
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
BRIEF RESEARCH REPORT article
Front. Psychiatry , 04 July 2024
Sec. Computational Psychiatry
Volume 15 - 2024 | https://doi.org/10.3389/fpsyt.2024.1330716
This article is part of the Research Topic Psychometrics in Psychiatry 2022: Computational Psychiatry View all 4 articles
 Kornél Vajsz1,2*
Kornél Vajsz1,2* Laura R. Paulina1
Laura R. Paulina1 Salvador Trejo3
Salvador Trejo3 Adrián A. Andaverde-Vega4
Adrián A. Andaverde-Vega4 James M. Swanson5
James M. Swanson5 Mónika Miklósi1,2,6
Mónika Miklósi1,2,6The Strengths and Weaknesses of ADHD Symptoms and Normal Behaviour Scale (SWAN) measures the full spectrum of attention and activity symptoms, not just the negative end of the distribution. Previous studies revealed strong psychometric properties of the parent and teacher report versions; however, there is little research on the new self-report form of the SWAN. Therefore, our research aimed to explore the psychometric characteristics of the SWAN self-report. A non-clinical sample of young women (N = 664, mean age: 20.01 years, SD: 3.08 years) completed the SWAN self-report, the Strengths and Difficulties Questionnaire (SDQ) and the Mental Health Continuum Short Form (MHC-SF). We tested several models using confirmatory factor analyses to assess the factorial validity of the SWAN self-report. Distributional characteristics, convergent, and predictive validity were assessed. A bifactor model with a general factor and a specific inattention factor (bifactor-1) provided the best fit in our data (CFI = 0.977, TLI/NFI = 0.972, RMSEA = 0.053 [90% CI: 0.047 – 0.059], SRMR = 0.061, ω = 0.90). The reliability of the general ADHD factor was good (ωh = 0.87), and the specific inattention factor was acceptable (ωh = 0.73). The distribution of the SWAN self-report scores did not differ from the normal distribution. A strong correlation between the SWAN and the SDQ Hyperactivity subscale was found. The analyses revealed good predictive validity. Our results suggest that the SWAN self-report is a valuable tool for assessing symptoms of ADHD in adolescents and young adults.
Attention-deficit/hyperactivity disorder (ADHD) is a neurodevelopmental disorder characterized by developmentally inappropriate symptoms of inattention, hyperactivity and impulsivity that lead to impairment in at least two domains of functioning (1). According to a recent meta-analysis (2), the prevalence of ADHD is 7.6% in children and 5.6% in adolescents. In adults, it was found to be 2.6% (3), with a risk as high as 70–75% for coexisting psychiatric disorders (4, 5), including mood and anxiety disorders, disruptive disorders, bipolar disorder, substance use, behavioural addictions, insomnia, and personality disorders (6–13). Though many environmental and genetic factors with small effects have already been identified, there are no definitive causal factors that can reliably predict ADHD (14–17). In their highly important work, Kapteyn and van Uven (18) proved that a high number of independent factors of small effects tend to cause normal distributions, whereas processes with few factors and large effects tend to cause more skewed distributions. In line with this, ADHD-related traits follow a continuous, normal distribution in the population (19, 20).
In children, the diagnosis is mainly based on parent and teacher ratings, as well as on the direct observation of the symptoms (21). The importance of self-reporting increases with age, however. Though parent-report predicts outcomes better than self-reports even in adolescents and college students (22, 23), by adulthood, self-report is the most valuable source of information in the diagnostic process (24). It should be noted that symptom list-based approaches are the predominant means of assessing adult ADHD through rating scales, such as the Adult AD/HD Rating Scale [AARS (25)], the Barkley Adult ADHD Rating Scale–IV [BAARS-IV (26)], the Conners’ Adult ADHD Rating Scale [CAARS (27)], and the Adult ADHD Self-Report Scale [ASRS (28)]. Although these measures have strong psychometric properties, they indicate normative functioning by the absence of symptoms, resulting in a skewed and truncated distribution of scores. The lack of fit to normal distribution causes difficulty in establishing the clinical cutoffs of symptom scales, which can lead to lower specificity and type 1 errors (29). Therefore, it is important to take the strengths in attention, activity, and impulse control into consideration as well to see the full picture (19, 20).
The Strengths and Weaknesses of ADHD Symptoms and Normal Behaviour Scale [SWAN (20)] was shown to satisfy this requirement. SWAN is an 18-item questionnaire with a 7-point Likert scale that examines traits related to ADHD symptoms. The scale is anchored to average behaviour, namely that –3 means the respondent observed far below average capability in the trait measured, 0 means average behaviour, and +3 means far above average ability that can be a strength in self-control or executive functioning (i.e., lower scores indicate greater difficulties). Consequently, the SWAN scores were shown to follow a normal distribution (20, 30–32), and, therefore, it was found to have just as good sensitivity but better specificity than other ADHD symptom scales (33). Originally, parent-, and teacher-report versions have been developed (20), and translated into several languages (30, 31, 33–37). More recently, Blume and colleagues (38) created a self-report version the German language, extending the SWAN family.
The Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition [DSM-5 (1)] conceptualizes ADHD with two primary dimensions; consequently, predominantly inattentive, predominantly hyperactive/impulsive, and combined presentations are described. However, it has been debated whether the two-factor structure best represents ADHD (39). Factor-analytic studies have reported the best fit for different measurement models, with mixed support for one-, two-, and three-factor models or more complex hierarchical or bifactor models. In terms of fit indices, most evidence seems to support the bifactor models (40–43). In bifactor models, a latent general ADHD construct may explain the diagnostic stability of ADHD, while the specific factors are in line with the clinical observation that symptom presentation may change over time (44). Converging results revealed a strong and reliable general ADHD factor in different age groups and across different measures (40). A specific inattention factor which acquired sufficient specificity and stability for interpretation beyond the general ADHD factor has also been supported by several studies, especially in clinical samples (42). However, a specific hyperactivity/impulsivity factor (bifactor-2 model) or separate hyperactivity and impulsivity factors (bifactor-3 models) were shown to explain only a small amount of additional variance and had low reliabilities and low construct replicabilities. It is important to note that, bifactor-3 models performed better when talks excessively (modulating verbal activity) was treated as a part of impulsivity rather than hyperactivity (41, 43). In line with this several authors argued that the hyperactivity and impulsivity symptoms listed in the DSM-5 (1) could be better grouped into motor and verbal hyperactivity/impulsivity (45). The weakness of specific factors led some researchers to view bifactor models as not interpretable, clinically irrelevant, or even statistical artefacts (46, 47). In that way, they suggested the use of either a total score of the scales (the general ADHD factor only) (46) or the acceptance of more traditional non-hierarchical two- or three-factor models (47) or hierarchical models (39), despite of their inferiority to bifactor models in term of fit indices. However, the hierarchical models had negative factor loadings and low internal consistencies which is a known issue for models with a general factor (48). The usage of bifactor-1 model was found to be a viable alternative by previous ADHD researchers (49, 50).
The factor structure of the SWAN has also been explored. In studies on the parent- and teacher-report versions, exploratory factor analysis resulted in a two-factor structure (inattention and hyperactivity/impulsivity) in different samples (20, 31). In studies using confirmatory factor analysis (31, 35, 51, 52), bifactor models were reported to have a better fit than non-hierarchical models; however, similar to studies with other measures, the results suggested a strong and reliable general ADHD factor but mostly weak or unreliable specific factors. A single study under peer review (38) reported similar results for the new self-report version of the SWAN. Blume et al. found an inferior fit of a non-hierarchical two-factor model in comparison to a bifactor model with a general and two specific factors; however, five of nine item-loadings of the specific hyperactivity/impulsivity factor were nonsignificant.
To gain more information about the self-report version of the SWAN, our study aimed to examine the psychometric properties of the Hungarian version in a sample of adolescents and young adults.
The Institutional Research Ethics Committee of the Psychological Institute Eötvös Loránd University approved the study (Nr. 2022/344). There was a 24-hour-long campaign through Mélylevegő Projekt (Deep Breath Project), a Hungarian psychoeducational social media page. Mélylevegő Projekt was founded during the 2020 COVID-19 lockdown by graduate psychology students as a platform connect and provide mental health related information for teens and young adults. Participants gave their informed consent before completing the online questionnaire.
In total, 2597 participants agreed to fill out the questionnaire, of whom 717 completed it. Completers’ gender distribution was highly skewed (N = 664 [92.6%] women, N = 47 [6.6%] men, N = 6 [0.8%] other), therefore, data from 664 women (age range: 14 − 25 years, mean age: 20.01 years, SD: 3.08) were analyzed (Table 1).
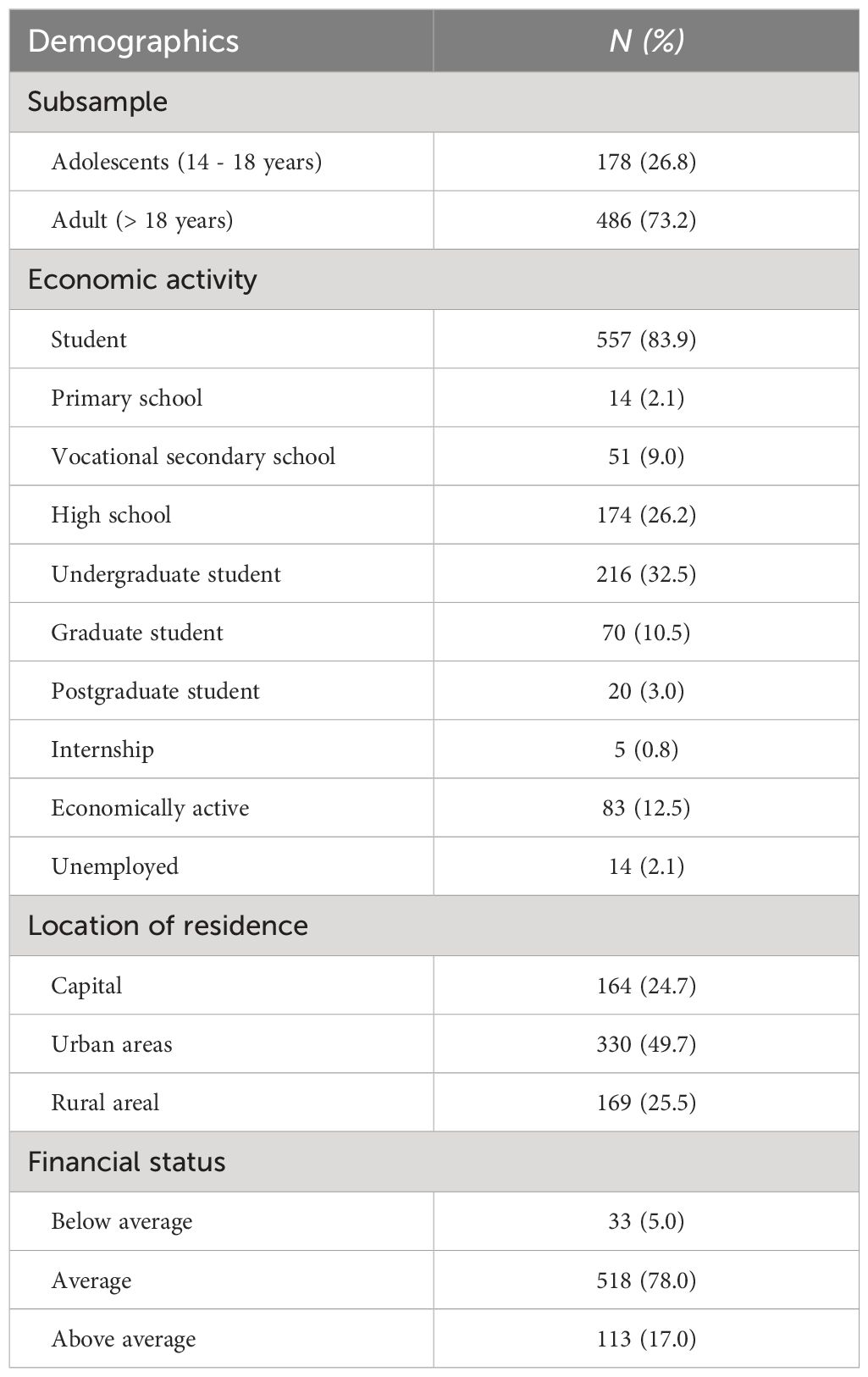
Table 1 Demographic characteristics (N = 664).
The self-report version of the SWAN (38) was used to assess ADHD symptoms. Blume et al. (38) reported good internal reliabilities for the German version (α = 0.85 – 0.90). Up to now, only the parent and teacher versions of the SWAN have been validated in the Hungarian language showing good internal consistencies (α = 0.87 – 0.93) and convergent validity with the Hyperactivity subscale of the Strengths and Difficulties Questionnaire [SDQ (53)] (r = 0.67 - 0.74) (30). The Hungarian version of the SWAN self-report was created by Paulina et al. (54). In their pilot study, they reported good internal reliability (α = 0.89) for the total score, but the factorial validity has not been evaluated yet.
The SDQ (53) assesses emotional and behavioral problems with four problem scales (Emotional problems, Conduct problems, Hyperactivity, Peer problems) and prosocial skills. The SDQ Hyperactivity subscale measures hyperactivity with two items (SDQ#2, SDQ#10), but includes an impulsivity item (SDQ#20) and two inattention items (SDQ#15, SDQ#25) as well. Higher scores indicate more emotional and behavioral problems. Internal reliabilities of the self-report version were αSDQ-ES = 0.66, αSDQ-CP = 0.60, αSDQ-H = 0.67, αSDQ-PP = 0.41, αSDQ-P = 0.66 (53). Psychometric properties of the Hungarian version have been reported by Turi et al. (55). In our sample, the Hyperactivity and Emotional problems subscales had acceptable reliability (αSDQ-H = 0.76 and αSDQ-ES = 0.68), but the Conduct problems and Peer problems subscales had poor reliabilities (αSDQ-CP = 0.47, αSDQ-PP = 0.45), therefore, we used only the Hyperactivity and Emotional problems subscales for further analyses.
The Mental Health Continuum - Short Form [MHC-SF (56)] measures emotional, psychological and social well-being with 14 Likert-type items measuring the frequency of indicators of positive mental health (from 1 = never to 6 = every day). Both the original (αMHC = 0.74) and the Hungarian versions (αMHC = 0.89) showed good internal consistencies (56, 57). In the present sample, the internal reliability was αMHC = 0.85.
Confirmatory factor analyses were conducted to assess the factorial validity of the SWAN self-report. Because of the significance of the Shapiro-Wilk Test for Multivariate Normality and the Mardia’s coefficients for multivariate skewness and kurtosis, we used the Diagonally Weighted Least Squares (DWLS) estimator (58). We compared several models: a non-hierarchical two-factor model and a bifactor model with a general ADHD factor and two specific factors for inattention and hyperactivity/impulsivity (bifactor-2), a bifactor model with a general factor and a specific inattention factor (bifactor-1), and two bifactor models with a general and three specific factors: inattention, hyperactivity + “Modulating verbal activity”, and impulsivity (bifactor-3-IA/H[MVA]/I), and inattention, hyperactivity, and hyperactivity+ “Modulating verbal activity” (bifactor-3-IA/H/I[MVA]). The analyses were conducted using the lavaan (version 0.6–15) package of JASP version 0.17.1 and R version 4.2.1. Factor scaling was assumed to be based on factor variances. Maximum likelihood estimators were used. Comparative Fit Indices (CFI) and Tucker-Lewis Indices/Normed Fit Indices (TLI/NFI) were calculated with a minimum acceptable threshold of 0.900 (59, 60). Root Mean Square Error of Approximation (RMSEA) was calculated with a maximum acceptable threshold of 0.07 (61). Standardized Root Mean Square Residual (SRMR) was calculated with a maximum acceptable threshold of 0.08 (62). Composite reliabilities were calculated with ωh > 0.50 as the criteria of minimal acceptability and ωh > 0.75 as the preferred reliability index (63). Explained common variance was calculated for the bifactor models to compare the factor loadings of the general factor with that of the one-factor model (64). Hancock’s H coefficient was calculated for each factor to measure how well each latent variable is represented by its group of items. The criterium of stability was H > 0.70, which means the factor is unlikely to fluctuate across samples (47, 65).
Normality was evaluated by the Shapiro-Wilk statistics, skewness, and kurtosis. Convergent validity was evaluated by computing the Person’s correlational coefficient of the SWAN and the SDQ Hyperactivity subscale. Predictive validity was examined by means of linear regression analyses with the MHC-SF and the SDQ Emotional problems subscale as dependent variables.
First, the non-hierarchical two-factor model was evaluated. The usage of Chi-square goodness of fit was largely eschewed due to the large sample size (66). Composite reliability of the two-factor model was ωh = 0.85 for inattention, ωh = 0.87 for hyperactivity/impulsivity, and ω = 0.92 for the total model. Construct replicability was good for both inattention (Hancock’s H-index = 0.86) and hyperactivity/impulsivity (Hancock’s H-index = 0.87) factors. The model showed a good fit to our data (CFI = 0.972, TLI/NFI = 0.968, RMSEA = 0.057 [90% CI: 0.051 – 0.063], SRMR = 0.066). All item loadings were significant (Table 2A).
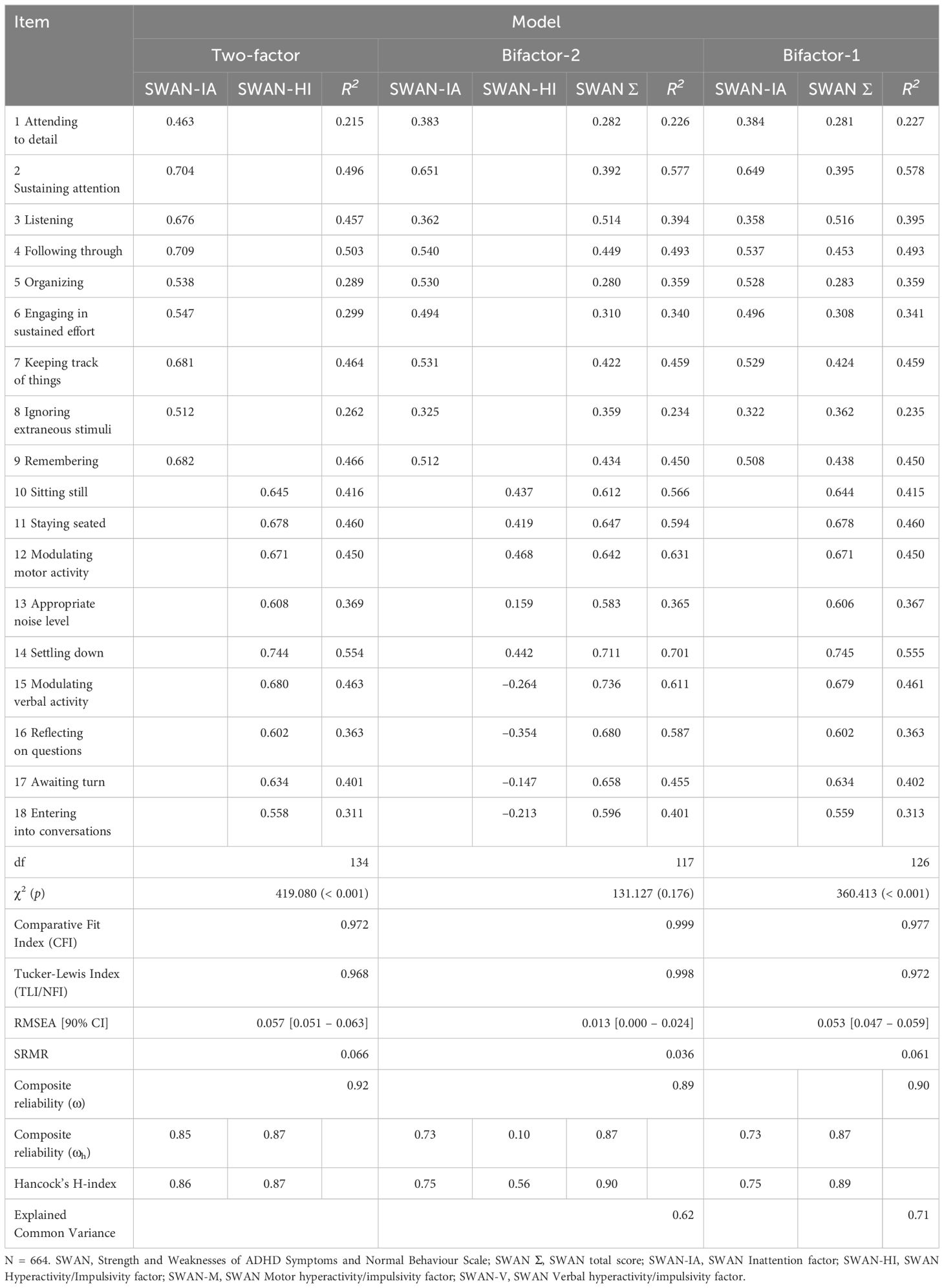
Table 2A Factor loadings and fit indices of the two-factor, bifactor-2, and bifactor-1 models.
The bifactor-2 model showed a very good fit (CFI = 0.999, TLI/NFI = 0.998, RMSEA = 0.013 [90% CI: 0.000 – 0.024], SRMR = 0.036), and the SRMR has shown a considerable decrease compared to the two-factor model (ΔSRMR = 0.030). All item loadings were statistically significant. Items 15–18 demonstrated significant, negative loadings on the hyperactivity/impulsivity factor. The overall reliability of the bifactor-2 model was good (ω = 0.89). The reliability of the general ADHD factor was also good (ωh = 0.87), the specific inattention factor was minimally acceptable (ωh = 0.73), and the reliability of the specific hyperactivity/impulsivity factor was poor (ωh = 0.10). The explained common variance of the model was ECV = 0.62, suggesting that the factor loadings of the general ADHD factor were slightly similar to those that might be obtained with the one-factor model. Analysis of construct replicability indicated that the general ADHD factor (Hancock’s H-index = 0.90) and the specific inattention factor (Hancock’s H-index = 0.76) were stable, but the specific hyperactivity/impulsivity factor was not (Hancock’s H-index = 0.56).
The bifactor-1 model showed a good fit (CFI = 0.977, TLI/NFI = 0.972, RMSEA = 0.053 [90% CI: 0.047 – 0.059], SRMR = 0.061). All factor loadings were significant, ranging from 0.28 to 0.75. The factor loadings of six of nine inattention-symptom items were substantially larger than their loadings on the general factor (Δb > 0.1). The overall reliability of the bifactor-1 model was good (ω = 0.90). The reliability of the general ADHD factor was also good (ωh = 0.87), and the specific inattention factor was minimally acceptable (ωh = 0.73). The explained common variance was 0.71, suggesting that the general ADHD factor explained more than two-thirds of the common variance. Analysis of construct replicability indicated that both the general ADHD factor (Hancock’s H-index = 0.89) and the inattention factor (Hancock’s H-index = 0.75) were stable.
Both bifactor-3 models (Table 2B) showed very good fit [bifactor-3-IA/H[MVA]/I: CFI = 0.995, TLI/NFI = 0.994, RMSEA = 0.025 [90% CI: 0.015 – 0.033], SRMR = 0.041; bifactor-3-IA/H/I[MVA]: CFI = 0.998, TLI/NFI = 0.998, RMSEA = 0.015 [90% CI: 0.000 – 0.025], SRMR = 0.037)], with the bifactor-3-IA/H/I[MVA] performing slightly better. “Modulating verbal activity” had a negative loading on the Hyperactivity factor (bifactor-3-IA/H[MVA]/I model) but loaded significantly and positively on the Impulsivity factor (bifactor-3-IA/H/I[MVA] model). In both models, the overall reliability of the model was good (ω = 0.91 for both); the reliability of the general ADHD factor was also good (ωh = 0.86 for both), and the specific inattention factor was minimally acceptable (ωh = 0.70 and 0.68, respectively). However, in both bifactor-3 models, the reliabilities of the hyperactivity and impulsivity factors were poor (< 0.70). The explained common variances of the models were 0.58 and 0.56, respectively, suggesting the general ADHD factor explained about half of the common variance in the bifactor-3 models. Construct replicability indicated that, both the general ADHD factor (Hancock’s H-index = 0.88 and 0.87, respectively) and the inattention factor (Hancock’s H-index = 0.73 and 0.71, respectively) were stable in both bifactor-3 models. The hyperactivity factor was unstable in both models (Hancock’s H-index = 0.65); however, the impulsivity factor did not show stability in both bifactor-3 models (Hancock’s H-index = 0.27 and 0.49, respectively).
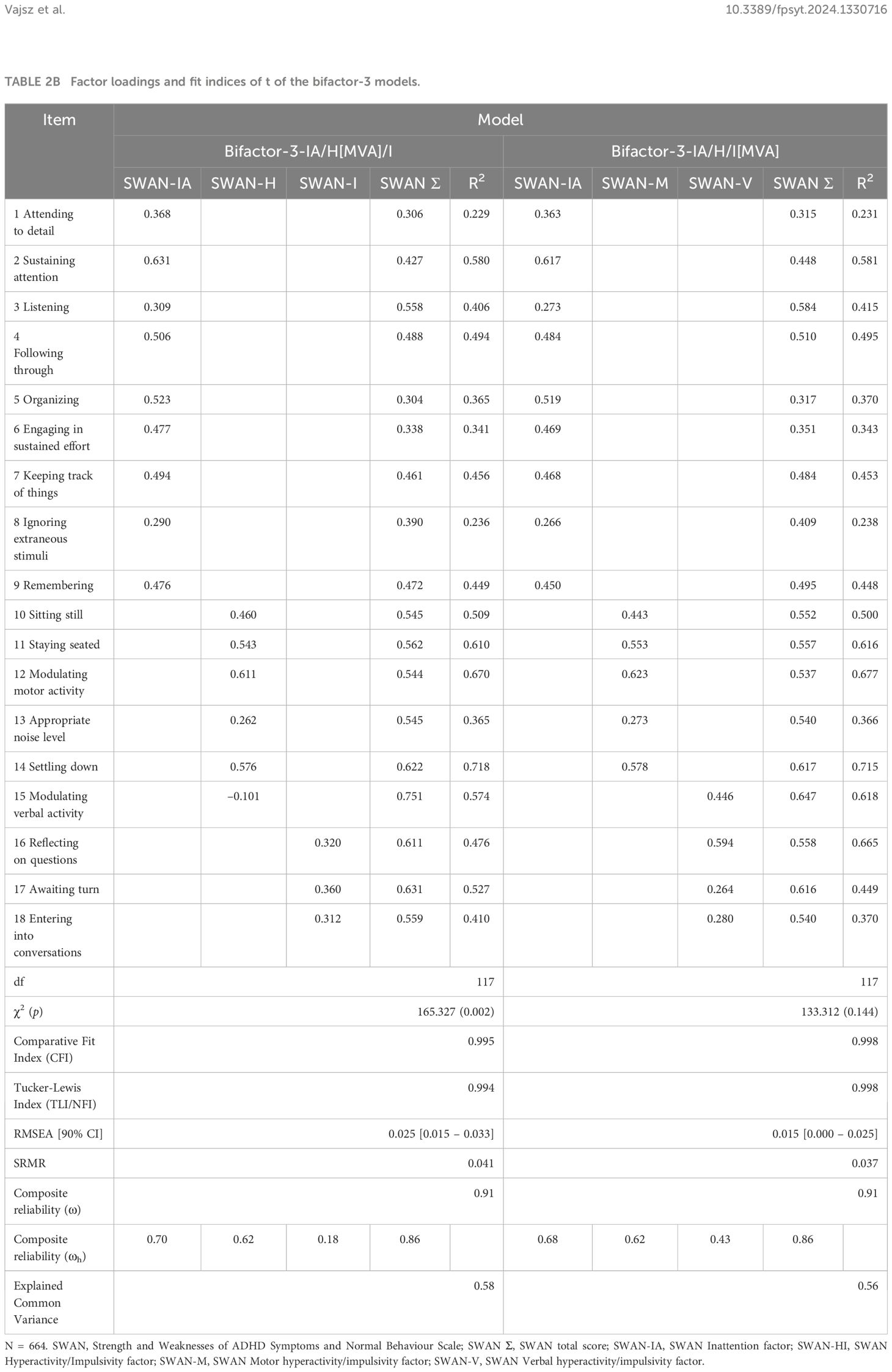
Table 2B Factor loadings and fit indices of t of the bifactor-3 models.
We compared the models by computing several Scaled Chi-Square Difference Tests. All bifactor models were proven to be significantly better than the two-factor model. However, the bifactor-2 (Δχ2(9) = 229.286, p < 0.05), and both the bifactor-3-IA/H[MVA]/I (Δχ2(9) = 195.086, p < 0.05) and bifactor-3-IA/H/I[MVA] models (Δχ2(9) = 227.101, p < 0.05) were significantly better than the bifactor-1 model.
Shapiro-Wilk statistics were non-significant for both adolescents (W = 0.994, p = 0.700) and young adults (W = 0.995, p = 0.137), indicating normality. The skewness of the SWAN scores in the adolescent and young adult samples was found to be 0.03 and 0.02, respectively, indicating a close fit to symmetrical distribution. The kurtosis of SWAN in the adolescent and young adult samples was found to be –0.39 and –0.44, respectively.
Descriptive statistics and bivariate relationships of study variables are shown in Table 3. The SWAN subscales showed significant negative correlations of large effect size with the SDQ Hyperactivity subscale indicating good convergent validity (Table 3).
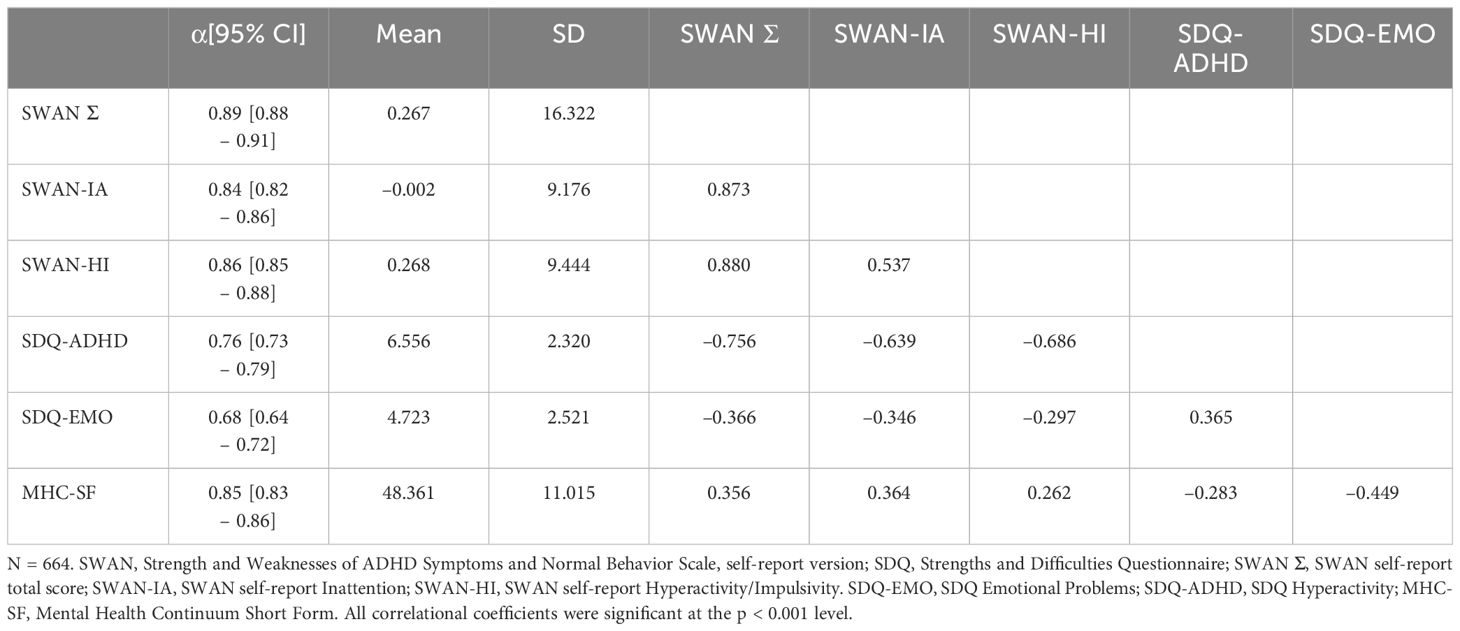
Table 3 Descriptive statistics, reliabilities and intercorrelations of study variables (Pearson’s correlational coefficients).
In a linear regression model with MHC-SF as the dependent variable and the total score of the SWAN self-report scale as an independent variable, the analysis resulted in a significant model (adjusted R2 = 0.125, F(1,663) = 96.125, p < 0.001). The SWAN was a significant predictor (β = 0.356, p < 0.001), explaining 12.5% of the variance of the dependent variable. When choosing the SDQ Hyperactivity subscale as the independent variable, the regression model was significant (adjusted R2 = 0.079, F(1,662) = 57.486, p < 0.001). The SDQ Hyperactivity was a significant predictor (β = -0.283, p < 0.001), explaining 7.9% of the variance of the dependent variable.
The next model, with SDQ Emotional problems as dependent and the SWAN as the independent variable, was significant (adjusted R2 = 0.133, F(1,662) = 102.694, p < 0.001). The SWAN was a significant predictor (β = –0.366, p < 0.001). Finally, the regression analysis with SDQ Emotional problems as dependent and the SDQ Hyperactivity scale as an independent variable resulted in a significant model (adjusted R2 = 0.132, F(1,662) = 101.770, p < 0.001). The SDQ Hyperactivity was a significant predictor (β = 0.365, p < 0.001).
There is a solid theoretical foundation for the relevance of measuring the full spectrum of ADHD symptoms, not just the negative end of the distribution (19, 20, 32). Also, several empirical studies using parent or teacher-report versions of the SWAN scale have demonstrated the merits of this approach [e.g (30, 67). (31, 34, 33) (35–37)]. Up to now, there was no self-report instrument available that would measure both strengths and weaknesses in attention, activity, and impulse control. Blume and colleagues (38) have filled this gap by developing a self-report version of the SWAN. Since they reported promisingly good psychometric characteristics for the German version of the SWAN self-report, it was worthwhile to conduct further research with the Hungarian version. Therefore, our research aimed to explore the factor structure, and distributional characteristics of the SWAN self-report, and to assess its convergent validity with the SDQ Hyperactivity subscale. Furthermore, we assessed its predictive validity in linear regression models by analyzing how well it can explain the variance in mental well-being and emotional problems.
Though all models tested showed acceptable fit, the bifactor models were superior to the non-hierarchical two-factor model in multiple fit indices: they had higher CFI and NFI/TLI and lower 90%CI for the RMSEA and SRMR. However, though the bifactor-2 and bifactor-3 models have shown a better fit than the bifactor-1, neither has shown an acceptable composite reliability nor Hancock’s H-index for each of their factors. The specific hyperactivity/impulsivity factor of the bifactor-2 model was shown to have poor composite reliability of ωh = 0.10. The items of the specific factor thus share 1% in common variance, the rest being accountable for measurement error. The bifactor-3 models were also shown to have poor composite reliabilities. Bifactor-3-IA/H[MVA]/I’s specific impulsivity factor was ωh = 0.18, having its items share 3.2% in common variance. Bifactor-3-IA/H/I[MVA]’s specific verbal hyperactivity/impulsivity factor was ωh = 0.43 having its items share 18.5% in common variance. The model with the best fit to show good composite reliability was the bifactor-1 model.
When evaluating the different factors, we concluded that both the general ADHD factor and the specific inattention factor had acceptable composite replicability and stability in the bifactor models. Our results suggested that more than two-thirds of the variance was explained by a single common source, i.e., a general ADHD factor, and there was also a substantial proportion of unique variance associated with the inattention factor. However, after partitioning out the variability explained by the general factor, there was little variance remaining that could have been attributed to the (joint or separated) specific hyperactivity and impulsivity factors. The comparison of the bifactor-3 models revealed that “modulating verbal activity” fitted better to the impulsivity than the hyperactivity factor, as suggested in previous research (41).
These findings converge with the results of previous studies exploring the structure of ADHD symptoms in different age groups and across different measures (40, 52, 68) and are in line with the findings of the single study on the SWAN self-report (38). On the other hand, diverging interpretations of similar findings have been formulated by different researchers. Some concluded that the bifactor models support the unidimensionality of ADHD symptoms and suggested using the total score (46). In contrast, Park and colleagues (47) recalled research findings showing different associations of attention deficit and hyperactivity/impulsivity factors with comorbid conditions, cognitive variables, and different domains of functional impairment (69), underlining the importance of different ADHD domains. They have argued that bifactor models only perform better because of their complexity, and in this way, they can be considered statistical artefacts and are not clinically useful. Our results support the notion that the only use of a general ADHD factor would lead to missing important information about the heterogeneity of the phenomenon; the inclusion of a separate inattention factor in the model is at least warranted. On the other hand, similarly to previous findings, our analysis found the hyperactivity and impulsivity factors to be problematic.
On one hand, these results may be related to the questionable validity or at least the low prevalence of predominantly hyperactive/impulsive presentation of ADHD, especially in adolescents and adults when hyperactivity typically decreases (70). For example, in a large sample of adults with ADHD, the prevalence of a clinical diagnosis of ADHD with hyperactive/impulsive presentation was very rare (3%), and this group had ratings of inattention comparable to the group with a clinical diagnosis of ADHD inattentive presentation (71). Furthermore, latent class analysis did not reveal a group with predominantly hyperactivity and impulsivity in children and adolescents aged between 6 and 18 years old (72). These results suggest that hyperactivity/impulsivity symptoms are accompanied by inattention symptoms in the vast majority of the cases, in that way, in factor-analytic studies they would be captured by the general ADHD factor.
On the other hand, DSM-based rating scales follow a relatively simplistic conceptualization of impulsivity as a single domain, however, impulsivity has been defined as a multidimensional construct in previous research (73, 74). Furthermore, all but one symptom of impulsivity in the DSM-5 symptom list (75) is specifically related to the verbal modality, while the assessment of motor impulsivity is very limited. These shortcomings may prevent the definition of an interpretable impulsivity factor in studies using these rating scales.
In line with previous research using different versions of the SWAN (30, 38), we found that the distribution of the SWAN self-report scores did not differ significantly from the normal distribution. Our analysis also confirmed the good convergent validity of the SWAN self-report by its very strong correlation with the SDQ Hyperactivity subscale. The correlation was even higher than the correlation of SWAN self-report with the Conners’ Adult ADHD Rating Scale (38) and that of the parent-report versions of the SWAN and the SDQ Hyperactivity subscale (34) in previous research.
Both measures explained a significant proportion of variance in emotional problems and mental health. In the case of the MHC-SF, the predictive power of the SWAN was better than that of the SDQ Hyperactivity. In previous research using the parent-report version, the association of the SWAN and SDQ Emotional problems was somewhat lower than in our study (34), which may be due to the different informants used.
The results can be viewed considering the limitations of the study. The cross-sectional design does not allow us to explore causality. Self-reports of ADHD symptoms and mental health may be biased by social desirability, insight, and cognitive abilities. Our sample consisted solely of women which may be related to the data collection method; young women may be more interested in mental health topics covered by the Mélylevegő Project website than men. Therefore, our results cannot be generalized to the population, future research should address these psychometric properties in more diverse demographic groups. Gender differences have been reported in symptom presentation, prevalence, comorbid profile, and social perception of ADHD symptoms (76, 77). Symptoms of inattention are more likely to be present than hyperactive symptoms in women, sometimes leading to delayed referral and diagnosis (77, 78). However, factor analytic studies reported gender invariance in adolescent (40) and adult (35) samples, suggesting that gender differences might not have a substantial influence on the results. On the other hand, cultural differences have been reported in the structure of ADHD symptoms; more research is needed in different cultural contexts (79).
Taken together, our results suggest that the SWAN self-report is a valuable tool for assessing symptoms of ADHD in adolescents and young adults. It has comparably good psychometric properties to measures in the SWAN family.
The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number(s) can be found below: https://osf.io/frvsw/?view_only=b9e81e7a8d824881b32070984b2a0ae6.
The Institutional Research Ethics Committee of the Psychological Institute Eötvös Loránd University approved the study (Nr. 2022/344). The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants’ legal guardians/next of kin.
KV: Conceptualization, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Software, Visualization, Writing – original draft, Writing – review & editing. LP: Conceptualization, Methodology, Writing – review & editing. ST: Methodology, Writing – review & editing, Supervision. AA-V: Methodology, Supervision, Writing – review & editing. JS: Methodology, Supervision, Writing – review & editing. MM: Methodology, Supervision, Writing – review & editing, Conceptualization, Formal analysis, Writing – original draft.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This work was supported by the National Research, Development, and Innovation Office (Nr. ÚNKP-22–2-I-ELTE-854).
The authors thank YouthInMind for providing us the license to use the online version of the SDQ (license number 101833). The authors thank Mélylevegő Projekt (Deep Breath Project) for their help in data collection.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2024.1330716/full#supplementary-material
1. APA. Diagnostic and Statistical Manual of Mental Disorders (2023). Available online at: https://www.appi.org/dsm-5-tr.
2. Salari N, Ghasemi H, Abdoli N, Rahmani A, Shiri MH, Hashemian AH, et al. The global prevalence of ADHD in children and adolescents: a systematic review and meta-analysis. Ital J Pediatr. (2023) 49:48. doi: 10.1186/s13052-023-01456-1
3. Song P, Zha M, Yang Q, Zhang Y, Li X, Rudan I. The prevalence of adult attention-deficit hyperactivity disorder: A global systematic review and meta-analysis. J Glob Health. (2022) 11:04009. doi: 10.7189/jogh.11.04009
4. Katzman MA, Bilkey TS, Chokka PR, Fallu A, Klassen LJ. Adult ADHD and comorbid disorders: clinical implications of a dimensional approach. BMC Psychiatry. (2017) 17:302. doi: 10.1186/s12888-017-1463-3
5. Biederman J. Impact of comorbidity in adults with attention-deficit/hyperactivity disorder. J Clin Psychiatry. (2004). 65(Suppl 3):3–7.
6. McGough JJ, Smalley SL, McCracken JT, Yang M, Del’Homme M, Lynn DE, et al. Psychiatric comorbidity in adult attention deficit hyperactivity disorder: findings from multiplex families. Am J Psychiatry. (2005) 162:1621–7. doi: 10.1176/appi.ajp.162.9.1621
7. Matthies S, Philipsen A. Comorbidity of personality disorders and adult attention deficit hyperactivity disorder (ADHD)–review of recent findings. Curr Psychiatry Rep. (2016) 18:33. doi: 10.1007/s11920-016-0675-4
8. Schiweck C, Arteaga-Henriquez G, Aichholzer M, Thanarajah SE, Vargas-Cáceres S, Matura S, et al. Comorbidity of ADHD and adult bipolar disorder: A systematic review and meta-analysis. Neurosci Biobehav Rev. (2021) 124:100–23. doi: 10.1016/j.neubiorev.2021.01.017
9. van Emmerik-van Oortmerssen K, van de Glind G, van den Brink W, Smit F, Crunelle CL, Swets M, et al. Prevalence of attention-deficit hyperactivity disorder in substance use disorder patients: A meta-analysis and meta-regression analysis. Drug Alcohol Depend. (2012) 122:11–9. doi: 10.1016/j.drugalcdep.2011.12.007
10. El Archi S, Barrault S, Brunault P, Ribadier A, Varescon I. Co-occurrence of adult ADHD symptoms and problematic internet use and its links with impulsivity, emotion regulation, anxiety, and depression. Front Psychiatry. (2022) 13:792206. doi: 10.3389/fpsyt.2022.792206
11. Fadeuilhe C, Daigre C, Richarte V, Grau-López L, Palma-Álvarez RF, Corrales M, et al. Insomnia disorder in adult attention-deficit/hyperactivity disorder patients: clinical, comorbidity, and treatment correlates. Front Psychiatry. (2021) 12. doi: 10.3389/fpsyt.2021.663889
12. Nunez NA, Coombes BJ, Romo-Nava F, Bond DJ, Vande Voort J, Croarkin PE, et al. Clinical and genetic correlates of bipolar disorder with childhood-onset attention deficit disorder. Front Psychiatry. (2022) 13:884217. doi: 10.3389/fpsyt.2022.884217
13. Slobodin O, Crunelle CL. Mini review: socio-cultural influences on the link between ADHD and SUD. Front Public Health. (2019) 7:173. doi: 10.3389/fpubh.2019.00173
14. Núñez-Jaramillo L, Herrera-Solís A, Herrera-Morales WV. ADHD: reviewing the causes and evaluating solutions. J Pers Med. (2021) 11:166. doi: 10.3390/jpm11030166
15. Bonvicini C, Faraone SV, Scassellati C. Attention-deficit hyperactivity disorder in adults: A systematic review and meta-analysis of genetic, pharmacogenetic and biochemical studies. Mol Psychiatry. (2016) 21:872–84. doi: 10.1038/mp.2016.74
16. Li JJ, He Q. Polygenic scores for ADHD: A meta-analysis. Res Child Adolesc Psychopathol. (2021) 49:297–310. doi: 10.1007/s10802-021-00774-4
17. Nikolas MA, Burt SA. Genetic and environmental influences on ADHD symptom dimensions of inattention and hyperactivity: a meta-analysis. J Abnorm Psychol. (2010) 119:1. doi: 10.1037/a0018010
18. Kapteyn JC, van Uven MJ. Skew frequency curves in biology and statistics. 2nd paper. Groningen: Hoitsema Bros (1916). 69 p.
19. Coghill D, Sonuga-Barke EJS. Annual Research Review: Categories versus dimensions in the classification and conceptualisation of child and adolescent mental disorders – implications of recent empirical study. J Child Psychol Psychiatry. (2012) 53:469–89. doi: 10.1111/j.1469-7610.2011.02511.x
20. Swanson JM, Schuck S, Porter MM, Carlson C, Hartman CA, Sergeant JA, et al. Categorical and dimensional definitions and evaluations of symptoms of ADHD: history of the SNAP and the SWAN rating scales. Int J Educ Psychol Assess. (2012) 10:51–70.
21. Pelham WE, Fabiano GA, Massetti GM. Evidence-based assessment of attention deficit hyperactivity disorder in children and adolescents. J Clin Child Adolesc Psychol. (2005) 34:449–76. doi: 10.1207/s15374424jccp3403_5
22. Du Rietz E, Cheung CHM, McLoughlin G, Brandeis D, Banaschewski T, Asherson P, et al. Self-report of ADHD shows limited agreement with objective markers of persistence and remittance. J Psychiatr Res. (2016) 82:91–9. doi: 10.1016/j.jpsychires.2016.07.020
23. Dvorsky MR, Langberg JM, Molitor SJ, Bourchtein E. Clinical utility and predictive validity of parent and college student symptom ratings in predicting an ADHD diagnosis. J Clin Psychol. (2016) 72:401–18. doi: 10.1002/jclp.2016.72.issue-4
24. Zucker M, Morris MK, Ingram SM, Morris RD, Bakeman R. Concordance of self- and informant ratings of adults’ current and childhood attention-deficit/hyperactivity disorder symptoms. Psychol Assess. (2002) 14:379–89. doi: 10.1037//1040-3590.14.4.379
25. DuPaul GJ, Power TJ, Anastopoulos AD, Reid R. ADHD Rating Scale—IV: Checklists, norms, and clinical interpretation. New York, NY: Guilford press (1998).
27. Conners CK, Erhardt D, Sparrow EP. Conners’ adult ADHD rating scales (CAARS): technical manual. North Tonawanda, NY: Multi-Health Systems (1999).
28. Kessler RC, Adler LA, Gruber MJ, Sarawate CA, Spencer T, Van Brunt DL. Validity of the World Health Organization Adult ADHD Self-Report Scale (ASRS) Screener in a representative sample of health plan members. Int J Methods Psychiatr Res. (2007) 16:52–65. doi: 10.1002/mpr.208
29. Mulraney M, Arrondo G, Musullulu H, Iturmendi-Sabater I, Cortese S, Westwood SJ, et al. Systematic review and meta-analysis: screening tools for attention-deficit/hyperactivity disorder in children and adolescents. J Am Acad Child Adolesc Psychiatry. (2022) 61:982–96. doi: 10.1016/j.jaac.2021.11.031
30. Lakatos K, Birkás E, Tóth I, Gervai J. Gyermekkori viselkedési problémák felismerésének lehetőségei rövid kérdőívekkel II: A SWAN (Strength and Weakness of ADHD-symptoms and Normal-behavior) skála magyar változata a figyelemhiányos/hiperaktivitás zavar szűrésére. Psych Hung. (2010) 25:493–502.
31. Schulz-Zhecheva Y, Voelkle M, Beauducel A, Buch N, Fleischhaker C, Bender S, et al. ADHD traits in German school-aged children: validation of the German strengths and weaknesses of ADHS symptoms and normal behavior (SWAN-DE) scale. J Atten Disord. (2019) 23:553–62. doi: 10.1177/1087054716676365
32. Arnett AB, Pennington BF, Friend A, Willcutt EG, Byrne B, Samuelsson S, et al. The SWAN captures variance at the negative and positive ends of the ADHD symptom dimension. J Atten Disord. (2013) 17:152–62. doi: 10.1177/1087054711427399
33. Robaey P, Amre D, Schachar R, Simard L. French version of the strengths and weaknesses of ADHD symptoms and normal behaviors (SWAN-F) questionnaire. J Can Acad Child Adolesc Psychiatry. (2007) 16:80–9. doi: 10.1037/t77132-000
34. Lakes KD, Swanson JM, Riggs M. The reliability and validity of the English and Spanish strengths and weaknesses of ADHD and normal behavior rating scales in a preschool sample: continuum measures of hyperactivity and inattention. J Attention Dis. (2012) 16(6):510516. doi: 10.1177/1087054711413550
35. Trejo S, Andaverde-Vega AA, Villalobos-Gallegos L, Swanson JM, Salum GA. Factor structure, measurement invariance, and scoring practices of the strengths and weaknesses of ADHD–symptoms and normal behavior. Psychol Assess. (2022) 3(3):269279. doi: 10.1037/pas0001201
36. Hurtig T, Taanila A, Ebeling H, Miettunen J, Moilanen I. Attention and behavioural problems of Finnish adolescents may be related to the family environment. Eur Child Adolesc Psychiatry. (2005) 14:471–8. doi: 10.1007/s00787-005-0492-5
37. So CYC, Leung PWL, Hung SF. Treatment effectiveness of combined medication/behavioural treatment with Chinese ADHD children in routine practice. Behav Res Ther. (2008) 46:983–92. doi: 10.1016/j.brat.2008.06.007
38. Blume F, Buhr L, Kühnhausen J, Köpke R, Weber LA, Fallgatter AJ, et al. Validation of a self-report version of the German strengths and weaknesses of ADHD symptoms and normal behavior scale (SWAN-DE-SB). Assessment. (2020) 10731911241236699. doi: 10.31234/osf.io/x6bpd
39. Nichols JQVA, Shoulberg EK, Garner AA, Hoza B, Burt KB, Murray-Close D, et al. Exploration of the factor structure of ADHD in adolescence through self, parent, and teacher reports of symptomatology. J Abnorm Child Psychol. (2017) 45:625–41. doi: 10.1007/s10802-016-0183-3
40. Gomez R. DSM-IV ADHD symptoms self-ratings by adolescents: test of invariance across gender. J Atten Disord. (2013) 17:3–10. doi: 10.1177/1087054711403715
41. Gomez R, Liu L, Krueger R, Stavropoulos V, Downs J, Preece D, et al. Unraveling the optimum latent structure of attention-deficit/hyperactivity disorder: evidence supporting ICD and hiTOP frameworks. Front Psychiatry. (2021) 12:666326. doi: 10.3389/fpsyt.2021.666326
42. Arias VB, Ponce FP, Núñez Daniel E. Bifactor models of attention-deficit/hyperactivity disorder (ADHD): an evaluation of three necessary but underused psychometric indexes. Assessment. (2018) 25:885–97. doi: 10.1177/1073191116679260
43. Arildskov TW, Virring A, Lambek R, Carlsen AH, Sonuga-Barke EJS, Østergaard SD, et al. The factor structure of attention-deficit/hyperactivity disorder in schoolchildren. Res Dev Disabil. (2022) 125:104220. doi: 10.1016/j.ridd.2022.104220
44. Martel MM, von Eye A, Nigg JT. Revisiting the latent structure of ADHD: is there a ‘g’ factor? J Child Psychol Psychiatry. (2010) 51:905–14. doi: 10.1111/j.1469-7610.2010.02232.x
45. Stanton K, Forbes MK, Zimmerman M. Distinct dimensions defining the Adult ADHD Self-Report Scale: Implications for assessing inattentive and hyperactive/impulsive symptoms. Psychol Assess. (2018) 30:1549–59. doi: 10.1037/pas0000604
46. Morin AJ, Tran A, Caci H. Factorial validity of the ADHD Adult Symptom Rating Scale in a French community sample: Results from the ChiP-ARD Study. J Atten Disord. (2016) 20:530–41. doi: 10.1177/1087054713488825
47. Park J, Silveira M, Elliott M, Savalei V, Johnston C. Confirmatory factor analysis of the structure of adult ADHD symptoms. J Psychopathol Behav Assess. (2018) 40:573–85. doi: 10.1007/s10862-018-9698-y
48. Eid M, Geiser C, Koch T, Heene M. Anomalous results in G-factor models: Explanations and alternatives. Psychol Methods. (2017) 22:541. doi: 10.1037/met0000083
49. Burke JD, Johnston OG. The bifactor S-1 model: a psychometrically sounder alternative to test the structure of ADHD and ODD? J Abnorm Child Psychol. (2020) 48:911–5. doi: 10.1007/s10802-020-00645-4
50. Burns GL, Geiser C, Servera M, Becker SP, Beauchaine TP. Application of the bifactor S – 1 model to multisource ratings of ADHD/ODD symptoms: an appropriate bifactor model for symptom ratings. J Abnorm Child Psychol. (2020) 48:881–94. doi: 10.1007/s10802-019-00608-4
51. Normand S, Flora DB, Toplak ME, Tannock R. Evidence for a general ADHD factor from a longitudinal general school population study. J Abnorm Child Psychol. (2012) 40:555–67. doi: 10.1007/s10802-011-9584-5
52. Gomez R, Vance A, Stavropoulos V. Measurement invariance of maternal ratings of ADHD symptoms across clinic referred children’s with and without ADHD. Adv Dev Educ Psychol. (2019) 1:7–17. doi: 10.25082/ADEP.2019.01.002
53. Goodman R. Psychometric properties of the strengths and difficulties questionnaire. J Am Acad Child Adolesc Psychiatry. (2001) 40:1337–45. doi: 10.1097/00004583-200111000-00015
54. Paulina LR, Csejtei I, Miklosi M. [Attention deficit/hyperactivity symptoms, quality of sleep, and social media use in young adults during the COVID-19 epidemic]. Neuropsychopharmacol Hung. (2023) 25:70–81.
55. Turi E, Gervai J, Áspán N, Halász J. A Képességek és Nehézségek Kérdőív (SDQ-Magy) validálása serdülőkorú klinikai populációban = Validation of the Hungarian Strengths and Difficulties Questionnaire in an adolescent clinical population. Psychiatr Hung. (2013) 28:165–79.
56. Keyes CL. Mental illness and/or mental health? Investigating axioms of the complete state model of health. J Consult Clin Psychol. (2005) 73:539. doi: 10.1037/0022-006X.73.3.539
57. Reinhardt M, Horváth Z, Morgan A, Kökönyei G. Well-being profiles in adolescence: psychometric properties and latent profile analysis of the mental health continuum model – a methodological study. Health Qual Life Outcomes. (2020) 18:95. doi: 10.1186/s12955-020-01332-0
58. Muthén BO. Goodness of fit with categorical and other nonnormal variables. Newbury Park, CA: SAGE Focus Ed (1993) 154: 205–5.
59. Hair JF, Black WC, Babin BJ. Multivariate Data Analysis: A Global Perspective. New York, NY: Pearson Education (2010). 800 p.
60. Afthanorhan WMAW. A Handbook on SEM Zainudin Awang -Universiti Sultan Zainal Abidin ANALYZING THE SEM STRUCTURAL MODEL 4.1 STEPS INVOLVED IN PERFORMING THE STRUCTURAL EQUATION MODELING . Available online at: https://www.academia.edu/34981108/A_Handbook_on_SEM_Zainudin_Awang_Universiti_Sultan_Zainal_Abidin_ANALYZING_THE_SEM_STRUCTURAL_MODEL_4_1_STEPS_INVOLVED_IN_PERFORMING_THE_STRUCTURAL_EQUATION_MODELING_SEM.
61. Steiger JH. Understanding the limitations of global fit assessment in structural equation modeling. Pers Individ Differ. (2007) 42:893–8. doi: 10.1016/j.paid.2006.09.017
62. Hu L, Bentler PM. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct Equ Model Multidiscip J. (1999) 6:1–55. doi: 10.1080/10705519909540118
63. Reise SP, Bonifay WE, Haviland MG. Scoring and modeling psychological measures in the presence of multidimensionality. J Pers Assess. (2013) 95:129–40. doi: 10.1080/00223891.2012.725437
64. Rodriguez A, Reise SP, Haviland MG. Applying bifactor statistical indices in the evaluation of psychological measures. J Pers Assess. (2016) 98:223–37. doi: 10.1080/00223891.2015.1089249
65. Cudeck R, Jöreskog K, Jöreskog KG, Du Toit SHC, Sörbom D eds. Structural equation modeling: present and future ; a festschrift in honor of Karl Jöreskog. In: Rethinking construct reliability within latent variable systems. SSI, Scientific Software International, Lincolnwood, IL. 598 p. (Methodology in the social sciences).
66. Kyriazos TA. Applied psychometrics: sample size and sample power considerations in factor analysis (EFA, CFA) and SEM in general. Psychology. (2018) 9:2207–30. doi: 10.4236/psych.2018.98126
67. Swanson JM, Wigal T, Lakes K, Volkow ND. Attention Deficit Hyperactivity Disorder: Defining A Spectrum Disorder and Considering Neuroethical Implications. In: Illes J, Sahakian BJ, editors. Oxford Handbook of Neuroethics. Oxford: Oxford University Press (2011). doi: 10.1093/oxfordhb/9780199570706.013.0075
68. Allan DM, Lonigan CJ. Examination of the structure and measurement of inattentive, hyperactive, and impulsive behaviors from preschool to grade 4. J Abnorm Child Psychol. (2019) 47:975–87. doi: 10.1007/s10802-018-0491-x
69. Willcutt EG. The prevalence of DSM-IV attention-deficit/hyperactivity disorder: A meta-analytic review. Neurotherapeutics. (2012) 9:490–9. doi: 10.1007/s13311-012-0135-8
70. Faraone SV, Biederman J, Mick E. The age-dependent decline of attention deficit hyperactivity disorder: a meta-analysis of follow-up studies. Psychol Med. (2006) 36:159–65. doi: 10.1017/S003329170500471X
71. Gibbins C, Weiss MD, Goodman DW, Hodgkins PS, Landgraf JM, Faraone SV. ADHD-hyperactive/impulsive subtype in adults. Ment Illn. (2010) 2:41–5. doi: 10.4081/mi.2010.e9
72. de Nijs PFA, Ferdinand RF, Verhulst FC. No hyperactive–impulsive subtype in teacher-rated attention-deficit/hyperactivity problems. Eur Child Adolesc Psychiatry. (2007) 16:25–32. doi: 10.1007/s00787-006-0572-1
73. Sharma L, Markon KE, Clark LA. Toward a theory of distinct types of “impulsive” behaviors: A meta-analysis of self-report and behavioral measures. Psychol Bull. (2014) 140:374–408. doi: 10.1037/a0034418
74. Reynolds B, Ortengren A, Richards JB, de Wit H. Dimensions of impulsive behavior: Personality and behavioral measures. Pers Individ Differ. (2006) 40:305–15. doi: 10.1016/j.paid.2005.03.024
75. American Psychiatric Association DS, Association AP. Diagnostic and statistical manual of mental disorders: DSM-5 Vol. 5. Washington, DC: American psychiatric association (2013). doi: 10.1176/appi.books.9780890425596
76. Attoe DE, Climie EA. Miss. Diagnosis: A systematic review of ADHD in adult women. J Atten Disord. (2023) 27(7):645–57. doi: 10.1177/10870547231161533
77. Williamson D, Johnston C. Gender differences in adults with attention-deficit/hyperactivity disorder: A narrative review. Clin Psychol Rev. (2015) 40:15–27. doi: 10.1016/j.cpr.2015.05.005
78. Young S, Adamo N, Ásgeirsdóttir BB, Branney P, Beckett M, Colley W, et al. Females with ADHD: An expert consensus statement taking a lifespan approach providing guidance for the identification and treatment of attention-deficit/hyperactivity disorder in girls and women. BMC Psychiatry. (2020) 20:404. doi: 10.1186/s12888-020-02707-9
Keywords: ADHD (attention-deficit hyperactivity disorder), adolescence, young Adult, self-report ADHD symptoms, factor structure, Strengths and Weaknesses of ADHD Symptoms and Normal Behavior Scale
Citation: Vajsz K, Paulina LR, Trejo S, Andaverde-Vega AA, Swanson JM and Miklósi M (2024) Psychometric properties of the self-report version of the Strengths and Weaknesses of ADHD Symptoms and Normal Behavior Scale in a sample of Hungarian adolescents and young adults. Front. Psychiatry 15:1330716. doi: 10.3389/fpsyt.2024.1330716
Received: 31 October 2023; Accepted: 10 June 2024;
Published: 04 July 2024.
Edited by:
Pietro Cipresso, University of Turin, ItalyReviewed by:
Hakan Öğütlü, Cognitive Behavioral Psychotherapies Association, TürkiyeCopyright © 2024 Vajsz, Paulina, Trejo, Andaverde-Vega, Swanson and Miklósi. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Kornél Vajsz, dmFqc3oua29ybmVsQHNlbW1lbHdlaXMuaHU=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.