
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
MINI REVIEW article
Front. Psychiatry , 15 May 2024
Sec. Mood Disorders
Volume 15 - 2024 | https://doi.org/10.3389/fpsyt.2024.1394787
This article is part of the Research Topic Treatment Resistant Depression (TRD): epidemiology, clinic, burden and treatment View all 23 articles
 Matteo Di Vincenzo1
Matteo Di Vincenzo1 Vassilis Martiadis2
Vassilis Martiadis2 Bianca Della Rocca1Eleonora Arsenio1Andrea D’Arpa1Antonio Volpicelli1
Bianca Della Rocca1Eleonora Arsenio1Andrea D’Arpa1Antonio Volpicelli1 Mario Luciano1
Mario Luciano1 Gaia Sampogna1*
Gaia Sampogna1* Andrea Fiorillo1
Andrea Fiorillo1Introduction and aims: Treatment-resistant depression (TRD) occurs when at least two different antidepressants, taken at the right dosage, for adequate period of time and with continuity, fail to give positive clinical effects. Esketamine, the S-enantiomer of ketamine, was recently approved for TRD treatment from U.S. Food and Drug Administration and European Medicine Agency. Despite proved clinical efficacy, many misconceptions by clinicians and patients accompany this medication. We aimed to review the most common “false myths” regarding TRD and esketemine, counterarguing with evidence-based facts.
Methods: The keywords “esketamine”, “treatment resistance depression”, “depression”, “myth”, “mythology”, “pharmacological treatment”, and “misunderstanding” were entered in the main databases and combined through Boolean operators.
Results: Misconceptions regarding the TRD prevalence, clinical features and predictors have been found. With respect of esketamine, criteria to start treatment, dissociative symptoms, potential addiction and aspects of administration and monitoring, were found to be affected by false beliefs by clinicians and patients.
Discussion and conclusion: TRD represents a challenging condition, requiring precise diagnosis in order to achieve patient’s full recovery. Esketamine has been proved as an effective medication to treat TRD, although it requires precautions. Evidence can inform clinical practice, in order to offer this innovative treatment to all patients with TRD.
Major Depressive Disorder (MDD) is a severe mental disorder affecting approximately 280 million people worldwide and representing globally the leading cause of disability. MDD has been conceptualized as a syndrome characterized by depressed mood, loss of pleasure and interest, and other affective, cognitive and somatic symptoms persisting for more than two weeks (1–3). Moreover, MDD impairs psychosocial functioning and quality of life (4, 5). A clinical characterization of the individual patient is necessary in order to develop personalized treatment plan with the final aim of reaching the full recovery (6–9). People with MDD report many physical comorbidities, with a negative impact on the long-term quality of life and reducing their life expectancy (10).
Patients suffering from MDD can report a recurrent course of the disorder, with up to 50% of them not experiencing a full recovery after the first episode, and up to 35% experience more than one episode (11). Therefore, based on the longitudinal course of the disorder, several authors have proposed to distinguish difficult to treat depression from treatment-resistant depression (TRD). In particular, it is a clinical condition characterized by lack of response to appropriate treatment. The construct of TRD is very complex, as witnessed by the fact that several definitions have been proposed (12). A consensus definition is still not available, with implications on epidemiology, policy decision-making and clinical utility (13, 14). No single biomarker has been identified so far which can be considered as a benchmark for depression (15, 16) and for TRD, reflecting a common difficulty in findings biomarkers for mental disorders (17–19).
The European Medicine Agency (EMA) defined TRD as a “failure to produce significant clinical results with a treatment of at least two different antidepressants (of the same or different classes) administered at the right doses and for an adequate amount of time, with verified patients’ compliance to treatment” (20). Although this definition focuses only on pharmacological aspects and does not consider psychotherapy as a strategy for mild conditions, it is widely applied in the context of research (21, 22).
Consistently to this conceptualization, EMA approved intranasal esketamine in combination with an SSRI or a SNRI for the treatment of adults with TRD in December 2019 (23), following the lead of U.S. Food and Drug Administration (24). The approval of esketamine for treating TRD has introduced an antidepressant drug with an innovative mechanism of action into clinicians’ armamentarium. According to recent guidelines for managing TRD, several strategies have been suggested, including the combination or switch of antidepressants; augmentation with antipsychotic and/or mood stabilizers (25); administration of intravenous/intranasal ketamine (26) and neurostimulation techniques (electroconvulsive therapy, deep brain stimulation, vagal nerve stimulation, repetitive transcranial stimulation) (27–29).
Esketamine is the S-enantiomer of ketamine, working as non-selective, non-competitive antagonist of N-methyl-D-aspartate (NDMA) receptor (30). Subsequent downstream of glutamate release stimulates the activation of AMPA receptors, by initiating intracellular signaling cascades, resulting in the activation of mammalian target of rapamycin (mTOR) and increase of brain-derived neurotrophic factor (BDNF) levels, with positive effects on synaptic plasticity (31, 32). In terms of pharmacokinetics, intranasal esketamine has mean bioavailability of about 48%, its peak is reached until to 40 minutes from last spray, presents biphasic half-life and undergoes metabolism through CYP-2B6, -3A4, -2C9, -2C19, hydroxylation and glucuronidation (33).
Esketamine may be associated with craving behavior and additional potential (34). Indeed, dissociative state is characterized by depersonalization and derealization (24), while hallucinations have been reported as a consequence of the recreational use of ketamine, not for esketamine (35, 36). In this regard, resistance by clinicians may be encountered to the detriment of proved clinical effectiveness in TRD. Based on such premises, we carried out a narrative review of the available literature on the most common “misconceptions” and “stereotypes” associated with esketamine use; for each false myth, we provide a list of “good reasons” for disconfirming such stereotypes.
The keywords “esketamine”, “treatment resistant depression”, “depression”, “myth”, “mythology”, “pharmacological treatment”, and “misunderstanding” were entered in PubMed, ISI Web of Knowledge, Scopus and Medline. Terms and databases were combined using the Boolean search technique, which consists of a logical information retrieval system (two or more terms combined to make searches more restrictive or detailed). The search strategy has been limited from March 2019, when the US Food and Drug Administration (FDA) approved the use of esketamine for the treatment of treatment-resistance depression (TRD), to March 2024. The following criteria were considered for including papers in the present narrative review: 1) papers written in English; 2) papers focused on the use of esketamine as add-on treatment for TRD patients; 3) focus on prevalence of TRD and/or on side effects of esketamine treatment and/or risk of addiction due to esketamine use and/or rules of clinical practice needed for administering esketamine.
Based on the search strategy, selected studies were used for counteracting the common false myths reported in clinical practice about the use of esketamine for the treatment of patients with TRD.
The most common false myths are the following: 1) the prevalence of TRD is low in clinical practice; 2) no specific clinical features characterize the individual patient with TRD; 3) TRD cannot be predicted before its clinical manifestation; 4) patient candidate to esketamine treatment must have reported nonresponse to either SSRIs or SNRIs; 5) patient candidate to esketamine treatment must be affected only from MDD; 6) patient treated with esketamine will report side effects, including dissociation and agitation; 7) esketamine is associated with high risk of addiction; 8) esketamine treatment requires long period of observation, with adequate room and many healthcare professionals involved in the administration procedure (Table 1).
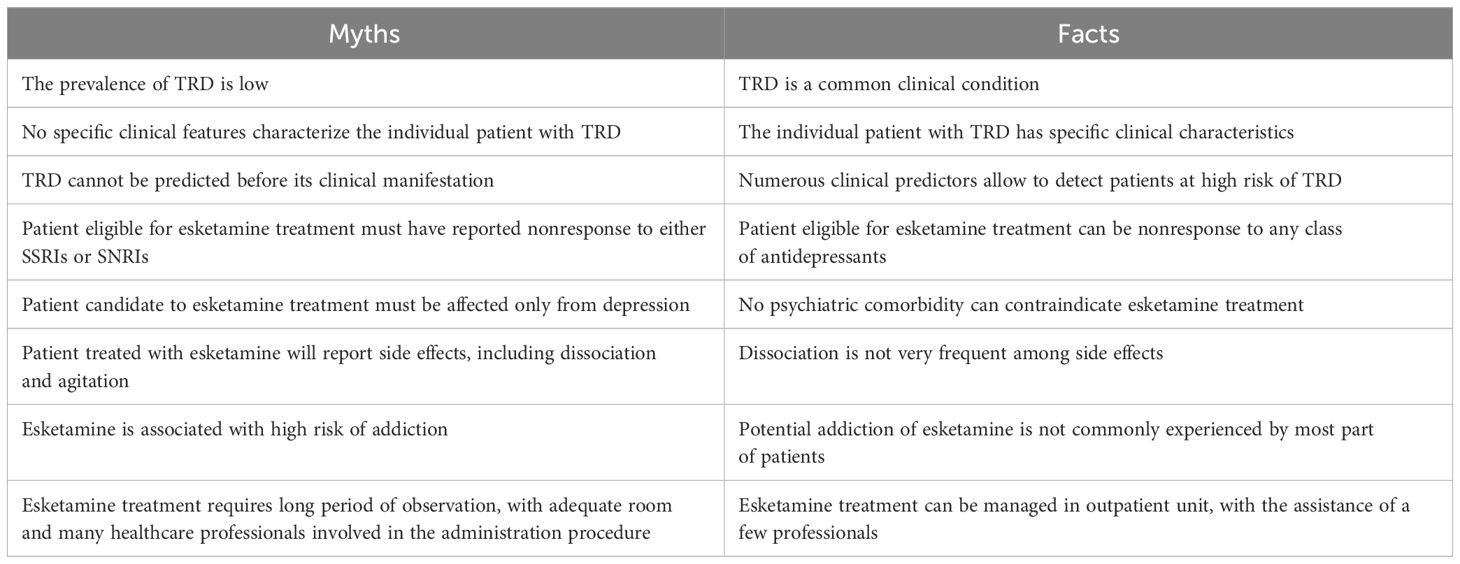
Table 1 The most common false myths and facts regarding TRD and esketamine treatment.
Myth 1: The prevalence of TRD is low
Fact 1: TRD is a common clinical condition
The Sequenced Treatment Alternatives to Relieve Depression (STAR*D) trial (37) found a cumulative remission rate of 67% throughout four acute treatment steps, while a TRD prevalence of up to 55% was detected in a cross-sectional study focused on primary care in United Kingdom (38). In more recent years, Liu et al. (39) found lower rates (5.8% and 6.0%) by analyzing data from two large databases encompassing almost 600,000 patients taking medications for depression in the United States, where a 12-month prevalence of 30.9% was also found in four claims studies (40). A similar French research detected 25.8 people suffering from TRD per 10,000 patients (41). Furthermore, TRD proportion was estimated to be 4.2% in Italy (42), 24.4% in Israel (43) and 19.6% in Thailand (44). Although prevalence data are heterogeneous, the common element is that TRD is quite frequent in ordinary clinical practice. Clinicians should be aware of the characteristics of TRD as well as of the different therapeutic strategies for managing patients suffering from TRD.
However, exact prevalence rate of TRD cannot be estimated due to the lack of a consensus definition and due to the different settings where patients can be treated (i.e., primary care, outpatient units, inpatient unit, academia) (14, 45, 46).
Myth 2: No specific clinical features characterize the individual patient with TRD
Fact 2: The individual patient with TRD has specific clinical characteristics
TRD is a clinical condition associated with high levels of social and personal burden (47), requiring half of expenditure for medical treatment of major depression in the United States (about $92.7 billion per year) (40). Patients with TRD experience significant impairment in psychosocial functioning, poor levels of quality of life, and adverse health outcomes (48–52). Hospitalization rate and emergency department utilization were found to be more than twice in TRD patients in comparison with general population (50, 53), with also significantly longer hospital stay (36% more) and higher costs (54). When compared with treatment-responding subjects, TRD patients reported more prevalent hypertension, hypothyroidism and chronic pulmonary disease (55), as well as substance use, anxiety, insomnia and pain (49). TRD patients have higher level of brain aging compared to responders (56). Furthermore, higher mortality risk (7-16 deaths per 1000 patients in 5 years) and mortality rates have been found (57–60). Compared with treatment-responsive patients, individuals with TRD are twice as likely to attempt suicide, showing a rate of 30% (61, 62).
Myth 3: TRD cannot be predicted before its clinical manifestations
Fact 3: Numerous clinical predictors allow to detect patients at high risk of TRD
Several variables have been studied as potential predictors of TRD. A European multicentric study performed on 702 patients with depression (63) detected significant association between TRD and comorbid panic disorder (OR: 3.2), anxiety (OR: 2.6), suicidal risk (OR: 2.2), social phobia (OR: 2.1), young age of onset (OR: 2.0), personality disorder (OR: 1.7), symptom severity (OR: 1.7), history of multiple hospitalizations (OR: 1.6), nonresponse to the first antidepressant taken (OR: 1.6), melancholia (OR: 1.5), and recurrent episodes (OR: 1.5). Severity and length of depressive episode, risk of suicide, psychotic symptoms, comorbid anxiety, non-response to previous antidepressants, recurrence and hospitalization were confirmed in association with TRD (64, 65), alongside with antidepressants at higher doses (66). Moreover, among physical health problems cardiovascular disease, pain and thyroid problems were most commonly reported to be associated, as well as female gender among sociodemographic variables (67). Few studies also tested the association between TRD and specific candidate genetic factors, but no specific biomarkers have been identified so far (68).
Myth 4: Patient eligible to esketamine treatment must have reported nonresponse to either SSRIs or SNRIs
Fact 4: Patient eligible for esketamine treatment can be nonresponse to any class of antidepressants
Both FDA (24) and EMA (23) approved esketamine treatment for patients with depression who had tried at least two different antidepressants without gaining benefits. In this regard, there is no specific mention of SSRIs and/or SNRIs in both approval release documents, so that failure of antidepressant treatment should be intended in general, also involving other classes (e.g., tricyclics, monoamine oxidases inhibitors, or dopamine/norepinephrine modulators, atypical antidepressants). Instead, it is worth mentioning that a SSRI or SNRI is specifically required to be used in combination with esketamine treatment. In a comparative study conducted in Italy (69), more than half of unipolar and bipolar TRD patients were taking other antidepressants besides SSRIs or SNRIs before starting esketamine. As well, no specification of class was provided regarding antidepressants taken by TRD subjects enrolled by Estrade et al. (70).
Myth 5: Patient candidate to esketamine treatment must be affected only from depression
Fact 5: No psychiatric comorbidity is a contraindication to esketamine treatment
TRD is a clinical condition often occurring with other comorbid psychiatric disorders, such as anxiety, obsessive compulsive disorder, attention-deficit/hyperactivity disorder, substance use disorder as well as self-harm behavior, fatigue, chronic pain, and insomnia (58, 71–74). In the real world, clinicians deal with patients suffering from TRD with other symptoms in comorbidity, which might benefit from esketamine treatment. No contraindications have been pointed out in release documents issued by FDA and EMA (23, 24). Furthermore, esketamine’s effectiveness was investigated in TRD patients with comorbid anxiety (75), post-traumatic stress disorder (76), and substance use disorder (77). The use of esketamine for treating patients with TRD and comorbid obsessive-compulsive disorder (78) and anorexia nervosa (79) has been described as well. Esketamine combined with an oral antidepressant has been approved in the United States for managing depression with acute suicidal ideation or behavior (80, 81), and in Europe for dealing with psychiatric emergencies in adults affected from depression.
Myth 6: Patient treated with esketamine will definitely experience dissociation and agitation
Fact 6: Dissociation is not very frequent among side effects
Dissociation is a complex construct defined as a “disruption and/or discontinuity in the normal integration of consciousness, memory, identity, emotion, perception, body representation, motor control, and behavior” (1). It encompasses depersonalization, derealization, illusions and distortion of time, which may be experienced within a few hours and mostly at a non-severe degree by 11.1-31.4% of people treated with esketamine (28). The meta-analysis by Yang et al. (82) found an overall relative risk of developing dissociation of 4.54 (p<.00001) among patients using esketamine when compared with placebo group. This value resulted almost twice (RR: 8.06, p<.00001) in the subgroup taking the dosage of 56 mg. The SUSTAIN-2 trial (83) reported dissociation rate of 23.4% during the 4-week induction period and of 18.7% during the 48-week maintenance phase. A post-hoc analysis found a prevalence of dissociation of 14.3% in patients forty minutes later the administration of the first dose of esketamine (84). The findings from the SUSTAIN-3 trial (85) showed dissociation in 24.4% of participants, 99.8% of whom resolved this condition during the same day of drug administration. In the real world, dissociative symptoms were detected in 39.7% of subjects (86). Causal role of dissociation in improving depressive symptoms was not consistently found (87–89). Trait dissociation, assessed through the Dissociative Experience Scale (DES) (90), was proved to be a significant predictor for the development of dissociation as side effect. Therefore, the DES should be used as potential screening tool for identifying patients at higher risk for developing dissociation.
Psychomotor agitation is not commonly reported as a side effect of esketamine treatment. In the REAL-ESK study (86), only one case of severe agitation was recorded among 116 treated subjects. Furthermore, a case report referring to a patient experiencing agitation and dissociation due to esketamine was described by Pereira and colleagues (91), who managed this condition throughout non-pharmacological approach.
Myth 7: Esketamine is associated with high risk of addiction
Fact 7: Potential addiction of esketamine is not commonly experienced by majority of patients
Potential addiction induced by intranasal esketamine is similar to that derived from intravenous racemic ketamine in non-dependent drug users (92). Although this aspect represents a concern for clinicians, lack of validated quantitative assessment of potential addiction in TRD patients treated with esketamine has contributed to limit evidence. Wang et al. (93) developed a visual analog scale for assessing esketamine craving and drug likeability, intended as a predictor of potential addition (94). The risk of esketamine addiction does not affect all patients equally (95). Moreover, slow de-tritation of esketamine and combined use of bupropion were suggested for managing drug-seeking and craving behaviors (34).
Myth 8: Esketamine treatment requires long period of observation, with adequate room and many healthcare professionals involved in the administration procedure
Fact 8: Esketamine treatment can be managed in outpatient unit, with the assistance of a few professionals
Esketamine treatment requires some specific conditions to be met to ensure patients monitoring and comfort. Administration should be performed in a peaceful room of hospital or outpatient unit, in which bed or chair allows patients to rest. The possibility to adjust the lighting also would be an optimal option. Sphygmomanometer and handkerchiefs are essential tool to have available. Patients have to come in the morning on an empty stomach. Esketamine is auto-administered through a nasal spray device containing 28 mg per 200 μl of vehicle solution (2 sprays). Before administration, patients are asked to clean their nose and recline their head to 45°. Blood pressure monitoring is required before and forty minutes after the last administration (20). People suffering from high blood pressure (more than 140/90 mmHg in adults; more than 150/90 mmHg in the elderly) have to be treated previously, as esketamine treatment can only start when blood pressure levels are within normal range. After monitoring by 60-90 minutes, in the absence of any problems patients can be discharged. Although they can also go home alone, they are advised not to drive the car until the next day.
The present narrative review aims at counteracting false myths regarding TRD and esketamine treatment by providing the most recent and updated evidence available.
TRD represents a complex clinical condition as confirmed by the lack of a consensus definition and clear epidemiological data (14, 96–99). According to EMA conceptualization (23), depression can be defined “resistant to treatment” if at least two antidepressants failed to improve depressive symptoms, despite their use at right dose, for adequate period and with adequate patient’s compliance. Therefore, many clinical conditions labelled as “depressions difficult to treat” do not fully satisfy criteria for TRD and they may not benefit from treatments approved for TRD. Some clinical features might be useful in detecting real condition of TRD, and the identification of clear predictors of TRD can be helpful for optimizing diagnosis and subsequently therapy. It has to be noted that esketamine is approved for treatment-resistant depression (TRD) and emergency suicidality only. However, recent trials have confirmed its efficacy also in patients suffering from bipolar disorder, with an actual depressive phase (69), but this use remains off-label and clinicians should carefully evaluate the risk/benefit ratio in administering such medication to patients with different clinical conditions. Although these positive results are encouraging, further longitudinal studies, designed with a rigorous methodology, are required.
Esketamine represents an additional tool in the clinicians’ therapeutic armamentarium for treating MDD and TRD. Clinical efficacy has been proved both in experimental and real-world settings. Superiority of esketamine combined with oral antidepressant compared to placebo plus oral antidepressant was found in the short-term by Popova et al. (100), unlike Fedgchin et al. (101) and Ochs-Ross et al. (102). In the long-term treatment, esketamine is effective in terms of significant reduction of depressive symptoms (83). Moreover, in the long-term maintenance study, adult patients with TRD treated with a continue use of esketamine report a significant delay in time to relapse compared with placebo, both considering stable remitters and stable responders (103). It is relevant to consider that no potential risk for abuse has been detected in the long-term treatment (i.e., up to one year from treatment) (104).
In the real world, significant improvements in terms of depressive symptoms and remission rates were reported after three months from the start of treatment (86), also in subjects affected by bipolar TRD (69), and in elder patients who however showed high levels of side effects (105).
Esketamine represents an important novelty among pharmacological treatments for patients with MDD, having an innovative mechanism of action (106). Indeed, depression has traditionally been conceptualized as a disorder underlying by an alteration in the neurotransmission pathways of serotonin, norepinephrine and dopamine pathways. Esketamine works as non-selective, non-competitive antagonist of NDMA receptor, determining subsequent activation of AMPA and intracellular cascades (31, 32). Higher levels of BDNF and synaptic plasticity represent positive effects. Therefore, esketamine has a specific target on a new pathway, which is represented by the glutamatergic system. However, given its similar pharmacological profile and the extensive literature on its safety and tolerability, it is crucial to briefly mention ketamine (107). Many randomized controlled trials have confirmed the acute efficacy of ketamine in patients with TRD, although only a few data come from the real-world practice. A recent systematic review (26) found that ketamine has a substantial antidepressant effect, although its effectiveness varies significantly across patients. Moreover, a recent study by Gałuszko-Węgielnik et al. (108) found that ketamine is an effective add-on treatment to standard of care for people with treatment-resistant depression presenting psychotic features. Ketamine is administered as intravenous infusion and the subsequent monitoring revealed no exacerbation of psychotic symptoms in short and long-term observation, while stable remission and fast antisuicidal effect was found. However, these data should be carefully considered since the rates of recreational use of ketamine is increasing and the potential addiction to ketamine shares the same neurobiological pathway of its clinical effectiveness in treating patients suffering from TRD (109).
Taking esketamine requires a safe setting, where healthcare professionals can monitor patient’s response in terms of side effects for up to 90 minutes. Dizziness, nausea, dissociation, headache, dysgeusia, vertigo, somnolence, hypoesthesia and vomiting were reported as common side effects (110). Usually, they appear at mild or moderate degree of severity, are dose-dependent, and last only in the same day of esketamine administration. When they are severe, adjunctive treatments, and/or treatment pause or interruption should be considered (111–113). Discontinuation rate due to adverse effects in clinical trials has been estimated in about 5% of cases (85). The most relevant limitation is using esketamine is related to patients at high risk of aneurysm, and those with history of cerebral bleeding or heart attack (20). Assisted administration and monitored setting may also be helpful to promptly detect any potential risk of addiction.
Basing on patients’ age, recommended dosage consists of one or two puffs in each nostril at day 1, while up to three sprays per nostril can be administered twice a week during the following 4 weeks. Depending on patient’s conditions, treatment can be performed once a week for 4 weeks and once or two times per week up to 6 months. This strict schedule may appear a limitation for patients, but real-world study does not mention this aspect among the reasons of esketamine discontinuation (69).
Intranasal administration is unusual in psychiatric setting. Indeed, consolidated use of tablets, capsules and drops formulations has allowed the patient to take antidepressant therapy in comfort and autonomy. Furthermore, repeated and intermittent nasal sprays encouraged researchers to investigate olfactory functionality and nasal mucosa of patients, who seem to well tolerate this practice also in the long term (114, 115).
Dissociative effects and the potential addictive effects of esketamine treatment are among the main concerns related to the use of esketamine in clinical practice.
As regards dissociative effects, these are experienced as feelings of disconnection from the reality, and are reporting in up to 40% of subjects taking esketamine in the real world setting, resolving within the same day of administration. Although a causal role of dissociation in improving depressive symptoms could be hypothesized, Ballard and Zarate (87) showed that it is not necessary to determine antidepressant effects of ketamine and derived medication. Moreover, the potential addiction from this drug resulted to involve patients treated with esketamine (95).
The present study has some limitations, which must be acknowledged. First, this is not a systematic review, but rather a narrative review which is more in line with the scope of the paper. It may be that relevant studies on esketamine have been omitted, but this was due to the need to identify papers related to the false myths addressed here. In fact, narrative reviews are a specific type of review in which researchers can pursue an extensive description and interpretation of previously published papers on a chosen topic. The description of the search strategy and selection criteria should be considered a major strength of the present paper. We believe that this approach has been appropriate for the topic of “myth and facts” related to the use of esketamine in ordinary routine clinical practice.
Another limitation is the inclusion of papers published in English only, which may have led to the exclusion of some papers/clinical experiences carried out in different countries with different languages.
TRD represents a challenging clinical condition, which needs to be adequately identified and diagnosed in order to achieve patient’s full recovery. Esketamine has been proved as an effective medication to treat TRD, although it requires precautions. Evidence can inform clinical practice, in order to offer this innovative treatment to all patients with TRD.
Although esketamine is an innovative treatment for the management of TRD patients, available data clearly confirm the efficacy, safety and good tolerability profile of this medication.
MDV: Investigation, Writing – original draft. VM: Conceptualization, Writing – review & editing. BDR: Methodology, Writing – review & editing. EA: Methodology, Writing – review & editing. AD’A: Methodology, Writing – review & editing. AV: Investigation, Writing – original draft. ML: Methodology, Writing – review & editing. GS: Conceptualization, Writing – original draft. AF: Supervision, Writing – original draft, Writing – review & editing.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. American Psychiatric Association. Diagnostic and statistical manual of mental disorders. 5th edition. Washington, DC: American Psychiatric Association (2013). doi: 10.1176/appi.books.9780890425596
2. Stein DJ, Shoptaw SJ, Vigo DV, Lund C, Cuijpers P, Bantjes J, et al. Psychiatric diagnosis and treatment in the 21st century: paradigm shifts versus incremental integration. World Psychiatry. (2022) 21:393–414. doi: 10.1002/wps.20998
3. World Health Organization. (2022). Available online at: https://icd.who.int/.
5. Fusar-Poli P, Estradé A, Stanghellini G, Esposito CM, Rosfort R, Mancini M, et al. The lived experience of depression: a bottom-up review co-written by experts by experience and academics. World Psychiatry. (2023) 22:352–65. doi: 10.1002/wps.21111
6. Rush AJ, Thase ME. Improving depression outcome by patient-centered medical management. Am J Psychiatry. (2018) 175:1187–98. doi: 10.1176/appi.ajp.2018.18040398
7. Maj M, Stein DJ, Parker G, Zimmerman M, Fava GA, De Hert M, et al. The clinical characterization of the adult patient with depression aimed at personalization of management. World Psychiatry. (2020) 19:269–93. doi: 10.1002/wps.20771
8. Greenberg PE, Fournier AA, Sisitsky T, Simes M, Berman R, Koenigsberg SH, et al. The economic burden of adults with major depressive disorder in the United States, (2010 and 2018). Pharmacoeconomics. (2021) 39:653–65. doi: 10.1007/s40273-021-01019-4
9. Maj M. Understanding depression beyond the “mind-body” dichotomy. World Psychiatry. (2023) 22:349–50. doi: 10.1002/wps.21142
10. Berk M, Köhler-Forsberg O, Turner M, Penninx BWJH, Wrobel A, Firth J, et al. Comorbidity between major depressive disorder and physical diseases: a comprehensive review of epidemiology, mechanisms and management. World Psychiatry. (2023) 22:366–87. doi: 10.1002/wps.21110
11. Eaton WW, Shao H, Nestadt G, Lee HB, Bienvenu OJ, Zandi P. Population-based study of first onset and chronicity in major depressive disorder. Arch Gen Psychiatry. (2008) 65:513–20. doi: 10.1001/archpsyc.65.5.513
12. Murphy JA, Sarris J, Byrne GJ. A review of the conceptualisation and risk factors associated with treatment-resistant depression. Depress Res Treat. (2017) 2017:4176825. doi: 10.1155/2017/4176825
13. Fava M. The challenges of defining and managing treatment-resistant depression in research and practice. World Psychiatry. (2023) 22:350–1. doi: 10.1002/wps.21128
14. McIntyre RS, Alsuwaidan M, Baune BT, Berk M, Demyttenaere K, Goldberg JF, et al. Treatment-resistant depression: definition, prevalence, detection, management, and investigational interventions. World Psychiatry. (2023) 22:394–412. doi: 10.1002/wps.21120
15. Abi-Dargham A, Moeller SJ, Ali F, DeLorenzo C, Domschke K, Horga G, et al. Candidate biomarkers in psychiatric disorders: state of the field. World Psychiatry. (2023) 22:236–62. doi: 10.1002/wps.21078
16. Mayberg HS, Dunlop BW. Balancing the beautiful and the good in pursuit of biomarkers for depression. World Psychiatry. (2023) 22:265–7. doi: 10.1002/wps.21081
17. Tamminga CA. Discovering informative biomarkers in psychiatry. World Psychiatry. (2023) 22:270–1. doi: 10.1002/wps.21084
18. Yatham LN. Biomarkers for clinical use in psychiatry: where are we and will we ever get there? World Psychiatry. (2023) 22:263–4. doi: 10.1002/wps.21079
19. Kumar R, Nuñez NA, Joshi N, Joseph B, Verde A, Seshadri A, et al. Metabolomic biomarkers for (R, S)-ketamine and (S)-ketamine in treatment-resistant depression and healthy controls: A systematic review. Bipolar Disord. (2024) 00:1–10. doi: 10.1111/bdi.13412
20. European Medicines Agency. Guideline on clinical investigation of medicinal products for the treatment of depression (2013). Available online at: https://www.ema.europa.eu/en/news/european-medicines-agency-publishes-guideline-clinical-investigation-medicines-depression (Accessed April 25, 2023).
21. Parker G. Treatment-resistant depression invites persistent reflection. World Psychiatry. (2023) 22:414–5. doi: 10.1002/wps.21135
22. Thase ME. Recent developments pertaining to treatment-resistant depression: a 40-year perspective. World Psychiatry. (2023) 22:413–4. doi: 10.1002/wps.21134
23. European Medicine Agency. Available online at: https://www.ema.europa.eu/en/medicines/human/EPAR/spravato.
24. Food and Drug Administration. (2019). Available online at: https://www.fda.gov/news-events/press-announcements/fda-approves-new-nasal-spray-medication-treatment-resistant-depression-available-only-certified.
25. Kennedy SH, Lam RW, McIntyre RS, Tourjman SV, Bhat V, Blier P, et al. Canadian Network for Mood and Anxiety Treatments (CANMAT) 2016 clinical guidelines for the management of adults with major depressive disorder: Section 3. Pharmacol Treatment Can J Psychiatry. (2016) 61(9):540–60. doi: 10.1177/0706743716659417
26. Alnefeesi Y, Chen-Li D, Krane E, Jawad MY, Rodrigues NB, Ceban F, et al. Real-world effectiveness of ketamine in treatment-resistant depression: A systematic review & meta-analysis. J Psychiatr Res. (2022) 151:693–709. doi: 10.1016/j.jpsychires.2022.04.037
27. McLachlan G. Treatment resistant depression: what are the options? BMJ. (2018) 363:k5354. doi: 10.1136/bmj.k5354
28. Swainson J, Thomas RK, Archer S, Chrenek C, MacKay M-A, Baker G, et al. esketamine for treatment resistant depression. Expert Rev Neurother. (2019) 19:899–911. doi: 10.1080/14737175.2019.1640604
29. Howes OD, Baxter L. The drug treatment deadlock in psychiatry and the route forward. World Psychiatry. (2023) 22:2–3. doi: 10.1002/wps.21059
30. Stahl S. Esketamine. In: Prescriber’s guide: stahl’s essential psychopharmacology. Cambridge University Press, Cambridge (2020). p. 275–80. doi: 10.1017/9781108921275.046
31. Duman RS, Aghajanian GK. Synaptic dysfunction in depression: potential therapeutic targets. Science. (2012) 338:68–72. doi: 10.1126/science.1222939
32. Duman RS, Aghajanian GK, Sanacora G. et al: Synaptic plasticity and depression: new insights from stress and rapid-acting antide- pressants. Nat Med. (2016) 22:238–49. doi: 10.1038/nm.4050
33. Bahr R, Lopez A, Rey JA. Intranasal esketamine (SpravatoTM) for use in treatment-resistant depression in conjunction with an oral antidepressant. P T. (2019) 44:340–75.
34. Orsolini L, Salvi V, Volpe U. Craving and addictive potential of esketamine as side effects? Expert Opin Drug Saf. (2022) 21:803–12. doi: 10.1080/14740338.2022.2071422
35. Goodwin GM. The psychedelic experience and treatment-resistant depression. World Psychiatry. (2023) 22:420–2. doi: 10.1002/wps.21140
36. Weissman MM. Does treatment-resistant depression need psychotherapy? World Psychiatry. (2023) 22:417–8. doi: 10.1002/wps.21137
37. Rush AJ, Trivedi MH, Wisniewski SR, Nierenberg AA, Stewart JW, Warden D, et al. Acute and longer-term outcomes in depressed outpatients requiring one or several treatment steps: a STAR*D report. Am J Psychiatry. (2006) 163:1905–17. doi: 10.1176/ajp.2006.163.11.1905
38. Thomas L, Kessler D, Campbell J, Morrison J, Peters TJ, Williams C, et al. Prevalence of treatment-resistant depression in primary care: cross-sectional data. Br J Gen Pract. (2013) 63:e852–8. doi: 10.3399/bjgp13X675430
39. Liu X, Mukai Y, Furtek CI, Bortnichak EA, Liaw KL, Zhong W. Epidemiology of treatment-resistant depression in the United States. J Clin Psychiatry. (2021) 83(1):21m13964. doi: 10.4088/JCP.21m13964
40. Zhdanava M, Pilon D, Ghelerter I, Chow W, Joshi K, Lefebvre P, et al. The prevalence and national burden of treatment-resistant depression and major depressive disorder in the United States. J Clin Psychiatry. (2021) 82:20m13699. doi: 10.4088/JCP.20m13699
41. Bosco-Lévy P, Grelaud A, Blin P, Astruc B, Falissard B, Llorca PM, et al. Treatment resistant depression incidence and prevalence using the French nationwide claims database. Pharmacoepidemiol Drug Saf. (2021) 30:169–77. doi: 10.1002/pds.5082
42. Perrone V, Sangiorgi D, Andretta M, Ducci G, Forti B, PC FM, et al. Assessment of patients affected by treatment-resistant depression: findings from a Real-World Study in Italy. J Psychiatry Psychiatr Disord. (2020) 4:104–17. doi: 10.26502/jppd.2572-519X0098
43. Sharman Moser S, Chodick G, Gelerstein S, Barit Ben David N, Shalev V, Stein-Reisner O. Epidemiology of treatment resistant depression among major depressive disorder patients in Israel. BMC Psychiatry. (2022) 22:541. doi: 10.1186/s12888-022-04184-8
44. Prasartpornsirichoke J, Pityaratstian N, Poolvoralaks C, Sirinimnualkul N, Ormtavesub T, Hiranwattana N, et al. The prevalence and economic burden of treatment-resistant depression in Thailand. BMC Public Health. (2023) 23:1541. doi: 10.1186/s12889-023-16477-y
45. Thase ME, Rush AJ. When at first you don’t succeed: sequential strategies for antidepressant nonresponders. J Clin Psychiatry. (1997) 58 Suppl 13:23–9.
46. Nemeroff CB. Prevalence and management of treatment-resistant depression. J Clin Psychiatry. (2007) 68 Suppl 8:17–25.
47. Keitner GI, Mansfield AK. Management of treatment-resistant depression. Psychiatr Clin North Am. (2012) 35:249–65. doi: 10.1016/j.psc.2011.11.004
48. Dibernardo A, Lin X, Zhang Q, Xiang J, Lu L, Jamieson C, et al. Humanistic outcomes in treatment resistant depression: A secondary analysis of the STAR*D study. BMC Psychiatry [Electronic Resource]. (2018) 18:352. doi: 10.1186/s12888-018-1920-7
49. Cepeda MS, Reps J, Fife D, Blacketer C, Stang P, Ryan P. Finding treatment-resistant depression in real-world data: How a data- driven approach compares with expert-based heuristics. Depression Anxiety. (2018) 35:220–8. doi: 10.1002/da.22705
50. Jaffe DH, Rive B, Denee TR. The humanistic and economic burden of treatment-resistant depression in Europe: a cross-sectional study. BMC Psychiatry. (2019) 19:247. doi: 10.1186/s12888-019-2222-4
51. Johnston KM, Powell LC, Anderson IM, Szabo S, Cline S. The burden of treatment-resistant depression: A systematic review of the economic and quality of life literature. J Affect Disord. (2019) 242:195–210. doi: 10.1016/j.jad.2018.06.045
52. Halaris A, Sohl E, Whitham EA. Treatment-resistant depression revisited: A glimmer of hope. J Pers Med. (2021) 11:155. doi: 10.3390/jpm11020155
53. Knoth RL, Bolge SC, Kim E, Tran QV. Effect of inadequate response to treatment in patients with depression. Am J Manag Care. (2010) 16:e188–96.
54. Lin J, Szukis H, Sheehan JJ, Alphs L, Menges B, Lingohr-Smith M, et al. Economic burden of treatment-resistant depression among patients hospitalized for major depressive disorder in the United States. Psychiatr Res Clin Pract. (2019) 1:68–76. doi: 10.1176/appi.prcp.20190001
55. Amos TB, Tandon N, Lefebvre P, Pilon D, Kamstra RL, Pivneva I, et al. Direct and indirect cost burden and change of employment status in treatment-resistant depression: A matched-cohort study using a US commercial claims database. J Clin Psychiatry. (2018) 79:17m11725. doi: 10.4088/JCP.17m11725
56. Dintica CS, Habes M, Erus G, Simone T, Schreiner P, Yaffe K. Long-term depressive symptoms and midlife brain age. J Affect Disord. (2023) 320:436–41. doi: 10.1016/j.jad.2022.09.164
57. Carney RM, Freedland KE. Treatment-resistant depression and mortality after acute coronary syndrome. Am J Psychiatry. (2009) 166:410–7. doi: 10.1176/appi.ajp.2008.08081239
58. Reutfors J, Andersson TML, Brenner P, Brandt L, DiBernardo A, Li G, et al. Mortality in treatment-resistant unipolar depression:aregister-basedcohortstudyin Sweden. J Affect Disord. (2018) 238:674–9. doi: 10.1016/j.jad.2018.06.030
59. Li G, Fife D, Wang G, Sheehan JJ, Bodén R, Brandt L, et al. All-cause mortality in patients with treatment-resistant depression: a cohort study in the US population. Ann Gen Psychiatry. (2019) 18:23. doi: 10.1186/s12991-019-0248-0
60. Brenner P, Reutfors J, Nijs M, Andersson TM. Excess deaths in treatment-resistant depression. Ther Adv Psychopharmacol. (2021) 11:20451253211006508. doi: 10.1177/20451253211006508
61. Bergfeld IO, Mantione M, Figee M, Schuurman PR, Lok A, Denys D. Treatment-resistant depression and suicidality. J Affect Disord. (2018) 235:362–7. doi: 10.1016/j.jad.2018.04.016
62. Gronemann FH, Jørgensen MB, Nordentoft M, Andersen PK, Osler M. Treatment-resistant depression and risk of all-cause mortality and suicidality in Danish patients with major depression. J Psychiatr Res. (2021) 135:197–202. doi: 10.1016/j.jpsychires.2021.01.014
63. Souery D, Oswald P, Massat I, Bailer U, Bollen J, Demyttenaere K, et al. Clinical factors associated with treatment resistance in major depressive disorder: results from a European multicenter study. J Clin Psychiatry. (2007) 68:1062–70. doi: 10.4088/jcp.v68n0713
64. Kautzky A, Dold M, Bartova L, Spies M, Kranz GS, Souery D, et al. Clinical factors predicting treatment resistant depression: affirmative results from the European multicenter study. Acta Psychiatr Scand. (2019) 139:78–88. doi: 10.1111/acps.12959
65. Bartova L, Dold M, Kautzky A, Fabbri C, Spies M, Serretti A, et al. Results of the European Group for the Study of Resistant Depression (GSRD) - basis for further research and clinical practice. World J Biol Psychiatry. (2019) 20:427–48. doi: 10.1080/15622975.2019.1635270
66. De Carlo V, Calati R, Serretti A. Socio-demographic and clinical predictors of non-response/non-remission in treatment resistant depressed patients: A systematic review. Psychiatry Res. (2016) 240:421–30. doi: 10.1016/j.psychres.2016.04.034
67. O’Connor SJ, Hewitt N, Kuc J, Orsini LS. Predictors and risk factors of treatment-resistant depression: A systematic review. J Clin Psychiatry. (2023) 85(1):23r14885. doi: 10.4088/JCP.23r14885
68. Fabbri C, Corponi F, Souery D, Kasper S, Montegomery S, Zohar J, et al. The genetics of treatment-resistant depression: a critical review and future perspectives. Int J Neuropsychopharmacol. (2019) 22(2):93–104. doi: 10.1093/ijnp/pyy024
69. Martinotti G, Dell’Osso B, Di Lorenzo G, Maina G, Bertolino A, Clerici M, et al. Treating bipolar depression with esketamine: Safety and effectiveness data from a naturalistic multicentric study on esketamine in bipolar versus unipolar treatment-resistant depression. Bipolar Disord. (2023) 25:233–44. doi: 10.1111/bdi.13296
70. Estrade I, Petit AC, Sylvestre V, Danon M, Leroy S, Perrain R, et al. Early effects predict trajectories of response to esketamine in treatment-resistant depression. J Affect Disord. (2023) 342:166–76. doi: 10.1016/j.jad.2023.09.030
71. Cepeda MS, Reps J, Ryan P. Findingfactorsthat predict treatment-resistant depression: results of a cohort study. Depress Anxiety. (2018) 35:668–73. doi: 10.1002/da.22774
72. Fabbri C, Hagenaars SP, John C, Williams AT, Shrine N, Moles L, et al. Genetic and clinical characteristics of treatment-resistant depression using primary care records in two UK cohorts. Mol Psychiatry. (2021) 26:3363–73. doi: 10.1038/s41380-021-01062-9
73. Brendle M, Ahuja S, Valle MD, Moore C, Thielking P, Malone DC, et al. Safety and effectiveness of intranasal esketamine for treatment-resistant depression: a real-world retrospective study. J Comp Eff Res. (2022) 11:1323–36. doi: 10.2217/cer-2022-0149
74. Lundberg J, Cars T, Lööv SÅ, Söderling J, Sundström J, Tiihonen J, et al. Association of treatment-resistant depression with patient outcomes and health care resource utilization in a population-wide study. JAMA Psychiatry. (2023) 80:167–75. doi: 10.1001/jamapsychiatry.2022.3860
75. Daly EJ, Turkoz I, Salvadore G, Fedgchin M, Ionescu DF, Starr HL, et al. The effect of esketamine in patients with treatment-resistant depression with and without comorbid anxiety symptoms or disorder. Depression Anxiety. (2021) 38:1120–30. doi: 10.1002/da.23193
76. Rothärmel M, Benosman C, El-Hage W, Berjamin C, Ribayrol D, Guillin O, et al. Efficacy and safety of intranasal esketamine in patients with treatment-resistant depression and comorbid chronic post-traumatic stress disorder: open-label single-arm pilot study. Front Psychiatry. (2022) 13:865466. doi: 10.3389/fpsyt.2022.865466
77. Chiappini S, d’Andrea G, De Filippis S, Di Nicola M, Andriola I, Bassetti R, et al. Esketamine in treatment-resistant depression patients comorbid with substance-use disorder: A viewpoint on its safety and effectiveness in a subsample of patients from the REAL-ESK study. Eur Neuropsychopharmacol. (2023) 74:15–21. doi: 10.1016/j.euroneuro.2023.04.011
78. Marcatili M, Cristian P, Laura M, Federico M, Chiara R, Lorenzo G, et al. The use of esketamine in comorbid treatment resistant depression and obsessive compulsive disorder following extensive pharmacogenomic testing: a case report. Ann Gen Psychiatry. (2021) 20:1–7. doi: 10.1186/s12991-021-00365-z
79. Keeler JL, Treasure J, Himmerich H, Brendle M, Moore C, Robison R. Case report: Intramuscular ketamine or intranasal esketamine as a treatment in four patients with major depressive disorder and comorbid anorexia nervosa. Front Psychiatry. (2023) 14:1181447. doi: 10.3389/fpsyt.2023.1181447
80. Johnson&Johnson. Available online at: https://www.jnj.com/janssen-announces-u-s-fda-approval-of-spravato-esketamine-ciii-nasal-spray-to-treat-depressive-symptoms-in-adults-with-major-depressive-disorder-with-acute-suicidal-ideation-or-behavior.
81. Pompili M. Intranasal esketamine and current suicidal ideation with intent in major depression disorder: beat the clock, save a life, start a strategy. Front Psychiatry. (2020) 11:325. doi: 10.3389/fpsyt.2020.00325
82. Yang S, Wang J, Li X, Wang T, Xu Z, Xu X, et al. Adverse effects of esketamine for the treatment of major depression disorder: findings from randomized controlled trials. Psychiatr Q. (2022) 93:81–95. doi: 10.1007/s11126-020-09871-x
83. Wajs E, Aluisio L, Holder R, Daly EJ, Lane R, Lim P, et al. Esketamine nasal spray plus oral antidepressant in patients with treatment-resistant depression: assessment of long-term safety in a phase 3, open-label study (SUSTAIN-2). J Clin Psychiatry. (2020) 81(3):19m12891. doi: 10.4088/JCP.19m12891
84. Williamson D, Turkoz I, Wajs E, Singh JB, Borentain S, Drevets WC. Adverse events and measurement of dissociation after the first dose of esketamine in patients with TRD. Int J Neuropsychopharmacol. (2023) 26:198–206. doi: 10.1093/ijnp/pyac081
85. Zaki N, Chen LN, Lane R, Doherty T, Drevets WC, Morrison RL, et al. Long-term safety and maintenance of response with esketamine nasal spray in participants with treatment-resistant depression: interim results of the SUSTAIN-3 study. Neuropsychopharmacology. (2023) 48:1225–33. doi: 10.1038/s41386-023-01577-5
86. Martinotti G, Vita A, Fagiolini A, Maina G, Bertolino A, Dell’Osso B, et al. Real-world experience of esketamine use to manage treatment-resistant depression: A multicentric study on safety and effectiveness (REAL-ESK study). J Affect Disord. (2022) 319:646–54. doi: 10.1016/j.jad.2022.09.043
87. Ballard ED, Zarate CA Jr. The role of dissociation in ketamine’s antidepressant effects. Nat Commun. (2020) 11:6431. doi: 10.1038/s41467-020-20190-4
88. Chen G, Chen L, Zhang Y, Li X, Lane R, Lim P, et al. Relationship between dissociation and antidepressant effects of esketamine nasal spray in patients with treatment-resistant depression. Int J Neuropsychopharmacol. (2022) 25:269–79. doi: 10.1093/ijnp/pyab084
89. Mathai DS, Nayak SM, Yaden DB, Garcia-Romeu A. Reconsidering “dissociation” as a predictor of antidepressant efficacy for esketamine. Psychopharmacology. (2023) 240:827–36. doi: 10.1007/s00213-023-06324-8
90. Bernstein EM, Putnam FW. Development, reliability, and validity of a dissociation scale. J Nerv Ment Dis. (1986) 174:727–35. doi: 10.1097/00005053-198612000-00004
91. Pereira S, Brennan E, Patel A, Moran M, Wallier J, Liebowitz MR. Managing dissociative symptoms following the use of esketamine nasal spray: a case report. Int Clin Psychopharmacol. (2021) 36:54–7. doi: 10.1097/YIC.0000000000000327
92. Janssen Research & Development. Crossover study to evaluate the abuse potential of intranasal esketamine compared to racemic intravenous ketamine in nondependent, recreational drug users. Clinical trial registration: 108104. Raritan, NJ: Janssen Research & Development (2017).
93. Wang J, Khullar A, McIntyre RS, Swainson J. The Drug Liking and Craving Questionnaire (DLCQ) to evaluate addiction risk for ketamine and esketamine. Psychiatry Res Commun. (2022) 2:100018. doi: 10.1016/j.psycom.2021.100018
94. Food and Drug Administration. U.S. Department of health and human services, food and drug administration, center for drug evaluation and research. Assessment of abuse potential of drugs guidance for industry (2017). Available online at: https://www.fda.gov/media/116739/download (Accessed June 15, 2022).
95. Chubbs B, Wang J, Archer S, Chrenek C, Khullar A, Wolowyk M, et al. A survey of drug liking and cravings in patients using sublingual or intranasal ketamine for treatment resistant depression: A preliminary evaluation of real world addictive potential. Front Psychiatry. (2022) 13:1016439. doi: 10.3389/fpsyt.2022.1016439
96. Cuijpers P. From treatment resistance to sequential treatments of depression. World Psychiatry. (2023) 22:418–9. doi: 10.1002/wps.21138
97. Furukawa TA. Complexities of treatment-resistant depression: cautionary notes and promising avenues. World Psychiatry. (2023) 22:419–20. doi: 10.1002/wps.21139
98. Rush AJ. Challenges of research on treatment-resistant depression: a clinician’s perspective. World Psychiatry. (2023) 22:415–7. doi: 10.1002/wps.21136
99. Souery D. Treatment-resistant depression: where to find hope? World Psychiatry. (2023) 22:422–3. doi: 10.1002/wps.21141
100. Popova V, Daly EJ, Trivedi M, Cooper K, Lane R, Lim P, et al. Efficacy and safety of flexibly dosed esketamine nasal spray combined with a newly initiated oral antidepressant in treatment-resistant depression: A randomized double-blind active-controlled study. Am J Psychiatry. (2019) 176:428–38. doi: 10.1176/appi.ajp.2019.19020172
101. Fedgchin M, Trivedi M, Daly EJ, Melkote R, Lane R, Lim P, et al. Efficacy and safety of fixed-dose esketamine nasal spray combined with a new oral antidepressant in treatment-resistant depression: results of a randomized, double-blind, active-controlled study (TRANSFORM-1). Int J Neuropsychopharmacol. (2019) 22:616–30. doi: 10.1093/ijnp/pyz039
102. Ochs-Ross R, Daly EJ, Zhang Y, Lane R, Lim P, Morrison RL, et al. Efficacy and safety of esketamine nasal spray plus an oral antidepressant in elderly patients with treatment-resistant depression-TRANSFORM-3. Am J Geriatr Psychiatry. (2020) 28:121–41. doi: 10.1016/j.jagp.2019.10.008
103. Daly EJ, Trivedi MH, Janik A, Li H, Zhang Y, Li X, et al. Efficacy of esketamine nasal spray plus oral antidepressant treatment for relapse prevention in patients with treatment-resistant depression: A randomized clinical trial. JAMA Psychiatry. (2019) 76:893–903. doi: 10.1001/jamapsychiatry.2019.1189
104. Jeon HJ, Ju PC, Sulaiman AH, Aziz SA, Paik JW, Tan W, et al. Long-term safety and efficacy of esketamine nasal spray plus an oral antidepressant in patients with treatment-resistant depression- an asian sub-group analysis from the SUSTAIN-2 study. Clin Psychopharmacol Neurosci. (2022) 20:70–86. doi: 10.9758/cpn.2022.20.1.70
105. d’Andrea G, Chiappini S, McIntyre RS, Stefanelli G, Carullo R, Andriola I, et al. Investigating the effectiveness and tolerability of intranasal esketamine among older adults with treatment-resistant depression (TRD): A post-hoc analysis from the REAL-ESK study group. Am J Geriatr Psychiatry. (2023) 31:1032–41. doi: 10.1016/j.jagp.2023.06.016
106. Leichsenring F, Steinert C, Rost F, Abbass A, Heim N, Ioannidis JPA. A critical assessment of NICE guidelines for treatment of depression. World Psychiatry. (2023) 22:43–5. doi: 10.1002/wps.21039
107. Serafini G, Howland RH, Rovedi F, Girardi P, Amore M. The role of ketamine in treatment-resistant depression: a systematic review. Curr Neuropharmacol. (2014) 12:444–61. doi: 10.2174/1570159X12666140619204251
108. Gałuszko-Węgielnik M, Chmielewska Z, Jakuszkowiak-Wojten K, Wiglusz MS, Cubała WJ. Ketamine as add-on treatment in psychotic treatment-resistant depression. Brain Sci. (2023) 13:142. doi: 10.3390/brainsci13010142
109. Kokane SS, Armant RJ, Bolaños-Guzmán CA, Perrotti LI. Overlap in the neural circuitry and molecular mechanisms underlying ketamine abuse and its use as an antidepressant. Behav Brain Res. (2020) 384:112548. doi: 10.1016/j.bbr.2020.112548
110. Sapkota A, Khurshid H, Qureshi IA, Jahan N, Went TR, Sultan W, et al. Efficacy and safety of intranasal esketamine in treatment-resistant depression in adults: A systematic review. Cureus. (2021) 13:e17352. doi: 10.7759/cureus.17352
111. Ceban F, Rosenblat JD, Kratiuk K, Lee Y, Rodrigues NB, Gill H, et al. Prevention and management of common adverse effects of ketamine and esketamine in patients with mood disorders. CNS Drugs. (2021) 35:925–34. doi: 10.1007/s40263-021-00846-5
112. McIntyre RS, Rosenblat JD, Nemeroff CB, Sanacora G, Murrough JW, Berk M, et al. Synthesizing the evidence for ketamine and esketamine in treatment-resistant depression: an international expert opinion on the available evidence and implementation. Am J Psychiatry. (2021) 178:383–99. doi: 10.1176/appi.ajp.2020.20081251
113. Swainson J, McGirr A, Blier P, Brietzke E, Richard-Devantoy S, Ravindran N, et al. The Canadian Network for Mood and Anxi- ety Treatments (CANMAT) Task Force recommendations for the use of racemic ketamine in adults with major depressive disorder: recommandations Du Groupe De Travail Du Reíseau Canadien Pour Les Traitements De L’humeur Et De L’anxieíteí (Canmat) Concernant L’utilisation de la Keítamine Raceímique Chez Les Adultes Souffrant De Trouble Deípressif Majeur. Can J Psychiatry. (2021) 66:113–25. doi: 10.1177/07067437
114. Doty RL, Popova V, Wylie C, Fedgchin M, Daly E, Janik A, et al. Effect of esketamine nasal spray on olfactory function and nasal tolerability in patients with treatment-resistant depression: results from four multicenter, randomized, double-blind, placebo-controlled, phase III studies. CNS Drugs. (2021) 35:781–94. doi: 10.1007/s40263-021-00826-9
115. Kasper S, Cubała WJ, Fagiolini A, Ramos-Quiroga JA, Souery D, Young AH. Practical recommendations for the management of treatment-resistant depression with esketamine nasal spray therapy: Basic science, evidence-based knowledge and expert guidance. World J Biol Psychiatry. (2021) 22:468–82. doi: 10.1080/15622975.2020.1836399
Keywords: treatment-resistant depression, esketamine, major depressive disorder, recovery, remission
Citation: Di Vincenzo M, Martiadis V, Della Rocca B, Arsenio E, D’Arpa A, Volpicelli A, Luciano M, Sampogna G and Fiorillo A (2024) Facts and myths about use of esketamine for treatment-resistant depression: a narrative clinical review. Front. Psychiatry 15:1394787. doi: 10.3389/fpsyt.2024.1394787
Received: 02 March 2024; Accepted: 22 April 2024;
Published: 15 May 2024.
Edited by:
Keming Gao, Case Western Reserve University, United StatesReviewed by:
Carlo Ignazio Cattaneo, Novara Medical School, ItalyCopyright © 2024 Di Vincenzo, Martiadis, Della Rocca, Arsenio, D’Arpa, Volpicelli, Luciano, Sampogna and Fiorillo. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Gaia Sampogna, Z2FpYS5zYW1wb2duYUBnbWFpbC5jb20=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.