 Alireza Jafari1†
Alireza Jafari1† Fatemehzahra Naddafi2†
Fatemehzahra Naddafi2† Mahbobeh Nejatian3
Mahbobeh Nejatian3 Elham Charoghchian Khorasani4,5
Elham Charoghchian Khorasani4,5 Hadi Tehrani4,5*
Hadi Tehrani4,5*- 1Department of Health Education and Health Promotion, School of Health, Social Development and Health Promotion Research Center, Gonabad University of Medical Sciences, Gonabad, Iran
- 2Student Research Committee, Gonabad University of Medical Sciences, Gonabad, Iran
- 3Social Determinants of Health Research Center, Gonabad University of Medical Sciences, Gonabad, Iran
- 4Social Determinants of Health Research Center, Mashhad University of Medical Sciences, Mashhad, Iran
- 5Department of Health Education and Health Promotion, School of Health, Mashhad University of Medical Sciences, Mashhad, Iran
Introduction: The prevalence of depression in the community is high. Therefore, it is necessary to examine the information needs on depression in the community. This cross-sectional study aimed to translate and evaluate the psychometric properties of the Depression Information Needs Scale (DINS) among the general population.
Methods: The translation and assessment of the validity and reliability of the DINS were conducted from February 2022 to May 2023 in Gonabad, Iran. The inclusion criteria in this study were individuals 18 years or older, those living in Gonabad for 1 year or more, and participants who provided written informed consent. Sample sizes of 546 and 629 were used for the exploratory factor analysis (EFA) and confirmatory factor analysis (CFA), respectively. The reliability of the DINS was examined using three methods: McDonald’s omega coefficient, test–retest reliability, and Cronbach’s alpha coefficient.
Results: Most participants were women, had a bachelor’s degree, and were married. The values of 0.959 for scale content validity index averaging (S-CVI/Ave) and 0.817 for content validity ratio (CVR) were calculated. In the EFA section, four factors with eigenvalues greater than 1 were extracted and explained 63.861% of the variance. Only two items were not placed in related or acceptable factors and were deleted. Finally, based on the results of the goodness-of-fit indexes (e.g., RMSEA = 0.074, CFI = 0.944, NFI = 0.930, and GFI = 0.911), the scale was approved with 18 items and 4 factors: lived experience (4 items), general (facts about depression) (6 items), research and policies (4 items), and specific treatments (4 items). For all the DINS items, the McDonald’s omega coefficient, Cronbach’s alpha coefficient, and Intraclass Correlation Coefficient (ICC) were 0.953, 0.950, and 0.957, respectively.
Conclusion: The Persian version of the DINS was validated with 18 items and 4 factors, and this scale can be used to assess depression information needs in the general public and specific groups.
Introduction
Depression is one of the most common mental illnesses, affecting approximately 280 million people around the world. Depression is one of the main causes of suicide, the major cause of disability, and the second leading cause of death among individuals 15–29 years of age (1–4). A systematic review study in Iran has shown that 52% of Iranian elderly (5) and 42.3% of Iranian children suffer from depression (6). In another systematic review, 2.3% of men and 4.8% of Iranian women had major depression disorder (7).
Depression is associated with loss of pleasure, sadness, guilt, weak focus, appetite disorders, sleep disorders, and fatigue (8). Studies have shown that depression is associated with decreased social performance and quality of life and increased risks of chronic diseases such as hypertension, diabetes, coronary artery disease, and even death (3, 9, 10). Depression prevention can reduce the burden of depression disorders, the occurrence of new episodes of major depression disorder, and costs (11). One of the initial depression prevention strategies is education and public awareness programs (12, 13), which in turn strengthen individual empowerment, improve self-management, improve treatment, facilitate decision-making, and ultimately improve mental health (14).
Unfortunately, in mental health educational resources, individuals’ educational needs in terms of mental health are rarely considered, and it is necessary to conduct needs assessment before any educational intervention is conducted to ensure its effectiveness (14). Assessment of information needs identifies the gap between current and desired situations. Needs assessment also facilitates community participation in programs, creating a basis for program analysis and preventing resource loss (15, 16). It will not be possible to understand and recognize the needs for depression information without a valid and reliable tool (14).
A study by Ghadirian et al. in 2017 in a population of people aged 18 to 68 living in Tehran showed that approximately half of the participants were not only unable to identify the signs and symptoms of depression but also did not intend to seek help (17). These findings indicate that Iranian adults have unmet informational needs related to depression. In another study of medical students in Iran, it was found that approximately 64.4% of the students were not able to recognize the signs and symptoms of depression, which highlights the depth of this information gap because it is expected that medical students will have more knowledge in this field (18). The results of another study conducted in 2020 on the general Iranian population revealed an inadequacy of depression literacy in most participants (19). These studies collectively highlight the unmet informational needs of depression and the necessity of comprehensive needs assessment and the implementation of targeted educational interventions. Furthermore, these studies raise the possibility that previous education on depression was not based on individuals’ real information needs and was not successful in promoting depression literacy. Therefore, untargeted depression education could only result in a waste of public funds.
One of the best tools for examining depression information needs is the Depression Information Needs Scale (DINS), which was designed by Griffiths and Crisp. The questionnaire has 20 questions and 4 subscales of lived experience, general (facts about depression), specific treatments, and research and policies (14). Based on the our search, there was not a suitable instrument can assess the unmet information needs of the Iranian population regards to depression. Given the importance of depression and the information needs for this disease, this cross-sectional study aimed to translate the DINS into the Persian language and evaluate its psychometric properties among the Iranian general population.
Methods
This cross-sectional study was conducted in Iran involving 1,175 patients referred to health centers from February 2022 to May 2023.
Sample size
Based on the previous studies by Tabatchnick and Williams, the recommended sample size for this type of study would be 500 or more (20, 21). Different samples need to be performed for exploratory factor analysis (EFA) and confirmatory factor analysis (CFA) (22). In this psychometric study, EFA and CFA were assessed using different sample sizes: 546 for EFA and 629 for CFA.
Sampling
Stratified random sampling was applied in this study. Considering that the target population of this study involved adults aged 18 years and older, community health centers were selected as the most suitable locations for sampling. In these centers, all members of society in any age group, including children, teenagers, adults, and the elderly, have electronic health records, and in this way, they receive health services either by telephone or in person. As a result, these centers provided researchers with the most comprehensive sampling frameworks; thus, they were selected as our sampling settings. After selecting all Gonabad health centers (n = 3) as strata, simple random sampling was performed according to the sampling framework and population ratio of each center. The inclusion criteria in this study were individuals aged 18 years or older, those living in Gonabad for more than 1 year, and participants who provided written informed consent to participate in this study. The only exclusion criterion in this study was an incomplete response to the questionnaire (questionnaire with more than 20 % missing data).
Instruments
The DINS, developed by Griffiths and Crisp, is one of the instruments used for assessing depression information needs, with 20 items and 4 subscales: lived experience (with 5 items), general (facts about depression) (with 7 items), research and policies (with 4 items), and specific treatments (with 4 items) (14). The items were scored using a five-point Likert scale, with 0 indicating completely disagree and 4 indicating completely agree. The minimum score is 0 and the maximum is 80, and a high score indicates that people need more information on depression (14). The validity results of this tool provided four factors, and the DINS had good reliability (Cronbach’s alpha coefficients of the general subscales, specific treatment, research and policies, and lived experience were 0.95, 0.92, 0.91, and 0.96, respectively) (14).
Translation and cultural adaptation
At first required written consent was obtained from Dr. Kathy Griffiths. After that, the DINS was translated according to the translation and cultural adaptation guidelines (23). First, two translators were recruited to translate the DINS from the original language into the target language (English to Persian). In the second stage, the research team combined the two translations and discussed possible differences. In the third step, two translators translated the combined version of the second step from the target language to the original language (Persian to English). In the fourth step, the two English translations were merged, and the merged English version was translated into Persian in the final step and used to evaluate the validity and reliability of the DINS.
Validity
To assess the content and face validity, the tool was sent to 11 experts (psychology professionals and specialists in health education and promotion), and their comments were used in the questionnaire. Also, qualitative face validity of the items of DINS were evaluated by 11 people in target group. Quantitative content validity was assessed using content validity ratio (CVR) and scale content validity index averaging (S-CVI/Ave). In the S-CVI/Ave section, each question of the DINS was assessed in terms of relevance (24), and a value >0.9 is acceptable for the S-CVI/Ave section (25), and a value >0.59 is acceptable for CVR (26). The modified kappa value was also calculated for each DINS item. A value from 0.40 to 0.59 is fair, a value from 0.60 to 0.74 is good, and a value >0.74 is excellent (24, 27).
EFA
Exploratory factor analysis was used to identify extractable factors. To this end, a factor loading ≥0.4, a scree map, and a maximum of 25 rotation repetitions were considered (28, 29). To perform the EFA, sample size sufficiency was assessed by Bartlett’s Test of Sphericity (BTS) and Kaiser–Meyer–Olkin (KMO) (30, 31). This section was implemented using SPSS v24.
CFA
Factors extracted in EFA were assessed in CFA using AMOS v24. In this section, to prepare the data for analysis, the Mahalanobis test was used to find the outlier data. To check the data normality, skewness and kurtosis were used. After preparing the data, factors extracted were evaluated by goodness-of-fit indexes such as the comparative fit index (CFI), Tucker–Lewis index (TLI), parsimonious normed fit index (PNFI), relative fit index (RFI), chi-square (χ2), degree of freedom (df), parsimony comparative fit index (PCFI), normed fit index (NFI), incremental fit index (IFI), root mean square error of approximation (RMSEA), and goodness-of-fit index (GFI) (32–34). Based on the literature, the acceptable value for each goodness-of-fit index is IFI >0.9, TLI >0.9, PNFI >0.5, RMSEA <0.08, GFI >0.9, NFI >0.9, CFI >0.9, χ2/df <5, PCFI >0.5, and RFI >0.9 (32–35).
Reliability
The reliability of the DINS was examined using three methods: McDonald’s omega coefficient, test–retest reliability, and Cronbach’s alpha. In test–retest reliability, the Intraclass Correlation Coefficient (ICC) was calculated. To check the reliability, 37 participants were studied, and the questionnaire was completed two times; the second time was 1 month after the first time. To evaluate reliability, two software programs (JASP v0.11.1.0 and SPSS v24) were used. Regarding Cronbach’s alpha, 0.6 ≤ α ≤ 0.7 is acceptable and α ≥0.8 is very good (36). ICC >0.9 is excellent, 0.75 ≤ ICC ≤ 0.9 is good, 0.5 ≤ ICC ≤ 0.75 is moderate, and ICC <0.5 is poor (37). In general, a reliability coefficient greater than 0.70 is acceptable (38).
Results
Demographic characteristics
In EFA, 51.1% (n = 279) were male, and in CFA, 53.7% (n = 338) were female (Table 1). In the EFA and CFA, the mean (SD) age of the participants was 33.91 (13.12) and 33.17 (13), respectively.
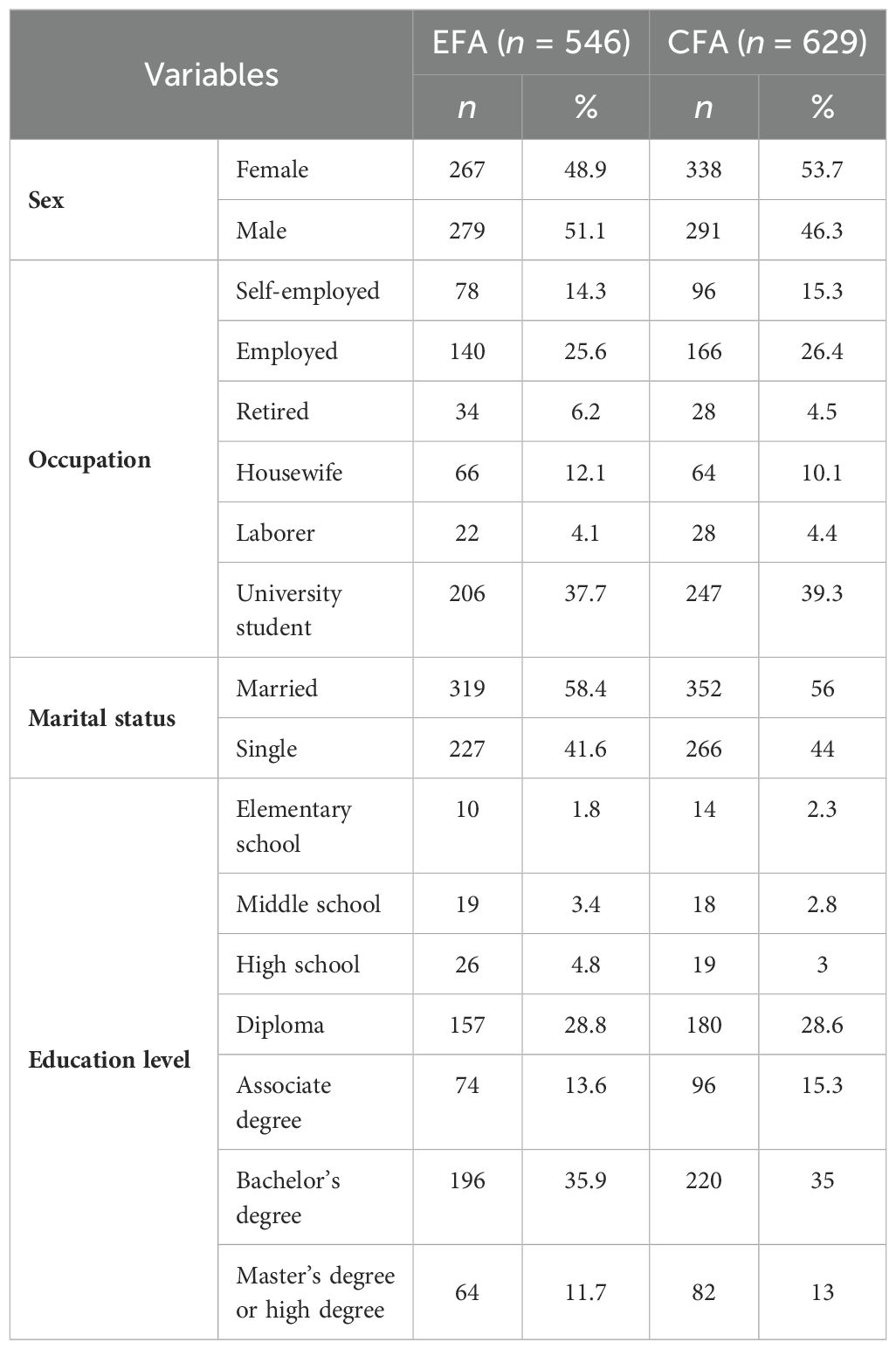
Table 1. Frequency distribution of demographic characteristics.
Face and content validity
After the validity assessment by 11 experts, two items in qualitative face validity and three items in qualitative content validity were modified (using simple and appropriate Persian words), respectively. In terms of quantitative content validity, values of 0.959 for S-CVI/Ave and 0.817 for CVR were calculated. The modified kappa for the 18 items was excellent, and the value for all items was 0.926 (Table 2).
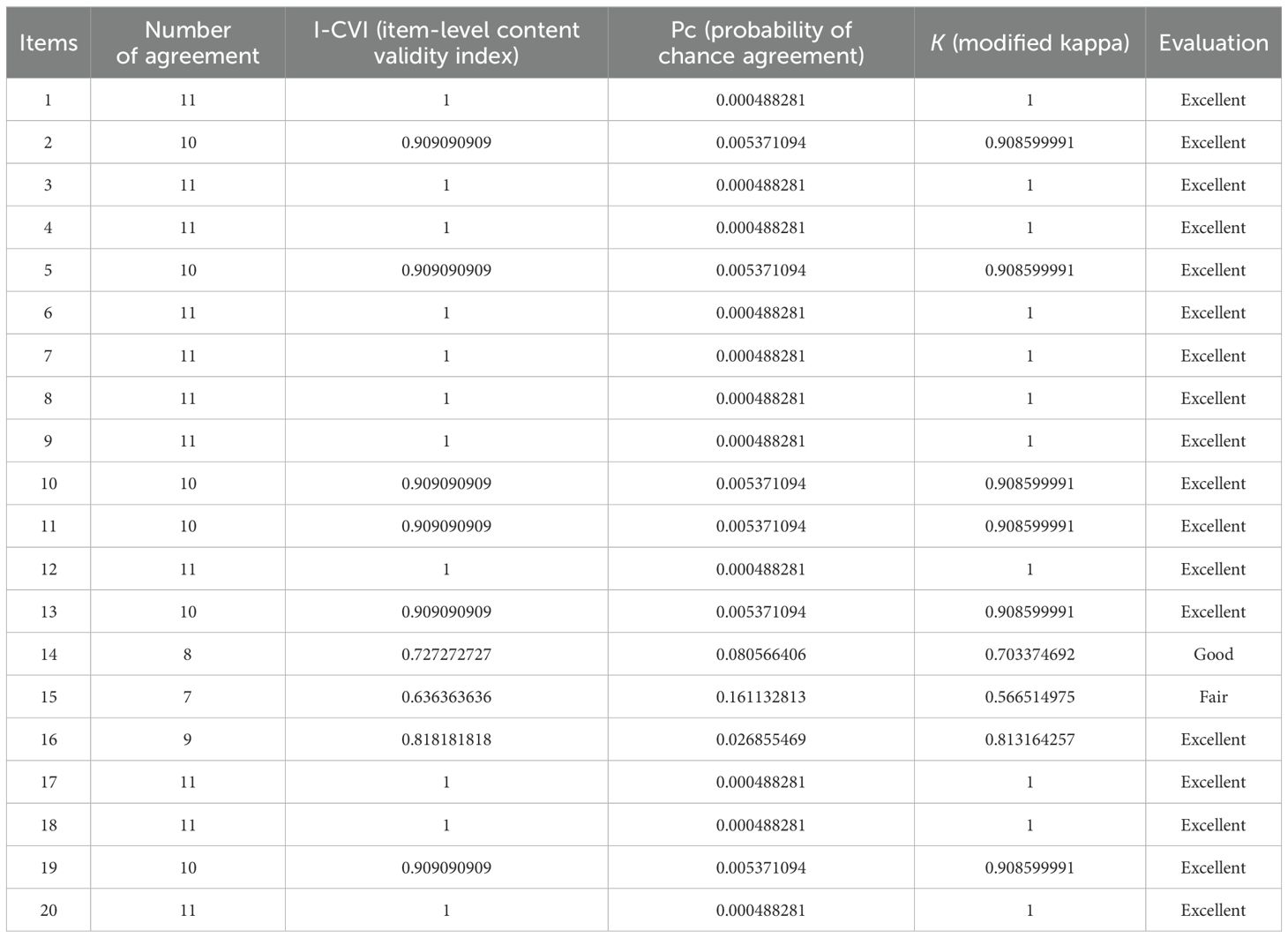
Table 2. The I-CVI and modified kappa for each item of the DINS.
EFA section
There were no missing data in this section. The results of the KMO (0.936) and BTS (χ2 = 7,603.659, df = 190, P < 0.001) showed that the samples were sufficient for EFA. In this section, four factors with eigenvalues greater than 1 were extracted and explained 63.861% of the variance (Table 3, Figure 1). The results of Table 4 show the place of each item in extracted factors and based on the original scale; only two items did not place in related and acceptable factors. Item D7 (“How I can help someone who is depressed”) moved from the general (facts about depression) factor to the lived experience factor, and item D12 (“People’s experiences of which treatments work for their depression”) moved from the lived experience factor to the specific treatments factor. After checking these results, two items, i.e., D7 and D12, were deleted (Table 4).
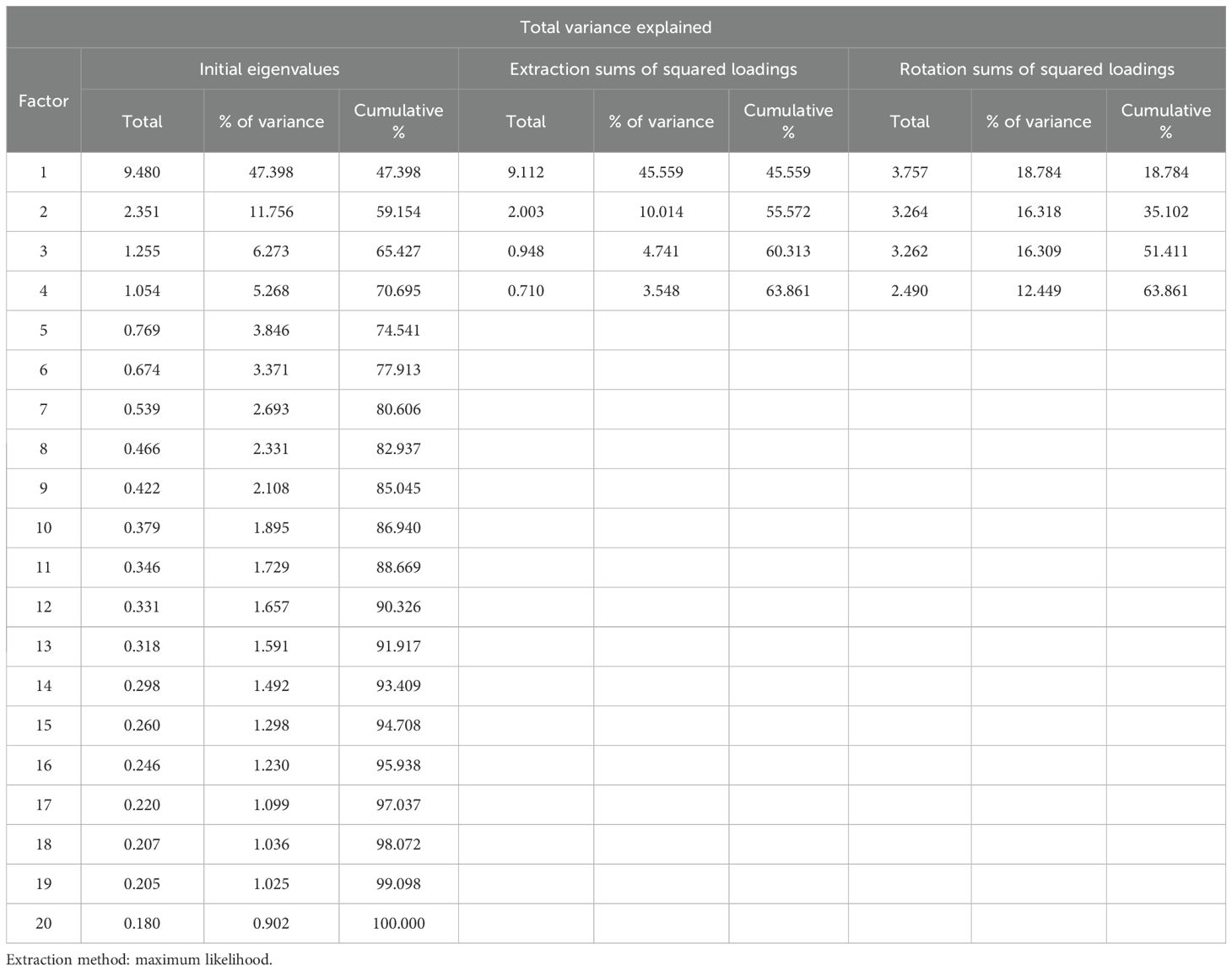
Table 3. The four-factor structure of the Persian version of the DINS.
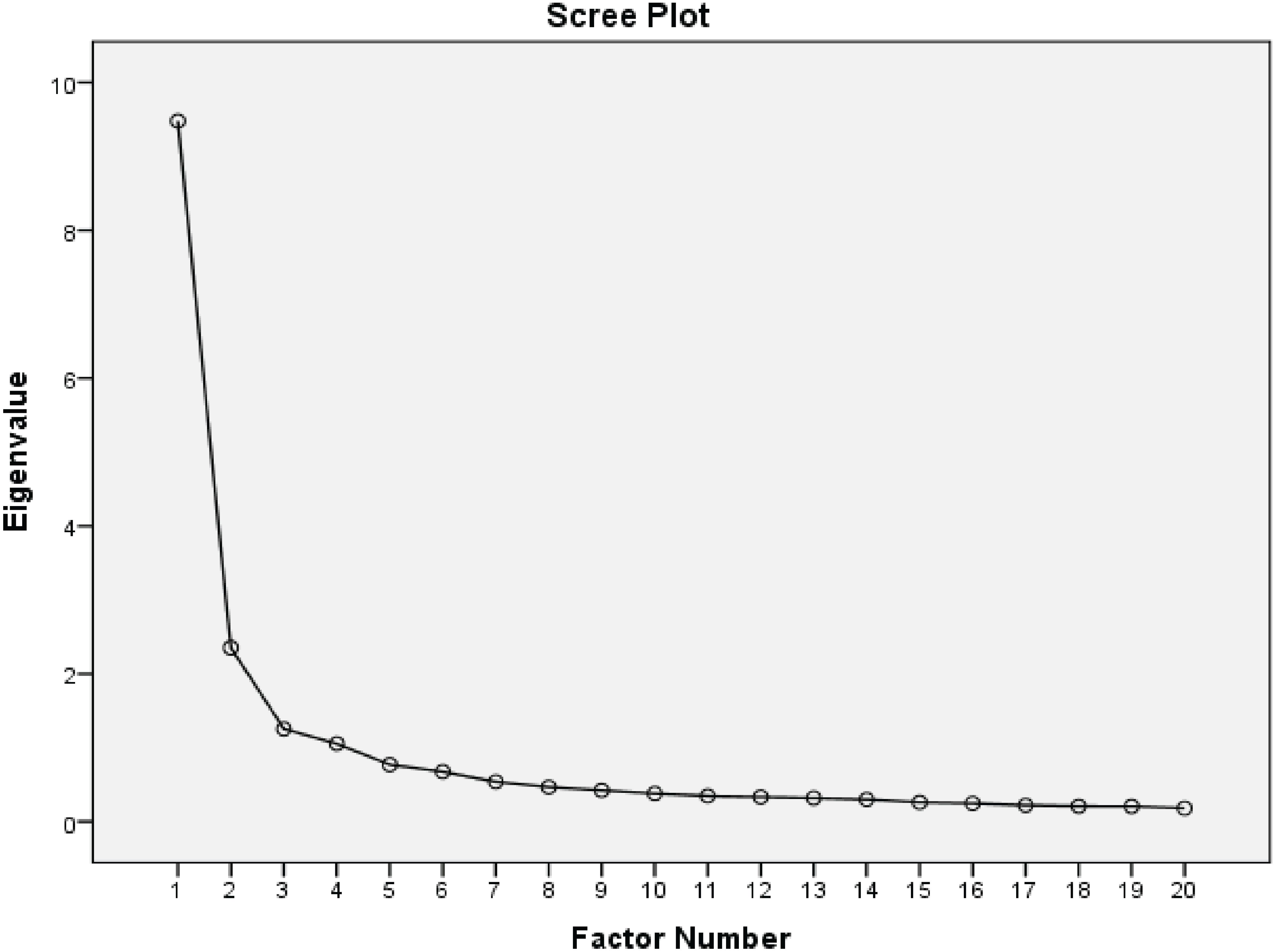
Figure 1. Scree plot of the factor analysis of the Persian version of the DINS.
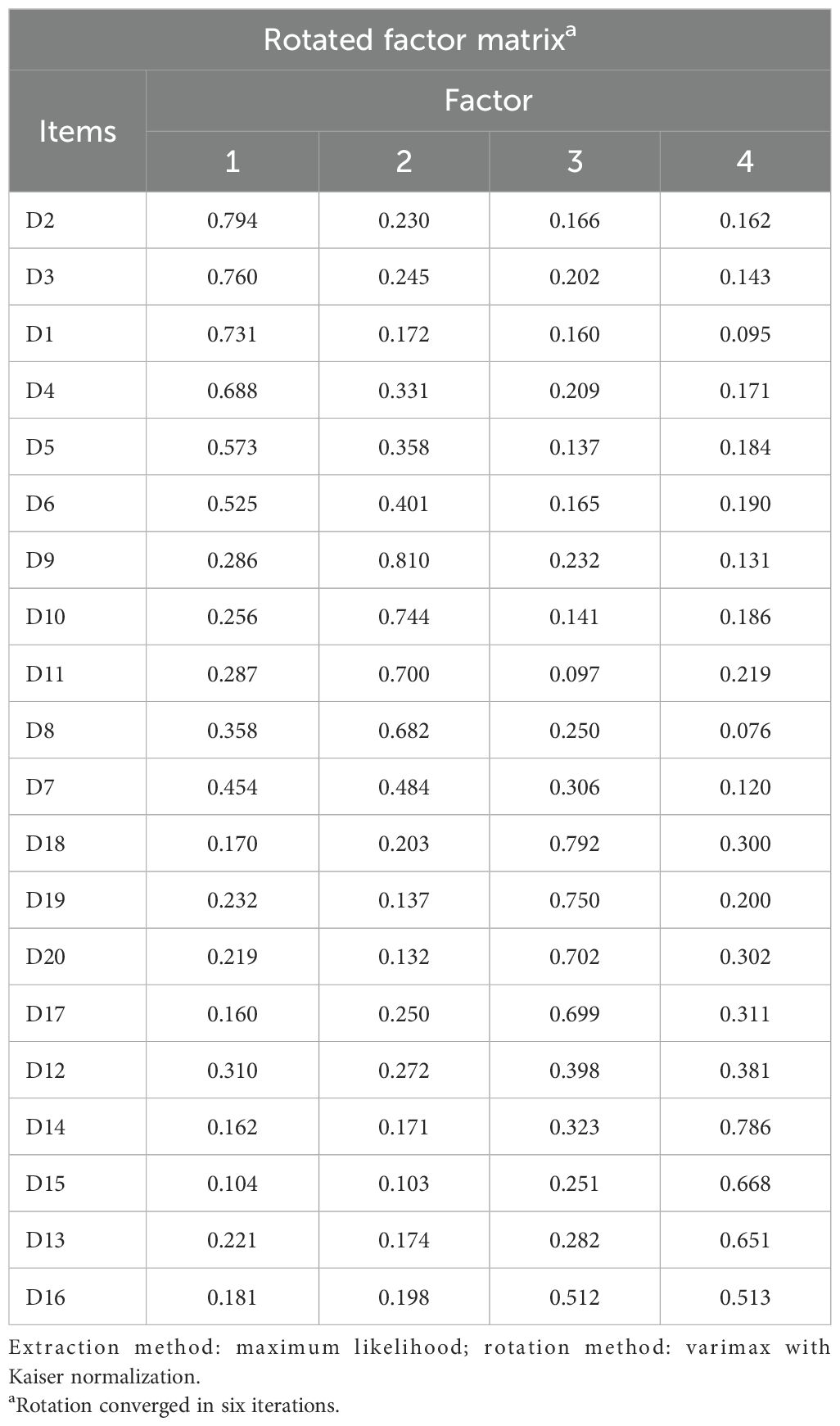
Table 4. Rotated factor matrix of the Persian version of the DINS.
CFA section
In this section, data were normal and there were no missing data. After that, four extracted factors with 18 items were evaluated by CFA. The results of Table 5 show that the factor loading of all items was greater than 0.7 (Table 5, Figure 2). Based on the results of Table 6, the model fit indicators (such as RMSEA = 0.074, NFI = 0.930) indicated that the final model was acceptable with 18 items and 4 factors: lived experience (4 items), general (facts about depression) (6 items), research and policies (4 items), and specific treatments (4 items) (Table 6). The final Persian version of the DINS was uploaded as Supplementary Material (Appendix 1).
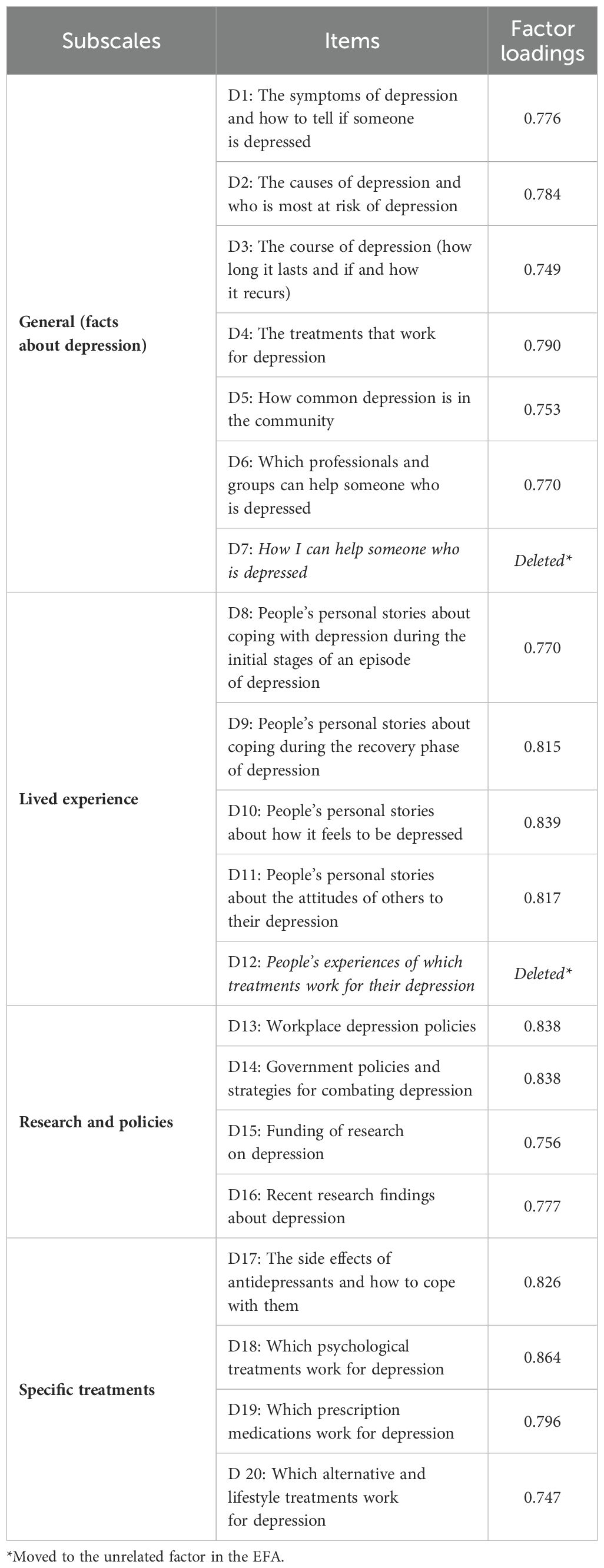
Table 5. Factor loadings of the Persian version of the DINS.
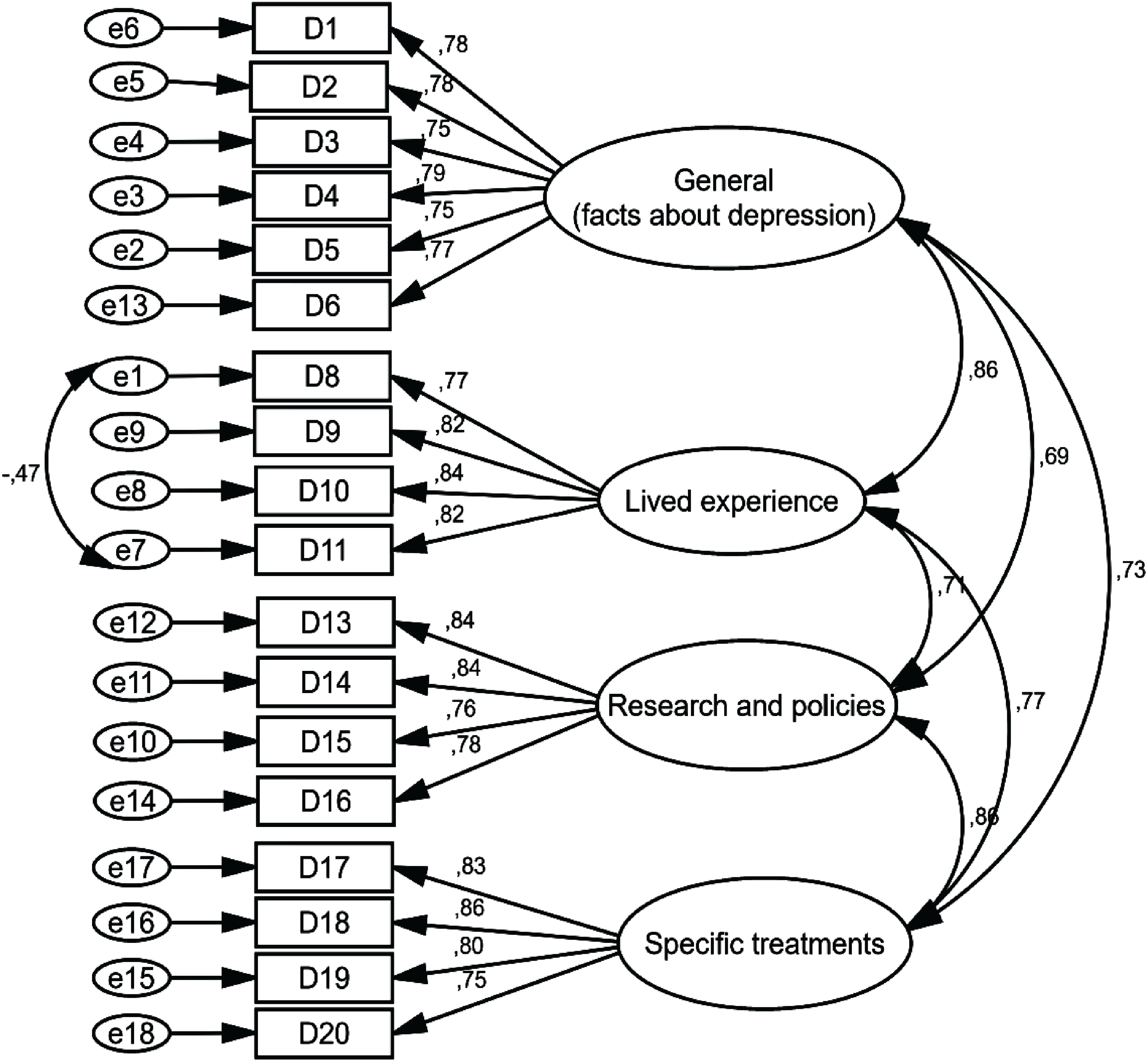
Figure 2. Standardized parameter estimates for the factor structure of the DINS.
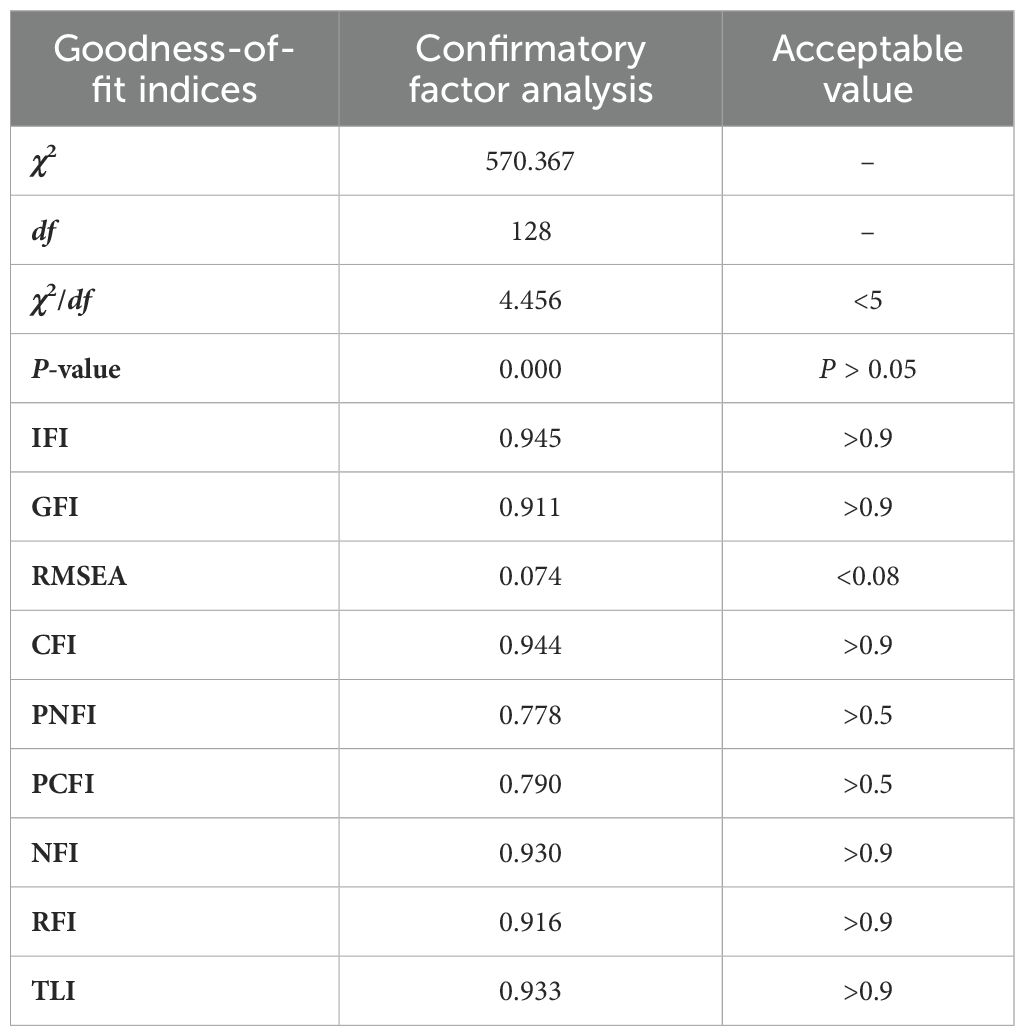
Table 6. The model fit indicators of the Persian version of the DINS.
Reliability section
Table 7 shows the scale reliability results. For all DINS items, the McDonald’s omega coefficient, Cronbach’s alpha coefficient, and ICC were 0.953, 0.950, and 0.957, respectively. The reliability of each factor is presented in Table 7.
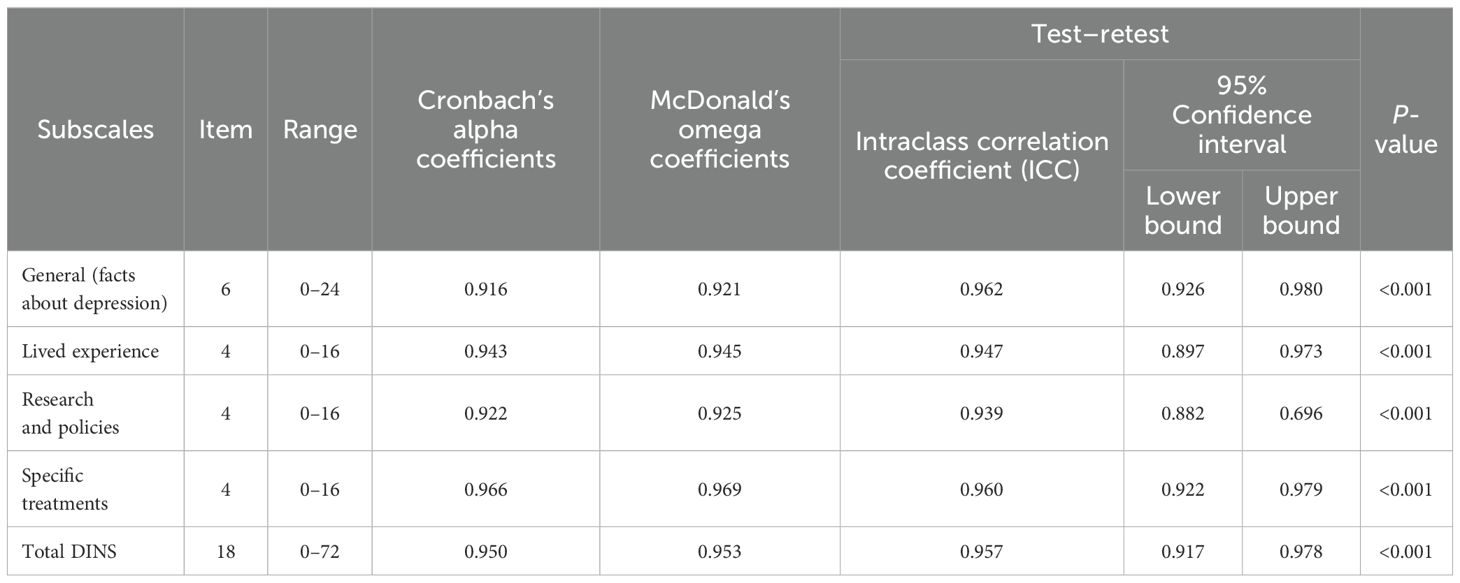
Table 7. Reliability and descriptive statistics of the Persian version of the DINS.
Discussion
This study aimed to evaluate the psychometric properties of DINS. In general, the Persian version of the DINS demonstrated robust psychometric properties.
Similar to the original DINS and according to the EFA results, the Persian version of the DINS also yielded four factors (general, lived experience, research and policies, and specific treatment) with specific values greater than 1 capable of predicting 63.861% of the variance. According to the EFA results, only two items were not in the relevant and acceptable factors, and 18 items were placed in the four main subscriptions. In addition, these four factors were examined in the CFA stage, and all questions in the questionnaire were confirmed.
In this study, the first factor was “general (facts about depression),” which was confirmed with six questions. This factor relates to the general facts of depression, including symptoms, causes, periods, treatment, outbreaks, and sources, and emphasizes that community members with depression have information needs regarding the general factors of the disease that must be properly available to them. The results of a study by Prins on perceived needs to take care of mental health and depression in the Netherlands showed that information needs were not provided by one-third of the participants about their illness or were provided at a very small amount (39). It is difficult to manage a disease when individuals with depression are not sufficiently well informed about their illness (40). On the other hand, numerous studies have shown that when people obtain accurate information about their illness, they are more likely to follow treatment, and unmet information needs can lead to delayed or inadequate treatment, poor adherence, increased stigma, and a higher risk of relapse or recurrence (41, 42). Therefore, a tool that can assess the depression information needs of individuals is necessary for conducting interventions.
According to the results of this study, the second factor to be approved was “lived experience,” which was confirmed by four questions. The lived experience factor refers to the personal experiences of people with depression regarding coping strategies during the acute period to improve their depression, their treatments, and others’ attitudes toward depression. In the study by Jorm et al., it was mentioned that the beliefs of people with experience of depression about mental disorders differ from those of health professionals. Therefore, patients with depression may have very different opinions from physicians regarding what interventions are useful (43). As a result, the experiences of depression patients can be part of the important information needs for the general people. Some studies have emphasized the critical role of lived experience perspectives in understanding and addressing the unique information needs of people with depression (2, 44). Therefore, incorporating these insights can lead to more impactful, person-centered resources and interventions to support those affected by this condition.
The third factor that was approved was “research and policies,” which was confirmed with four questions. The focus of this factor is on workplace policies, government policies, financing research, and research-related depression results. By understanding the specific areas where information is lacking and implementing policies that enhance access to this information, stakeholders can better support individuals struggling with depression. Patients’ information about the results of research on depression can help them better understand the disease and its effective treatments (45). Policies can also increase confidence among patients with depression in accessing the required care services. Therefore, awareness of research findings and policies is an important information requirement for people with mental disorders (46). Griffiths demonstrated that providing information about workplace laws and government policies to individuals suffering from depression, along with updates on the latest research findings in the field, significantly improved disease management and motivated patients to adhere to their treatment plans (14). Numerous studies underscore the critical role of research and policies in understanding, prioritizing, and addressing the multifaceted information needs of people with depression (2, 47). Therefore, by using an appropriate tool that can measure this factor, more comprehensive and effective informational resources and interventions can be developed to support people affected by depression.
According to the results of this study, the fourth factor that was approved was “specific treatments,” which was confirmed by four questions. This factor refers to information about specific treatments for depression and the side effects of treatments and psychological treatments. The results of a qualitative study by Fossey et al. showed that patients with mild to moderate mental disorders lack information regarding diagnosis and treatment options (48). Bowskill et al. also reported patient dissatisfaction with the information provided by health professionals for mental disorder therapies, including the nature, treatment period, and prescribed medications (49). In general, targeted information is important not only for patients with mental disorders but also for community members because mental health literacy is likely to help people diagnose the primary symptoms of mental illness and seek mental health services in the early stages of the disease (2). Various studies have emphasized the vital role of providing comprehensive and tailored information about specific treatment options to meet the needs of people with depression (14, 50). By prioritizing this aspect, healthcare providers and information resources can support depressed people in making informed choices about their care and participating more actively in the treatment process.
Strengths and limitations
The large sample size of this study and the fact that it was conducted in the public community were the strengths of the study, and the DINS is useful for different target groups. The use of a self-report questionnaire may introduce cognitive biases, which is a limitation of this research. Another limitation of this study was that it was conducted in a single region and city, which may limit the generalizability of the findings to a broader population of people with depression.
Conclusion
The Persian version of the DINS is of crucial importance at this juncture given the shift of focus and huge emphasis on mental health worldwide, including Iran. It is hoped that this scale will improve the quality of educational interventions related to depression and address the knowledge gap among the Iranian public. This scale can be used to evaluate the information needs of patients with depression, as well as the effect of various interventions to improve information. The scale can also serve as a basis for developing clinical guidelines for providing appropriate and targeted information to consumers with mental health. However, further research is required to confirm the validity and reliability of the DINS in different subgroups. The replication of the study in other regions, cities, or countries is also suggested to evaluate the transferability of the findings.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Materials. Further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving humans were approved by the Ethics Committee of Mashhad University of Medical Sciences with the code of ethics IR.MUMS.REC.1401.365. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
AJ: Validation, Software, Project administration, Methodology, Investigation, Formal analysis, Data curation, Writing – review & editing, Writing – original draft, Conceptualization. MN: Writing – review & editing, Writing – original draft, Methodology, Investigation, Data curation, Conceptualization. FN: Writing – review & editing, Writing – original draft, Investigation, Conceptualization. EC: Writing – review & editing, Writing – original draft, Investigation, Conceptualization. HT: Writing – review & editing, Writing – original draft, Validation, Supervision, Software, Project administration, Methodology, Investigation, Formal analysis, Conceptualization.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Acknowledgments
The authors of the study express their sincere gratitude of Mashhad University of Medical Sciences. We would also like to thank all the people who assisted us in conducting this research project.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2024.1388447/full#supplementary-material
Abbreviations
DINS, Depression Information Needs Scale; CVR, content validity ratio; S-CVI/Ave, scale content validity index averaging; EFA, exploratory factor analysis; KMO, Kaiser–Meyer–Olkin; CFA, confirmatory factor analysis; PCFI, parsimony comparative fit index; GFI, goodness-of-fit index; IFI, incremental fit index; RMSEA, root mean square error of approximation; PNFI, parsimonious normed fit index; χ2, chi-square; df, degree of freedom; CFI, comparative fit index; TLI, Tucker–Lewis index; RFI, relative fit index; NFI, normed fit index.
References
1. Aina B, Adebowale D. Knowledge and prevalence of depression among students on College of Medicine University of Lagos. Eur J Public Health. (2020) 30:ckaa166. doi: 10.1093/eurpub/ckaa166.1048
2. Chan FH, Lin X, Griva K, Subramaniam M, Ćelić I, Tudor Car L. Information needs and sources of information among people with depression and anxiety: a scoping review. BMC Psychiatry. (2022) 22:502. doi: 10.1186/s12888-022-04146-0
3. WHO. Depressive disorder (depression) (2023). Available online at: https://www.who.int/news-room/fact-sheets/detail/depression (Accessed: October 10, 2023).
4. Patria B. The longitudinal effects of education on depression: finding from the Indonesian national survey. Front Public Health. (2022) 10:1017995. doi: 10.3389/fpubh.2022.1017995
5. Jafari H, Ghasemi-Semeskandeh D, Goudarzian AH, Heidari T, Jafari-Koulaee A. Depression in the Iranian elderly: a systematic review and meta-analysis. J Aging Res. (2021) 2021:1–9. doi: 10.1155/2021/9305624
6. Zohrabi T, Ziaee A, Salehi-Abargouei A, Ferns GA, Ghayour-Mobarhan M, Khayyatzadeh SS. Dietary total anti-oxidant capacity is inversely related to the prevalence of depression in adolescent girls. BMC pediatrics. (2022) 22:1–10. doi: 10.1186/s12887-022-03589-4
7. Gharraee B, Tajrishi KZ, Sheybani F, Tahmasbi N, Mirzaei M, Farahani H, et al. Prevalence of major depressive disorder in the general population of Iran: A systematic review and meta-analysis. Med J Islamic Republic Iran. (2019) 33:151. doi: 10.47176/mjiri
8. Lim GY, Tam WW, Lu Y, Ho CS, Zhang MW, Ho RC. Prevalence of depression in the community from 30 countries between 1994 and 2014. Sci Rep. (2018) 8:2861. doi: 10.1038/s41598-018-21243-x
9. Alanazi A, Alsharif S, Alzahrani Z, Alanazi A. Knowledge and practice of depression management among primary healthcare physicians. J Family Med Primary Care. (2022) 11:2442–7. doi: 10.4103/jfmpc.jfmpc_2083_21
10. Kim J, Kim Y-K. Crosstalk between depression and dementia with resting-state fMRI studies and its relationship with cognitive functioning. Biomedicines. (2021) 9:82. doi: 10.3390/biomedicines9010082
11. Cuijpers P, Beekman AT, Reynolds CF. Preventing depression: a global priority. Jama. (2012) 307:1033–4. doi: 10.1001/jama.2012.271
12. Hoare E, Collins S, Marx W, Callaly E, Moxham-Smith R, Cuijpers P, et al. Universal depression prevention: An umbrella review of meta-analyses. J Psychiatr Res. (2021) 144:483–93. doi: 10.1016/j.jpsychires.2021.10.006
13. Mamun MA, Naher S, Moonajilin MS, Jobayar AM, Rayhan I, Kircaburun K, et al. Depression literacy and awareness programs among Bangladeshi students: an online survey. Heliyon. (2020) 6:e04901. doi: 10.1016/j.heliyon.2020.e04901
14. Griffiths KM, Crisp DA. Unmet depression information needs in the community. J Affect Disord. (2013) 146:348–54. doi: 10.1016/j.jad.2012.09.018
15. Garira E. Needs assessment for the development of educational interventions to improve quality of education: A case of Zimbabwean primary schools. Soc Sci Humanities Open. (2020) 2:100020. doi: 10.1016/j.ssaho.2020.100020
16. Li Y, Cao J, Lin H, Li D, Wang Y, He J. Community health needs assessment with precede-proceed model: a mixed methods study. BMC Health Serv Res. (2009) 9:1–14. doi: 10.1186/1472-6963-9-181
17. Ghadirian L, Sayarifard A. Depression literacy in urban and suburban residents of tehran, the capital of Iran; recognition, help seeking and stigmatizing attitude and the predicting factors. Int J Prev Med. (2019) 10:134. doi: 10.4103/ijpvm.IJPVM_166_18
18. Sayarifard A, Ghadirian L, Mohit A, Eftekhar M, Badpa M, Rajabi F. Assessing mental health literacy: What medical sciences students’ know about depression. Med J Islamic Republic Iran. (2015) 29:161.
19. Tehrani H, Vali M, Nejatian M, Moshki M, Charoghchian Khorasani E, Jafari A. The status of depression literacy and its relationship with quality of life among Iranian public population: a cross sectional study. BMC Psychiatry. (2022) 22:607. doi: 10.1186/s12888-022-04251-0
20. Tabatchnick BG, Fidell LS. (2001). Using multivariate statistics. 4th Edition, Allyn and Bacon, Boston.
21. Williams B, Onsman A, Brown T. Exploratory factor analysis: a five-step guide for novices. Australas J Paramedicine. (2010) 8:1–13. doi: 10.33151/ajp.8.3.93
22. Fokkema M, Greiff S. How performing PCA and CFA on the same data equals trouble: overfitting in the assessment of internal structure and some editorial thoughts on it. Eur J Psychol Assess. (2017) 33:399402. doi: 10.1027/1015-5759/a000460
23. Sousa VD, Rojjanasrirat W. Translation, adaptation and validation of instruments or scales for use in cross-cultural health care research: a clear and user-friendly guideline. J Eval Clin practice. (2011) 17:268–74. doi: 10.1111/j.1365-2753.2010.01434.x
24. Polit DF, Beck CT, Owen SV. Is the CVI an acceptable indicator of content validity? Appraisal and recommendations. Res Nurs Health. (2007) 30:459–67. doi: 10.1002/nur.20199
25. Shi J, Mo X, Sun Z. Content validity index in scale development. Zhong Nan Da Xue Xue Bao Yi Xue Ban. (2012) 37:152–5. doi: 10.3969/j.issn.1672-7347.2012.02.007
26. Lawshe CH. A quantitative approach to content validity 1. Personnel Psychol. (1975) 28:563–75. doi: 10.1111/j.1744-6570.1975.tb01393.x
27. Cicchetti DV, Sparrow SA. Developing criteria for establishing interrater reliability of specific items: applications to assessment of adaptive behavior. Am J Ment deficiency. (1981) 86:127–37.
30. Kaiser HF, Rice J. Little jiffy, mark IV. Educ psychol measurement. (1974) 34:111–7. doi: 10.1177/001316447403400115
31. Harrington D. Confirmatory factor analysis (Illustrated ed.). US: Oxford University Press (2008).
32. Henry JW, Stone RW. A structural equation model of end-user satisfaction with a computer-based medical information system. Inf Resour Manage J (IRMJ). (1994) 7:21–33. doi: 10.4018/IRMJ
33. Lomax RG, Schumacker RE. (2004). A beginner’s guide to structural equation modeling: psychology press. New York, Psychology Press.
34. Kline R. Details of path analysis. Principles and practice of structural equation modeling. New York: Guilford (2005).
35. Schreiber JB, Nora A, Stage FK, Barlow EA, King J. Reporting structural equation modeling and confirmatory factor analysis results: A review. J Educ Res. (2006) 99:323–38. doi: 10.3200/JOER.99.6.323-338
36. Ursachi G, Horodnic IA, Zait A. How reliable are measurement scales? External factors with indirect influence on reliability estimators. Proc Economics Finance. (2015) 20:679–86. doi: 10.1016/S2212-5671(15)00123-9
37. Koo TK, Li MY. A guideline of selecting and reporting intraclass correlation coefficients for reliability research. J Chiropr Med. (2016) 15:155–63. doi: 10.1016/j.jcm.2016.02.012
38. Viladrich C, Angulo-Brunet A, Doval E. A journey around alpha and omega to estimate internal consistency reliability. Anales Psicologia. (2017) 33:755–82. doi: 10.6018/analesps.33.3.268401
39. Prins MA, Verhaak PF, Bensing JM, van der Meer K. Health beliefs and perceived need for mental health care of anxiety and depression—The patients’ perspective explored. Clin Psychol review. (2008) 28:1038–58. doi: 10.1016/j.cpr.2008.02.009
40. Barney LJ, Griffiths KM, Banfield MA. Explicit and implicit information needs of people with depression: a qualitative investigation of problems reported on an online depression support forum. BMC Psychiatry. (2011) 11:1–11. doi: 10.1186/1471-244X-11-88
41. Stevenson W, Bryant J, Watson R, Sanson-Fisher R, Oldmeadow C, Henskens F, et al. A multi-center randomized controlled trial to reduce unmet needs, depression, and anxiety among hematological cancer patients and their support persons. J Psychosocial Oncol. (2020) 38:272–92. doi: 10.1080/07347332.2019.1692991
42. Møller J-JK, Jespersen E, Lindahl-Jacobsen R, Ahrenfeldt LJ. Associations between perceived information needs and anxiety/depressive symptoms among cancer caregivers: A cross-sectional study. J psychosocial Oncol. (2020) 38:171–87. doi: 10.1080/07347332.2019.1664699
43. Jorm AF, Korten AE, Jacomb PA, Rodgers B, Pollitt P, Christensen H, et al. Helpfulness of interventions for mental disorders: beliefs of health professionals compared with the general public. Br J Psychiatry. (1997) 171:233–7. doi: 10.1192/bjp.171.3.233
44. Sheikh A, Jacob J, Vostanis P, Ruby F, Spuerck I, Stankovic M, et al. What should personalised mental health support involve? views of young people with lived experience and professionals from eight countries. Adm Policy Ment Health. (2024). doi: 10.1007/s10488-024-01382-2
45. Herrera PA, Campos-Romero S, Szabo W, Martínez P, Guajardo V, Rojas G. Understanding the relationship between depression and chronic diseases such as diabetes and hypertension: A grounded theory study. Int J Environ Res Public Health. (2021) 18:12130. doi: 10.3390/ijerph182212130
46. Ludman EJ, Peterson D, Katon WJ, Lin EH, Von Korff M, Ciechanowski P, et al. Improving confidence for self care in patients with depression and chronic illnesses. Behav Med. (2013) 39:1–6. doi: 10.1080/08964289.2012.708682
47. Bernstein MT, Walker JR, Sexton KA, Katz A, Beatie BE. Gathering opinions on depression information needs and preferences: samples and opinions in clinic versus web-based surveys. JMIR Ment Health. (2017) 4:e13. doi: 10.2196/mental.7231
48. Fossey E, Harvey C, Mokhtari MR, Meadows GN. Self-rated assessment of needs for mental health care: a qualitative analysis. Community Ment Health J. (2012) 48:407–19. doi: 10.1007/s10597-011-9433-6
49. Bowskill R, Clatworthy J, Parham R, Rank T, Horne R. Patients’ perceptions of information received about medication prescribed for bipolar disorder: implications for informed choice. J Affect Disord. (2007) 100:253–7. doi: 10.1016/j.jad.2006.10.018
Keywords: psychometric, validity, reliability, depression, translation
Citation: Jafari A, Naddafi F, Nejatian M, Charoghchian Khorasani E and Tehrani H (2024) Validity and reliability of the Depression Information Needs Scale among the Iranian general population. Front. Psychiatry 15:1388447. doi: 10.3389/fpsyt.2024.1388447
Received: 19 February 2024; Accepted: 05 August 2024;
Published: 03 September 2024.
Edited by:
Nicholas Pang, Universiti Malaysia Sabah, MalaysiaReviewed by:
Mohd Amiruddin Mohd Kassim, University of Malaysia Sabah, MalaysiaMohammadreza Shalbafan, Iran University of Medical Sciences, Iran
Copyright © 2024 Jafari, Naddafi, Nejatian, Charoghchian Khorasani and Tehrani. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Hadi Tehrani, dGVocmFuaWhAbXVtcy5hYy5pcg==
†These authors have contributed equally to this work and share first authorship