
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychiatry , 23 July 2024
Sec. Mood Disorders
Volume 15 - 2024 | https://doi.org/10.3389/fpsyt.2024.1410252
This article is part of the Research Topic Understanding Vulnerability to Major Depressive Disorder View all 11 articles
 Alicja Kubanek1*
Alicja Kubanek1* Marcin Renke1
Marcin Renke1 Beata R. Godlewska2
Beata R. Godlewska2 Przemysław Paul1Mateusz Przybylak3Anna S. Kowalska4Piotr Wąż5Michał Błaszczyk6Aleksandra Macul-Sanewska6Przemysław Rutkowski7
Przemysław Paul1Mateusz Przybylak3Anna S. Kowalska4Piotr Wąż5Michał Błaszczyk6Aleksandra Macul-Sanewska6Przemysław Rutkowski7 Kamila Czarnacka8Krzysztof Bednarski8
Kamila Czarnacka8Krzysztof Bednarski8 Jakub Grabowski3
Jakub Grabowski3Background: Depressive disorder is common among haemodialysis patients. The purpose of this study was to explore approaches to diagnosing depression in the context of a real-life setting, with the view of creating practical recommendations. It also aimed to evaluate the prevalence of depression and dementia.
Methods: We conducted a cross-sectional study in two Dialysis Centres in Poland. Cognitive functions were evaluated using Mini–Mental State Examination (MMSE). The screening for depressive symptoms was assessed using Beck Depression Inventory II (BDI-II). The diagnosis of major depressive disorder was confirmed by a psychiatrist using Diagnostic and Statistical Manual of Mental Disorders 5 (DSM-5). Sociodemographic and clinical data were also collected.
Results: Initially, 136 patients agreed to participate in the study. Dementia was found in 13% of the study group. Sixty-two patients did not agree to perform all the proposed tests and were not included in the analysis, which eventually consisted of 70 patients. According to BDI-II, depressive symptoms were present in 35.7% of patients, while the diagnosis of major depressive disorder (MDD) was confirmed by the psychiatrist in 25.7%. According to the ROC analysis the optimal cut-off score for diagnosing MDD using BDI-II was ≥13 points.
Conclusions: This study suggests that the regular screening for depressive symptoms, followed by a psychiatric consultation in selected patients, might improve diagnosing depression with the goal of achieving a higher quality of life and a lower mortality rate. It may also be a cost-effective model for the management of depression among the haemodialysis population.
Major depressive disorder (MDD) is a common psychiatric condition, with a twelve-month prevalence of around 5–10% and lifetime prevalence of around 20% (1–3). Among outpatients with general medical disorders the prevalence of depression largely exceeds that in the general population, reaching above 50% in groups with certain conditions (4). Given the burden of symptoms, high numbers of sufferers, and the fact that depression often goes undetected, the development of effective strategies for early identification and management of depression in such populations has become an important goal of clinical research (4).
Kidney diseases are among somatic disorders associated with high levels of depression, in particular in their more advanced chronic stages. Chronic kidney disease (CKD) has become a growing public health problem, with the number of individuals with all-stage CKD reaching almost 700 million and over 3 million patients requiring dialysis in 2017 (5). This number is expected to keep rising over the next decade to reach over 5.4 million by 2030, driven by the aging of population and increasing incidence of diabetes and hypertension (6). Among users of in-centre maintenance haemodialysis (MHD) - the most common form of renal replacement therapy (RRT) (7, 8)-depression is present in up to 40% of patients (9).
Estimates of depression prevalence among MHD users however vary between studies. One possible explanation is that depression may be not accurately diagnosed. This may be related to the presence of overlapping somatic symptoms, or differences in the diagnostic processes, such as assessment techniques, diagnostic tools, definitions and thresholds used (10, 11). It has been shown that the use of self- or clinician-administered questionnaires leads to higher estimations of depression compared with the interview-based diagnosis using Diagnostic and Statistical Manual of Mental Disorders 5 (DMS-5) criteria (12). Inaccurate diagnosing of depression has important clinical implications. Particularly noteworthy is the strong correlation between depression and all-cause mortality risk in patients receiving MHD (13, 14), with affective and cognitive symptoms of depression being a better predictor of long-term mortality than its somatic symptoms (15). Depressive symptoms are also independently associated with dialysis nonadherence, lower health resource utilisation (16) and decreased quality of life (17). Performing routine screening for depression has been recommended by Centres for Medicare and Medicaid Services in the United States (18) and in Kidney Disease Outcomes Quality Initiative (KDOQI) guidelines for cardiovascular disease in dialysis patients (19). Nevertheless, depression screening and integrated management of depression in the dialysis population remain insufficient (20, 21).
In the dialysis centres, where access to psychiatric care is often limited, diagnostic scales are frequently used to screen for depression in end-stage renal disease (ESRD). A number of screening tools have been used, including the Cognitive Depression Index (CDI) (22, 23),, the Center for Epidemiological Studies Depression Scale (CES-D) (24), the Hospital Anxiety and Depression Scale-Depressive Subscale (HADS-D) (25), Geriatric Depression Scale 15 (GDS-15) (26), and Initial Depression Inventory- Maintenance Haemodialysis (ID-MHD) (27). The most commonly used assessment tool has however been the self-administered Beck Depression Inventory, both in its original (BDI) and revised (BDI-second edition, BDI-II) versions (11, 28–31). Only few studies compared the consistency of diagnostic outcomes between different scales and clinical diagnosis made by a psychiatrist using DSM criteria (22, 23, 32, 33). Most of the studies performed in the elderly MHD population (26) suggested that in order for BDI and BDI-II to be valid tools comparable to the clinical interview, a traditional cut-off score of 14 points needed to be replaced by the threshold of 15 points or higher (22, 32, 33). This is mostly related to the impact of depressive somatic symptoms common in the MHD population. Establishing a threshold is crucial for promoting the use of BDI-II as a reliable screening tool. This should have important clinical value as on-dialysis assessments using BDI-II, thanks to the ease of using the scale, could constitute a convenient screenings procedure encouraging regular evaluation during the dialysis session, at a time when patients are easily accessible (22). There are some considerations when assessing patients for depression, especially in the elderly population. An important one is the presence of dementia. Approximately thirty percent of haemodialysis patients suffer from dementia (34, 35), with even higher rates among older patients and those with severe somatic conditions (36). The limitations of the use of self-administered rating scales should be considered in this context. Excluding cognitive impairment before making the diagnosis of depression seems to be of significant importance (37). The purpose of this study was to explore commonly used approaches to diagnosing depression in the context of the real-life setting of the haemodialysis centre, with the view of contributing to the development of practical recommendations for depression assessment in haemodialysis patients. To achieve this, we compared recognition of depression using common approaches, specifically the self-rated questionnaire BDI-II, chosen because it remains an easy-to-administer, commonly used tool in the everyday clinical practice, with psychiatrist led assessment based on DSM-5 criteria. Additionally, individuals with and without depression were compared in terms of sociodemographic and clinical features. Dementia screening using Mini-Mental State Examination (MMSE) (38) and clinical evaluation was conducted in order to exclude its impact on depression screening. The study was designed to reflect the daily operating conditions of the haemodialysis centre.
Adult ESRD patients from two Haemodialysis Centres were enrolled into the study. Individuals over 18 years old, with proper speaking abilities who had been receiving haemodialysis for at least 3 months were recruited consecutively by the medical staff of the dialysis centre. Patients with major psychiatric disorders other than depression, or those with visual or hearing impairments that prevented them performing the tests, were excluded. The study group received the high-flux haemodialysis or hemodiafiltration three times weekly. All participants gave their written informed consent for inclusion. The study was conducted in accordance with the Declaration of Helsinki, and the protocol was approved by the Independent Bioethics Committee for Scientific Research of Medical University of Gdansk.
The study was conducted in two Dialysis Centres in Poland (NZOZ Diaverum Gdańsk and Fresenius Nephrocare Ostróda). All the tests and interviews during the dialysis sessions were performed at least one hour after the initiation and one hour before the termination of the procedure, in order to reduce the risk of intradialysis hypotension impacting cognition. Before performing the depression screening, the MMSE was administered to all the patients by a trained researcher, in order to evaluate their cognitive function. Patients meeting the criteria of moderate or severe dementia (score <19 points) were excluded from the depression evaluation, to avoid the risk of dementia’s impact on their ability to retrospectively assess their mental state. Individuals with mild cognitive impairment (MCI) (24–26 points) and mild dementia (19–23 points) remained in the study, due to the possibility of pseudodementia in the course of MDD. Depression was initially assessed with Beck Depression Inventory II (29). We used a validated version of BDI-II, the language used to collect the data was Polish. The BDI–II is a self-reported, 21-item inventory designed to assess the presence and severity of depressive symptoms. BDI-II assesses symptoms within cognitive, affective and somatic domains. Each item is rated from 0 to 3 points, and the total score ranges from 0 to 63. The score ≥14 points in BDI-II was interpreted as the presence of depressive symptoms. The original authors of the BDI-II recommended the following practical interpretation of their instrument: 0–13 points considered as none to minimal range depression, 14–19 mild depression, 20–28 moderate and 29–63 severe depression (29, 39, 40). All the patients, regardless of the BDI-II score, were subsequently invited for the clinical assessment performed by a senior psychiatrist, experienced in diagnosing MDD and assessing patients with chronic somatic illnesses. The psychiatrist was blind to BDI-II results. The psychiatrists conducted the diagnostic interview based on the DSM-5 criteria (41, 42), and subsequently applied the Montgomery-Asberg Depression Rating Scale (MADRS) to establish the severity of depression (43). MADRS is a standard in monitoring depressive symptoms and has been used in haemodialysis populations in previous studies (44, 45). The psychiatrists additionally used the Clinical Global Impression - Severity scale (CGI-S) to evaluate the severity of depression (46) and the Personal and Social Performance Scale (PSP) (47) to assess psychosocial functioning. The same procedure was followed by all three psychiatrists involved in the study. All the patients diagnosed with depression (regardless of the severity) were offered to remain under psychiatric care.
In one of the centres psychiatrists examined patients within the dialysis setting during the haemodialysis sessions. In the other the psychiatrist was only available in the ambulatory, which meant that patients had to attend a separate session that was scheduled independently of the dialysis treatment. In this centre, none of the patients who filled out the BDI-II questionnaire during their haemodialysis session agreed to the ambulatory clinical evaluation.
The demographic, clinical and laboratory data of the study group were obtained (Tables 1, 2). The severity of comorbidities was scored with the use of Charlson Comorbidity Index (CCI) (48), adjusted for age.
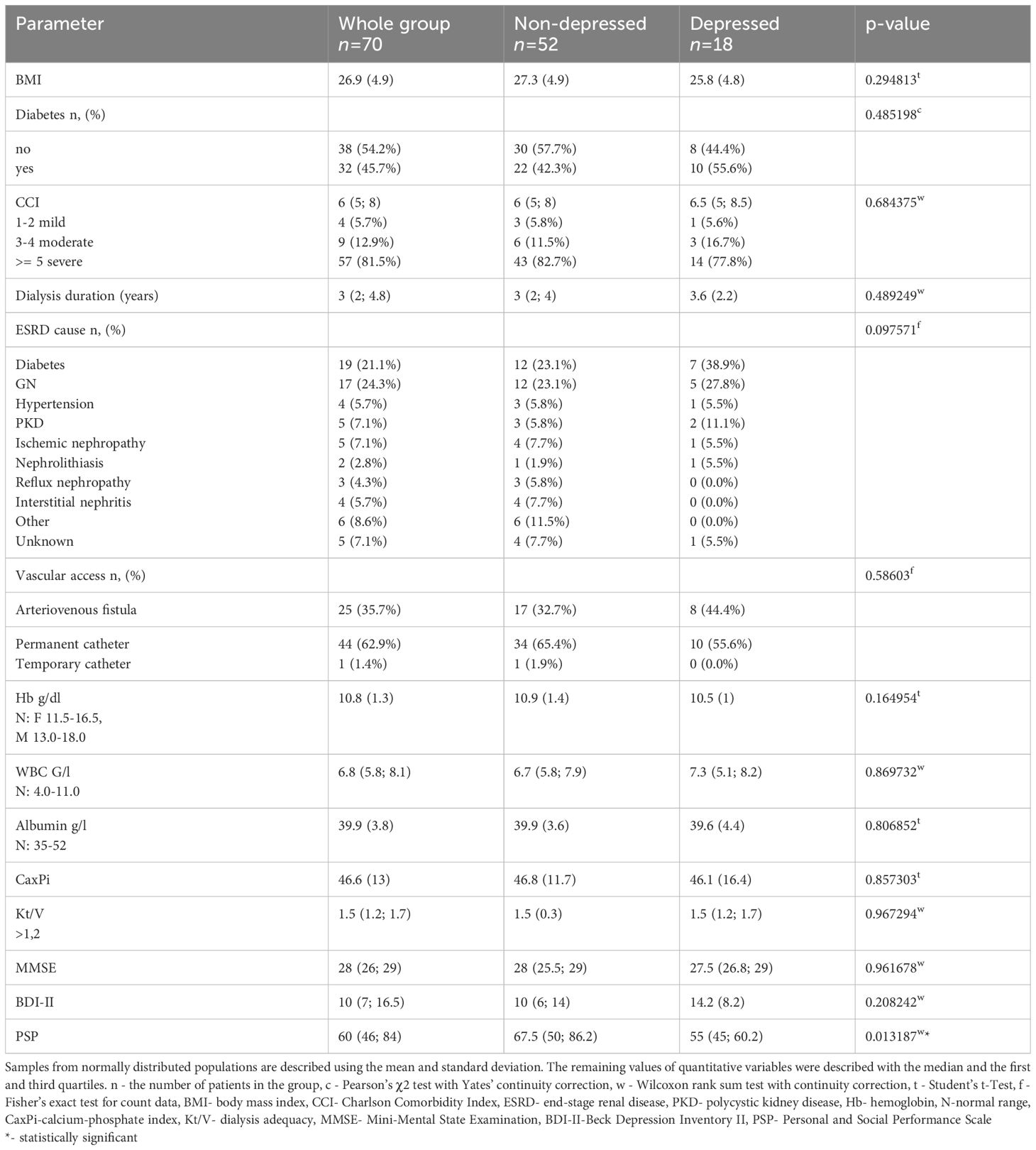
Table 1 Clinical data. Comparison between the non-depressed (MADRS < 10 or CGI < 3) and depressed (DSM-5 criteria, MADRS ≥ 10 and CGI ≥3) patients.
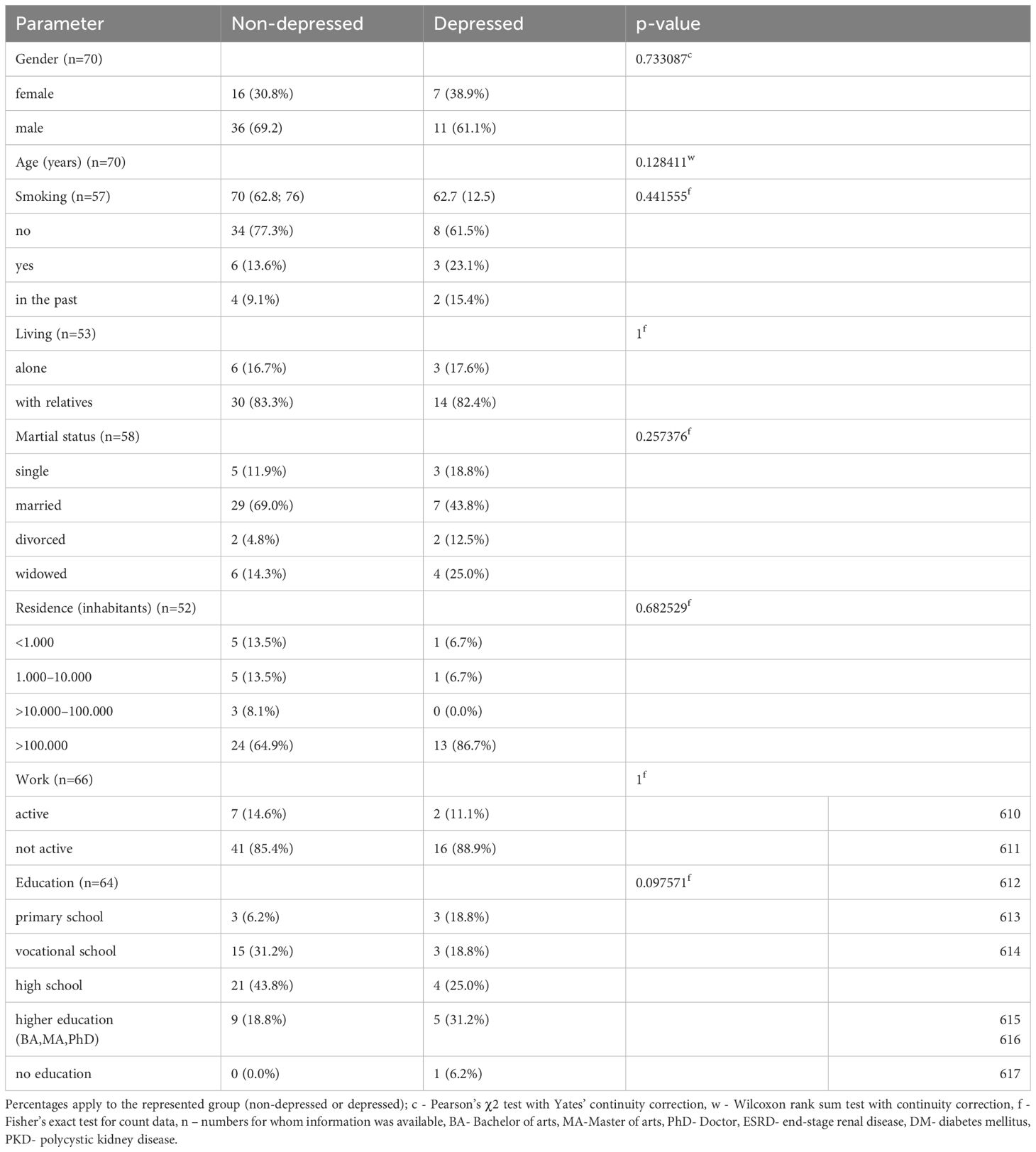
Table 2 Sociodemographic data. Comparison between non-depressed (MADRS < 10 or CGI < 3) and depressed (DSM-5 criteria, MADRS ≥ 10 and CGI ≥3) individuals.
The statistical analysis was performed using the functions and procedures of the R package (49). Differences between both groups of quantitative variables were tested using the Wilcoxon test or Student’s t-test. The appropriate tests (and additional options) were selected depending on the p value of the Shapiro-Wilk test and the homogeneity of the variance test. If the samples came from a normally distributed population, the basic features describing the variables were mean values and standard deviations. In other cases, values are described using the median as well as the first and third quartiles. The Pearson’s χ2 test with Yates’ continuity correction and the Fisher’s exact test for count data were used to test the independence of qualitative variables collected in tables presenting the size of individual groups. The research also used ROC analysis and logistic regression (50). For each of the tests used, the level of significance was set at α = 0.05.
Initially, 136 patients from two Dialysis Centres agreed to participate in the study. Four patients were diagnosed with moderate or severe dementia and were excluded from further evaluation. Patients diagnosed with MCI (14.2% of the whole group), mild dementia (12.9%), and those who did not agree to the MMSE screening (10%), remained in the study. Sixty-two patients (47%) did not agree to participate in some of the study procedures and were excluded from the analysis. Seventy patients (51.5%) who performed all depression evaluations were included in the final analysis. This group consisted of 23 females (32.8%) and 47 males (67.1%). The median age of participants was 69 years.
The numbers of patients with depression diagnosed using BDI-II only, differed from the numbers diagnosed by the psychiatrist using DSM-5 criteria and the scores of MADRS≥10 and CGI ≥3.
Forty-five patients (64.3% of the whole group) had BDI-II score of 0–13, which corresponded to no depression or minimal symptoms. Out of this group, 9 (12.9% of the whole group) were diagnosed with depression by a psychiatrist using the DSM-5 criteria and the scores of MADRS≥10 and CGI ≥3.
Twenty-five patients (35.7% of the whole group) scored ≥14 points on BDI-II, consistent with the cut-off point for depression diagnosis. Of these patients, nine (12.9% of the whole group) were diagnosed with depression by a psychiatrist based on the DSM-5 criteria and scores of MADRS≥10 and CGI ≥3.
In more detail, 13 patients (18.6% of the whole group) had the BDI-II score of 14–19, which corresponded to mild depression. Of these, 4 (5.7% of the whole group) were diagnosed with depression by a psychiatrist based on the DSM-5 criteria and scores of MADRS≥10 and CGI ≥3.
BDI-II criteria for moderate (20–28) and severe (29–63) depression were met by, respectively, 8 patients (11.4% of the whole group) and 4 patients (5.7% of the whole group). Of these, respectively, 4 (5.7% of the whole group) and 1 (1.4% of the whole group) were diagnosed with depression by a psychiatrist based on the DSM-5 criteria and scores of MADRS≥10 and CGI ≥3.
Subsequently, we analysed the differences in qualitative and quantitative data between groups with and without depression based on the diagnosis made by the psychiatrist (depression: DSM-5 criteria, MADRS≥10 and CGI ≥3; no depression: remaining patients). The basic characteristics (sociodemographic and clinical data) for the whole group, as well as depressed and non-depressed subgroups, are presented in Tables 1 and 2.
In the whole group, the most common known primary cause of ESRD was diabetes mellitus (DM) (45.7% of all participants) and glomerulonephritis, followed by hypertension, policystic kidney disease and ischemia. The dominant vascular access was the permanent catheter. The CCI score interpreted as the severe comorbidity was found in 81.5% of participants, while mild comorbidity was found in in 5.7%.
The only statistically significant difference for quantitative variables was observed for the PSP score, which suggests that functioning of depressed and non-depressed patients differs across the dimensions assessed by the scale (socially useful activities, personal and social relationships, self-care, disturbing and aggressive behaviours). There were no statistically significant differences between depressed and non-depressed groups in terms of other quantitative variables, as well as qualitative variables, as shown in Tables 1 and 2 (all p-values >0.05). The number of patients with diabetes mellitus did not differ between groups. We also found no statistically significant differences in the albumin level, body mass index or comorbidity. However, in both groups the average CCI score met the criteria for severe comorbidity.
Using ROC analysis and logistic regression, the possibility of creating a potential tool to determine the absence of depression in dialysis patients based on the BDI-II score variable was examined. For this purpose, a logistic regression model was created, in which the dependent variable was membership of the group (with or without depression), determined using scores on the MADRS and CGI-S scales, as described above. The independent variable was the BDI-II score. Based on the model created in this way, an ROC curve was plotted and the cut-off point for the obtained model was calculated (Figure 1).
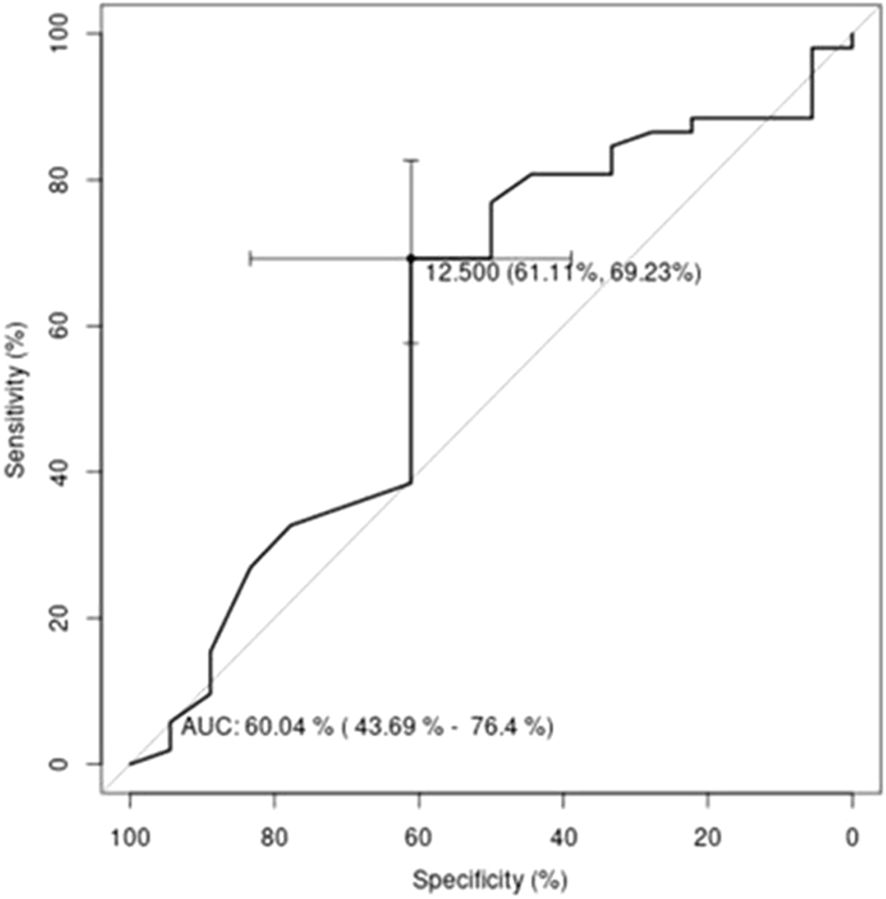
Figure 1 ROC curve for the logistic regression model. The independent variable is the BDI-II score and the dependent variable is membership of the group “no depression” or “depression”.
The cut-off point established for BDI-II was the value dividing patients into two groups. Patients with predicted depression were those with a BDI-II score of 13 or greater and the remaining patients with scores of less than 13 were classified as ‘predicted no depression’. Contingency tables were created on the basis of the groups defined in this way (Table 3).

Table 3 Contingency table for the Beck variable.
The result of the independence test was statistically significant. It indicated that there is a relationship between the groups defined by BDI-II and the groups defined by the MADRS and CGI-S scales. The quality of the classification was assessed by determining values for parameters such as: TPR=69.2% (True Positive Rate - associated with the group “no depression”), TNR=61.1% (True Negative Rate - associated with the group “depression”), PPV=83.7% (Positive Predictive Value) and NPV=40.7% (Negative Predictive Value). In the created model for grouping the values of the BDI-II score variable, only the parameters assessing the classification into the “no depression” group could be considered satisfactory.
In the studied population of patients with ESRD undergoing MHD, 35.7% had BDI-II scores corresponding to mild depression (the cut-off point of 14 points), with 17.1% with scores indicating moderate or severe depression (≥20 points). The number of patients diagnosed with MDD by the psychiatrist using DSM-5 criteria and scores of MADRS≥10 and CGI ≥3 however differed from this, with 25.8% diagnosed with depression. With the exception of PSP score, no statistically significant differences were found in terms of the sociodemographic and clinical features between the depressed and non-depressed patients. In our study, using ROC analysis and logistic regression, the suggested optimal cut-off point for BDI-II, which indicated patients without depression in the clinical evaluation, was 13 points. The compliance rate was low; 47% of the patients, that had agreed to participate in the study, refused to perform some of the proposed tests. MCI and mild dementia were observed in 27.1% of patients.
We used BDI-II as the screening tool as despite its limitations (11, 27), it remains a commonly used measure to explore depressive symptoms in the clinical settings, and this study was designed to reflect the common practices. Using the MADRS scale alone, applied by the psychiatrist, the percentage of individuals with depression reached 35.7%, equal to the number identified in BDI-II screening. These results are comparable with the prevalence of depressive symptoms observed in outpatient populations across different specialties [4]. Psychiatric evaluation attributed diagnosis of MDD based on DSM-5 criteria, with MADRS and CGI scores to assess severity, to 25.8% patients, hence lower than when the scales were used alone. This finding is consistent with previous reports of higher depression rates when self-reported questionnaires were used, compared to the clinical evaluation (12). Such discrepancy may be linked to a number of factors, specific to the researched population. Relevant to our studied population, somatic symptoms may get reported through questionnaires, while in fact they are related to the somatic condition, rather than depression. Indeed, numerous somatic comorbidities were seen in our tested population, and the CCI score indicated severe comorbidity in 81.5% of patients, consistent with the epidemiological data (7). Although the groups with and without depression did not differ in terms of clinical features, people with depression may be more sensitive to somatic problems (for example, it was shown that depression increases sensitivity to pain) (51), which may translate to allocating higher scores to somatic items, whereas a trained psychiatrist may have more clarity whether reported symptoms are related to depression or not. We noted that the number of patients meeting the criteria for depression according to MADRS alone, was equal to the number of patients whose scores on BDI-II indicated depression (35.7% in both cases). At the same time, only 27.8% of patients were diagnosed with depression by the psychiatrist using DSM-5 criteria. This suggests no superiority of clinician applied scales as compared with self-rated scales, and indicates that a full clinical assessment is warranted for a diagnosis. Importantly, this also suggests that some haemodialysis patients whose scores on depression assessment scales, whether self-rated or clinician applied, were indicative of depression, might not in fact have MDD. In such cases, starting depression treatment may be ineffective or even harmful, with the symptoms presented possibly reflecting mild depression, requiring psychological therapy rather than pharmacotherapy. Patients may also be suffering from dementia or yet another mental disorder requiring a different therapeutic approach altogether. The lack of precise diagnostics in the studies on the efficacy of antidepressant treatment in this group of patients may be one of the reasons for the ineffectiveness of therapy, giving false negative results (52).
An intriguing observation was that while BDI-II suggested depression (score ≥14) in a higher number of patients than later confirmed by a psychiatrist, some patients who had scores on BDI-II corresponding to no or minimal depression (≤13), were diagnosed with depression in a psychiatric assessment. This suggests that a psychiatrist may recognise depression based on DSM-5 criteria, when the key symptoms are present, which however may not reach the severity required for the diagnosis using BDI-II. Whether diagnosing patients with such low severity of symptoms is important, for example in the context of offering counselling, is an important questions, however beyond the scope of this study.
Unfortunately, in reality, availability of psychiatric support is low and regular psychiatric assessments in physical health settings are rare. Using a self-rated scale such as BDI-II would help identify patients who could potentially benefit most from a psychiatric assessment, hence focusing the resources available. Therefore, the regular screening using self-administered questionnaires is advisable. BDI-II is easy to perform and can be done while patients are having their haemodialysis session, with no additional burden on their time. The value of performing such a screening cannot be overappreciated. Depression has many adverse effects, from its intrinsic impact on well-being to the worsening of physical health and increased non-compliance with treatments. Therefore its recognition and management are crucial for regular clinical practice and the management of somatic health problems.
According to our results, the optimal cut-off point for BDI-II in diagnosing MDD in the haemodialysis population was equal to or greater than 13 points. It is similar to the one recommended in the general population (i.e. 14 points) (29, 39) and lower compared with cut-off points suggested in the previous studies (22, 32, 33).
Our studied group of patients had high average age and high rate of severe comorbidities. Population aging and increases in comorbidities, observed in patients receiving renal replacement therapy, is in line with changes in the general population. Both have been identified as risk factors for developing depression (7, 53, 54). In both groups the average CCI score suggested severe comorbidity, although with no statistical differences between depressed and non-depressed groups. One such comorbidity, present in the high percentage of patients in our group, was diabetes mellitus. DM is the most common cause of ESRD. Although our study did not identify statistical differences in any of the clinical factors between depressed and non-depressed groups, some of the aspects of somatic health warrant attention. For example, cardiovascular problems are a risk factor for depression, hence an assessment of their indices, especially modifiable ones, is potentially important (55). Phosphate retention is a risk factor for cardiovascular mortality in patients with CKD, and can be potentially modified with diet (56, 57). Although this study did not allow for an assessment of the relationship between adherence to dietary recommendations, which influences phosphate levels, and the occurrence of depressive symptoms, this might be an important practical aspect of future studies. There were no significant between-group differences in other parameters suggested to be associated with future cardiovascular events, such as albumin and haemoglobin levels (57). We have not found statistically significant differences between depressed and non-depressed patients according to Kt/V, used to evaluate haemodialysis adequacy. However, its interpretation as a single parameter has many limitations (58).
One of the reasons for the lack of identification of between-group differences might be the small study sample. Almost half of the recruited patients were lost to the analysis as they refused to perform one or more of the required tests. Our observations of low compliance rate regarding diagnosing depression are consistent with the previous research (59, 60). In our studied population, almost half of the patients who initially gave their written consent to participate, did not agree to follow through with the further psychiatric evaluation. This seemed to be associated with the setup of the assessment. While 84% of patients agreed to a psychiatric assessment provided during their dialysis session, none of the patients followed up with a psychiatric assessment if it was offered in the ambulatory. One possible explanation may be the reluctance to use additional services, considering the time that patients already devote to the regular dialysis procedure. The attitudes to psychiatric assessments may also play a role. Interestingly, none of the patients from the dialysis centre which was in a small town – and incidentally where the assessment was offered in the ambulatory only – agreed to see the psychiatrist. Although not examined in the study, the stigma around psychiatric assessments is still an important issue, and may be more pronounced in particular social contexts. Even if the examination during a dialysis session is challenging given the lack of privacy in the setting where a number of patients share the dialysis room, as well as the noise of regular hospital activities, it seemed to be more acceptable for the patients in our study than when a separate appointment was required.
Therefore, on-dialysis consultations may be recommendable (22).
Our study included dementia screening using MMSE. The percentage of patients diagnosed with MCI or mild dementia was 27.1%. An assessment of cognitive impairments when assessing depression, especially in the elderly populations, is important, as dementia can distort the diagnosis of depression and influence the results of its treatment. At the same time, the results of MMSE have to be considered carefully as higher scores may be related to pseudo-dementia in the course of depression, as well as be related to the conditions of the examination itself. Previous research showed that dialysis patients with greater burdens of depressive symptoms performed worse in cognitive tests related to processing speed and executive function (61). Therefore, individuals who met the criteria of MCI and mild dementia in MMSE were not excluded.
In the real world, the access to a psychiatric assessment in the dialysis setting is very restricted. Employing a psychiatrist full-time is usually not considered cost-effective; examining all the patients would be associated with high costs and an additional pressure on scarce resources. However, given how common depression is in this population of patients, and how big its impact on general health is, an identification of depressed individuals is an important issue. One solution, supported by this study, could be the regular screening for depression using self-reported scales, applied during the dialysis session, in order to identify patients requiring a psychiatric consultation. Our results suggest that this consultation might be best offered during the dialysis session, as shown by differences in accepting an assessment depending on the setting during and outside of the dialysis session. Such models could be more beneficial both for patients and the service providers. Increasing the availability of psychiatric consultations in the dialysis settings for the selected patients, might improve the effectiveness of diagnosing and treating depression in this population, and in turn have an impact on physical health and treatment adherence. The proper screening algorithm might improve the treatment of depression and have an impact on patients’ quality of life as well as compliance with the dialysis recommendations.
One of the study limitations was the small sample size, discussed above. The others were related to the differences between the two settings regarding the place and time of the psychiatric evaluation, which may be the reason why patients from one of the settings refused a psychiatric consultation. Performing the clinical evaluation during the dialysis session might be considered a limitation as well, given a relative lack of privacy and other factors discussed above. However, as our study suggested, in real life, even if such conditions are not ideal, this approach may still be more acceptable for patients than a separate appointment.
The future research on depression screening in the haemodialysis patients leading to the development of the practical recommendations regarding diagnosis and treatment, is an important clinical need. It might also be of importance to explore the correlation between depression and the compliance to the dialysis treatment itself.
This study suggests that, although the psychiatric assessment is considered superior to using depression rating scales, the regular use of self-rated questionnaires to assess depression during haemodialysis sessions may help to identify a subgroup of patients with suspected depression, who would benefit from a psychiatric assessment. This might be a cost-effective model for the management of depression among the haemodialysis population. Performing dementia screening should be taken into consideration before diagnosing depressive disorders. The regular screening for depressive symptoms, followed by a psychiatric consultation in selected patients as a part of regular care in Dialysis Centre, might improve diagnosing depression, with the goal of achieving a higher quality of life, better treatment adherence, and a lower mortality rate.
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
The studies involving humans were approved by Independent Bioethics Committee for Scientific Research of Medical University of Gdansk. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
AK: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Writing – original draft, Writing – review & editing. MR: Formal analysis, Funding acquisition, Supervision, Writing – review & editing. BG: Data curation, Formal analysis, Methodology, Supervision, Validation, Writing – review & editing. PP: Data curation, Formal analysis, Investigation, Writing – review & editing. MP: Conceptualization, Data curation, Investigation, Writing – review & editing. ASK: Data curation, Investigation, Writing – original draft. PW: Data curation, Formal analysis, Methodology, Supervision, Writing – original draft, Writing – review & editing. MB: Data curation, Investigation, Writing – original draft. AM-S: Data curation, Investigation, Writing – original draft. PR: Data curation, Investigation, Supervision, Writing – review & editing. KC: Data curation, Investigation, Writing – review & editing. KB: Data curation, Investigation, Writing – review & editing. JG: Data curation, Formal Analysis, Investigation, Methodology, Supervision, Writing – review & editing.
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. Financial support was received for the publication of this article from the Medical University of Gdańsk.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Thornicroft G, Chatterji S, Evans-Lacko S, Gruber M, Sampson N, Aguilar-Gaxiola S, et al. Undertreatment of people with major depressive disorder in 21 countries. Br J Psychiatry. (2017) 210:119–24. doi: 10.1192/bjp.bp.116.188078
2. GBD 2019 Mental Disorders Collaborators. Global, regional, and national burden of 12 mental disorders in 204 countries and territories, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet Psychiatry. (2022) 9:137–50. doi: 10.1016/S2215-0366(21)00395-3
3. Hasin DS, Sarvet AL, Meyers JL, Saha TD, Ruan WJ, Stohl M, et al. Epidemiology of adult DSM-5 major depressive disorder and its specifiers in the United States. JAMA Psychiatry. (2018) 75:336–46. doi: 10.1001/jamapsychiatry.2017.4602
4. Wang J, Wu X, Lai W, Long E, Zhang X, Li W, et al. Prevalence of depression and depressive symptoms among outpatients: a systematic review and meta-analysis. BMJ Open. (2017) 7:e017173. doi: 10.1136/bmjopen-2017-017173
5. GBD Chronic Kidney Disease Collaboration. Global, regional, and national burden of chronic kidney disease, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. (2020) 395:709–33. doi: 10.1016/S0140-6736(20)30045-3
6. Liyanage T, Ninomiya T, Jha V, Neal B, Patrice HM, Okpechi I, et al. Worldwide access to treatment for end-stage kidney disease: a systematic review. Lancet. (2015) 385:1975–82. doi: 10.1016/S0140-6736(14)61601-9
7. Johansen KL, Chertow GM, Foley RN, Gilbertson DT, Herzog CA, Ishani A, et al. US renal data system 2020 annual data report: epidemiology of kidney disease in the United States. Am J Kidney Dis. (2021) 77:A7–8. doi: 10.1053/j.ajkd.2021.01.002
8. Htay H, Bello AK, Levin A, Lunney M, Osman MA, Ye F, et al. Hemodialysis use and practice patterns: an international survey study. Am J Kidney Dis. (2021) 77:326–335.e1. doi: 10.1053/j.ajkd.2020.05.030
9. Kimmel PL, Fwu CW, Abbott KC, Moxey-Mims MM, Mendley S, Norton JM, et al. Psychiatric illness and mortality in hospitalized ESKD dialysis patients. Clin J Am Soc Nephrol. (2019) 14:1363–71. doi: 10.2215/CJN.14191218
10. Cukor D, Peterson RA, Cohen SD, Kimmel PL. Depression in end-stage renal disease hemodialysis patients. Nat Clin Pract Nephrol. (2006) 2:678–87. doi: 10.1038/ncpneph0359
11. Kondo K, Antick JR, Ayers CK, Kansagara D, Chopra P. Depression screening tools for patients with kidney failure: A systematic review. Clin J Am Soc Nephrol. (2020) 15:1785–95. doi: 10.2215/CJN.05540420
12. Palmer S, Vecchio M, Craig JC, Tonelli M, Johnson DW, Nicolucci A, et al. Prevalence of depression in chronic kidney disease: systematic review and meta-analysis of observational studies. Kidney Int. (2013) 84:179–91. doi: 10.1038/ki.2013.77
13. Farrokhi F, Abedi N, Beyene J, Kurdyak P, Jassal SV. Association between depression and mortality in patients receiving long-term dialysis: a systematic review and meta-analysis. Am J Kidney Dis. (2014) 63:623–35. doi: 10.1053/j.ajkd.2013.08.024
14. Palmer SC, Vecchio M, Craig JC, Tonelli M, Johnson DW, Nicolucci A, et al. Association between depression and death in people with CKD: a meta-analysis of cohort studies. Am J Kidney Dis. (2013) 62:493–505. doi: 10.1053/j.ajkd.2013.02.369
15. Cheng HT, Ho MC, Hung KY. Affective and cognitive rather than somatic symptoms of depression predict 3-year mortality in patients on chronic hemodialysis. Sci Rep. (2018) 8:5868. doi: 10.1038/s41598-018-24267-5
16. Weisbord SD, Mor MK, Sevick MA, Shields AM, Rollman BL, Palevsky PM, et al. Associations of depressive symptoms and pain with dialysis adherence, health resource utilization, and mortality in patients receiving chronic hemodialysis. Clin J Am Soc Nephrol. (2014) 9:1594–602. doi: 10.2215/CJN.00220114
17. Belayev LY, Mor MK, Sevick MA, Shields AM, Rollman BL, Palevsky PM, et al. Longitudinal associations of depressive symptoms and pain with quality of life in patients receiving chronic hemodialysis. Hemodial Int. (2015) 19:216–24. doi: 10.1111/hdi.12247
18. Centers for Medicare & Medicaid Services. ESRD quality incentive program (2018). Available online at: https://www.cms.gov/medicare/quality-initiatives-patient-assessment-instruments/esrdqip/ (Accessed April 5, 2018).
19. K/DOQI Workgroup. K/DOQI clinical practice guidelines for cardiovascular disease in dialysis patients. Am J Kidney Dis. (2005) 45:S1–S153.
20. Hedayati SS, Yalamanchili V, Finkelstein FO. A practical approach to the treatment of depression in patients with chronic kidney disease and end-stage renal disease. Kidney Int. (2012) 81:247–55. doi: 10.1038/ki.2011.358
21. Li Y, Zhu B, Shen J, Miao L. Depression in maintenance hemodialysis patients: What do we need to know? Heliyon. (2023) 9:e19383. doi: 10.1016/j.heliyon.2023.e19383
22. Chilcot J, Wellsted D, Farrington K. Screening for depression while patients dialyse: an evaluation. Nephrol Dial Transplant. (2008) 23:2653–9. doi: 10.1093/ndt/gfn105
23. Bautovich A, Katz I, Loo CK, Harvey SB. Beck Depression Inventory as a screening tool for depression in chronic haemodialysis patients. Australas Psychiatry. (2018) 26:281–4. doi: 10.1177/1039856218758582
24. Fan L, Sarnak MJ, Tighiouart H, Drew DA, Kantor AL, Lou KV, et al. Depression and all-cause mortality in hemodialysis patients. Am J Nephrol. (2014) 40:12–8. doi: 10.1159/000363539
25. Preljevic VT, Østhus TB, Sandvik L, Opjordsmoen S, Nordhus IH, Os I, et al. Screening for anxiety and depression in dialysis patients: comparison of the Hospital Anxiety and Depression Scale and the Beck Depression Inventory. J Psychosom Res. (2012) 73:139–44. doi: 10.1016/j.jpsychores
26. Balogun RA, Turgut F, Balogun SA, Holroyd S, Abdel-Rahman EM. Screening for depression in elderly hemodialysis patients. Nephron Clin Pract. (2011) 118:c72–7. doi: 10.1159/000320037
27. Wang YY, Zhang WW, Feng L, Gao D, Liu C, Zhong L, et al. Development and preliminary validation of a depression assessment tool for maintenance hemodialysis patients. Ther Apher Dial. (2019) 23:49–58. doi: 10.1111/1744-9987.12749
28. Beck AT, Rush AJ, Shaw BF, Emery G. Cognitive therapy of depression. New York: Guilford Press. (1979).
29. Beck AT, Steer RA, Brown GK. Manual for the Beck depression inventory-II. San Antonio, TX: Psychological Corporation (1996). doi: 10.1037/t00742-000
30. Shanmukham B, Varman M, Subbarayan S, Sakthivadivel V, Kaliappan A, Gaur A, et al. Depression in patients on hemodialysis: A dilapidated facet. Cureus. (2022) 14:e29077. doi: 10.7759/cureus.29077
31. Ye W, Wang L, Wang Y, Wang C, Zeng J. Depression and anxiety symptoms among patients receiving maintenance hemodialysis: a single center cross-sectional study. BMC Nephrol. (2022) 23:417. doi: 10.1186/s12882-022-03051-8
32. Grant D, Almond MK, Newnham A, Roberts P, Hutchings A. The Beck Depression Inventory requires modification in scoring before use in a haemodialysis population in the UK. Nephron Clin Pract. (2008) 110:c33–8. doi: 10.1159/000151230
33. Watnick S, Wang PL, Demadura T, Ganzini L. Validation of 2 depression screening tools in dialysis patients. Am J Kidney Dis. (2005) 46:919–24. doi: 10.1053/j.ajkd.2005.08.006
34. Sehgal AR, Grey SF, DeOreo PB, Whitehouse PJ. Prevalence, recognition, and implications of mental impairment among hemodialysis patients. Am J Kidney Dis. (1997) 30:41–9. doi: 10.1016/S0272-6386(97)90563-1
35. Murray AM, Tupper DE, Knopman DS, Gilbertson DT, Pederson SL, Li S, et al. Cognitive impairment in hemodialysis patients is common. Neurology. (2006) 67:216–23. doi: 10.1212/01.wnl.0000225182.15532.40
36. O’Lone E, Connors M, Masson P, Wu S, Kelly PJ, Gillespie D, et al. Cognition in people with end-stage kidney disease treated with hemodialysis: A systematic review and meta-analysis. Am J Kidney Dis. (2016) 67:925–35. doi: 10.1053/j.ajkd.2015.12.028
37. Grabowski J, Kubanek A. A psychiatrist’s view on patient-reported outcomes in patients undergoing hemodialysis. Am J Kidney Dis. (2019) 74:711. doi: 10.1053/j.ajkd.2019.06.015
38. Folstein MF, Folstein SE, McHugh PR. Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res. (1975) 12:189–98. doi: 10.1016/0022-3956(75)90026-6
39. Smarr KL, Keefer AL. Measures of depression and depressive symptoms: Beck Depression Inventory-II (BDI-II), Center for Epidemiologic Studies Depression Scale (CES-D), Geriatric Depression Scale (GDS), Hospital Anxiety and Depression Scale (HADS), and Patient Health Questionnaire-9 (PHQ-9). Arthritis Care Res (Hoboken). (2011) 63 Suppl 11:S454–66. doi: 10.1002/acr.20556
40. Vanheule S, Desmet M, Groenvynck H, Rosseel Y, Fontaine J. The factor structure of the Beck Depression Inventory-II: an evaluation. Assessment. (2008) 15:177–87. doi: 10.1177/1073191107311261
41. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, fifth edition (DSM-5). Arlington, VA: American Psychiatric Association (2013). doi: 10.1176/appi.books.9780890425596
42. Regier DA, Kuhl EA, Kupfer DJ. The DSM-5: Classification and criteria changes. World Psychiatry. (2013) 12:92–8. doi: 10.1002/wps.20050
43. Montgomery SA, Asberg M. A new depression scale designed to be sensitive to change. Br J Psychiatry. (1979) 134:382–9. doi: 10.1192/bjp.134.4.382
44. Blumenfield M, Levy NB, Spinowitz B, Charytan C, Beasley CM Jr, Dubey AK, et al. Fluoxetine in depressed patients on dialysis. Int J Psychiatry Med. (1997) 27:71–80. doi: 10.2190/WQ33-M54T-XN7L-V8MX
45. Friedli K, Guirguis A, Almond M, Day C, Chilcot J, Da Silva-Gane M, et al. Sertraline versus placebo in patients with major depressive disorder undergoing hemodialysis: A randomized, controlled feasibility trial. Clin J Am Soc Nephrol. (2017) 12:280–6. doi: 10.2215/CJN.02120216
46. Busner J. Targum SD The clinical global impressions scale: applying a research tool in clinical practice. Psychiatry (Edgmont). (2007) 4:28–37.
47. Morosini PL, Magliano L, Brambilla L, Ugolini S, Pioli R. Development, reliability and acceptability of a new version of the DSM-IV Social and Occupational Functioning Assessment Scale (SOFAS) to assess routine social functioning. Acta Psychiatr Scand. (2000) 101:323–9.
48. Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. (1987) 40:373–83. doi: 10.1016/0021-9681(87)90171-8
49. R Core Team. R: A language and environment for statistical computing. Vienna, Austria: R Foundation for Statistical Computing (2021). Available at: https://www.R-project.org/.
50. Robin X, Turck N, Hainard A, Tiberti N, Lisacek F, Sanchez JC, et al. pROC: an open-source package for R and S+ to analyze and compare ROC curves. BMC Bioinf. (2011) 12:77. doi: 10.1186/1471-2105-12-77
51. Michaelides A, Zis P. Depression, anxiety and acute pain: links and management challenges. Postgrad Med. (2019) 131:438–44. doi: 10.1080/00325481.2019.1663705
52. Palmer SC, Natale P, Ruospo M, Saglimbene VM, Rabindranath KS, Craig JC, et al. Antidepressants for treating depression in adults with end-stage kidney disease treated with dialysis. Cochrane Database Syst Rev. (2016) 2016:CD004541. doi: 10.1002/14651858.CD004541.pub3
53. Alencar SBV, de Lima FM, Dias LDA, Dias VDA, Lessa AC, Bezerra JM, et al. Depression and quality of life in older adults on hemodialysis. Braz J Psychiatry. (2020) 42:195–200. doi: 10.1590/1516-4446-2018-0345
54. Khan A, Khan AH, Adnan AS, Sulaiman SAS, Mushtaq S. Prevalence and predictors of depression among hemodialysis patients: a prospective follow-up study. BMC Public Health. (2019) 19:531. doi: 10.1186/s12889-019-6796-z
55. Krittanawong C, Maitra NS, Qadeer YK, Wang Z, Fogg S, Storch EA, et al. Association of depression and cardiovascular disease. Am J Med. (2023) 136:881–95. doi: 10.1016/j.amjmed.2023.04.036
56. Lopes MB, Karaboyas A, Bieber B, Pisoni RL, Walpen S, Fukagawa M, et al. Impact of longer term phosphorus control on cardiovascular mortality in hemodialysis patients using an area under the curve approach: results from the DOPPS. Nephrol Dial Transplant. (2020) 35:1794–801. doi: 10.1093/ndt/gfaa054
57. Major RW, Cheng MRI, Grant RA, Shantikumar S, Xu G, Oozeerally I, et al. Cardiovascular disease risk factors in chronic kidney disease: A systematic review and meta-analysis. PloS One. (2018) 13:e0192895. doi: 10.1371/journal.pone.0192895
58. Jones CB, Bargman JM. Should we look beyond Kt/V urea in assessing dialysis adequacy? Semin Dial. (2018) 31:420–9. doi: 10.1111/sdi.12684
59. Kugler C, Vlaminck H, Haverich A, Maes B. Nonadherence with diet and fluid restrictions among adults having hemodialysis. J Nurs Scholarsh. (2005) 37:25–9. doi: 10.1111/j.1547-5069.2005.00009.x
60. Ghimire S, Castelino RL, Lioufas NM, Peterson GM, Zaidi ST. Nonadherence to medication therapy in haemodialysis patients: A systematic review. PloS One. (2015) 10:e0144119. doi: 10.1371/journal.pone.0144119
Keywords: depression, screening, haemodialysis, compliance, dementia, BDI-II, MADRS
Citation: Kubanek A, Renke M, Godlewska BR, Paul P, Przybylak M, Kowalska AS, Wąż P, Błaszczyk M, Macul-Sanewska A, Rutkowski P, Czarnacka K, Bednarski K and Grabowski J (2024) Screening for depression in chronic haemodialysis patients as a part of care in dialysis setting: a cross-sectional study. Front. Psychiatry 15:1410252. doi: 10.3389/fpsyt.2024.1410252
Received: 31 March 2024; Accepted: 18 June 2024;
Published: 23 July 2024.
Edited by:
Ali Saffet Gonul, Ege University, TürkiyeReviewed by:
Eilean Rathinasamy Lazarus, Sultan Qaboos University, OmanCopyright © 2024 Kubanek, Renke, Godlewska, Paul, Przybylak, Kowalska, Wąż, Błaszczyk, Macul-Sanewska, Rutkowski, Czarnacka, Bednarski and Grabowski. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Alicja Kubanek, YWt1YmFuZWtAZ3VtZWQuZWR1LnBs
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.