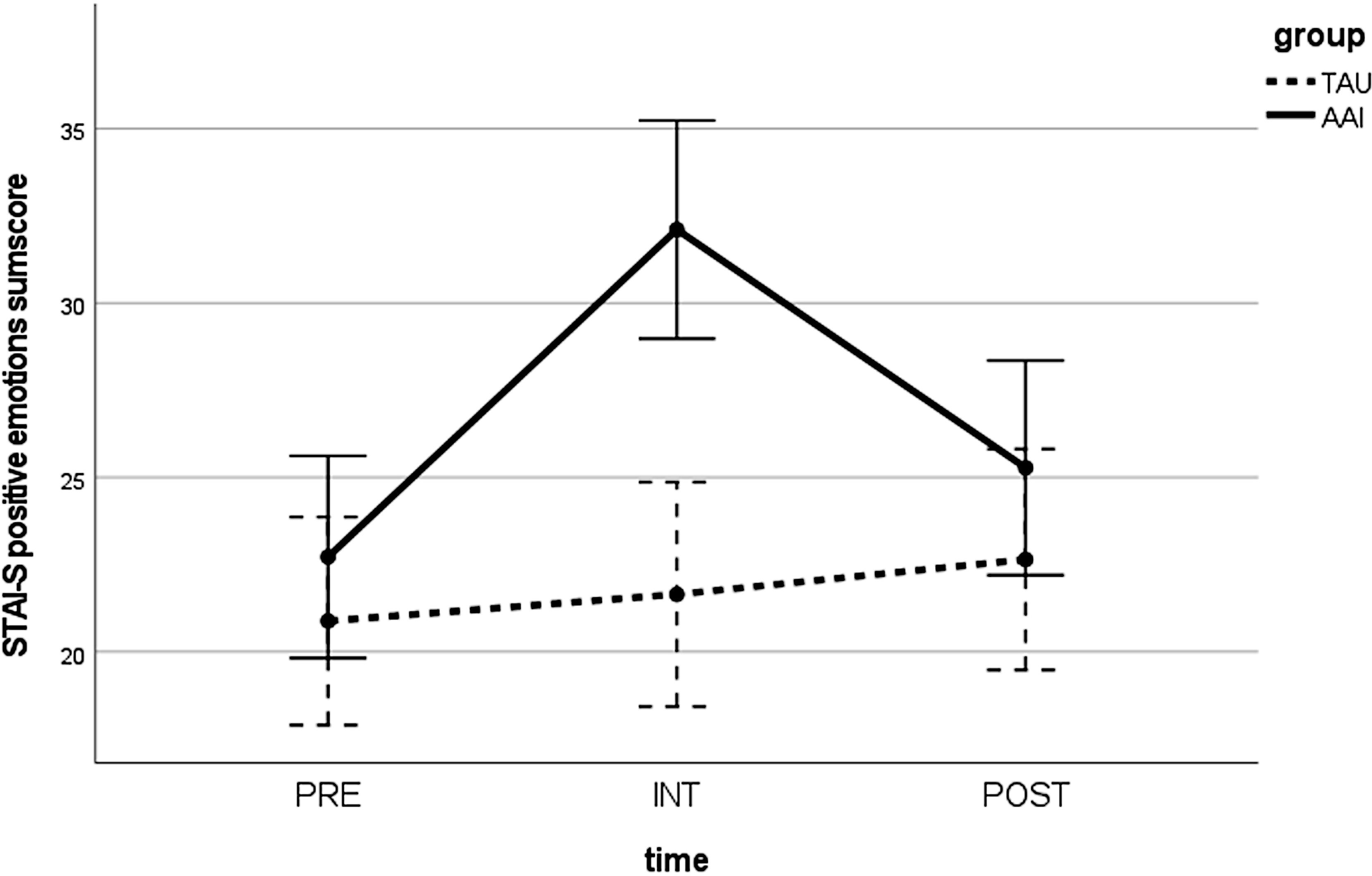
Figure 3. Values in the STAI-S negative emotion sum score over time (PRE, INT, and POST) for both groups (AAI vs. TAU). STAI-S, State-Trait Anxiety Inventory—state version; PRE, pre-measurement before intervention; INT, measurement directly after intervention; POST, post-measurement 1 week after intervention; AAI, animal-assisted intervention; TAU, treatment as usual.
Secondary outcomes
In the mindfulness score (FMI), the AAI group improved significantly from PRE to POST [t(18) = −3.020; p <.01; Cohen’s d = .637] in contrast to TAU [t(16) = −0.495; p >.05]. The two groups did not differ significantly at either PRE [t(32.212) = 0.134; p >.05] or POST [t(33.922) = −1.1483; p >.05]. When including INT in the analysis, a significant time × group interaction [F(2,68) = 7.261; p <.01] was observed. Both groups showed similar levels of mindfulness at PRE. While the TAU group remained at a stable level of mindfulness throughout, the AAI group improved in their mindfulness at INT, but this effect diminished at POST (see Figure 4).
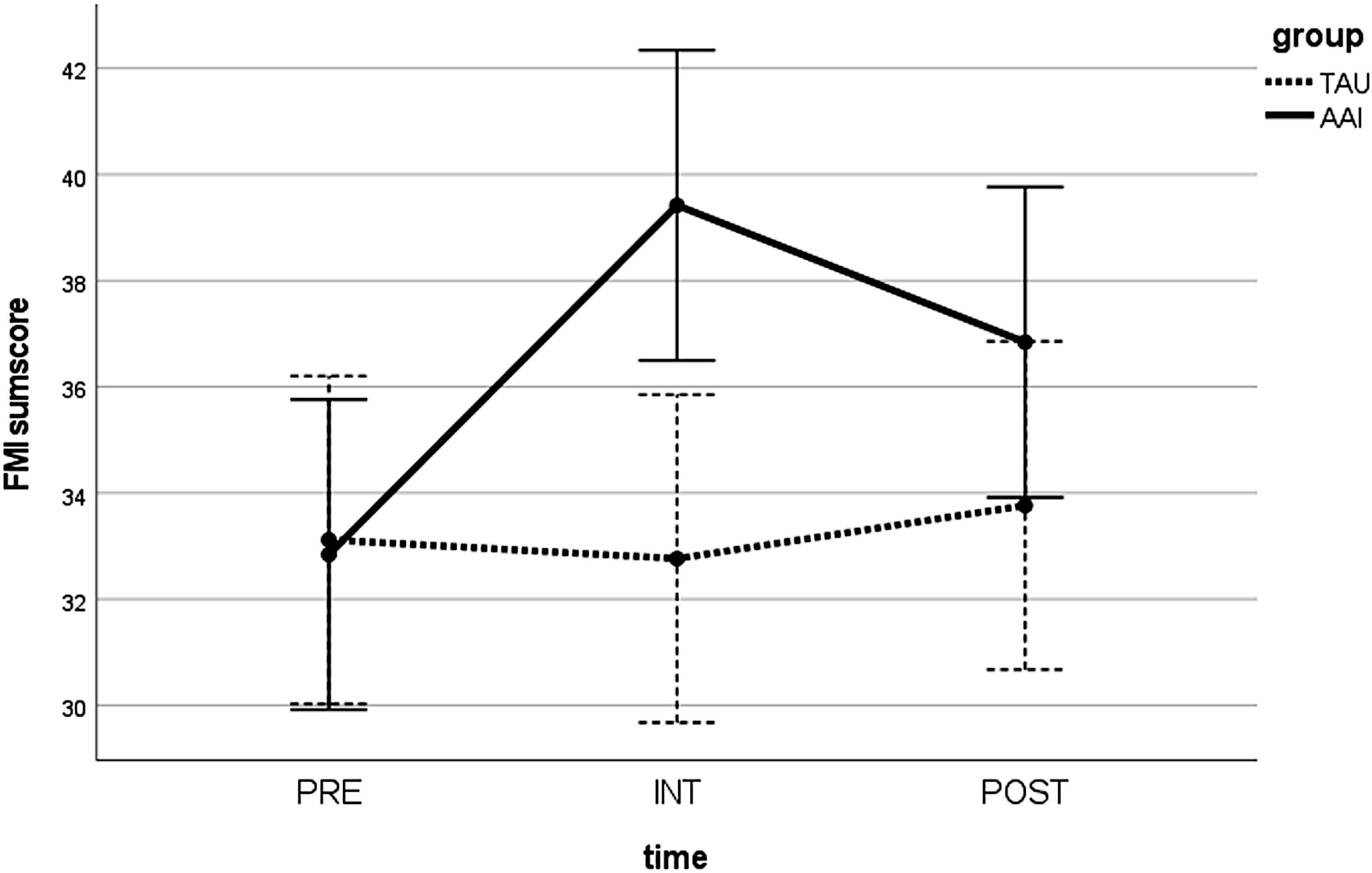
Figure 4. Values in the FMI sum score over time (PRE, INT, and POST) for both groups (AAI vs. TAU). FMI, Freiburg Mindfulness Inventory; PRE, pre-measurement before intervention; INT, measurement directly after intervention; POST, post-measurement 1 week after intervention; AAI, animal-assisted intervention; TAU, treatment as usual.
The AAI group demonstrated also significant improvements in self-efficacy expectancy (SWE) at POST [t(18) = −4.095; p <.01; Cohen’s d = .536], while the TAU group did not [t(16) = 0.982; p >.05]. Again, the groups did not differ significantly from each other at either PRE [t(34) = 0.899; p >.05] or POST [t(32.664) = −0.774; p >.05]. Also, a significant time × group interaction resulted [F(2,68) = 9.112; p <.05]. Both groups started at similar levels, with the TAU participants’ scores changing little over time, while the AAI group’s scores showed a peak at INT (Figure 5).
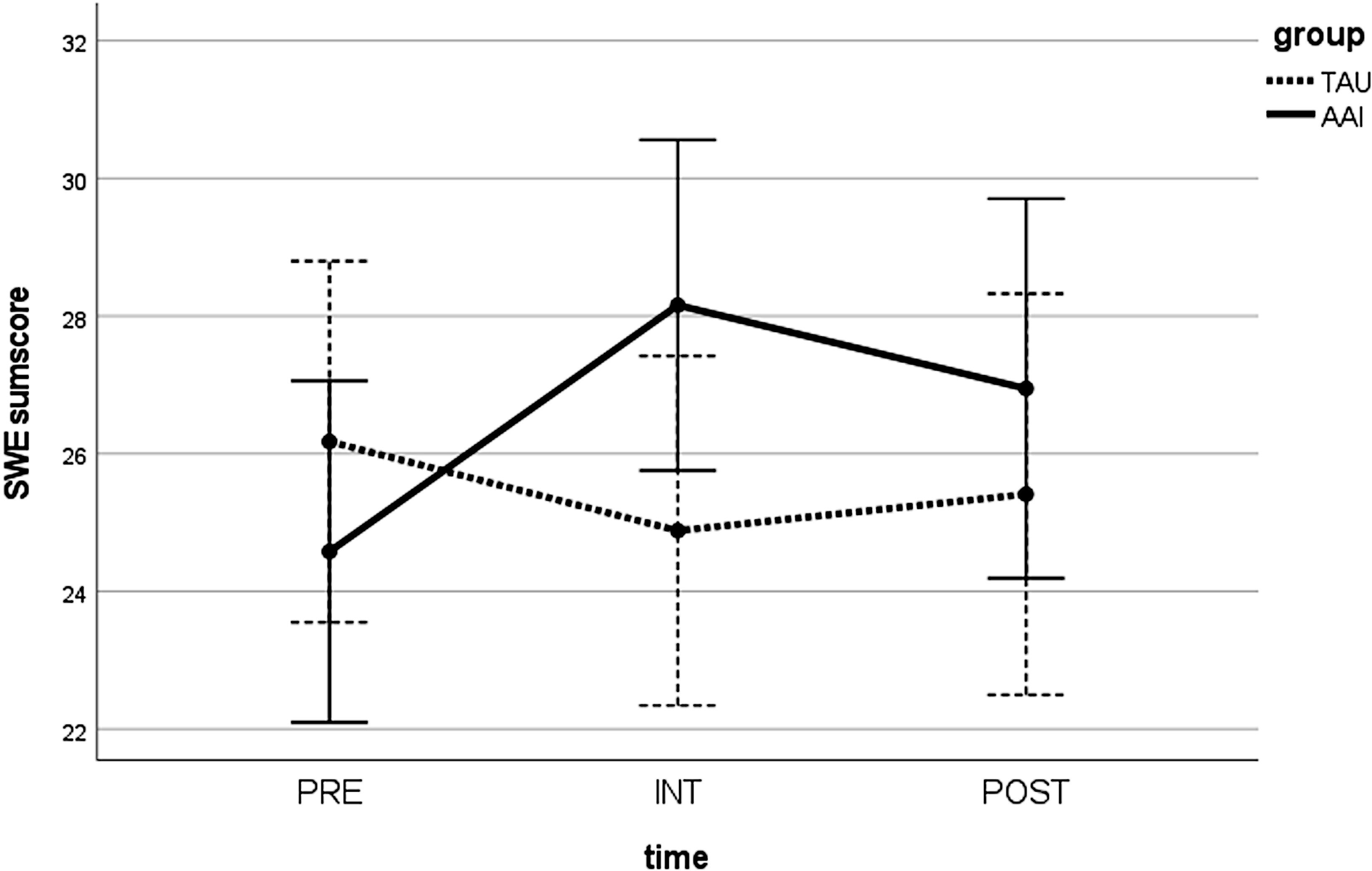
Figure 5. Values in the SWE sum score over time (PRE, INT, and POST) for both groups (AAI vs. TAU). SWE, General Self-Efficacy Expectancy Scale, German version; PRE, pre-measurement before intervention; INT, measurement directly after intervention; POST, post-measurement 1 week after intervention; AAI, animal-assisted intervention; TAU, treatment as usual.
Qualitative analysis of participants’ statements
The n = 78 statements made by the n = 19 AAI participants in response to the question “What did the animal-assisted intervention accomplish?” could be grouped into three categories. As Table 2 displays, the category “evoking positive valence” was mentioned most frequently, with a total of 53 statements. The participants verbalized mainly to have experienced some kind of mindfulness (n = 18), joy and fun (n = 10), and some sort of closeness (n = 8). The second main category is “decreasing negative valence” with n = 9 statements. The participants reported experiencing reduced rumination, prejudice, fear, and tension. In the last category with n = 16 statements, aspects of “positive valence in interacting with animals and nature” were included.
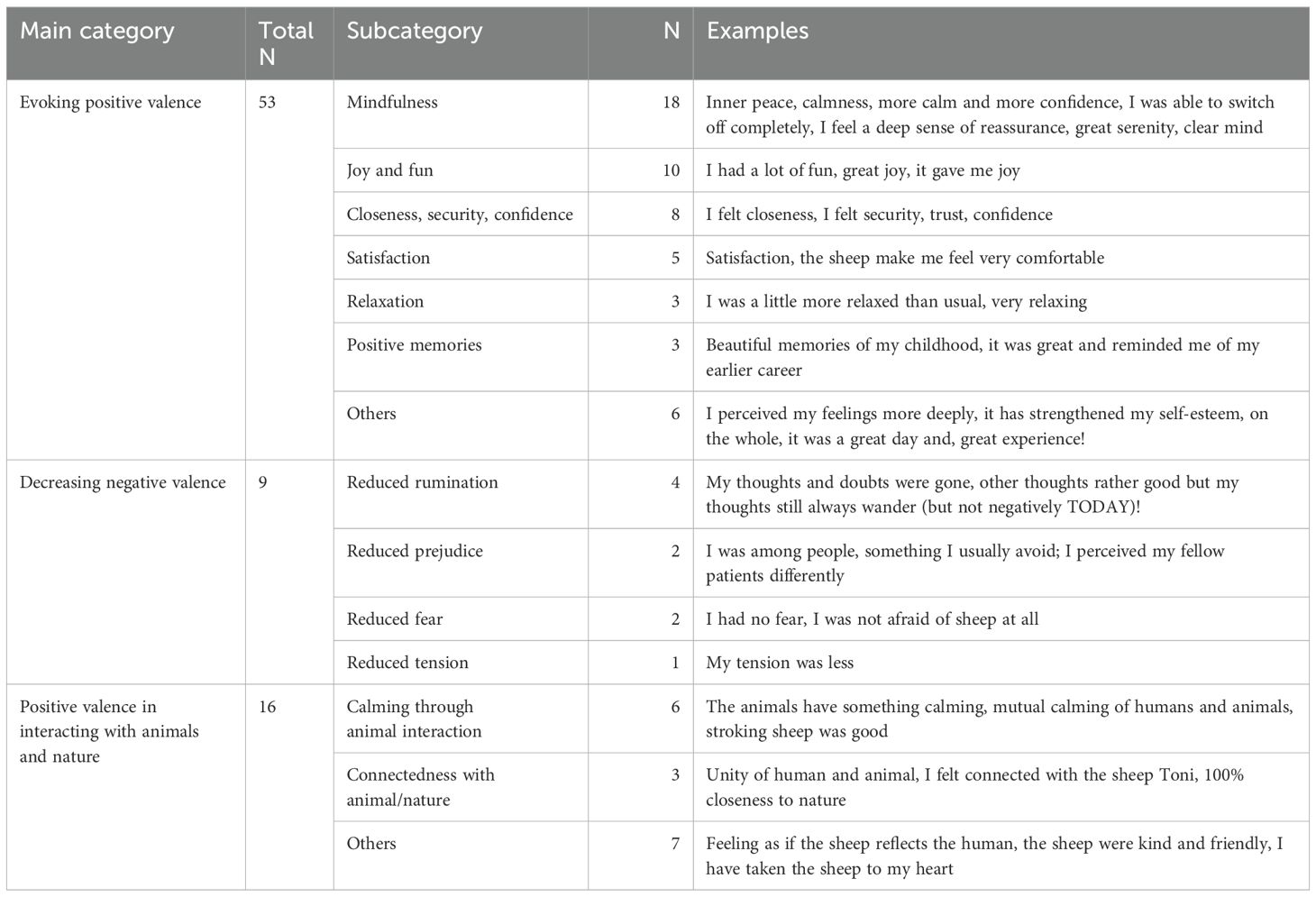
Table 2. Categorized main categories and subcategories from the statements of the n = 19 participants of the AAI group to the question: “What did the animal-assisted intervention accomplish?”.
Discussion
The feasibility of a single-session AAI with sheep as an enhanced CBT-based group therapy for SUDs with comorbid disorders was examined. The effect of reducing negative emotions and improving positive emotions as well as mindfulness and self-efficacy expectancy was investigated. In n = 36 participants, the primary outcome STAI-S positive emotions revealed a significant improvement with a medium effect size for the AAI group (r = .397). No effect was observed in the control group with treatment as usual. Thus, our AAI-enhanced CBT treatment was effective in improving positive emotions, which was still measurable 1 week after the intervention (POST). This is consistent with previous studies examining the effectiveness of AAI in changing emotionality in only a single session (24–26). In these studies, the effects were measured before and immediately after the intervention. For this reason, in addition to the reported results between PRE and POST, the effects immediately after the AAI (INT) were also examined. Here, the analyses yielded an even greater effect size for the changes in the positive (r = .596) and negative emotion sum scores (r = .548). In the secondary outcomes, mindfulness (FMI) and self-efficacy expectancy (SWE) also improved significantly between PRE and POST and again even more immediately after the intervention (INT). Taken together, our AAI-enhanced CBT approach seems to have succeeded in activating positive emotions on the one hand and reducing negative emotions on the other hand, both from a mindful, non-judgmental, accepting attitude. It also appears that the participants have succeeded in internally attributing the processes described above and therefore increasing self-efficacy expectancy. In SUDs associated with the presence of overwhelming negative emotions and deficits in emotion regulation (9), this AAI-enhanced CBT approach could help to improve therapeutic outcomes. The advantage could be that our approach promotes positive emotions and normalizes negative emotions instead of focusing only on emotion regulation, as opposed to CBT alone. This is also supported by the results of the qualitative analysis. Participants’ statements about evoking positive valences (e.g., joy, closeness, mindfulness, contentment, and relaxation) and decreasing negative valences (e.g., anxiety, rumination, prejudice, and tension) can be seen in relation to the STAI-S results with its changes in positive and negative emotions.
The challenge for subsequent studies will be how to maintain the large effect seen in our and other reported studies (24–26) immediately after the intervention (INT) over a longer period of time. Schramm et al. (14) conducted therefore one booster session 3 months after finishing their 8-week program. Further studies will have to address the question of how the emotional moment of the AAI, which was experienced directly in the AAI, can be recreated and retrieved later. Imaginative techniques enriched with external representations of the sheep intervention are conceivable here. This could be realized, for example, through a guided imagination about the individual emotional moment of the AAI experience, anchored externally via a piece of sheep wool. Further research is needed to address this point.
Another issue to discuss is the effect of being outdoors in nature and how these circumstances impact participants. Nature-based interventions have proved to increase positive emotions and reduce negative emotions as well as anxiety and depression (46, 47). Our study also demonstrates the importance of the nature-based effect. The third category in the qualitative analysis included statements containing participants’ interaction with animals and nature, which was valued positively. It must therefore ultimately remain open whether the interaction with sheep, the interaction with nature, or a combination of both is the basic principle for the reported results. Subsequent studies will have to investigate this.
There are several limitations. The main limitation is that we were not able to conduct a randomized controlled trial due to organizational feasibility. Instead, we used a non-randomized control group design. The advantage of this approach was the high clinical–ecological validity. An attempt was made to eliminate a possible selection bias by checking the comparability of the two groups. There were no differences in sociodemographic and clinical data, and thus, a comparability of the groups was assumed. However, the risk of a selection bias is high and cannot be excluded. In a subsequent study, the use of an RCT design is therefore strongly recommended, but a blinding strategy would not be possible in a clinical sample where the TAU group receives no further intervention.
A second limitation concerns the duration of the observation period, which was limited to a total of 1 week. This does not allow any statement about the effect of the AAI beyond this period. Even if such clear effects occurred with INT, statements about the further course of therapy and outcome as well as the further disorder progression are not possible. Perhaps ecological momentary assessments (EMAs) would be useful to more precisely capture and monitor the effect detected at INT. This could also happen over a longer period of time.
At last, the generalizability of the results found in our study is limited. The inpatients studied here were a highly selective sample of SUD patients with a high rate of comorbidity, a somewhat impaired level of functioning, and only a short duration of abstinence. Also, AAI results may vary in other farms and other species, such as dogs.
In conclusion, according to empirical studies, CBT has been the treatment of choice for SUDs alongside medication. However, given the high relapse rates of even successfully treated SUD patients, the question arises of how to enrich CBT. The activation of positive emotions and the simultaneous enabling of a non-judgmental perception and acceptance of negative emotions could provide a new treatment ingredient. Our concept of AAI-enhanced CBT follows this approach. As demonstrated, the AAI was successful in reducing negative emotions and improving positive emotions as well as mindfulness and self-efficacy expectancy immediately after the intervention. Unfortunately, the effect could not be fully maintained after 1 week. Nevertheless, the investigated AAI-enhanced CBT approach seems to be beneficial for emotion activation and tolerance, and therefore, it could be useful in the treatment of emotional dysregulation of SUDs, which is to date under too little consideration in pure CBT.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Ethikkommission der Universität Ulm. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
PS: Conceptualization, Data curation, Formal Analysis, Methodology, Writing – original draft. CN: Conceptualization, Investigation, Writing – review & editing. CJ-E: Writing – review & editing. PP: Investigation, Writing – review & editing. ST: Writing – review & editing. CU: Conceptualization, Formal Analysis, Methodology, Writing – original draft.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Acknowledgments
The authors would like to thank all study participants, humans and sheep. Thanks to the team of ward 2062 of the ZfP Südwürttemberg, Weissenau, for the dedicated support during this research work. Many thanks to PS for his support in creating the graphics. The authors would like to thank Tilman Steinert for being himself.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
AAI, animal-assisted intervention; CBT, cognitive behavioral therapy; EMA, ecological momentary assessment; FMI, Freiburg Mindfulness Inventory; INT, measurement directly after intervention; ISAAT, International Society for animal assisted Therapy; POST, post-measurement 1 week after intervention; PRE, pre-measurement before intervention; SCL-K-9, Symptom-Checklist short version; SIX, Objective Social Outcome Index; STAI-S, State-Trait Anxiety Inventory—state version; SUDs, substance use disorders; SWE, General Self-Efficacy Expectancy Scale, German version; TAU, treatment-as-usual.
References
1. Volkow ND, Blanco C. Substance use disorders: a comprehensive update of classification, epidemiology, neurobiology, clinical aspects, treatment and prevention. World Psychiatry. (2023) 22:203–29. doi: 10.1002/wps.21073
2. GBD 2016. Alcohol and Drug Use Collaborators. The global burden of disease attributable to alcohol and drug use in 195 countries and territories, 1990-2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Psychiatry. (2018) 5:987–1012. doi: 10.1016/S2215-0366(18)30337-7
3. Uhlmann C, Nauß C, Worbs A, Pfund U, Schmid P. Effekte einer tiergestützten Intervention in der stationären psychiatrischen Suchtbehandlung – eine Pilotstudie. Fortschr Neurol Psychiatr. (2019) 87:305–11. doi: 10.1055/a-0832-8810
4. Marlatt GA, Donovan DM. Relapse prevention: maintenance strategies in the treatment of addictive behaviors. New York: Guilford (2005).
5. Bandura A. Self-efficacy: Toward a unifying theory of behavioural change. psychol Review. (1977) 84:191–215. doi: 10.1037/0033-295X.84.2.191
6. Magill M, Ray L, Kiluk B, Hoadley A, Bernstein M, Tonigan JS, et al. A meta-analysis of cognitive-behavioral therapy for alcohol or other drug use disorders: Treatment efficacy by contrast condition. J Consult Clin Psychol. (2019) 87:1093–105. doi: 10.1037/ccp0000447
7. McLellan AT, Lewis DC, O'Brien CP, Kleber HD. Drug dependence, a chronic medical illness: implications for treatment, insurance, and outcomes evaluation. JAMA. (2000) 284:1689–95. doi: 10.1001/jama.284.13.1689
8. Bowen S, Witkiewitz K, Clifasefi SL, Grow J, Chawla N, Hsu SH, et al. Relative efficacy of mindfulness-based relapse prevention, standard relapse prevention, and treatment as usual for substance use disorders: a randomized clinical trial. JAMA Psychiatry. (2014) 71:547–56. doi: 10.1001/jamapsychiatry.2013.4546
9. Stellern J, Xiao KB, Grennell E, Sanches M, Gowin JL, Sloan ME. Emotion regulation in substance use disorders: a systematic review and meta-analysis. Addiction. (2023) 118:30–47. doi: 10.1111/add.16001
10. Kabat-Zinn J. Full catastrophe living: using the wisdom of your body and mind to face stress, pain, and illness. New York: Delta Trade Paperback/Bantam Dell (2005).
11. Bishop SR, Lau M, Shapiro S, Carlson L, Anderson ND, Carmody J, et al. Mindfulness: A proposed operational definition. Clin psychology: Sci practice. (2004) 11:230. doi: 10.1093/clipsy.bph077
12. Iani L, Lauriola M, Chiesa A, Cafaro V. Associations between mindfulness and emotion regulation: the key role of describing and nonreactivity. Mindfulness. (2019) 10:366–75. doi: 10.1007/s12671-018-0981-5
13. Moniz-Lewis DI, Stein ER, Bowen S, Witkiewitz K. Self-efficacy as a potential mechanism of behavior change in mindfulness-based relapse prevention. Mindfulness. (2022) 13:2175–85. doi: 10.1007/s12671-022-01946-z
14. Schramm E, Breuninger C, Wohlfarth R, Elsaesser M, Piosczyk H, Fangmeier T. Effectiveness of nature- and animal assisted mindfulness for relapse prevention in depressed patients with a history of childhood maltreatment. Front Psychiatry. (2022) 13:899318. doi: 10.3389/fpsyt.2022.899318
15. Kiers AH, Nishimura KM, Dewa CS. Leveraging campus landscapes for public health: A pilot study to understand the psychological effects of urban sheep grazing on college campuses. Int J Environ Res Public Health. (2023) . 20:1280. doi: 10.3390/ijerph20021280
16. Teo JT, Johnstone SJ, Römer SS, Thomas SJ. Psychophysiological mechanisms underlying the potential health benefits of human-dog interactions: A systematic literature review. Int J Psychophysiol. (2022) . 180:27–48. doi: 10.1016/j.ijpsycho.2022.07.007
17. Bert F, Gualano MR, Camussi E, Pieve G, Voglino G, Siliquini R. Animal assisted intervention: A systematic review of benefits and risks. Eur J Integr Med. (2016) 8:695–706. doi: 10.1016/j.eujim.2016.05.005
18. Santaniello A, Dicé F, Claudia Carratú R, Amato A, Fioretti A, Menna LF. Methodological and terminological issues in animal-assisted interventions: an umbrella review of systematic reviews. Animals. (2020) 10:759. doi: 10.3390/ani10050759
19. Jones MG, Rice SM, Cotton SM. Incorporating animal-assisted therapy in mental health treatments for adolescents: A systematic review of canine assisted psychotherapy. PLoS One. (2019) 14:e0210761. doi: 10.1371/journal.pone.0210761
20. Perkins J, Bartlett H, Travers C, Rand J. Dog-assisted therapy for older people with dementia: a review. Australas J Ageing. (2008) 27:177–82. doi: 10.1111/j.1741-6612.2008.00317.x
21. Hediger K, Wagner J, Künzi P, Haefeli A, Theis F, Grob C, et al. Effectiveness of animal-assisted interventions for children and adults with post-traumatic stress disorder symptoms: a systematic review and meta-analysis. Eur J Psychotraumatol. (2021) 12:1879713. doi: 10.1080/20008198.2021.1879713
22. Widmayer S, Borgwardt S, Lang UE, Huber CG. Could animal-assisted therapy help to reduce coercive treatment in psychiatry? Front Psychiatry. (2019) 10:794. doi: 10.3389/fpsyt.2019.00794
23. Wagner C, Grob C and Hediger K. Specific and non-specific factors of animal-assisted interventions considered in research: A systematic review. Front Psychol. (2022) 13:931347. doi: 10.3389/fpsyg.2022.931347
24. Barker SB, Dawson KS. The effects of animal-assisted therapy on anxiety ratings of hospitalized psychiatric patients. Psychiatr Serv. (1998) 49:797–801. doi: 10.1176/ps.49.6.79
25. Lang UE, Jansen JB, Wertenauer F, Gallinat J, Rapp MA. Reduced anxiety during dog assisted interviews in acute schizophrenic patients. Eur J Integr Med. (2010) 2:123–7. doi: 10.1016/j.eujim.2010.07.002
26. Hoffmann AO, Lee AH, Wertenauer F, Ricken R, Jansen JJ, Gallinat J, et al. Dog-assisted intervention significantly reduces anxiety in hospitalized patients with major depression. Eur J Integr Med. (2009) 1:145–8. doi: 10.1016/j.eujim.2009.08.002
27. Nauss C. Wo(h)llige Schafstunden, Projekt zur tiergestützten schematherapeutischen Beziehungsarbeit. Institut Tiere im Einsatz, Schongau (2022).
28. Hediger K, Meisser A, Zinsstag J. A one health research framework for animal-assisted interventions. Int J Environ Res Public Health. (2019) 16:640. doi: 10.3390/ijerph16040640
29. IAHAIO. IAHAIO White Paper 2014, Updated for 2018. The IAHAIO Definitions for Animal Assisted Intervention and Guidelines for Wellness of Animals Involved in AAI (2018). Available online at: http://pat.org.za/wp-content/uploads/2021/04/IAHAIO-WHITE-PAPER-TASK-FORCE-FINAL-REPORT_2018.pdf (Accessed August 02, 2023).
30. Wohlfarth R, Sandstedt L. Animal assisted activities with dogs. In: Guideline for Basic Requirements & Knowledge. Publishing House of Janusz Korczak Pedagogical University in Warsaw, Warsaw (2016).
31. Wohlfarth R, Olbrich E. Qualitätsentwicklung und Qualitätssicherung in der Praxis tiergestützter Interventionen. Zürich: ISAAT (2014).
32. Tierärztliche Vereinigung für Tierschutz e.V, in: Nutzung von Tieren im soziale Einsatz Merkblatt Nr. 131.11 Schafe (2011). Belm. Available online at: https://www.tierschutz-tvt.de/alle-merkblaetter-undstellungnahmen/c304 (Accessed March 03; 2022).
33. Tierärztliche Vereinigung für Tierschutz e.V, in: Tiere im sozialen Einsatz Merkblatt Nr. 131 (Allgemeine Grundsätze) (2021). Belm. Available online at: https://www.tierschutz-tvt.de/alle-merkblaetterund-stellungnahmen/c304 (Accessed March 03; 2022).
34. Brelsford VL, Dimolareva M, Gee NR, Meints K. Best practice standards in animal-assisted interventions: how the LEAD risk assessment tool can help. Animals. (2020) 10:974. doi: 10.3390/ani10060974
35. Schmid P, Nauss C, Uhlmann C. Schematherapie mit Schafen: Tiergestützte Intervention in der schematherapeutischen, psychiatrischen Suchtbehandlung. Psychiat Prax. (2023) 50:209–13. doi: 10.1055/a-1933-6540
36. Spielberger CD, Gorsuch RL, Lushene R, Vagg PR, Jacobs GA. Manual for the State-Trait Anxiety Inventory. Palo Alto, CA: Consulting Psychologists Press (1983).
37. Walach H, Buchheld N, Buttenmüller V, Kleinknecht N, Schmidt S. Measuring mindfulness-The Freiburg Mindfulness Questionnaire. Construction, validation, short version. J Medit Med Res. (2003) 3:97–8.
38. Walach H, Buchheld N, Buttenmüller V, Kleinknecht N, Grossman P, Schmidt S. Empirische Erfassung der Achtsamkeit – die Konstruktion des Freiburger Fragebogens zur Achtsamkeit (FFA) und weitere Validierungsstudien. In: Heidenreich T, Michalak J, editors. Achtsamkeit und Akzeptanz in der Psychotherapie. Deutsche Gesellschaft für Verhaltenstherapie, Tübingen (2004). p. 727–70.
39. Jerusalem M, Schwarzer R. SWE. Skala zur allgemeinen selbstwirksamkeitserwartung. In: Brähler E, Schumacher J, Strauß B, editors. Diagnostische Verfahren in der Psychotherapie. Hogrefe, Göttingen (2001).
40. Schumacher J, Klaiberg A, Brähler E. Bevölkerungsrepräsentative Normierung der Skala zur Allgemeinen Selbstwirksamkeitserwartung. IAGNOSTICA | Manuskriptfassung vom 29.03.2001. Available online at: http://userpage.fu-berlin.de/~health/swe_norm.pdff. (Accessed October 10, 2019).
41. Hessel A, Schumacher J, Geyer M, Brähler E. Symptom-checkliste SCL-90-R. Diagnostica. (2001) . 47:27–39. doi: 10.1026//0012-1924.47.1.27
42. Franke GH. SCL-90-R. Die Symptom-Checkliste von Derogatis – Deutsche Version. Göttingen: Beltz Test Gesellschaft (2002).
43. Priebe S, Watzke S, Hansson L, Burns T. Objective social outcomes index (SIX): a method to summarise objective indicators of social outcomes in mental health care. Acta Psychiatr Scand. (2008) 118:57–63. doi: 10.1111/j.1600-0447.2008.01217.x
44. Cohen J. Statistical power analysis for the behavioural sciences. New York: Academic Press (1988).
46. Browning MHEM, Mimnaugh KJ, van Riper CJ, Laurent HK, LaValle SM. Can simulated nature support mental health? Comparing short, single-doses of 360-degree nature videos in virtual reality with the outdoors. Front Psychol. (2020) 10:2667. doi: 10.3389/fpsyg.2019.02667
Keywords: animal-assisted intervention, sheep, psychiatric, inpatient, addiction, emotion, substance use disorder
Citation: Schmid P, Nauss C, Jauch-Ederer C, Prinz P, Tschöke S and Uhlmann C (2024) Can sheep help to improve positive emotions, mindfulness, and self-efficacy expectancy? A pilot study of animal-assisted intervention as an enhanced CBT-based therapy for substance use disorders. Front. Psychiatry 15:1432679. doi: 10.3389/fpsyt.2024.1432679
Received: 14 May 2024; Accepted: 16 September 2024;
Published: 15 October 2024.
Edited by:
Emily Shoesmith, University of York, United KingdomReviewed by:
Morgana Galardi, Experimental Zooprophylactic Institute of the Venezie (IZSVe), ItalyLaura Contalbrigo, Experimental Zooprophylactic Institute of the Venezie (IZSVe), Italy
A. Haven Kiers, University of California, Davis, United States
Copyright © 2024 Schmid, Nauss, Jauch-Ederer, Prinz, Tschöke and Uhlmann. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Petra Schmid, cGV0cmEuc2NobWlkQHpmcC16ZW50cnVtLmRl
†ORCID: Petra Schmid, orcid.org/0000-0002-9066-4147
Stefan Tschöke, orcid.org/0000-0002-8612-7752
Carmen Uhlmann, orcid.org/0000-0002-0119-0286