 Alicja Jeżuchowska1
Alicja Jeżuchowska1 Daria Schneider-Matyka2
Daria Schneider-Matyka2 Kamila Rachubińska2Artur Reginia3
Kamila Rachubińska2Artur Reginia3 Mariusz Panczyk4Dorota Ćwiek5
Mariusz Panczyk4Dorota Ćwiek5 Elżbieta Grochans2
Elżbieta Grochans2 Anna Maria Cybulska2*
Anna Maria Cybulska2*- 1Department of Clinical Nursing, Faculty of Health Sciences, Wroclaw Medical University, Wroclaw, Poland
- 2Department of Nursing, Faculty of Health Sciences, Pomeranian Medical University in Szczecin, Szczecin, Poland
- 3Department of Psychiatry, Pomeranian Medical University, Szczecin, Poland
- 4Department of Education and Research in Health Sciences, Faculty of Health Sciences, Medical University of Warsaw, Warsaw, Poland
- 5Department of Obstetrics and Pathology of Pregnancy, Pomeranian Medical University in Szczecin, Szczecin, Poland
Introduction: Non-adherence to treatment recommendations is a significant problem, as it contributes to the progression of the disease and to the exacerbation of distressing symptoms. Failure to cope with the disease and elevated levels of stress, in turn, influence the choice of strategy for coping with a difficult situation, and thus adherence to recommendations.
Objectives: The purpose of our study was to evaluate the impact of the subjects’ stress coping styles on therapeutic adherence, life satisfaction, disease acceptance and quality of life (QoL) in people with mood disorders.
Methods: This survey-based study included 102 respondents diagnosed with mood disorders, living in the West Pomeranian Voivodeship. It was performed using the sociodemographic questionnaire and standardized tools: The Coping Inventory for Stressful Situations (CISS), The Satisfaction with Life Scale (SWLS), The Short Form-36 (SF-36) Health Survey, The Adherence to Refills and Medication Scale (ARMS), and The Acceptance of Illness Scale (AIS).
Results: Some 47.06% of the respondents suffered from depressive disorders, while 34.31% had depression or mixed anxiety disorder. Patients who made greater use of an emotion-focused style were found to have significantly lower life satisfaction than other patients. Moreover, this style was related to such SF-36 domains as general health, social functioning, role emotional, vitality, and mental health, as well as to physical component summary (PCS) and mental component summary (MCS).
Conclusion: Treatment non-adherence is a serious challenge in the treatment of patients with mood disorders. Individuals who do not adequately follow treatment recommendations often resort to alternative activities as a mechanism for coping with difficult situations. Patients who predominantly adopt an emotion-oriented coping style tend to experience lower life satisfaction and greater difficulty accepting their condition compared to their peers. Conversely, patients who adopt a task-oriented coping style report better quality of life than those who rely on emotion-oriented coping or alternative activities.
1 Introduction
Mental disorders constitute a global public health challenge, with almost 450 million people suffering from them worldwide (1). Mood disorders are among the most prevalent and debilitating mental conditions affecting world population. They are the second most common category of mental disorders after anxiety disorders, and contribute to an increase in mortality among those affected (2). Mental disorders affect individuals’ current functioning, as well as their quality of life (QoL) and life satisfaction (3). The symptomatology of mood disorders is very rich and varied. Individual symptoms occur with different frequency. Primary symptoms include depressed mood, a lack of energy, objectively visible psychomotor retardation, anhedonia, and a lack of self-esteem (4). Mental disorders are related to individual factors, as well as social support, culture, social protection, standard of living, and other environmental issues (5). Therefore, treatment adherence is important, but a challenge in treating serious mental disorders (6).
Adherence to treatment recommendations is defined as the patient’s acceptance of and compliance with basic health and treatment suggestions; this definition covers various aspects, such as access to treatment, taking medications, and understanding further advice (7–9). The WHO defines medication non-adherence as “a case in which a person’s behavior while taking medication does not conform to the established recommendations of medical personnel” (10). The term “treatment adherence” is therefore broader than “medication adherence”, which refers only to prescribed medications. A review of the literature indicates that treatment adherence is difficult to achieve, and is an obstacle to achieving good clinical outcomes in people with severe mental disorders (11). Patients with serious psychiatric problems are most likely to fail to adhere to medication due to poor reasoning and lack of knowledge about their illness and treatment (8, 12, 13). In turn, non-compliance with taking psychotropic drugs can lead to exacerbation of the disease, reduce the effectiveness of treatment or make the patient less amenable to subsequent treatment. Other consequences include: rehospitalization, worse QoL, recurrence of symptoms, and increased suicide rates (14–16). Since non-adherence is recognized to elevate the risk of unfavorable clinical outcomes, patient-specific non-adherence risk should be evaluated, and individuals at high risk for non-adherence should be closely monitored (17). However, it should be mentioned that some researchers have not found a direct positive effect of medication adherence on the functioning of patients with mood disorders (18).
Stress coping involves cognitive and behavioral strategies used by people facing stressful situations and life events (19). The choice of stress coping strategies has an impact on how patients perceive the symptoms they experience, and how they deal with them. Coping can be defined as thoughts and behaviors that are used to handle internal and external demands of situations perceived as stressful (20). A review of the literature indicates that coping styles are closely related to an individual’s health, and is a mechanism in between stress and disease. If patients’ coping is not effective and properly managed, it may have a negative impact on both their QoL and mental state (21). Active coping strategies have been shown to improve psychosocial functioning, while maladaptive strategies (e.g. pondering on negative states) have been linked to increased depression (22). Apart from influencing the course of the disease, various coping strategies (e.g., low levels of acceptance and high levels of denial) are associated with poor adherence to treatment recommendations (23). Denial is defined as a lack of belief in the existence of a stressor or an attempt to recognize the stressor as untrue, while acceptance is the awareness that a given stressful situation is real and should be dealt with (24). Acceptance is associated with many benefits, for example it makes it easier to cope with the disease and is a key predictor of recovery (24, 25). A review of the literature indicates that patients with mood disorders tend to use maladaptive or emotion-oriented strategies (26), which may affect their QoL, perception of their own illness, and adherence to treatment recommendations.
According to recent reports, so far no factors have been identified that affect treatment adherence among patients with mood disorders. There are a number of potential variables that may affect adherence to treatment recommendations. These may be related to the patient (socioeconomic characteristics, perceptions, beliefs), the doctor (doctor-patient relationship), the treatment (efficacy, side effects, drug dose, number of pills, number of medications), and the type of disorder (severity of illness). Each of these risk factors can affect adherence and interact with other factors. Therefore, it is important to examine the variables that increase or decrease adherence. The main objective of our study was to assess the impact of the subjects’ stress coping styles on their therapeutic adherence, life satisfaction, disease acceptance, and QoL.
2 Materials and methods
2.1 Settings and design
The study recruited 150 people diagnosed with mood disorders, living in the West Pomeranian Voivodeship. The inclusion criteria were: age over 18, confirmed clinical mood disorders (depression, bipolar disorder, depressive disorder, and mixed anxiety disorder), consent to participate in the study, and completion of the entire questionnaire. The exclusion criteria were: age below 18 years, lack of consent to participate in the study, no mood disorders, and failure to complete the entire questionnaire.
The study was conducted in accordance with the Declaration of Helsinki after obtaining approval from the Bioethics Committee of the Pomeranian Medical University in Szczecin (KB-0012/153/17). It is part of a larger project that aims to identify factors affecting treatment adherence, life satisfaction, acceptance of the disease, and QoL in people with mood disorders.
This survey-based study was performed using a questionnaire technique, and the traditional method of distributing paper copies of the questionnaires was employed. After obtaining approval for the study, the previously prepared questionnaires were administered to individuals. The respondents were informed about the study’s objectives and the opportunity to ask questions and receive comprehensive answers. They also learned that participation in the study was anonymous and that they could opt out at any stage. Then, they provided consent to take part in the project. Ultimately, 102 people (68%) were included.
2.2 Research tools
Data collection was carried out using the sociodemographic questionnaire containing a series of questions on basic sociodemographic data (age, sex, marital status, education, place of residence, employment status), and medical data (type of disorder, duration of illness, time of taking medications, number of medications used, awareness of the need to attend medical appointments). Additionally, the following standardized research tools were applied:
• The Coping Inventory for Stressful Situations (CISS) is a 48-item self-report questionnaire that measures three types of stress coping strategies, namely: task-oriented coping (TOC), emotion-oriented coping (EOC), and avoidance-oriented coping (AOC). The last of these styles takes two forms: distraction (engaging in alternative activities), and social diversion (seeking social contact). The results are converted into sten norms, with 1-3 sten scores regarded as low results, 4-7 sten scores—average results, and 8-10 sten scores—high results. Higher scores indicate increased utilization of a specific coping strategy. The value of Cronbach’s alpha ranges from 0.7 to 0.88 depending on the subscale (27, 28).
• The Satisfaction with Life Scale (SWLS)―is a tool that assesses the level of satisfaction with life. It contains 5 statements rated on a seven-point Likert scale, where 1 means I strongly disagree, and 7―I strongly agree. The total score ranges from 5-35 points― the higher the score, the higher the satisfaction with life. When interpreting the results, reference should be made to the sten norms: 1-4 sten―low score, 5-6 sten―average score, 7-10 sten―high score. The value of Cronbach’s alpha was 0.87 (29).
• The Short Form-36 (SF-36) Health Survey is one of the most frequently used health-related quality of life (HRQoL) measures. It consists of 35 items divided into eight health domains, namely: physical function (PF) (10 items), role physical (RP) (4 items), bodily pain (BP) (2 items), general health (GH) (5 items), vitality (VT) (4 items), social functioning (SF) (2 items), role emotional (RE) (3 items), and mental health (MH) (5 items). Some items are rated on a 3-point scale, while others on a 5-point scale. The domains can be combined into two summary measures:
• physical component summary (PCS)—calculated as the sum of PF, RP, BP, and GH scores,
• mental component summary (MCS)—calculated as the sum of RE, SF, MH, and VT scores.
• The 36th item—self-reported health transition (HT)—asks about health change, and does not contribute to the domain or summary scores.
• The quality of life index is the sum of points obtained in all eight scales, and reflects the overall HRQoL. The possible scores range from 0 to 100—the higher the score, the better the QoL (30).
• The Adherence to Refills and Medication Scale (ARMS) consists of 12 questions divided into two subscales: the first 8 questions are about medication adherence, and the next 4 questions are about prescription adherence. Each answer is scored on a 4-point Likert scale, where 1 = never, and 4 = most of the time. The total score reflects the general level of adherence, with a low score indicating better adherence to the recommendations (31).
• The Acceptance of Illness Scale (AIS) is used to assess the degree of acceptance of a disease―the greater the acceptance, the better the adaptation and the lesser the psychological discomfort. The AIS contains eight statements rated on a five-point Likert scale, where 1 denotes poor adaptation to a disease, and 5 its full acceptance. Low scores (0–29) indicate a lack of acceptance and poor adaptation to a disease, and strong mental discomfort. High scores (35–40) indicate acceptance of the disease, manifesting as a lack of negative emotions associated with it. The total score is a sum of all points, and can range from 8 to 40, reflecting the overall degree of acceptance of the disease (32).
2.4 Statistical analysis
Quantitative and categorical variables were characterized using descriptive statistics methods. For quantitative variables, we determined: measures of central tendency (M—mean, Mdn—median), measures of variability (SD—standard deviation, IQR/2— interquartile range, CV—coefficient of variation). For categorical variables, measures of structure were determined: number (n) and frequency (%). The results of standardized psychometric measurements were calculated in accordance with the principles described by their creators, and transformed into a sten scale using norms for the Polish general population.
Classical statistics based on null hypothesis testing was used for statistical inference. The effects of selected sociodemographic and medical variables, the severity of depression symptoms, ways of coping with stress, and selected personality traits on life satisfaction (according to the SWLS), QoL (according to the SF-36), adherence (according to the ARMS) and acceptance of the disease (according to the AIS) were analyzed using regression models. Multivariate linear regression models with least-squares parameter estimation were tested. The multicollinearity of independent variables was checked by determining the tolerance coefficient to avoid model redundancy.
Categorical variables were coded using a sigma-constraint method (quasi-experimental). All predictors were entered into the model simultaneously. Stepwise progressive introduction of predictors was used to build a model of determinants that explained the variance of the dependent variable to the greatest extent. The degree of overall explained variance of the dependent variable was estimated by determining the adjusted R2 value. For each predictor, the unstandardized (b) and standardized (βstand.) regression coefficients along with the 95% confidence interval (95% CI) were determined.
A default statistical significance level of 0.05 was assumed for all analyses. Calculations were performed using the Statistica v. 13.3 software (TIBCO Software Inc., Palo Alto, California, USA).
3 Results
3.1 Brief characteristics of the respondents
The study included 102 respondents diagnosed with mood disorders, the majority of whom were women (91.18%), people in a relationship (64.71%), those living in cities with over 100,000 inhabitants (48.04%), and those employed (59.80%). Some 47.06% of the respondents suffered from depressive disorders, while 34.31% had depression or mixed anxiety disorder. The remaining respondents had bipolar disorder (11.76%) or other types of disorders (6.86%). The duration of the disorder ranged from 1 to 36 years (Me = 7 years) (Table 1).
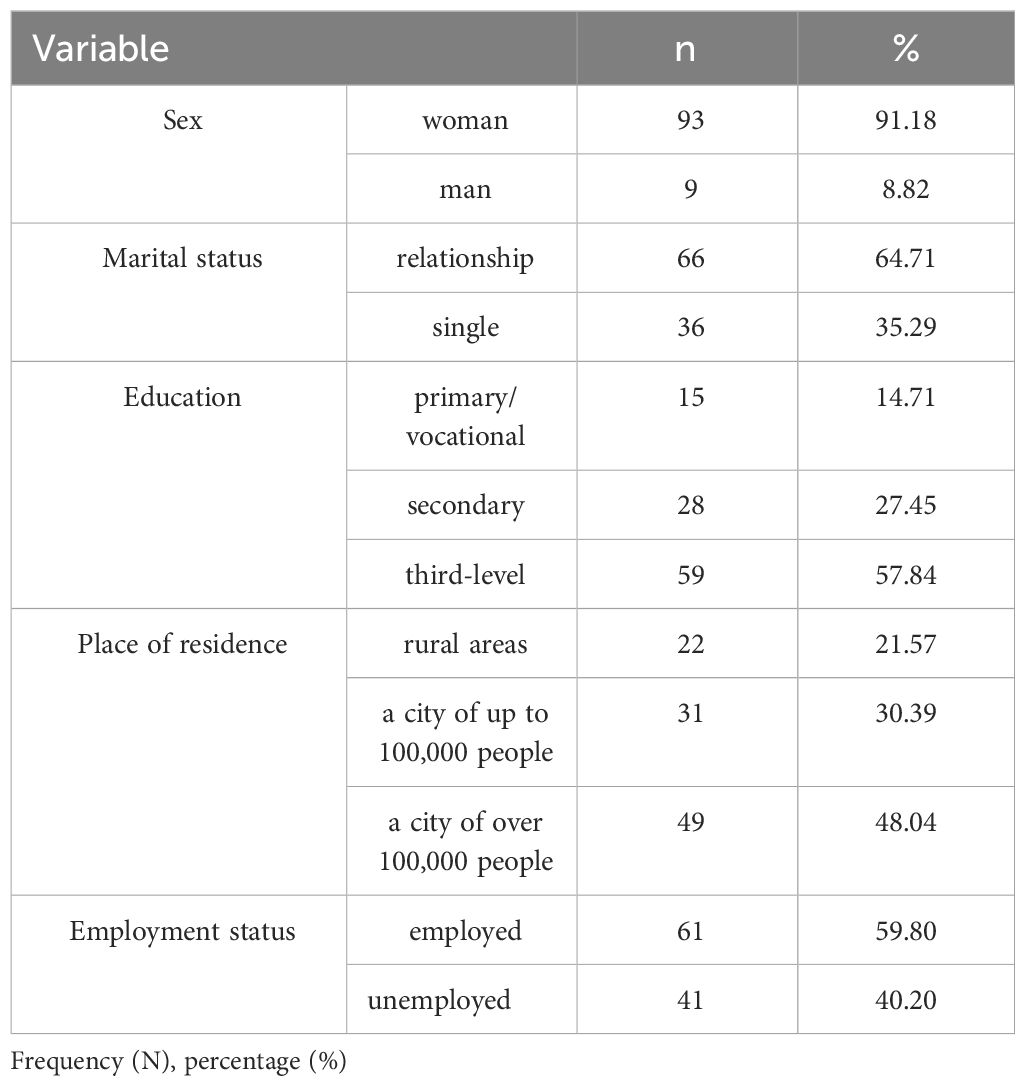
Table 1 Characteristics of the study group by sociodemographic status.
3.2 Analysis of variable values
The study analyzed stress coping styles according to the CISS, life satisfaction according to the SWLS, QoL according to the SF-36, adherence according to the ARMS, and acceptance of the disease according to the AIS.
Table 2 shows the ways of coping with stress according to the CISS. Based on the collected data, it was shown that the subjects obtained the lowest average score for task-oriented coping (TOC) and the highest for avoidance-oriented coping (EOC). For life satisfaction (SWLS), adherence (ARMS), and acceptance of illness (AIS), the respondents scored 15.8 points, 19.13 points, and 23.47 points, respectively.
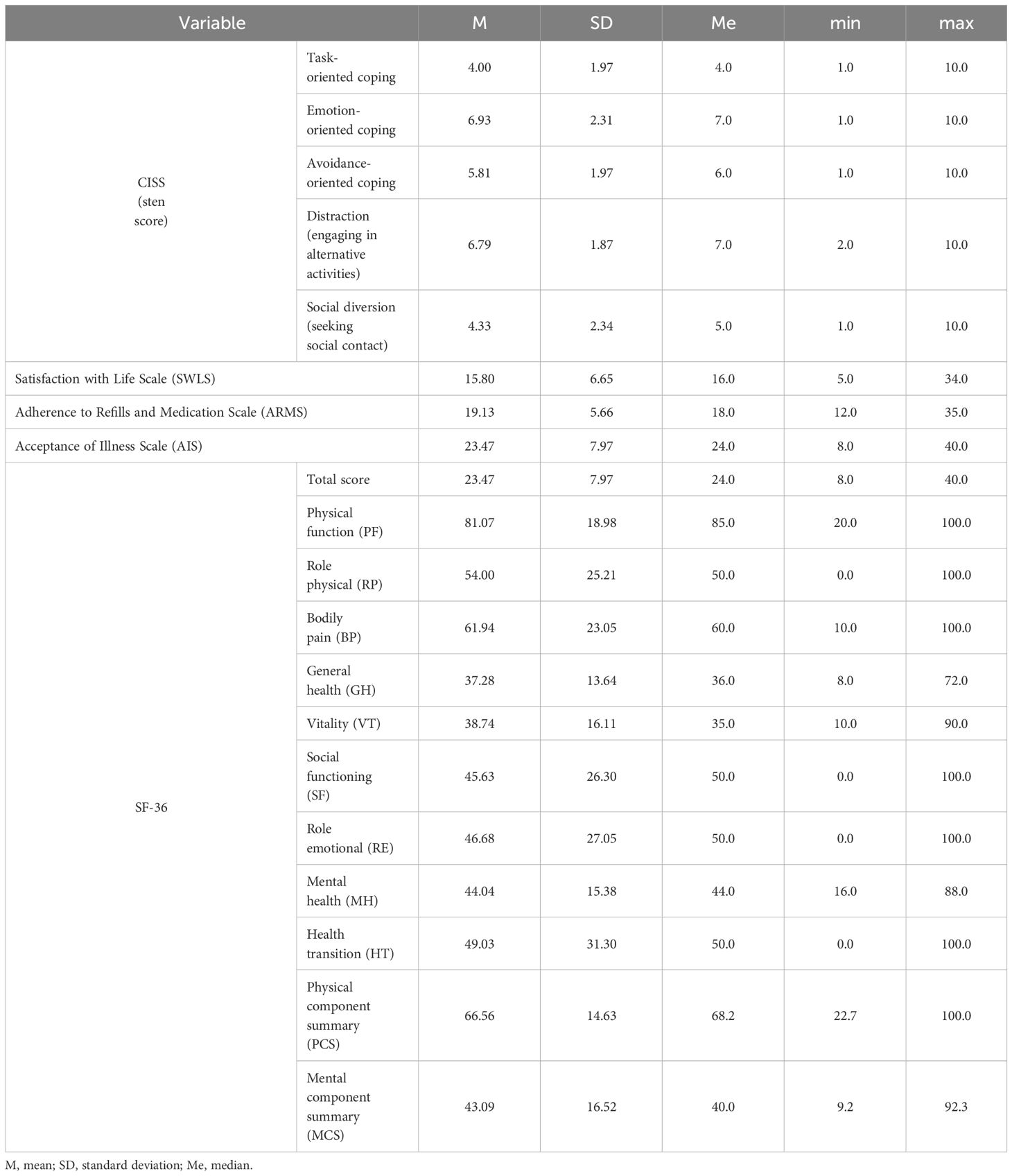
Table 2 The subjects’ stress coping styles according to the CISS, life satisfaction according to the SWLS, adherence according to the ARMS, acceptance of illness according to the AIS, and QoL according to the SF-36.
The highest average QoL scores (SF-36) were obtained for the domains of physical function (PF) (81.07 points) and bodily pain (BP) (61.94 points), and for physical component summary (PCS) (66.56 points). The lowest average QoL scores were achieved for vitality (VT) (38.74 points) and general health (GH) (37.28 points) (Table 2).
The study analyzed the impact of stress coping styles according to the CISS on selected variables such as life satisfaction according to the SWLS, adherence according to the ARMS, and acceptance of illness according to the AIS.
Based on the results, it was observed that life satisfaction according to the SWLS was only affected by emotion-oriented coping. Patients using this style of coping with stress to a greater extent were characterized by significantly lower life satisfaction than other patients (βstd. = -0.445, p < 0.001). There were no statistically significant relationships between the other stress coping styles according to the CISS and life satisfaction (Table 3).
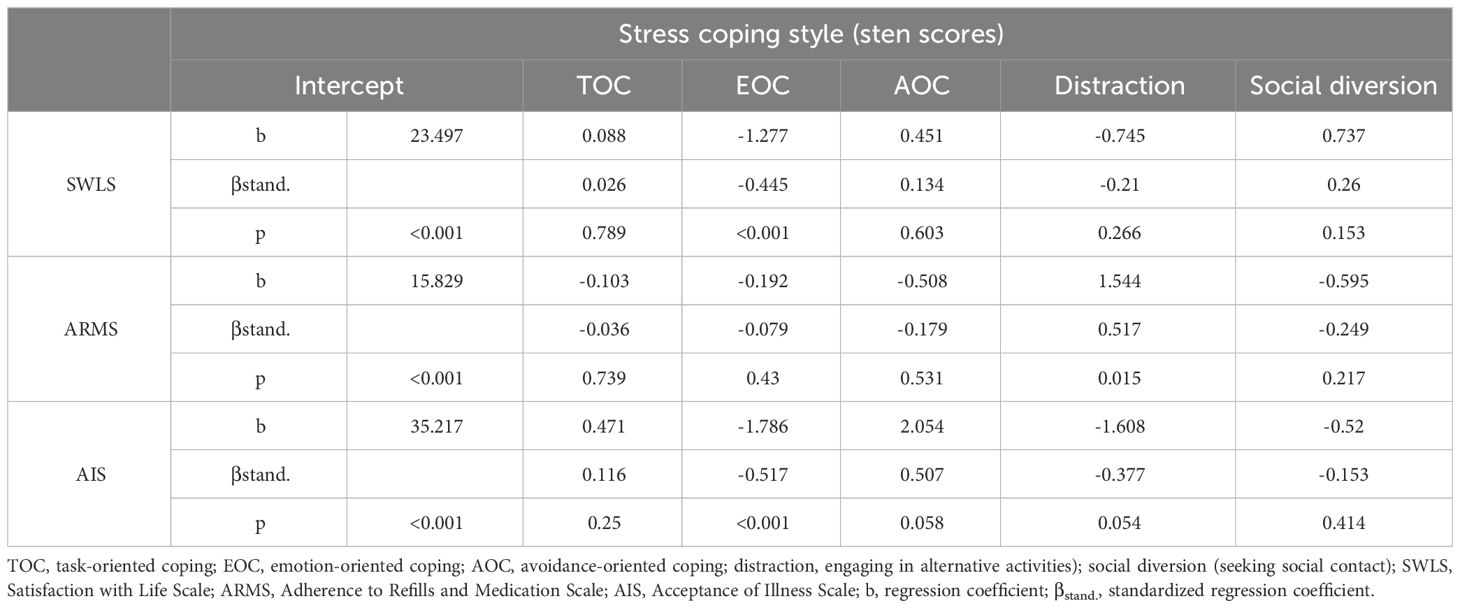
Table 3 The effect of a stress coping style according to the CISS on the variables studied.
The stress coping style in the form of distraction (engaging in alternative activities) was found to significantly affect the level of adherence in chronic diseases according to the ARMS. Patients who used this style to a greater extent scored significantly higher on the adherence scale (worse adherence to therapeutic recommendations) than the rest of the respondents (βstd. = 0.517, p = 0.015). There were no statistically significant relationships between the other stress coping styles according to the CISS and the level of adherence (Table 3).
Based on the collected data, emotion-oriented coping had a statistically significant impact on the level of illness acceptance according to the AIS. Patients who used this style to a greater extent were characterized by significantly worse acceptance of the disease than the rest of the respondents (βstd. = -0.517, p < 0.001). There were no statistically significant relationships between the other stress coping styles according to the CISS and acceptance of the disease (Table 3).
The study analyzed the impact of a stress coping style according to the CISS on QoL according to the SF-36.
Task-oriented coping was found to have an impact on QoL. It was related to the domains of role physical (RP) (βstd. = 0.237, p = 0.042) and mental health (MH) (βstd. = 0.287, p = 0.001), as well as to physical component summary (PCS) (βstd. = 0.228, p = 0.042) and mental component summary (MCS) (βstd. = 0.188, p = 0.034). There were no statistically significant relationships with the other SF-36 domains (Table 4).
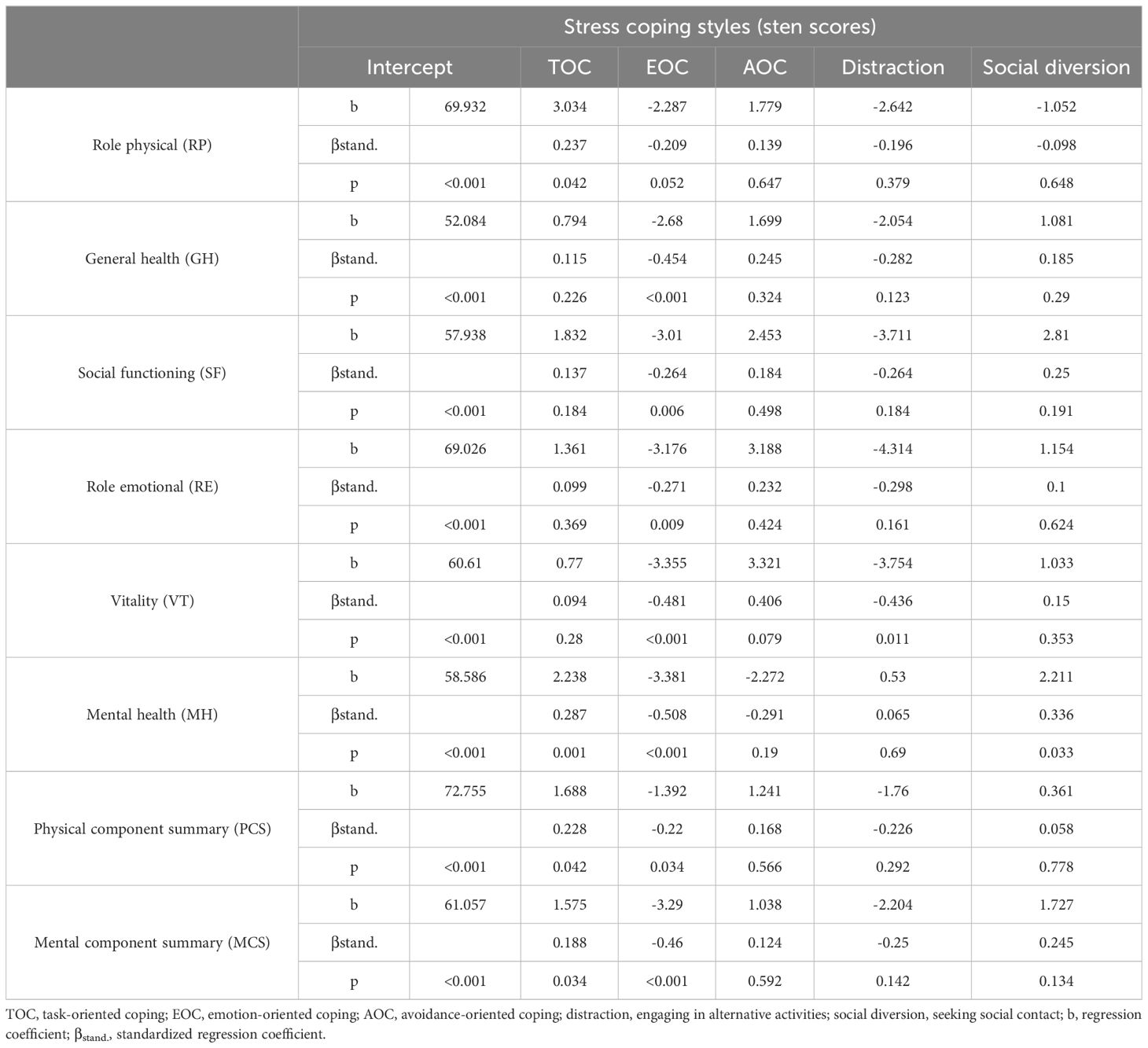
Table 4 The impact of a stress coping style according to the CISS on QoL according to the SF 36.
The results of the study showed that QoL was also affected by an emotion-oriented coping style. This style was linked to the domains of general health (GH) (βstd. = -0.454, p < 0.001), social functioning (SF) (βstd. = -0.264, p = 0.006), role emotional (RE) (βstd. = -0.271, p = 0.009), vitality (VT) (βstd. = -0.481, p < 0.001), and mental health (MH) (βstd. = -0.508, p < 0.001), as well as to physical component summary (PCS) (βstd. = -0.220, p = 0.034) and mental component summary (MCS) (βstd. = -0.460, p < 0.001). There were no statistically significant relationships with the other SF-36 domains.
Distraction (engaging in alternative activities) had an impact on vitality (VT) (βstd. = -0.436, p = 0.011). Respondents who made greater use of this coping style had a significantly lower QoL than those who made less use of it. There were no statistically significant relationships between engaging in alternative activities and the other SF-36 domains.
Social diversion (seeking social contact) had an impact on mental health (MH) (βstd. = 0.336, p = 0.033). Patients who made greater use of this style had significantly higher QoL than those who used it to a lesser extent (Table 4). There were no statistically significant relationships between seeking social contact and the other SF-36 domains.
Avoidance-oriented coping had no statistically significant effect on any of the SF-36 domains (Table 4).
4 Discussion
Once an accurate diagnosis is provided and appropriate medications are prescribed, treatment adherence plays an important role in achieving good health outcomes and maintaining good quality of life in patients with mood disorders. Non-adherence is a barrier to effective treatment.
A review of the literature indicates that there are few publications on the effects of stress coping styles on treatment adherence, life satisfaction, acceptance of a disease, and QoL among people with mood disorders. Our study is probably the first to assess the impact of stress coping styles on psychological variables in this population.
In our study, the main stress coping style significantly affecting the examined psychological variables was emotion-oriented coping. It was found to influence acceptance of a disease, QoL, and life satisfaction. Patients who made greater use of this style were characterized by significantly lower acceptance of the disease and lower life satisfaction. Poor QoL was mainly noted in the dimensions of general health (GH), social functioning (SF), role emotional (RE), vitality (VT), mental health (MH), and physical function (PF), as well as in physical component summary (PCS) and mental component summary (MCS). We also observed that distraction (engaging in alternative activities) had a significant effect on vitality (VT) and adherence in chronic diseases. Patients who used this style to a greater extent achieved substantially higher scores for adherence, and had significantly lower QoL in the vitality (VT) domain than the rest of the respondents. Task-oriented coping affected the domains of role physical (RP), mental health (MH), as well as physical component summary (PCS) and mental component summary (MCS). Seeking social contact, on the other hand, is related to the domain of mental health (MH).
A study by Szeliga-Lewinska and Landowki showed that people from the clinical group were characterized mainly by an emotion-oriented style, while the general population more often used task-oriented coping. In terms of personality traits, people with depression had higher levels of neuroticism, while the level of extraversion was higher in the control population (33). Similar results were obtained by Borowiecka-Karpiuk et al. in their study of people with depressive disorders or bipolar disorder, the dominant stress coping style was focused on emotions (34). McWilliams et al. found that emotion-oriented coping was associated with depression (35). Suh et al. used the CISS and the Beck Depression Inventory (BDI) to analyze similarities and differences in stress coping strategies in a group of 135 people with bipolar disorder and 100 people with depressive disorders. They found that the severity of depressive symptoms can affect the style of coping with stress, therefore the authors divided the group with bipolar disorder into patients with and without depressive symptoms, and the group with depression into patients with and without exacerbation of symptoms. Thanks to this division, it was noted that patients with bipolar disorder and depressive symptoms were less likely to use task-oriented coping and avoidance-oriented coping, and more likely to apply emotion-oriented coping than bipolar patients without depression (36). A review of the literature indicates that many people with mood disorders choose maladaptive methods of coping with the disease (37–41).
Alemayehu et al. (42) demonstrated that poor QoL of patients with depressive disorders was significantly linked to their non-adherence to treatment recommendations. Similar results were obtained in a study conducted as part of the EU National Health and Wellbeing Survey (NHWS) (43). The likely reasons for this phenomenon may be the fact that patients with chronic conditions (including depression) do not adhere to treatment due to social, physical and mental health problems, which are indicators of poor QoL (44, 45).
Pacian et al. (46) found no statistically significant differences between the risk of depression and overall QoL. It has been observed that with older age, depression becomes more common and QoL in the mental and social domains decreases. Makara-Studzińska et al. (47), on the other hand, confirmed a significant relationship between the severity of depression and QoL in the physical domain in schizophrenic patients, and Daly et al. (48) informed that depressive disorders negatively affected QoL.
Kelly et al. (49) provided evidence that people with mood disorders showed more emotional reactions, which was associated with choosing maladaptive coping styles by both women and men. Furthermore, in women, greater control over depression was related to more adaptive coping strategies.
5 Conclusions
Treatment non-adherence is a serious challenge in the treatment of patients with mood disorders. Individuals who do not adequately follow treatment recommendations often resort to alternative activities as a mechanism for coping with difficult situations. Patients who predominantly adopt an emotion-oriented coping style tend to experience lower life satisfaction and greater difficulty accepting their condition compared to their peers. Conversely, patients who adopt a task-oriented coping style report better QoL than those who rely on emotion-oriented coping or alternative activities. Additionally, patients who actively seek out social contacts tend to enjoy a significantly higher QoL than those who are less likely to use this coping style.
6 Limitation
Our study has some limitations. Most data were measured using self-report questionnaires, which may have led to biased reporting of experiences. Our study is cross-sectional, so the current study is unable to demonstrate a temporal causal relationship between treatment non-adherence and the main potential contributors. Another limitation pertains to the sample size. The Polish sample was not representative, which limits the ability to generalize the results to other populations.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Bioethics Committee of the Pomeranian Medical University in Szczecin (KB-0012/153/17). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
AJ: Writing – review & editing, Project administration, Methodology, Formal analysis, Conceptualization. DS-M: Writing – review & editing, Validation, Software. KR: Writing – review & editing, Investigation, Formal analysis, Data curation. AR: Writing – review & editing, Formal analysis. MP: Writing – review & editing, Data curation. ĆD: Writing – review & editing, Supervision. EG: Writing – review & editing, Resources, Funding acquisition. AC: Writing – review & editing, Writing – original draft, Visualization, Methodology, Conceptualization.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Acknowledgments
We thank all participants for their participation and all the staff of the survey team for their efforts that made this study possible.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. World Bank Group and, WHO. Out of the shadows: making mental health a global development priority. Washington D.C: World Bank Group&WHO (2016). Available at: http://www.worldbank.org/en/events/2016/03/09/out-of-the-shadows-making-mental-health-a-global-priority.
2. Rumble ME, White KH, Benca RM. Sleep disturbances in mood disorders. Psychiatr Clinics North America. (2015) 38:4. doi: 10.1016/j.psc.2015.07.006
3. Defar S, Abraham Y, Reta Y, Deribe B, Jisso M, Yeheyis T, et al. Health related quality of life among people with mental illness: The role of socio-clinical characteristics and level of functional disability. Front Public Health. (2023) 11:1134032. doi: 10.3389/fpubh.2023.1134032
4. Xie Z, Tanner R, Striley CL, Marlow NM. Association of functional disability with mental health services use and perceived unmet needs for mental health care among adults with serious mental illness. J Affect Disord. (2022) 299:449–55. doi: 10.1016/j.jad.2021.12.040
5. WHO. Comprehensive mental health action plan 2013-2020. Geneva: World Health Organization (2013). Available at: https://www.who.int/mental_health/action_plan_2013/en/.
6. Cramer JA, Rosenheck R. Compliance with medication regimens for mental and physical disorders. Psychiatr Serv. (1998) 49:196–201. doi: 10.1176/ps.49.2.196
7. Semahegn A, Torpey K, Manu A, Assefa N, Tesfaye G, Ankomah A. Psychotropic medication non-adherence and associated factors among adult patients with major psychiatric disorders: a protocol for a systematic review. BMC Syst Rev. (2018) 7:10. doi: 10.1186/s13643-018-0676-y
8. Ramamurthy P, Jayasree A, Solomon S, Rudravaram VV, Menon V, Thilakan P. Medication nonadherence and its associated factors in psychiatric patients in India: A systematic review and meta-analysis. Indian J Psychiatry. (2023) 65:506–25. doi: 10.4103/Indianjpsychiatry.Indianjpsychiatry_249_22
9. Semahegn A, Torpey K, Manu A, Assefa N, Tesfaye G, Ankomah A. Psychotropic medication non-adherence and its associated factors among patients with major psychiatric disorders: a systematic review and meta-analysis. Syst Rev. (2020) 9:17. doi: 10.1186/s13643-020-1274-3
10. WHO. Adherence to long-term therapies; Evidence for action. Geneva: World Health Organization (2003). Available at: https://apps.who.int/iris/bitstream/handle/10665/42682/9241545992.pdf;jsessionid.
11. Sajatovic M, Ignacio RV, West JA, Cassidy KA, Safavi R, Kilbourne AM, et al. Predictors of nonadherence among individuals with bipolar disorder receiving treatment in a community mental health clinic. Compr Psychiatry. (2009) 50:100–7. doi: 10.1016/j.comppsych.2008.06.008
12. Colom F, Vieta E. Non-adherence in psychiatric disorders: misbehaviour or clinical feature? Acta Psychiatr Scand. (2002) 105:161–3. doi: 10.1034/j.1600-0447.2002.1e003.x
13. Loots E, Goossens E, Vanwesemael T, Morrens M, Van Rompaey B, Dilles T. Interventions to improve medication adherence in patients with schizophrenia or bipolar disorders: A systematic review and meta-analysis. Int J Environ Res Public Health. (2021) 18:10213. doi: 10.3390/ijerph181910213
14. Taj F, Tanwir M, Aly Z, Khowajah AA, Tariq A, Syed FK, et al. Factors associated with non-adherence among psychiatric patients at a Tertiary Care Hospital, Karachi, Pakistan: a questionnaire based cross-sectional study. J Pak Med Assoc. (2008) 58:432–6.
15. Farooq S, Naeem F. Tackling nonadherence in psychiatric disorders: current opinion. Review. Dovepress Neuropsychiatr Dis Treat. (2014) 10:1069–77. doi: 10.2147/NDT.S40777
16. Smith F, Clifford S. Adherence to medication among chronic patients in Middle Eastern countries: review of studies. East Mediterr Heal J. (2011) 17:356–63. doi: 10.26719/2011.17.4.356
17. Lintunen J, Lähteenvuo M, Tanskanen A, Tiihonen J, Taipale H. Non-adherence to mood stabilizers and antipsychotics among persons with bipolar disorder - A nationwide cohort study. J Affect Disord. (2023) 333:403–8. doi: 10.1016/j.jad.2023.04.030
18. Senner F, Hiendl L, Bengesser S, Adorjan K, Anghelescu IG, Baune BT, et al. Medication adherence and cognitive performance in schizophrenia-spectrum and bipolar disorder: results from the PsyCourse Study. Transl Psychiatry. (2023) 13:99. doi: 10.1038/s41398-023-02373-x
19. Burton WN, Chen C-Y, Conti DJ, Schultz AB, Edington DW. The association of antidepressant medication adherence with employee disability absences. Am J Manag Care. (2007) 13:105–13.
20. Taylor SE, Stanton AL. Coping resources, coping processes, and mental health. Annu Rev Clin Psychol. (2007) 3:377–401. doi: 10.1146/annurev.clinpsy.3.022806.091520
22. Elphee EE. Understanding the concept of uncertainty in patients with indolent lymphoma. Oncol Nurs Forum. (2008) 35:449–54. doi: 10.1188/08.ONF.449-454
23. Suh H, Kang TU, Moon E, Park JM, Lee BD, Lee YM, et al. Similarities and differences of strategies between bipolar and depressive disorders on stress coping. Psychiatry Investig. (2020) 17:71–7. doi: 10.30773/pi.2019.0152
24. Greenhouse WJ, Meyer B, Johnson SL. Coping and medication adherence in bipolar disorder. J Affect Disord. (2000) 59:237–41. doi: 10.1016/s0165-0327(99)00152-4
25. Kabzińska-Milewska K, Czajeczny D, Wójciak RW. Acceptance, coping strategies and health behaviors in bipolar disorder patients taking and not taking lithium carbonate. Health Psychol Rep. (2022) 10:168–76. doi: 10.5114/hpr.2021.112090
26. Endler NS, Parker J. Coping inventory for stressful situations. Toronto: Multi-Health Systems Incorporated (1990).
27. Tomczak-Witych A. Coping with stress strategies among female patients suffering from a depression. Psychiatr Polska. (2006) 40:491–502.
28. Jabłońska A. Trafność teoretyczna Kwestionariusza radzenia sobie w sytuacjach stresowych CISS ze szczególnym uwzględnieniem trafności teoretycznej skali stylu skoncentrowanego na unikaniu. Testy Psychologiczne W Praktyce I Badaniach. (2021) 1:31–51. doi: 10.14746/tppb.2015.1.4
29. Juczyński Z. Narzędzia pomiaru w promocji i psychologii zdrowia. Skala Satysfakcji z Życia. In: Pracownia testów psychologicznych polskiego towarzystwa psychologicznego. Warszawa: Pracownia Testów Psychologicznych Polskiego Towarzystw Psychologicznego (2001). (s. 134-138).
30. Tylka J, Piotrowicz R. Kwestionariusz oceny jakości życia SF-36 – wersja polska Quality of life SF-36 questionnaire – the Polish version. Kardiol Pol. (2009) 67:1166–69.
31. Lomper K, Chabowski M, Chudiak A, Białoszewski A, Dudek K, Jankowska-Polańska B. Psychometric evaluation of the Polish version of the Adherence to Refills and Medications Scale (ARMS) in adults with hypertension. Patient Prefer Adherence. (2018) 12:2661–70. doi: 10.2147/PPA.S185305
32. Czerw A, Religioni U, Szumilas P, Sygit K, Partyka O, Mękal D, et al. Normalization of the AIS (Acceptance of Illness Scale) questionnaire and the possibility of its use among cancer patients. Ann Agric Environ Med. (2021) 29(2):269–73. doi: 10.26444/aaem/144197
33. Szeliga- Lewińska J, Landowski J. Sposób tworzenia świata przez chorych z epizodem depresyjnym a strategie radzenia sobie ze stresem. Via Med. (2006) 3:22–6.
34. Borowiecka-Karpiuk J, Dudek D, Siwek M, Jaeschke R. Spousal burden in partners of patients with major depressive disorder and bipolar disorder. Psychiatr Pol. (2014) 48:773–87.
35. McWilliams L, Cox B, Enns M. Use of the Coping Inventory for Stressful Situations in a clinically depressed sample: factor structure, personality correlates, and prediction of distress. J Clin Psychol. (2003) 59:423–37. doi: 10.1002/jclp.10080
36. Meule A, Voderholzer U. Life satisfaction in persons with mental disorders. Qual Life Res. (2020) 29:3043–52. doi: 10.1007/s11136-020-02556-9
37. Adan A, Antúnez JM, Navarro JF. Coping strategies related to treatment in substance use disorder patients with and without comorbid depression. Psychiatry Res. (2017) 251:325–32. doi: 10.1016/j.psychres.2017.02.035
38. Coriale G, Bilotta E, Leone L, Cosimi F, Porrari R, De Rosa F, et al. Avoidance coping strategies, alexithymia and alcohol abuse: a mediation analysis. Addict. Behav. (2012) 37:1224–9. doi: 10.1016/j.addbeh.2012.05.018
39. Marquez-Arrico JE, Benaiges I, Adan A. Strategies to cope with treatment in substance use disorder male patients with and without schizophrenia. Psychiatry Res. (2015) 28:752–9. doi: 10.1016/j.psychres.2015.05.028
40. Pence BW, Thielman NM, Whetten K, Ostermann J, Kumar V, Mugavero MJ. Coping strategies and patterns of alcohol and drug use among HIV-infected patients in the United States Southeast. AIDS Patient Care STDS. (2015) 22:869–77. doi: 10.1089/apc.2008.0022
41. Kiral K, Yetim Ü, Özge A, Aydin A. The relationships between coping strategies, social support and depression: an investigation among Turkish care-givers of patients with dementia. Ageing Soc. (2015) 37(1):167–87. doi: 10.1017/S0144686X1500104X
42. Alemayehu Y, Asfaw H, Girma M. Magnitude and factors associated with treatment non-adherence among patients with depressive disorders at St. Amanuel Mental Specialized Hospital, Addis Ababa, Ethiopia, 2019: A cross sectional study. PloS One. (2022) 17:e0271713. doi: 10.1371/journal.pone.0271713
43. Pedersini R, Kuehl M. The burden associated with non-adherence in european patients with depression. Value Health. (2014) 17:A329. doi: 10.1016/j.jval.2014.08.606
44. Voros V FS, Tenyi T, Rihmer Z, Szili I, Osvath P. Untreated depressive symptoms significantly worsen quality of life in old age and may lead to the misdiagnosis of dementia: a cross-sectional study. Ann Gen Psychiatry. (2020) 19:52. doi: 10.1186/s12991-020-00302-6
45. Hayhurst K DR, Massie J, Dunn G, Barnes T, Jones P, et al. Improved quality of life over one year is associated with improved adherence in patients with schizophrenia. Eur Psychiatry. (2014) 29:191–6. doi: 10.1016/j.eurpsy.2013.03.002
46. Pacian A B, Kulik TB, Chruściel P, Mazurek-Sitarz M, Sitarz K, Derewiecki T. Jakość życia a ryzyko depresji wśród osób starszych. Hygeia Public Health. (2014) 49:820–4.
47. Makara-Studzińska M, Wołyniak M, Koślak A. Jakość życia a nasilenie objawów lęku i depresji w rodzinach osób chorych na schizofrenią – badania wstępne. Bad Schizofr. (2009) 10:194–9.
48. Daly EJ, Trivedi MH, Wisniewski SR, Nierenberg AA, Gaynes BN, Warden D, et al. Health-related quality of life in depression: A STAR*D report. Ann Clin Psychiatr. (2010) 22:43–55.
Keywords: adherence, coping strategies, stress, mood disorder, quality of life
Citation: Jeżuchowska A, Schneider-Matyka D, Rachubińska K, Reginia A, Panczyk M, Ćwiek D, Grochans E and Cybulska AM (2024) Coping strategies and adherence in people with mood disorder: a cross-sectional study. Front. Psychiatry 15:1400951. doi: 10.3389/fpsyt.2024.1400951
Received: 14 March 2024; Accepted: 22 April 2024;
Published: 21 May 2024.
Edited by:
Samet Kose, University of Health Sciences, TürkiyeReviewed by:
Ewa Kupcewicz, University of Warmia and Mazury in Olsztyn, PolandGrazyna Nowak-Starz, Jan Kochanowski University in Kielce, Poland
Copyright © 2024 Jeżuchowska, Schneider-Matyka, Rachubińska, Reginia, Panczyk, Ćwiek, Grochans and Cybulska. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Anna Maria Cybulska, YW5uYS5jeWJ1bHNrYUBwdW0uZWR1LnBs