
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychiatry , 27 June 2024
Sec. Addictive Disorders
Volume 15 - 2024 | https://doi.org/10.3389/fpsyt.2024.1420508
 Alessio Zizzi1*
Alessio Zizzi1* Isabel Margherita Berri2Alessandro Berri3Martina Occhipinti2Andrea Escelsior1,3
Isabel Margherita Berri2Alessandro Berri3Martina Occhipinti2Andrea Escelsior1,3 Riccardo Guglielmo1,3Beatriz Pereira Da Silva1
Riccardo Guglielmo1,3Beatriz Pereira Da Silva1 Mario Amore1
Mario Amore1 Gianluca Serafini1,3
Gianluca Serafini1,3Background: Alcohol use disorder (AUD) is a major public health concern due to its various physical, psychological, and social consequences. Despite regulatory differences, abstinence remains the primary treatment objective. Addressing the multifaceted nature of alcohol use disorder requires a comprehensive approach.
Methods: 150 AUD patients (66%male) with a mean age of 54.10 ± 11.3 years were recruited for the study. Depression, impulsivity, alexithymia, and hopelessness were assessed to determine if there were significant differences in these dimensions between abstinent (N=72) and active drinkers (N=78).
Results: The study found significant differences in the psychological dimensions scores, active drinkers exhibited higher levels of depression, impulsivity, alexithymia, and hopelessness compared to abstinent patients.
Conclusion: Treatment outcomes for patients with AUD vary between regulatory agencies, but abstinence remains the safest and most preferred objective in managing AUD. Prioritizing abstinence-oriented interventions is crucial for achieving long term recovery and minimizing relapse risk. These results emphasize the intricate relationship between AUD and mental health issues, highlighting the need for comprehensive interventions addressing both alcohol consumption and associated psychological distress. Promoting abstinence (or at least reducing alcohol consumption) not only preserves mental health but also prevents life-threatening consequences such as suicide.
Alcohol use disorder (AUD) is an insidious disorder, characterized by an often intermittently relapsing course. In Europe, AUD affects approximately 66.2 million people aged 15 and over, predominantly men, with Italy showing one of the lowest prevalences, both for men (1.7%) and women (1.0%) (1). As an individual relapses into drinking, they become more likely to develop a variety of additional somatic complications. including metabolic disorders, hypertension and cerebrovascular diseases (2). The World Health Organization (WHO), ranks harmful alcohol consumption as the third risk factor for premature death and disability in the world (3).The consequences related to AUD do not only concern the physical sphere, but also extend to psychological and social spheres (4–6).
AUD increases the risk of physical harm and dangerous behavior and impacts school and work performance, childcare and household responsibilities, among other things. Using alcohol in dangerous circumstances, such as driving a car or operating machinery while intoxicated, is common. Furthermore, individuals with AUD may persist in drinking despite being aware of the significant physical, psychological, social, or interpersonal problems that result (4).
The framework outlined by Scafato (1) in the Report of the Italian National Institute of Health highlights the urgency of considering “harmful consumers” of alcohol as subjects “in need for treatment” pursuant to the DSM-5, clinically assimilating them to alcohol dependents. This perspective underlines the need for timely management and intervention in local services.
In a bio-psycho-social perspective, Sliedrecht and colleagues (7), identified several factors associated with AUD relapse, including the presence of psychiatric comorbidity, duration of abstinence, substance use disorder (polyaddiction), smoking, age (particularly the age of onset of AUD), sex, family history of AUD, physical health status, employment status, socioeconomic status, education level, presence of a supportive relationship (such as marriage), and motherhood for women. These factors contribute to a deeper understanding of the disorder and its involved variables.
Several psychological dimensions play a direct role in the achievement and maintenance of alcohol abstention. The interconnection between AUD and depression is well-documented, with numerous studies revealing close and complex links between the two disorders. Research by Boden and Fergusson (8) indicates that AUD significantly increases the risk of developing depression, which can manifest bidirectionally or coexist in comorbidity. Sadock et al. (9)highlight that while 80% of individuals with AUD report intense negative affect, only about 10% meet criteria for an independent diagnosis of depression. Treatment for AUD often leads to rapid improvement in depressive symptoms (10–14). Recent research by Hallgren et al. (15) suggests that reduction in alcohol consumption is associated with decreased prevalence of positive depression screenings. However, depression comorbid with AUD predicts less favorable treatment outcomes (16, 17). Similarly, heavy alcohol users have an increased risk of depression even after reducing alcohol consumption (18). Depression comorbid with AUD is associated with poorer clinical outcomes, including higher rates of treatment dropout, relapse risk, and rapid post-treatment relapse (19–21). Depression and hopelessness are closely intertwined, with research consistently indicating an increased risk of suicide among individuals dealing with AUD (22–28). Hopelessness, closely linked to suicidal intent, is prevalent in individuals with AUD further increasing suicide risk (29–31). Research indicates that alcohol can be used as a form of self-medication to manage dysphoric affects, suggesting that hopelessness may exacerbate alcohol use or other impulsive behaviors (32–34). Regarding AUD and impulsivity, studies highlight impulsivity’s significant contribution to AUD severity (35–38). High impulsivity levels in AUD patients are associated with family history of AUD and characterize individuals who drink to experience pleasurable effects (39, 40). Impulsivity, known to predict relapse during treatment, particularly early relapse, significantly impacts post-treatment quality of life and well-being. This tendency toward impulsive behaviors not only jeopardizes the effectiveness of treatment interventions but also undermines efforts to maintain long-term sobriety (7, 41–44). Interestingly, impulsivity’s adverse effects on treatment outcomes may be compounded by its association with alexithymia (45). Research indicates that alexithymia serves as a significant risk factor for the development and severity of AUD, with alexithymia individuals exhibiting a propensity to consume more alcohol and experiencing poorer treatment outcomes (46–48). This suggests a potential synergistic relationship between impulsivity and alexithymia, wherein impulsivity exacerbates emotional dysregulation, while alexithymia amplifies impulsive behaviors, creating a challenging cycle that impedes successful recovery from AUD (49–56).From the study of the literature, we can grasp the importance of abstinence as a goal for the treatment of patients with AUD. Possible variations overtime of the impact of psycopathological predictors on the risk of relapse are still unclear. Evidence suggests that certain personality traits and impulsivity play a more important role than other factors in early phases of addiction treatment, whereas the effect of alexithymia on AUD seems to be mediated by negative mood and craving, which might be sustained over time (47). Despite the large quantity of studies on the positive effects of prolonged abstinence, there is a scarcity of studies investigating the possible presence of modifications or advantages of abstinence in relation to psychological dimensions such as depression, hopelessness, impulsivity, and alexithymia in a population of patients with AUD. Given the high influence of these dimensions on the quality of life and more generally on the treatment outcomes of patients with AUD, we decided to conduct a study with the aim to verify whether there were substantial differences with respect to these dimensions between abstinent and active drinkers diagnosed with AUD.
We enrolled 150 outpatients (100 males, 50 females) with a diagnosis of AUD according to the DSM-5 (57).The patients were recruited from the outpatient alcohol unit at the Ligurian Regional Alcohol Centre (San Martino Hospital, Genoa). The study was approved by the Institutional Review Board and national regulatory authorities in accordance with local requirements and was conducted in accordance with Good Clinical Practice Guidelines and the Declaration of Helsinki (1964) and subsequent revisions (D.3.2.764.14). After receiving information on the intervention, all subjects provided written informed consent.
Once the reference population was identified (patients who regularly attend the department for detoxification and/or check-ups N=245), the appropriate sample size was calculated for the analyses to be carried out using the online program “Sample Size Calculator” of the Creative Research Systems provided by the Istituto Superiore della Sanità (58). The analyses showed that 150 subject measurements were necessary to have a confidence level of 95%, therefore it was decided that the sample size should be n=150 patients using simple random extraction.
The inclusion criteria chosen to understand if a patient was eligible to enrol were: having a diagnosis of AUD according to DSM-5, being adults (aged 18 and over), having mastered the spoken and written Italian language, not being in a state of acute alcohol or drug intoxication at the time of the test and the absence of organic brain syndromes (e.g. Wernicke – Korsakoff syndrome or alcoholic encephalopathy).
At the time of testing, 78 outpatients were active drinkers while 72 outpatients were abstinent (we considered a patient abstinent after 12 weeks of sobriety, the mean time of abstinent group was 64 weeks).
Data of sociodemographic and clinical interest were collected through a specifically constructed questionnaire. Furthermore, 4 psychometric scales were administered: Beck Depression Inventory II (BDI-II), Beck Hopelessness Scale (BHS), Barratt Impulsiveness Scale (BIS-11), Toronto Alexithymia Scale (TAS-20). The BDI developed by Beck and colleagues in 1961 is one of the most used self-report questionnaires for the self-assessment of depression in clinical and research settings. This scale is made up of 21 items that allow us to detect the behavioral manifestations of depression and measure their level of severity. BHS (59)is one of the first instruments used in a clinical setting to measure patients’ suicidal risk. The BHS is a self-report questionnaire consisting of 20 items assessed on a dichotomous response scale (True or False). For the total scoring of the scale, a score of 1 or 0 is assigned depending on whether the subject answered true or false to an item and whether the item is formulated in a positive or negative key. (BIS) is a standard instrument that has had an influence in shaping current theories of impulse control and has played a key role in studies of impulsivity and its biological, psychological, and behavioral correlates (60).
BIS is made up of 30 items to which the subject responds on a Likert-type scale ranging from 1 (never/rarely) to 4 (almost always/always), the final score is therefore given by the sum of the item scores. TAS-20 (61) is one of the most used instruments in the clinical setting to measure alexithymia. The TAS-20 is a self-report questionnaire composed of 20 items assessed on a 5-point Likert scale (1 = strongly disagree; 5 = strongly agree) which measures the degree of alexithymia present in the person.
The IBM SPSS Statistics program was used to carry out the data analysis (62).
Chi squares were used for nominal values, while the Mann-Whitney U test was used for differences in test scores between the drinking and abstinent groups (after checking for normality using Shapiro-Wilks). To correct the p values with multiple comparison, False Discovery Rate (FDR) was used.
A total of 150 patients diagnosed with AUD were included in the study, consisting of 100 men (66.7%) and 50 women (33.3%), with a mean age of 54.10 years (SD = 11.3). Sociodemographic and clinical characteristics are summarized in Table 1. The sample consisted of two groups: 78 active drinkers and 72 abstinent patients. There were no statistically significant differences between active drinkers and abstinent individuals in terms of age, sex, nicotine use, annual income, or AUD family history.
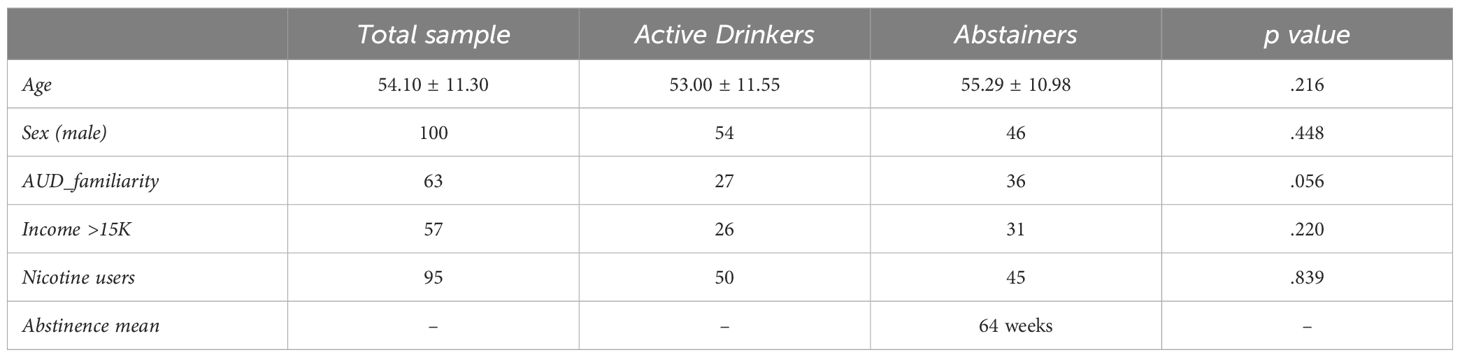
Table 1 Descriptives of the sample comparing abstainers and active drinkers.
Results from the non-parametric analysis corrected for multiple comparisons (FDR) are shown in Table 2 and Figure 1. Active drinkers had significantly higher BDI-II scores compared to abstinent patients (Mann-Whitney U = .0001, p = .004). The mean BDI-II score for active drinkers was 18.49 (SD = 11.31) while for abstinent patients it was 11.90 (SD = 10.28). BHS scores were higher in active drinkers than in abstinent patients (Mann-Whitney U = .030, p = .030). Active drinkers had a mean BHS score of 8.28 (SD = 5.50), whereas abstinent patients had a mean score of 6.40 (SD = 4.78). According to the BIS-11, active drinkers exhibited higher impulsivity levels compared to abstinent patients (Mann-Whitney U = .001, p = .002). The mean BIS-11 score for active drinkers was 69.67 (SD = 11.09) versus 63.40 (SD = 11.29) for abstinent patients. TAS-20 scores indicated that active drinkers had higher levels of alexithymia than abstinent patients (Mann-Whitney U = .012, p = .016). The mean TAS-20 score was 54.27 (SD = 13.56) for active drinkers, compared to 48.01 (SD = 14.20) for abstinent patients.
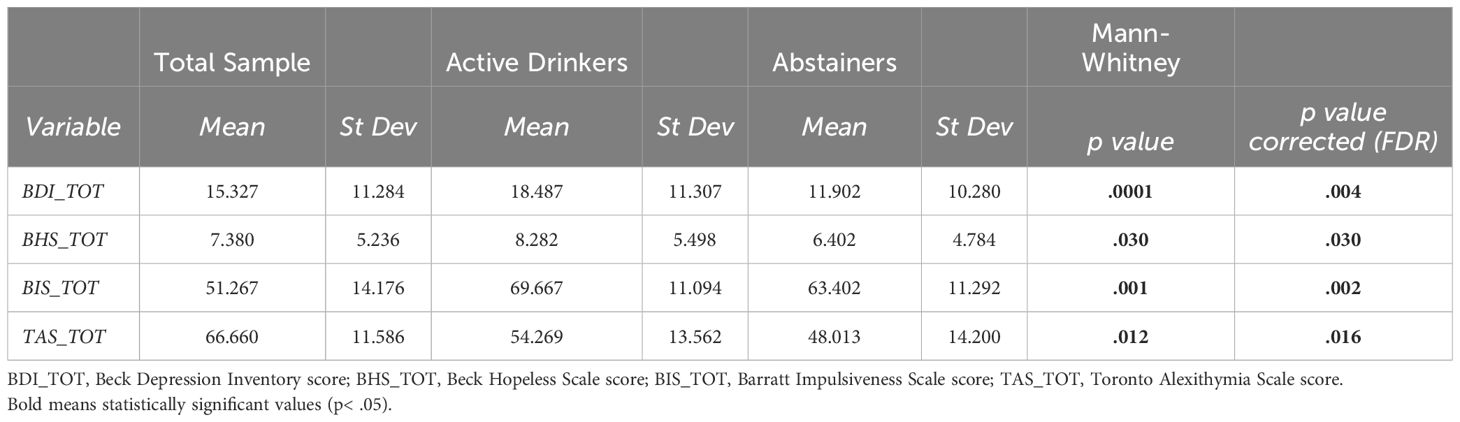
Table 2 Psychological dimensions scores in abstinent vs active drinkers.
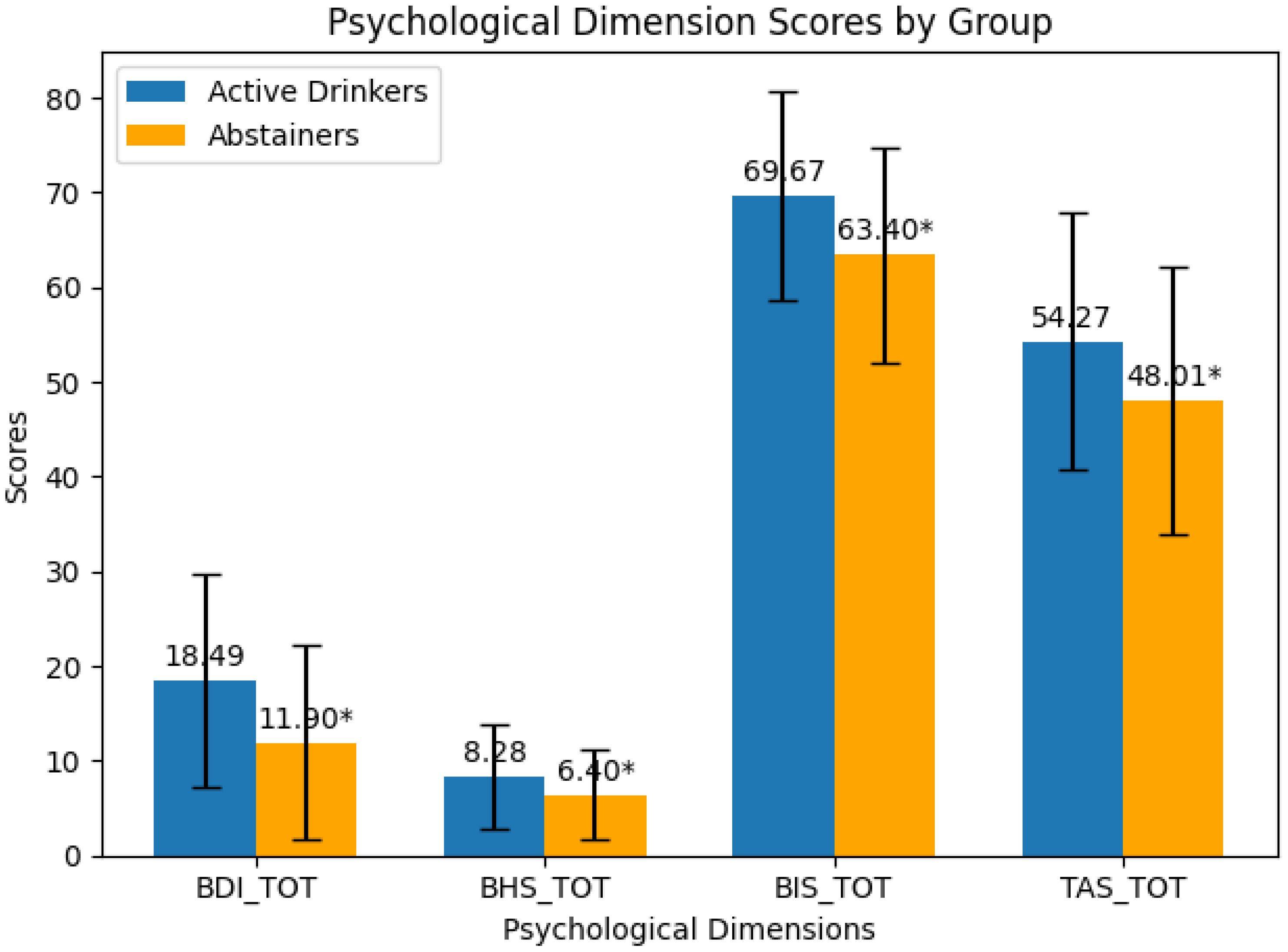
Figure 1 Graphical score of psychological dimensions.
Rating results showing significant and non-significant comparisons in abstinent vs active drinkers. Asterisks represent significant comparisons (p<.05). BDI= Beck Depression Inventory - BHS= Beck Hopelessness Scale - BIS-11= Barratt Impulsiveness Scale - TAS20= Toronto Alexithymia Scale.
The results of the present study revealed significant differences in the scores of depression, hopelessness, impulsivity, and alexithymia among AUD patients, categorized as either active drinker or abstinent. These findings are in line with previous studies and offer important insights into understanding the complexities of AUD and its implications for physical and mental health. It emerged that participants who continued to drink showed significantly higher levels of depression compared to their abstinent counterparts. This finding aligns with previous studies establishing a close association between alcohol consumption and depression (8). Excessive alcohol use may act as a coping mechanism for dealing with depressive symptoms; however, depression itself may also increase the risk of AUD, creating a vicious cycle that warrants particular attention in clinical practice. During withdrawal from alcohol, there is a focus on reduced experiences of reward and increases in negative affect, which can then contribute to the restart of alcohol consumption. These psychological experiences are coupled with changes in the striatum, extended amygdala, and insula functioning. These brain structures are critical nodes involved in the salience network (SN) (63). SN is highly relevant to the development and maintenance of AUD by influencing negative affect (64), incentive salience (65), and executive function (66) networks. Reduction in alcohol consumption is associated with a decrease in the prevalence of positive screening for depression (15) and mood-related symptoms tend to dissipate within the first weeks for the majority of patients (11). The results also indicated that active-drinker participants reported higher impulsivity scores compared to abstinent patients. Impulsivity has been extensively studied in the context of AUD and has proven to be a significant risk factor for its development and maintenance (35–38). Impulsivity can influence the ability to resist the temptation to drink and may also contribute to a lack of awareness of the risks associated with AUD (39). Subsequentially, active-drinker reported higher levels of alexithymia compared to abstinent patients. Alexithymia, the difficulty in identifying and expressing emotions, has been associated with increased vulnerability to the negative effects of substance misuse (52, 53) and previous studies found that alexithymic individuals appear to consume greater quantities of alcohol than non-alexithymic individuals (51).Alcohol’s numbing effect on emotions can hinder individuals’ ability to identify and express their feelings, leading to interpersonal difficulties and psychological distress. Additionally, the presence of alexithymia may further complicate the treatment of AUD as a lack of emotional awareness can impede effective participation in therapy and recovery programs. Finally, the higher levels of hopelessness reported by active-drinkersraise significant concerns about the mental health and well-being of those struggling with AUD. The association between AUD and suicide has been well-documented and demands immediate attention from mental health professionals to enact effective prevention strategies and targeted interventions (24, 26, 27, 67). The correlation between alcohol use and suicidal ideation highlights the life-threatening consequences of AUD. Alcohol’s depressant effects can exacerbate feelings of hopelessness and despair, increasing the likelihood of suicidal thoughts and behaviors. As these dimensions are known risk factors in predicting alcohol relapse in a time-varying manner (42), our results emphasize the importance of recognizing and treating the different degrees of severity of these dimensions from a personalized care perspective.
The investigation of psychopathological dimensions, may be useful to identify different phenotypes of AUD patients. The baseline assessment of specific features, that is, impulsivity, hopelessness depression and alexithymia, among others, could identify patients more at risk for relapse and support clinicians to adjust therapeutic program during crucial moments of treatment and follow up. This implies that, maintaining low levels of impulsivity, alexithymia, depression and hopelessness are of primordial importance for relapse prevention. This can be done through the choice of the right integrated therapy with regard to the specific patient. The choice of appropriate therapy can also benefit from the use of digital assessment methods. Among the various tools available to the clinician to monitor a patient’s daily life and response mechanisms to stressors, we can mention the ecological momentary assessment (EMA). EMA describes a type of data collection that allows clinicians and researchers to gather detailed insight into the daily lives of patients by inquiring about the subjects’ mental state in the moment, avoiding memory recall bias. EMA techniques provide methods by which a patient can report on symptoms, affect, behavior and cognitions close in time to experience, and these reports are obtained many times over the course of a day (68).
Psychological treatment of AUD is of considerable importance to improve patients’ quality of life, avoiding clinical treatments that lead to discontinuation. Approaches based on motivational interviewing and cognitive behavioral therapy (CBT) are the most effective and appropriate psychological treatments for AUD (69). At the same time, it has been shown that the 12 Steps program (70)appears to be very effective and produces economic benefits (71), (72), (73)Mindfulness-Based Therapies have also shown promise in treating AUD by helping patients increase their awareness and acceptance of cravings without acting on them, thus reducing relapse rates. Furthermore, Interpersonal Therapy (IPT) focuses on improving interpersonal functioning and has been found to be beneficial in treating AUD by addressing the social and relational issues that often accompany the disorder (74, 75). On the other side, pharmacological treatments for AUD may include different approaches to address various stages and symptoms of this condition. Disulfiram is used for alcohol aversion, it induces unpleasant reactions when drinking alcohol, such as nausea, vomiting and headaches. This helps to dissuade the patient from drinking. Methadoxine works by reducing alcohol levels in the blood and facilitating its elimination in the urine. Acamprosate leads to a reduction of glutamatergic excitability during alcohol withdrawal reducing the risk of alcohol consumption and to increase the total duration of abstinence (76). Naltrexone blocks the euphoric effects associated with alcohol (77). Benzodiazepines can be used to manage withdrawal and reduce anxiety. The different mechanisms of action and effects of these drug therapies, in conjunction with brief weekly adherence counseling, rehabilitation or psychotherapy, can only give their best when paired with the specific psychopathological constructs of the patient (78). This means that to target alcohol abstention, instead of only turning the patient away from the substance use, we will need to better understand his or her specific dimensions and treat that in the first place.
Some limitations must be acknowledged like the cross-sectional design of our study, which involves observing participants at a single point in time. This approach limits our ability to establish cause-and-effect relationships between the variables examined. Longitudinal studies may be necessary to evaluate dynamics over time. Also, it should be noted that the sample size, although appreciable is limited to 150 subjects. This restriction could affect the generalizability of the findings to a broader population. Further studies with larger samplings are needed to confirm and generalize our findings.
Moreover, we did not consider the presence of other comorbidities such as ADHD and personality disorders, which could influence the results of our study. The exclusion of these variables may limit the comprehensiveness of the analysis.
Finally, the use of self-administered questionnaires can be subject to self-report bias and variability in participants’ understanding and interpretation of the questions, thus affecting the accuracy of the data collected.
Conversely, the study has the following strengths: the real-world outpatient setting, the naturalistic design and the comprehensive assessment of the four psychopathological constructs.
In conclusion, the results of this research confirm the importance of understanding the multifaceted nature of the AUD. One of the key implications of this research is the critical role played by specific psychopathological dimensions in alcohol abstinence. By abstaining from alcohol or moderating its use, individuals can mitigate the risk of developing or worsen the course of various mental health conditions, promoting a positive circle. The relationship between alcohol abstinence and mental health is reciprocal: prioritizing mental well-being can support efforts toward alcohol abstinence, while abstaining from alcohol can contribute to improved mental health outcomes.
Future studies, should use a longitudinal approach and with the help of digital assessment methods, identify the different stages of AUD in relation to the different psychopathological constructs and consequently the different specific lines of treatment.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving humans were approved by Comitato Etico per la Ricerca di Ateneo (CERA). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
AZ: Writing – review & editing, Writing – original draft, Data curation. IB: Writing – review & editing, Writing – original draft, Investigation. AB: Writing – review & editing, Writing – original draft, Conceptualization. MO: Writing – review & editing, Writing – original draft, Data curation. AE: Writing – review & editing, Methodology. RG: Writing – review & editing, Visualization. BD: Writing – review & editing, Software. MA: Writing – review & editing, Supervision. GS: Writing – review & editing, Supervision.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This workshop was supported by 5x1000 San Martino Hospital (Genoa).
This workshop was supported by #NEXTGENERATIONEU (NGEU) and funded by the Italian Ministry of University and Research (MUR), National Recovery and Resilience Plan (NRPP), project MNESYS (PE0000006) - A Multiscale integrated approach to the study of the nervous system in health and disease (DN. 1553 11.10.2022).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
The handling editor AS declared a shared parent affiliation with the authors AB, AE, and GS at the time of review.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Scafato E, Ghirini S, Gandin C, Matone A, Vichi M, gruppo di lavoro Centro Servizi Documentazione Alcol (CSDA), il. Epidemiologia e monitoraggio alcol-correlato in Italia e nelle Regioni. Istituto Superiore di Sanità (2023). Available at: https://www.iss.it/-/rapporto-istisan-23/3-epidemiologia-e-monitoraggio-alcol-correlato-in-italia-e-nelle-regioni.-valutazione-dell-osservatorio-nazionale-alcol-sull-impatto-del-consumo-di-alcol-ai-fini-dell-implementazione-delle-attivit%C3%A0-del-piano-nazionale-alcol-e-salu.
2. Skarstein S, Lien L, Abebe DS. The burden of somatic diseases among people with alcohol- and drug use disorders are influenced by mental illness and low socioeconomic status. A registry-based cohort study in Norway. J Psychosomatic Res. (2023) 165. doi: 10.1016/J.JPSYCHORES.2022.111137
4. Association AP. DSM-5. Manuale diagnostico e statistico dei disturbi mentali. 5th ed. Cortina Raffaello (2014).
5. Kendler KS, Ohlsson H, Karriker-Jaffe KJ, Sundquist J, Sundquist K. Social and economic consequences of alcohol use disorder: a longitudinal cohort and co-relative analysis. psychol Med. (2017) 47:925–35. doi: 10.1017/S0033291716003032
6. Castillo-Carniglia A, Keyes KM, Hasin DS, Cerdá M. Psychiatric comorbidities in alcohol use disorder. Lancet Psychiatry. (2019) 6:1068–80. doi: 10.1016/S2215–0366(19)30222–6
7. Sliedrecht W, De Waart R, Witkiewitz K, Roozen HG. Alcohol use disorder relapse factors: A systematic review. Psychiatry Research-Neuroimaging. (2019) 278:97–115. doi: 10.1016/j.psychres.2019.05.038
8. Boden JM, Fergusson DM. Alcohol and depression. Addiction. (2011) 106:906–14. doi: 10.1111/j.1360-0443.2010.03351.x
10. Schuckit MA. The clinical implications of primary diagnostic groups among alcoholics. Arch Gen Psychiatry. (1985) 42:1043. doi: 10.1001/archpsyc.1985.01790340021003
11. Brown SA, Schuckit MA. Changes in depression among abstinent alcoholics. J Stud Alcohol. (1988) 49:412–7. doi: 10.15288/jsa.1988.49.412
12. Brown SS, Inaba RK, Gillin JC, Schuckit MA, Stewart MG, Irwin MR. Alcoholism and affective disorder: clinical course of depressive symptoms. Am J Psychiatry. (1995) 152:45–52. doi: 10.1176/ajp.152.1.45
13. Kiefer F, Barocka A. SECONDARY DEPRESSION IN WEANED ALCOHOLICS: IMPLICATIONS OF LESCH’S TYPOLOGY OF CHRONIC ALCOHOLISM. Alcohol Alcoholism. (1999) 34:916–7. doi: 10.1093/alcalc/34.6.916
14. Baker AL, Kay-Lambkin F, Gilligan C, Kavanagh DJ, Baker F, Lewin TJ. When does change begin following screening and brief intervention among depressed problem drinkers? J Subst Abuse Treat. (2013) 44:264–70. doi: 10.1016/j.jsat.2012.07.009
15. Hallgren KA, Jack HE, Oliver MM, Berger DB, Bobb JF, Kivlahan DR, et al. Changes in alcohol consumption reported on routine healthcare screenings are associated with changes in depression symptoms. Alcoholism: Clin Exp Res. (2023). doi: 10.1111/acer.15075
16. Lejoyeux M, Lehert P. Alcohol-use disorders and depression: results from individual patient data meta-analysis of the acamprosate-controlled studies. Alcohol Alcoholism. (2010) 46:61–7. doi: 10.1093/alcalc/agq077
17. Pettinati HM, O’Brien C, Dundon WG. Current status of Co-Occurring Mood and Substance Use Disorders: a new therapeutic target. Am J Psychiatry. (2013) 170:23–30. doi: 10.1176/appi.ajp.2012.12010112
18. Hasin DS, Grant BF. Major depression in 6050 former drinkers. Arch Gen Psychiatry. (2002) 59:794. doi: 10.1001/archpsyc.59.9.794
19. Glenn SA, Parsons OA. Prediction of resumption of drinking in posttreatment alcoholics. Int J Addict. (1991) 26:237–54. doi: 10.3109/10826089109053186
20. Greenfield SF, Weiss RD, Muenz LR, Vagge LM, Kelly JM, Bello LR, et al. The effect of depression on return to drinking. Arch Gen Psychiatry. (1998) 55:259. doi: 10.1001/archpsyc.55.3.259
21. Curran GM, Kirchner JE, Worley M, Rookey C, Booth BM. Depressive symptomatology and early attrition from intensive outpatient substance use treatment. J Behav Health Serv Res. (2002) 29:138–43. doi: 10.1007/bf02287700
22. Murphy GE. The lifetime risk of suicide in alcoholism. Arch Gen Psychiatry. (1990) 47:383. doi: 10.1001/archpsyc.1990.01810160083012
23. Conner KR, Duberstein PR. Predisposing and Precipitating Factors for suicide among Alcoholics: Empirical review and Conceptual integration. Alcoholism: Clin Exp Res. (2004) 28:6S–17S. doi: 10.1097/01.ALC.0000127410.84505.2A
24. Bernal M, Haro JM, Bernert S, Brugha T, De Graaf R, Bruffaerts R, et al. Risk factors for suicidality in Europe: Results from the ESEMED study. J Affect Disord. (2007) 101:27–34. doi: 10.1016/j.jad.2006.09.018
25. Flensborg-Madsen T, Knop J, Mortensen EL, Becker U, Sher L, Grønbæk M. Alcohol use disorders increase the risk of completed suicide — Irrespective of other psychiatric disorders. A longitudinal cohort study. Psychiatry Research-Neuroimaging. (2009) 167:123–30. doi: 10.1016/j.psychres.2008.01.008
26. Amiri S, Behnezhad S. Alcohol use and risk of suicide: a systematic review and Meta-analysis. J Addictive Dis. (2020) 38:200–13. doi: 10.1080/10550887.2020.1736757
27. Crossin R, Cleland L, McLeod GFH, Beautrais AL, Witt K, Boden JM. The association between alcohol use disorder and suicidal ideation in a New Zealand birth cohort. Aust New Z J Psychiatry. (2021) 56:1576–86. doi: 10.1177/00048674211064183
28. Pavarin RM, Fabbri C, Turino E, Marani S, Sanchini S, De Ronchi D. Epidemiology and Clinical-Demographic Characteristics of suicide attempts in alcohol use disorders in an Italian population. J Psychoactive Drugs. (2022) 55:1–8. doi: 10.1080/02791072.2022.2107464
29. Weishaar ME, Beck AT. Hopelessness and suicide. Int Rev Psychiatry. (1992) 4:177–84. doi: 10.3109/09540269209066315
30. Glanz LM, Haas GL, Sweeney JA. Assessment of hopelessness in suicidal patients. Clin Psychol Rev. (1995) 15:49–64. doi: 10.1016/0272–7358(94)00040–9
31. Beck AT, Steer RA, Brown GK. BDI-II, Beck Depression Inventory. APA (1996). doi: 10.1037/t00742-000
32. Beck AT, Weissman A, Kovacs M. Alcoholism, hopelessness and suicidal behavior. J Stud Alcohol. (1976) 37:66–77. doi: 10.15288/jsa.1976.37.66
33. Baines L, Jones A, Christiansen P. Hopelessness and alcohol use: The mediating role of drinking motives and outcome expectancies. Addictive Behav Rep. (2016) 4:65–9. doi: 10.1016/J.ABREP.2016.11.001
34. Beck AT, Steer RA, McElroy MG. Relationships of hopelessness, depression and previous suicide attempts to suicidal ideation in alcoholics. J Stud Alcohol. (1982) 43:1042–6. doi: 10.15288/jsa.1982.43.1042
35. Fox H, Bergquist K, Gu P, Sinha R. Interactive Effects of cumulative stress and impulsivity on alcohol consumption. Alcoholism: Clin Exp Res. (2010). doi: 10.1111/j.1530–0277.2010.01221.x
36. Hamilton KR, Ansell EB, Reynolds B, Potenza MN, Sinha R. Self-reported impulsivity, but not behavioral choice or response impulsivity, partially mediates the effect of stress on drinking behavior. Stress. (2012) 16:3–15. doi: 10.3109/10253890.2012.671397
37. Charfi N, Smaoui N, Turki M, Bouali MM, Omri S, Thabet J, et al. Enquête sur la consommation d’alcool et sa relation avec la recherche de sensations et l’impulsivité chez l’adolescent de la région de Sfax, Tunisie. Rev D Epidemiologie Et Sante Publique. (2019) 67:13–20. doi: 10.1016/j.respe.2018.10.007
38. Liu Z, Luo R, Fu R, Yuan C, Xu X, Zhou D, et al. The influences of impulsivity and education levels on severity of alcohol dependence. Front Psychiatry. (2020) 11:737. doi: 10.3389/fpsyt.2020.00737
39. Westman JG, Bujarski S, Ray LA. Impulsivity moderates subjective responses to alcohol in Alcohol-Dependent individuals. Alcohol Alcoholism. (2016). doi: 10.1093/alcalc/agw096
40. Khemiri L, Kaag AM, Joos L, Dom G, Franck J, Goudriaan AE, et al. Family history of alcohol abuse associated with higher impulsivity in patients with alcohol use disorder: A multisite study. Eur Addict Res. (2020) 26:85–95. doi: 10.1159/000505621
41. Reyes-Huerta HE, Dos Santos C, Martínez KIM. Impulsive mechanisms influencing relapse in alcohol drinking. Med Hypotheses. (2018) 112:27–9. doi: 10.1016/j.mehy.2018.01.007
42. Pepe M, Di Nicola M, Panaccione I, Franza R, De Berardis D, Cibin M, et al. Impulsivity and alexithymia predict early versus subsequent relapse in patients with alcohol use disorder: A 1-year longitudinal study. Drug Alcohol Rev. (2022) 42:367–72. doi: 10.1111/dar.13568
43. Reichl D, Enewoldsen N, Weisel KK, Fuhrmann L, Lang C, Saur S, et al. Association of impulsivity with quality of life and well-being after alcohol withdrawal treatment. J Clin Psychol. (2022). doi: 10.1002/jclp.23316
44. Sliedrecht W, Roozen HG, Witkiewitz K, De Waart R, Dom G. The Association Between Impulsivity and Relapse in Patients with Alcohol Use Disorder: A literature review. Alcohol Alcoholism. (2020) 56:637–50. doi: 10.1093/alcalc/agaa132
45. Velotti P, Garofalo C, Petrocchi C, Cavallo F, Popolo R, Dimaggio G. Alexithymia, emotion dysregulation, impulsivity and aggression: A multiple mediation model. Psychiatry Res. (2016) 237:296–303. doi: 10.1016/J.PSYCHRES.2016.01.025
46. Cruise KE, Becerra R. Alexithymia and problematic alcohol use: A critical update. Addictive Behav. (2018) 77:232–46. doi: 10.1016/J.ADDBEH.2017.09.025
47. Thorberg FA, Young RMD, Hasking P, Lyvers M, Connor JP, London ED, et al. Alexithymia and alcohol dependence: the roles of negative mood and alcohol craving. Subst Use Misuse. (2019) 54:2380–6. doi: 10.1080/10826084.2019.1650773
48. Lyvers M, Thorberg FA. Alexithymia and alcohol use: evaluating the role of interoceptive sensibility with the revised multidimensional assessment of interoceptive awareness. J Psychopathol Behav Assess. (2023), 1–13. doi: 10.1007/s10862-023-10034-y
49. Loas G, Fremaux D, Otmani O, Lecercle C, Delahousse J. Is alexithymia a negative factor for maintaining abstinence? A follow-up study. Compr Psychiatry. (1997) 38:296–9. doi: 10.1016/s0010–440x(97)90063–8
50. Thorberg FA, Young RM, Sullivan KA, Lyvers M. Alexithymia and alcohol use disorders: A critical review. Addictive Behav. (2009) 34:237–45. doi: 10.1016/j.addbeh.2008.10.016
51. Bruce G, Curren C, Williams L. Alexithymia and alcohol consumption: The mediating effects of drinking motives. Addictive Behav. (2012) 37:350–2. doi: 10.1016/j.addbeh.2011.11.024
52. Haan H, Joosten EAG, Wijdeveld TAGM, Boswinkel P, van der Palen J, De Jong C. Alexithymia is not a stable personality trait in patients with substance use disorders. Psychiatry Research-Neuroimaging. (2012) 198:123–9. doi: 10.1016/j.psychres.2011.09.027
53. De Haan HA, van der Palen J, Wijdeveld TGM, Buitelaar JK, De Jong CAJ. Alexithymia in patients with substance use disorders: State or trait? Psychiatry Research-Neuroimaging. (2014) 216:137–45. doi: 10.1016/j.psychres.2013.12.047
54. Pombo S, Da Costa NF, Ismail F, Cardoso JMN, Figueira ML. Alexithymia and alcohol dependence: Do different subtypes manifest different emotion regulations? Addict Res Theory. (2014) 23:187–95. doi: 10.3109/16066359.2014.949697
55. Thorberg FA, Young RM, Sullivan KA, Lyvers M, Connor JP, Feeney GFX. Alexithymia, craving and attachment in a heavy drinking population. Addictive Behav. (2011) 36:427–30. doi: 10.1016/j.addbeh.2010.12.016
56. Ziółkowski M, Gruss T, Rybakowski J. Does alexithymia in male alcoholics constitute a negative factor for maintaining abstinence? Psychother Psychosomatics. (1995) 63:169–73. doi: 10.1159/000288955
57. American Psychiatric Association. Diagnostic and statistical manual of mental disorders. Am Psychiatr Assoc. (2013). doi: 10.1176/appi.books.9780890425596
58. EpiCentro. Sample Size Calculator. . Available online at: https://www.epicentro.iss.it/strumenti/SampleSize.
59. Beck AT, Weissman A, Trexler DL. The measurement of pessimism: The Hopelessness Scale. J Consulting Clin Psychol. (1974) 42:861–5. doi: 10.1037/h0037562
60. Reise SP, Moore TM, Sabb FW, Brown AK, London ED. The Barratt Impulsiveness Scale-11: reassessment of its structure in a community sample. psychol Assess. (2013) 25:631–42. doi: 10.1037/A0032161
61. Bagby M, Taylor GJ, Ryan D. Toronto Alexithymia Scale: Relationship with personality and psychopathology measures. Psychother Psychosomatics. (1986) 45:207–15. doi: 10.1159/000287950
62. IBM Corp Released 2021. IBM SPSS Statistics for Windows, Version 28.0 Armonk, NY; IBM Corp (2023). Available at: https://www.ibm.com/it-it/spss.
63. Padula CB, Tenekedjieva LT, McCalley DM, Al-Dasouqi H, Hanlon CA, Williams LM, et al. Targeting the salience network: A mini-review on a novel neuromodulation approach for treating alcohol use disorder. Front Psychiatry. (2022) 13:893833/BIBTEX. doi: 10.3389/fpsyt.2022.893833
64. Yang H, Devous MD, Briggs RW, Spence JS, Xiao H, Kreyling N, et al. Altered neural processing of threat in alcohol-dependent men. Alcoholism Clin Exp Res. (2013) 37:2029–38. doi: 10.1111/ACER.12187
65. Schacht JP, Anton RF, Myrick H. Functional neuroimaging studies of alcohol cue reactivity: a quantitative meta-analysis and systematic review. Addict Biol. (2013) 18:121–33. doi: 10.1111/j.1369-1600.2012.00464.x
66. Morris LS, Kundu P, Baek K, Irvine MA, Mechelmans DJ, Wood J, et al. Jumping the gun: mapping neural correlates of waiting impulsivity and relevance across alcohol misuse. Biol Psychiatry. (2016) 79:499–507. doi: 10.1016/J.BIOPSYCH.2015.06.009
67. Darvishi N, Farhadi M, Haghtalab T, Poorolajal J. Alcohol-related risk of suicidal ideation, suicide attempt, and completed suicide: A meta-analysis. PloS One. (2015) 10:e0126870. doi: 10.1371/journal.pone.0126870
68. Guglielmo R, Escelsior A, Amore M, Serafini G. Mood instability as prodrome of bipolar disorder. J Psychopathol. (2024) 30:31–7. doi: 10.36148/2284–0249-N456
69. Coriale G, Fiorentino D, De Rosa F, Solombrino S, Scalese B, Ciccarelli R, et al. Treatment of alcohol use disorder from a psychological point of view. Rivista Di Psichiatria. (2018) 53:141–8. doi: 10.1708/2925.29416
70. Breuninger MM, Grosso JA, Hunter W, Dolan SL. Treatment of alcohol use disorder: Integration of Alcoholics Anonymous and cognitive behavioral therapy. Training Educ Prof Psychol. (2020) 14:19–26. doi: 10.1037/TEP0000265
71. Kelly JF, Abry A, Ferri M, Humphreys K. Alcoholics anonymous and 12-step facilitation treatments for alcohol use disorder: A distillation of a 2020 cochrane review for clinicians and policy makers. Alcohol Alcoholism. (2020) 55:641–51. doi: 10.1093/ALCALC/AGAA050
72. Riper H, Andersson G, Hunter SB, de Wit J, Berking M, Cuijpers P. Treatment of comorbid alcohol use disorders and depression with cognitive-behavioural therapy and motivational interviewing: a meta-analysis. Addiction. (2014) 109:394–406. doi: 10.1111/ADD.12441
73. Naqvi NH, Srivastava AB, Sanchez-Peña J, Lee JK, Drysdale AT, Mariani JJ, et al. Neural correlates of drinking reduction during a clinical trial of cognitive behavioral therapy for alcohol use disorder. Alcohol: Clin Exp Res. (2024) 48:260–72. doi: 10.1111/ACER.15259
74. Yalom ID. GROUP THERAPY AND ALCOHOLISM. Ann New York Acad Sci. (1974) 233:85–103. doi: 10.1111/j.1749-6632.1974.tb40286.x
75. Fernandez AC, Wood MD, Stein LAR, Rossi JS. Measuring mindfulness and examining its relationship with alcohol use and negative consequences. Psychol Addictive Behav. (2010) 24:608–16. doi: 10.1037/A0021742
76. Guglielmo R, Ioime L, Solaroli S, Janiri L. Pharmacological treatments in alcohol use disorders: state of art and new perspectives. La Clinica Terapeutica. (2015) 166:262–70. doi: 10.7417/CT.2015.1899
77. Guglielmo R, Kobylinska L, de Filippis R. Topiramate, naltrexone, and acamprosate in the treatment of alcohol use disorders. NeuroPsychopharmacotherapy. (2021), 1–16. doi: 10.1007/978–3-319–56015-1_430–1
Keywords: alcohol use disorder, suicide risk, abstinence, impulsivity, alexithymia
Citation: Zizzi A, Berri IM, Berri A, Occhipinti M, Escelsior A, Guglielmo R, Pereira Da Silva B, Amore M and Serafini G (2024) Psychological dimensions in alcohol use disorder: comparing active drinkers and abstinent patients. Front. Psychiatry 15:1420508. doi: 10.3389/fpsyt.2024.1420508
Received: 20 April 2024; Accepted: 03 June 2024;
Published: 27 June 2024.
Edited by:
Alessio Simonetti, Fondazione Policlinico Universitario “Agostino Gemelli” IRCCS, ItalyReviewed by:
Silvia Montanari, Catholic University of the Sacred Heart, ItalyCopyright © 2024 Zizzi, Berri, Berri, Occhipinti, Escelsior, Guglielmo, Pereira Da Silva, Amore and Serafini. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Alessio Zizzi, ei5hbGVzc2lvOThAZ21haWwuY29t
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.