 Alfredo Calcedo-Barba1,2*†
Alfredo Calcedo-Barba1,2*† Joaquín Antón Basanta3,4†
Joaquín Antón Basanta3,4† Silvia Paz Ruiz5Alvaro Muro Alvarez6Edorta Elizagárate Zabala7
Silvia Paz Ruiz5Alvaro Muro Alvarez6Edorta Elizagárate Zabala7 Verónica Estévez Closas5Angeles López López8Luis Fernando Barrios Flores8
Verónica Estévez Closas5Angeles López López8Luis Fernando Barrios Flores8- 1Institute of Psychiatry and Mental Health, Gregorio Marañón General University Hospital, Medical School, Complutense University of Madrid, Madrid, Spain
- 2Spanish Society of Legal Psychiatry, Madrid, Spain
- 3General Practice Penitentiary Health Care, Albolote Penitentiary Centre, Granada, Spain
- 4Spanish Society of Penitentiary Health, Barcelona, Spain
- 5SmartWorking4U, Valencia, Spain
- 6Penitentiary Psychiatry Services, Barcelona, Spain
- 7Psychiatry Service of the Mental Health Network of Araba, Mental Health Centre, Zaballa Penitentiary Center, Spanish Society of Clinical Psychiatry, Deusto University Medical School, Bilbao, Spain
- 8Retired, Alicante, Spain
Background: Spain healthcare system is decentralized, with seventeen autonomous regions overseeing healthcare. However, penitentiary healthcare is managed nationally, except in Catalonia, the Basque Country, and Navarra. These variations impact mental health care provision for inmates with serious mental illness (SMI).
Objective: To delineate differences between regions in terms of mental health care provision for individuals with SMI, available resources, and the perspectives of healthcare professionals operating in the Spanish prison environment.
Methods: Employing an explanatory sequential mixed-method approach, the study conducted an extensive literature review, quantitative data collection through structured questionnaires, and qualitative data collection via focus groups and four in-depth interviews. Analysis involved calculating percentages and ratios for quantitative data and thematic analysis for qualitative data interpretation to comprehensively understand mental healthcare provision.
Results: In December 2021, about 4% of inmates in Spain had SMI. There are three distinct models of mental healthcare within the Spanish prison system. The traditional penitentiary model, representing 83% of the incarcerated population, operates independently under the General Secretariat of Penitentiary Institutions at a national level. This model relies on an average of 5.2 penitentiary General Practitioners (pGP) per 1,000 inmates for psychiatric and general healthcare. External psychiatrists are engaged for part-time psychiatric assessment. Acute psychiatric hospitalization occurs in general nursing modules within penitentiary centers or in Restricted Access Units (RAUs) in reference hospitals. Two penitentiary psychiatric hospitals provide care to unimputable SMI inmates from all over Spain. Innovative penitentiary models, constituting 17% of the prison population, integrate penitentiary healthcare within regional public health systems. The Basque Country features a Mental Health Unit with full-time care teams within the penitentiary center. Catalonia emphasizes community care, providing full-time dedicated psychiatric services within and outside prisons, ensuring continued care in the community. Both models prioritize personnel with specialized mental health training and compensation akin to non-prison healthcare settings.
Conclusions: Regional disparities in penitentiary mental healthcare models in Spain result in resource inequalities, impacting specialized care for inmates with SMI and opportunities for healthcare professionals. The models in the Basque Country and Catalonia offer valuable experiences for penitentiary healthcare.
1 Introduction
The occurrence of mental illnesses among incarcerated individuals ranges from as low as 2% to as high as 48% in various studies (1). In most cases, this rate surpasses the estimated prevalence of these disorders in the general community. In the challenging prison environment, individuals grappling with serious mental illness (SMI) confront heightened vulnerability (1). This vulnerability stems from the debilitating psychiatric symptoms they often endure, compromised overall health, and significant limitations in their social functioning, necessitating support for basic daily tasks. SMI is a practical classification based on clinical diagnosis, lasting over two years, and the presence of disability, whether functional or intellectual (2, 3) This classification empowers healthcare professionals to identify individuals most in need and tailor mental health interventions accordingly (4).
Spain comprises 17 autonomous regions, each with the authority to oversee its healthcare system and provide healthcare services to residents under the public National Health System. However, penitentiary healthcare has remained under the jurisdiction of the General Secretariat of Penitentiary Institutions at the national Ministry of Interior, a non-health care orientated institution, in most regions, except Catalonia, the Basque Country and Navarra. This raises concerns, particularly when one considers that prisons are not designed to function as clinical treatment facilities and lack the adequate expertise, infrastructure and funding to provide the comprehensive care necessary for individuals with SMI (1, 5).
Spanish overarching legal framework guarantees inmates the same health rights and healthcare services, including pharmaceutical and non-pharmaceutical benefits, as the general population outside prison walls. It stresses the importance of healthcare objectives, the proportionality of security measures, and the desirability of delivering care and treatment as close to the inmate’s home community as possible (6–9).
In 2003, the Cohesion and Quality of the National Health System Law mandated the crucial transfer of penitentiary healthcare responsibilities from the Ministry of the Interior’s General Secretariat of Penitentiary Institutions to regional governments (10). This transfer aimed to integrate these healthcare services into regional healthcare systems, covering the healthcare needs of all residents in the regions under the public National Healthcare System. Regions were provided with the option to decide when to assume these responsibilities within an 18-month period (10). As of 2023, only Catalonia, the Basque Country, and Navarra have embraced these roles. The other 14 regions are not yet in compliance with the law and the General Secretariat of Penitentiary Institutions at the national level remains responsible for the psychiatric and overall healthcare of inmates.
Given this uneven landscape, regional differences determine the disparate organization, structure, and management of healthcare services within prisons, impacting the most vulnerable groups, including inmates with SMI. This research seeks to answer the question: How is healthcare provision for incarcerated individuals with SMI managed in Spanish penitentiary facilities? It aims to describe regional differences in healthcare provision for individuals with SMI, available resources, and the perspectives of healthcare professionals operating in the prison environment. Additionally, it seeks to showcase the achievements attainable by integrating penitentiary healthcare provision into regional healthcare systems, highlighting two innovative models in the Basque Country and Catalonia that may serve as references for future endeavors.
2 Materials and methods
An explanatory sequential mixed-method approach was employed. Mixed-methods research is an investigative technique in which a researcher or a team combines elements of both qualitative and quantitative research methods, including qualitative and quantitative perspectives, data collection, analysis, and inference techniques (11).
The research process involved three main steps: a literature review was conducted to establish the current knowledge on the topic; structured questionnaires were used to collect quantitative data from the General Secretariat of Penitentiary Institutions regarding healthcare resources; and qualitative data was gathered through focus groups with healthcare professionals involved in SMI care within penitentiary settings, followed by in-depth interviews with experts from regions that had transitioned penitentiary healthcare responsibilities from national to regional governments. It is important to note that Navarra is included in the group of regions that have not yet assumed responsibility for their penitentiary healthcare. As of the time of reporting these research findings, the traditional model of penitentiary healthcare provision still prevails, as Navarra only acquired these responsibilities in 2021.
Supplementary Figure 1 illustrates the research methodology used.
2.1 Literature review
An extensive and organized narrative review of the literature was conducted to comprehensively depict the current state of healthcare for individuals with SMI in Spanish penitentiary facilities (12). This review encompassed both indexed literature and gray literature, serving as the foundation for the research thesis and helping to identify gaps in existing knowledge.
For indexed literature, searches were conducted on databases like PubMed, Scopus, Google Scholar, MEDES, and Dialnet, targeting relevant publications in both Spanish and English (Supplementary Table 1 and Supplementary Figure 2 provide search details). In the gray literature, data was collected from official Spanish and international websites, with a particular emphasis on European sources offering content in Spanish or English. Additionally, non-indexed specialized electronic journals were consulted, conference publications were reviewed, and both indexed and gray literature were manually searched to supplement the insights gained from focus groups and expert interviews.
The extensive and organized narrative review of the literature conducted helped to identify and summarize diverse sources, which may not have been captured in a systematic review. In these cases, a comprehensive narrative review allows for the flexibility to include diverse sources, explore the complexity of the topic, and achieve a more comprehensive understanding (13). Due to the diverse nature of the publications, the comprehensiveness of the review, and the fact that literature was also sought to contrast and compare findings in the research, it is not possible to state the final number of publications retrieved and reviewed. This approach aligns with the recommendations for comprehensive literature searches, which emphasize the importance of thorough and systematic searches to minimize bias and ensure comprehensive coverage of the research topic (14).
The review uncovered inconclusive evidence in several areas, including the availability of healthcare resources, the profile and prevalence of individuals with SMI in penitentiary centers, the presence of specialized care resources, drugs consumptions, and the care trajectory for inmates requiring mental health services both within and outside prison. While pockets of knowledge existed regarding best practices and effective care models, notably the Catalan penitentiary mental health care model and the developing penitentiary mental healthcare unit in the Basque Country, their visibility within the scientific literature remained limited. To address these knowledge gaps, focus groups were conducted, expert interviews were held, and additional data was obtained from the Spanish General Secretariat of Penitentiary Institutions through a structured questionnaire (see Supplementary Figure 1).
2.2 Quantitative data collection
The quantitative data presented in this research was obtained from various sources. This included referring to the annual reports published by the General Secretariat of Penitentiary Institutions, which contained data up to 2020 and had been updated in 2021. Additionally, other reports from the same institution were consulted as they were published in response to specific inquiries from the Spanish Parliament and were made available in the Official Gazette of the Cortes Generales.
Furthermore, a structured questionnaire was employed to request supplementary data from the General Secretariat of Penitentiary Institutions. This questionnaire focused on human and healthcare resources, as well as drug usage in penitentiary centers in regions where penitentiary healthcare management had not been transferred from the national to the regional authorities. The data request was for the year 2020 and was submitted electronically through the transparency portal of the General State Administration.
2.3 Qualitative data collection
2.3.1 Focus groups
Five focus groups were conducted between May 31 and July 19, 2022. Each group consisted of 2 to 6 health professionals, totaling 11 primary care physicians and psychiatrists, 4 nurses, and 3 pharmacists who provide daily healthcare in Spanish prisons, and care for inmates with serious mental health problems. Focus groups allowed to gain insight into participants’ perspectives, attitudes, beliefs, and opinions on mental healthcare provision for seriously ill inmates (15, 16).
Multiple focus groups were conducted to ensure information saturation, a point at which recurring data no longer adds interpretive value or when emerging theories adequately explain collected data (17). Three to six different focus groups, or the same meeting several times, are sufficient to achieve information saturation in research contexts like this (18).
A limited number of participants were chosen for each focus group (intentional sampling), with selection criteria based on their specialized knowledge and professional experience within the specific domain of penitentiary healthcare (17). Invitations were extended to the medical director of all 71 Spanish penitentiary centers, and those who responded affirmatively (n=23) were invited to contribute to this study.
Invitations were sent via email, and all participants who accepted (n=18) took part in focus groups lasting between 100 and 153 minutes. Two participants were located in the Basque Country, while the remaining focus group interviewees worked in regions that did not have penitentiary healthcare responsibilities at the time of the study. Participants were categorized based on two criteria: either they belonged to a large (> 1000), medium (450-1000), or small (< 450) penitentiary center according to the number of detainees in their respective centers, or they were associated with the penitentiary psychiatric hospitals. Participants from Catalonia preferred to provide written information and declined to participate in the focus groups.
To guide these focus groups, a set of open-ended questions was used to address various topics, including the specific care needs of inmates with SMI, human and structural care support resources available for penitentiary and community penitentiary healthcare, everyday mental healthcare provision.
2.3.2 In-depth interviews
The primary objective of the in-depth interviews was to gain a comprehensive understanding of good practices and innovative models for the provision of mental healthcare identified in the literature review and focus groups. They had been implemented in specific penitentiary settings in concrete regions (19–21). Key experts responsible for these initiatives were selected and invited to participate in two-hour interviews, which were audio-recorded and transcribed.
To guide these interviews, the researcher used a set of open-ended questions that focused on various aspects of the practice or model core characteristics. These questions covered topics such as the model’s inception, the needs it addresses, the care it provides, the political and financial context in which it operates, its structure, and organization, the profile of beneficiaries, factors contributing to its success, areas for improvement, and prospects.
2.4 Data analysis
2.4.1 Quantitative data
Due to limited and sometimes inconsistent data, percentages were used to describe aspects of prison populations, and no additional scales or statistical tests were applied to summarize the data. Data on the total prison population by region and penitentiary center was primarily derived from 2020 figures with updates through 2021 (see Supplementary Table 2 for source details). Information about inmates with high mental healthcare needs was obtained from the PAIEM (Programa de Atención Integral al Enfermo Mental) program as of July 2019, the latest publicly available data (22). Calculations for assessing the relationship between individuals with SMI and the total prison population by region were based on 2019 data (see Supplementary Table 3).
Data on structural healthcare resources within penitentiary facilities, including the number of nursing module beds and the availability of Restricted Access Units (RAU) in referral hospitals, were extracted from the 2020 and 2021 General Reports of the General Secretariat of Penitentiary Institutions (23, 24). Ratios of these resources per 100 incarcerated individuals were calculated using 2020 data, as specified in Supplementary Table 3. The Reports of the General Secretariat of Penitentiary Institutions, issued annually, provide an overview of facilities, resources, and the health situation of the incarcerated population in Spain. However, the data is reported in aggregated form, limiting its interpretation and research usability. Additionally, the National Institute of Statistics (INE), which provides data on the total incarcerated population size grouped by regions, gender, type of offense, and sentence, was consulted in this study to contrast findings (25). The Report of the General Secretariat of Penitentiary Institutions was chosen for consistency.
Ratios assessing the availability of physicians working in prisons for 2020 were estimated using data obtained from the General Secretariat of Penitentiary Institutions in response to a public information request (see Supplementary Table 2) (26). Additionally, ratios of penitentiary General Practitioners (pGP) per 1000 inmates, categorized by region, were calculated for 2018, 2019, and 2021 following the methodology outlined in Supplementary Table 3, with data sources referenced in Supplementary Table 2.
The percentage of medical personnel who retired for various reasons, including voluntary retirement or age-related factors, relative to the total medical staff, was calculated based on annual reports from the General Secretariat of Penitentiary Institutions for 2018, 2019, 2020, and 2021 (23, 24, 27, 28).
The ratio of psychiatrists specializing in mental health per 1,000 inmates at each penitentiary center was based on 2019 data obtained from a parliamentary response (29). The percentage of full-time dedication among psychiatrists was estimated using input from prison healthcare professionals in focus groups. Estimates of psychiatric healthcare resource utilization in 2020 were derived from data provided by the General Secretariat of Penitentiary Institutions (26, 30, 31), covering specialized psychiatric consultations, admissions to nursing modules for psychiatric pathologies, and hospital discharges following admission to reference hospitals for mental disorders, relative to the total available healthcare resources.
2.4.2 Qualitative data
The analysis of both the focus groups and the individual interviews involved a team of three researchers. Initially, two researchers independently analyzed the transcripts, and any discrepancies in their analyses were resolved by the third researcher. To facilitate this process, the researchers utilized the MAXQDA® tool, which provided support for coding, analysis, and synthesis of the transcripts.
2.4.2.1 Focus groups
The focus group sessions were recorded, transcribed, and analyzed using a deductive-inductive approach following the constant comparison thematic analysis technique (32). This technique allowed for assessing information saturation across multiple focus groups, revealing recurring themes with subtle variations based on the penitentiary center’s size to which participants were affiliated (17).
2.4.2.2 In-depth interviews
Thematic analysis of the in-depth interview transcripts was conducted with a deductive approach (32). The findings from the in-depth interviews encompassed themes such as the Extended Bridge (Puente Extendido) program, deprescribing practices, rational medication usage, innovative and comprehensive mental healthcare provision models in the Basque Country and Catalonia, respectively. This paper focuses on mental healthcare provision models existing in the Spanish penitentiary setting, with subsequent publications addressing good practices like deprescribing and rational medication use in prisons.
2.5 Ethical aspects
The research protocol received approval from the Research Ethics Committee at Ramón y Cajal University Hospital on February 22, 2022 (MINUTES 428).
3 Results
3.1 The Spanish incarcerated population
Official data from December 2021 revealed that Spain’s total prison population stood at 55,097 inmates, which included pre-trial detainees. Among them, 45,617 individuals (83.0%) were under the jurisdiction of regions still managed by the General Secretariat of Penitentiary Institutions (33) (Figure 1). Women comprised 7.1% of the overall inmate population in ordinary Spanish prisons (33). In Spain, the majority of women were incarcerated in mixed penitentiary centers (34, 35).
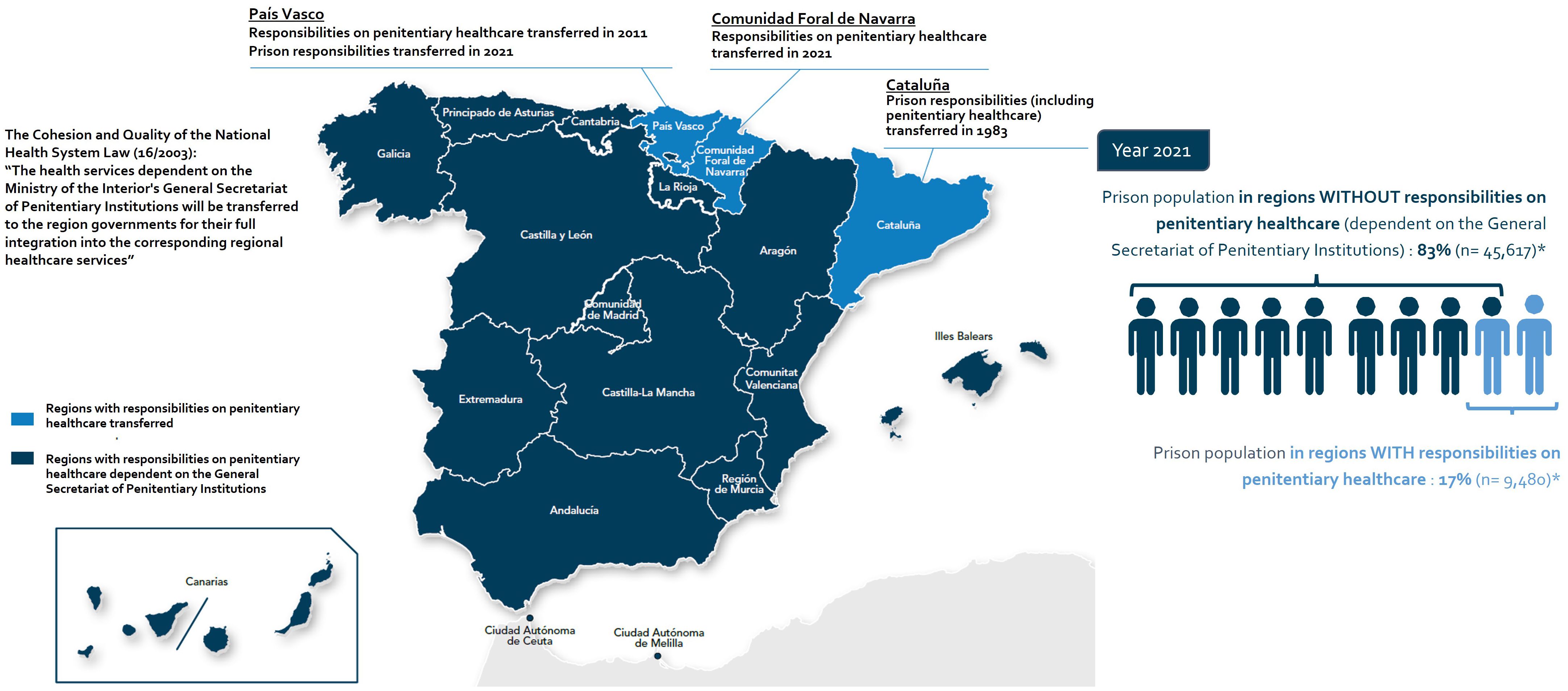
Figure 1. Distribution of the prison population in penitentiary centers in regions with and without responsibilities on penitentiary healthcare provision in Spain. * Estimate made based on the three regions with transferred prison healthcare responsibilities, using as prison population data those corresponding to the year 2021, extracted from the National Statistical Data Report on the prisoner population for December 2021 issued by the General Secretariat of Penitentiary Institutions (33). For the preparation of this map, the Spanish official names of the regions were used.
These numbers remain very similar in 2023 representing a prison population rate of 113 per 100,000 inhabitants based on an estimated national population of 48.06 million at beginning of January 2023 (36).
The distribution of the incarcerated population varied across regions, as did the available resources for their care. In 2020, the General Secretariat of Penitentiary Institutions oversaw a total of 66 ordinary penitentiary centers (excluding Catalonia and the Basque Country). The most populous regions, Andalusia, the Community of Madrid, and the Valencian Community, had the highest number of incarcerated individuals and the most prisons (26) (Supplementary Table 4).
3.2 The Spanish incarcerated population with SMI
Although several epidemiological studies have sought to assess the prevalence of individuals with SMI in Spanish prisons (Supplementary Table 5) determining its precise percentage poses a challenge due to data limitations (37).
Considering 2021 estimates from the General Secretariat of Penitentiary Institutions, around 4% of inmates in Spanish penitentiary centers had SMI. This estimate took into account the number of individuals participating in the PAIEM that registered 1,834 inmates during that year (Supplementary Table 4) (24). Based on PAIEM participation data, SMI was present in 90.2% of male inmates and 9.8% of female inmates (23, 24). Their distribution varied across Spanish regions, with Andalusia (24%) and the Valencian Community (20%) reporting the highest percentages (22).
The most common diagnoses were psychotic (32%), dual (a mental health disorder associated with a substance use disorder (SUD), 27%), and affective disorders (14%) (23). Personality disorders accounted for 21% of all diagnoses (24, 38). More than one third of those with SMI required a high level of assistance due to reduced autonomy (23, 24) (Supplementary Table 6).
3.3 The traditional mental healthcare model for the incarcerated population with SMI in regions without penitentiary healthcare responsibilities
In 14 out of 17 regions (all regions with the exception of the Basque Country, Catalonia and Navarra), healthcare provision in the penitentiary setting remains dependent on the General Secretariat of Penitentiary Institutions and operates as a parallel, separated system with limited integration into the National Healthcare System (39, 40) (Figure 1).
The traditional penitentiary healthcare model delivers primary care using resources within the penitentiary institutions. Specialized healthcare, on the other hand, draws upon resources from the National Healthcare System outside of prisons (39, 40) (Figure 2A). Psychiatric hospitalization takes place in two penitentiary psychiatric hospitals situated in Alicante and Seville, which serve the entire Spanish unimputable population with SMI outside Catalonia and the Basque Country. Due to limited capacity, individuals judicially involved and diagnosed with SMI requiring psychiatric care and treatment are admitted to ordinary penitentiary centers. Here, psychiatric care is provided by part-time, external consultants who visit inmates in prisons while acute hospitalizations mostly take place in general nursing modules within the penitentiary center or at general referral hospitals (41) (Supplementary Table 4).
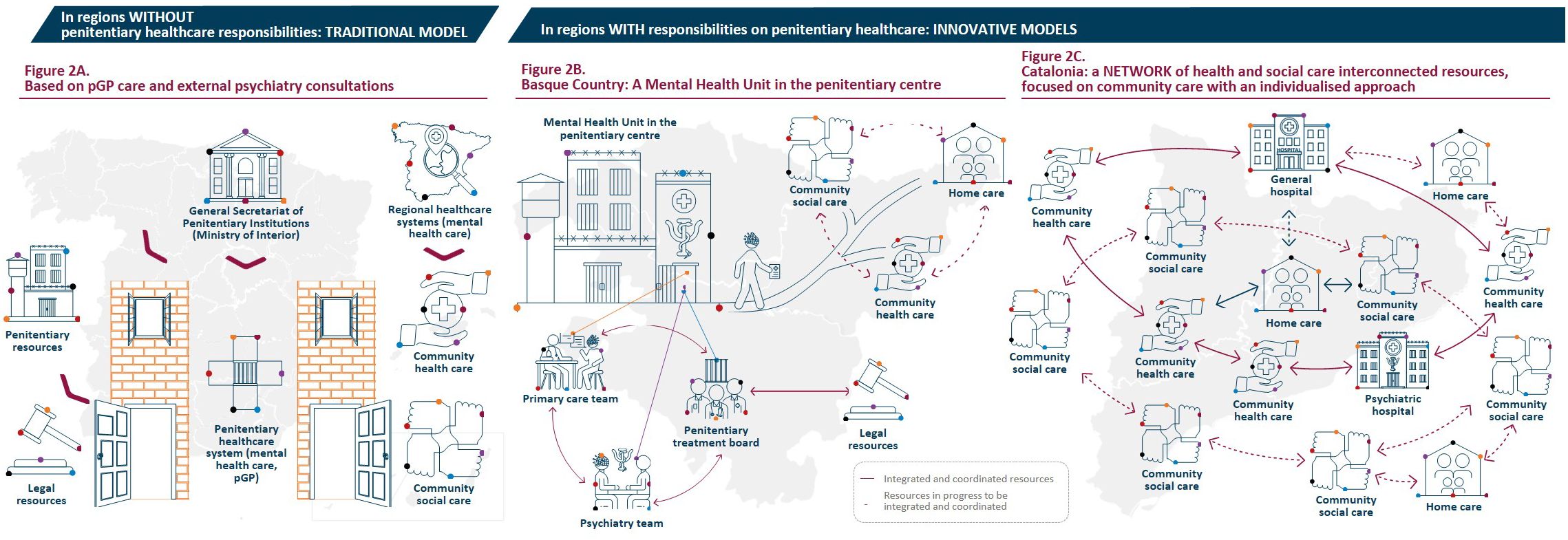
Figure 2. Models for mental healthcare provision in penitentiary centers in Spain. (A) in regions without penitentiary healthcare responsibilities, a traditional model prevails in which the penitentiary healthcare system operates independently and in parallel with the regional healthcare systems. Health care is mostly provided by pGP and access to specialized healthcare, including psychiatric care, is significantly compromised in this scenario. (B, C) in regions with penitentiary healthcare responsibilities, innovative models have emerged. The integration of the penitentiary healthcare system into the regional healthcare systems has improved the availability and access to healthcare resources, promoting coordinated services to ensure adequate psychiatric care. pGP, penitentiary general practitioner.
3.3.1 General practitioners in the traditional penitentiary healthcare model
In 2020, ordinary penitentiary centers had an average of 5.2 pGP per 1,000 inmates (23), lower than the World Health Organization (WHO) European region average of 8.0 (42). Although some regions exceeded the WHO average, most of them had ratios at or below 7 pGP per 1,000 inmates. The ratio was lower in larger penitentiary centers (2.0 - 6.3 pGP per 1,000) compared to the smaller ones (4.0 - 21.7 pGP per 1,000) (Supplementary Table 7). In over 40% of the ordinary penitentiary centers, medical staff primarily worked on-call, with no in-person duties unless deemed necessary (26).
Moreover, between 2018 and 2020, the ratio of primary care General Practitioners (pGPs) per 1,000 inmates declined from 6.1 to 5.2. This decrease primarily stemmed from limited recruitment of professionals, resulting in a more pronounced reduction in medical personnel compared to the growth of the prison population. This trend persisted into 2021 (23, 24, 27, 28, 43). Healthcare professionals who participated in the focus groups corroborated these findings, which are also documented in the literature (44, 45) (Tables 1, 2). Challenging working conditions, lack of professional recognition and incentives, and uncertainty regarding career advancement prompt many to explore alternative career paths outside of correctional facilities. With a relatively small penitentiary healthcare workforce, replenishing it poses significant challenges, leading to fewer professionals bearing heavier workloads (44, 45).
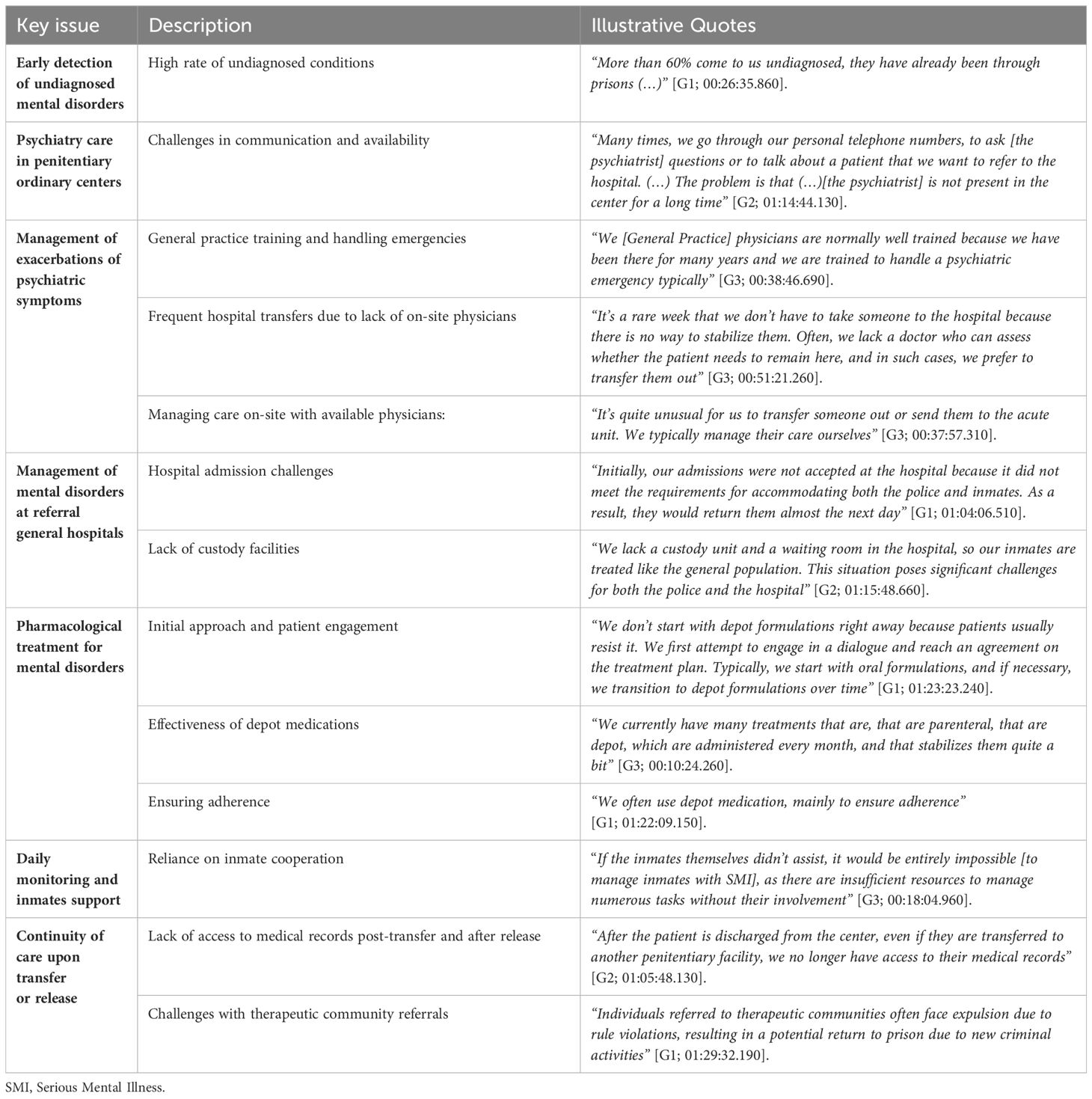
Table 1. Challenges in managing SMI in central penitentiary administration’s ordinary prisons: insights from healthcare professionals in focus groups.
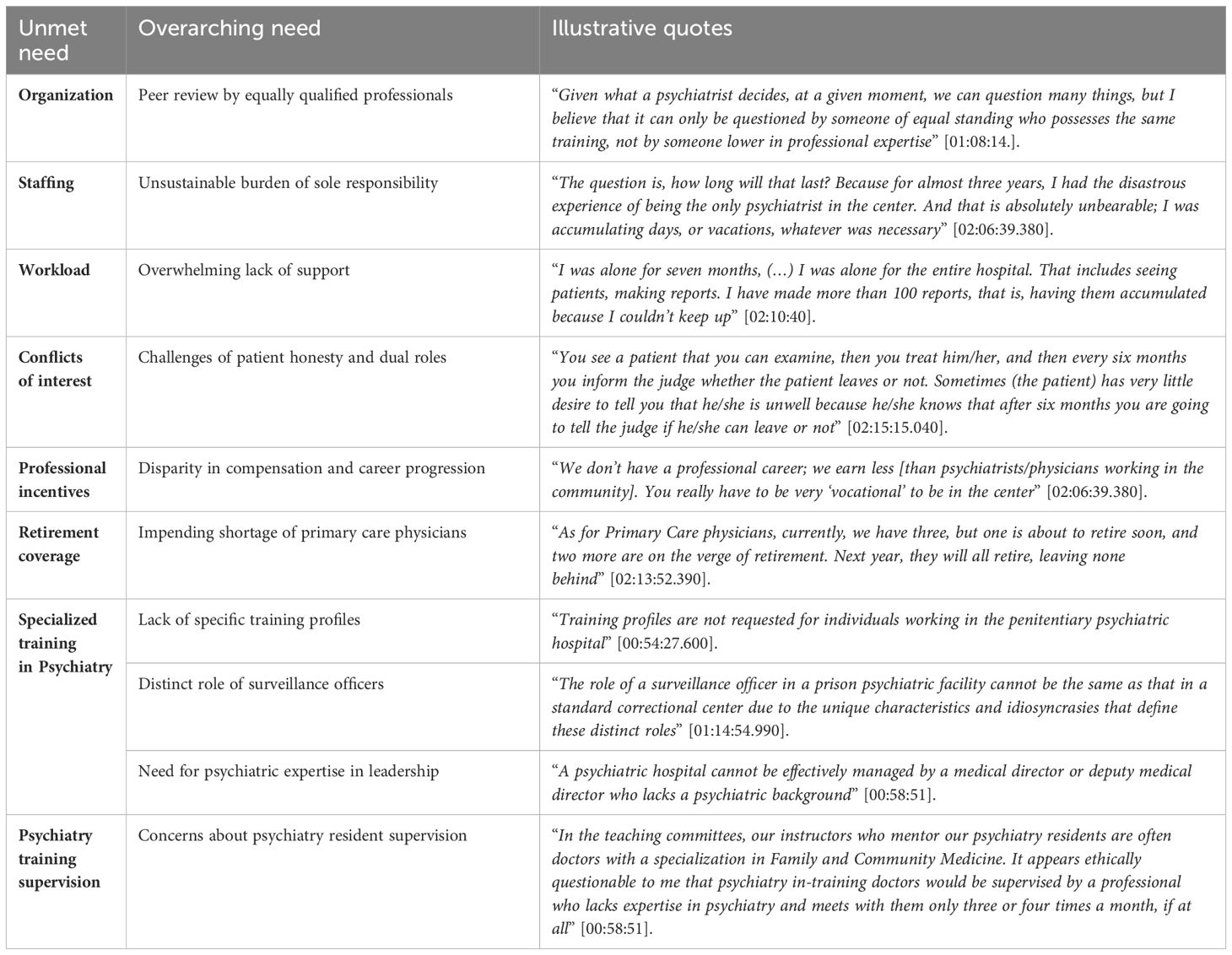
Table 2. Unmet needs in penitentiary psychiatric hospitals under the central penitentiary administration in Spain: insights from healthcare professionals in focus groups.
3.3.2 Psychiatrists in the traditional penitentiary healthcare model
Ambulatory specialized psychiatric care within ordinary penitentiary centers ruled by the General Secretariat of Penitentiary Institutions relies on psychiatrists working part-time as referral consultants under various contractual arrangements (Supplementary Table 4). Psychiatric care was available in 95% of ordinary penitentiary centers, and out of these, 61% (38 out of 62) were provided by psychiatrists affiliated with public healthcare services (30). As of 2019, only one psychiatrist was employed by the Central Penitentiary Administration, who served at the Madrid II Penitentiary Center (29, 46). However, in the absence of official data to reference, healthcare professionals who participated in focus groups estimated that referral psychiatrists spent around three hours per week in those penitentiary centers with more visitation needs. This estimate amounted to less than 7.5% of a full-time work schedule, which typically involves 40 hours per week. Supplementary Table 7 provides a summary of key dedication estimates based on information shared by focus group participants, categorized according to prison size (small, medium, or large-sized). Interestingly, in 2020, psychiatry emerged as the second most sought-after specialty in Spanish prisons, trailing behind dentistry/stomatology (30) (Figure 3).
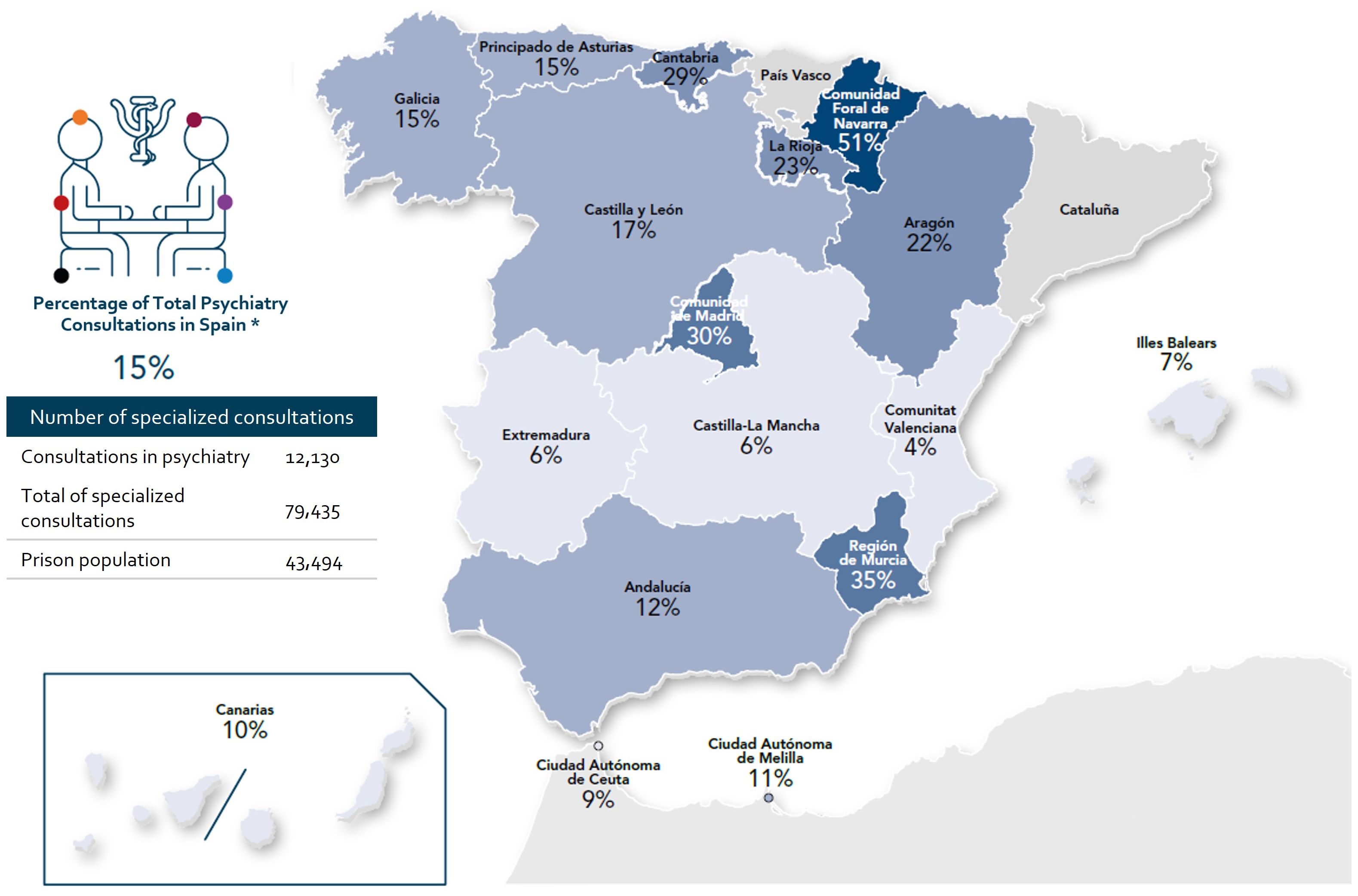
Figure 3. Percentage of psychiatry consultations compared to the total number of specialized consultations in regions without penitentiary healthcare provision responsibilities in 2020. *Percentages calculated from the data on the number psychiatry consultations by regions and total number of specialized consultations by regions*100, extracted from the report generated by the Secretariat General of Penitentiary Institutions (Ministry of the Interior) in response to the request for transparency made by Dr. A. Calcedo, on September 5, 2022 (Annex I Specialized care: global and centers2020 (30). These data do not include the population of the Penitentiary Psychiatric Hospitals of Alicante and Seville. Important note: All presented data are estimates of a specific moment that pretend to reflect the status of the situation and trends at the time of data collection. Data should be interpreted with caution, and the status should be verified at each point in time. For the preparation of this map, the Spanish official names of the regions were used.
3.3.3 Acute psychiatric hospitalization in the traditional penitentiary healthcare model
In 2020, acute psychiatric hospitalization within Spanish ordinary penitentiary centers primarily relied on the general nursing modules operating in the center (Supplementary Table 4). Of the 66 ordinary penitentiary centers under the General Secretariat of Penitentiary Institutions management, 64 were equipped with a total of 2,916 nursing beds, while 2 centers lacked nursing services altogether. The national average ratio of nursing beds to inmates was 6.7 per 100 inmates, but there was significant variation among centers. The ratios ranged from 1.2 to 19.8 beds per 100 inmates, with smaller centers (those with fewer than 450 inmates) typically reporting higher ratios compared to the larger ones (23, 26) (Supplementary Table 7).
During the same year, the nursing modules in these penitentiary centers recorded a total of 21,504 admissions due to various diseases, with 34% attributed to psychiatric pathology (26). For more severe cases and when no nursing resources were available within the penitentiary center, hospitalizations took place within custody areas or RAUs located in reference general hospitals of the public healthcare system. There were 209 RAUs distributed across 39 reference hospitals, with a maximum total capacity of 294 beds. This meant that 86% of penitentiary centers had a reference general hospital with RAUs, with an average of 0.6 beds per 100 inmates (23, 47) (Supplementary Table 7).
In 2020, mental health disorders represented 4% of the total 2,460 hospital discharges reported for the prison population (31). They ranked as the ninth most frequent diagnosis at hospital discharge, following other conditions such as digestive, respiratory, or circulatory diseases (31).
3.3.4 Penitentiary psychiatric hospitals in the traditional healthcare model
Penitentiary psychiatric hospitals are designed to treat individuals who have been declared not fully responsible or not responsible at all for their offenses due to mental health disorders. These hospitals combine psychiatric medical care with correctional measures, and the admission and release of persons in Spain are governed by judicial decisions (48–50).
The General Secretariat of Penitentiary Institutions operates two penitentiary psychiatric hospitals, located in Alicante (caring for a mixed population of males and females inmates) and Seville (caring for only males) (50, 51). In 2021, these hospitals provided care for a total of 573 inmates, with admissions originating from various parts of Spain, excluding Catalonia and the Basque Country, which manage their own prison healthcare provision (24) (Figure 4). The location of these hospitals raises concerns about treatment proximity, a factor recognized as crucial in the recovery and rehabilitation of individuals with SMI (52).
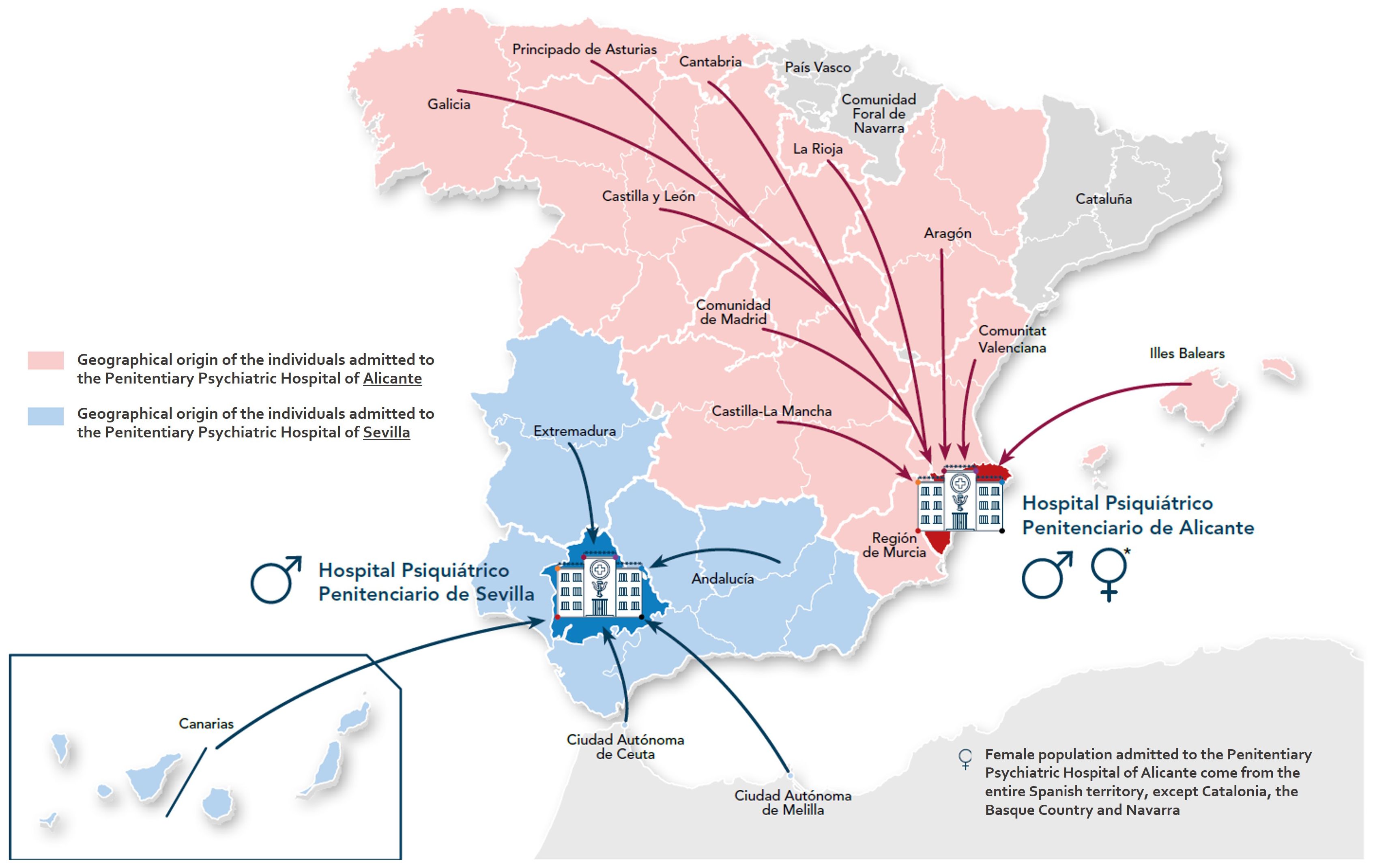
Figure 4. Geographical origin of individuals with SMI admitted to the two penitentiary psychiatric hospitals (in Alicante and Seville) dependent upon the general secretariat of penitentiary institutions (Ministry of Interior) (50, 51). For the preparation of this map, the Spanish official names of the regions were used. Important note: All presented data are estimates of a specific moment that pretend to reflect the status of the situation and trends at the time of data collection. Data should be interpreted with caution, and the status should be verified at each point in time.
The psychiatric hospitals in Alicante and Seville distinguish themselves from standard hospitals by having psychiatrists fulfill dual roles as clinical caregivers and medico-legal experts, with their organization overseen by penitentiary professionals (53). Consequently, a penitentiary approach to care takes precedence over a healthcare approach (51). A shortage of staff was reported in 2020, with 0.8 psychiatrists per 100 inmates in Alicante and 2.6 in Seville (23).
3.4 Innovative mental healthcare models for the incarcerated population with SMI in regions with penitentiary healthcare responsibilities
3.4.1 The Basque country experience
In 2011, the Basque Country government assumed responsibility for healthcare in Basque prisons, committing to uphold inmates’ rights, ensure access to quality healthcare, and promote equitable access, including medical-legal activities (54). One significant challenge was addressing inmates’ mental health needs due to high prevalence, limited resources, and complex organizational structures with unclear medical and legal competencies within prisons (55).
The transfer of prison healthcare from the General Secretariat of Penitentiary Institutions to Osakidetza, the Basque public healthcare service provider, involved 43 professionals across three Basque penitentiary centers serving 1,493 inmates (55). Healthcare professionals were integrated into Osakidetza with the same status as their counterparts outside prisons. Penitentiary healthcare center managers were appointed, healthcare roles and responsibilities were defined, and procedures for covering vacancies were established (55).
Penitentiary centers were transformed into healthcare facilities equivalent to community health centers (56), adopting the same names with “PC” for “penitentiary center” added to their denominations. Each center was linked to a reference hospital and had access to the full medical resources of the three provinces in the Basque Country (57).
3.4.2 A mental health unit within the penitentiary center
The mental healthcare model adopted at the Zaballa penitentiary center in the Basque Country involves a mental health unit, affiliated with Osakidetza, featuring specialized care teams that undertake preventive, diagnostic, and therapeutic interventions, as well as actionable programs directed towards operationalizing the mental health unit within the penitentiary center and with resources in the community outside the prison (Figure 2B) (55, 58, 59).
In 2023, the Mental Health Unit at the Zaballa Penitentiary Center consists of a full-time specialized team (Supplementary Tables 4, 8). This team undergoes continuous training within the unit and develops specific skills through on-the-job experience to address the unique challenges of the penitentiary environment. The work of the multidisciplinary team in the Mental Health Unit is organized into six interconnected workstream areas. These areas are designed to address critical actions. They aim to meet the immediate mental health needs of inmates, such as suicide prevention and promoting appropriate prescribing habits of psychotropic drugs. They also focus on promoting seamless coordination among healthcare, legal, and correctional teams within the penitentiary center and in the community. This coordination aims to enhance healthcare management, improve outcomes for inmates, secure the adequate management of health-related information and facilitate continued care in the community after release from prison.
At the heart of the model’s success is the establishment of effective collaboration between the professional teams in the penitentiary Mental Health Unit, the penitentiary primary care center, both under the purview of Osakidetza, which handles the healthcare responsibilities, and the penitentiary treatment board, which undertakes disciplinary roles. These three teams collectively address the various aspects of inmates’ lives, including their health and compliance with their sentences in the correctional environment.
This model represents an intermediate level of specialized psychiatric care provision (Figure 2B). It is more comprehensive than the traditional penitentiary model, where psychiatrists make specific interventions on an averageable weekly basis (common in most ordinary penitentiary centers in Spain dependent upon the General Secretariat of Penitentiary Institutions). However, it is less complex than models centered around penitentiary psychiatric hospitals seen, for example, in England (51, 60) or the integrated, community care orientated model seen in Barcelona in Catalonia.
Among the medium to long-term psychiatric hospitalization options for judicialized individuals, the 2023-2028 Strategy for Mental Health in the Basque Country (61) describes a range of specific resources. There are acute units located within general hospitals to provide intensive care. Persons with SMI may be admitted urgently through emergency services or scheduled from other care structures, such as the Mental Health Unit in the Zaballa penitentiary center. Stays are typically tailored to individual treatment needs, including diagnostic procedures, detoxification from substances, and attention from various specialists (61). In Gipuzkoa, there is a subsidized penitentiary psychiatry unit at Aita Menni Hospital in Mondragon that functions as a judicial hospitalization facility, admitting individuals with confirmed SMI under court-ordered security measures, offering long-term care for extended psychiatric needs (51, 62) (Supplementary Table 4).
Subacute units, situated in psychiatric hospitals, cater to persons needing longer-term treatment, typically lasting from 1 to 3 months. Additionally, rehabilitation units in psychiatric hospitals offer extended care for persons with severe and chronic mental disorders, with the average length of stay estimated at 365 days. Intermediate care devices, such as mental health day hospitals, aim to prevent relapses and promote early discharges, providing intensive care for patients without requiring full-time hospitalization once released from prison. Residential centers and supported housing options cater to individuals with psychiatric disorders requiring ongoing assistance and stimulation for activities of daily living (61).
The continuity of social and health care in the community post-release of individuals with SMI has been crucial. The integration of Health Management Units, streamlining administrative referrals across Basque provinces, has successfully bypassed administrative barriers for primary care in the community. This allows for direct referrals of individuals within mental healthcare resources across the three Basque provinces. Nonetheless, similar to other regions in Spain, resources often fall short in meeting the long-term health and social needs of these individuals in the community.
3.5 The Catalan experience
In 2021, the total number of inmates in the Catalan penitentiary system was 7,746, a figure that has remained fairly consistent through 2023 (63). The lifetime prevalence of mental health and SUD among inmates in a Catalan penitentiary setting at the end of their sentence has been estimated at 81.4%, with SUD and attention deficit/hyperactivity disorder (ADHD) being the most common diagnoses (51.4% and 31.4%, respectively) (56). The current prevalence of mental health and SUD is 59.0% (56).
3.5.1 Key feature of the Catalan penitentiary mental healthcare model: comprehensive, individualized, community orientated
Following the transfer of healthcare responsibilities to the Catalan Health System, comprehensive agreements and targeted initiatives improved mental health services, integrating them into the public healthcare network (64–67). By 2017, political efforts emphasized enhancing mental healthcare in prisons to ensure equitable access to community-based care, prioritizing the well-being of incarcerated individuals (68–75).
As a result, Catalonia’s current penitentiary healthcare model is well-established, encompassing in-prison psychiatric services with beds, hospitalization, and acute care units, along with rehabilitation units providing individualized monitoring and continuity of care in the community (Figure 2C). The specialized Mental Health Units for hospitalization and rehabilitation, and the Mental Healthcare Programs for continued care in the community are pivotal elements of the model (Supplementary Table 9).
The Penitentiary Psychiatric Hospitalization Unit of Catalonia (PPHU-C) operates as a mixed unit, providing diagnosis and treatment to individuals of all genders under judicial supervision, regardless of their legal status. The unit focuses on those who can benefit from specific programs within its purview (70). It functions as a high-security unit where admission is based solely on medical criteria, with discharge determined by both medical and legal considerations (70). Serving as a supra-sectoral resource, the PPHU-C centralizes Catalonia’s penitentiary mental health services and accommodates a total of 66 inpatient beds. It houses various services and units, each with specific objectives tailored to the required level of care (Supplementary Table 10). Following psychiatric diagnosis, a comprehensive individualized therapeutic plan (ITP) is devised based on the patient’s specific needs (70).
The Psychiatric Hospitalization and Intensive Rehabilitation Unit of Catalonia (PHIRU-C) stands as a highly specialized unit in penitentiary mental health rehabilitation, catering to the entire Catalan incarcerated population with mental disorders (Supplementary Table 10) (69, 75). It adopts a multidisciplinary, recovery-focused approach organized into a continuum of two programs: the Rehabilitation Program which focuses on skill recovery, functional enhancement, and symptom stabilization, and the Community Transition Program, which supports the individual’s reintegration into civilian life. The PHIRU-C works alongside other outpatient services within Catalonia’s sociosanitary care model for judicialized individuals with mental health issues.
Within the community, the Individualized Support Program (ISP) ensures continuity of care through a clinical-social model with intensive follow-up. It assigns a professional case manager to coordinate a tailored therapeutic plan for each individual. In the penitentiary setting, the ISP aims to provide seamless care for individuals with SMI who are at high risk of social exclusion, preventing the onset and persistence of mental health problems (69, 76, 77).
The Primary Care Support Program (PCSP) integrates health and social resources for preventive, proactive, and community-based care. It fosters collaboration between Primary Care Centers (PCC) and Adult Mental Health Centers (AMHC) to enhance mental health care provision. A specialized team, including a psychiatrist, psychologist, and nurse, provides direct care at PCCs, focusing on early detection of decompensation and prevention of self-harm or suicide-related behaviors. The PCSP also offers training and technical support to primary care teams in the community. Each penitentiary center has a dedicated PCSP team collaborating with the regional mental healthcare service provider (73, 78).
The Program for Mental Health Ambulatory Care (PMHAC) is a community-based, multidisciplinary team serving outpatients aged 18 and above with mental disorders. It ensures care continuity, supports families and the community, and participates in rehabilitation and reintegration strategies. The PMHAC prioritizes assisting primary care professionals, caring for individuals with SMI, and coordinating with the entire healthcare system. The PMHAC network collaborates with various levels of health and social care resources within the community (79).
In this way, mental health interventions in Catalonia’s penitentiary psychiatry setting follow a person-centered recovery approach. This empowers individuals to enhance their own capabilities and life skills to improve their quality of life. Recovery-oriented care emphasizes well-being through self-care and early intervention, promoting the long-term recovery efforts, especially for those with SMI. This approach aims to keep SMI individuals in the community, facilitate their reintegration, maintain social connections, and enhance socio-healthcare quality whenever possible (66).
3.6 Challenges and opportunities in penitentiary mental healthcare in Spain: insights from healthcare professionals
Healthcare professionals identified significant challenges and opportunities in the mental health care provided within ordinary penitentiary centers and penitentiary psychiatric hospitals that operate outside the National Health System. In ordinary prisons, they emphasized the need for early detection of mental disorders, the critical role of psychiatrists, managing symptom exacerbations, and ensuring continuity of care upon release (Table 1).
The penitentiary psychiatric hospitals faced issues such as lack of coordination, conflicts of interest for psychiatrists, heavy workloads, insufficient staffing, training and supervision. Both settings suffer from disparities in working conditions compared to community healthcare, affecting professional motivation and service quality (Table 2). However, aligned with findings from the literature (80), healthcare professionals recognized that imprisonment provides an opportunity to engage with socially disadvantaged individuals who often have difficulty accessing community healthcare services and experience relatively poor health outcomes. This presents the potential for achieving significant health improvements
Conversely, in the Basque Country, healthcare professionals noted improvements after the Basque government’s integration of the penitentiary healthcare system into the regional healthcare system. Benefits included better job coverage, satisfaction, training opportunities, and salary parity, contributing to enhanced healthcare provision and professional growth (Table 3). The integration also facilitated data sharing through a unified electronic medical record system, improving the continuity and efficiency of care for inmates, especially those with SMI. These insights highlight the potential benefits perceived by healthcare professionals of integrating penitentiary healthcare into broader regional systems to improve outcomes for this vulnerable population.
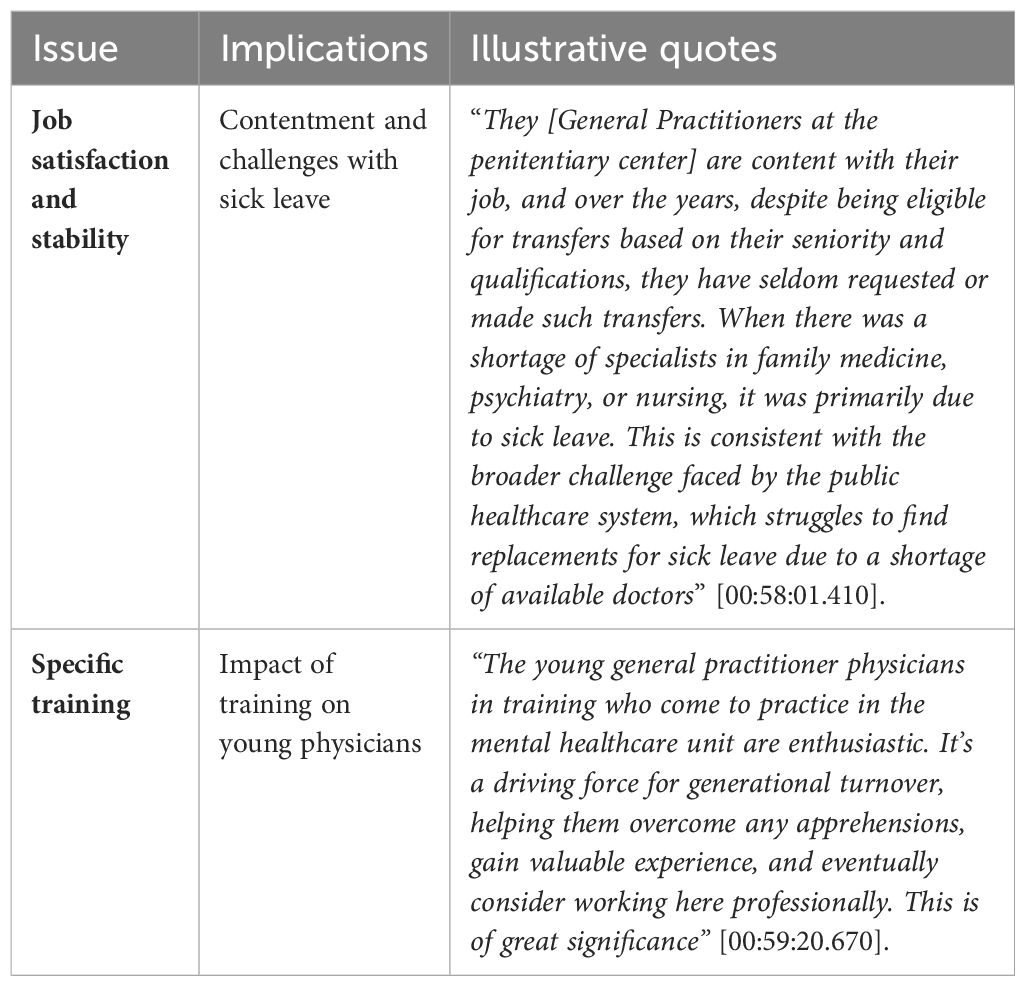
Table 3. Job and training conditions in Basque country penitentiary centers with integrated healthcare: insights from healthcare professionals in focus groups.
4 Discussion
This paper outlines the contrasting models for providing mental health care to inmates with SMI in Spain as of 2023. Using a mixed-method approach, it sheds light on the disparate opportunities available to inmates and penitentiary healthcare professionals based on their location. The analysis reveals that Spain, alongside the United Kingdom, Poland, Germany, France, and Italy, is among the European countries with the highest prison population (81). Additionally, Spain’s proportion of women in its prisons was just above 7% in 2021, which is relatively high compared to other European average of 5.7% for the same year (81). Reported frequencies of SMI in the incarcerated population align with estimates from the 2023 WHO/Europe report on prison health, indicating that mental health disorders were present in 32.8% of the European prison population (82). However, underreporting is likely due to incomplete records of noncommunicable diseases and limited data availability (82).
One key factor contributing to this disparity is whether the handover of penitentiary healthcare responsibilities from the General Secretariat of Penitentiary Institutions at the Ministry of the Interior to regional governments and integration into regional healthcare systems has occurred, as mandated in the early 2000s. The traditional penitentiary model persists in regions that have not sought the assigning of healthcare competencies, covering psychiatric and healthcare services in ordinary penitentiary centers and two penitentiary psychiatric hospitals, impacting over 80% of the inmate population in Spain. In contrast, more innovative models have been implemented in regions with transferred competencies and integrated healthcare systems. As of 2023, this applies to Catalonia (since 1983) the Basque Country (since 2011), and Navarra (since 2021), collectively serving approximately 17% of Spain’s inmate population within their respective territories (54, 68, 83). This disparity leads to unequal access to mental healthcare in the penitentiary setting in Spain, significantly disadvantaging the majority of the incarcerated population with SMI. Consequently, precision in psychiatric diagnoses differs, impacting the mental health treatment received by individuals with a psychiatric disorder, the reliability of prevalence data, and the comparability of the available information across penitentiary centers (84, 85).
The findings described in this paper highlights deficiencies in the prevailing traditional penitentiary mental healthcare model in most Spanish penitentiary centers. These deficiencies encompass a shortage of medical professionals in both ordinary prisons and psychiatric hospitals, insufficient staffing, disparities in working conditions and compensation, limited training and specialization, reliance on pGP for psychiatric care and on general nursing modules for psychiatric hospitalization in ordinary penitentiary centers, and limited access to shared medical records due to the lack of integration into the regional healthcare systems. In 2019 and 2020, the WHO recommended a reference ratio of 1.3 full-time dedicated psychiatrists per 1,000 inmates for the European region to address the needs of SMI inmates (42, 86). However, this target remains far from being met in Spanish regions where penitentiary healthcare provision still relies on the General Secretariat of Penitentiary Institutions. Similarly, the allocation of psychiatric staff in both penitentiary psychiatric hospitals is notably lower than in other European countries such as Germany, France, Italy, and the United Kingdom. In these nations, the ratio of specialist psychiatrists to incarcerated individuals in penitentiary psychiatric hospitals has been estimated to be around 5 (51), despite documented challenges in staff coverage and inconsistent utilization of psychiatric penitentiary hospitalization resources (87–91).
This situation may resemble the challenges faced in penitentiary healthcare systems in other parts of the world where prisoners with SMI lack prompt access to specialist mental healthcare professionals or aftercare services on return to prison from in-patient psychiatric services (92–95). Instead, they may receive care from non-specialist healthcare providers, sometimes with the informal support of peer workers (90). In contrast, countries with larger mental health budgets and more psychiatrists per capita, such as Australia, Portugal, and Germany, provide prisoners with access to comprehensive mental health multidisciplinary care (92) similar to the care offered in Alava in the Basque Country and in Catalonia. Experience in England and Wales highlights the need for sufficient resources to ensure screening, triage, assessment, intervention, and reintegration, which constitute essential elements of prison mental health provision to enhance the well-being of this diverse population (80). Other studies confirm the generally positive change in mental health symptoms during detention when adequate mental healthcare is provided (96).
The insufficiency of psychiatric care within correctional facilities due to limited structural and human resources has been well-documented in Spain since 2004 and beyond (97–100). This shortage mirrors the broader situation outside correctional centers, with Spain exhibiting one of the lowest ratios of psychiatric specialists per 100,000 inhabitants in Europe, standing at just 12 psychiatrists per 100,000 inhabitants. This is in contrast to the regional European average of 18 to 20 psychiatrists per 100,000 inhabitants reported for 2020 (101). Notably, there is considerable variability in the availability of psychiatric specialists among different regions, with the Basque Country and Catalonia boasting the highest ratios at 15 and 13 per 100,000 inhabitants, respectively. This difference is likely attributed to the political importance and incentives given to mental healthcare in these regions. Furthermore, Spain significantly lags behind the European average in terms of the number of psychiatric hospital beds available in the community (101). Additionally, the ratio of primary care physicians operating in the community is notably low, with just 0.8 professionals per 1,000 inhabitants as of 2020 (102). Although similar shortcomings have also been described in France, Germany, Italy and the United Kingdom, available resources seem to be more widely available compared with the scenario that predominates in most parts of Spain (87–91, 103).
The traditional penitentiary healthcare model in Spain which assigns the mental health care of inmates with SMI to ordinary penitentiary centers and two penitentiary psychiatric hospitals in regions without assumed prisons healthcare responsibilities, contrasts with the European Commission’s recommendations for mental health and well-being actions (104). These recommendations advocate for transitioning from institutional to community-based mental health care (105). However, providing care for inmates with SMI in the community requires multidisciplinary teams, comprehensive health and social care networks, recovery-focused care, staff training, digital technology use, suitable housing, sustainable policies, and collaborative relationships (106). This underscores the importance of significant investment and collective commitment (107) as demonstrated by the experiences in the Basque and Catalan regions reflected in this study. Stakeholder involvement is crucial in deinstitutionalization planning and barriers such as low political priority, insufficient funding, consensus gaps, and limited cooperation between health and social sectors have been widely reported (92, 108). Consequently, the development of effective and efficient community-based service networks remains partial in many European countries, and primary mental health care for SMI continues limited (109).
The experience in Italy comprises the deinstitutionalization of the forensic psychiatric system that involved replacing psychiatric hospitals with Residenze per l’Esecuzione delle Misure di Sicurezza (REMS) and transitioning to community-based treatment for forensic psychiatric patients (110, 111). By 2019, 30 REMS facilities were established across different regions, designed to house up to 20 patients each with a primary focus on therapy and rehabilitation. Notably, these treatments have a limited duration and do not involve police officers. This shift to the Italian REMS model was prompted by the prior forensic psychiatric hospital system, which faced significant issues such as overcrowding, poor hygiene, inadequate treatment programs, non-therapeutic hospitalizations, the presence of penitentiary police personnel, and potentially indefinite admissions (112). Similar challenges were encountered in the two penitentiary psychiatric hospitals run by the General Secretariat of Penitentiary Institutions in Spain. The implementation of the REMS model has effectively addressed these challenges, marking a positive shift in Italy’s approach to forensic psychiatric care (51, 111).
On the other hand, the mental health intervention model implemented in Emilia-Romagna prisons introduces other innovative aspects. Firstly, it adopts a therapeutic approach modeled on multi-professional treatments commonly offered in Italian adult community mental healthcare services. Secondly, it establishes intramural multi-disciplinary Mental Healthcare Service Teams (MHSTs) dedicated to addressing mental health issues. Thirdly, it promotes a culture of collaboration in planning personalized therapeutic-rehabilitation interventions in conjunction with prisoners, their families, and local social/mental healthcare services, ensuring continuity of care during the individual’s transition between prison and the community. This model aims to be accessible to all prisoners in need, structured across different phases of incarceration including assessment, detention, and release. Contrary to traditional approaches, this model emphasizes the role of a multi-disciplinary team rather than solely relying on psychiatrists, thereby redefining the organizational structure of intramural MHSTs (113).
The Mental Health Unit in the Zaballa penitentiary center established in the Basque Country share common features with a similar model established in England (60). Both units are conceived to provide short-term care and ongoing support to prisoners with acute and complex mental health needs until transfer to a psychiatric hospital or back into the prison system. Planning, development and implementation of both models include clear commitment, political will, budgetary responsibility, and pathways for effective collaboration with mental health community teams and services (60).
The establishment of full-time inpatient units designed for inmates, known as Unités d’Hospitalisation Spécialement Aménagées (UHSA), in France, such as the one created at the Paul-Guiraud de Villejuif hospital, also resembles the experience described in the Mental Health Unit at the Zaballa penitentiary center. The significant changes in forensic psychiatry services have led to improvements in mental health care access and positive outcomes at the UHSA, including a slight decrease in prison suicide rates, similar to the objectives promoted in the Zaballa’s mental health unit. By 2016, eight UHSAs with 380 beds were operational in France (114), but frequent hospitalization of inmates in general psychiatric hospitals (47% of 5,121 psychiatric inmates hospitalizations) persists (114, 115). This trend may stem from the relatively low capacity of UHSAs compared to the increasing incarcerated population. Additionally, substantial distances of up to 300 km between UHSAs and certain prisons might impede emergency UHSA hospitalization, necessitating reliance on local, reachable, general psychiatric facilities. Limited human resources further complicate prisoner transfers from prisons to UHSAs (114). Despite these hardnesses, a satisfaction survey conducted in two UHSAs indicated inmates’ preference for and contentment with hospitalization within the UHSAs over general psychiatric hospitals (116). These changes in penitentiary mental health care have sparked debates (117, 118). Some argue for a dedicated care system within French prisons, while others advocate for keeping psychiatric teams separate from prison environments (117). In line with this debate, the French system prioritizes the separation between the justice and healthcare systems, emphasizing the importance of caregivers’ professional independence and medical confidentiality. This approach aligns with the delineation of roles and functionalities advocated at the Zaballa penitentiary center mental health unit.
In Catalonia, integrating the penitentiary healthcare system into the public healthcare network, establishing specialized units, and expanding mental health services within penitentiary centers and the community have led to a comprehensive and community-focused approach. This represents a significant shift in prison mental healthcare, emphasizing individual needs, recovery support, and community reintegration. Catalonia’s evolving model showcases commitment to care and rehabilitation for inmates with SMI. Given the diversity and lack of evidence in mental health systems for offenders across Europe (89), the Catalan and the Basque models may offer valuable experiences for other regions.
Overall, the experiences of most Spanish regions, where psychiatric care takes place in ordinary penitentiary centers with limited access to other specialized resources, including the penitentiary psychiatric hospitals, differ significantly from those in the Basque Country and Catalonia. Political will, stakeholder understanding, compromise, and leadership are needed to optimize penitentiary mental healthcare provision. After release from prison, accessible pharmacological interventions are paramount in any prevailing model of mental health care. Long-acting injectable antipsychotic medications (depot) with extended dosing intervals that provide adequate symptom control over long periods once symptoms stabilize and treatment simplifies, significantly enhance adherence in individuals with SMI in the community, This effect remains consistent regardless of the impact of sustained outpatient commitment lasting 6 months or longer (119, 120). Long-acting injectable antipsychotic medications offer crucial treatment for SMI individuals, especially those struggling with daily oral medication or limited healthcare access. Biannual dosing, with relapse rates as low as 3.9% over 2 years, ensures efficacy and safety, reducing relapses and functional impairment (121). Eliminating the need for daily doses may enhance patient acceptance, diminish stigma, and boost self-esteem favoring their permanence in the community. Longer medication intervals particularly suit higher-risk patients, like those with recent-onset schizophrenia or in transitional care or challenging living conditions (122).
Limitations in this study stem from a lack of a more detailed information on the therapeutic services within traditional administrative structures, impeding a comprehensive understanding of their approach. While newer systems in the Basque Country and Catalonia show promise, the absence of reported results and outcome measures prevents a thorough assessment of their effectiveness. Additionally, the study does not incorporate perspectives from individuals, as well as their caregivers, with lived experience of SMI within the prison environment, restricting insight into their attitudes towards the newer systems and their potential impact on well-being. The paper also overlooks the empirical question of whether these changes will result in tangible improvements in the lives of incarcerated individuals with SMI, underscoring a gap in understanding and evaluation that warrants further research.
Regarding the methods used, potential subjective and cognitive biases were mitigated through comparison, contextualization and consensus. Caution is necessary when interpreting quantitative data from official reports and public information requests due to poor data availability, which aligns with the lack of high-quality, systematically collected data in forensic psychiatry reported across many European countries (123, 124).
5 Conclusions
In conclusion, a dichotomy persists in Spain where both traditional and innovative models of mental healthcare for inmates with SMI coexist in different regions. This divide primarily hinges on whether the responsibility for managing and delivering healthcare in prisons has been decentralized from the national Ministry of Interior to regional healthcare systems as legally stated. Regrettably, this anomaly begets a glaring imbalance in the availability of healthcare resources, processes, and opportunities, disadvantaging both inmates and healthcare professionals working within the prison system and undermining the quality of penitentiary healthcare in most parts of Spain. The innovative and comprehensive models for providing mental healthcare to inmates with SMI, as exemplified in the Basque Country and Catalonia, are feasible and can serve as blueprints for other regions as they assume responsibility for penitentiary healthcare provision.
Data availability statement
The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number(s) can be found in the article/Supplementary Material.
Author contributions
AC-B: Conceptualization, Funding acquisition, Investigation, Resources, Supervision, Validation, Visualization, Writing – review & editing. JAB: Conceptualization, Funding acquisition, Investigation, Methodology, Resources, Supervision, Validation, Writing – review & editing. SPR: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Resources, Visualization, Writing – original draft, Writing – review & editing. AMA: Data curation, Investigation, Resources, Supervision, Validation, Writing – review & editing. EEZ: Data curation, Investigation, Resources, Supervision, Validation, Writing – review & editing. VEC: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Writing – review & editing. ALL: Investigation, Resources, Supervision, Validation, Writing – review & editing. LFBF: Investigation, Resources, Validation, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This research was funded by an Educational Grant (ICD: 1619588) awarded by Janssen Pharmaceuticals. The grant supported various activities essential to the development and publication of this research, including data collection, analysis, and manuscript preparation. The funding source had no role in the conception, analysis, or communication of the results of this study. The research was developed and published independently by the authors.
Acknowledgments
The authors express their special gratitude to all the professionals who willingly and selflessly participated in the focus groups and individual interviews, dedicating their time and sharing their valuable insights. Furthermore, the authors extend their thanks to the Spanish General Secretariat of Penitentiary Institutions for their cooperation in providing data by completing the relevant questionnaire. Lastly, the authors acknowledge and appreciate the support received from the respective Scientific Societies in Spain (Sociedad Española de Psiquiatría Legal and Sociedad Española de Sanidad Penitenciaria) throughout the entire project’s completion.
Conflict of interest
SPR and VEC were employed by company SmartWorking4u.
The authors declare that this study received funding from Janssen Pharmaceuticals. The funder had the following involvement in the study: data collection, analysis, and manuscript preparation. The funding source had no role in the conception, analysis, or communication of the results of this study. The research was developed and published independently by the authors.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2024.1340155/full#supplementary-material
Abbreviations
ADHD, attention deficit/hyperactivity disorder; AMHC, Adult Mental Health Centers; ISP, Individualized Support Program; ITP, individualized therapeutic plan; PAIEM, Programa de Atención Integral al Enfermo Mental; pGP, penitentiary General Practitioners; PCC, Primary Care Centers; PHIRU-C, Psychiatric Hospitalization and Intensive Rehabilitation Unit of Catalonia; PMHAC, Program for Mental Health Ambulatory Care; PPHU-C, Penitentiary Psychiatric Hospitalization Unit of Catalonia; PCSP, Primary Care Support Program; RAU, Restricted Access Units; REMS, Residenze per l’Esecuzione delle Misure di Sicurezza; SMI, Serious Mental Illness; SUD, Substance Use Disorder; UHSA, Unités d’Hospitalisation Spécialement Aménagées; WHO, World Health Organization.
References
1. Canada K, Barrenger S, Bohrman C, Banks A, Peketi P. Multi-level barriers to prison mental health and physical health care for individuals with mental illnesses. Front Psychiatry. (2022) 13:777124. doi: 10.3389/fpsyt.2022.777124
2. Martínez-Martínez C, Richart-Martínez M, Ramos-Pichardo JD. Operational definition of serious mental illness: heterogeneity in a review of the research on quality-of-life interventions. J Am Psychiatr Nurses Assoc. (2020) 26:229–44. doi: 10.1177/1078390320902823
3. Zumstein N, Riese F. Defining severe and persistent mental illness-A pragmatic utility concept analysis. Front Psychiatry. (2020) 11:648. doi: 10.3389/fpsyt.2020.00648
4. Conejo Cerón S, Moreno Peral P, Morales Asencio JM, Alot Montes A, García-Herrera JM, González López MJ, et al. Opiniones de los profesionales del ámbito sanitario acerca de la definición de trastorno mental grave. Un estudio cualitativo [Opinions of healthcare professionals on the definition of severe mental illness: a qualitative study]. Sist Sanit Navar. (2014) 37:223–33. doi: 10.4321/s1137-66272014000200005
5. Brooker C, Monteiro J. Prisons and probation: a Council of Europe White Paper on the management of offenders with mental health disabilities and disorders(2021). Available online at: https://rm.coe.int/pc-cp-2021-8-rev-6-white-paper-regarding-persons-with-mental-health-di/1680a69439 (Accessed October 26, 2023).
6. Gobierno de España. Jefatura del Estado. Ley General de Sanidad 14/1986 de 25 de abril. Boletín Of del Estado- BOE-A-1986-10499(1986). Available online at: https://www.boe.es/buscar/act.php?id=BOE-A-1986-10499 (Accessed September 20, 2023).
7. Gobierno de España - Ministerio de Justicia e Interior. Real Decreto 190/1996, de 9 de febrero, por el que se aprueba el Reglamento Penitenciario. Boletín Of del Estado - BOE-A-1996-3307(1996). Available online at: https://www.boe.es/buscar/act.php?id=BOE-A-1996-3307 (Accessed September 20, 2023).
8. Gobierno de España- Jefatura del Estado. Ley Orgánica 1/1979, de 26 de septiembre, General Penitenciaria. Boletín Of del Estado- BOE-A-1979-23708(1979). Available online at: https://www.boe.es/eli/es/lo/1979/09/26/1/con (Accessed October 20, 2023).
9. Gobierno de España- Jefatura del Estado. Ley Orgánica 10/1995, de 23 de noviembre, del Código Penal. Bol Of del Estado - BOE-A-1995-25444(1995). Available online at: https://www.boe.es/buscar/act.php?id=BOE-A-1995-25444 (Accessed September 20, 2023).
10. Gobierno de España- Jefatura del Estado. Ley 16/2003, de 28 de mayo, de cohesion y calidad del Sistema Nacional de Salud. Bol Of del Estado - BOE-A-2003-10715(2003). Available online at: https://www.boe.es/buscar/act.php?id=BOE-A-2003-10715 (Accessed September 20, 2023).
11. Schoonenboom J, Johnson RB. How to construct a mixed methods research design. Kolner Z Soz Sozpsychol. (2017) 69:107–31. doi: 10.1007/s11577-017-0454-1
12. Williams J. A comprehensive review of seven steps to a comprehensive literature review. Qual Rep. (2018) 23:345–9. doi: 10.46743/2160-3715/2018.3374
13. Sukhera J. Narrative reviews: flexible, rigorous, and practical. J Grad Med Educ. (2022) 14:414–7. doi: 10.4300/JGME-D-22-00480.1
14. Gentles SJ, Charles C, Nicholas DB, Ploeg J, McKibbon KA. Reviewing the research methods literature: Principles and strategies illustrated by a systematic overview of sampling in qualitative research. Syst Rev. (2016) 5:1–11. doi: 10.1186/s13643-016-0343-0
15. Wong L. Focus group discussion: a tool for health and medical research. Singapore Med J. (2008) 49:256.
16. Donaldson DR, Koepke JW. A focus groups study on data sharing and research data management. Sci Data. (2022) 9:1–7. doi: 10.1038/s41597-022-01428-w
17. Onwuegbuzie AJ, Dickinson WB, Leech NL, Zoran AG. A qualitative framework for collecting and analyzing data in focus group research. Int J Qual Methods. (2009) 8:1–21. doi: 10.1177/160940690900800301
18. Hennink M, Kaiser B, Weber M. What influences saturation? Estimating sample sizes in focus group research. Qual Heal Res. (2019) 29:1483–96. doi: 10.1177/1049732318821692
19. Hughes KL, Williamson PR, Young B. In-depth qualitative interviews identified barriers and facilitators that influenced chief investigators’ use of core outcome sets in randomised controlled trials. J Clin Epidemiol. (2022) 144:111–20. doi: 10.1016/J.JCLINEPI.2021.12.004
20. Azad A, Sernbo E, Svärd V, Holmlund L, Brämberg EB. Conducting in-depth interviews via mobile phone with persons with common mental disorders and multimorbidity: the challenges and advantages as experienced by participants and researchers. Int J Environ Res Public Health. (2021) 18(21):11828. doi: 10.3390/IJERPH182211828
21. Brazier J, Connell J, Papaioannou D, Al E. Chapter 6. A qualitative analysis of interviews with mental health service users, in: A systematic review, psychometric analysis and qualitative assessment of generic preference-based measures of health in mental health populations and the estimation of mapping functions from widely used specific measures. (2014). Southampton (UK). Available online at: https://www.ncbi.nlm.nih.gov/books/NBK262013/ (Accessed October 18, 2022).
22. Secretaría de Estado de Relaciones con las Cortes y Asuntos Constitucionales, Gobierno de España. Respuesta del Gobierno a la pregunta escrita (entrada 2492) al Congreso 184/284- 18/06/2019 por Jon Iñarritu García (GMx). Boletín Of las Cortes Gen(2019). Available online at: https://www.congreso.es/entradap/l13p/e0/e_0002492_n_000.pdf (Accessed September 7, 2022).
23. Secretaria General de Instituciones Penitenciarias, Ministerio del Interior - Gobierno de España. Informe General de Instituciones Penitenciarias 2020(2020). Available online at: https://www.institucionpenitenciaria.es/es/web/home/fondo-documental/publicaciones (Accessed September 8, 2022).
24. Secretaría General de Instituciones Penitenciarias, Ministerio del Interior - Gobierno de España. Informe General de Instituciones Penitenciarias 2021(2021). Available online at: https://www.institucionpenitenciaria.es/es/web/home/fondo-documental/publicaciones (Accessed February 8, 2023).
25. Instituto Nacional de Estatística. Estadística de Condenados: Adultos/Menores. Año 2021. Condenados por Sentenc firme - Año 2021(2021). Available online at: https://www.ine.es/dyngs/INEbase/es/operacion.htm?c=Estadistica_C&cid=1254736176793&menu=ultiDatos&idp=1254735573206 (Accessed September 22, 2022).
26. Secretaría General de Instituciones Penitenciarias, Ministerio del Interior- Gobierno de España. Respuesta a la solicitud por transparencia realizada por el Dr. A. Calcedo, el 5 de septiembre 2022. (Anexo II- Estadística Sanitaria 2020. Atención primaria en instituciones penitenciarias (global y centros). Madrid, Spain: Ministerio del Interior (2022). pp. 1–76 p.
27. Secretaría General de Instituciones Penitenciarias, Ministerio del Interior - Gobierno de España. Informe General de Instituciones Penitenciarias 2019(2019). Available online at: https://www.institucionpenitenciaria.es/es/web/home/fondo-documental/publicaciones (Accessed September 8, 2022).
28. Secretaría General de Instituciones Penitenciarias, Ministerio del Interior - Gobierno de España. Informe General de Instituciones Penitenciarias 2018(2018). Available online at: https://www.institucionpenitenciaria.es/es/web/home/fondo-documental/publicaciones (Accessed September 8, 2022).
29. Secretaría de Estado de Relaciones con las Cortes y Asuntos Constitucionales, Gobierno de España. Respuesta del Gobierno a la pregunta escrita (entrada 12086) al Congreso 184/1595- 23/12/2019 de Jon Iñarritu García (GEHB). Boletín Of las Cortes Gen(2019). Available online at: https://www.congreso.es/entradap/l14p/e1/e_0012086_n_000.pdf (Accessed September 7, 2022).
30. Secretaría General de Instituciones Penitenciarias, Ministerio del Interior- Gobierno de España. Respuesta a la solicitud por transparencia realizada por el Dr. A. Calcedo, el 5 de septiembre 2022 (Anexo I Estadística sanitaria 2020. Atención especializada global y por centros). Madrid, Spain: Ministerio del Interior (2022). pp. 1–68 p.
31. Secretaría General de Instituciones Penitenciarias, Ministerio del Interior- Gobierno de España. Respuesta a la solicitud por transparencia realizada por el Dr. A. Calcedo, el 5 de septiembre 2022. (Anexo IV Ingresos hospitalarios de II.PP. Nacional, CC.AA. y centros 2020). Madrid, Spain: Ministerio del Interior (2022). pp. 1–189 p.
32. Bonner C, Tuckerman J, Kaufman J, Costa D, Durrheim DN, Trevena L, et al. Comparing inductive and deductive analysis techniques to understand health service implementation problems: a case study of childhood vaccination barriers. Implement Sci Commun. (2021) 2:100. doi: 10.1186/s43058-021-00202-0
33. Secretaría General de Instituciones Penitenciarias, Subdirección General de Relaciones Institucionales y Coordinación Territorial, Ministerio del Interior - Gobierno de España. Datos estadísticos de la población reclusa. Total Nacional Diciembre 2021(2021). Available online at: https://www.institucionpenitenciaria.es/es/estadística-mensual-2021 (Accessed September 5, 2022).
34. Comité Europeo de Prevencion de la Tortura. Informe al Gobierno Español sobre la visita a España realizada por el Comité Europeo Para La Prevención de la Tortura y tratos o penas inhumanas o degradantes CPT/Inf (2021) 27. Counc Eur(2021). Available online at: https://rm.coe.int/1680a47a78 (Accessed September 21, 2022).
35. Dorado CJ. Delincuencia y población penitenciaria femeninas: situación actual de las mujeres en prisión en España. Rev Electrónica Cienc Penal y Criminol. (2018) 20:1–32.
36. Institute for Crime & Justice Policy Research. World prison brief data(2023). Available online at: https://www.prisonstudies.org/country/Spain (Accessed October 31, 2023).
37. López M, Laviana M, Saavedra FJ, López A. Problemas de salud mental en población penitenciaria. Un enfoque de salud pública. Rev la Asoc Española Neuropsiquiatría. (2021) 41:87–111. doi: 10.4321/S0211-57352021000200005
38. Secretaría General de Instituciones Penitenciarias, Ministerio del Interior - Gobierno de España. Informe general instituciones penitenciarias 2022(2022). Available online at: https://www.institucionpenitenciaria.es/es/web/home/fondo-documental/publicaciones (Accessed November 1, 2023).
39. Iñigo C, Márquez I, Grupo de trabajo sobre Salud Mental en Prisión. Guía: Atencion primaria de las salud mental en prisión. (2011). Available online at: https://consaludmental.org/publicaciones/Guiaatencionprimariasaludmentalprision.pdf (Accessed September 22, 2022).
40. Barrios Flores LF. La internación psiquiátrica por razón penal en España: ejecución de la medida en el ámbito penitenciario. Rev Crim. (2015) 57:45–60.
41. Barrios Flores LF. Derecho y salud mental: logros conseguidos y retos pendientes en España. Informe SESPAS 2020. Gac Sanit. (2020) 34:76–80. doi: 10.1016/j.gaceta.2020.04.011
42. WHO Regional Office for Europe. Status report on prison health in the WHO European Region(2020). Available online at: https://www.who.int/europe/publications/i/item/9789289058674 (Accessed October 1, 2023).
43. Procesos selectivos-Cuerpo Facultativo de Sanidad Penitenciaria (Acceso libre). Minist del Inter - Gob España(2022). Available online at: https://www.interior.gob.es/opencms/es/servicios-al-ciudadano/empleo-publico/procesos-selectivos/cuerpos-de-instituciones-penitenciarias/cuerpo-facultativo-de-sanidad-penitenciaria/acceso-libre/ (Accessed May 1, 2023).
44. García Guerrero J. Transferencia de competencias en materia de Sanidad Penitenciaria a las Comunidades Autónomas: la visión de los profesionales. Rev Española Sanid Penit. (2006) 8:103–5.
45. Vera E. Biomedical research in Spanish prisons: a reality full of difficulties. Rev Española Sanid Penit. (2021) 23:46–8. doi: 10.18176/resp.00030
46. Arnau Peiró F. Atención psiquiátrica en prisiones: hacia la inevitable integración de los servicios de salud autonómicos en el abordaje de los internos con problemas de salud mental. Rev Española Sanid Penit. (2022) 24:40–2.
47. Secretaría General de Instituciones Penitenciarias, Subdirección General de Relaciones Institucionales y Coordinación Territorial, Ministerio del Interior - Gobierno de España. Datos estadísticos de la población reclusa. Total Nacional Diciembre 2020(2020). Available online at: https://www.institucionpenitenciaria.es/es/estadística-mensual-2020 (Accessed September 5, 2022).
48. Añaños-Bedriñana FT, Burgos-Jiménez R, Rodríguez-Sanjuán A, Turbi-Pinazo AM, Soriano C, Llopis-Llacer JJ. Salud mental en prisión. Las paradojas socieducativas EduPsykhé. (2017) 16:98–116.
49. Roldán Barbero H. ¿A dónde van los enfermos mentales que cometen delitos? Rev Electrónica Estud Penal y la Segur. (2019) (5):HR–1.
50. Dirección General de Coordinación Territorial de Medico Abierto, Coordinación de Sanidad, Secretaría General de Instituciones Penitenciarias, Ministerio del Interior. Hospitales Psiquiátricos dependientes de la Administración Penitenciaria. Propuesta de Acción. Minist del Inter(2011). Available online at: https://consaludmental.org/publicaciones/Hospitalespsiquiatricosadministracionpenitenciaria.pdf (Accessed September 21, 2022).
51. Barrios LF. El internamiento psiquiátrico penal en España: situación actual y propuestas de futuro. Norte salud Ment. (2021) XVII:25–38.
52. Simpson AIF, Gerritsen C, Maheandiran M, Adamo V, Vogel T, Fulham L, et al. A systematic review of reviews of correctional mental health services using the STAIR framework. Front Psychiatry. (2022) 12:747202/FULL. doi: 10.3389/FPSYT.2021.747202/FULL
53. FEAFES Andalucía Salud Mental, Jimenez Fernandez A, Torres Platero A. Buenas prácticas en intervención por personas con enfermedad mental(2016). Available online at: https://consaludmental.org/publicaciones/Buenas-practicas-intervencion-salud-mental-Andalucia.pdf (Accessed September 20, 2023).
54. Gobierno de España, Ministerio de Política Territorial y Administración Pública. Real Decreto 894/2011, de 24 de junio, sobre traspaso de funciones y servicios de la Administración del Estado a la Comunidad Autónoma del País Vasco en materia de sanidad penitenciaria. Madrid Spain: Agencia Estatal Boletín Oficial del Estado (2011).
55. Instituto de Reintegración Social de Bizkaia (IRSE) - ARARTEKO. La atención sociosanitaria a la salud mental de las personas privadas de libertad en la Comunidad Autonoma del País Vasco. (2014). Available online at: https://consaludmental.org/publicaciones/Atencionsociosanitariasaludmentalprivacionlibertad.pdf (Accessed October 20, 2022).
56. Pagerols M, Valero S, Dueñas L, Bosch R, Casas M. Psychiatric disorders and comorbidity in a Spanish sample of prisoners at the end of their sentence: Prevalence rates and associations with criminal history. Front Psychol. (2023) 13:1039099. doi: 10.3389/fpsyg.2022.1039099
57. Zulaika D, Etxeandia P, Bengoa A, Caminos J, Arroyo-Cobo JM. [A new prison health care model: the experience of the Basque Country]. Rev española Sanid Penit. (2012) 14:91–8. doi: 10.4321/s1575-06202012000300004
58. InfoPrision. Araba/Álava(2022). Available online at: https://infoprision.com/centros-penitenciarios/arabaálava (Accessed January 3, 2023).
59. Gobierno Vasco- Departamento de Igualdad Justicia y Politicas Sociales. Bases para la implantación del modelo penitenciario en Euskadi. (2021). Available online at: https://www.euskadi.eus/contenidos/informacion/administracion_penitenciaria/es_def/adjuntos/modelo_penitenciario_euskadi_2021.pdf.
60. Dyer W, Cassidy K, Ridley L, Biddle P, McClelland N, Brandon T. The development of a prison mental health unit in england: understanding realist context(s). Int J Forensic Ment Health. (2021) 20:101–17. doi: 10.1080/14999013.2020.1830890
61. Departamento de Salud - Gobierno Vasco. Estrategia de Salud Mental de Euskadi 2023-2028(2024). Available online at: https://www.euskadi.eus/contenidos/documentacion/doc_sosa_esme/es_def/estrategia_salud_mental:es.pdf (Accessed January 18, 2024).
62. Hermanas Hospitalarias. Unidad de Psiquiatría Legal. Unidad Psiquiatr Leg(2023). Available online at: https://www.aita-menni.org/es/unidad/unidad-psiquiatria-legal-mondragon/ (Accessed April 23, 2023).
63. Gencat, Instituto de Estadística de Cataluña. Población penitenciaria. Por sexo. Provincias(2022). Available online at: https://www.idescat.cat/indicadors/?id=aec&n=15858&lang=es&t=202200 (Accessed October 30, 2023).
64. Carlson Aburto J, Balsera Gómeza J, Lalucat Job L, Teixidó Casasb M, Berruezo Ortizc M, Ureña Hidalgod T, et al. Perfil de los usuarios de dos programas de gestión de casos para la atención a pacientes con trastornos mentales severos (TMS): el Programa de Seguimiento Individualizado (PSI-TMS) vs. El Programa de Atención Específica (PAE-TMS). Rehabil Psicosoc. (2008) 5:9–16.
65. Generalitat de Catalunya. Programa de Prevenciò i Atenciò a la Cronicitat. Bases para un modelo catalán de atención a las personas con necesidades complejas(2017). Available online at: https://scientiasalut.gencat.cat/bitstream/handle/11351/3305/bases_modelo_catalan_atencion_personas_necesidades_complejas_2017_cas.pdf?sequence=5 (Accessed October 28, 2023).
66. Davidson L, González-Ibáñez À. La recuperación centrada en la persona y sus implicaciones en salud mental. Rev la Asoc Española Neuropsiquiatría. (2017) 37:189–205. doi: 10.4321/S0211-57352017000100011
67. Parc Sanitari Sant Joan de Deu, Xarxa de Salud Mental. Psiquiatria penitenciària(2020). Available online at: https://www.pssjd.org/serveis-assitencials/xarxa-salut-mental/psiquiatria-penitenciaria (Accessed September 20, 2023).
68. Gobierno de España- Presidencia del Gobierno. Real Decreto 3482/1983, de 28 de diciembre, sobre traspasos de servicios del Estado a la Generalidad de Cataluña en materia de Administración Penitenciaria(1984). Available online at: https://www.boe.es/buscar/doc.php?id=BOE-A-1984-4310 (Accessed October 1, 2023).
69. Generalitat de Catalunya, Departament de Salut, Departament de Justicia. Acord de coordinació entre el Departament de Justícia i el Departament de Salut per al desenvolupament D’un Programa D’atenció A La Salut Mental i les Addiccions en el marc de les actuacions dels serveis d’execució penal a Catalunya(2021). Available online at: https://justicia.gencat.cat/web/.content/home/departament/convenis_i_acords/2022/ep-c-dept-salut-programa-salut-mental.pdf (Accessed October 30, 2023).
70. Sant Joan de Déu Servei de Salut Mental. Unitat D’hospitalizació Psiquiàtrica Penitenciària de Catalunya(2008). Available online at: https://www.sepapbcn.org/archivos/cauce27_noviembre_2.pdf (Accessed October 1, 2023).
71. Parc Sanitari Sant Joan de Deu, Xarxa de Salud Mental. Psiquiatria penitenciària. Barcelona, Spain: Parc Sanitari Sant Joan de Deu (2020).
72. GenCat - Portal Jurídic de Catalunya. Decret 399/2006, de 24 d’octubre, pel qual s’assignen al Departament de Salut les funcions en matèria de salut i sanitàries de les persones privades de llibertat i de menors i joves internats en centres de justícia juvenil, i s’integren en el sistema sani(2006). Available online at: https://portaljuridic.gencat.cat/eli/es-ct/d/2006/10/24/399.
73. Pérez-Ibáñez O, García-Pedrajas C, Grases N, Marsó E, Cots I, Aparicio S, et al. Programa de soporte a la primaria: un análisis descriptivo y de concordancia diagnóstica entre médico/a de atención primaria y psicólogo/a. Rev la Asoc Española Neuropsiquiatría. (2015) 35:257–66. doi: 10.4321/s0211-57352015000200002
74. Generalitat de Catalunya, Departament de Salut. Pla Director de Salut Mental i Adiccions de Catalunya(2006). Available online at: https://consaludmental.org/publicaciones/PlandirectorsaludmentalCatalunyacatalan.pdf (Accessed October 28, 2023).
75. Generalitat de Catalunya, Departament de Salut, Departament de Justicia. Acord de coordinació entre el Departament de Justícia i el Departament de Salut per al desenvolupament d’un programa d’atenció a la salut mental i les addiccions en el marc de les actuacions dels serveis d’execució penal a Catalunya(2017). Available online at: https://justicia.gencat.cat/web/.content/home/departament/convenis_i_acords/2017/sp_c_salut.pdf (Accessed October 28, 2023).
76. Generalitat de Cataluyna. Pla de serveis individualitzats (PSI). CatSalut - Estudis i informes tècnics [279](2003). Available online at: https://scientiasalut.gencat.cat/handle/11351/3316?locale-attribute=ca (Accessed August 8, 2022).
77. Macià-Astorch L, Martínez-Azofra A, Luna E, Plazas F, Llerena S, Fernández-García S, et al. El gestor de casos: reinserción en la comunidad y continuidad asistencial en población penitenciaria con Trastorno Mental Severo (TMS), in: Ponencias y comunicaciones del XII Congreso Nacional y XX Jornadas Nacionales de la Sociedad Española de Sanidad Penitenciaria COnference. Cartagena Spain. (2018). p. 87.
78. Caballero Calvo-Rayo S, Cuadrado-Vives C, Olivé A. Programa Soporte a la primaria en centros penitenciarios de Catalunya, in: Ponencias y comunicaciones del XII Congreso Nacional y XX Jornadas Nacionales de la Sociedad Española de Sanidad Penitenciaria COnference. Cartagena, Spain (2018).
79. Ajuntament del Prat de Llobregat. Centro de Salud Mental de Adultos (CSMA)(2022). Available online at: https://www.elprat.cat/persones/invertim-en-salut/centre-de-salut-mental-dadults-csma?lan=es#googtrans(ca%7Ces) (Accessed October 10, 2022).
80. Forrester A, Till A, Simpson A, Shaw J. Mental illness and the provision of mental health services in prisons. Br Med Bull. (2018) 127:101–9. doi: 10.1093/bmb/ldy027
81. European Prison Observatory. Prisons in Europe. 2019 report on European prisons and penitentiary systems(2019). Available online at: http://www.prisonobservatory.org/upload/Prisons in Europe. 2019 report.pdf (Accessed September 21, 2023).
82. World Health Organization (WHO). One-third of people in prison in Europe suffer from mental health disorders. World Heal Organ Eur(2023). Available online at: https://www.who.int/europe/news/item/15-02-2023-one-third-of-people-in-prison-in-europe-suffer-from-mental-health-disorders (Accessed October 31, 2023).
83. Gobierno de España Ministerio de Política Territorial y Función Pública. Real Decreto 494/2021, de 6 de julio, de traspaso de funciones y servicios de la Administración del Estado a la Comunidad Foral de Navarra en materia de sanidad penitenciaria. Madrid: Agencia Estatal Boletín Oficial del Estado (2021).
84. Reingle Gonzalez JM, Connell NM. Mental health of prisoners: identifying barriers to mental health treatment and medication continuity. Am J Public Health. (2014) 104:2328–33. doi: 10.2105/AJPH.2014.302043
85. Mundt AP, Rozas Serri E, Siebenförcher M, Alikaj V, Ismayilov F, Razvodovsky YE, et al. Changes in national rates of psychiatric beds and incarceration in Central Eastern Europe and Central Asia from 1990-2019: A retrospective database analysis. Lancet Reg Heal - Eur. (2021) 7:100137. doi: 10.1016/j.lanepe.2021.100137
86. WHO Regional Office for Europe. Status report on prison health in the WHO European Region(2019). Available online at: https://apps.who.int/iris/bitstream/handle/10665/329943/9789289054584-eng.pdf (Accessed September 15, 2022).
87. Prison Insider. Germany. Germany(2023). Available online at: https://www.prison-insider.com/en/countryprofile/allemagne-2023?s=sante-5cab190969190 (Accessed March 26, 2024).
88. Fovet T, Chan-Chee C, Baillet M, Horn M, Wathelet M, D’Hondt F, et al. Psychiatric hospitalisations for people who are incarcerated, 2009–2019: An 11-year retrospective longitudinal study in France. eClinicalMedicine. (2022) 46:1–12. doi: 10.1016/j.eclinm.2022.101374
89. Salize HJ, Dressing H, Fangerau H, Gosek P, Heitzman J, Markiewicz I, et al. Highly varying concepts and capacities of forensic mental health services across the European Union. Front Public Heal. (2023) 11:1095743. doi: 10.3389/fpubh.2023.1095743
90. Testoni I, Nencioni I, Arbien M, Iacona E, Marrella F, Gorzegno V, et al. Mental health in prison: Integrating the perspectives of prison staff. Int J Environ Res Public Health. (2021) 18(21):11254. doi: 10.3390/ijerph182111254
91. House of Commons - Committee of Public Accounts. Mental health in prisons - Eighth report of Session 2017-19(2017). Available online at: www.parliament.uk (Accessed October 20, 2023).
92. Aboaja A, Pandurangi P, Almeida S, Castelletti L, Rivera-Arroyo G, Opitz-Welke A, et al. Six nations: a clinical scenario comparison of systems for prisoners with psychosis in Australia, Bolivia and four European nations. BJPsych Int. (2023) 20:13–7. doi: 10.1192/bji.2022.16
93. Office of the Inspector of Prisons. Thematic inspection: an evaluation of the provision of psychiatric care in the Irish prison system(2024). Available online at: https://www.oip.ie/wp-content/uploads/2024/02/OIP-Thematic-Inspection-Report-on-Provision-of-Psychiatric-Care-in-Prisons_Feb-2024-Publish.pdf (Accessed October 9, 2023).
94. Bright AM, Higgins A, Grealish A. Women’s experiences of prison-based mental healthcare: a systematic review of qualitative literature. Int J Prison Health. (2022) 19(2): 1–18. doi: 10.1108/IJPH-09-2021-0091
95. Leonard S-J, Webb RT, Shaw JJ. Service transitions, interventions and care pathways following remittal to prison from medium secure psychiatric services in England and Wales: national cohort study. BJPsych Open. (2020) 6:1–8. doi: 10.1192/bjo.2020.62
96. Weber M, Baggio S, Gonçalves LC, Nieuwbeerta P, Dirkzwager AJE. Longitudinal trajectories of mental health problems and their association with reoffending in a Dutch pre-trial prison cohort. Front Psychiatry. (2022) 13:976832. doi: 10.3389/fpsyt.2022.976832
98. Arnau-Peiró F, García-Guerrero J, Herrero-Matías A, Castellano-Cervera JC, Vera-Remartínez EJ, Jorge-Vidal V, et al. Descripción de la consulta psiquiátrica en centros penitenciarios de la Comunidad Valenciana. Rev Española Sanid Penit. (2012) 14:20–31. doi: 10.4321/S1575-06202012000200003
99. Zabala-Baños M, Segura A, Maestre-Miquel C, Martínez-Lorca M, Rodríguez-Martín B, Romero M, et al. Prevalencia de trastorno mental y factores de riesgo asociados en tres prisiones de España. Rev Española Sanid Penit. (2016) 18:13–24.
100. Arnau F, García-Guerrero J, Benito A, Vera-Remartínez EJ, Baquero A, Haro G. Sociodemographic, clinical, and therapeutic aspects of penitentiary psychiatric consultation: toward integration into the general mental health services. J Forensic Sci. (2020) 65:160–5. doi: 10.1111/1556-4029.14137
101. Sociedad Española de Psiquiatría y Salud Mental. Libro Blanco de la Psiquiatría en España(2022). Available online at: https://sepsm.org/wp-content/uploads/2023/06/Libro-Blanco-de-la-Psiquiatria-en-Espana_SEPSM-ok.pdf (Accessed June 8, 2023).
102. Ministerio de Sanidad - Equipo de trabajo del Sistema Nacional de Salud. Informe Anual del Sistema Nacional de Salud 2020-2021. Inf Estud E Investig 2022(2022). Available online at: https://www.sanidad.gob.es/estadEstudios/estadisticas/sisInfSanSNS/tablasEstadisticas/InfAnualSNS2020_21/INFORME_ANUAL_2020_21.pdf (Accessed October 1, 2023).
103. Fovet T, Thibaut F, Parsons A, Salize HJ, Thomas P, Lancelevée C. Mental health and the criminal justice system in France: A narrative review. Forensic Sci Int Mind Law. Article 100028 (2020) 1:100028. doi: 10.1016/j.fsiml.2020.100028
104. European Commission. Joint action on mental health and well-being(2017). Available online at: https://health.ec.europa.eu/system/files/2019-02/2017_towardsmhcare_en_0.pdf (Accessed October 1, 2023).
105. Shields-Zeeman L, Petrea I, Smit F, Walters BH, Dedovic J, Kuzman MR, et al. Towards community-based and recovery-oriented care for severe mental disorders in Southern and Eastern Europe: aims and design of a multi-country implementation and evaluation study (RECOVER-E). Int J Ment Health Syst. (2020) 14:30. doi: 10.1186/s13033-020-00361-y
106. Neave S, Glorney E. Caring for male prisoners who self-harm: perceptions, attitudes and experiences of custodial prison staff and male prisoners in England. Int J Forensic Ment Health. (2023) 0:1–13. doi: 10.1080/14999013.2023.2258103
107. van Genk C, Roeg D, van Vugt M, van Weeghel J, Van Regenmortel T. Current insights of community mental healthcare for people with severe mental illness: A scoping review. Front Psychiatry. (2023) 14:1156235. doi: 10.3389/fpsyt.2023.1156235
108. European Commission. Joint action on mental health and well-being(2017). Available online at: https://health.ec.europa.eu/system/files/2019-02/2017_towardsmhcare_en_0.pdf (Accessed October 9, 2023).
109. Barbato A, Vallarino M, Rapisarda F, Lora A, Caldas De Almeida M. EU Compass for action on mental health and well-being - Access to mental health care in Europe - Consensus paper(2014). Available online at: https://health.ec.europa.eu/system/files/2016-12/ev_20161006_co04_en_0.pdf (Accessed October 10, 2023).
110. Catanesi R, Mandarelli G, Ferracuti S, Valerio A, Carabellese F. The new Italian residential forensic psychiatric system (REMS). a one-year population study. Rass Ital di Criminol. (2019) 13:7–23. doi: 10.7347/RIC-NS2019-p07
111. Leone L, Giunta G, Motta G, Cavallaro G, Martinez L, Righetti A. An innovative approach to the dismantlement of a forensic psychiatric hospital in Italy: A ten-year impact evaluation. Clin Pract Epidemiol Ment Heal. (2022) 19:1–9. doi: 10.2174/18740179-v18-e221221-2022-11
112. Carabellese F, Parente L, La Tegola D, Rossetto I, Franconi F, Zanalda E, et al. The DUNDRUM ToolKit, Italian version and its potenzial use in the italian forensic treatment model. Rass Ital di Criminol. (2022) 16:271–82. doi: 10.7347/RIC-042022-p271
113. Pelizza L, Pupo S. Mental health interventions in Italian prisons: are we ready for a new model? Suggestions from the Parma experience. Riv Psichiatr. (2024) 59:35–42. doi: 10.1708/4205.41947
114. Fovet T, Thomas P. Forensic care in France. Eur Psychiatry. (2017) 41:S61–1. doi: 10.1016/j.eurpsy.2017.01.050
115. Fovet T, Amad A, Horn M, Thomas P, Chan-Chee C. Utilization of hospital-level mental health care services for inmates in France: A transversal study. Psychiatr Serv. (2020) 71:824–8. doi: 10.1176/appi.ps.201900497
116. de Labrouhe D, Plancke L, Amad A, Charrel C-L, Touitou D, Bodon-Bruzel M, et al. [Hospitalization in French forensic units: Results of a patient satisfaction survey]. Rev Epidemiol Sante Publique. (2017) 65:285–94. doi: 10.1016/j.respe.2017.03.129
117. Eyraud B, Velpry L, Doron CO, Lancelevée C, Litzler A, Protais C, et al. The creation of the UHSA: A new regulation of detention? Deviance Soc. (2015) 39:429–53. doi: 10.3917/ds.394.0429
118. Contrast C. La création des UHSA: une nouvelle régulation de l’enfermement? Déviance Société. (2015) 39:429–53. doi: 10.3917/ds.394.0429
119. Swartz MS, Swanson JW, Wagner HR, Burns BJ, Hiday VA. Effects of involuntary outpatient commitment and depot antipsychotics on treatment adherence in persons with severe mental illness. J Nerv Ment Dis. (2001) 189:583–92. doi: 10.1097/00005053-200109000-00003
120. Khan AY, Salaria S, Ovais M, Ide GD. Depot antipsychotics: Where do we stand? Ann Clin Psychiatry Off J Am Acad Clin Psychiatr. (2016) 28:289–98.
121. Najarian D, Turkoz I, Knight RK, Galderisi S, Lamaison HF, Zalitacz P, et al. Long-term efficacy and safety of paliperidone 6-month formulation: an open-label 2-year extension of a 1-year double-blind study in adult participants with schizophrenia. Int J Neuropsychopharmacol. (2023) 26:537–44. doi: 10.1093/ijnp/pyad028
122. Milz R, Benson C, Knight K, Antunes J, Najarian D, Lopez Rengel PM, et al. The effect of longer dosing intervals for long-acting injectable antipsychotics on outcomes in schizophrenia. Neuropsychiatr Dis Treat. (2023) 19:531–45. doi: 10.2147/NDT.S395383
123. Tomlin J, Lega I, Braun P, Kennedy HG, Herrando VT, Barroso R, et al. Forensic mental health in Europe: some key figures. Soc Psychiatry Psychiatr Epidemiol. (2021) 56:109–17. doi: 10.1007/s00127-020-01909-6
124. WHO Regional Office for Europe. Status report on prison health in the WHO European Region(2023). Available online at: https://www.who.int/europe/publications/i/item/9789289058674 (Accessed January 30, 2024).
Keywords: mental healthcare models, prisons, mental healthcare resources, serious mental illness, mental healthcare provision
Citation: Calcedo-Barba A, Antón Basanta J, Paz Ruiz S, Muro Alvarez A, Elizagárate Zabala E, Estévez Closas V, López López A and Barrios Flores LF (2024) Indifferent minds, broken system: a critical examination of mental health care provision for Spain’s incarcerated population with serious mental illnesses. Front. Psychiatry 15:1340155. doi: 10.3389/fpsyt.2024.1340155
Received: 17 November 2023; Accepted: 25 July 2024;
Published: 21 August 2024.
Edited by:
Birgit Angela Völlm, University of Rostock, GermanyReviewed by:
Peter Bartlett, University of Nottingham, United KingdomLuis Gutiérrez-Rojas, University of Granada, Spain
Miguel Hernandez Viadel, University of Valencia, Spain
Copyright © 2024 Calcedo-Barba, Antón Basanta, Paz Ruiz, Muro Alvarez, Elizagárate Zabala, Estévez Closas, López López and Barrios Flores. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Alfredo Calcedo-Barba, YWxmcmVkb0BhbGZyZWRvY2FsY2Vkby5uZXQ=
†These authors contributed equally to this work and share first authorship