
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychiatry , 13 November 2024
Sec. Addictive Disorders
Volume 15 - 2024 | https://doi.org/10.3389/fpsyt.2024.1418339
 Maria Ciccarelli1*
Maria Ciccarelli1* Barbara Pizzini2
Barbara Pizzini2 Marina Cosenza1
Marina Cosenza1 Francesca D’Olimpio1
Francesca D’Olimpio1 Mark D. Griffiths3
Mark D. Griffiths3 Giovanna Nigro1
Giovanna Nigro1Background: Despite the increasing proportion of older-aged individuals suffering from problematic gambling, research on gambling among this specific age cohort is still in its infancy. Chasing is a pathognomonic feature of disordered gambling and is considered one of the key risk factors in the transition from recreational to disordered gambling. Despite the increased research on chasing over the past decade, no previous study has ever examined the psychological determinants of chasing behavior among old-aged gamblers. Given the importance of chasing in facilitating and maintaining problem gambling, and the paucity of research examining gambling among older individuals, the present study is the first to empirically investigate the joint role of chasing behavior, negative affectivity, and mentalizing among older-aged gamblers.
Methods: The sample comprised 116 older-aged gamblers who were administered the South Oaks Gambling Screen (SOGS), the Depression Anxiety Stress Scale (DASS-21) and the Reflective Functioning Questionnaire (RFQ-8) to assess gambling severity, psychological distress, and mentalizing, respectively. Participants also performed the ChasIT, a computerized task that assesses chasing behavior, in which participants were randomly assigned to three different experimental conditions: loss, control, and win.
Results: No effect of the experimental conditions of ChasIT on chasing behavior was observed. Regression analyses indicated that heightened levels of gambling severity and lower levels of certainty about mental states (i.e., hypermentalizing) predicted both the decision to chase and chasing frequency. Along with problem gambling and hypermentalizing, chasing frequency was also predicted by high levels of depression.
Conclusions: The present study demonstrated the association between disordered gambling, depression, and hypermentalizing in chasing behavior among older-aged gamblers. The findings make an important contribution to providing insight regarding variables that are associated with chasing among older-aged gamblers, one of the least represented populations of gamblers in the literature. The results suggest that specific training on mentalizing abilities could help gamblers to reflect on their own behaviors in terms of mental states, rather than following the impulse to gamble in order to ameliorate poor mood.
Epidemiological studies have shown that between 0.1% and 5.8% of the adult general population worldwide suffer from problematic gambling (1). Among these, an increasing proportion are older aged individuals (2). In fact, gambling participation rates among the elderly have risen, to the point that older-aged people have been identified as an at-risk group of developing gambling-related problems (2), due to several interacting risk factors that can contribute to causing gambling problems among this age cohort. From an environmental perspective, a lack of familiar and/or social support (3), stressful life events (e.g., widowhood and retirement) (4), and poor social adjustment (5) can have a significant impact on gambling participation. From a psychological perspective, high levels of impulsivity, deficits in coping strategies and problem-solving, and negative affectivity (e.g., worry, anxiety, and stress) could lead to problematic gambling, as a way to soothe emotional suffering (6). Moreover, neurobiological modifications, mainly involving the frontal areas of the brain, may result in deficits in executive functions, leading to impairments in inhibition response, planning, and decision-making (7; see also 8, 9).
Among the most characterizing features of disordered gambling is chasing behavior. It consists of the drive to invest increasing amounts of money in gambling after losses in an attempt to recoup the money that was previously lost. In other words, instead of serving as a deterrent, gambling losses represent an incentive for continued gambling, and has been recognized as a behavior that facilitates problematic gambling involvement (10, 11). For some scholars, chasing has been conceptualized as a behavioral equivalent to substance seeking (12) and represents a pathognomonic feature of disordered gambling which occurs among approximately 80% of individuals with a problematic gambling involvement (13) and is a key risk factor in the transition from recreational to disordered gambling (14–17). Chasing losses represents a directly observable and measurable diagnostic criterion of gambling disorder, and is an idiosyncratic characteristic in the field of addictions, that differentiates gambling disorder from substance use disorders (18, 19).
Criterion 6 for gambling disorder in the DSM-5 (14, 20) refers to chasing (“After losing money gambling, often returns another day to get even [“chasing” one’s losses]”). This refers exclusively to chasing losses, and to between-session chasing, namely to return another day to recoup gambling losses. However, recent studies have broadened this construct, showing how chasing concerns not only losses but also wins, with the hope of earning more (21–23), and that chasing behavior is realized not only by returning another day to gambling but also occurring in the same gambling session while it is still ongoing, i.e., within-session chasing (24; see 25 for a review). Chasing plays a prominent role in several theoretical models, such as the pathways model (26), according to which, chasing of both wins and losses, is recognized as a consequence of classical and operant conditioning, as well as a factor that, across the different pathways, leads to gambling disorder. In other words, engaging in chasing can triple the risk of developing disordered gambling (27).
The importance of chasing in maintaining gambling involvement is evidenced by the number of studies over the past decade that have focused upon the investigation of the endophenotypes, both gambling- and personality-related, that contribute to chasing behavior. The majority of research studies that have empirically investigated chasing behavior have highlighted the role of different personality features mostly related to impulsivity (e.g., 24), including sensation seeking (28), disinhibition (29), and a present-oriented time perspective (30, 31).
As well as impulsiveness, gamblers exposing themselves to the risk of further losses by persisting in gambling, may be related to negative emotions. In support of this, O’Connor and Dickerson (32) conducted an interview-study involving 18 regular gamblers to investigate the factors influencing the decisions to chase within-session. They reported that chasing allowed gamblers to modulate the frustration and anger after gambling losses and to experience feelings of relief and excitement. In another study, gamblers with high levels of depression reported a significantly greater number of games played and longer duration of gambling (33). Devos et al. (34) observed an increased persistence in gambling on a simulated slot machine task after experimentally inducing sadness in a group of recreational gamblers. Although the association between negative emotions and gambling is well established, the relationship between negative emotions and chasing has not been widely explored, especially among older-aged gamblers, considering that the aforementioned studies only recruited early- or early-middle aged adults (e.g., 32–34).
Mentalizing is an ability that develops within early attachment relationships that “can protect individuals from stress-affected emotional arousal” (35, p.5), allowing an adaptive regulation of emotions (e.g., 36–38), and preventing the impulsive acting out of negative emotions with the consequent risk of engaging in problematic behaviors. Mentalizing is a concept derived from different disciplines from psychoanalysis to social cognition (38) and comprises the imaginative ability of individuals to perceive and interpret their own and others’ behaviors in terms of mental states, such as thoughts, beliefs, wishes, and desires (39–41). Mentalizing is a fundamental developmental achievement by which behavior becomes meaningful and predictable, with both interpersonal and intrapsychic implications (38, 42). On an interpersonal level, mentalizing facilitates social relationships, while on an intrapsychic level, it is associated with the development of second-order representations that allow the modification of mental states (41, 43). Consequently, mentalizing represents an important skill not only in increasing awareness of the mental states but also in constituting a fundamental requirement for the modification of the mental states themselves (40, 41). Several studies have demonstrated an association between gambling and mentalizing deficits (e.g., 44, 45) that, according to Fonagy and Bateman (46), can decline in two different forms: hypomentalization and hypermentalization. Hypomentalization consists of a difficulty in interpreting human behaviors in terms of internal mental states, while hypermentalization consists of excessive and inaccurate mentalizing. It has been demonstrated that both the deficit dimensions of mentalization are involved in gambling (47–49). These mentalizing impairments could be responsible for the confidence that gamblers have in their own performance in both gambling and non-gambling tasks, as well as for the tendency to manage emotional distress in a dysfunctional and impulsive way (45, 50, 51).
Although the association of gambling with mentalizing deficits has been previously documented among both adults and adolescents (e.g., 44, 47–49, 52, 53), to date, the role of mentalizing deficits in chasing behavior among older-aged gamblers is unknown. This aspect should instead be thoroughly investigated, especially in light of the results of some studies having observed a decline in mentalization abilities over time and, more specifically, from the age of 50 years onwards (e.g., 54, 55).
In the light of the aforementioned literature gaps, the present study empirically investigated chasing behavior among older-aged gamblers, in order to identify its psychological determinants. More specifically, the present study investigated the (previously) unexplored relationship between chasing, gambling severity, psychological distress, and mentalizing among older-aged gamblers. Based on previous chasing research, it was hypothesized that depression, mentalizing deficits and gambling severity would predict chasing behavior among older-aged gamblers.
The sample comprised 116 gamblers (59% males), aged between 56 and 84 years (Mage = 67.59 years; SD = 6.04). They were recruited from several Italian gambling venues, and of those approached to do so, 26% declined the invitation. Participants performed the ChasIT, a computerized task, to assess chasing behavior (56) and completed the Italian versions of the South Oaks Gambling Screen (SOGS; 57, 58) to assess problem gambling severity, the Depression Anxiety Stress Scale (DASS-21; 59, 60) to assess psychological distress, and the Reflective Functioning Questionnaire (RFQ-8; 61, 62), to assess mentalization, respectively. Half of the sample carried out the ChasIT before the paper-and-pencil psychometric scales, in order to balance any potential influence of each measure on the others. Because the ChasIT task includes three experimental conditions (control, loss, and win), each participant was randomly assigned to each condition, resulting in approximately the same number of participants being assigned to each condition (Control, N = 39; Loss, N = 40; Win, N = 38). The self-report measures were administered in counterbalanced order and, for each psychometric instrument, participants received written instructions.
The completion of both computerized task and self-report measures took place in a quiet room of the gambling venues, where each participant was individually and anonymously tested, after being informed about the general purpose of the study and having provided written informed consent. They were also assured that they could withdraw from the study whenever they wanted.
Participation in the study took approximately 25 minutes. After data collection, participants were debriefed about the real aims of the study, obtaining more detailed information about the specific hypotheses of the study. Participation in the study was voluntary and participants did not receive any reward. The present study was conducted adhering to the Helsinki Declaration and was approved by the Institutional Ethical Review Board of the first author’s university.
The SOGS is a self-report scale assessing gambling frequency and severity. The first section of the SOGS comprises non-scored items providing information about the frequency of participation in gambling, the largest amount of money gambled on any one day, and the preferred gambling activities (e.g., cards, horses, bingo, etc.). The second section comprises 20 scored dichotomous (yes/no) questions assessing the severity of gambling involvement through items that investigate the chasing behavior, the guilt related to gambling, the loss of control over gambling, etc. The scores range from 0 to 20, with higher scores reflecting more severe gambling involvement. More specifically, scores from 0 to 2 indicate no gambling problems, scores of 3 and 4 indicate problem gambling, and a score of 5 or above denotes (probable) pathological gambling. In the present study, the SOGS had very good internal consistency (α = 0.83).
The DASS-21 is a 21-item self-report measure assessing three negative psychological mood states (i.e., depression, anxiety, and stress) during the past two weeks. Items rated on a four-point Likert scale ranging from 0 (did not apply to me at all) to 3 (applied to me very much, or most of the time). The scores range from 0 to 63 for the whole scale, and 0 to 21 for the three subscales. Higher scores reflect greater psychological distress. In the present study, the full DASS-21 had excellent internal consistency (α = 0.93) and the subscales had very good internal consistency: depression (α = 0.83), anxiety (α = 0.84), and stress (α = 0.85).
The RFQ-8 is an eight-item self-report measure assessing two different dimensions of mentalization (i.e., certainty about mental states and uncertainty about mental states). Items are rated on a seven-point Likert scale, from 1 (strongly disagree) to 7 (strongly agree). Scores range from 0 to 28 on the two subscales (but there is no overall scale score). Low scores on the certainty subscale scale indicate inaccurate mentalizing (i.e., hypermentalizing) while high scores on uncertainty subscale reflect a lack of knowledge about mental states (i.e., hypomentalizing). In the present study, the certainty (α = 0.75) and uncertainty (α = 0.72) subscales both had very good internal consistency.
The ChasIT is a computerized task developed with SuperLab 4.0 experimental software that assesses chasing behavior frequency. It simulates a card game in which participants play against the house with a virtual amount of money (€10) that participants are asked to treat as real money. Each of the 60 trials consists of the presentation of the back of two cards, one from the player and one from the house. Each card reports a number ranging from 1 to 9. For each trial, if participants have the highest card they win €1, whereas if they have the lowest card they lose €1. Unbeknownst to the participants, gambling outcomes were predetermined whereby the rate of winning and losing trials depend upon the experimental conditions: in the control condition, after the first half of the task, participants keep the entire budget; in the loss condition, participants lose more than the initial budget (i.e., €12); in the win condition, participants win more than the initial budget (i.e., €12). However, in all three conditions, for each of the subsequent 30 trials, participants are allowed to continue or to stop gambling and were informed about the amount of money remaining. Participants who choose to stop gambling at the beginning of the second phase of the task are classified as “non-chasers”, whereas participants who decide to continue gambling are classified as “chasers”. Both the decision to chase and the number of trials played are measures of chasing behavior.
Data were analyzed with the IBM Statistical Package for the Social Sciences, version 20.0. The alpha significance level was set at p<.05. All variables were initially screened for missing data, distribution abnormalities, and outliers (63). Because the distributions of chasing frequency and SOGS were positively skewed, square-root transformation was performed on these variables, so that the assumptions of normality, linearity, and homoscedasticity were adequately met. Correlational analyses were performed to examine the relationships between the study variables. Chi-square tests were used to assess differences in percentages for categorical data. Analysis of variance was used to assess mean differences on continuous variables. Logistic and linear regression analyses were performed to identify the predictors of chasing behavior. To control for the presence of multicollinearity, before interpreting the regression coefficients, the variance inflation factor (VIF) was calculated. In the present study, the VIF was below the recommended cut-off of 2.5 (64), indicating no issues with multicollinearity.
Most of the sample only gambled offline (77%), whereas the 7.8% preferred online gambling, and 14.7% participated in both online and offline gambling. More than one-third of the sample reported gambling onset before the age of 18 years (38.8%), and the 70.7% before the age of 30 years, with only 5.3% having started gambling at the age of 60 years or over. The most reported gambling types (participants could report more than one type of gambling) were buying lottery tickets (95.8%), gambling on card games (46.3%), and sports betting (40.6%). The most popular places to gamble were tobacco shops (47%), home (21.9%), bars (26%), and betting centers (12.5%). Participants preferred gambling with friends (49%) or alone (21.9%). The most reported motivations for gambling (participants could report more than one motivation) were: entertainment (31.3%), money (20.8%), socializing (13.5%), and hobby (10.4%). Table 1 reports the socio-demographic variables of the overall sample.
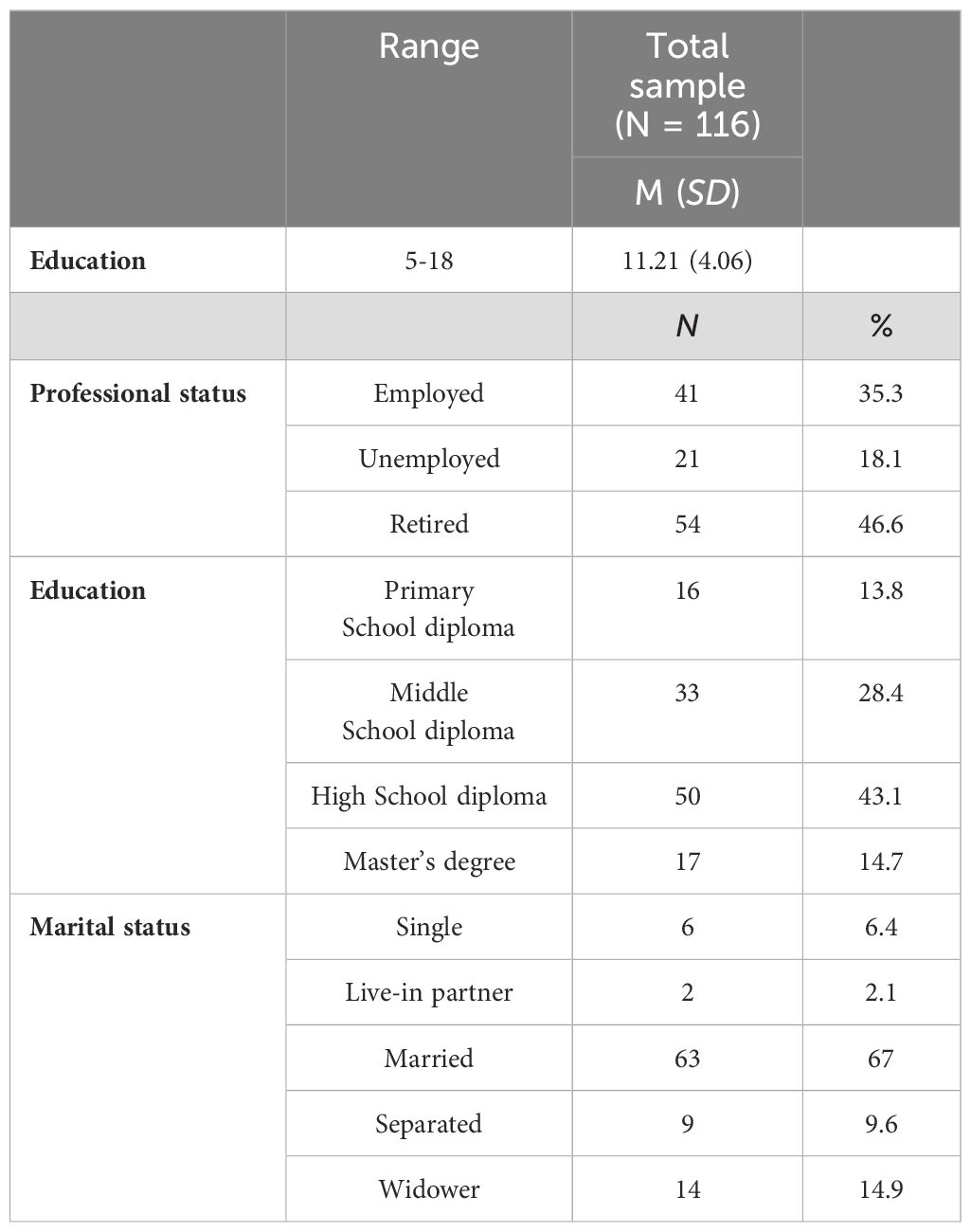
Table 1. Socio-demographic variables of the total sample.
Correlational analysis showed that both SOGS and chasing behavior (ChasIT performance) (i) positively correlated with all three DASS-21 subscales, and the uncertainty subscale of the RFQ-8, and (ii) negatively correlated with the certainty subscale of the RFQ-8. SOGS scores and chasing behavior were positively correlated each other (see Table 2).
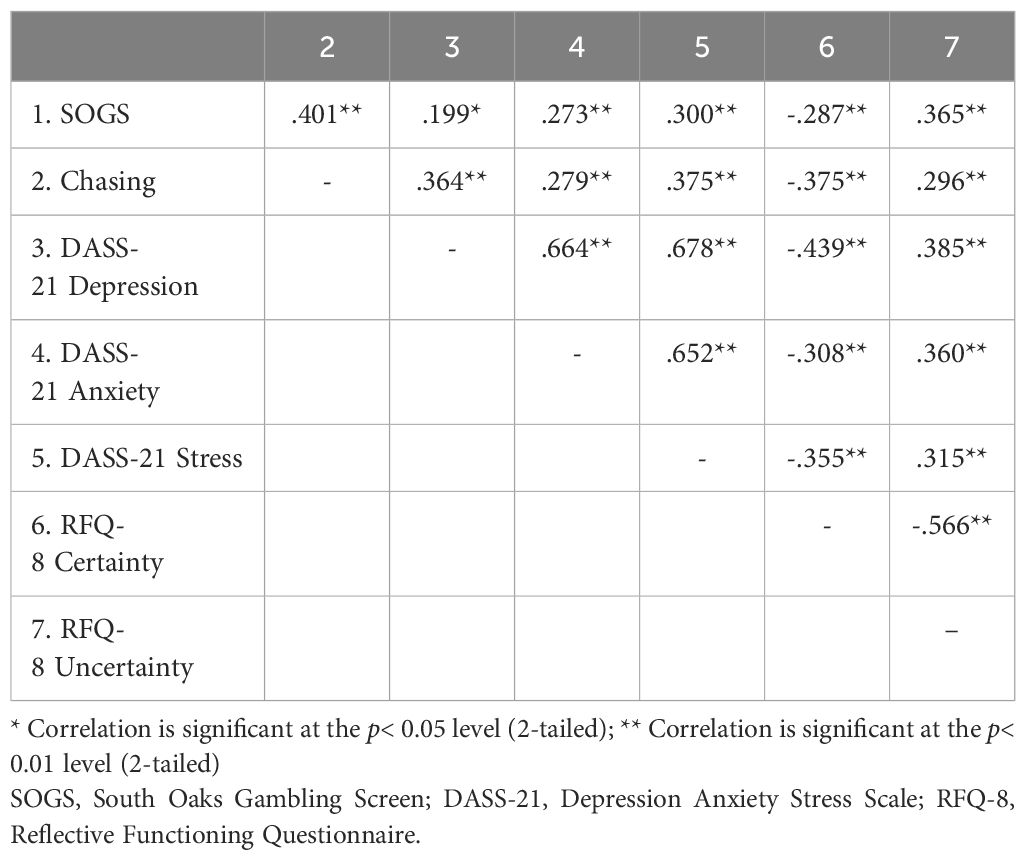
Table 2. Pearson correlation coefficients among measures.
To verify the presence of any differences between participants randomly assigned to the different experimental conditions of the ChasIt task on the examined variables (gender, age, education, SOGS, DASS-21, and RFQ-8 scores), the data were analyzed using either χ2 test or univariate ANOVA. Mixed ANOVA was performed on RFQ-8, given that the scale does not have an overall total score. The results indicated that the three groups did not differ in terms of gender (χ2 [2]= 4.54; p= 0.10) and age (F2,113 = 0.21; p= 0.81), as well as scores on the SOGS (F2,113 = 1.64; p= 0.20), DASS-21 (F2,113 = 0.54; p= 0.58), and RFQ-8 (F2,113 = 0.14; p= 0.87), except for education (in years, F2,113 = 3.25; p<.05), with participants in the control group reporting a significantly lower number of years of education.
Similarly, to ascertain whether SOGS, DASS-21, and RFQ-8 scores, and ChasIT performance varied by gender, analysis was carried out using χ2 test or univariate ANOVA. Mixed ANOVA was performed on RFQ-8, given that the scale does not have an overall total score. The results indicated no significant gender differences for scores on the DASS-21 (F1,114 = 0.06; p=0.80), and RFQ-8 scores (F1,114 = 0.13; p= 0.72), as well as on the decision to chase (χ2 [1]= 1.62; p= 0.20) and chasing frequency (F1,114 = 0.52; p= 0.47). However, there was a significant gender difference in SOGS scores (F1,114 = 11.01; p<.01, η²p= 0.09), with males reporting higher scores than females. The descriptive statistics by gender and ChasIT experimental conditions are shown in the Table 3. For ease of interpretation, descriptive statistics are reported for the untransformed variables.
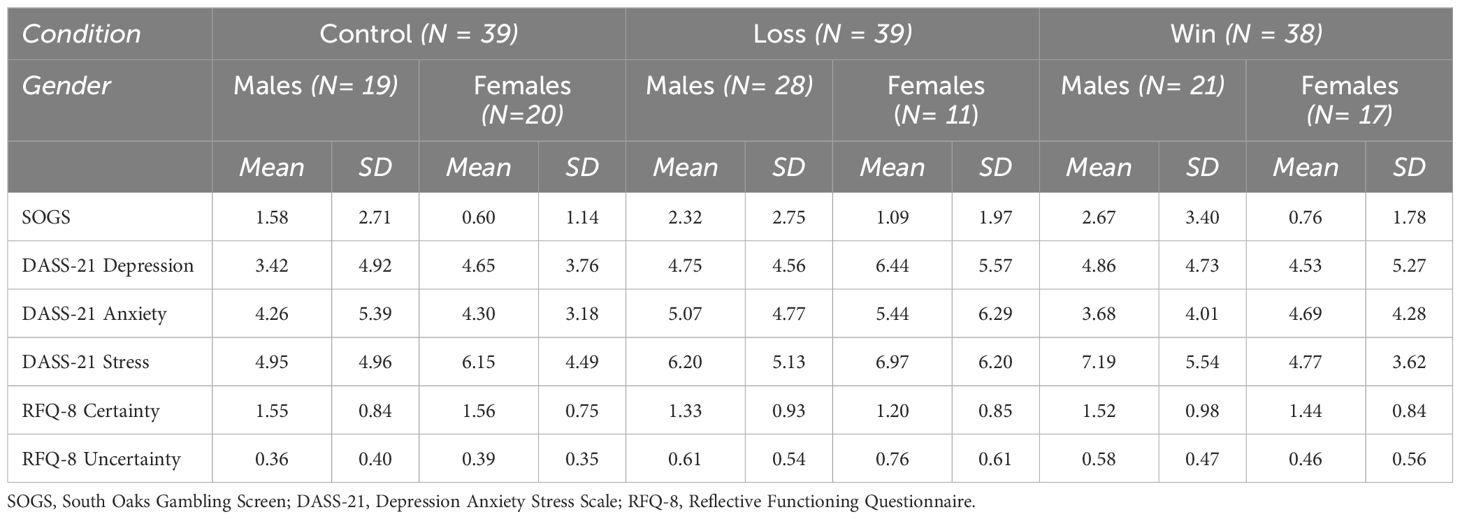
Table 3. Means and standard deviations by ChasIT experimental conditions and gender.
To verify whether SOGS, DASS-21, and RFQ-8 scores, and ChasIT performance varied by age of onset of gambling involvement, analysis was carried out using χ2 test or univariate ANOVA using the four groups of gambling onset (before 18 years, between 18 and 30 years, between 31 and 59 years, and 60 years or over) as the grouping variable. Mixed ANOVA was performed on RFQ-8, given that the scale does not have an overall total score. The results indicated no significant differences for scores on the SOGS (F3,112 = 2.05; p= 0.11), DASS-21 (F3,112 = 0.76; p= 0.52ns), and RFQ-8 scores (F3,112 = 1.43; p= 0.24), as well as on the decision to chase (χ2 [3]= 2.69; p= 0.44) and chasing frequency (F3,112 = 0.13; p= 0.94).
To ascertain whether the decision to chase after the first phase of the ChasIT task was affected by the experimental condition, χ2 was conducted. The analysis showed that the decision to continue gambling did not vary as a function of experimental condition (χ2[2] = 4.10; p= 0.13). Furthermore, to verify if chasing frequency (i.e., the number of trials played during the second phase of the ChasIT task) was affected by the experimental condition, univariate ANOVA was conducted. The analysis showed that the chasing frequency did not vary as a function of experimental condition (F2,113 = 1.31; p= 0.27).
Of the total sample, 29.3% decided to continue gambling in the second half of the ChasIT task for an average number of 12.73 trials played (SD= 10.80). Based on the decision to chase, participants were divided into two groups: chasers and non-chasers. Analyses showed that the two groups did not differ in gender (χ2 [1]= 1.62; p= 0.20) or age (F1,114 = 0.56; p= 0.45), but did on SOGS scores (F1,114 = 15.88; p<.001; η²p= 0.10). Chasers reported higher problem gambling scores on the SOGS than non-chasers. All subsequent analyses were therefore performed controlling for gambling severity.
Chasers and non-chasers were also compared on negative affectivity and mentalizing scores. The ANCOVA performed on the DASS-21 subscales, using decision to chase as the group variable (controlling for SOGS scores) showed no effect for negative affectivity (F2,112 = 3.06; p<.05) but a significant main effect for SOGS scores (F1,113 = 6.71; p=.01; η²p= 0.05), and significant interaction effect for negative affectivity with chasing group (F2,112 = 5.58; p<.01; η²p= 0.09). No main effect for the chasing group (F1,113 = 2.94; p= 0.09) and no interaction for negative affectivity with SOGS scores (F2,112 = 2.29; p= 0.11) were found. The results indicated greater level of depression and stress among chasers, as compared to non-chasers. The difference remained significant even after controlling for gambling severity.
An ANCOVA was also performed on the RFQ-8 subscales, using the decision to chase as the group variable (controlling for SOGS scores). This showed a significant main effect for mentalizing (F1,113 = 31.99; p<.001; η²p= 0.22), and significant interactions for mentalizing with both SOGS (F1,113 = 11.12; p=.001; η²p= 0.09) and chasing group (F1,113 = 6.47; p=.01; η²p= 0.05). No significant main effects for both SOGS (F1,113 = 0.70; p= 0.40) and chasing group (F1,113 = 2.79; p= 0.10) were found. The results indicated greater levels of mentalizing deficits (in the direction of hypermentalizing) among chasers, as compared to non-chasers. The difference remained significant even after controlling for gambling severity.
To evaluate the contributions of gender, age, education, chasing task condition, SOGS scores, DASS-21 and RFQ-8 subscales to chasing behavior, a hierarchical logistic regression analysis was conducted, using decision to chase as the criterion variable. The results of the final regression model indicated that depression and anxiety subscale of DASS-21 and SOGS scores significantly predicted chasing decision (χ2[3, N= 116] = 24.19; p<.001). The overall model explained 27% of variance (Nagelkerke R2). The overall classification accuracy was 75.9% (see Table 4).
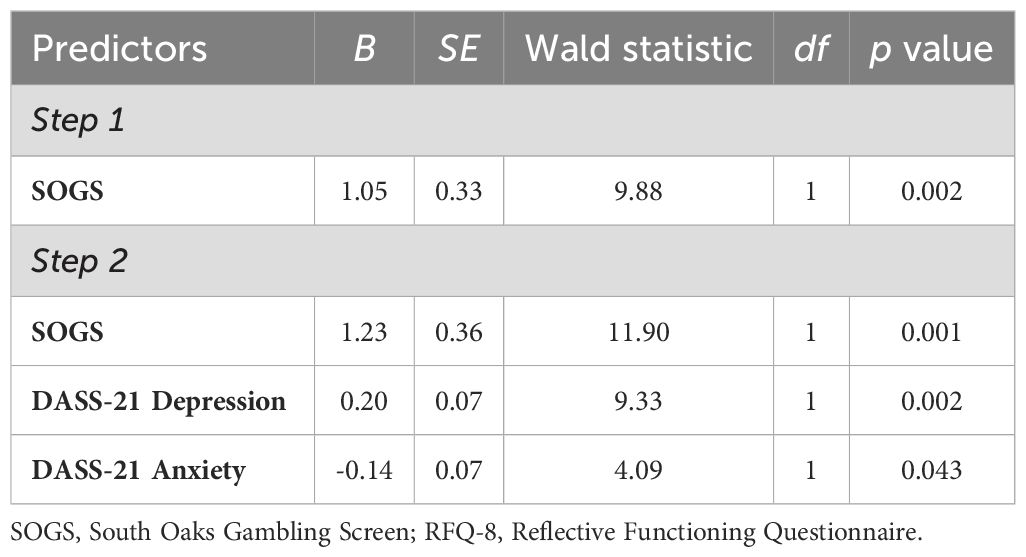
Table 4. Results of hierarchical logistic regression analysis on the decision to chase.
A hierarchical linear regression analysis was also carried out on ChasIT total score (chasing frequency), with gender, age, education, chasing task condition, SOGS scores, DASS-21 and RFQ-8 subscales as independent variables. SOGS, depression subscale of DASS-21 and certainty subscale of RFQ-8 emerged as significant predictors of chasing frequency, with the overall model explaining nearly 30% of the total variance (R2adj= 0.28; F3,112 = 15.91; p <.001) (Table 5).
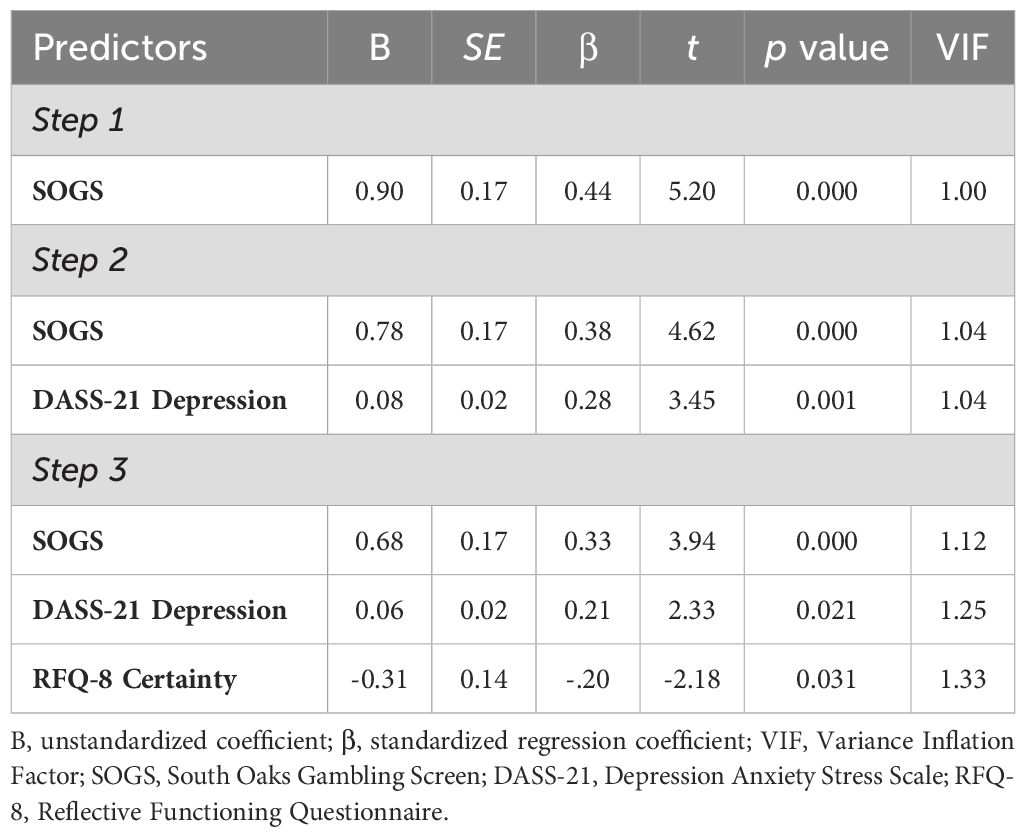
Table 5. Results of hierarchical linear regression analysis on the chasing persistence.
The aim of the present study was to investigate chasing behavior among older-aged gamblers, using an experimental task that is frequently adopted in the literature and has demonstrated good construct validity (29–31, 53, 56, 65, 66), allowing the overcoming of all the limitations of self-report measures (67). More specifically, the study focused on the previously unexplored relationship between chasing, gambling severity, negative affectivity, and mentalizing among older-aged gamblers.
Firstly, the results of the present study showed that the ChasIT conditions (i.e., win, control, and loss, to which each participant was randomly assigned) had no effect on chasing behavior, neither on the decision to continue betting, nor on the frequency of trials played in the task. In other words, participants decided to continue or not continue gambling and how many trials to play irrespective of previous gambling outcomes. While this result may appear odd in light of the fact that DSM-5 diagnostic criteria for gambling disorder explicitly refers to the effect of losses on chasing behavior (14), this observation was not unexpected, given that the majority of studies investigating the role of gambling outcomes (both win and losses) on subsequent decision to persist in gambling have reported no effect of loss or win conditions (30, 31, 56, 65; for a review, see 25). This result, which is echoed in most previous studies, can be interpreted as evidence in support of what was previously suggested by Nigro et al. (29), where chasing behavior represents a personality trait-like characteristic, which therefore disregards contextual variables such as previous gambling outcomes, but is only affected by variables intrinsic to the gambler’s personality, such as impulsivity-related characteristics.
In support of this, past studies have demonstrated strong associations of chasing with both delay discounting (65), foreshortened time horizon (30), alcohol consumption (53), cognitive distortions (66), and subjective feeling of craving (31). In summary, the lack of effect of previous gambling outcomes on chasing behavior could indicate that endophenotypic characteristics have greater weight in incentivizing gamblers to chasing behavior as compared to contextual variables (such as previous wins or losses). However, this result was in contrast to a wealth of studies that, interviewing people about their loss-chasing behavior, showed a frequent continuing and/or intensifying gambling in the face of losses (e.g., 17, 27, 68–72). Regarding this, it cannot be ruled out that within-session chasing (assessed using the ChasIT), i.e., the persistence in the same gambling session, and loss-chasing between-session, i.e., returning another day to gamble, although strongly related, are not overlapping constructs. Moreover, results obtained from the laboratory studies are somewhat inconsistent. Although the majority of studies failed to support this effect (22, 30, 31, 56, 65, 66, 73), a handful of studies have shown that gamblers play more extra trials after losses (29, 74, 75) or wins (51). As suggested by a recent review (25), laboratory study results may mainly depend on the operationalization of the ‘chasing’ construct, on the characteristics of the task used, as well as on the level of gambling severity of the sample recruited.
It should be noted that chasing varied as a function of problem gambling severity. More specifically, participants who decided to chase reported more severe gambling involvement. These results corroborate what was previously found in literature by Yakovenko (75) that, assessing chasing persistence in a laboratory-based slot machine task, found higher levels of persistence among those whose gambling was disordered, compared to those whose gambling was social. Similarly, Auer and Griffiths (76), in a behavioral tracking study involving online casino players, found that chasing varied as a function of problem gambling severity. These findings are further confirmed in regression analyses where severe gambling involvement was found to be a predictor of both the decision to chase and chasing frequency. It is difficult to determine the directionality of this association: individuals may start chasing when their gambling involvement become problematic or could they may develop problem gambling because of repeated attempts to recover losses. Either way, the present study’s results confirm the importance of chasing as an indicator of a severe gambling involvement.
Interestingly, chasers reported higher levels of depression and stress than non-chasers, indicating that chasing, as well as being an indicator of more severe gambling involvement, could be a risk factor for other mental health disorders and/or symptoms. The co-occurrence of gambling disorder with other mental health disorders, including mood disorders (e.g., 9, 77), is very common. Some scholars argue that gambling disorder is a dual disorder due to the difficulty of recognizing gambling as a single nosological entity (78–81).
In general, the present pattern of results (no effect of previous gambling outcomes but an effect of gambling severity on chasing behavior) strongly resemble those of Lister et al. (73). Using a different task (i.e., a slot machine in an immersive virtual casino where gamblers played in a loss or in a win condition), they did not find a significant impact of previous outcomes on chasing persistence and decision to chase but found that participants with problem gambling and those motivated to win money were more likely to chase and gambled for more trials.
With regard to psychological distress, the present study is the first to show that negative affectivity is among the factors that predict chasing behavior. High levels of anxiety and depression were associated with the decision to chase, with depression also being associated with a larger number of trials played. Studies investigating gambling-related motivations have observed that one of the most reported is the relief from negative psychological states (21, 82, 83). Given the frequent association of gambling with negative affectivity (e.g., 49, 84–89; see 90 for a review), alexithymia (e.g., 91, 92), and emotional dysregulation (e.g., 44, 93), gambling may serve not only to ameliorate mood states (e.g., 21, 94) but also to experience excitement, and relieving boredom (95). In fact, individuals who are emotionally dysregulated could react to negative emotions engaging in impulsive behavior, such as persevering in gambling participation (96; see 97 and 98 for reviews), consequently using gambling as a kind of dysfunctional coping strategy. Indirect confirmation of this association also comes from the wealth of studies that have indicated coping as the most reported motivation to gamble, as well as a risk factor for the development of problematic gambling (21, 99–102). The negative reinforcement resulting from mood amelioration provides even more incentive for gambling participation (103) and raises the risk of disordered gambling (104, 105). In the specific field of chasing research, the present findings resonate with those that have identified a significant positive correlation between alexithymia (i.e., the difficulty in processing emotional information) and within-session loss chasing. More specifically, in two laboratory-based studies, Bibby (106) and Bibby and Ross (107) found increasing stake sizes after losses among participants with high levels of alexithymia.
Interestingly, as the regression analyses showed, mentalizing deficits contributed to chasing frequency, complementing a previous study investigating mentalizing ability among those with gambling problems (53). The present study also highlighted that hypermentalizing is an important predictor of chasing frequency among older-aged gamblers. The fact that hypermentalizing (which refers to excessive but inaccurate mentalizing) was associated with a greater number of trials played resembles the same phenomenon that has been observed in previous studies (50, 51), where participants with gambling problems, while performing worse than controls by making disadvantageous decisions, were so confident in their performance to the point that they were willing to bet on the quality of their own decisions. This lack of self-awareness in both gambling and non-gambling situations of decision-making, combined with an individual’s overconfidence in their own abilities, could push the gambler to persist in gambling in the belief that they will be able to get even. Moreover, the present study’s results further corroborate the importance of mentalizing in maintaining gambling problems (44, 47–49, 52, 53), and also extending its role as a risk factor for problem gambling among older-age gamblers.
Taken together, the present results indicate that depression and anxiety may motivate the decision to continue gambling irrespective of previous gambling outcomes in the attempt to ameliorate poor mood. The inability of gamblers to mentalize and, therefore, to reflect on their behavior and understand their underlying mental states, may explain the increased frequency of chasing, (i.e., why gamblers are unable to stop this dysfunctional behavior that, over time, is strongly associated with a problematic gambling involvement).
As for the study’s limitations, a non-clinical sample was used, although it must be considered that almost all the gamblers in the sample were familiar with playing cards, in line with the task that was used (ChasIT). Furthermore, the low sample size and potential selection bias in the recruitment of the sample are also potential limitations. It should also be noted that some of the psychometric scales used have not been specifically validated among older population. Moreover, the card game adopted to assess chasing behavior had limitations regarding the present study’s ecological validity, for different reasons. First, the small bets used may have been unattractive, given winning money is among the most reported motivations to both gamble and chasing (73; see also 108). Second, even if the influence of the type of rewards in influencing behaviors in the gambling task was unclear (e.g., 109–112), it should be noted that ChasIT task used non-real money. All these structural characteristics of the task might ultimately reduce the generalizability of the present findings. Finally, it should be noted that (i) a large proportion of gamblers now play online, whereas in the present study only a small proportion of the sample preferred gambling online; and (ii) elderly individuals constitute a heterogeneous group regarding gambling phenotypes (113), therefore, the present findings cannot be not generalized to all old-age gamblers, especially in the light of the observation that, in the present study, only 5.3% started gambling at the age of 60 years or older. It appears rare that individuals start gambling in old age. In general, given the small effect sizes, the present results should be interpreted cautiously, suggesting that the relationship between the study variables should be investigated using larger samples. Moreover, future studies should also compare the endophenotypic characteristics of older gamblers who start gambling at an older age with those who start at a young age.
The present study is the first to assess the role of gambling severity, psychological distress, and mentalizing in chasing behavior among older-age gamblers. The results demonstrated that depression and hypermentalizing, along with high levels of gambling involvement, contributed significantly to chasing behavior among the older age cohort, which, in turn, maintain problem gambling. In the light of gambling literature, it is conceivable that, in conditions of a compromised mentalization, depressed gamblers seek relief by persevering in gambling. Considering the close relationship between the ability to mentalize and the regulation of the emotional states, with mentalizing predicting both adaptive and maladaptive emotion regulation strategies (35), the present study’s results suggest that a specific training on mentalizing abilities is needed. This could help gamblers to acquire more awareness of their internal states and to reflect on their own behaviors in terms of mental states, through a process of reflection rather than following the impulse to gamble. Individuals reflecting on their own behaviors in terms of mental states involves recognizing the motivations underlying gambling behavior, as well as the choice to chase losses. Given the study’s findings, the ability to mentalize allows the opportunity to break the vicious cycle that might lead gamblers to gamble when they are depressed, finding alternative and more functional ways to improve their mood. Such interventions could have the potential to offset the trajectory toward the disorder among old age gamblers (as well as gamblers of any age).
Despite the limitations, the findings of the present study make an important contribution, providing insight into the variables that, among older-aged gamblers, contribute to chasing that is a key risk factor in several theoretical models of gambling disorder, as well as a crucial transition point from initial gambling involvement to the development of gambling disorder.
The raw data supporting the conclusions of this article will be made available by the corresponding author upon reasonable request.
The studies involving humans were approved by the Ethics Committee of the Department of Psychology, University of Campania “Luigi Vanvitelli”. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
MCi: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Writing – original draft, Writing – review & editing, Project administration. BP: Data curation, Methodology, Writing – original draft. MCo: Investigation, Data curation, Writing – original draft. FD’O: Formal Analysis, Methodology, Writing – original draft. MDG: Supervision, Writing – review & editing. GN: Conceptualization, Investigation, Software, Supervision, Methodology, Writing – review & editing.
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. This research was supported by the Young Researcher Grant initiative of the University of Campania “Luigi Vanvitelli” (project “GOLD – Gambling in OLD age”, cup number B63C23000650005).
MDG has received research funding from Norsk Tipping (the gambling operator owned by the Norwegian government); has received funding for a number of research projects in the area of gambling education for young people, social responsibility in gambling and gambling treatment from Gamble Aware (formerly the Responsibility in Gambling Trust), a charitable body which funds its research program based on donations from the gambling industry; undertakes consultancy for various gambling companies in the area of player protection and social responsibility in gambling.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Calado F, Griffiths MD. Problem gambling worldwide: An update and systematic review of empirical research (2000–2015). J Behav Addict. (2016) 5:592–613. doi: 10.1556/2006.5.2016.073
2. Tse S, Hong SI, Wang CW, Cunningham-Williams RM. Gambling behavior and problems among older adults: A systematic review of empirical studies. J Gerontol B Psychol Sci Soc Sci. (2012) 67:639–52. doi: 10.1093/geronb/gbs068
3. Zaranek RR, Lichtenberg PA. Urban elders and casino gambling: Are they at risk of a gambling problem? J Aging Stud. (2008) 22:13–23. doi: 10.16/j.jaging.2007.11.001
4. Bazargan M, Bazargan S, Akanda M. Gambling habits among aged African Americans. Clin Gerontol: J Aging Ment Health. (2001) 22:51–62. doi: 10.1300/J018v22n03_06
5. Pietrzak RH, Morasco BJ, Blanco C, Grant BF, Petry NM. Gambling level and psychiatric and medical disorders in older adults: Results from the National Epidemiologic Survey on alcohol and related conditions. Am J Geriatr Psychiatry. (2007) 15:301–13. doi: 10.1097/01.JGP.0000239353.40880.cc
6. Subramaniam M, Wang P, Soh P, Vaingankar JA, Chong SA, Browning CJ, et al. Prevalence and determinants of gambling disorder among older adults: A systematic review. Addict Behav. (2015) 41:199–209. doi: 10.1016/j.addbeh.2014.10.007
7. McCarrey AC, Henry JD, von Hippel W, Weidemann G, Sachdev PS, Wohl MJA, et al. Age differences in neural activity during slot machine gambling: an fMRI study. PloS One. (2012) 7:e49787. doi: 10.1371/journal.pone.0049787
8. Warrier V, Chamberlain SR, Thomas SA, Bowden-Jones H. Genetics of gambling disorder and related phenotypes: The potential uses of polygenic and multifactorial risk models to enable early detection and improve clinical outcomes. J Behav Addict. (2024) 13:16–20. doi: 10.1556/2006.2023.00075
9. Potenza MN, Balodis IM, Derevensky J, Grant JE, Petry NM, Verdejo-Garcia A, et al. Gambling disorder. Nat Rev Dis Primers. (2019) 5:51. doi: 10.1038/s41572-019-0099-7
10. Sharpe L. A reformulated cognitive-behavioral model of problem gambling: A biopsychosocial perspective. Clin Psychol Rev. (2002) 22:1–25. doi: 10.1016/S0272-7358(00)00087-8
11. Zhang K, Clark L. Loss-chasing in gambling behaviour: Neurocognitive and behavioural economic perspectives. Curr Opin Behav Sci. (2020) 31:1–7. doi: 10.1016/j.cobeha.2019.10.006
12. Everitt BJ, Giuliano C, Belin D. Addictive behaviour in experimental animals: prospects for translation. Philos Trans R Soc Lond B Biol Sci. (2018) 373:20170027. doi: 10.1098/rstb.2017.0027
13. Toce-Gerstein M, Gerstein DR, Volberg RA. A hierarchy of gambling disorders in the community. Addict. (2003) 98:1661–72. doi: 10.1111/j.1360-0443.2003.00545.x
14. American Psychiatric Association. Diagnostic and statistical manual of mental disorders. 5th ed. Arlington, VA: American Psychiatric Publishing (2013).
15. Ladouceur R, Walker M. A cognitive perspective on gambling. In: Salkovskis PM, editor. Trends in cognitive therapy. Wiley, Oxford (UK (1996). p. 89–120.
16. Lesieur HR. The compulsive gambler’s spiral of options and involvement. Psychiatry. (1979) 42:79–87.
17. Stinchfield R, Govoni R, Ron Frisch G. DSM-IV diagnostic criteria for pathological gambling: Reliability, validity, and classification accuracy. Am J Addict. (2005) 14:73–82. doi: 10.1080/10550490590899871
18. Gainsbury SM, Suhonen N, Saastamoinen J. Chasing losses in online poker and casino games: Characteristics and game play of internet gamblers at risk of disordered gambling. Psychiatry Res. (2014) 217:220–5. doi: 10.1016/j.psychres.2014.03.033
19. Quester S, Romanczuk-Seiferth N. Brain imaging in gambling disorder. Curr Addict Rep. (2015) 2:220–9. doi: 10.1007/s40429-015-0063-x
20. American Psychiatric Association. Diagnostic and statistical Manual of Mental Disorders. 3rd ed. Washington, DC: American Psychiatric Association (1980).
21. Blaszczynski A, Nower L. A pathways model of problem and pathological gambling. Addict. (2002) 97:487–99. doi: 10.1046/j.1360-0443.2002.00015.x
22. O’Connor J, Dickerson M. Definition and measurement of chasing in off-course betting and gaming machine play. J Gambl Stud. (2003) 19:359–86. doi: 10.1023/A:1026375809186
23. Subramaniam M, Chong SA, Browning C, Thomas S. Cognitive distortions among older adult gamblers in an Asian context. PloS One. (2017) 12:e0178036. doi: 10.1371/journal.pone.0178036
24. Breen RB, Zuckerman M. [amp]]lsquo;Chasing’ in gambling behavior: Personality and cognitive determinants. Pers Individ Diff. (1999) 27:1097–111. doi: 10.1016/S0191-8869(99)00052-5
25. Banerjee N, Chen Z, Clark L, Noël X. Behavioural expressions of loss-chasing in gambling: A systematic scoping review. Neurosci Biobehav Rev. (2023) 153:105377. doi: 10.1016/j.neubiorev.2023.105377
26. Nower L, Blaszczynski A, Anthony WL. Clarifying gambling subtypes: The revised pathways model of problem gambling. Addict. (2022) 117:2000–8. doi: 10.1111/add.15745
27. Sleczka P, Romild U. On the stability and the progression of gambling problems: Longitudinal relations between different problems related to gambling. Addict. (2021) 116:116–25. doi: 10.1111/add.15093
28. Linnet J, Røjskjær S, Nygaard J, Maher BA. Episodic chasing in pathological gamblers using the Iowa Gambling Task. Scand J Psychol. (2006) 47:43–9. doi: 10.1111/j.1467-9450.2006.00491.x
29. Nigro G, Ciccarelli M, Cosenza M. Tempting fate: Chasing and maladaptive personality traits in gambling behavior. Psychiatry Res. (2018) 267:360–7. doi: 10.1016/j.psychres.2018.05.088
30. Ciccarelli M, Cosenza M, Griffiths MD, D’Olimpio F, Nigro G. The interplay between chasing behavior, time perspective, and gambling severity: An experimental study. J Behav Addict. (2019) 8:259–67. doi: 10.1556/2006.8.2019.29
31. Cosenza M, Matarazzo O, Ciccarelli M, Nigro G. Chasing the desire: An investigation on the role of craving, time perspective, and alcohol use in adolescent gambling. Addict Behav. (2020) 111:106566. doi: 10.1016/j.addbeh.2020.106566
32. O’Connor J, Dickerson M. Emotional and cognitive functioning in chasing gambling losses. In: Coman G, Evans B, Wootton R, editors. Responsible gambling: A future winner. National Association for Gambling Studies, Melbourne, Australia (1997). p. 280–5.
33. Thomsen KR, Callesen MB, Linnet J, Kringelbach ML, Møller A. Severity of gambling is associated with severity of depressive symptoms in pathological gamblers. Behav Pharmacol. (2009) 20:527–36. doi: 10.1097/FBP.0b013e3283305e7a
34. Devos G, Clark L, Maurage P, Billieux J. Induced sadness increases persistence in a simulated slot machine task among recreational gamblers. Psychol Addict Behav. (2018) 32:383–8. doi: 10.1037/adb0000364
35. Schwarzer NH, Nolte T, Fonagy P, Gingelmaier S. Mentalizing and emotion regulation: Evidence from a nonclinical sample. Int Forum Psychoanalysis. (2021) 30:34–45. doi: 10.1080/0803706X.2021.1873418
36. Ballespi S, Vives J, Alonso N, Sharp C, Salvadora Ramirez M, Fonagy P, et al. To know or not to know: Mentalization as a protection from somatic complaints. PloS One. (2019) 14:e0215308. doi: 10.1371/journal.pone.0215308
37. Nolte T, Bolling D, Hudac C, Fonagy P, Mayes L, Pelphrey K. Brain mechanisms underlying the impact of attachment-related stress on social cognition. Front Hum Neurosci. (2013) 7:816. doi: 10.3389/fnhum.2013.00816
38. Taubner S. Konzept Mentalisieren. Eine Einführung in Forschung und Praxis [Concept mentalizing. Introduction into research and practice]. Gießen: Psychosozial-Verlag (2015).
39. Allen JG, Fonagy P, Bateman A. Mentalisieren in der psychotherapeutischen Praxis [Mentalizing in clinical practice]. Stuttgart: Klett-Cotta (2011).
40. Fonagy P, Allison E. The role of mentalizing and epistemic trust in the therapeutic relationship. Psychother. (2014) 51:372–80. doi: 10.1037/a0036505
41. Fonagy P, Gergely G, Jurist E, Target M. Affektregulierung, Mentalisierung und die Entwicklung des Selbst [Affect regulation, mentalization, and the development of the self]. Stuttgart: Klett-Cotta (2015).
42. Bateman A, Fonagy P. Psychotherapie der Borderline-Persönlichkeitsstörung: ein mentalisierungsgestütztes Behandlungskonzept; mit einem umfangreichen Behandlungsmanual. Gießen: Psychosozial-Verlag (2008).
43. Fonagy P, Target M. Psychoanalyse und die Psychopathologie der Entwicklung [Psychoanalytic theories: Perspectives from developmental psychopathology]. Stuttgart: Klett-Cotta (2011).
44. Ciccarelli M, Nigro G, D’Olimpio F, Griffiths MD, Cosenza M. Mentalizing failures, emotional dysregulation, and cognitive distortions among adolescent problem gamblers. J Gambl Stud. (2021) 37:283–98. doi: 10.1007/s10899-020-09967-w
45. Pizzini B, Cosenza M, Nigro G, Sacco M, Ciccarelli M. Maladaptive personality trait facets and mentalization in youth gambling. Int J Ment Health Addict. (2023), 1–22. doi: 10.1007/s11469-023-01210-y
46. Fonagy P, Bateman AW. Adversity, attachment, and mentalizing. Compr Psychiatry. (2016) 64:59–66. doi: 10.1016/j.comppsych.2015.11.006
47. Cosenza M, Ciccarelli M, Nigro G. The steamy mirror of adolescent gamblers: Mentalization, impulsivity, and time horizon. Addict Behav. (2019) 89:156–62. doi: 10.1016/j.addbeh.2018.10.002
48. Cosenza M, Ciccarelli M, Pizzini B, Griffiths MD, Sacco M, Nigro G. The role of loneliness, negative affectivity, mentalization, and alcohol use in adolescent gambling. Med J Clin Psychol. (2022) 10. doi: 10.13129/2282-1619/mjcp-3425
49. Cosenza M, Ciccarelli M, Sacco M, Nigro G, Pizzini B. Attachment dimensions and adolescent gambling: The mediating role of mentalization. Med J Clin Psychol. (2022) 10. doi: 10.13129/2282-1619/mjcp-3446
50. Brevers D, Cleeremans A, Bechara A, Greisen M, Kornreich C, Verbanck P, et al. Impaired self-awareness in pathological gamblers. J Gambl Stud. (2013) 29:119–29. doi: 10.1007/s10899-012-9292-2
51. Brevers D, Cleeremans A, Bechara A, Greisen M, Kornreich C, Verbanck P, et al. Impaired metacognitive capacities in individuals with problem gambling. J Gambl Stud. (2014) 30:141–52. doi: 10.1007/s10899-012-9348-3
52. Ciccarelli M, Cosenza M, Nigro G, Griffiths MD, D’Olimpio F. Gaming and gambling in adolescence: the role of personality, reflective functioning, time perspective and dissociation. Int Gambl Stud. (2022) 22:161–79. doi: 10.1080/14459795.2021.1985583
53. Nigro G, Matarazzo O, Ciccarelli M, D’Olimpio F, Cosenza M. To chase or not to chase: A study on the role of mentalization and alcohol consumption in chasing behavior. J Behav Addict. (2019) 8:743–53. doi: 10.1556/2006.8.2019.67
54. Moran JM, Jolly E, Mitchell JP. Social-cognitive deficits in normal aging. J Neurosci. (2012) 32:5553–61. doi: 10.1523/JNEUROSCI.5511-11.2012
55. Pardini M, Nichelli PF. Age-related decline in mentalizing skills across adult life span. Exp Aging Res. (2009) 35:98–106. doi: 10.1080/03610730802545259
56. Nigro G, Ciccarelli M, Cosenza M. The illusion of handy wins: Problem gambling, chasing, and affective decision-making. J Affect Disord. (2018) 225:256–9. doi: 10.1016/j.jad.2017.08.010
57. Lesieur HR, Blume SB. The South Oaks Gambling Screen (SOGS): A new instrument for the identification of pathological gamblers. Am J Psychiatry. (1987) 144:1184–8. doi: 10.1176/ajp.144.9.1184
58. Cosenza M, Matarazzo O, Baldassarre I, Nigro G. Deciding with (or without) the future in mind: Individual differences in decision-making. In: Bassis S, Esposito A, Morabito F, editors. Recent advances of neural network models and applications. Springer, Cham, Switzerland (2014). p. 435–43.
59. Henry JD, Crawford JR. The short-form version of the Depression Anxiety Stress Scales (DASS-21): Construct validity and normative data in a large non-clinical sample. Br J Clin Psychol. (2005) 44:227–39. doi: 10.1348/014466505X29657
60. Bottesi G, Ghisi M, Altoè G, Conforti E, Melli G, Sica C. The Italian version of the Depression Anxiety Stress Scales-21: Factor structure and psychometric properties on community and clinical samples. Compr Psychiatry. (2015) 60:170–81. doi: 10.1016/j.comppsych.2015.04.005
61. Fonagy P, Luyten P, Moulton-Perkins A, Lee YW, Warren F, Howard S, et al. Development and validation of a self-report measure of mentalizing: The reflective functioning questionnaire. PloS One. (2016) 11:e0158678. doi: 10.1371/journal.pone.0158678
62. Morandotti N, Brondino N, Merelli A, Boldrini A, De Vidovich GZ, Ricciardo S, et al. The Italian version of the Reflective Functioning Questionnaire: Validity data for adults and its association with severity of borderline personality disorder. PloS One. (2018) 13:e0206433. doi: 10.1371/journal.pone.0206433
64. Johnston R, Jones K, Manley D. Confounding and collinearity in regression analysis: a cautionary tale and an alternative procedure, illustrated by studies of British voting behaviour. Qual Quant. (2018) 52:1957–76. doi: 10.1007/s11135-017-0584-6
65. Ciccarelli M, Cosenza M, D’Olimpio F, Griffiths MD, Nigro G. An experimental investigation of the role of delay discounting and craving in gambling chasing behavior. Addict Behav. (2019) 93:250–6. doi: 10.1016/j.addbeh.2019.02.002
66. Nigro G, Matarazzo O, Ciccarelli M, Pizzini B, Sacco M, Cosenza M. Positive Illusions: The role of cognitive distortions related to gambling and temporal perspective in chasing behavior. J Gambl Stud. (2022) 38:889–904. doi: 10.1007/s10899-021-10068-5
67. Orford J. The fascination of psychometrics: Commentary on Gerstein. Addict. (2003) 98:1675–7. doi: 10.1111/j.1360-0443.2003.00578.x
68. Christensen DR, Jackson AC, Dowling NA, Volberg RA, Thomas SA. An examination of a proposed DSM-IV pathological gambling hierarchy in a treatment seeking population: Similarities with substance dependence and evidence for three classification systems. J Gambl Stud. (2015) 31:787–806. doi: 10.1007/s10899-014-9449-2
69. Delfabbro P, King DL. Is there a continuum of behavioural dependence in problem gambling? Evidence from 15 years of Australian prevalence research. Int J Ment Health Addict. (2021) 20:2208–20. doi: 10.1007/s11469-021-00509-y
70. James RJE, O’Malley C, Tunney RJ. Loss of control as a discriminating factor between different latent classes of disordered gambling severity. J Gambl Stud. (2016) 32:1155–73. doi: 10.1007/s10899-016-9592-z
71. McBride O, Adamson G, Shevlin M. A latent class analysis of DSM-IV pathological gambling criteria in a nationally representative British sample. Psychiatry Res. (2010) 178:401–7. doi: 10.1016/j.psychres.2009.11.010
72. Nong SZ, Fong LHN, Fong DKC, Lam D. Segmenting Chinese gamblers based on gambling forms: A latent class analysis (MEDLINE®). J Gambl Stud. (2020) 36:141–59. doi: 10.1007/s10899-019-09877-6
73. Lister JJ, Nower L, Wohl MJ. Gambling goals predict chasing behavior during slot machine play. Addict Behav. (2016) 62:129–34. doi: 10.1016/j.addbeh.2016.06.018
74. Bonini N, Grecucci A, Nicolè M, Savadori L. Reduced risk-taking after prior losses in pathological gamblers under treatment and healthy control group but not in problem gamblers. J Gambl Stud. (2018) 34:429–47. doi: 10.1007/s10899-017-9709-z
75. Yakovenko I. Chasing the loss: Factors that predict within-and between-session chasing in gamblers. Calgary, Canada: University of Calgary (2017). doi: 10.11575/PRISM/25310
76. Auer M, Griffiths MD. The relationship between structural characteristics and gambling behaviour: An online gambling player tracking study. J Gambl Stud. (2023) 39:265–79. doi: 10.1007/s10899-022-10115-9
77. Miles M, Rothschild J, Åkesson G, Håkansson A. Nationwide, multioperator self-exclusion and psychiatric comorbidity in patients with gambling disorder: A retrospective chart review study from a regional treatment unit. J Addict. (2023) 1:5532259. doi: 10.1155/2023/5532259
78. Szerman N, Martinez-Raga J. Dual disorders: two different mental disorders? Adv Dual Diagn. (2015) 8:61–4. doi: 10.1108/ADD-03-2015-0004
79. Szerman N, Peris L. Precision psychiatry and dual disorders. J Dual Diagn. (2018) 14:237–46. doi: 10.1080/15504263.2018.1512727
80. Szerman N, Ferre F, Basurte-Villamor I, Vega P, Mesias B, Marín-Navarrete R, et al. Gambling dual disorder: A dual disorder and clinical neuroscience perspective. Front Psychiatry. (2020) 11:589155. doi: 10.3389/fpsyt.2020.589155
81. Szerman N, Basurte-Villamor I, Vega P, Mesías B, Martínez-Raga J, Ferre F, et al. Is there such a thing as gambling dual disorder? Preliminary evidence and clinical profiles. Eur Neuropsychopharmacol. (2023) 66:78–91. doi: 10.1016/j.euroneuro.2022.11.010
82. Blaszczynski A, McConaghy N. Anxiety and/or depression in the pathogenesis of addictive gambling. Int J Addict. (1989) 24:337–50. doi: 10.3109/10826088909047292
83. Dickerson MG, Baron E, Hong SM, Cottrell D. Estimating the extent and degree of gambling related problems in the Australian population: A national survey. J Gambl Stud. (1996) 12:161–78. doi: 10.1007/BF01539172
84. Blinn-Pike L, Worthy SL, Jonkman JN. Adolescent gambling: A review of an emerging field of research. J Adolesc Health. (2010) 47:223–36. doi: 10.1016/j.jadohealth.2010.05.003
85. Ciccarelli M, Nigro G, Griffiths MD, Cosenza M, D’Olimpio F. Attentional biases in problem and non-problem gamblers. J Affect Disord. (2016) 198:135–41. doi: 10.1016/j.jad.2016.03.009
86. Ciccarelli M, Nigro G, Griffiths MD, Cosenza M, D’Olimpio F. Attentional bias in non-problem gamblers, problem gamblers, and abstinent pathological gamblers: an experimental study. J Affect Disord. (2016) 206:9–16. doi: 10.1016/j.jad.2016.07.017
87. Ciccarelli M, Griffiths MD, Nigro G, Cosenza M. Decision making, cognitive distortions and emotional distress: A comparison between pathological gamblers and healthy controls. J Behav Ther Exp Psychiatry. (2017) 54:204–10. doi: 10.1016/j.jbtep.2016.08.012
88. Nigro G, Cosenza M, Ciccarelli M. The blurred future of adolescent gamblers: Impulsivity, time horizon, and emotional distress. Front Psychol. (2017) 8:486. doi: 10.3389/fpsyg.2017.00486
89. Nigro G, D’Olimpio F, Ciccarelli M, Cosenza M. The fuzzy future: Time horizon, memory failures, and emotional distress in gambling disorder. Addict Behav. (2019) 97:7–13. doi: 10.1016/j.addbeh.2019.05.012
90. Richard J, Fletcher E, Boutin S, Derevensky J, Temcheff C. Conduct problems and depressive symptoms in association with problem gambling and gaming: A systematic review. J Behav Addict. (2020) 9:497–533. doi: 10.1556/2006.2020.00045
91. Estévez A, Jauregui P, Macía L, López-González H. Gambling and attachment: The mediating role of alexithymia in adolescents and young adults. J Gambl Stud. (2021) 37:497–514. doi: 10.1007/s10899-020-09965-y
92. Topino E, Griffiths MD, Gori A. Attachment and gambling severity behaviors among regular gamblers: A path modeling analysis exploring the role of alexithymia, dissociation, and impulsivity. Int J Ment Health Addict. (2023). doi: 10.1007/s11469-023-01080-4
93. Mestre-Bach G, Granero R, Fernández-Aranda F, Potenza MN, Jiménez-Murcia S. Roles for alexithymia, emotion dysregulation and personality features in gambling disorder: A network analysis. J Gambl Stud. (2023) 39:1207–23. doi: 10.1007/s10899-022-10164-0
94. Wood RT, Griffiths MD. A qualitative investigation of problem gambling as an escape-based coping strategy. Psychol Psychother: Theory Res Pract. (2007) 80:107–25. doi: 10.1348/147608306X107881
95. Griffiths M. The role of subjective mood states in the maintenance of fruit machine gambling behavior. J Gambl Stud. (1995) 11:123–35. doi: 10.1007/BF02107111
96. Tice DM, Bratslavsky E, Baumeister RF. Emotional distress regulation takes precedence over impulse control: If you feel bad, do it! J Pers Soc Psychol. (2001) 80:53–67. doi: 10.1037//0022-3514.80.1.53
97. Rogier G, Velotti P. Conceptualizing gambling disorder with the process model of emotion regulation. J Behav Addict. (2018) 7:239–51. doi: 10.1556/2006.7.2018.52
98. Marchica L, Mills D, Derevensky J, Montreuil T. The role of emotion regulation in video gaming and gambling disorder: A systematic review. Can J Addict. (2019) 10:19–29. doi: 10.1097/CXA.0000000000000070
99. Canale N, Vieno A, Griffiths MD, Rubaltelli E, Santinello M. How do impulsivity traits influence problem gambling through gambling motives? The role of perceived gambling risk/benefits. Psychol Addict Behav. (2015) 29:813–23. doi: 10.1037/adb0000060
100. Devos G, Challet-Bouju G, Burnay J, Maurage P, Grall-Bronnec M, Billieux J. Adaptation and validation of the Gambling Motives Questionnaire-Financial (GMQ-F) in a sample of French-speaking gamblers. Int Gambl Stud. (2017) 17:87–101. doi: 10.1080/14459795.2016.1264080
101. Milosevic A, Ledgerwood DM. The subtyping of pathological gambling: A comprehensive review. Clin Psychol Rev. (2010) 30:988–98. doi: 10.1016/j.cpr.2010.06.013
102. Nower L, Blaszczynski A. Development and validation of the gambling pathways questionnaire (GPQ). Psychol Addict Behav. (2017) 31:95–109. doi: 10.1037/adb0000234
103. Schreiber LR, Grant JE, Odlaug BL. Emotion regulation and impulsivity in young adults. J Psychiatr Res. (2012) 46:651–8. doi: 10.1016/j.jpsychires.2012.02.005
104. Stewart SH, Zack M. Development and psychometric evaluation of a three-dimensional Gambling Motives Questionnaire. Addict. (2008) 103:1110–7. doi: 10.1111/j.1360-0443.2008.02235.x
105. Stewart SH, Zack M, Collins P, Klein RM, Fragopoulos F. Subtyping pathological gamblers on the basis of affective motivations for gambling: Relations to gambling problems, drinking problems, and affective motivations for drinking. Psychol Addict Behav. (2008) 22:257–68. doi: 10.1037/0893-164X.22.2.257
106. Bibby PA. Loss-chasing, alexithymia, and impulsivity in a gambling task: Alexithymia as a precursor to loss-chasing behavior when gambling. Front Psychol. (2016) 7:3. doi: 10.3389/fpsyg.2016.00003
107. Bibby PA, Ross KE. Alexithymia predicts loss chasing for people at risk for problem gambling. J Behav Addict. (2017) 6:630–8. doi: 10.1556/2006.6.2017.076
108. Young MM, Wohl MJ, Matheson K, Baumann S, Anisman H. The desire to gamble: The influence of outcomes on the priming effects of a gambling episode. J Gambl Stud. (2008) 24:275–93. doi: 10.1007/s10899-008-9093-9
109. Fernie G, Tunney RJ. Some decks are better than others: The effect of reinforcer type and task instructions on learning in the Iowa gambling task. Brain Cognit. (2006) 60:94–102. doi: 10.1016/j.bandc.2005.09.011
110. Johnson MW, Bickel WK. Within-subject comparison of real and hypothetical money rewards in delay discounting. J Exp Anal Behav. (2002) 77:129–46. doi: 10.1901/jeab.2002.77-129
111. Lagorio CH, Madden GJ. Delay discounting of real and hypothetical rewards III: Steady-state assessments, forced-choice trials, and all real rewards. Behav Processes. (2005) 69:173–87. doi: 10.1016/j.beproc.2005.02.003
112. Weinberg A, Riesel A, Proudfit GH. Show me the money: The impact of actual rewards and losses on the feedback negativity. Brain Cognit. (2014) 87:134–9. doi: 10.1016/j.bandc.2014.03.015
Keywords: gambling, problem gambling, older-aged gambling, chasing, psychological distress, mentalizing, depression, hypermentalizing
Citation: Ciccarelli M, Pizzini B, Cosenza M, D’Olimpio F, Griffiths MD and Nigro G (2024) Chasing among older-aged gamblers: the role of mentalizing and psychological distress. Front. Psychiatry 15:1418339. doi: 10.3389/fpsyt.2024.1418339
Received: 16 April 2024; Accepted: 22 October 2024;
Published: 13 November 2024.
Edited by:
Carlos Roncero, University of Salamanca, SpainReviewed by:
Nestor Szerman, Gregorio Marañón Hospital, SpainCopyright © 2024 Ciccarelli, Pizzini, Cosenza, D’Olimpio, Griffiths and Nigro. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Maria Ciccarelli, bWFyaWEuY2ljY2FyZWxsaUB1bmljYW1wYW5pYS5pdA==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.