
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Psychiatry , 22 July 2024
Sec. Public Mental Health
Volume 15 - 2024 | https://doi.org/10.3389/fpsyt.2024.1373083
 Mohammedamin Hajure1*†
Mohammedamin Hajure1*† Solomon Seyife Alemu2
Solomon Seyife Alemu2 Zakir Abdu3
Zakir Abdu3 Gebremeskel Mulatu Tesfaye4
Gebremeskel Mulatu Tesfaye4 Yadeta Alemayehu Workneh3
Yadeta Alemayehu Workneh3 Aman Dule3
Aman Dule3 Mustefa Adem Hussen5
Mustefa Adem Hussen5 Lema Fikadu Wedajo6
Lema Fikadu Wedajo6 Wubishet Gezimu4†
Wubishet Gezimu4†Objective: This review aimed to assess the current evidence on the relationship between resilience and mental health employed in response to the impacts of mental health.
Method: This review was conducted in accordance with the Preferred Reporting Items for Systematic Review and Meta-analysis (PRISMA). The protocol of this review was registered on the International Prospective Register of Systematic Reviews (PROSPERO: CRD42023470966). Three authors searched peer-reviewed articles using several electronic databases, including Scopus, PubMed/MEDLINE, Psych Info, EMBASE, and Web of Science, from September to October 2023 and included all the studies from any time until November 1, 2023. The review included all eligible quantitative observational and qualitative studies, irrespective of geographical boundaries.
Result: Depression, anxiety, and post-traumatic stress disorders were found to be the most common, but not the only, mental health disorders during the perinatal period, and higher maternal resilience during perinatal periods was found to reduce mental health disorders. It was also found that pregnant women were more resilient to mental health disorders than postpartum women. Tolerance of uncertainty and a positive cognitive appraisal, women’s self-behavior and family functioning, and protective psychosocial resources such as dispositional optimism, parental sense of mastery, self-esteem, gratitude, and forgiveness were found to be the most common mechanisms of resilience among perinatal women. Older age, having an adolescent partner, family income, and distress were found to affect resilience.
Conclusion: Noting that women’s resilience is an important tool to prevent perinatal mental health disorders, maternal healthcare providers need to counsel perinatal women on resilience-boosting mechanisms, such as applying self-behavior and having social support or close family relationships. It is recommended to counsel or provide psychosocial interventions for the woman’s companion or partner to give strong support for the woman in each of the perinatal periods.
Systematic review registration: https://www.crd.york.ac.uk/prospero/display_record.php?RecordID=470966, identifier CRD42023470966.
Mental health is the backbone of other health, defined as a state of mental well-being that permits individuals to cope with stress conditions, realize their abilities, and be productive in their communities. It’s a fundamental human right of an individual and a milestone in personal, community, and socioeconomic development (1).
Resilience is the ability to bounce back from struggling or challenging life experiences with a successful outcome, mainly through mental, psychological, and behavioral flexibility and adjustment to external and internal demands (2). Every person will experience difficulties or challenges in their life. However, the main concern is the ability to respond to these difficulties without serious harm because it allows them to overcome negative experiences and helps them to learn from them (2, 3).
Nowadays, mental health disorders (MHDs) are a worldwide burden of diseases. As described from the updated data in the 2019 global burden of diseases reports, mental disorders account for more than 14% of years lost due to disability for about 30 years (4). Furthermore, globally, more than 300 million and 280 million individuals suffer from anxiety and depression, respectively (4, 5).
Perinatal mental disorders (PMDs) are mental and behavioral disorders that occur during pregnancy and postpartum period. It affects more than 20% of perinatal women (6). Depression and anxiety are among the common mental disorders that occur during the perinatal period, followed by posttraumatic stress disorder and postpartum psychosis (7). Those mental disorders during the perinatal period may occur as a result of experiences associated with childbirth, neonatal loss, malformation birth, intimate partner violence, previous history of abuse, unwanted pregnancy, complications in labor, and higher perceived stress (8–10).
Mental disorders during the perinatal period result in many devastating impacts on both mothers and their newborns unless they are detected early and managed accordingly (11). The negative consequences of mental disorders include maternal morbidity and mortality associated with increased risk of maternal suicide and impaired motherhood capability that extremely affect the physical, emotional, social, and cognitive development of their newborns (12, 13). Furthermore, perinatal mental disorders have a huge economic burden; for instance, in the United Kingdom (UK), an estimated £75,728 and £34,840 expenditure per woman for perinatal depression and anxiety, respectively, with an aggregate cost of £6.6 billion (14).
Despite the perinatal period being the most challenging time with a lot of psychological, physical, and social changes for women, most women adapt to the situation and care for their family members by accepting the change as exciting and joyous (15). Besides this, several women experience a wide range of negative emotions, which can result in biopsychosocial distress (15, 16). Thus, perinatal resilience is crucial for the woman’s well-being, family balance, adaptation, or acceptance when faced with stressors, challenges, or adversity during the perinatal period (17).
Some of the studies show the impact of resilience in overcoming mental disorders like depression, anxiety, and post-traumatic stress disorders (15, 18–20). As identified in different literature, mechanisms of resilience that help to recover from perianal mental disorders are mastery, optimism, spirituality, social support, adequate financial resources, and a healthy perinatal environment (20–22). In addition to this, cognitive behavioral therapy and mindfulness interventions are also identified as mechanisms for coping with mental disorders during the perinatal period (23). In other ways, various studies assessed resilience specifically for anxiety, depression, and posttraumatic stress disorders in different perinatal periods. Thus, there is no consistent finding on the mechanism of resilience to the perinatal period of mental disorders. Therefore, this review aimed to assess the current evidence on the relationship between resilience and mental health employed in response to the impacts of mental health.
The protocol of this review was registered on the International Prospective Register of Systematic Reviews (PROSPERO) with the accession number (CRD42023470966). This review was conducted in accordance with the Preferred Reporting Items for Systematic Review and Meta-analysis (PRISMA).
Three authors searched peer-reviewed articles using several electronic databases including Scopus, PubMed/MEDLINE, Psych Info, EMBASE, and Web of Science, from September to October 2023, and included all the studies from any time until November 1, 2023. In addition, they searched for different relevant gray literature using Google Scholar. Boolean operators ‘OR’ and ‘AND’ were used in between the articles’ keywords and the medical subject heading terms (MeSH). The keywords used were ‘resilience’ OR ‘coping’ AND ‘antenatal’ OR ‘prenatal’ OR ‘during pregnancy’ OR ‘pregnant women’ OR ‘intrapartum’ OR ‘during birth’ OR ‘during labor’ OR ‘during childbirth’ OR ‘postpartum’ OR ‘postnatal’ OR ‘after birth’ AND ‘depression’ OR ‘anxiety’ OR ‘suicide’ OR ‘substance’ OR ‘post-traumatic stress disorder (PTSD)’ OR ‘general psychological distress’.
Since there is no agreed-upon definition of resilience, authors have instead defined it as it is also described as a circular process towards a greater wellbeing in the form of personal growth, family balance, adaptation or acceptance when faced with stressors, challenges, or adversity during the perinatal period (15).
refers to the period between pregnancy and the first 12 months following delivery (24).
All full-length articles published in English, irrespective of time and geographical boundary, were selected according to Mattos TC. et al.’s PICO/PECO format (Patient/Problem/Population; Intervention/Exposure; Comparison and Outcomes) ideal questions intended to solve a clinical problem (25). Accordingly, this review included all original studies conducted among perinatal (prenatal, intranatal, and postnatal) women (P). The resilience of perinatal women was the exposure (E) status of the review. The outcome (O) interests of this review were the mental health outcomes, including depression, anxiety, suicide, substance use, post-traumatic stress disorder, and general psychological distress. Even if the current review primarily targeted the above-stated mental health conditions, it was not restricted to this but rather included mental health conditions affecting women in the perinatal period, such as sleep disorders, child psychiatric disorders, and lifetime trauma.
In addition, in this review, all published and unpublished studies in the English language that have a clear outcome of interest and are available in full text were included, including all published and unpublished randomized controlled trials (RCTs), observational studies, and qualitative studies. The review included all eligible quantitative observational and qualitative studies, irrespective of geographical boundaries. For the inclusion of qualitative studies, a discussion guide with queries related to mental health should be available. However, it excluded editorials, corrigendum, case studies, reviews, commentaries, conference abstracts, reports, and any articles published in languages other than English that were not published in full-length and utilized designs other than RCT, observational, and qualitative studies.
Two authors (MAH and WG) conducted the data extraction and article section from October 13 to 16, 2023. The third author (SS) was enlisted to settle disagreements among authors about whether to include or exclude manuscripts from the review process. The full texts of every study that was included were compared again to the specifications, and any discrepancies were resolved by the authors. The data were extracted based on the article’s author name, year of publication, study setting and period, study design, sample size, perinatal period, data collection methods, population demography, magnitude of mental health conditions, mechanism of resilience employed, association of resilience with mental health, and risk impacts or determinants of resilience/future implications. The extracted articles were transferred to Endnote version X9 to manage references and duplications. Then the extracted articles were independently screened by the three authors.
Two independent reviewers (SS, YA) evaluated the quality of the included studies using the Joanna Briggs Institute (JBI) and the Mixed-Methods Appraisal Tool (MMAT). The reviewers discussed any discrepancies in the evaluation until they could come to a consensus and when a disagreement arose, the third reviewer (ZA) took the study into consideration and mediated a settlement.
The methodological qualities of the quantitative observational studies were appraised using the JBI Systematic Reviews Checklist for Systematic Reviews and Research Syntheses. The modified JBI checklist has nine (9) items to which a response of “yes” or “no” is possible. For this review, the checklist was converted to a scale. A total quality score, ranging from 0 to 18, was obtained by adding the scores of each item, which were assigned a value of 2 (excellent), 1 (good), or 0 (not available, unclear, or poor) (26). In other ways, the Mixed Approaches Appraisal Instrument (27), a critical appraisal instrument, was employed to assess the quality of the mixed studies included because papers using a variety of approaches were included in this study, and they have been validated and demonstrated to have good reliability (28). The MMAT has five quality criteria and wasutilized to evaluate the possibility of bias in the results and to give an insightful description of overall quality. Quality assessment of mixed-methods research was conducted both in the contexts in which the quantitative and qualitative components were employed, and in their own context (29).
In order to find pertinent literature for our review, we employed a variety of databases as search engines, including PubMed/MEDLINE, Scopus, Embase, PsychInfo, and the Web of Science database. Gray literature has also been checked for in other places, such as Google Scholar. As a consequence, 2,840 articles were initially sourced from various sources, including five databases. 1,770 studies were still available for further review after being screened for duplicates and irrelevant themes. Then, 1,714 studies were discarded after title and abstract verification. Afterward, 56 studies had become candidates for full-text review. The authors finally included 28 papers that fulfill the methodological or eligibility requirements to conduct systematic review (Figure 1).
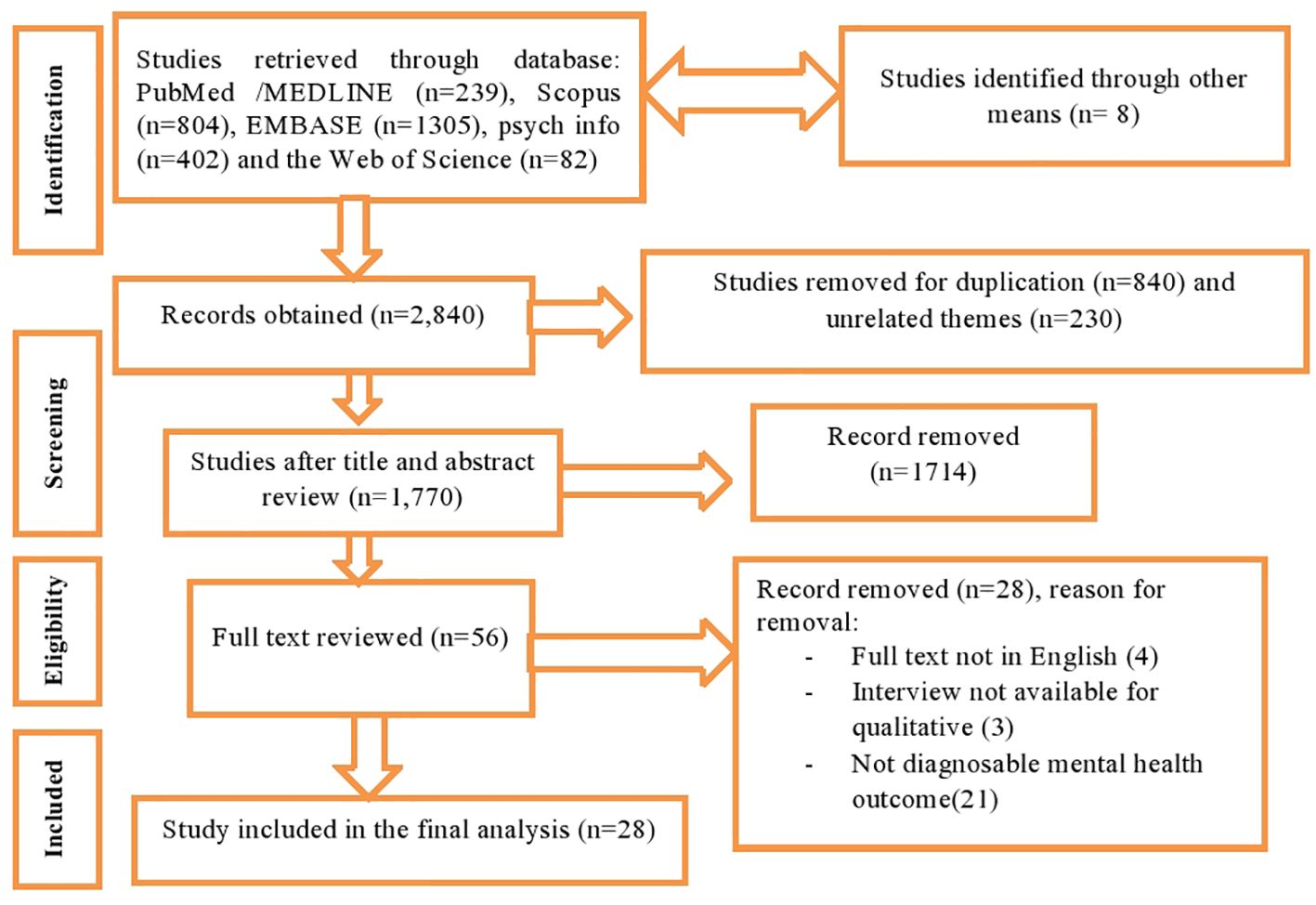
Figure 1 PRISMA flow chart displaying the selection process of identified studies.
Regarding the study settings, the majority of the included studies were conducted in developed nations, with Asia following in second. Accordingly, the USA reported nine of the studies, followed by China with seven studies. Additionally, three and two studies came from Australia and India, respectively. For this review, single studies were donated from a variety of other nations, including Spain, Poland, Brazil, Ecuador, Saudi Arabia, Nigeria, and Ethiopia Table 1.
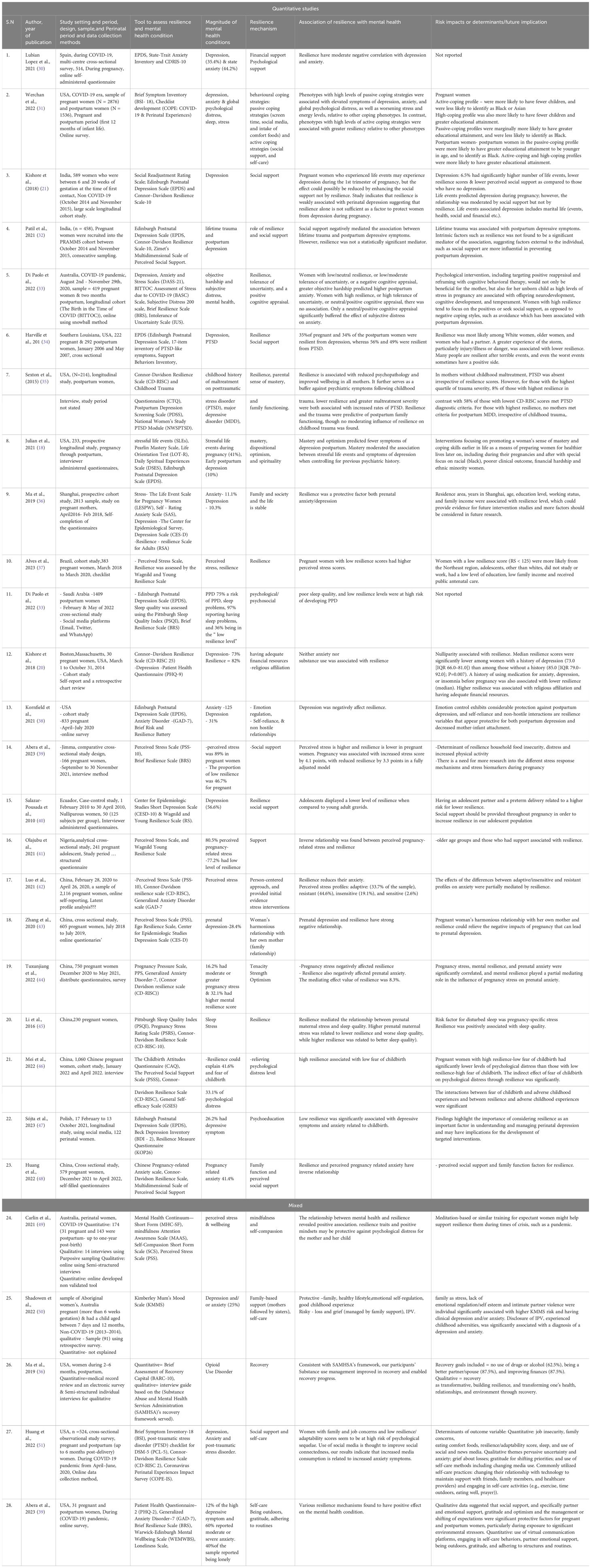
Table 1 Characteristics of included studies, 2024.
Twenty-three of the studies were quantitative observational, and five were mixed-methods research. Nine of the observational quantitative studies were carried out during the COVID-19 era, and twenty-two studies equally shared eleven cross-sectional and longitudinal cohorts amongst them. A total of 17,453 sample sizes were included, with the minimum and maximum sample sizes in the current review evidenced in the USA ranging from 30 to 4412 (31, 52).
Almost all the studies included in the current review used standard and cross-culturally validated instruments to assess mental health outcomes. Accordingly, the Connor-Davidson Resilience Scale-10 and 25 items (CD-RISC) were the most commonly used instruments in more than 45% of the retrieved reviews (13 out of 28 studies) (21, 30, 32, 35, 40, 42, 43, 51–56) for measuring resilience, followed by the Brief Resilience Scale (BRS) (33, 39, 57, 58) and the Wagnild Young Resilience Scale (37, 40, 41). The other instruments used for the assessment of resilience include the Resilience Measure Questionnaire (KOP26), the Ego Resilience Scale, the Brief Risk and Resilience Battery, and the Resilience Scale for Adults (RSA). Even if the study period was undertaken during the perinatal period from conception to the postnatal period, eleven studies were exclusively undertaken during pregnancy, while the rest of the studies were done during both the pregnancy and postpartum periods. Considering the mental health conditions examined for their association with resilience, depression, and anxiety take a leading role in most of the studies, followed by perceived stress.
The Edinburgh Postnatal Depression Scale (EPDS) was commonly used for assessing postpartum depression in the current review (8 of the 28 studies) (18, 21, 30, 32, 34, 38, 57, 59), followed by the Epidemiologic Studies Depression Scale (CES-D) in about four studies (3/28) (36, 40, 43), and Patient Health Questionnaire-2 (PHQ-9)(2/28) (52, 58) Moreover, the Beck Depression Inventory (BDI-2) (59) and the Depression, Anxiety, and Stress Scales (DASS-21) (33) were also employed to measure depression in the retrieved reviews. Of the 28 studies, eight were completed between 2009 and 2019 (21, 34–36, 38, 40, 52, 54), and twenty were undertaken between 2021 and 2023 (18, 30, 31, 33, 37, 39, 41–43, 49–51, 53–60) Table 1.
Regarding risk of bias, we utilized the Joanna Briggs Institute (JBI) criteria to assess the quality of the quantitative research, and we discovered that twenty one of the studies had low risk bias (18, 21, 30–37, 39–43, 51–54, 57, 59), two had medium risk (38, 57), and no study reported had high risk. The MMAT was another method used to assess the quality of the mixed research. According to previously published systematic literature reviews as well as recommended practices for using the MMAT to communicate the quality of the study, overall quality rating scores have been given. Accordingly, four studies, each two of them scored 60% and 80%, respectively, and one study scored 100% Supplementary File 1.
According to the studies reviewed in this review, there are differences in the types and degree to which different mental health problems are associated with resilience. This includes depression, which is the most commonly studied common mental health condition in more than 50% of the studies (16/28 studies) (18, 21, 30–32, 34–36, 38, 40, 43, 49, 50, 52, 56, 58, 59), followed by anxiety disorders (8/28 studies) (30, 31, 36, 38, 49, 51, 56, 58). The third commonly investigated mental health condition is perceived pregnancy stress (7/28 studies) (18, 37, 39, 41, 42, 53, 60). Post-traumatic stress disorder was another condition commonly reported (3/28) (34, 35, 56), followed by psychological distress (31, 54) and sleep disorders (31, 55, 57). Besides, opioid use disorders, lifetime trauma, childhood maltreatment and fear of childbirth were the least reported in the current review (32, 35, 50, 55). The magnitude of depression has been reported in about 13 studies in various settings, ranging from 6.5% in India (21) to 75% in Saudi Arabia (57), both for antenatal and postnatal depression, and the report seems lower as to anxiety disorders comparatively (ranging from 11.1% to 60%). Additionally, more perceived pregnancy stress was reported than any other condition, ranging from 16.2% in China to 89% in Ethiopia.
Studies have shown that resilience can protect us from psychological disorders, and this could take different forms, such as directly reducing the impacts of the condition or offsetting determinants that increase the risk of mental health conditions. Particularly during the perianal period, numerous circumstances affect the resilience of individuals living with mental health conditions, which might vary depending on the perinatal period (pregnancy and postnatal), parity, individual capability, sociocultural, environmental, and other significant attributes.
Accordingly, the current review highlighted the highest resilience scores for pregnancy compared to the postpartum period, specific to psychological disorders such as depression and PTSD. Resilience was found to decrease 34% of depression and 49% of post-traumatic stress disorder in the postpartum period, whereas 35% of depression and 56% of post-traumatic stress disorder occurred during pregnancy (33). In line with the current findings, a lower score of resilience was found to have an association with the highest score of depression and PTSD in the presence of a maternal history of childhood maltreatment (35). Psychological distress was the other mental health outcome and was 41.6% explained by resilience (55). In our review, the lowest score of resilience among pregnant women ranges from 36% in Saudi Arabia (57) to 77.2% in Nigeria (40), with the highest score evidenced among nulliparous women compared to those in the pregnant and postnatal periods (52). In sum, studies in the current review reported a higher resilience score with reduced mental health outcomes, including depression and anxiety (18, 21, 30, 31, 33, 34, 36, 38, 43, 51, 56, 58, 59), PTSD (34, 35, 56), stress (18, 37, 39, 42, 53), psychological distress (31), and sleep disturbance (54, 57). In contrast to this, study from Massachusetts, USA, among pregnant women show neither anxiety nor substance use was associated with resilience (52), and similarly, resilience did not significantly mediate the association of lifetime trauma and postpartum depression (32). This might be explained from dose response relationship in which low exposure to adversity help them to learn on how to cope with or become resilient to negative experiences and thereby improve their mental health. Conversely, individuals who face hardships on a regular basis could give up on hope for better results, while those who never face difficulties are unable to acquire coping mechanisms, increasing their chance of developing mental health conditions. Moreover, a study found that the absence of a relationship between anxiety and resilience might be related to the study’s use of self-reported anxiety (20) rather than a validated measure (61).
Physiological, neurobehavioral, and psychological factors are highlighted in models of psychological resilience as important contributors to safeguarding resilience. Psychological factors, including optimism, self-efficacy, high IQ, and the application of responsive emotional regulation techniques, have all been demonstrated in the earlier report to make a positive contribution to resilience (62–65). Resilience is a risk factor for some clinical diseases, such as suicide, as well as a protective factor against the onset of mental disorders. The available data from research studies indicates that resilience is a controllable factor, which creates opportunities for several novel psychosocial and biological therapies.Likewise, numerous mechanisms or techniques of resilience from perinatal mental health outcomes have been identified in the current review, including financial or psychological support (30, 52, 55, 57), behavioral coping strategies (passive coping strategies (screen time, social media, and intake of comfort foods), and active coping strategies (social support) (21, 31, 32, 34, 36, 39–41, 51, 56, 57) and self-care). A study revealed women with active coping skills and high coping profiles were more likely to have greater educational attainment compared to those with passive coping (31). According to a study, women who practice active coping strategies, including situational adjustment, accommodation, and symptom reduction, are more likely to maintain their social networks, take care of themselves, stay away from harmful material that could affect their health, and spend less time vegging out. Passive coping pregnant women avoided social interaction, concealed their feelings from others, and seldom employed self-stimulation or diversion during stressful situations such as COVID-19. Moreover, avoidance was the least common prenatal coping strategy, while prayer was the most commonly used, and higher levels of uncertainty were associated with lower emotional well-being, less positive interpretation, less social support, and greater avoidance during pregnancy (31, 66). A study revealed that pregnant women benefit intellectually and emotionally from psychological support, which also eases their transition to parenting and they may feel more stress and worry related to childbirth if they don’t have psychological support (67).
In the context of a secure existence with family or society, low resilience was substantially linked with reduced depressive symptoms and anxiety connected to childbirth. Also, the provision of psycho-education strengthens the negative impact of resilience on mental health conditions among pregnant and postpartum women (36, 59). Depending on the social context in which it was placed, a particular stressor may intensify or lessen, and it may also be viewed as posing varying degrees of perceived stress or requiring varying levels of resilience. In addition, being able to tolerate uncertainty and having a positive cognitive appraisal (33) were also protective measures for explaining resilience during the perinatal period. Consequently, it was discovered that women with lower resilience, lower uncertainty tolerance, a negative cognitive evaluation, and greater objective suffering were more likely to have postpartum anxiety. Only a neutral or positive cognitive appraisal was able to considerably lessen the impact of subjective discomfort on anxiety. Women with high resilience are more likely to turn to positive reinforcement or seek out social support than to use negative coping methods linked to depression after childbirth. A neutral or positive cognitive appraisal significantly mitigated the influence of subjective distress on anxiety (33).
Implementation of person-centered strategies including mindfulness and self-compassion (60), regulating emotions (58), self-reliance and non-hostile interactions (38), tenacity and strength (53), and offering early evidence stress interventions (42), has been demonstrated to influence resilience in pregnant women. This supported the idea that resilience shows a robust link by playing a mediating role in the influence of pregnancy stress on prenatal anxiety. Positive attitudes and resilience attributes can safeguard both the mother and the child from psychological suffering (42, 53).
In the context of severe psychosocial stressors or crises such as the COVID-19 pandemic, women reported the use of online communication platforms, engaging in self-care behaviors (49, 56, 58)(e.g., adequate sleep, physical activity, and healthy eating), seeking partner emotional support, being outdoors, practicing gratitude, and adhering to structures and routines shown to enhance resilience. Furthermore, a study conducted in the USA examined the effectiveness of a recovery-oriented intervention among postpartum women with opioid use disorder utilizing the Substance Abuse and Mental Health Service Administration (SAMHSA) framework. It has been demonstrated to have a positive impact on resilience and facilitate recovery (50).
Numerous studies have provided explanations for coping strategies that lessen the adverse effects of mental health disorders on prenatal populations, one of which is social support.
Consequently, a study by Prabha S et al. found that social support, rather than resilience, mediated the link between life events and depression during the first trimester of pregnancy. This demonstrates that resilience alone cannot avoid depression (21). Likewise, the scenario also applies to the postpartum phase, where resilience was unable to statistically buffer the correlation between lifetime trauma and postpartum depressive symptoms, and social support negatively mediated the relationship. It is important to offer social support to expectant mothers in order to build resilience in our adolescent population (40, 41). Social support and resilience demonstrated an inverse association with anxiety (51) and will be improved by adjusting our relationship with technology, particularly during the COVID-19 pandemic (56).
Another resilience approach that affected the mental health outcomes of pregnant and postpartum women was practicing self-care behaviors, such as getting enough sleep, following routines, being grateful, exercising, eating healthily, spending time outside, and praying (49, 56, 58). Given this, women who struggle with family and work-related issues and who score poorly on resilience and adaptation appear to be more vulnerable to psychological disorders.
Additionally, social media use is expected to enhance social connectivity, which in turn increases anxiety symptoms. Family functioning is the extent to which a family functions as a unit to manage circumstances, events, outside stimuli, or activities that produce stress. In the current review, family functioning (35, 51), specifically a woman’s positive relationship with her own mother (43), followed by a sister (49) was shown to inversely affect anxiety and depression and promote well-being among pregnant women. Resilience in mothers is linked to a decrease in psychopathology and an increase in general well-being. While there was no evidence of resilience having a moderating effect on childhood trauma, resilience and trauma were predictive of postpartum family functioning. It also acts as a protective barrier against mental health conditions that arise from childhood trauma (35).
It has been shown that spirituality and a variety of psychosocial resources, such as dispositional optimism, parental sense of mastery, self-esteem, gratitude, and forgiveness, positively correlate with resilience and affect the mental health outcomes of perinatal women. According to a study, among postpartum women, depression was predicted by optimism and mastery but not by spirituality. The only resilience resource that can moderate the association between the number of stressful life experiences and postpartum depression symptoms with a small effect size is mastery (18, 52, 53).
Various factors influence perinatal women’s resilience in terms of mental health outcomes. Even the worst situations can occasionally have a silver lining, and many people bounce back from traumatic experiences with resilience. In the current review, resilience was associated with among older (34, 36, 37, 41), white (34), residence area (34, 36), educational level (37), employment status (36, 37, 56), northeast region (37), having an adolescent partner (37, 40) family income (36, 37), and receiving public antenatal care (37), household food-security, distress, and increased physical activity (39), and women having a partner while experiencing higher extreme weather events (storms), especially one involving threat, sickness, or trauma, was linked to poorer resilience (34, 36).
Compared to women without a history of depression, women with a history of depression had considerably lower median resilience ratings. Lower resilience was also linked to a prior history of using medication for depression, anxiety, or sleeplessness before becoming pregnant (median). Belonging to religion and having sufficient finances were connected with higher resilience (38).
Moreover, preterm delivery (40) and poor sleep quality (53) were related to a higher risk of lower resilience. Psychological distress was much lower in pregnant women with strong resilience and low fear of childbirth than in those with poor resilience and high fear of childbirth. Significant relationships were found between the fear of childbirth and negative childhood experiences, as well as resilience and negative childhood experiences (55).
Five of the retrieved reviews used mixed methods, and the qualitative results from these contributed to clarifying and amplifying the quantitative conclusions. As a result, the results of qualitative data suggests that positive family relationships suggested are protective factors and have the tendency to reduce anxiety and depression among perinatal women (49). Furthermore, Jacqueline A. et al.’s study, 2021 (60), conducted during the COVID-19 pandemic, examined resilience in prenatal mothers into four main qualitative themes, which are as follows: The first theme clarified a rise in psychological distress (stress, anxiety, and/or depression), especially during the period of acute constraint and family absence. The absence of in-person services, uncertainty about where to get them, and lack of information about hospital admission restrictions fall under theme two. Separation from friends and family, a greater need for assistance and guidance, and favorable outcomes (such as time-bound and flexible work schedules) fall under theme number four. In sum, women stated that throughout this period of their lives, support from peers, family, and friends, getting adequate information (58), being thankful for changing priorities, and using self-care techniques (56), were found crucial in helping them become resilient in the face of stressors like COVID-19 (49), which also explains the role of recovery in building resilience among substance users (50).
Over the past few years, policymakers, medical professionals, and researchers have shown an increased interest in the concept of resilience. This interest stems primarily from the potential benefits of resilience for happiness, health, and quality of life (68). Earlier research (36, 68–71) focused on the rare trajectories of the presence of difficulties or trauma, such as intimate partner violence or adolescent pregnancy, for the investigation of resilience during the perinatal period.
Furthermore, previous reviews on perinatal resilience-focused primarily on explaining how women’s resilience has been conceived and defined in scientific studies (72), while the current review aims at the evidence that connects resilience to common mental health outcomes like depression, anxiety, suicide, stress, sleep quality, substance abuse, and PTSD.
Comprehending the risk and promoting features of resilience provides many stakeholders with an opportunity to guarantee the well-being of mothers and children. In addition, the review investigated the specific resilience mechanisms used to mitigate the effects of mental health and related variables.
The current review conceptualizes resilience integration for evaluating its impact on perinatal women’s mental health outcomes, and nearly all of the studies (26/28) consider resilience to have a negative impact on mental health conditions and to promote well-being, regardless of the degree of association. However, the studies from Massachusetts, the USA, and India, where anxiety, substance use, and lifetime trauma lack associations with resilience, did not support this finding (32, 41). In other ways, studies among abstinent individuals with substance use disorder show resilient people disclose more about themselves, easily recover (50), and are less likely to relapse into alcohol use (73, 74).
The associations between mood disorders, trauma-related disorders, and resilience have been investigated in our reviews. Subsequently, higher scores of depression were shown to have an association with lower resilience scores. Resilience was found to decrease depression and post-traumatic stress disorder during the postpartum and pregnancy periods by 34% and 49% and 35% and 56%, respectively (34).
Moreover, resilience explained psychological distress by about 41.6% (55) and negatively affected other mental health disorders, including stress, sleep, and PTSD. This could be because psychological resilience enables individuals to build strong coping mechanisms, seek assistance when necessary, and apply their abilities to overcome obstacles in their mental health conditions. Besides, as a protective characteristic, resilience has been demonstrated to substantially decrease the correlation between risky exposure in life and depression, thereby functioning as a safeguard against adverse consequences including anxiety, depression, and post-traumatic stress disorder (75).
Family functions and social support are several instances of resilience mechanisms or coping strategies that have been invoked to explain mental health among pregnant women. As a result, previous reports indicate that women with depression and anxiety during the perinatal period received poorer social support (76), despite the fact that most of the retrieved reviews tested the provision of this support to buffer perinatal maternal adaptation to mental health outcomes and improve well-being. In other ways, Sexton et al. (35) hypothesized that the key components of lowering psychological distress are that resilient people are more likely to have supportive peers and to share their opinions.
It has also been demonstrated that family functioning negatively affects depression and anxiety while enhancing pregnant women’s well-being. Previous literature supported these findings (77, 78). This may result from the beneficial influence of fathers on their offspring as well as the cortisol responsiveness of newborns after a stressful event, which is partly mediated by a lower risk of antenatal depression and more optimistic mother-infant interactions (79).
In the current review, mastery was one of the resilience resources that have been shown to be essential for controlling the association between the number of stressful life events and postpartum depression symptoms. Women who experience a high sense of mastery are less vulnerable to the psychological impacts of stress because they are more likely to believe they can manage or control life’s obstacles (80).
Several factors impact the resilience of women in the perinatal period. For instance, older age was positively associated with resilience. According to particular situations and contexts, adaptive behavior rather than necessarily a progressively continuous quality might explain resilient behavior among older adults (81, 82). Lower family income and unemployed status among perinatal women were less likely to become resilient in response to mental health suffering compared to their counterparts. Employment is one significant factor in fostering mental wellness. It has a significant role in determining identity and self-worth. It can offer chances for relationships as well as a sense of fulfillment, and in most cases, their primary source of income comes from their job (83, 84). Therefore, increasing standards for employment and enhancing working conditions may help to reduce health inequalities and enhance wellbeing.
This review included all articles regardless of time and geographical boundaries, addressing all quantitative and qualitative studies. Thus, it could be generalizable for the global population. However, the study excluded articles published in languages other than English, and data synthesis was not done, so the impact of heterogeneity, publication bias, and study variability were not assessed. Thus, this issue and some methodological issues, including study design shortcomings and sample size issues of the included studies, should be carefully considered while interpreting the findings.
According to this systematic review, depression, anxiety, and post-traumatic stress disorders were found to be the most common, but not the only, mental health disorders during the perinatal period. The review found that higher maternal resilience during perinatal periods reduces mental health disorders. It was also found that pregnant women were more resilient to mental health disorders than postpartum women. Regarding the mechanisms of resilience to mental health disorders during the perinatal period, tolerating uncertainty and a positive cognitive appraisal, women’s self-behaviour and family functioning, and protective psychosocial resources such as dispositional optimism, parental sense of mastery, self-esteem, gratitude, and forgiveness were found to be the most common mechanisms of resilience. Older age, residence area, educational level, employment status, having an adolescent partner, family income, distress, and increased physical activity were found to be detrimental factors of resilience.
Noting that women’s resilience is an important tool to prevent perinatal mental health disorders, maternal healthcare providers need to counsel perinatal women on resilience-boosting mechanisms, such as applying self-behaviour and having social support or close family relationships. The current review took into consideration the need for healthcare providers to implement perinatal programs that aim to promote resilience by enhancing existing preventative measures and taking into account resilience mechanisms like active coping skills, self-care behaviors, social support, and cohesion. The integration of capacity building initiatives within current healthcare institutions could not only assist perinatal mothers, but also healthcare provider’s ability to provide quality services. Since high-level perinatal mental health conditions impair the biological and psychosocial development of the offspring, the mother and her unborn child would benefit more from positive reflection and protective psychosocial resources (85–89). We think it is also better to counsel the woman’s companion or partner to give strong support to the woman in each of the perinatal periods. Moreover, the concerned bodies need to incorporate counselling on resilience-boosting mechanisms into the antenatal and postpartum counselling packages.
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding authors.
MJ: Writing – original draft, Writing – review & editing. SA: Conceptualization, Data curation, Investigation, Methodology, Writing – review & editing. ZA: Conceptualization, Investigation, Methodology, Writing – original draft, Writing – review & editing. GT: Data curation, Investigation, Methodology, Supervision, Writing – review & editing. YW: Conceptualization, Data curation, Investigation, Project administration, Writing – review & editing. AD: Conceptualization, Data curation, Investigation, Software, Supervision, Writing – original draft. MH: Conceptualization, Investigation, Methodology, Project administration, Writing – review & editing. LW: Conceptualization, Investigation, Methodology, Writing – original draft. WG: Writing – original draft.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
We (the authors) acknowledge all the authors of the original articles used in this review.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2024.1373083/full#supplementary-material
1. WHO. Mental health (2022). Available online at: https://www.who.int/news-room/fact-sheets/detail/mental-health-strengthening-our-response/?gclid=CjwKCAjwyY6pBhA9EiwAMzmfwWXzTxod_Q83dQ8vbTN9CiWN9pgz6gHduQRb3p2PV10_9kqSqtBhKBoCz1MQAvD_BwE.
2. APA. Resilience (2022). Available online at: https://wwwapaorg/topics/resilience.
3. Cohn MA, Fredrickson BL, Brown SL, Mikels JA, Conway AM. Happiness unpacked: positive emotions increase life satisfaction by building resilience. Emotion (Washington DC). (2009) 9:361–8. doi: 10.1037/a0015952
4. Ferrari AJ, Santomauro DF, Herrera AMM, Shadid J, Ashbaugh C, Erskine HE, et al. Global, regional, and national burden of 12 mental disorders in 204 countries and territories 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet Psychiatry. (2022) 9:137–50. doi: 10.1016/S2215-0366(21)00395-3
5. Abraham A, Chaabna K, Doraiswamy S, Bhagat S, Sheikh J, Mamtani R, et al. Depression among healthcare workers in the Eastern Mediterranean Region: a systematic review and meta-analysis. Hum Resour Health. (2021) 19:1–18. doi: 10.1186/s12960-021-00628-6
6. Howard LM, Molyneaux E, Dennis C-L, Rochat T, Stein A, Milgrom J. Non-psychotic mental disorders in the perinatal period. Lancet. (2014) 384:1775–88. doi: 10.1016/S0140-6736(14)61276-9
7. Awini E, Agyepong IA, Owiredu D, Gyimah L, Ashinyo ME, Yevoo LL, et al. Burden of mental health problems among pregnant and postpartum women in sub-Saharan Africa: systematic review and meta-analysis protocol. BMJ Open. (2023) 13:e069545. doi: 10.1136/bmjopen-2022-069545
8. Milgrom J, Hirshler Y, Reece J, Holt C, Gemmill AW. Social support—a protective factor for depressed perinatal women? Int J Environ Res Public Health. (2019) 16:1426. doi: 10.3390/ijerph16081426
9. Ogbo FA, Eastwood J, Hendry A, Jalaludin B, Agho KE, Barnett B, et al. Determinants of antenatal depression and postnatal depression in Australia. BMC Psychiatry. (2018) 18:1–11. doi: 10.1186/s12888-018-1598-x
10. Biaggi A, Conroy S, Pawlby S, Pariante CM. Identifying the women at risk of antenatal anxiety and depression: a systematic review. J Affect Disord. (2016) 191:62–77. doi: 10.1016/j.jad.2015.11.014
11. Patabendige M, Athulathmudali SR, Chandrasinghe SK. Mental Health Problems during Pregnancy and the Postpartum Period: A Multicenter Knowledge Assessment Survey among Healthcare Providers. J Pregnancy. (2020) 2020:4926702. doi: 10.1155/2020/4926702
12. Leddy M, Haaga D, Gray J, Schulkin J. Postpartum mental health screening and diagnosis by obstetrician–gynecologists. J Psychosomatic Obstetrics Gynecology. (2011) 32:27–34. doi: 10.3109/0167482X.2010.547639
13. Stewart DE, Robertson E, Dennis C-L, Grace SL, Wallington T. Postpartum depression: Literature review of risk factors and interventions. Toronto: University Health Network Women’s Health Program for Toronto Public Health (2003) p. 1–289.
14. Bauer A, Knapp M, Parsonage M. Lifetime costs of perinatal anxiety and depression. J Affect Disord. (2016) 192:83–90. doi: 10.1016/j.jad.2015.12.005
15. Van Haeken S, Braeken M, Nuyts T, Franck E, Timmermans O, Bogaerts A. Perinatal resilience for the first 1,000 days of life. Concept analysis and delphi survey. Front Psychol. (2020) 11:563432. doi: 10.3389/fpsyg.2020.563432
16. Dekel S, Stuebe C, Dishy G. Childbirth induced posttraumatic stress syndrome: a systematic review of prevalence and risk factors. Front Psychol. (2017) 8:560. doi: 10.3389/fpsyg.2017.00560
17. Van Haeken S, Braeken MAKA, Horsch A, Oosterman M, Bogaerts A. Development of a resilience-enhancing intervention during and after pregnancy: a systematic process informed by the behaviour change wheel framework. BMC Psychol. (2023) 11:267. doi: 10.1186/s40359-023-01301-4
18. Julian M, Le HN, Coussons-Read M, Hobel CJ, Dunkel Schetter C. The moderating role of resilience resources in the association between stressful life events and symptoms of postpartum depression. J Affect Disord. (2021) 293:261–7. doi: 10.1016/j.jad.2021.05.082
19. Yamamoto T, Nishinaka H, Matsumoto Y. Relationship between resilience, anxiety, and social support resources among Japanese elementary school students. Soc Sci Humanities Open. (2023) 7:100458. doi: 10.1016/j.ssaho.2023.100458
20. Johnson KM, Paley FM, Modest AM, Hacker MR, Shaughnessy S, Ricciotti HA, et al. An assessment of depression, psychosocial factors, and resilience among women seeking prenatal care at an urban community health center. Int J Gynaecol Obstet. (2018) 140:153–8. doi: 10.1002/ijgo.12358
21. Kishore MT, Satyanarayana V, Ananthanpillai ST, Desai G, Bhaskarapillai B, Thippeswamy H, et al. Life events and depressive symptoms among pregnant women in India: Moderating role of resilience and social support. Int J Soc Psychiatry. (2018) 64:570–7. doi: 10.1177/0020764018789193
22. Gagnon AJ, Stewart DE. Resilience in international migrant women following violence associated with pregnancy. Arch women's Ment Health. (2014) 17:303–10. doi: 10.1007/s00737-013-0392-5
23. Walker AL, Witteveen AB, Otten RHJ, Verhoeven CJ, Henrichs J, de Jonge A. Resilience-enhancing interventions for antepartum depressive symptoms: systematic review. BJPsych Open. (2022) 8:e89. doi: 10.1192/bjo.2022.60
24. Helfer RE. The perinatal period, a window of opportunity for enhancing parent-infant communication: an approach to prevention. Child Abuse Negl. (1987) 11:565–79. doi: 10.1016/0145-2134(87)90082-2
25. Mattos CT, Ruellas AC. Systematic review and meta-analysis: what are the implications in the clinical practice? Dental Press J Orthod. (2015) 20:17–9. doi: 10.1590/2176-9451.20.1.017-019.ebo
26. Aromataris E, Fernandez R, Godfrey C, Holly C, Kahlil H, Tungpunkom P. Summarizing systematic reviews: methodological development, conduct and reporting of an Umbrella review approach. Int J Evid Based Healthc. (2015) 13:132–40. doi: 10.1097/XEB.0000000000000055
27. Hong QN, Gonzalez-Reyes A, Pluye P. Improving the usefulness of a tool for appraising the quality of qualitative, quantitative and mixed methods studies, the Mixed Methods Appraisal Tool (MMAT). J Eval Clin Pract. (2018) 24:459–67. doi: 10.1111/jep.12884
28. Crowe M, Sheppard L. A review of critical appraisal tools show they lack rigor: Alternative tool structure is proposed. J Clin Epidemiol. (2011) 64:79–89. doi: 10.1016/j.jclinepi.2010.02.008
29. Pluye P, Hong QN. Combining the power of stories and the power of numbers: mixed methods research and mixed studies reviews. Annu Rev Public Health. (2014) 35:29–45. doi: 10.1146/annurev-publhealth-032013-182440
30. Lubian Lopez DM, Butron Hinojo CA, Arjona Bernal JE, Fasero Laiz M, Alcolea Santiago J, Guerra Vilches V, et al. Resilience and psychological distress in pregnant women during quarantine due to the COVID-19 outbreak in Spain: a multicentre cross-sectional online survey. J Psychosom Obstet Gynaecol. (2021) 42:115–22. doi: 10.1080/0167482X.2021.1896491
31. Werchan DM, Hendrix CL, Ablow JC, Amstadter AB, Austin AC, Babineau V, et al. Behavioral coping phenotypes and associated psychosocial outcomes of pregnant and postpartum women during the COVID-19 pandemic. Sci Rep. (2022) 12:1209. doi: 10.1038/s41598-022-05299-4
32. Patil DM, Bajaj A, Supraja TA, Chandra P, Satyanarayana VA. Lifetime traumatic experiences and postpartum depressive symptoms in a cohort of women in South India. Arch Womens Ment Health. (2021) 24:687–92. doi: 10.1007/s00737-021-01111-w
33. Di Paolo AL, King S, McLean MA, Lequertier B, Elgbeili G, Kildea S, et al. Prenatal stress from the COVID-19 pandemic predicts maternal postpartum anxiety as moderated by psychological factors: The Australian BITTOC Study. J Affect Disord. (2022) 314:68–77. doi: 10.1016/j.jad.2022.06.055
34. Harville EW, Xiong X, Buekens P, Pridjian G, Elkind-Hirsch K. Resilience after hurricane Katrina among pregnant and postpartum women. Womens Health Issues. (2010) 20:20–7. doi: 10.1016/j.whi.2009.10.002
35. Sexton MB, Hamilton L, McGinnis EW, Rosenblum KL, Muzik M. The roles of resilience and childhood trauma history: main and moderating effects on postpartum maternal mental health and functioning. J Affect Disord. (2015) 174:562–8. doi: 10.1016/j.jad.2014.12.036
36. Ma X, Wang Y, Hu H, Tao XG, Zhang Y, Shi H. The impact of resilience on prenatal anxiety and depression among pregnant women in Shanghai. J Affect Disord. (2019) 250:57–64. doi: 10.1016/j.jad.2019.02.058
37. Alves AC, Souza RT, Mayrink J, Galvao RB, Costa ML, Feitosa FE, et al. Measuring resilience and stress during pregnancy and its relation to vulnerability and pregnancy outcomes in a nulliparous cohort study. BMC Pregnancy Childbirth. (2023) 23:1–15. doi: 10.1186/s12884-023-05692-5
38. Kornfield SL, White LK, Waller R, Njoroge W, Barzilay R, Chaiyachati BH, et al. Risk and resilience factors influencing postpartum depression and mother-infant bonding during COVID-19. Maternal Health. (2021) 40:1566–74. doi: 10.1377/hlthaff.2021.00803
39. Abera M, Hanlon C, Fedlu H, Fewtrell M, Tesfaye M, Wells JCK. Stress and resilience during pregnancy: A comparative study between pregnant and non-pregnant women in Ethiopia. PloS Global Public Health. (2023) 3:1–5. doi: 10.1371/journal.pgph.0001416
40. Salazar-Pousada D, Arroyo D, Hidalgo L, Pérez-López FR, Chedraui P. Depressive symptoms and resilience among pregnant adolescents: A case-control study. Obstetrics Gynecology Int. (2010) 2010:1–7. doi: 10.1155/2010/952493
41. Olajubu AO, Omoloye GO, Olajubu TO, Olowokere AE. Stress and resilience among pregnant teenagers in Ile-Ife, Nigeria. Eur J Midwifery. (2021) 5:9. doi: 10.18332/ejm/134181
42. Luo Z, Shen Y, Yuan J, Zhao Y, Liu Z, Shangguan F. Perceived stress, resilience, and anxiety among pregnant Chinese women during the COVID-19 pandemic: latent profile analysis and mediation analysis. Front Psychol. (2021) 12:1–9. doi: 10.3389/fpsyg.2021.696132
43. Zhang L, Yang X, Zhao J, Zhang W, Cui C, Yang F, et al. Prevalence of prenatal depression among pregnant women and the importance of resilience: A multi- site questionnaire-based survey in Mainland China. Front Psychiatry. (2020) 11:374. doi: 10.3389/fpsyt.2020.00374
44. Tuxunjiang X, Li L, Wumaier G, Zhang W, Sailike B, Jiang T. The mediating effect of resilience on pregnancy stress and prenatal anxiety in pregnant women. Front Psychiatry. (2022) 13:961689. doi: 10.3389/fpsyt.2022.961689
45. Li G, Kong L, Zhou H, Kang X, Fang Y, Li P. Relationship between prenatal maternal stress and sleep quality in Chinese pregnant women: the mediation effect of resilience. Sleep Med. (2016) 25:8–12. doi: 10.1016/j.sleep.2016.02.015
46. Mei X, Mei R, Liu Y, Wang X, Chen Q, Lei Y, et al. Associations among fear of childbirth, resilience and psychological distress in pregnant women: A response surface analysis and moderated mediation model. Front Psychiatry. (2022) 13:1091042. doi: 10.3389/fpsyt.2022.1091042
47. Sójta K, Margulska A, Plewka M, Płeska K, Strzelecki D, Gawlik-Kotelnicka O. Resilience and psychological well-being of polish women in the perinatal period during the COVID-19 Pandemic. J Clin Med. (2023) 12:6279. doi: 10.3390/jcm12196279
48. Huang J, Xu L, Xu Z, Luo Y, Liao B, Li Y, et al. The relationship among pregnancy-related anxiety, perceived social support, family function and resilience in Chinese pregnant women: a structural equation modeling analysis. BMC Womens Health (2022) 22:546. doi: 10.1186/s12905-022-02145-7
49. Carlin E, Seear KH, Ferrari K, Spry E, Atkinson D, Marley JV. Risk and resilience: a mixed methods investigation of Aboriginal Australian women’s perinatal mental health screening assessments. Soc Psychiatry Psychiatr Epidemiol. (2021) 56:547–57. doi: 10.1007/s00127-020-01986-7
50. Shadowen C, Jallo N, Parlier-Ahmad AB, Brown L, Kinser P, Svikis D, et al. What recovery means to postpartum women in treatment for opioid use disorder. Women’s Health Rep. (2022) 3:93–103. doi: 10.1089/whr.2021.0064
51. Huang J, Xu L, Xu Z, Luo Y, Liao B, Li Y, et al. The relationship among pregnancy−related anxiety, perceived social support, family function and resilience in Chinese pregnant women: a structural equation modeling analysis. BMC Women’s Health. (2022) 22:546. doi: 10.1186/s12905-022-02145-7
52. Johnson KM, Paley FM, Modest AM, Hacker MR, Shaughnessy S, Ricciotti HA, et al. An assessment of depression, psychosocial factors, and resilience among women seeking prenatal care at an urban community health center. Int J Gynecol Obstet. (2017) 140:1–6. doi: 10.1002/ijgo.12358
53. Tuxunjiang X, Li L, Wumaier G, Zhang W, Sailike B, Jiang T. The mediating effect of resilience on pregnancy stress and prenatal anxiety in pregnant women. Front Psychiatry. (2020) 13:1–8. doi: 10.3389/fpsyt.2022.961689
54. Li G, Kong L, Zhou H, Kang X, Fang Y, Li P. Relationship between prenatal maternal stress and sleep quality in Chinese pregnant women: the mediation effect of resilience. Sleep Med (2016), 8–12. doi: 10.1016/j.sleep.2016.02.015
55. Mei X, Mei R, Liu Y, Wang X, Chen Q, Lei Y, et al. Associations among fear of childbirth, resilience and psychological distress in pregnant women: A response surface analysis and moderated mediation mode. Front Psychiatry. (2020) 13:1–12. doi: 10.3389/fpsyt.2022.1091042
56. Kinser PA, Jallo N, Amstadter AB, Thacker LR, Jones E, Moyer S, et al. Depression, anxiety, resilience, and coping: the experience of pregnant and new mothers during the first few months of the COVID-19 pandemic. J Women’s Health. (2021) 30:654–64. doi: 10.1089/jwh.2020.8866
57. Baattaiah BA, Alharbi MD, Babteen NM, Al−Maqbool HM, Babgi FA, Albatati AA. The relationship between fatigue, sleep quality, resilience, and the risk of postpartum depression: an emphasis on maternal mental health. BMC Psychol. (2023) 11:1–17. doi: 10.1186/s40359-023-01043-3
58. Farewell CV, Jewell J, Walls J, Leiferman JA. A mixed-methods pilot study of perinatal risk and resilience during COVID-19. J Primary Care Community Health. (2020) 11:1–8. doi: 10.1177/2150132720944074
59. Sójta K, Margulska A, Plewka M, Płeska K, Strzelecki D, Gawlik-Kotelnicka O. Resilience and psychologicalWell-being of polishWomen in the perinatal period during the COVID-19 pandemic. J Clin Med. (2023) 12:1–14. doi: 10.3390/jcm12196279
60. Davis JA, Gibson LY, Bear NL, Finlay-Jones AL, Ohan JL, Silva DT, et al. Can Positive Mindsets Be Protective against Stress and Isolation Experienced during the COVID-19 Pandemic? A Mixed Methods Approach to Understanding Emotional Health and Wellbeing Needs of PerinatalWomen. Int J Environ Res Public Health. (2021) 18:1–20. doi: 10.3390/ijerph18136958
61. Roos A, Lochner C, Vythilingum B, Stein DJ. Predictors of distress and anxiety during pregnancy. Afr J Psychiatry (Johannesbg). (2013) 16:118–22. doi: 10.4314/ajpsy.v16i2.15
62. Ong AD, Bergeman CS, Bisconti TL, Wallace KA. Psychological resilience, positive emotions, and successful adaptation to stress in later life. J Pers Soc Psychol. (2006) 91:730–49. doi: 10.1037/0022-3514.91.4.730
63. Cai WP, Pan Y, Zhang SM, Wei C, Dong W, Deng GH. Relationship between cognitive emotion regulation, social support, resilience and acute stress responses in Chinese soldiers: Exploring multiple mediation model. Psychiatry Res. (2017) 256:71–8. doi: 10.1016/j.psychres.2017.06.018
64. Afek A, Ben-Avraham R, Davidov A, Berezin Cohen N, Ben Yehuda A, Gilboa Y, et al. Psychological resilience, mental health, and inhibitory control among youth and young adults under stress. Front Psychiatry. (2020) 11:608588. doi: 10.3389/fpsyt.2020.608588
65. Mestre JM, Nunez-Lozano JM, Gomez-Molinero R, Zayas A, Guil R. Emotion regulation ability and resilience in a sample of adolescents from a suburban area. Front Psychol. (2017) 8:1980. doi: 10.3389/fpsyg.2017.01980
66. Giurgescu C, Penckofer S, Maurer MC, Bryant FB. Impact of uncertainty, social support, and prenatal coping on the psychological well-being of high-risk pregnant women. Nurs Res. (2006) 55:356–65. doi: 10.1097/00006199-200609000-00008
67. Xie RH, He G, Koszycki D, Walker M, Wen SW. Prenatal social support, postnatal social support, and postpartum depression. Ann Epidemiol. (2009) 19:637–43. doi: 10.1016/j.annepidem.2009.03.008
68. Powley EH. Reclaiming resilience and safety: Resilience activation in the critical period of crisis. Hum Relations. (2009) 62:1289–326. doi: 10.1177/0018726709334881
69. Barnett ML, Kia-Keating M, Ruth A, Garcia M. Promoting equity and resilience: wellness navigators' Role in addressing adverse childhood experiences. Clin Pract Pediatr Psychol. (2020) 8:176–88. doi: 10.1037/cpp0000320
70. Freed P, SmithBattle L. Teen mothers’ Mental health Vol. 41. Philadelphia, USA: Wolters Kluwer Health (2016) p. 32–6.
71. Wilson AL, McNaughton D, Meyer SB, Ward PR. Understanding the links between resilience and type-2 diabetes self-management: a qualitative study in South Australia. Arch Public Health. (2017) 75:56. doi: 10.1186/s13690-017-0222-8
72. Hannon SE, Daly D, Higgins A. Resilience in the perinatal period and early motherhood: A principle-based concept analysis. Int J Environ Res Public Health. (2022) 19:1–29. doi: 10.3390/ijerph19084754
73. Rathinam B, Ezhumalai S. Resilience among abstinent individuals with substance use disorder. Indian J Psychiatr Soc Work. (2021) 12:96–102. doi: 10.29120/ijpsw.2021.v12.i2.276
74. Ezhumalai S, Muralidhar D, Murthy P. Occupational factors associated with long-term abstinence among persons treated for alcohol dependence: A follow-up study. Indian J Occup Environ Med. (2022) 26:122–8. doi: 10.4103/ijoem.ijoem_37_22
75. Poole JC, Dobson KS, Pusch D. Childhood adversity and adult depression: The protective role of psychological resilience. Child Abuse Negl. (2017) 64:89–100. doi: 10.1016/j.chiabu.2016.12.012
76. Zheng B, Yu Y, Zhu X, Hu Z, Zhou W, Yin S, et al. Association between family functions and antenatal depression symptoms: a cross-sectional study among pregnant women in urban communities of Hengyang city, China. BMJ Open. (2020) 10:e036557. doi: 10.1136/bmjopen-2019-036557
77. Naja S, Al Kubaisi N, Singh R, Bougmiza I. Generalized and pregnancy-related anxiety prevalence and predictors among pregnant women attending primary health care in Qatar 2018-2019. Heliyon. (2020) 6:e05264. doi: 10.1016/j.heliyon.2020.e05264
78. Puertas-Gonzalez JA, Marino-Narvaez C, Romero-Gonzalez B, Vilar-Lopez R, Peralta-Ramirez MI. Resilience, stress and anxiety in pregnancy before and throughout the pandemic: a structural equation modelling approach. Curr Psychol. (2022) 12:1–11. doi: 10.1007/s12144-022-03305-6
79. Letourneau N, Leung B, Ntanda H, Dewey D, Deane AJ, Giesbrecht GF, et al. Maternal and paternal perinatal depressive symptoms associate with 2- and 3-year-old children's behaviour: findings from the APrON longitudinal study. BMC Pediatr. (2019) 19:435. doi: 10.1186/s12887-019-1775-1
80. Folkman S. Positive psychological states and coping with severe stress. Soc Sci Med. (1997) 45:1207–21. doi: 10.1016/S0277-9536(97)00040-3
81. Wagnild GM, Collins JA. Assessing resilience. J Psychosoc Nurs Ment Health Serv. (2009) 47:28–33. doi: 10.3928/02793695-20091103-01
82. Kocalevent RD, Zenger M, Heinen I, Dwinger S, Decker O, Brahler E. Resilience in the general population: standardization of the resilience scale (RS-11). PloS One. (2015) 10:e0140322. doi: 10.1371/journal.pone.0140322
83. Mollard E, Kupzyk K, Moore T. Postpartum stress and protective factors in women who gave birth in the United States during the COVID-19 pandemic. Womens Health (Lond). (2021) 17:17455065211042190. doi: 10.1177/17455065211042190
84. Excellence NIfHaC. Promoting mental wellbeing through productive and healthy working conditions: guidance for employers. London: NICE public health guidance (2009).
85. Aktar E, Qu J, Lawrence PJ, Tollenaar MS, Elzinga BM, Bogels SM. Fetal and infant outcomes in the offspring of parents with perinatal mental disorders: earliest influences. Front Psychiatry. (2019) 10:391. doi: 10.3389/fpsyt.2019.00391
86. Stein A, Pearson RM, Goodman SH, Rapa E, Rahman A, McCallum M, et al. Effects of perinatal mental disorders on the fetus and child. Lancet. (2014) 384:1800–19. doi: 10.1016/S0140-6736(14)61277-0
87. Edge D, Rogers A. Dealing with it: Black Caribbean women's response to adversity and psychological distress associated with pregnancy, childbirth, and early motherhood. Soc Sci Med. (2005) 61:15–25. doi: 10.1016/j.socscimed.2004.11.047
88. Shaikh A. Resilience in the face of postpartum depression: perspectives of women and their supporting others in Northern Ontario. Ottawa, Canada: Library and Archives Canada (2011).
89. Gewalt SC, Berger S, Ziegler S, Szecsenyi J, Bozorgmehr K. Psychosocial health of asylum seeking women living in state-provided accommodation in Germany during pregnancy and early motherhood: A case study exploring the role of social determinants of health. PloS One. (2018) 13:e0208007. doi: 10.1371/journal.pone.0208007
Keywords: mental health, associated factor, perinatal, women, resilience
Citation: Hajure M, Alemu SS, Abdu Z, Tesfaye GM, Workneh YA, Dule A, Adem Hussen M, Wedajo LF and Gezimu W (2024) Resilience and mental health among perinatal women: a systematic review. Front. Psychiatry 15:1373083. doi: 10.3389/fpsyt.2024.1373083
Received: 19 January 2024; Accepted: 28 June 2024;
Published: 22 July 2024.
Edited by:
Tadashi Takeshima, Kawasaki City Inclusive Rehabilitation Center, JapanReviewed by:
Natanael Karjanto, Sungkyunkwan University, Republic of KoreaCopyright © 2024 Hajure, Alemu, Abdu, Tesfaye, Workneh, Dule, Adem Hussen, Wedajo and Gezimu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Mohammedamin Hajure, c2lrb2FkbzM0MEBnbWFpbC5jb20=
†ORCID: Mohammedamin Hajure Jarso, orcid.org/0000-0002-4596-9611
Wubishet Gezimu, orcid.org/0000-0002-5503-1360
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.